renaissance in anesthesia machine safety the modern anesthesia machine (workstation) &...
TRANSCRIPT
Renaissance in Anesthesia Machine Safety
The Modern Anesthesia Machine (Workstation) & Anesthesia Delivery Unit (ADU): Improved Safety Features
Charles G. McCombs, Jr. CRNA, BSA

Morton’s Ether Inhaler (1846)
Wm. T. G. Morton
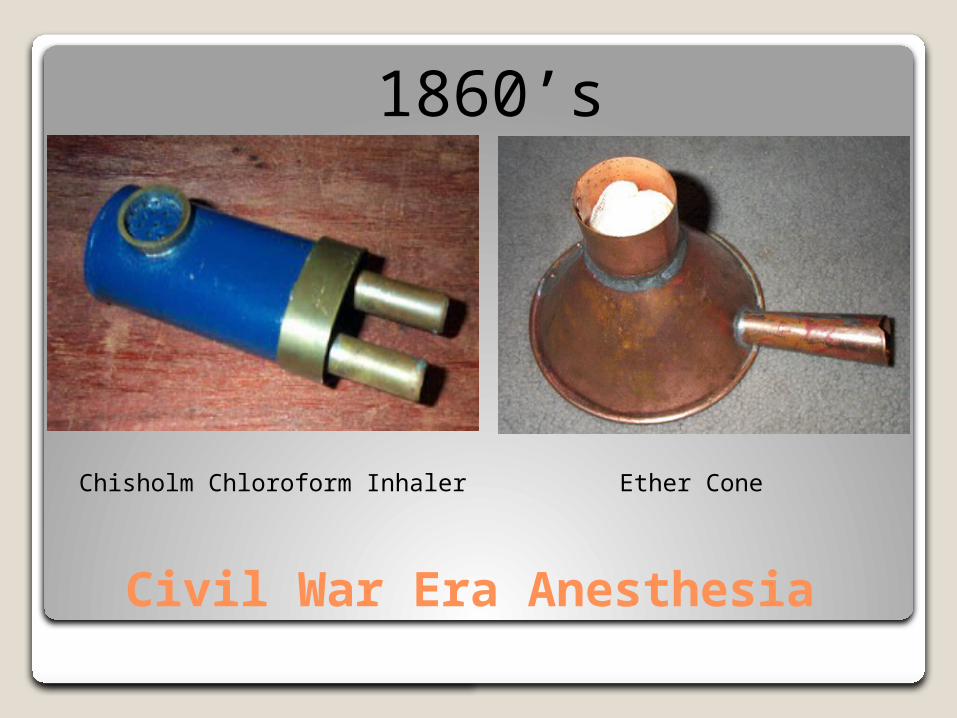
Civil War Era Anesthesia
Chisholm Chloroform Inhaler Ether Cone
1860’s
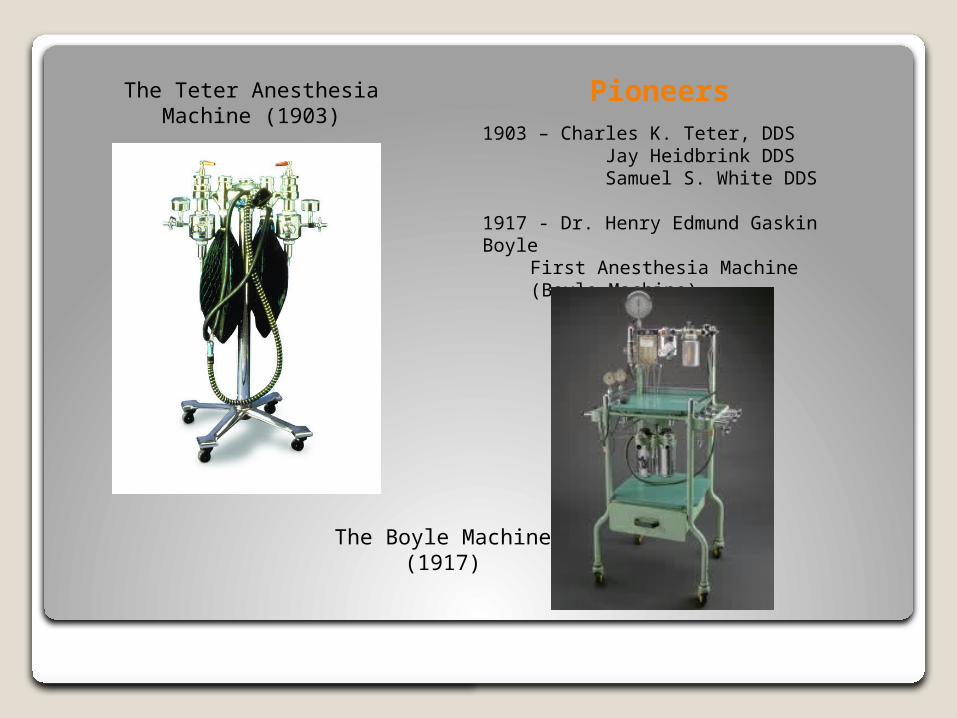
Pioneers1903 – Charles K. Teter, DDS Jay Heidbrink DDS Samuel S. White DDS 1917 - Dr. Henry Edmund Gaskin Boyle
First Anesthesia Machine (Boyle Machine)
The Teter Anesthesia Machine (1903)
The Boyle Machine (1917)
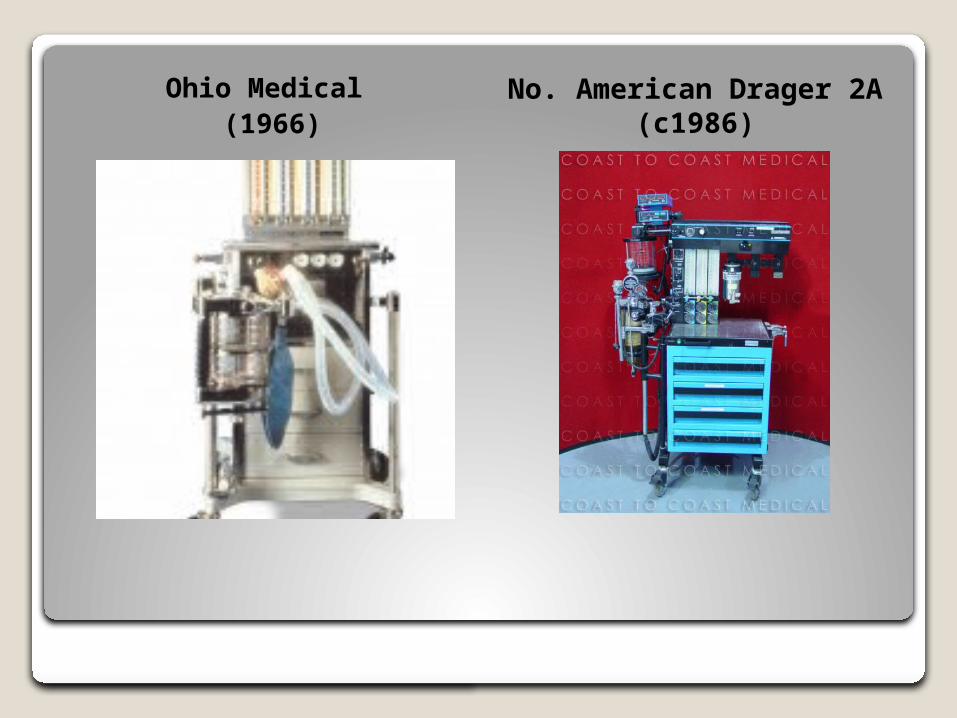
Ohio Medical (1966)
No. American Drager 2A (c1986)
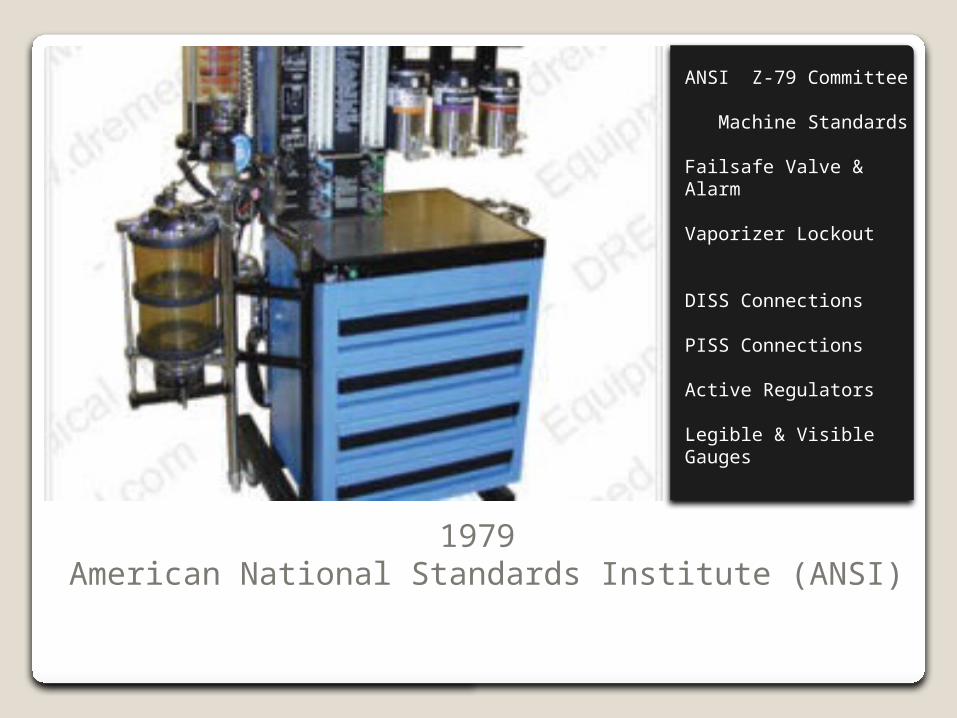
1979 American National Standards Institute (ANSI)
ANSI Z-79 Committee Machine Standards
Failsafe Valve & Alarm
Vaporizer Lockout
DISS Connections
PISS Connections
Active Regulators
Legible & Visible Gauges
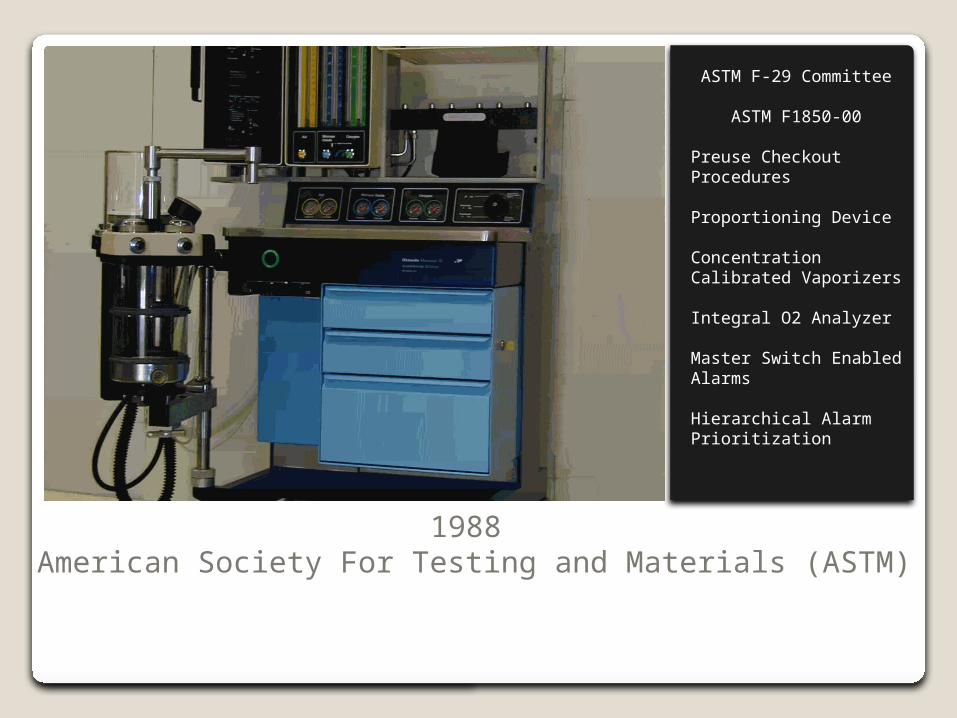
1988 American Society For Testing and Materials (ASTM)
ASTM F-29 Committee
ASTM F1850-00
Preuse Checkout Procedures
Proportioning Device
Concentration Calibrated Vaporizers
Integral O2 Analyzer
Master Switch Enabled Alarms
Hierarchical Alarm Prioritization
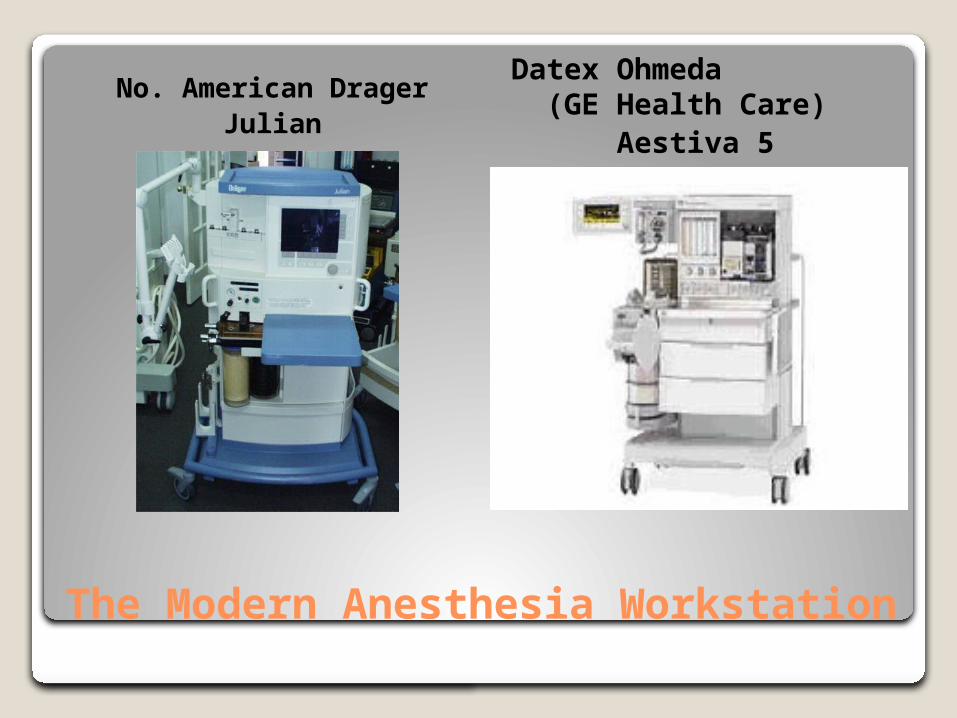
The Modern Anesthesia Workstation
No. American DragerJulian
Datex Ohmeda (GE Health Care)
Aestiva 5

The Modern Anesthesia Workstation
GE Health CareADU/5
ADU/5 Aladin Cassette Vaporizers
“Brain Damage & Death Related to Anesthesia Machines” (Caplan, 1997)
RA Caplan (1997) - Study of 3791 Closed Anesthesia Claims (1962 – 1991) 72 claims related gas delivery system Claim frequency decreased from 2.2% to
1.2% from 1985 – 1991 Pure equipment failures were rare Rate of equipment misuse, 3 x higher than
pure failures 76% of claims – Death or Brain Damage 78% of injuries could have been prevented
by better monitoring Caplan,RA, Visica, MF, Posner, KL, Cheney, FW Adverse anesthetic outcomes arising from gas delivery equipment; a close claims analysis. Anesthesiology 1997;87:741-8
Specific Damaging Events (Caplan, 1997)
Breathing Circuit (39%) - The #1 Culprit Caused 70% of the incidence of death & Brain
Damage Most Frequent Circuit Event – Disconnects or
misconnects leading to hypoventilation or barotrauma
Vaporizers (21%) Overdose or awareness Gas analysis or cerebral monitoring may have
prevented
Ventilators (17%) Improper activation or excessive Vt /Inspiratory
pressure
Specific Damaging Events (Caplan, 1997)
High Pressure Gas Supplies (11%) – direct connection to respiratory system w/o proper decompression
Human Error – 3 times more common than failure of equipment Failure to precheck Unfamiliarity with equipment Lack of Vigilance Unauthorized repair or “jury rigging”
Caplan,RA, Visica, MF, Posner, KL, Cheney, FW Adverse anesthetic outcomes arising from gas delivery equipment; a close claims analysis. Anesthesiology 1997;87:741-8
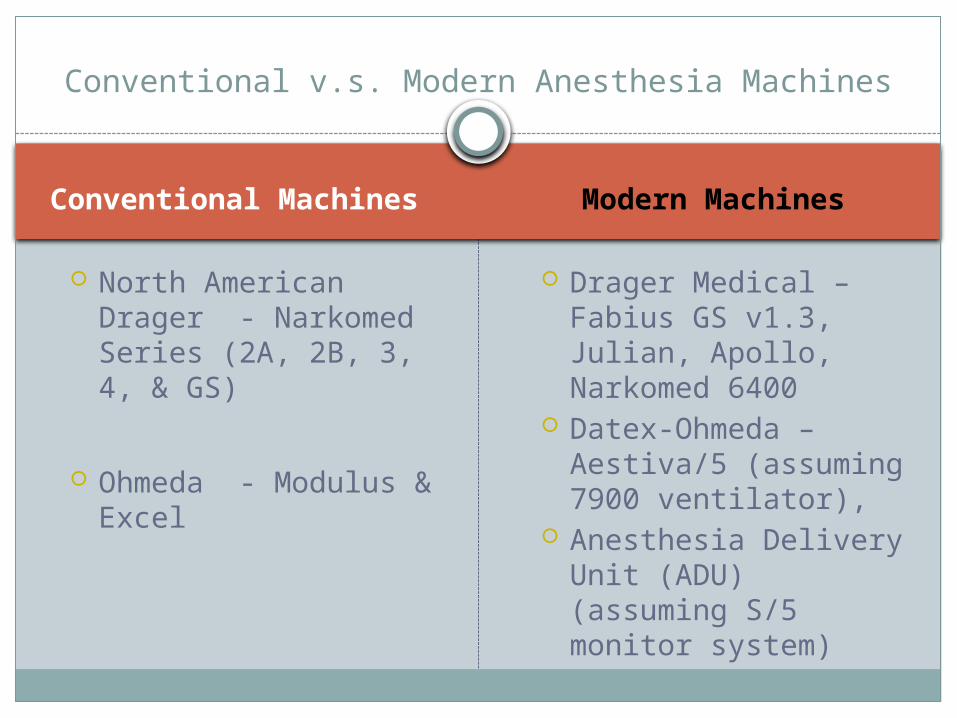
Conventional Machines Modern Machines
North American Drager - Narkomed Series (2A, 2B, 3, 4, & GS)
Ohmeda - Modulus & Excel
Drager Medical – Fabius GS v1.3, Julian, Apollo, Narkomed 6400
Datex-Ohmeda – Aestiva/5 (assuming 7900 ventilator),
Anesthesia Delivery Unit (ADU) (assuming S/5 monitor system)
Conventional v.s. Modern Anesthesia Machines
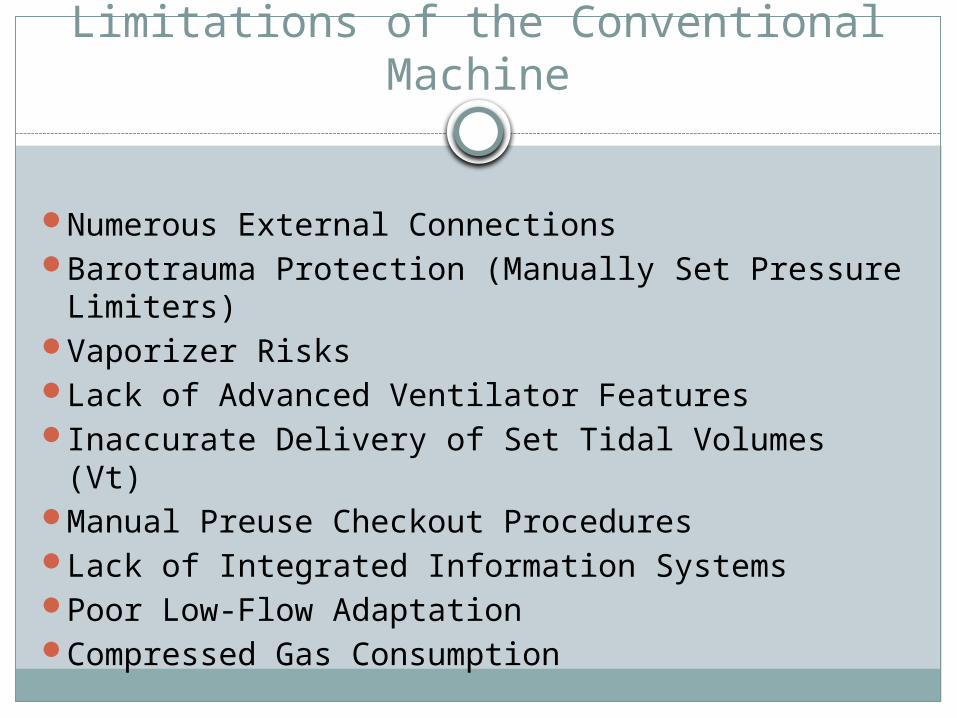
Limitations of the Conventional Machine
Numerous External ConnectionsBarotrauma Protection (Manually Set
Pressure Limiters)Vaporizer RisksLack of Advanced Ventilator FeaturesInaccurate Delivery of Set Tidal Volumes (Vt)Manual Preuse Checkout ProceduresLack of Integrated Information SystemsPoor Low-Flow AdaptationCompressed Gas Consumption
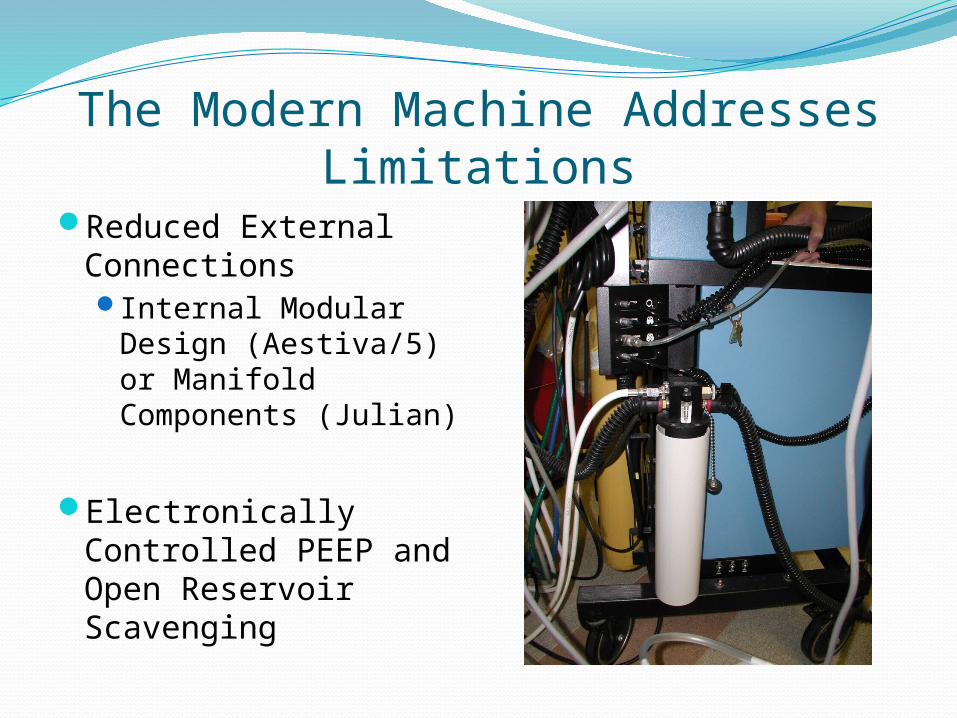
The Modern Machine Addresses Limitations
Reduced External ConnectionsInternal Modular
Design (Aestiva/5) or Manifold Components (Julian)
Electronically Controlled PEEP and Open Reservoir Scavenging

Electronic Vaporizer Cassettes
ADU, Aladin Cassettes (GE Healthcare)
Electronically Control & Measure Vaporization
Eliminates need for multiple vaporizers
Color Coded, magnetically labeled
Agent delivery reported to Information Management System (IMS).
Overfill protection
Automatically leak tested
Check valve protection for bypass circuit
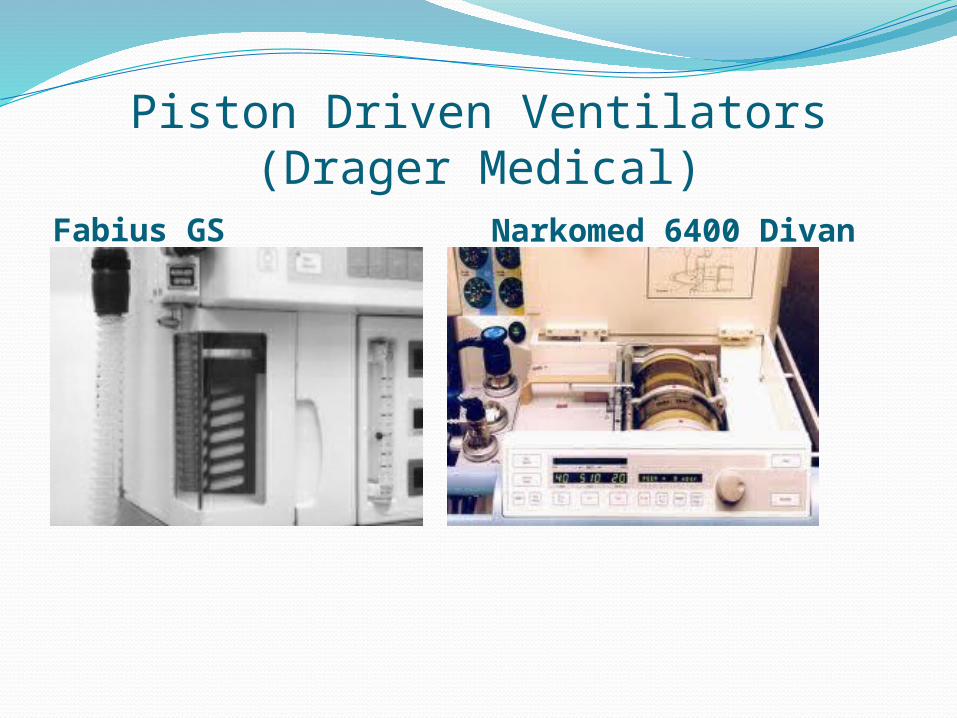
Piston Driven Ventilators (Drager Medical)Fabius GS Narkomed 6400 Divan
Modern Ventilators“Conventional” Dual Circuit, Pneumatic
Drive 7900 “SmartVent” (GE Healthcare)Single Circuit Electronic Piston Drive
Divan or Fabius GS (Drager Medical)Allows Flexibility in ventilation
Pressure Control Ventilation (PCV)Volume Control Ventilation (VCV)Pressure Support Ventilation (PSV)Synchronized Intermittent Mandatory
Ventilation (SIMV-Vol & SIMV-PC)
Modern VentilatorsMethods to Assure Accuracy in Delivery of
set Tidal Volumes (Vt)Fresh Gas Decoupling (FGD)Compliance Testing and CompensationLeak Testing/Measurement and ReportingLocation and Electronic Activation of PEEP Electronic Settings Reduce Operator ErrorOne-step activation of Control Mode Ventilation
(CMV)
Automated Checkout Procedures and Monitoring
User cannot Circumvent Multitude of Surveillance Alarms Critical Systems Checked
Computer Circuit Loops Flow Meters Pressure Sensors Piston Drive Gears Coordination /operation of Valves Compliance Compensation Fresh Gas Control Display of Ventilation & Airway
Pressures
Information Management Systems (IMS)
Integrated Systems exceed ASTM Standards
Integrated Physiological and Respiratory Monitoring Data
Digital Fresh Gas & Volatile Agent Flow Data (Inspired & Expired Concentration)
Data Exported to Anesthetic Record Data MAY be Exported to other
Demographic and Financial Records
New Machines; New ConcernsOperator Learning Curve - even less
understanding of machine functions)Over reliance on Technology – Are you sure it
will tell you all that fails?Dependence on Electricity - How does your
machine function in a power failure?Piston Ventilators – quiet, hidden – Will you
know if the piston fails to move?
New Machines; New ConcernsCan a machine have a clinically significant
failure after passing an automated checkout?The new machines still do not warn of oxygen
consumption from open cylinders if wall pressures drop
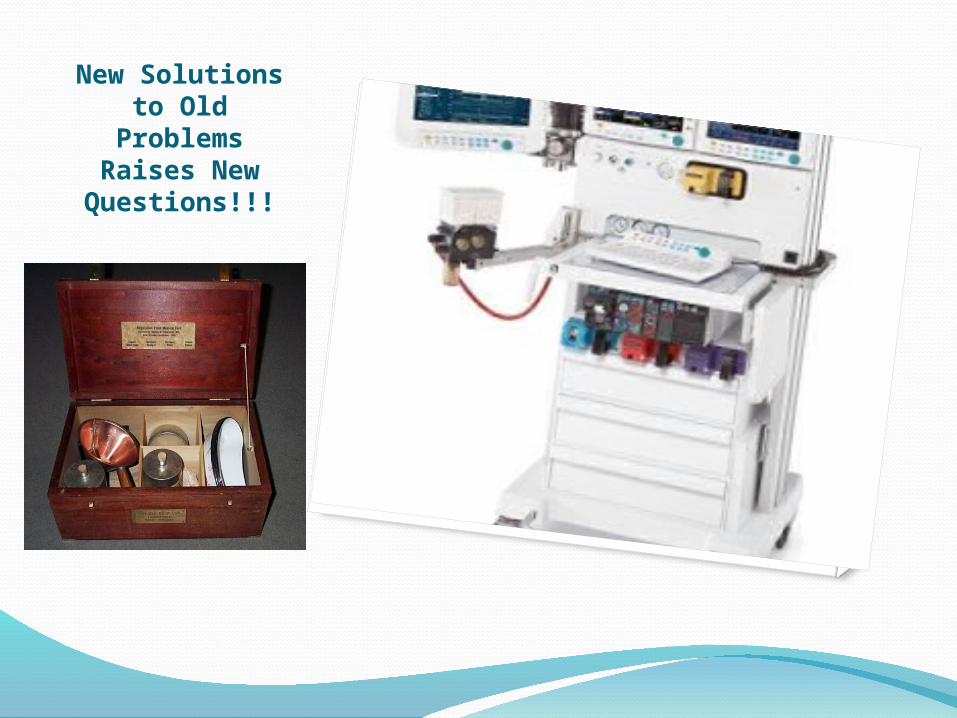
New Solutions to Old Problems Raises New Questions!!!