remediation of the medical learner of the struggling ... jama 2000; 284;1099-104. ... kern de, et...
TRANSCRIPT
Remediation of the Struggling 1
Medical LearnerJeannette Guerrasio, MD University of Colorado, School of Medicine

G l
2
Goals
Obt i B i U d t di f O St li R id t Obtain a Basic Understanding of Our Struggling Residents
Learn Early Identification Methods
Diagnose Learner Deficits
Create Successful Remediation Strategies Create Successful Remediation Strategies
Understand Remediation Outcomes
Legal Considerations
If time allows: Building the Necessary Infrastructureg y

A d
3
Agenda
O S li L 1 i Our Struggling Learners 15 minutes
Identification 25 minutes
Diagnosis 30 minutes
Remediation Plan Part I 20 minutes
***Break***
Remediation Plan Part II 40 minutes Remediation Plan Part II 40 minutes
Outcomes Data 5 minutes
L l C id i 30 i Legal Considerations 30 minutes
Adapting One’s Infrastructure ‐‐

4
How do you define remediation?How do you define remediation?

Wh t W K
5
What We Know
15%15%

Wh id tifi id t i diffi lt ?
6
Who identifies residents in difficulty?
/
N i
Patients and Families
The Resident Him/Herself
Other Residents
Attendings, Written Evals
Nursing
Attendings Verbal Evals
Program Directors
Other Residents
0 10 20 30 40 50 60 70 80 90
Chief Resident
Attendings, Verbal Evals
Yao DC and Wright SM. JAMA 2000; 284;1099-104.
0 10 20 30 40 50 60 70 80 90
Number of Responses
7
Importance
Time
Morale
Reputation Reputation
Patient Safety! .
Lavin B. Acad Med 1998;73(9):998-1002.
8
What struggles have you observed have you observed in your learners?y
.

9
Professionalism
Mental Well-Being
I t l Skill
Communication
F ll /Att di
Time Management & Organization
Interpersonal Skills Fellow/AttendingResidentStudent
Clinical Skills
Clinical Reasoning
0 5 10 15 20 25 30 35 40 45
Medical Knowledge
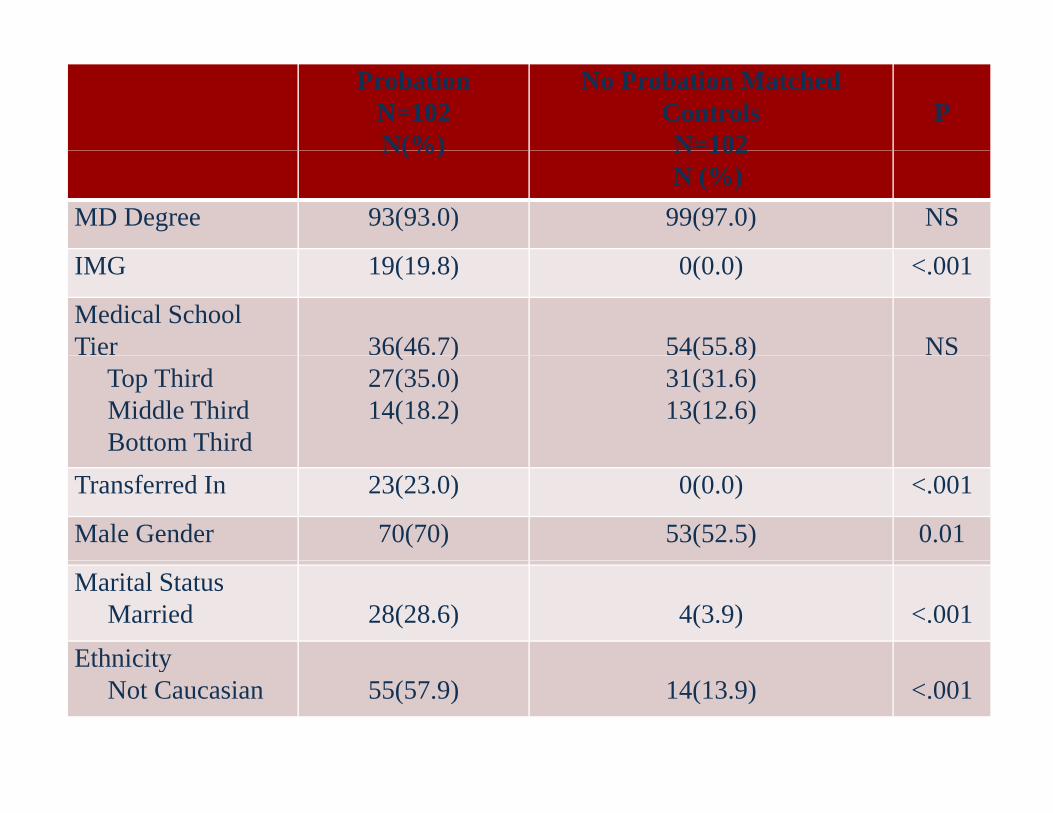
ProbationN=102N(%)
No Probation Matched ControlsN=102
PN(%) N 102
N (%)MD Degree 93(93.0) 99(97.0) NS
IMG 19(19.8) 0(0.0) <.001
Medical School Tier 36(46.7) 54(55.8) NS
Top ThirdMiddle ThirdBottom Third
( )27(35.0)14(18.2)
( )31(31.6)13(12.6)
Transferred In 23(23.0) 0(0.0) <.001
Male Gender 70(70) 53(52.5) 0.01
Marital StatusMarried 28(28.6) 4(3.9) <.001
EthnicityEthnicityNot Caucasian 55(57.9) 14(13.9) <.001

ProbationN=102
Mean (SD)
No Probation Matched ControlsN=102
PMean (SD) N 102
Mean (SD)Age 33.4(5.3) 30.6(3.3) <.001
Years between 2.2(5.1) 0(0) <.001
USMLE Step 1 211.3(17.5) 233.8(15.6) <.001
USMLE Step 2 208.9(22.4) 224.9(14.1) <.001
USMLE Step 3 205.2(13.3) 228.1(12.2) <.001

ProbationN(%)
ACGME Deficits1
Patient CareMedical Knowledge
65(65.0)60(60.0)
Interpersonal Skills and CommunicationProfessionalismSystems-based PracticeP ti b d L i d I t
31(31.0)70(70.0)10(10.0)13(13 0)Practice-based Learning and Improvement 13(13.0)

ProbationMean(SD)
Number of ACGME Deficits 2.5(1.4)
Post Graduate Year Placed on Probation 2 6(1 6)Post Graduate Year Placed on Probation 2.6(1.6)
Months on Probation 8.0(6.8)
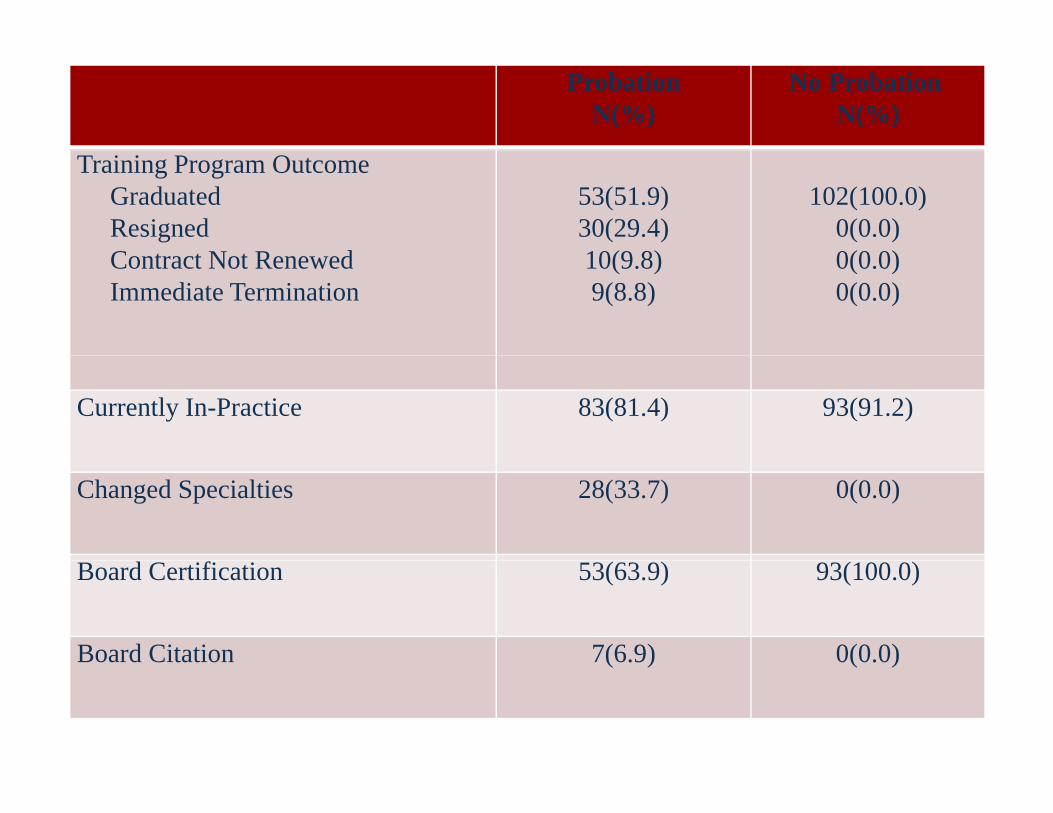
ProbationN(%)
No ProbationN(%)
Training Program OutcomeGraduatedResignedC t t N t R d
53(51.9)30(29.4)10(9 8)
102(100.0)0(0.0)0(0 0)Contract Not Renewed
Immediate Termination10(9.8)9(8.8)
0(0.0)0(0.0)
Currently In-Practice 83(81.4) 93(91.2)
Changed Specialties 28(33.7) 0(0.0)
Board Certification 53(63.9) 93(100.0)
Board Citation 7(6.9) 0(0.0)( ) ( )

OUTCOMESOUTCOMES
Once on probation they are more likely to: have adverse consequences
not graduate from their training program change specialties failure of board certification failure of board certification state medical board citations

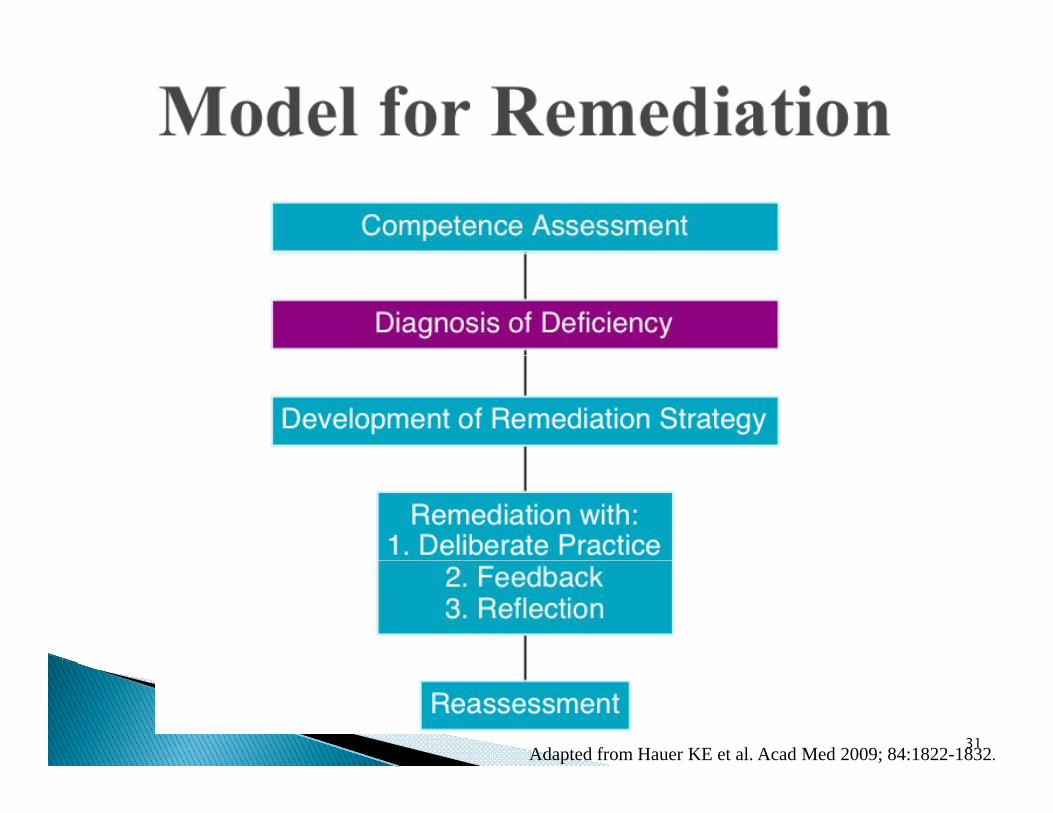
R di ti
16
Remediation
Limitations: Rare published evidence to guide Rare published evidence to guide
best practices in remediation
Advantages: Wealth of knowledge on this topic
Hauer KE. Acad Med 2009; 84(12):1822-1832.
17
Amaazon.ccom
18
Amaazon.ccom

Jeannette Guerrasio, MD
19

33Adapted from Hauer KE. Acad Med 2009; 84:1822-1832.

Poor grades in 1 or more clerkships USMLE <200 Need to repeat medical school courses
Sanfey H. Arch Surg. 2012;147(7):642-7.Eva, K.W. Med Educ. 2004, 38, 314-326. 21

Age >29
Sanfey H. Arch Surg. 2012;147(7):642-7.Eva, K.W. Med Educ. 2004, 38, 314-326. 22
Few glowing comments in letters of recommendationrecommendation,
Negative or neutral comments in thecomments in the deans letter
Transfers
Sanfey H. Arch Surg. 2012;147(7):642-7.Eva, K.W. Med Educ. 2004, 38, 314-326. 23

Multiple mini-interviews
Sanfey H. Arch Surg. 2012;147(7):642-7.Eva, K.W. Med Educ. 2004, 38, 314-326. 24

Coordinator input! Delayed completion of ERAS application
Sanfey H. Arch Surg. 2012;147(7):642-7.Eva, K.W. Med Educ. 2004, 38, 314-326. 25

Present a Case OSCEs 3D Task Group Project Personality Testing
26

Intrusive Interviewing
27

Formal written evaluations of competencies Formal written evaluations of competencies Peer assessments Examinations Examinations
Written Clinical performance
28

29

Verbal comments Reporting system for concerns Mid-rotation performance evaluations
43
Adapted from Hauer KE et al. Acad Med 2009; 84:1822-1832.31

a resident's actual ≠ perceived by thed f ddeficit attending
32

60
50Cougar
Attendings
40
20
30
10
20
0Att Int Com Pt care TM Reas Know
33
DO Principles and Practice Medical Knowledge Patient Care Interpersonal Skills and Communication Professionalism
P ti B d L i Practice-Based Learning Systems-Based Practice
47The Outcomes Project. Accreditation Council for Graduate Medical Education. 1999.

Medical Knowledge Patient Care◦ Clinical Skills
Clinical Reasoning◦ Clinical Reasoning◦ Organization & Time Management
Interpersonal Skills and Communicationp S C Professionalism Practice-Based Learningg Systems-Based Practice
48

Medical Knowledge Patient Care◦ Clinical Skills
Clinical Reasoning◦ Clinical Reasoning◦ Organization & Time Management
Interpersonal Skills and Communicationp S C Professionalism Practice-Based Learningg Systems-Based Practice Mental Well-being
49
50

1 Medical Knowledge1. Medical Knowledge2. Clinical Skills3. Clinical Reasoning and Judgment4. Time Management and Organization5. Interpersonal Skills and Communication6. Professionalism6. Professionalism7. Practice-Based Learning and Improvement8. Systems-Based Practice9. Mental Well-Being
51

Presentation◦ A history of poor exam scores◦ Unable to answer fact based questions
52
Presentation◦ During Presentations Extraneous information
Unable to focus Unable to focus Too many tests DifficultyDifficulty differential diagnosis analyzing diagnoses
i di id li i l / i id li individualizing protocols/practice guidelines
53
Presentationd d d b◦ Most evident during direct observation
◦ Physical exams lack key elements, are performed incorrectly or inaccurate information is obtainedy◦ Does not understand what type of information is
obtained by individual exam element ◦ Poor procedural/surgical skills◦ Poor procedural/surgical skills◦ Unable to answer technique questions about the
exam or procedure
41
Presentation◦ Unprepared for deadlines◦ Disorganized in appearance◦ Presentations and notes missing sections◦ Presentations and notes missing sections
and out of order◦ Arrival and departure times
42
Presentation◦ Recurrent episodes of misunderstandingRecurrent episodes of misunderstanding◦ Frequent interpersonal conflicts◦ Despite good knowledge and organization, the oral
presentations are poorp p Not as articulate Struggle to answer questions, in contrast to exam scores Struggle to convey information ie: diagnosis, plan or giving bad news
◦ Difficulty formulating and asking questions of their consultants◦ Struggle to sign out patients◦ Struggle to sign-out patients Severity of illness Tasks to be done
43

Presentation◦ Inappropriately dressed◦ Frequently late or absent, unreliable ◦ Dishonest◦ Dishonest◦ Try to pass off work ◦ Poor patient - doctor relationships◦ Specific unethical actions may be brought to
your attention
44
Presentation◦ Does not show evidence of self-directed
learning◦ Does not show evidence of reading◦ Does not show evidence of reading Not reviewing literature to answer patient care
questions◦ Does not seek or defensive with feedback◦ Does not understand own limitations
45

Presentation◦ Does not value interprofessional input◦ Neglects health care resources
Does not seek resources for patients◦ Does not seek resources for patients◦ Neglects transitions of care
46

Presentationh◦ Anything
◦ Inconsistency
47***BREAK***

Make sure the learner Actual Make sure the learner receives the feedback as soon as possible 1
Actual
0
0.5
men
t da
rd-1
-0.5or
e A
sses
smtiv
e to
Sta
nd
-2
-1.5
Bottom Third
Middle Third
Top Third
Z-Sc
oR
elat
63
Third Third
Level of Resident By Expert Assessment
Hodges B Acad Med 2001;76(10 S):S87-9.

Make sure the learner Actual Perceived Make sure the learner receives the feedback as soon as possible
0 5
1
Actual Perceived
0 5
0
0.5
men
t da
rd
1 5
-1
-0.5or
e A
sses
smtiv
e to
Sta
nd
-2
-1.5
Bottom Third
Middle Third
Top Third
Z-Sc
oR
elat
64
Third Third
Level of Resident By Expert Assessment
Hodges B Acad Med 2001;76(10 S):S87-9.

Medical Studentl k h◦ Clerkship Director
◦ Office of Student Affairs at the SOM◦ Remediation Team
Resident or Fellow◦ Program Director◦ Program Director◦ Dean of Graduate Medical Education◦ Remediation Team
50
52
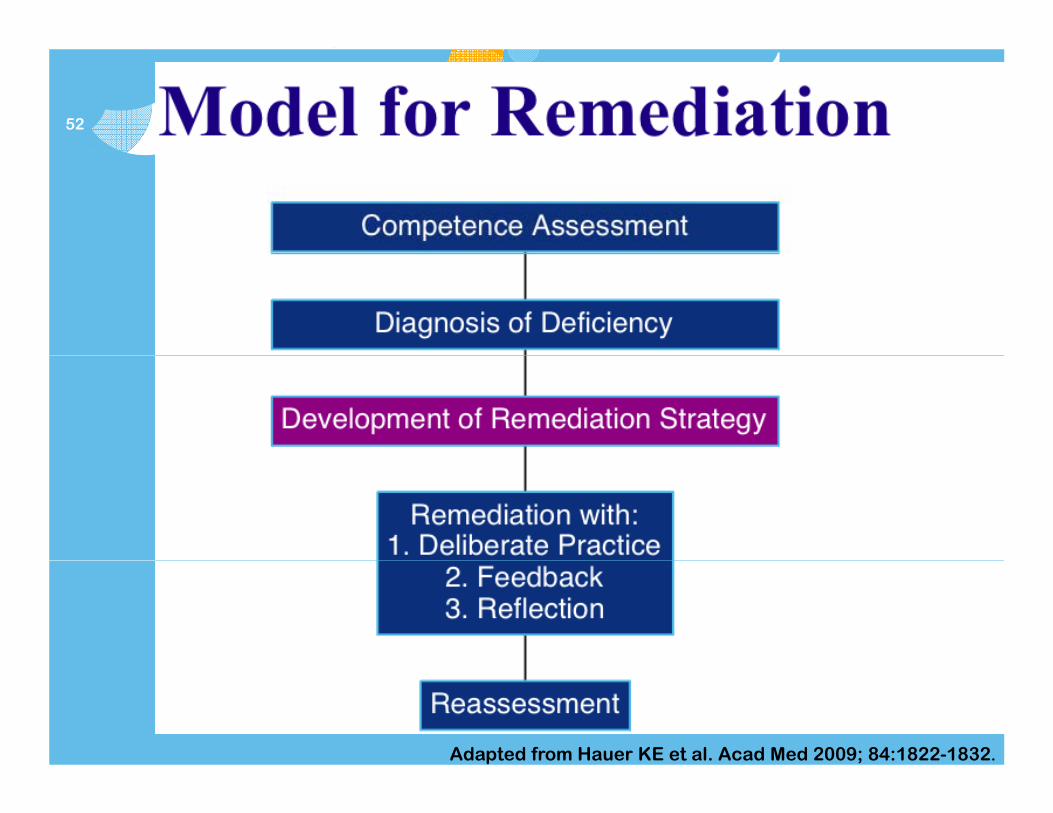
Adapted from Hauer KE et al. Acad Med 2009; 84:1822-1832.

53
R di ti St tRemediation Strategy
The goal of remediation is to target and fix: is to target and fix:
the greatest deficit!the greatest deficit!

54
Adapted from Hauer KE et al. Acad Med 2009; 84:1822-1832.

55
56
57
Cli i l R iClinical Reasoning
Deliberate PracticeDeliberate Practice
F k f ti F k f ti ddddFramework for creating a Framework for creating a ddxddx
Create Create ddxddx: age, gender, : age, gender, / th i it & / th i it & race/ethnicity, & ccrace/ethnicity, & cc
FeedbackFeedback
Use BackUse Back--up resourcesup resources

58
Cli i l R iClinical Reasoning
ReflectionReflection
Update list of differential Update list of differential diagnosesdiagnoses
What was missing? What was What was missing? What was more or less prevalent?more or less prevalent?pp

59
Cli i l R iClinical Reasoning
Deliberate Practice ContinuedDeliberate Practice Continued
C d t t diC d t t diCompare and contrast diagnosesCompare and contrast diagnoses

Presenting Symptom: Chest Pain
Symptoms and historical info.
Signs Diagnostic Work-up
Treatment60
Chest Pain
GERD Subacute, epigastric, burning supine
Tenderness to palpation of the
History alone, Abnormal EGD
Raise head of bed, change diet avoid burning, supine,
relief with antacids
the epigastrium
diet, avoid tobacco and alcohol, weight loss, H2 blocker, PPI
Stable Angina
Male, advanced age, pressure with radiation to
May have murmur, lateral PMI gallop
Abnormal EKG, Dynamic EKG, Stress test
Modify risk factors such as weight with radiation to
arm or jaw, exertional, +/-SOB, nausea,
H N HL
PMI, gallop, paradox split S2, or normal
Stress test, Cath
as… weight reduction, DM control, HTN control,
ki DM, HTN, HLD, tobacco,+ FmHx
smoking cessationASA, statin, +/-ACE-I ACE I B-blocker, NTG
Etc.
Blankenburg R. et al.. PAS May 2011.

61
Rhinorrhea Wheezing Unilateral Fever No edemaRhinorrhea Wheezing Unilateral crackles
Fever No edema
Deliberate PracticeDeliberate Practice
Review CasesReview Cases
Pna Review CasesReview Cases
CHF
Etc.
Blankenburg R. et al.. PAS May 2011.

62
Cli i l R iClinical Reasoning
Receiving FeedbackReceiving Feedback
ReRe enforce the use of resources and enforce the use of resources and ReRe--enforce the use of resources and enforce the use of resources and seniors or consultants for feedbackseniors or consultants for feedback

63
Cli i l R iClinical Reasoning
ReflectionReflection
Reflect on the identifying differences Reflect on the identifying differences Reflect on the identifying differences Reflect on the identifying differences between diagnoses between diagnoses
What questions would be pertinent while What questions would be pertinent while What questions would be pertinent while What questions would be pertinent while taking a history?taking a history?

64
I GIn Groups
Develop a remediation plan for Develop a remediation plan for your scenario that includes:your scenario that includes:your scenario that includes:your scenario that includes:
deliberate practicedeliberate practiceppfeedback and feedback and
reflectionreflectionreflectionreflection
65
C #1Case #1

66
Th D tThe Data
Unprofessional behavior in medical schoolUnprofessional behavior in medical school
Subsequent disciplinary action by the state Subsequent disciplinary action by the state medical boardmedical boardmedical boardmedical board
Papadakis MA, et al. N Engl J Med 2005; 353:2673-82.Kern DE, et al. Curric Devel for Med Educ. 2009; p 67.

67
Th D tThe Data
Unprofessional behavior in medical schoolUnprofessional behavior in medical school
Subsequent disciplinary action by the state Subsequent disciplinary action by the state medical boardmedical boardmedical boardmedical board
Papadakis MA, et al. N Engl J Med 2005; 353:2673-82.Kern DE, et al. Curric Devel for Med Educ. 2009; p 67.
68
G ti YGeneration Y
Generation MeGeneration Me
Millennial GenerationMillennial GenerationMillennial GenerationMillennial Generation
Peter Pan GenerationPeter Pan Generation
Generation WHY?Generation WHY?Generation WHY?Generation WHY?

69
Generation Y
ConfidenceConfidence
ToleranceToleranceToleranceTolerance
EntitlementEntitlement
NarcissismNarcissism
Desire to Be WealthyDesire to Be WealthyDesire to Be WealthyDesire to Be Wealthy
Helicopter ParentsHelicopter Parents
MediaMedia
70
The Adaptable Instructor
Avoid LecturesAvoid Lectures
Teach ContextuallyTeach Contextually
Rewards and Rewards and ConsequencesConsequencesTeach ContextuallyTeach Contextually
Role ModelRole Model
Feedback from Stable Feedback from Stable PersonPerson
Use TechnologyUse Technology
Acknowledge Technology Acknowledge Technology
PersonPerson
Allowed to Reflect Allowed to Reflect Aloud and DiscussAloud and DiscussFree TimesFree Times
Rules! (esp. Rules! (esp. professionalism)professionalism)
Aloud and DiscussAloud and Discuss
SchedulesSchedulesprofessionalism)professionalism)
ConsistencyConsistency

71
U i E t l RUsing External Resources
State Physician Health Program State Physician Health Program
Psychiatrists on Your Resident’s Insurance PanelPsychiatrists on Your Resident’s Insurance PanelPsychiatrists on Your Resident s Insurance PanelPsychiatrists on Your Resident s Insurance Panel
Human Resources DepartmentHuman Resources Department
OmbudsOmbuds OfficeOffice
Pastoral ServicesPastoral Services

72
Adapted from Hauer KE et al. Acad Med 2009; 84:1822-1832.

73
R tReassessment•• Repeat Repeat
l k hi /l k hi / t tit ti•• Chart reviews & ChartChart reviews & Chart--
ti l t d llti l t d llclerkships/clerkships/rotationsrotations•• Standardized Standardized patient patient
encounters & encounters & simulationsimulationDi tl Di tl b d b d
stimulated recallstimulated recall•• MultiMulti--source evaluationssource evaluations•• Arrival and Departure Arrival and Departure
TiTi•• Directly Directly observed observed encounters in clinical encounters in clinical environmentenvironmentW itt W itt b b b d b d
TimesTimes•• AttendanceAttendance•• AttireAttire
R t lfR t lf•• Written Written or webor web--based based assessmentsassessments
•• Chart Chart reviews & Chartreviews & Chart--ti l t d ti l t d llll
•• Responses to selfResponses to self--assessment assessment
•• Patient and procedure Patient and procedure l l stimulated stimulated recallrecall logs logs
74
O t D tOutcomes Data

75
ou
rsty
Tim
e in
Ho
Fa
cu
lt

76
Value of Faculty Time?y
the odds of probation the odds of probation by 3.1% by 3.1% per hour per hour pp
negative outcomesnegative outcomes by 2 6% perby 2 6% per negative outcomes negative outcomes by 2.6% per by 2.6% per hourhour

100%
Terminated77
60%
80%Terminated
Withdrew
40%
60%Transferred but Did Not Graduate
20%
40%Probation/Restricted PracticeT f d d
0%
20% Transferred and GraduatedGood StandingGood Standing
Graduated
78

79
SSummary
IDENTIFYIDENTIFY
DIAGNOSEDIAGNOSE
REMEDIATE withREMEDIATE with
DELIBERATE PRACTICEDELIBERATE PRACTICE
FEEDBACKFEEDBACK
REFLECTION IN ACTIONREFLECTION IN ACTION
Success for teacher, learner and patients!Success for teacher, learner and patients!

Jeannette Guerrasio, MD
80

Not all students who start Not all students who start medical school shouldgraduate
... but they ydo.
81
Michael aced his first two years of medical Michael aced his first two years of medical school, honoring every course. This success fuels his arrogant confrontational
li D i d f db k f personality. Despite repeated feedback from faculty and peers his behavior does not change. While his reputation for challenging change. While his reputation for challenging interpersonal interactions worsens throughout the clerkship years, these concerns never appear on his written evaluations and he continues to do well academically graduates and matches into a academically, graduates and matches into a residency program.
82
Early in internship, while on his way home from an “end-of-rotation” celebration he is from an end-of-rotation celebration he is in a bike accident during which he sustains a closed head injury. After one week in the hospital, he has recovered from the acute injuries and starts his second rotation. His unprofessional behavior and poor unprofessional behavior and poor interpersonal skills continue unabated on his return and he is referred for remediation. f fDuring the remediation process, the team also notices that he is having difficultly processing information It is unclear if this processing information. It is unclear if this is new from his head injury or if this deficit was present during his medical school years. p g y
83

Finding addition financial resourcesg To lengthen training Provide one-one teaching
Additi l b k i Additional books or review courses, Time with standardized patients or in simulation labs
Institutional culture Institutional culture Patient safety Student’s effort and abilities Schedule flexibility Limited trained faculty to conduct remediation Faculty time for direct observation and feedback
84

Recurrent unprofessional behavior - when a Recurrent unprofessional behavior when a cause cannot be elucidated and remediated
Egregious unprofessional behavior including criminal activity
Poor insight into deficits A learner that appears “not teachable” Refusal to participate in remediation
85
Used to convince a student or resident that Used to convince a student or resident that they have a deficiency
Gives the remediation team information to build a remediation strategy
Used to justify grades, remedial actions, and di i l dismissal.
Protects individuals and institutions from legal action legal action.
86

87

Expected performance for each course and Expected performance for each course and each academic year written goals and objectives defined performance targets grading policies consequences for failure to meet expectations consequences for failure to meet expectations which may also include an outline of the procedures
for remediation, probation and dismissal
88

Identification of the Learner’s Deficits Identification of the Learner s Deficits Compile: e-mail communications or written
evaluations, assessments from multiple sources d l th i t th d i dand place them into the academic record
Documentation of comments regarding a learner’s performance is as valid for making p gacademic decisions as written evaluation forms.
89
Academic discussions about the learner summary of each meeting
held to discuss the learner’s held to discuss the learner s academic progress with date and list of
attendeesattendees
document decisions to share performance difficulties with upcoming faculty and with upcoming faculty and your reasoning note if the learner was
notifiednotified
90

Each document should include Each document should include the date of observation or identification of
deficit(s) who made the observation specific examples of objective behaviors or
actions that highlight the deficiency(ies)actions that highlight the deficiency(ies) whether or not feedback was given to the learner
(ideally with proof)
91

Documentation that all residents (including Michael) received directions on how to access each rotation’s and received directions on how to access each rotation’s and post graduate year’s expectations for competent performance.
A dated e-mail from a faculty member reporting that y p gMichael’s interpersonal skills and professionalism are poor, which included, “Michael often brags about his grades in front of other residents. Whenever residents in conference are discussing a case, he interrupts the conversation to g pshout out the answer and follows with a comment about how easy the cases are… this behavior continues despite two breakfast conversations with me during which I gave him respectful but direct feedback and suggested he cut-it-out!.”
A dated e-mail from another faculty member reporting that Michael doesn’t let his simulation lab partner participate, because as he states “he can do a better job”. participate, because as he states he can do a better job .
92

Notes documenting unsolicited feedback by the resident’s clinic preceptor In the conversation the preceptor clinic preceptor. In the conversation, the preceptor expressed that “Michael continues to interrupt her while she is speaking with patients, to provide advice that is often incorrect… confronts her about patient care decisions in front of patients uses inappropriate jargon decisions in front of patients… uses inappropriate jargon and is arrogant with patients, often talking to them as if they are children, i.e. You are supposed to exercise. Do you know what that means?”
There are four meetings with the resident and his advisor, dated and documented by the advisor with follow up emails summarizing the conversations and consequences of ongoing difficulties. The e-mails also contained a list of recommended resources to assist with these skills. Upon request, Michael acknowledged having received each summary e-mail.
A letter from Michael requesting an excused absence to A letter from Michael requesting an excused absence to recover from his bicycle accident.
93

A letter granting his request. A current grade transcript A documented conversation between a peer and the Dean
of Graduate Medical Education, in which the peer reported that Michael has been drinking alcohol excessively outside that Michael has been drinking alcohol excessively outside of work.
2 additional e-mails from his rotation attending describing Michael’s inability to work with the other residents and students on his team “Michael often interrupts the other students on his team. Michael often interrupts the other intern’s presentation with additional information or with the plan” “He is not respectful of the other residents’ time consistently interrupting and when he asks if he could help the team he says he wants to help because he can get the the team, he says he wants to help because he can get the work done faster.”
A dated e-mail referring him to the remediation team, letting Michael know that they will be given access to his
i d i dentire academic record.
94

the competency being addressed the competency being addressed a specific description of the behaviors or
actions of concern the time frame for remediation the specific plan objective measures that will be used to
assess the deficit post remediation h d h l i d h the date the plan was communicated to the
learner provide either written evidence or a witness to a provide either written evidence or a witness to a
verbal conversation
95
Focused Review Probation Internal process Serves as a warning
prior to possible
Internal Process Serves as a warning
prior to possible p pprobation
Not considered disciplinary
p pdismissal
Is disciplinary Is reported to outside
Not reported to outside reviewers
Is reported to outside reviewers future education
programs employers credentialling agencies insurers
96

97

Promotions committee meeting date(s) when decision d t h th d i t t f d was made to change the academic status from good
to focused review, Date that the status change will take effect,
Deficit(s) or competencies to be remedied Deficit(s) or competencies to be remedied, Summary of the information that led to the decision,
including source of information, assessment technique and format such as written or verbal technique, and format such as written, or verbal.
Date when the learner’s status will be reassessed, typically 90 days after change in status,
Performance or actions required to reverse the Performance or actions required to reverse the change in academic status, and how that will be measured,
Consequences for achieving or failing the reassessment.
98

Following 4 weeks of remediation Michael g ffailed his reassessment. The Residency Review and Education Committee reviewed his entire academic record He was then his entire academic record. He was then invited to appear before the committee to present his grievances. The promotions committee decided to skip a warning or committee decided to skip a warning or focused review and to place him directly on probation because of his rotation failure, failure to progress, and because he refused neuropsychiatric testing and alcohol and drug monitoring.g g
99
Medical students and residents are Medical students and residents are increasingly resorting to grievance committees and the judicial system.
Faculty and institutions need to be prepared to defend:
Dismissal Dismissal Admission Allegations of Cheatingg g Retaking work
100
Adhere to your institution’s policies!Adhere to your institution s policies!
101
Students (residents) are protected under the 14th( ) pamendment protects property and liberty interests and requires
the right of procedural due process g p p
Translation: the learner must be notified of the deficiencies, a warning of potential consequences, , g p q ,and given adequate time to prepare prior to an opportunity for a hearing to air grievances and share their perspective
L h ld b ll d h i f Learners should be allowed to have a witness present for the hearing, attorneys may be denied access to these proceedings
An appeals process is not required for due process, An appeals process is not required for due process, though it is recommended
102

Courts will review the documentation Courts will review the documentation presented and ask 3 questions: 1. Do the institutional rules follow the
i d b idi appropriate due process by providing notification of deficiencies, a warning of potential consequences, and an option to air their grievances (with or without a hearing)?
2. Did the institution follow its own rules? 3 Were the procedures equally applied to all 3. Were the procedures equally applied to all
students in a similar situation?
If yes, the the courts consider 3 principles...y , p p
103

Principle One: Judicial deference to the Principle One: Judicial deference to the professional judgment in reviewing the entire medical record of the student’s
fperformance. Principle Two: Judicial support of reasoned
academic decision making academic decision-making. Principle Three: Judicial nonintervention.
104

1. Courts will not reverse a decision as long as 1. Courts will not reverse a decision as long as the faculty reviewed the student’s entire academic record.
2. The faculty decision cannot be arbitrary or capricious, but based on facts and reason. (Students hold burden of proof)(Students hold burden of proof)
3. Courts will not overturn faculty decisionsunless there is clear evidence of arbitrary unless there is clear evidence of arbitrary and capricious action.
105
Students and residents have also sued facultyStudents and residents have also sued faculty members for libel
the court has found that negative evaluations are not defamatory if documentation shown only to those whodefamatory, if documentation shown only to those who need to know and the statements made are relevant to the evaluation
students and residents give implied consent for s ude s a d es de s g e p ed co se oevaluations to be used by the school or program when they enter an academic institution
106

Residents: Students or Employees?Residents: Students or Employees? Resident dismissals have been treated the same as
students and the same academic procedures and information appliespp
Despite the fact that residents are also employees, the courts have classified them as students.
Contract law does apply It is always easier to deny a resident their contract
renewal then to dismiss them mid contract. While waiting for a contract to expire, the resident may have th i t ti h d t li i l t i dtheir rotations changed to non-clinical or customized rotations.
107
Michael was evaluated by the Physicians Health Program. While he completed the alcohol and drug monitoring While he completed the alcohol and drug-monitoring program without incident, he refused their recommendations for psychotherapy. He never acknowledged that he had interpersonal skills problems, struggles with professionalism and poor clinical reasoning struggles with professionalism and poor clinical reasoning. Overall, he failed to progress. He continued to maintain that he was a leader among he peers. After much debate, the Residency Review and Education Committee decided not to renew his yearly contract Despite an initial fear of not to renew his yearly contract. Despite an initial fear of litigation and threatening letters from his lawyer, Michael never sought legal action.
Two years later, he requested a letter of recommendation from the residency program director, so that he could apply for another residency position. With the support of the Committee, the program director wrote a very honest and frank letter about his strengths and weaknesses, including why his contract had not been renewed.
108

Trainees are dismissed from medical school and id t i i residency training programs.
This is usually preceded by a carefully documented and rigorous attempt at remediation. When d e process has been ser ed and the When due process has been served and the institution’s policies are applied without discrimination, the courts have repeatedly upheld academic and disciplinary decisions made by medical p y yschool faculty.
Our job is to hold the learner accountable for their responsibilities and to point out the need for improvement as it arises improvement as it arises.
Medical schools and residency programs also have lawyers, to assist faculty and committees to ensure that they are following the school’s policies Consult that they are following the school s policies. Consult them early in the process.
109

Eva Aagaard, MD Maureen Garrity, PhD Carol Rumack, MD◦ [email protected]◦ www.clinicalremediation.com
110
111

112
Adapting One’s Infrastructure to Maximize Remediation Maximize Remediation
Jeannette Guerrasio, MDAssociate Professor of MedicineUniversity of Colorado School of Medicine
Faculty Development 2013

113
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• Faculty Development • Measurable Outcomes to Determine Success• Measurable Outcomes to Determine Success• Financial Resources and Institutional Backing

114
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• Faculty Development • Measurable Outcomes to Determine Success• Measurable Outcomes to Determine Success• Financial Resources and Institutional Backing

115
A System of Identificationy
• Establish thresholds
• Needs to be standardized ▫ to capture all struggling ▫ to capture all struggling
learners▫ to treat all fairly and y
consistently

116
Potential Thresholds• Course Failure• Written or Clinical Exam Score or Below 2 S D• Written or Clinical Exam Score or Below 2 S.D.• Evaluation Rating Scale Score• ≥2 Related Negative Comments g• Clinical or Procedural Error/Patient Safety
Concern I d t P d L• Inadequate Procedure Logs
• Violating Work Hours• ≥2 Reported Interpersonal Conflicts• ≥2 Reported Interpersonal Conflicts
117
Potential Thresholds
• ≥2 Unexcused AbsencesArriving Late or Leaving Early More Than 2x• Arriving Late or Leaving Early More Than 2x
• ≥2 reports of Unprofessional Behavior or 1 Egregious Act Egregious Act
• Incomplete assignment/requirements• Not Seeking Help When NeededNot Seeking Help When Needed• Inconsistent Performance• Not Improving/Not Teachablep g/• Health Impairing Work Performance
118
Potential Thresholds
• Asks all evaluators for all learners, if remediation is needed remediation is needed
• Also take self-referrals

119

120
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• Faculty Development • Measurable Outcomes to Determine Success• Measurable Outcomes to Determine Success• Financial Resources and Institutional Backing

Remediation Team
121
Remediation Team
Director
Medical Education Specialists
Mental Health
PractitionersSpecialists
Practicing Non-Cli i i
Practitioners
On Campus On I
Physicians H lth Practicing
Clinicians Clinician Educators
On Campus Wellness Insurance
PanelHealth
Program

122
Remediation Team
• Director ▫ to build and implement the program▫ to build and implement the program▫ lead creation of policies and procedures▫ know the institution’s technical standardsknow the institution s technical standards▫ monitor and modify the program▫ provide faculty development ▫ assist with the remediation of learners

123
Remediation Team
• Core Team of Remediation Specialists▫ diagnosis of learner deficits ▫ diagnosis of learner deficits ▫ development of remediation plans▫ assist with documentationassist with documentation▫ suggest reassessment methods

124
Remediation Team
• Core Team of Remediation Specialists▫ must be available to provide support to▫ must be available to provide support to each other in discussing complicated or challenging cases g p g g to learn from each other’s experiences
supervising facultyprogram/course directors program/course directors
the learner’s peers

125
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• A Faculty Development • Measurable Outcomes to Determine Success• Measurable Outcomes to Determine Success• Financial Resources and Institutional Backing
126
Faculty Development
• All Supervising Faculty▫ the program’s mission and philosophy▫ the program s mission and philosophy▫ how to access the program ▫ address expectationsaddress expectations▫ goals or outcomes▫ assist with documentation
127
128

129
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• Faculty Development • Measurable Outcomes to Determine • Measurable Outcomes to Determine
Success• Financial Resources and Institutional BackingFinancial Resources and Institutional Backing

130
Measuring Outcomesg
• Graduation outcomes: on-time, delayed, withdrawal dismissalwithdrawal dismissal
• Probation Rates• Exam Scores• Exam Scores• Successful entry into the next level of training or
career• Feedback from learner and supported faculty

131
Key Componentsy p
• A System of IdentificationA Remediation Team• A Remediation Team
• Faculty Development • Measurable Outcomes to Determine Success• Measurable Outcomes to Determine Success• Financial Resources and Institutional
BackingBacking
132
Financial Resources• Program director (FTE
20 to 50%)• Web-based tools• Clinical skills 5 )
• Remediation specialists (FTE<5%)Administrati e
Clinical skills examinations
• Practice procedural eq ipment • Administrative
assistance• Standardized patients,
equipment • Psychiatric services• Additional rotations p
simulation and lab fees• Video recordings• Written examinations
beyond standard training
• Research assistance• Written examinations, question banks
• Research assistance

133
Institutional Backingg
• National medical education organizations have strongly supported remediation of learnersstrongly supported remediation of learners▫ Some institutions are less inclined or able to devote concentrated resources to a small number of learners. ▫ Other institutions feel that it is their educational
i i d l bli timission and moral obligation.

134
Institutional Backingg• Consider:
Where might resistance to the program come from? Where might resistance to the program come from? How can your program meet shared goals? What local barriers do you anticipate?
C il t th ? Can you pilot the program? If your program is successful, how will your
institution respond to your publications which k l d h (lik ll i i i ) h acknowledge that you (like all institutions) have
struggling learners? What is their willingness to support faculty
development?
135
AcknowledgementsAcknowledgements
Eva Aagaard, MD Maureen Garrity, PhDC l k Carol Rumack, MD◦ [email protected]
li i l di ti◦ www.clinicalremediation.com