reliability and validity of a scale for measurement of
TRANSCRIPT
Arq Neuropsiquiatr 2011;69(4):636-641
636
Article
Reliability and validity of a scale for measurement of trunk mobility in Parkinson’s diseaseTrunk Mobility Scale
Clarissa R.C. Franco1, Paula Leão2, Raquel Townsend3, Carlos R.M. Rieder4
ABSTRACTAxial rigidity is an important motor manifestation in Parkinson’s disease (PD). Trunk mobility impairment can cause gait, balance and postural problems. However, only few instruments analyze the trunk mobility in PD patients. The aim of this study is to present a new Trunk Mobility Scale (TMS) and its validation in PD. The TMS constituted of dynamic tests involving trunk movements in sagittal, transversal and coronal planes. Ninety eight PD patients and 31 normal controls were analyzed. A strong correlation was found between the TMS scores and the Hoehn & Yahr staging scale (r: 0.72; p<0.01), motor Unified Parkinson’s Disease Rating Scale (r: 0.84; p<0.01) and Schwab and England Activities of Daily Living (r: –0.72; p<0.01). The scale showed a satisfactory reliability rate (αCronbach: 0.85, ICC: 099). TMS is a simple and reliable instrument to evaluate trunk mobility impairment in patients with PD. Key words: Parkinson’s disease, Trunk Mobility Scale, rigidity.
Confiabilidade e validade de uma escala de mensuração da mobilidade do tronco na doença de Parkinson: Escala de Mobilidade de Tronco
RESUMORigidez axial é importante manifestação motora na doença de Parkinson (DP). Prejuízos na mobilidade do tronco podem ocasionar problemas na marcha, equilíbrio e postura. No entanto, poucos instrumentos analisam a mobilidade do tronco em pacientes com DP. O objetivo deste estudo é apresentar uma nova Escala de Mobilidade do Tronco (TMS) e sua validação na DP. A TMS é constituída de provas dinâmicas que envolvem os movimentos do tronco no plano sagital, transversal e coronal. Noventa e oito pacientes com DP e 31 controles normais foram analisados. Uma forte correlação foi encontrada entre os escores do TMS e os do Hoehn & Yahr Staging Scale (r: 0,72; p <0,01), Unified Parkinson’s Disease Rating Scale (r: 0,84; p<0,01) e Schwab and England England Activities of Daily Living (r: –0,72, p <0,01). A escala mostrou uma taxa de confiabilidade satisfatória (αCronbach: 0,85; ICC: 099). TMS é um instrumento simples e confiável para avaliar comprometimentos da mobilidade de tronco em pacientes com DP.Palavras-chave: doença de Parkinson, Escala de Mobilidade de Tronco, rigidez.
CorrespondenceCarlos R.M. RiederHCPA - Serviço de Neurologia Rua Ramiro Barcelos 235090035-903 Porto Alegre RS - BrasilE-mail: [email protected]
SupportFinancial support granted by the Fundo de Incentivo a Pesquisa e Eventos (FIPE) of the Hospital de Clínicas de Porto Alegre
Conflicts of interestThe authors report no conflict of interest
Received 13 March 2011Accepted 6 April 2011
Study conducted at the Hospital de Clínicas de Porto Alegre (HCPA), Porto Alegre RS, Brazil. 1Department of Physical Therapy, HCPA; 2Physiotherapy, Santa Casa de Porto Alegre, Porto Alegre RS, Brazil; 3Medical School, Universidade Federal do Rio Grande do Sul, Porto Alegre RS, Brazil; 4Movement Disorders Clinic, Neurology Service, HCPA.
Parkinson’s disease (PD) is a degenera-tive and progressive disease that presents bradykinesia, tremor at rest, postural in-stability and rigidity as main motor man-ifestations1-3. Axial rigidity can be respon-
sible for functional impairments of gait, balance and motor control4-6. Although axial rigidity is one incapacitating charac-teristics of disease, most methods for as-sessing muscle tone have focused on ap-

Arq Neuropsiquiatr 2011;69(4)
637
Parkinson: Trunk Mobility ScaleFranco et al.
pendicular rigidity including the arms, wrists, and knees. Many researchers suggest that axial rigidity may be re-sponsible for trunk en bloc turning movement, charac-teristic in patients with PD7-9. Furthermore, alteration in tonus and mobility of trunk may affect the daily activi-ties and the quality of life of PD patients. Axial rigidity may cause difficulty in rolling over in bed and standing up when in sitting position5,6,10.
In order to monitor the disease progress or even the effectiveness of a certain medication or physiotherapeutic action, fast assessment mechanism of easy clinical ac-cess are required to help health professionals2, 11,12. Most available studies analyze the rigidity of limbs, neglecting however, the movement alterations that the axial rigidity causes to a patient with PD13,14. Besides insufficient lit-erature on that, the tools that assess the trunk mobility are scarce and restricted to the movement quantification in the transversal plane (rotation)15-17. Although some scales associate the rotation assessment with forward in-clination measurements (sagittal plane)18, flexion mea-surement is not part of any integrated scale that quan-tifies the two movement planes in a single instrument.
Scales for the trunk movement assessment in patients with PD include the Functional Rotation Test (FRT)15 and the Functional Axial Rotation (FAR)18. Both scales re-quire a special infrastructure, such as rooms with gradua-tion marks on the walls, referential points attached to pa-tients and/or tripods to enable the execution of tasks and measurements, which makes them of difficult clinical uti-lization. Another important limitation of the FRT scale is that it is not easy to collect data from individuals with ac-centuated tremor at rest and dyskinesia, as these patients have difficulty in keeping the final position required for such measurement16. On the other hand the FAR scale evaluates only one movement plane (transversal) and it is not predictor of functionality18. The Trunk Impair-ment Scale (TIS) was validated to PD9. However, this scale was originally created to evaluate the static bal-ance, the dynamic balance and the coordination in pa-tients with cerebral vascular accident and one limitation of this scale is that it does not evaluate the sagittal plane.
This study aims to create and validate an instrument for trunk mobility evaluation of patients with PD. The instrument, named Trunk Mobility Scale (TMS), evalu-ates trunk movement in all planes (sagittal, coronal and transversal).
METHODThe study involved 98 patients with diagnosis of PD
according to the criteria of the UK Parkinson’s Disease Society Brain Bank19. Patients were recruited from the Movement Disorder Clinic of Hospital de Clínicas de Porto Alegre RS, Brazil. The study had the participation
of 31 controls, healthy subjects, recruited for this study among patient’s relatives and companions. Exclusion cri-teria included diagnosis of other neurological diseases (ataxia, cerebral vascular accident, dementia etc.), ortho-pedic surgeries (spine arthrodesis at any level) and trau-matological and orthopedic diseases (fracture, arthrosis), that prevented the tests from being performed.
ProceduresPatients in the study were evaluated using Unified
Parkinson’s Disease Rating Scale-III (UPDRS-III)20,
Schwab and England Activities of Daily Living (S&E)21 and Hoehn & Yahr scale (H&Y)22. Disease duration, gender and age were controlled.
The TMS was based on six dynamic tests that in-volve the trunk movements in the sagittal plane (exten-sion/flexion), transversal (rotation) and coronal (side in-clination) and one static test that evaluated the sitting posture. The tests were performed with the patient sit-ting on a chair, with no arm support, feet on the floor and the back kept 10 cm from the chair. All movements were previously demonstrated to the patient by the study investigator.
Scores of dynamic items ranges from 0 to 3. The pa-tient that performs the movement with no compensation receives score 0. The patient that is unable to make the requested movement receives score 3. Scores 1 and 2 are attributed to individuals that perform the movements, but with compensations. The score is 1 for small com-pensations, and 2 for great compensations. Great com-pensations are exaggerated movements, easily noticed by an investigator (for instance, when inclining side-ways, the patient associate trunk rotation and/or flexion and/or extension movements). Small compensations are subtle movements, but that are present when the move-ment is performed. In the static aspect, the sitting pos-ture analysis may range from 0 (upright sitting position) to 4 (strong flexion and/or side inclination with extreme posture abnormality). In the other aspects, the posture may be severely, moderately and slightly inclined, items 3, 2 and 1, respectively.
A neurologist performed the UPDRS-III, S&E and H&Y scales. Two other investigators simultaneously re-corded the TMS scores. The investigators were blind re-garding the results obtained by one another in the TMS and were previously trained on how to apply the scales.
All patients and participants signed the Consent Term. This study was approved by the Research and Ethics Committee of the involved institution (HCPA).
Statistical analysisThe categorical variables were described through ab-
solute and relative frequencies. The quantitative variables

Arq Neuropsiquiatr 2011;69(4)
638
Parkinson: Trunk Mobility ScaleFranco et al.
were described through mean and standard deviation values. The criteria validation, i.e., the comparison to gold standards, was performed through the correlation with the scales: H&Y, UPDRS-III and S&E, and the in-strument proposed through Spearman’s Correlation Co-efficient and Pearson’s Correlation Coefficient (rs and r, respectively). A factorial analysis was performed to verify the specific domains of the scale. In order to assess the scale reliability, the internal consistence of the instru-ment was measured using Cronbach’s alpha (αCronbach) and the investigators’ agreement through the Intra-Class Correlation Coefficient (ICC). The significance level ad-opted in the study was p<0.05 and the application pro-gram SPSS (Statistical Package for Social Sciences) ver-sion 14.0 performed the analyses.
RESULTSNinety-eight patients with PD were assessed, 48 of
them were female (49%) and 50 were male (51%), pre-senting mean age of 67.23 (±11.25) and disease time of 7.88 (±5.22) years. The study also assessed 31 controls: 24 women (77%) and 7 men (22%), who presented mean age of 60.90 (±11.57) years. Table 1 shows the clinical characteristics of the sample.
Age and gender did not have influence on the TMS scores in patients and controls. The relation between age and the TMS was meaningless, with correlation rate of r=0.07. Gender did not show any influence on the TMS results either. Women obtained mean score of 5.61 (±4.70) and men obtained mean score of 5.95 (±4.91) in the TMS scale (p=0.69).
ReliabilityThe reliability rate between examiners of the pro-
posed scale was very significant, with ICC of 0.99. The
Table 1. Clinical characteristics of patients with Parkinson’s disease (PD) and controls.
PD group(n=98)
Controlgroup (n=31)
Age 67.23 (±11.25)* 60.90 (±11.57)*
Gender Female 48 (49%) 24 (77%)
Male 50 (51%) 7 (22%)
Diagnosis (years) 7.88 (±5.22) NA
Scales
TMS 6.75 (±4.92)* 2.64 (±2.43)*
UPDRS-III 31.84 (±24.09) NA
H&Y 2.66 (±1.12) NA
S&E 79.18 (±19.98) NA
TMS: Trunk Mobility Scale; UPDRS-III: Unified Parkinson’s Disease Rating Scale; H&Y: Hoehn and Yahr Scales; S&E: Schwab & England Activities of Daily Living Scale; NA: not assessed; *p<0.01.
Table 2. Reliability - Cronbach’s Alpha for Trunk Mobility Scale Items.
ICC αCronbachαCronbach if
item excluded
Trunk Mobility Scale 0.99 0.85
Inclination to righ 0.82
Inclination to left 0.82
Rotation to right 0.84
Rotation to left 0.84
Flexion 0.84
Extention 0.85
Sitting 0.83
Table 3. Factorial analysis of the Trunk Mobility Scale with rotation.
1 2
Values 3.21 1.99
% variation 45.89 28.46
% accumulative 45.89 74.35
Trunk Mobility Scale
Inclination to right 0.86 0.23
Inclination to left 0.87 0.20
Rotation to right 0.18 0.94
Rotation to left 0.22 0.93
Flexion 0.75 0.15
Extension 0.75 0.06
Sitting 0.71 0.34
Table 4. Correlation between the Trunk Mobility Scale and UPDRS-III items.
UPDRS-III TMS
Speech 0.56*
Facial expression 0.56*
Rest tremor 0.52*
Action tremor 0.41*
Rigidity 0.89*
Finger taps 0.64*
Hand movements 0.66*
Pronation/supination of hands 0.63*
Leg agility 0.70*
Arising from chair 0.60*
Posture 0.65*
Gait 0.65*
Postural stability 0.50*
Bradykinesia 0.65*
UPDRS-III: Unified Parkinson’s Disease Rating Scale; TMS: Trunk Mobility Scale. *p<0.01.
Arq Neuropsiquiatr 2011;69(4)
639
Parkinson: Trunk Mobility ScaleFranco et al.
internal consistence was high, with αCronbach of 0.85 (Table 2). This value did not change with the exclusion of any scale item.
Internal validationThe factorial analysis showed that the scale presents
two domains, with values over 1, which correspond to 74.35% of the total variance. Side inclination, flexion and extension movements and the static analysis of the sit-ting posture present similar values in the factorial anal-ysis. Therefore, all these variables are interrelated. The second domain was established by the rotation move-ments, which showed a different tendency from the others. Table 3 shows the factorial analysis data.
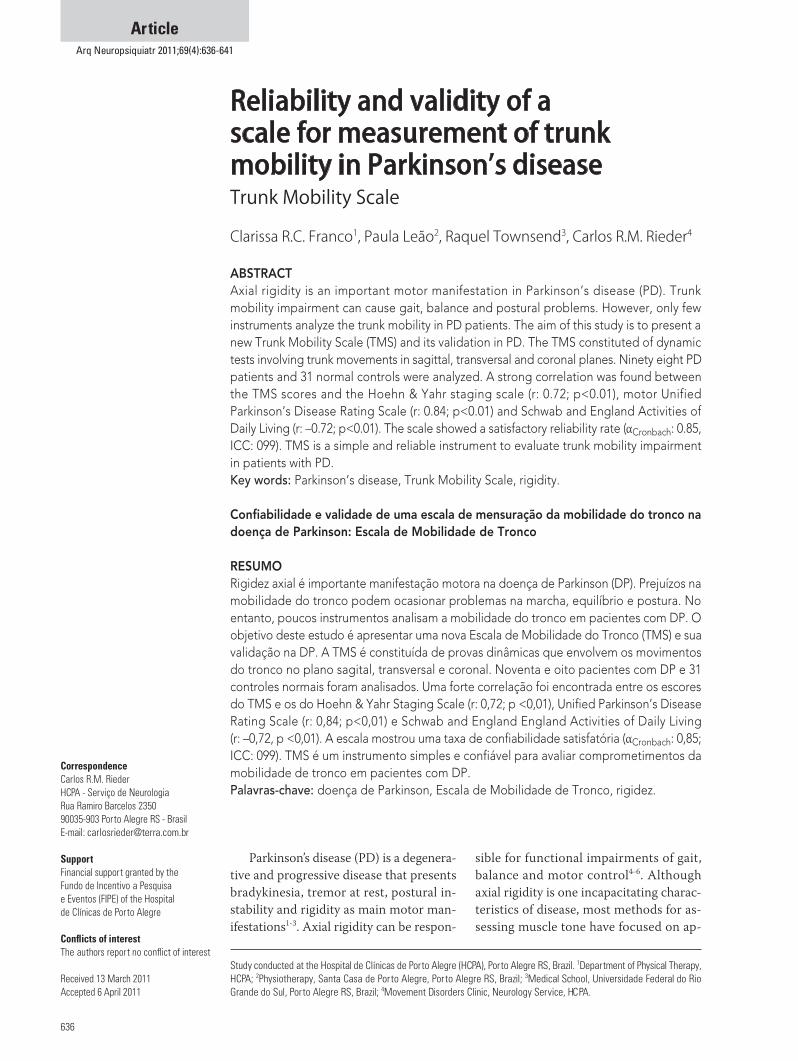
External validationThere was a high correlation between TMS and the
UPDRS-III, H&Y and S&E scales, with r : 0.84, 0.72 and
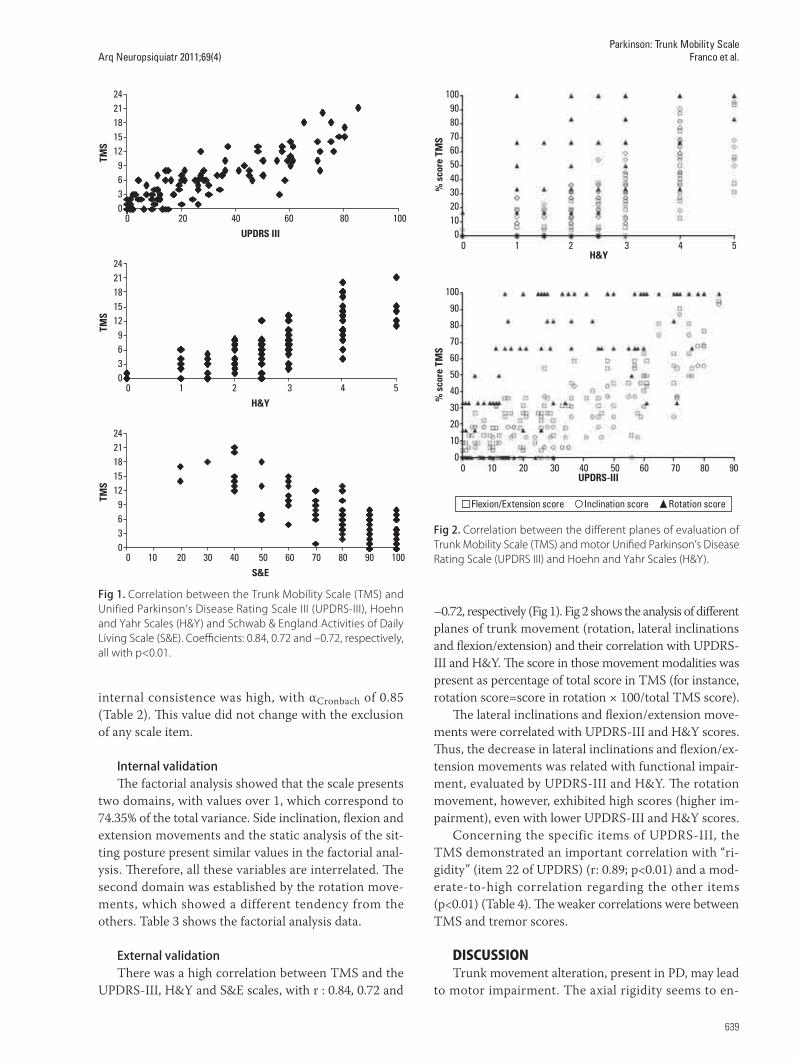
–0.72, respectively (Fig 1). Fig 2 shows the analysis of different planes of trunk movement (rotation, lateral inclinations and flexion/extension) and their correlation with UPDRS-III and H&Y. The score in those movement modalities was present as percentage of total score in TMS (for instance, rotation score=score in rotation × 100/total TMS score).
The lateral inclinations and flexion/extension move-ments were correlated with UPDRS-III and H&Y scores. Thus, the decrease in lateral inclinations and flexion/ex-tension movements was related with functional impair-ment, evaluated by UPDRS-III and H&Y. The rotation movement, however, exhibited high scores (higher im-pairment), even with lower UPDRS-III and H&Y scores.
Concerning the specific items of UPDRS-III, the TMS demonstrated an important correlation with “ri-gidity” (item 22 of UPDRS) (r: 0.89; p<0.01) and a mod-erate-to-high correlation regarding the other items (p<0.01) (Table 4). The weaker correlations were between TMS and tremor scores.
DISCUSSIONTrunk movement alteration, present in PD, may lead
to motor impairment. The axial rigidity seems to en-
24211815129630
0 20 40 60 80 100UPDRS III
TMS
24211815129630
0 1 2 3 4 5H&Y
TMS
24211815129630
0 10 20 30 40 50 60 70 80 90 100S&E
TMS
Fig 1. Correlation between the Trunk Mobility Scale (TMS) and Unified Parkinson’s Disease Rating Scale III (UPDRS-III), Hoehn and Yahr Scales (H&Y) and Schwab & England Activities of Daily Living Scale (S&E). Coefficients: 0.84, 0.72 and –0.72, respectively, all with p<0.01.
100908070605040302010
0
% s
core
TM
S
0 1 2 3 4 5H&Y
0 10 20 30 40 50 60 70 80 90UPDRS-III
100
90
80
70
60
50
40
30
20
10
0
% s
core
TM
S
Flexion/Extension score Inclination score Rotation score
Fig 2. Correlation between the different planes of evaluation of Trunk Mobility Scale (TMS) and motor Unified Parkinson’s Disease Rating Scale (UPDRS III) and Hoehn and Yahr Scales (H&Y).

Arq Neuropsiquiatr 2011;69(4)
640
Parkinson: Trunk Mobility ScaleFranco et al.
hance the loss of functionality in patients with PD in the execution of daily activities, such as walk, change direc-tion while walking or rolling over in bed4. Therefore, re-liable clinical measurements of trunk movement are re-quired to monitor the disease progress and its treatment effectiveness.
The Trunk Mobility Scale, validated by this study, evaluates PD patients in a satisfactory manner. It was showed that TMS is an easy and fast application scale. When compared with UPDRS scores, TMS shows strong correlation with that. UPDRS-III is a widely applied scale to evaluate motor PD symptoms23. However, it practically evaluated only appendicular rigidity. In UPDRS-III, axial mobility is only evaluated by the item that measure cer-vical rigidity.
The TMS presented good correlation with the H&Y, showing highest scores in advanced stages of the disease. The Schwab & England activities of daily living scale also presented a substantial correlation with TMS. Patients with higher scores in TMS showed more dependency to activities of daily living.
For clinical application, according to a systematic assessment of the scales utilized in PD, it has been rec-ommended the minimum level of Cronbach’s alpha of 0.7024,25. The internal consistence in this study was high, with αCronbach of 0.85. This value did not change with the exclusion of any scale item and all TMS items were sig-nificantly and positively associated with total score indi-cating a high inter correlation between all TMS items. Therefore, the investigator’s reliability of the TMS was excellent and the scale score is unlikely to present differ-ences due to different application interpretation.
Regarding the internal structure of the instrument, the factorial analysis showed that patients presented a similar performance in the following items: side inclina-tion, flexion, extension and sitting posture. However, re-garding the rotation assessment, the results showed to be independent of the others. Patients with worst score in flexion, stretching and inclination movements and in the sitting posture analysis presented worst performance in rotation. But patients with difficulty in performing only the rotation did not necessarily present difficulties in performing the other proposed movements. Our find-ings agree with the literature and indicate higher and premature difficulties to perform the trunk rotation movements6,26. This is clear when we observe that the rotation movement is altered early in the H&Y stage of disease in comparison to the other trunk movements. Therefore, patients with less severe disease, based in H&Y and UPDRS-III scales, may have already presented rotation impairments detected in TMS. The high pro-portion of subjects with early maximum rotation scores suggests a ceiling effect to rotation scores. This is dif-
ferent from the observed in flexion, extension and incli-nation movement impairment that are present in more advanced disease.
Analysis of different categorical items of the UPDRS-III showed that the TMS scores presented a significant correlation with them. Moreover, “rigidity” item showed the strongest correlation (r: 0.89), which emphasizes the important link between the trunk mobility and this symptom.
The performance in the TMS between controls and patients with PD, in terms of age and gender, did not show any significant difference. Therefore, the most im-portant factor to trunk mobility reduction in this study was the presence and severity of PD, result that agrees with the literature18.
The present study showed that the TMS is a func-tional and reliable instrument for clinical assessment of trunk mobility. Moreover it is of easy clinical utilization and can be useful to monitoring evolution and thera-peutic response in PD patients.
REFERENCES 1. de Goede CJ, Keus SH, Kwakkel G, Wagenaar RC. The effects of physical
therapy in Parkinson’s disease: a research synthesis. Arch Phys Med Rehabil 2001;82:509-515.
2. Schenkman M, Cutson TM, Kuchibhatla M, Chandler J, Pieper C. Reliability of impairment and physical performance measures for persons with Parkinson’s disease. Phys Ther 1997;77:19-27.
3. Wolters E. Variability in the clinical expression of Parkinson’s disease. J Neurol Sci 2008;266:197-203.
4. Bridgewater KJ, Sharpe MH. Trunk muscle performance in early Parkinson’s disease. Phys Ther 1998;78:566-576.
5. Carpenter MG, Allum JH, Honegger F, Adkin AL, Bloem BR. Postural ab-normalities to multidirectional stance perturbations in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2004;75:1245-1254.
6. Nikfekr E, Kerr K, Attfield S, Playford DE. Trunk movement in Parkinson’s disease during rising from seated position. Mov Disord 2002;17:274-282.
7. Lang AE, Lozano AM. Parkinson’s disease. First of two parts. N Engl J Med 1998;339:1044-1053.
8. Van Emmerik RE, Wagenaar RC, Winogrodzka A, Wolters EC. Identification of axial rigidity during locomotion in Parkinson disease. Arch Phys Med Rehabil 1999;80:186-191.
9. Verheyden G, Willems AM, Ooms L, Nieuwboer A. Validity of the trunk impairment scale as a measure of trunk performance in people with Parkinson’s disease. Arch Phys Med Rehabil 2007;88:1304-1308.
10. Horak FB, Dimitrova D, Nutt JG. Direction-specific postural instability in subjects with Parkinson’s disease. Exp Neurol 2005;193:504-521.
11. Brusse KJ, Zimdars S, Zalewski KR, Steffen TM. Testing functional perfor-mance in people with Parkinson disease. Phys Ther 2005;85:134-141.
12. Nieuwboer A, De Weerdt W, Dom R, Bogaerts K, Nuyens G. Development of an activity scale for individuals with advanced Parkinson disease: reliability and “on-off” variability. Phys Ther 2000;80:1087-1096.
13. Mak MK, Wong EC, Hui-Chan CW. Quantitative measurement of trunk rigidity in parkinsonian patients. J Neurol 2007;254:202-209.
14. Wright WG, Gurfinkel VS, Nutt J, Horak FB, Cordo PJ. Axial hypertonicity in Parkinson’s disease: direct measurements of trunk and hip torque. Exp Neurol 2007;208:38-46.
15. Batavia M, Gianutsos JG. Test-retest reliability of the functional rotation test in healthy adults. Percept Mot Skills 2003;96:185-196.
16. Batavia M, Gianutsos JG. Test-retest reliability of the seated Functional Rotation Test in people with Parkinson’s disease: a preliminary study. Percept Mot Skills 2004;99:259-270.
17. Schenkman M, Hughes MA, Bowden MG, Studenski SA. A clinical tool for measuring functional axial rotation. Phys Ther 1995;75:151-156.

Arq Neuropsiquiatr 2011;69(4)
641
Parkinson: Trunk Mobility ScaleFranco et al.
18. Schenkman ML, Clark K, Xie T, Kuchibhatla M, Shinberg M, Ray L. Spinal movement and performance of a standing reach task in participants with and without Parkinson disease. Phys Ther 2001;81:1400-1411.
19. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55:181-184.
20. Fahn S, Elton, RL, and Members of the UPDRS Development Committee. Unified Parkinson’s disease rating scale. In: Fahn SM, Calne D, Goldstein M (Eds). Recent Developments in Parkinson’s Disease: Macmillan Healthcare Information; 1987:153-163.
21. Martinez-Martin P, Gil-Nagel A, Gracia LM, Gomez JB, Martinez-Sarries J, Bermejo F. Unified Parkinson’s Disease Rating Scale characteristics and structure. The Cooperative Multicentric Group. Mov Disord 1994;9: 76-83.
22. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17:427-442.
23. Siderowf A, McDermott M, Kieburtz K, Blindauer K, Plumb S, Shoulson I. Test-retest reliability of the unified Parkinson’s disease rating scale in patients with early Parkinson’s disease: results from a multicenter clinical trial. Mov Disord 2002;17:758-763.
24. Gerlach J, Korsgaard S, Clemmesen P, et al. The St. Hans Rating Scale for extrapyramidal syndromes: reliability and validity. Acta Psychiatr Scand 1993;87:244-252.
25. Ramaker C, Marinus J, Stiggelbout AM, Van Hilten BJ. Systematic evalua-tion of rating scales for impairment and disability in Parkinson’s disease. Mov Disord 2002;17:867-876.
26. Stack EL, Ashburn AM, Jupp KE. Strategies used by people with Parkinson’s dis-ease who report difficulty turning. Parkinsonism Relat Disord 2006;12:87-92.