renal calculli veeresh vg rn
TRANSCRIPT


RENAL CALCULI

OUTLINE OF THE CONTENT
DEFINITION OF RENAL CALCULI
INCIDENCE OF RENAL CALCULI
RISK FACTORS FOR RENAL CALCULI
CLASSIFICATION OF RENAL CALCULI
ETIOLOGY : PATHOPHYSIOLOGY
SITES OF IMPACTION

OUTLINE OF THE CONTENT
• SIGNS AND SYMPTOMS OF RENAL
CALCULI
• COMPLICATIONS OF RENAL CALCULI
• DIAGNOSIS OF RENAL CALCULI
• MANAGEMENT OF RENAL CALCULI
• VEDIO ON ESWL

INTRODUCTION
Kidney stones (called renal calculi (from
Latin renes, "kidney" and calculi, "pebbles")
are solid concretions or crystal aggregations
formed in the kidneys from dietary minerals.

DEFINITION OF RENAL CALCULI
Renal calculi a condition in which there is a
formation of stones within the renal system
that is kidney, urethra and bladder.

INCIDENCE OF RENAL CALCULI
Kidney stones are a significant source of
morbidity with an annual incidence of 1–2 per
1000 and a lifetime prevalence of 3–5%.
80% of those with kidney stones are men;
most stones in women are due to either
metabolic defects (such as cystinuria) or
infection.

INCIDENCE OF RENAL CALCULI CONT...
Recurrence rates are estimated at 50% over a
10 year period and 75% over 20 years, with
some experiencing ten or more episodes over
the course of a lifetime.
The incidence of urolithiasis increases to 20-
25% in the Middle East, partly due to the
increased risk of dehydration in hot climates.

INCIDENCE OF RENAL CALCULI CONT...
Men most commonly experience their first
episode between age 30- 40 years, while for
women the age at first presentation is
somewhat later.

RISK FACTORS OF RENAL CALCULI
Occupation
Family history (cystinuria inherited metabolic
disorder)
Dietary pattern of family diet high in
calcium, vitaminD, milk, protein, oxalate,
alkali.
Dehydration
Small bowel disease : Krohn’s disease
Medical conditions: Hypercalcuria
Hyperparathyrodism, and Gout

RISK FACTORS OF RENAL CALCULI CONT…
Urinary tract infection
Urinary stasis
Immobility
Urinary tract obstruction
Hypercalcemia

CLASSIFICATION OF RENAL CALCULI
Kidney stones are typically classified by their
1. Location
2. Chemical composition

CLASSIFICATION OF RENAL CALCULI…
1. Location
Urolithiasis
Nephrolithiasis
Calyceal
ureterolithiasis
cystolithiasis.

CLASSIFICATION OF RENAL CALCULI…
Urolithiasis refers to stones originating
anywhere in the urinary system, including the
kidneys and bladder.
Nephrolithiasis refers to the presence of such
calculi in the kidneys.

CLASSIFICATION OF RENAL CALCULI…
Calyceal calculi refers to aggregations in
either the minor or major calyx, parts of the
kidney which pass urine into the ureter.
The condition is called ureterolithiasis when a
calculus or calculi are located in the ureter.
Stones may also form or pass into the bladder,
condition referred to as cystolithiasis.

CLASSIFICATION OF RENAL CALCULI…
2. Chemical composition
Calcium-containing stones
Struvite stones
Uric acid stones

CLASSIFICATION OF RENAL CALCULI…
2. Chemical composition
Calcium-containing stones
Calcium-containing stones represent about
80% of cases.
These typically contain calcium oxalate either
alone or in combination with calcium
phosphate
The formation of calcium phosphate stones is
associated with conditions such as
hyperparathyroidism and renal tubular acidosis

CLASSIFICATION OF RENAL CALCULI…
Struvite stones
• 10-15% of urinary calculi are composed of
struvite (ammonium magnesium phosphate).
• Struvite stones (also known as "infection
stones“ “Staghorn stone”, urease or triple-
phosphate stones), form most often in the
presence of infection by urea-splitting bacteria.

CLASSIFICATION OF RENAL CALCULI…
Struvite stones cont…..
The enzyme urease, these organisms metabolize
urea into ammonia and carbon dioxide.
This alkalinizes the urine, resulting in favorable
conditions for the formation of struvite stones.
Proteus vulgaris
Klebsiella,
Enterobacter
Ureaplasma urealyticum are the most common
organisms

CLASSIFICATION OF RENAL CALCULI…
Struvite stones cont…..
These infection stones are commonly observed in
people who have factors which predispose them
to urinary tract infections, such as those with
spinal cord injury and other forms of neurogenic
bladder, ileal conduit urinar diversion,
vesicoureteral reflux, and obstructive uropathies.

CLASSIFICATION OF RENAL CALCULI…
Uric acid stones
About 5-10% of all stones are formed from uric
acid.
Uric acid stones may form in association with
conditions that cause hyperuricosuria (an
excessive amount of uric acid in the urine) with
or without high hyperuricemia (an excessive
amount of uric acid in the serum)

CLASSIFICATION OF RENAL CALCULI…
Uric acid stones cont…..
People afflicted with xanthinuria often produce
stones composed of xanthine
People with certain rare inborn errors of
metabolism have a propensity to accumulate
crystal-forming substances in their urine. For
example, those with cystinuriaform stones
composed of cystine

ETIOLOGY : PATHOPHYSIOLOGY
Supersaturation of urine
Inhibitors of stone formation
Calcium
others

ETIOLOGY : PATHOPHYSIOLOGY
Supersaturation of urine
When the urine becomes supersaturated (when
the urine solvent contains more solutes than it
can hold in solution) with one or more crystal-
forming substances,
a seed crystal may form through the process of
nucleation.

Heterogeneous nucleation (where there is a
solid surface present on which a crystal can
grow) proceeds more rapidly than
homogeneous nucleation (where a crystal must
grow in liquid medium with no such surface),
because it requires less energy.
Adhering to cells on the surface of a renal
papillae, a seed crystal can grow and aggregate
into an organized mass.

• Depending on the chemical composition of the
crystal, the stone-forming process may proceed
more rapidly when the urine pH is unusually
high or low.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Inhibitors of stone formation
Normal urine contains chelating agents such as
citrate that inhibit the nucleation, growth, and
aggregation of calcium-containing crystals.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Inhibitors of stone formation:
Other endogenous inhibitors include
calgranulin(an S-100 calcium binding protein),
nephrocalcin (an acidic glycoprotein),
prothrombin F1 peptide, and bikunin (uronic
acid-rich protein).
When these substances fall below their normal
proportions, stones can form out of an
aggregation of crystals.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
CalciumPeople who take supplemental calcium have a
higher risk of developing kidney stones
In the Women's Health Initiative,
postmenopausal women who consumed
1,000 milligrams of supplemental calcium and
400 IU of vitamin D per day for 7 years had a
17% higher risk of developing kidney stones
than subjects taking a placebo.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Calcium
This is perhaps related to the role of calcium in
binding ingested oxalate in the gastrointestinal
tract.
Unlike supplemental calcium, high intakes of
dietary calcium do not appear to cause kidney
stones and may actually protect against their
development

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Role of dietary animal protein
Animal protein than the body needs, and as the
excess amino acids are broken down and
excreted, the sulfurous amino acids (typically
derived from animal rather than vegetarian
foods) cause calcium to be excreted in the
urine.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
• Red meat also contains acids that need to be
excreted and this acidity constitutes another
risk factor for kidney stones
• High intake of animal protein also presents a
greater uric acid load to be excreted by the
kidney. This in turn acidifies the urine,
increasing the risk of uric acid stones.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Other
Water fluoridation may increase the risk of
kidney stone formation.
Ingestion of vitamin C supplements is
associated with an increased incidence of
kidney stones.

ETIOLOGY : PATHOPHYSIOLOGY CONT.
Other
Alcohol consumption, binge drinking can lead
to systemic dehydration, which can in turn lead
to the development of kidney stones.
Astronauts seem to show a higher risk of
developing kidney stones during or after space
flights of long duration.

UROLITHIASIS – SITES OF IMPACTION

SIGNS AND SYMPTOMS OF RENAL CALCULI
Obstruction of urine flow through one or both
ureters.
Oliguria (reduced urinary volume) caused by
obstruction of the bladder or urethra by a stone or
rarely, simultaneous obstruction of both ureters by
two separate stones.
Postrenal azotemia and
Hydronephrosis (distension and dilation of the
renal pelvis and calyces

SIGNS AND SYMPTOMS OF RENAL CALCULI…
Flank pain
Costovertebral
tenderness
Cool, moist skin
Pallor,
DiaphoresisDiagram showing the typical
location of renal colic, from below
the rib cage to just above the pelvis

SIGNS AND SYMPTOMS OF RENAL CALCULI…
Frequency and urgency in urination
dysuria,
Chills and fever
Hematuria
Nausea and vomiting

SIGNS AND SYMPTOMS OF RENAL CALCULI…
• Hallmark symptoms of
kidney stones include
renal colic, fever,
blood, pus in the urine,
and painful urination.
• Pain, most commonly
felt in the flank, lower
abdomen and groin (a
condition called renal
colic.

SIGNS AND SYMPTOMS OF RENAL CALCULI…
Renal colic, which typically comes in waves
lasting 20 to 60 minutes, is caused by peristaltic
contractions of the ureter as it attempts to expel
the stone.
It typically begins in the flank or lower back,
often radiating to the groin or in men, to the
testes.
Renal colic can be associated with nausea and
vomiting.

COMPLICATIONS OF RENAL CALCULI
Chronic Urinary Tract Infection
RENAL OBSTRUCTION
UTERO-VESICAL REFLUX
HYDRO NEPHROSIS
PYELO NEPHROSIS
Acute Renal Failure
Chronic Renal Failure

DIAGNOSIS OF RENAL CALCULI
Diagnosis of kidney stones is made on the basis
of information obtained from the
History,
Physical examination,
Urinalysis, and
Radiographic studies

DIAGNOSIS OF RENAL CALCULI…
History and physical examination
Clinical diagnosis is usually made on the basis of
the location and severity of the pain, which is
typically colicky in nature (comes and goes in
spasmodic waves).
Physical examination may reveal fever and
tenderness at the costovertebral angle on the
affected side.

DIAGNOSIS OF RENAL CALCULI…
Urinalysis
Provides excellent information about renal function and
condition relative to fluids and Electrolytes
Urinalysis – know normal (color, odor, consistency &
related teaching)
Clean catch – know teaching of method and purpose
Culture and Sensitivity – know teaching
Urine chemistry pyuria, proteinuria, hematuria, and
wbc’s count.

DIAGNOSIS OF RENAL CALCULI…
Urinalysis
pH: Indicates acidity or alkalinity
Normal range 4.5-8.0
Normal for urine 6.0 (acid)
Osmolality
pinpoints fluid balance
normal = 300-1200 mOsm/kg
example: as urine Osm. increases. urine
volume decreases (urine more concentrated)

DIAGNOSIS OF RENAL CALCULI…
Electrolytes
Not frequently measured
Requires 24-hour specimen
Changes in urinary electrolytes highly
suggestive of renal impairment
Sodium extremely suggestive of type of acute
renal failure
<20 mEq/L = pre-renal
Normal or high >20 mEq/L

DIAGNOSIS OF RENAL CALCULI…
Creatinine Clearance test
A direct measurement of glomerular
filtration rate
Best indicator of overall kidney function
Clearance expressed in ml/min
Normal: male 90-139mL/min
female 80-125mL/min
Measured by completing a 24 hr urine with
corresponding blood test.

DIAGNOSIS OF RENAL CALCULI…
Serum Creatinine
By-product of muscle metabolism
Appears in serum in amts. proportional to body
muscle mass
Fluctuates little – excreted entirely by kidneys
Normal about 0.7-1.5 mg/dL
• ↓ elderly and with low muscle mass
• Creatinine: >1.5 (>50% loss), >4.8 (75% loss)
and >10 (90% loss)

DIAGNOSIS OF RENAL CALCULI…
• BUN/Creatinine Ratio
Normal ratio = between 6:1 to 20:1
When both BUN and [Cr] levels increase at same
rate (ratio remains normal) – suggestive of renal
dysfunction
When BUN rises faster then [Cr] (ratio increased)
suggestive of dehydration, hypo perfusion,
protein catabolism, GI bleeds

DIAGNOSTICS: KUB
KUB (kidney, ureters,
bladder)
No preparation
No contrast
Shows:
• Stones
• Strictures
• Calcifications
• Obstructions

DIAGNOSTICS: INTRAVENOUS PYELOGRAM
IVP/ IVU
Series of x-ray after
dye injection
To measure size,
shape, etc of kidneys
Detect obstructions
Assess for masses
Client preparation and
teaching important
nursing function
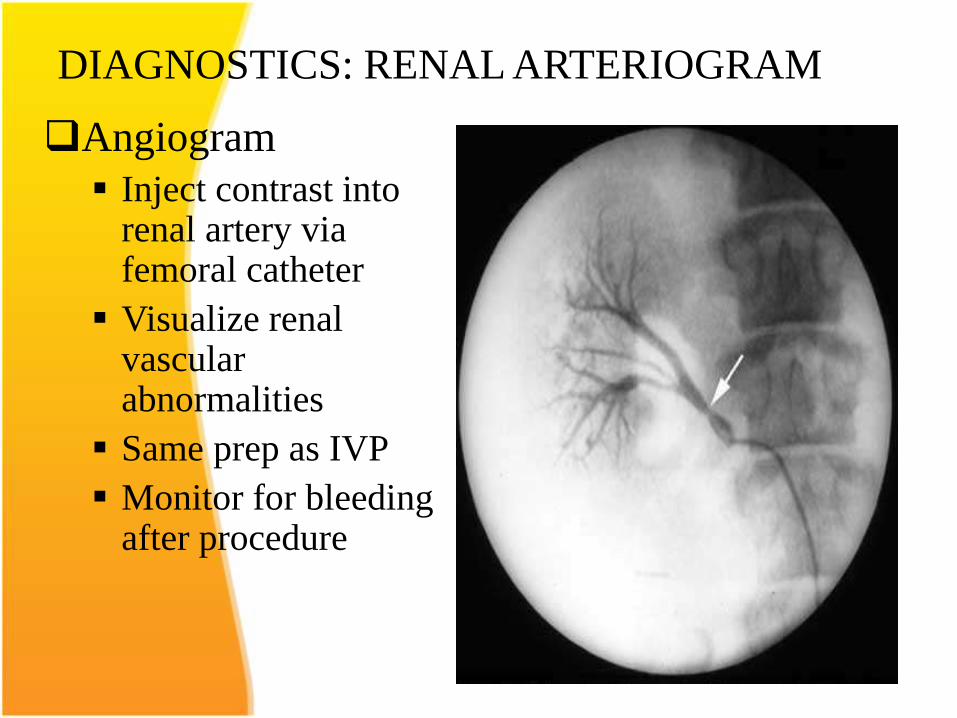
DIAGNOSTICS: RENAL ARTERIOGRAM
Angiogram
Inject contrast into renal artery via femoral catheter
Visualize renal vascular abnormalities
Same prep as IVP
Monitor for bleeding after procedure

DIAGNOSTICS: MRI: ARTERIAL
New and thought to
be more useful than
other artery/venous
grams
Very expensive

DIAGNOSTICS: CYSTOGRAM
Cystogram
Contrast into
bladder
Evaluate bladder
and vesicoureteral
reflux

DIAGNOSTICS: RETROGRADE PYELOGRAM
RETROGRADE
PYELOGRAM
x-ray after contrast
into kidneys.
Done by
cystoscope and
urethral catheters
placed into renal
pelvis

DIAGNOSTICS OF RENAL CALCULI
• Ultrasound – differentiates between fluid and
mass, notes obstructions (no dye)
• Cystoscopy – direct visualization of bladder, can
be used for diagnosis or treatment (no dye)
• Biopsy – used for definitive diagnosis (no dye)

MANAGEMENT OF RENAL CALCULI
• Medical management
• Surgical management
• Nursing management

MANAGEMENT OF RENAL CALCULI
Medical management
• 85% of the time, it is possible to spontaneously
pass a kidney stone with urination
• Stones larger than 6 millimeters will almost
always require some form of intervention,
however.
• Assuming there is no high-grade obstruction or
associated infection in the urinary tract, and
symptoms are relatively mild, various non-
surgical measures can be used to encourage the
passage of a stone.

MANAGEMENT OF RENAL CALCULI…
Analgesia
requires intravenous administration of NSAIDs
or opioids in an emergency department setting.
Intravenous acetaminophen appears to be
effective.

MANAGEMENT OF RENAL CALCULI…
Alpha adrenergic blockers
as tamsulosin (Flomax) may increase the
spontaneous passage of the stone by 30%.

MANAGEMENT OF RENAL CALCULI…
Diuretics (dietary and medicinal)
One of the recognized medical therapies for
prevention of stones is the thiazide diuretics.
Thiazides inhibit the formation of calcium-
containing stones by reducing urinary calcium
excretion, an effect independent of their
diuretic properties.

MANAGEMENT OF RENAL CALCULI…
Urine alkalinization
The mainstay for medical management of uric
acid stones is alkalinization (increasing the
pH) of the urine. Uric acid stones are among
the few types amenable to dissolution therapy,
referred to as chemolysis.
Acetazolamide (Diamox) is a medication that
alkalinizes the urine.

MANAGEMENT OF RENAL CALCULI…
Allopurinol
For people with hyperuricosuria and calcium
stones, Allopurinol (Zyloprim) is one of the
few treatments.

MANAGEMENT OF RENAL CALCULI…
Allopurinol interferes with the production of
uric acid in the liver.
The drug is also used in patients with gout or
hyperuricemia (high serum uric acid levels).
Dosage is adjusted to maintain a reduced
urinary excretion of uric acid.
Serum uric acid level at or below
6 milligrams/100 mL) is often a therapeutic
goal for patients with gout or hyperuricemia.

MANAGEMENT OF RENAL CALCULI…
Diet for the calcium stones ( acid ash with limited
intake of calcium and milk products
for oxalates stones ( alkaline ash with limited intake of foods high in oxalates
for uric acid stones ( alkaline ash with limited intake of foods high in purine
A high fluid of 3000ml per day after episode of urolithiasis to produce urine output of 2L per day
Intravenous therapy (fluid replacement )
Activity as tolerated

MANAGEMENT OF RENAL CALCULI…
Surgical management
Invasive management
Non invasive managements

MANAGEMENT OF RENAL CALCULI…
Surgical management
Non invasive managements
Electro hydraulic lithotripsy
Ultrasonic lithotripsy
Laser impulse (holmium laser)
Extra corporeal shock wave lithotripsy

MANAGEMENT OF RENAL CALCULI…
Electro hydraulic lithotripsy

MANAGEMENT OF RENAL CALCULI…
Ultrasonic lithotripsy
Laser impulse
Extra corporeal shock wave lithotripsy
Extracorporeal shock wave lithotripsy (ESWL)
involves the use of a lithotriptor machine to
deliver externally-applied, focused, high-
intensity pulses of ultrasonic energy to cause
fragmentation of a stone over a period of
around 30–60 minutes.

MANAGEMENT OF RENAL CALCULI…
Surgical management
Invasive managements
Percutaneous nephrostolithotomy
Cystolithophaxy
Pyelolithotomy (incision into renal pelvis)
Cystotomy(bladder calculi)
Nephrotomy
Ureteroscopic surgery

MANAGEMENT OF RENAL CALCULI…
Nursing management
Maintain proper nutrition
Force fluids 3 Liter / day
Assess renal status
Monitor and record vital signs, urine output,
input and output, daily weight, specific gravity,
lab studies, and urine pH.
Administer medication as prescribed
Allay the patient anxiety

MANAGEMENT OF RENAL CALCULI…
Continue straining urine and giving warm baths
and warm soaks to flanks to reduce pain
Instruct on home care
Increase fluid intake during hot
Weather, illness, and exercise
Void when urge is felt
Test urine PH
Increase fluid at night and void frequently

NURSING DIAGNOSIS
• Acute pain related to irritation of stone and inadequate pain control or comfort as manifested by complaints of pain, facial grimicing, restlessness.
• Ineffective therapeutic regimen management related to lack of knowledge about prevention, recurrence, diet, fluid requirement as manifested by questions that indicate lack of knowledge.


