report under p.g. 205-21 police department … packages/uniform_fmla_package...1 report under p.g....
TRANSCRIPT

1
Report Under P.G. 205-21
POLICE DEPARTMENT CITY OF NEW YORK
From: Commanding Officer, Military and Extended Leave Desk To: Uniformed Members of the Service Subject: INSTRUCTIONS AND FORMAT TO FOLLOW WHEN
REQUESTING A LEAVE OF ABSENCE WITHOUT PAY, UNDER THE FAMILY AND MEDICAL LEAVE ACT.
1. Prepare a report using the attached sample and format as a guide. This report will be addressed to your Commanding Officer and forwarded to this command after the C.O. endorses the request (after conferral with the Borough Commander). All doctor’s notes submitted in connection with this leave request, must be original and written on official letterhead. 2. You must surrender all Department property, as listed on the Discontinuance of Service Form before starting this leave to your Commanding Officer. Restricted/HQ Annex Parking Permit must be returned to the Integrity Control Officer at your command. All Department property will be recorded on the Property Receipt-Discontinuance of Service Form, the original will be forwarded, along with the green copy of the Property Clerk’s Voucher, to the Commanding Officer, Military and Extended Leave Desk. If applicable, all members must return their personal portable radio with all accessories to Communications Division, Electronics Section 50-16 59th Place, Woodside, NY 11377. If applicable, all members, must return their personally assigned cellular telephones and all accessories to Communications Division, Telecommunications Unit, One Police Plaza, Room 910B. Metro Card must be delivered to Employee Management Division located in 1 Police Plaza, Room 1014 (this will be noted on Property Receipt-Discontinuance of Service Form or on a separate receipt). All members of the service MUST forward their Shield and Identification Card to the Shield and ID Unit, 1 Police Plaza, Room 502. Attach a copy of all property receipts to leave request package. 3. All accrued vacation and other accrued leave MUST be exhausted prior to start of leave. As a uniformed member, vacation is granted January 1st for that year. You DO NOT accrue vacation while on an UNPAID leave, thus vacation may not be taken before a leave which includes vacation time which would have accrued during the months you are on a leave of absence. If vacation time was already taken, it will be deducted from your vacation allowance for the following year when you return to active

2
employment with the NYCPD. You must reimburse the NYCPD for vacation days which you were paid, but were not earned. 4. While on this leave of absence without pay, you may be entitled to twelve (12) weeks of health insurance under the Family and Medical Leave Act (FMLA). If you have any questions concerning your health insurance coverage, please contact the Health Insurance Section at (646) 610-5122. 5. After the leave of absence is approved, you will be transferred to the Military and Extended Leave Desk (MELD), located at 1 Police Plaza, New York, NY., Room 1008. If you plan to terminate your leave prior to its scheduled expiration date, contact MELD for an appointment. You must notify the Commanding Officer, Military and Extended Leave Desk, in writing of any change of address or telephone number while on leave including any temporary change of address or telephone number. If you are permanently changing your address or telephone number, you will need to officially inform the Department by preparing form PD451-021 (Change of Name, Residence or Social Condition).
6. You must not accept outside employment while on this leave without the Department’s prior approval, obtained through the Commanding Officer, Military and Extended Leave Desk, by submitting an Off-Duty Employment Application (PD407-164), as per Patrol Guide Procedure 205-40.
7. While on leave, you will respond to and make all court appearances for any Department hearings or trials that are pending in which you are a witness, arresting officer, or respondent. In addition, all Members of the Department must report all Police Incidents/Off-Duty Incidents as per Patrol Guide Procedure 212-32, and any Family Offenses and Domestic Violence, involving Members of the Department, as per Patrol Guide Procedure 208-37. 8. If you have any further questions, please call the Military and Extended Leave Desk at (646) 610-5513. Rebecca Mayo Sergeant C.O., Military and Extended Leave Desk Rev. 05/11
3
SAMPLE FORMAT SAMPLE FORMAT POLICE DEPARTMENT CITY OF NEW YORK Date ________________ From: P.O. Janice Jones; Shield# 9999; Tax# 999999; SS# 9999 To: Commanding Officer, 099 Precinct Subject: REQUEST FOR A LEAVE OF ABSENCE WITHOUT PAY,
UNDER THE FAMILY AND MEDICAL LEAVE ACT (FMLA) 1. It is requested that I be granted a twelve (12) week leave of absence without pay, under the provisions of the Family and Medical Leave Act, from 0001 hours, ________________ to 2400 hours, _______________. This leave is being requested so that I may care for _________ (sick parent, child or spouse). I am enclosing medical documentation to substantiate this request. 2. In this paragraph, state in detail why you are requesting this leave and submit any documentation you may have, i.e. letter from an attending physician giving a diagnosis and prognosis of the person to be cared for, (certification of physician or other health care provider). The medical documentation must state that you, the employee, will be the full time care giver. 3. As a uniform member appointed on ______________, I understand that I am not entitled to use any annual vacation which would have accrued while on this unpaid leave and I must use all other accrued time which I have earned prior to commencing this leave. I further understand that if I have already taken any vacation which would have accrued while on this leave, such leave will be deducted from the next year’s allowance. If for any reason, I do not return to active employment with the New York City Police Department, I must reimburse the New York City Police Department for vacation days I was paid, but did not earn. 4. I have worked for the New York City Police Department for at least one year, and for 1250 hours over the previous 12 months. I understand that while on this leave of absence, my health insurance will be paid for by the City of New York for up to 12 weeks. 5. Before starting my leave, I will surrender all Department property, as listed on the Discontinuance of Service Form to my Commanding Officer. The Restricted/HQ Annex Parking Permit was returned to my Integrity Control Officer. I delivered my Shield and Identification Card to the Shield and ID Desk, the Metro Card to
4
the Employee Management Division. Copies of my Property Receipt-Discontinuance of Service Form, Property Clerk’s Voucher, and receipt for my Shield and ID are attached. 6. While on leave, I may be reached at: Full Address (including apartment number, city and zip code) Telephone Number (including area code) Cell Phone Number Resident Precinct 7. I will notify the Commanding Officer, Military and Extended Leave Desk, in writing of any change of address or telephone number while on leave of absence, including any temporary change of address or telephone number. I am aware that if I am permanently changing my address or telephone number that I will need to officially inform the Department by preparing form PD451-021 (Change of Name, Residence, Social Condition).
8. I agree that I will not accept outside employment while on this leave without the Department’s prior approval, obtained through the Commanding Officer, Military and Extended Leave Desk, by submitting an Off-Duty Employment Application (PD407-164), as per Patrol Guide Procedure 205-40.
9. I understand that while on this leave, I will respond to and make all court appearances for any Department hearings or trials that are pending in which I am a witness, arresting officer, or respondent. I also understand that I will report all Police Incidents/Off-Duty Incidents, Family Offenses, and Domestic Violence Incidents, as per Patrol Guide Procedures 212-32 and 208-37. Signature Jane Jones Police Officer
5
Report Under P.G. 205-21 SAMPLE FORMAT SAMPLE FORMAT
1st ENDORSEMENT
Commanding Officer, 099th Precinct, to Commanding Officer, Military and Extended Leave Desk, (Date). Conferred with Borough Commander. Member has worked for the New York City Police Department for at least one year, and for 1250 hours over the previous 12 months. All Department property (except Patrol Guide) has been surrendered and recorded on the Property Receipt-Discontinuance of Service Form (attached) and all weapons as listed on the member’s force record card, have been vouchered (green copy of Property Clerk’s Voucher attached). Recommend APPROVAL/DISAPPROVAL. Henry Ford Captain THIS LEAVE REQUEST WILL BE FORWARDED DIRECTLY TO THE MILITARY AND EXTENDED LEAVE DESK.
Certification of Health Care Provider for Family Member's Serious Health Condition (Family and Medical Leave Act}
SECTION ' I:d?~r .CoIrti mti6Iij)i':CitH~'iEMPLOYER '-. • • •••••••• W'.' P ._ ..... '. y".," .. ,. __ .• _ ._ .. c ••• ·".'" ••.
U.S. Department of Labor Employment Standards Administration Wage and Hour Division
OMB Control Number: 1215-0181 Expires: 12131 12011
INSTRUCTIONS to the EMPLOYER: The Family and Medical Leave Act (FMLA) provides that an employer may require an employee seeking FMLA protections because of a need for leave to care for a covered family member with a serious health condition to submit a medical certification issued by the health care provider of the covered family member. Please complete Section I before giving this form to your employee. Your response is voluntary. While you are not required to use this form, you may not ask the employee to provide more information than allowed under the FMLA regulations, 29 C.P.R. §§ 825.306-825.308. Employers must generally maintain records and documents relating to medical certifications, recertifications, or medical histories of employees' family members, created for FMLA purposes as confidential medical records in separate files/records from the usual personnel files and in accordance with 29 C.F.R. § 1630.14( c)(l), if the Americans with Disabilities Act applies.
SE'Q]!:QNtfj~,i;tEQtl;G~mpX~tj~!i1!~],l~W~~~M:li:~~~i), INSTRUCTIONS to the EMPLOYEE: Please complete Section II before giving this form to your family member or his/her medical provider. The FMLA permits an employer to require that you submit a timely, complete, and sufficient medical certification to support a request for FMLA leave to care for a covered family member with a serious health condition. If requested by your employer, your response is required to obtain or retain the benefit of FMLA protections. 29 U.S.c. §§ 2613, 2614( c)(3). Failure to provide a complete and sufficient medical certification may result in a denial of your FMLA request. 29 C.F.R. § 825 .313. Your employer must give you at least 15 calendar days to return this form to your employer. 29 C.F.R. § 825 .305.
Your name: First Middle Last
Name of family member for whom you will provide care:-::::-:--_____ ---:-::-:-:-:-:-__________ _ First Middle Last
Relationship of family member to you : _ __________________________ _
If family member is your son or daughter, date of birth: ________ ____________ _
Describe care you will provide to your fami ly member and estimate leave needed to provide care:
Employee Signature Date
Page 1 CONTINUED ON NEXT PAGE Form WH-380-F Revised January 20()9

~E~I'iQ~r !!I::ifarCgmplitiXi~:6y;th~:H~A~Tii: ?M~R~IpRQ:Yj:Ii<~R INSTRUCTIONS to the HEALTH CARE PROVIDER: The employee listed above has requested leave under the FMLA to care for your patient. Answer, fully and completely, all applicable parts below. Several questions seek a response as to the frequency or duration of a condition, treatment, etc. Your answer should be your best estimate based upon your medical knowledge, experience, and examination of the patient. Be as specific as you can; terms such as " lifetime," "unknown," or " indeterminate" may not be sufficient to determine FMLA coverage. Limit your responses to the condi tion for which the patient needs leave. Page 3 provides space for additional information, should you need it. Please be sure to sign the form on the last page.
Provider's name and business address: ------------------------------------------------~-------
Type of practice I Medical specialty: ___________________________ _
Telephone : (,. ____ J. _____________ Fax:,,-! ____ . ___ '--_________ _
1. Approximate date condition commenced: _______________________________________ _
Probable duration of condition: _____________________________ _
Was the patient admitted for an overnight stay in a hospital, hospice, or residential medical care facility? _No _Yes. If so, dates of admission: ________________________ _
Date(s) you treated the patient for condition:
Was medication, other than over-the-counter medication, prescribed? _No Yes.
Will the patient need to have treatment visits at least twice per year due to the condition? No Yes
Was the patient referred, to other health care provider(s) for evaluation or treatment (U, physical therapist)? No Yes. If so, state the nature of such treatments and expected duration of treatment:
2. Is the medical condition pregnancy? _No _Yes. If so, expected delivery date: __________ _
3. Describe other relevant medical facts, if any, related to the condition for which the patient needs care (such medical facts may include symptoms, diagnosis, or any regimen of continuing treatment such as the use of specialized equipment):
CONTI NUED ON NEXT PAGE Form WH-380- F Revised Jan uary 200'!
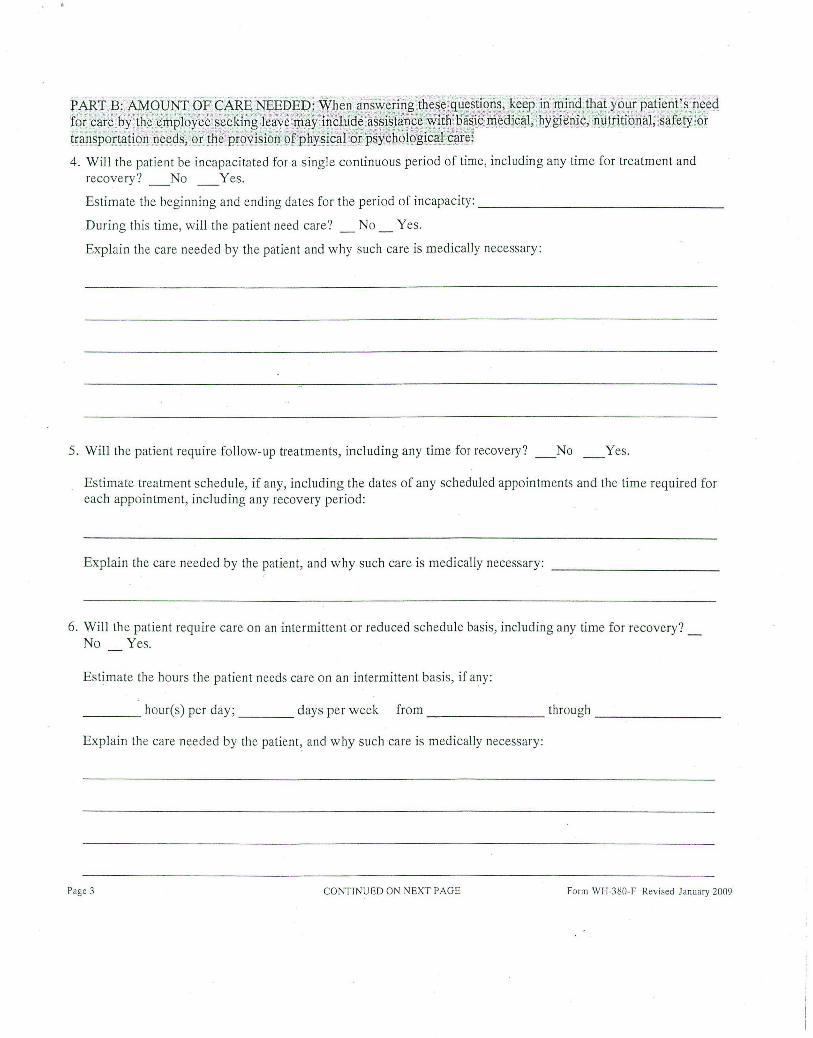
PAl{t.~:'AMqlJtrI . cfECAR)~:.:NEEbE f9f" S~f~';~~:@~'''~JTIP18y'#~';~,~:~&pg .•. " trans brtatioil'neecis 'ofthe"' i6'visi6n"6 p ....... ............. , .......... . P ...... " .. .......... .
4 . Will the patient be incapacitated for a single continuous period of time, including any time for treatment and recovery? _No _Yes.
Estimate the beginning and ending dates for the period of incapacity: ________________ _
During this time, will the patient need care? _ No _ Yes.
Explain the care needed by the patient and why such care is medically necessary :
5. Will the patient require follow-up treatments, including any time for recovery? No Yes.
Estimate treatment schedule, if any, including the dates of any scheduled appointments and the time required for each appointment, including any recovery period:
Explain the care needed by the patient, and why such care is medically necessary:
6. Will the patient require care on an intermittent or reduced schedule basis, including any time for recovery? _ No Yes.
Estimate the hours the patient needs care on an intermittent basis, if any:
____ houres) per day; ____ days per week from ________ through _______ _
Explain the care needed by the pa tient ~ and why such care is medically necessary :
Page 3 CONTINUED ON NEXT PAGE Fo rm WJ-I ·3S0 .. F Revised January 2009
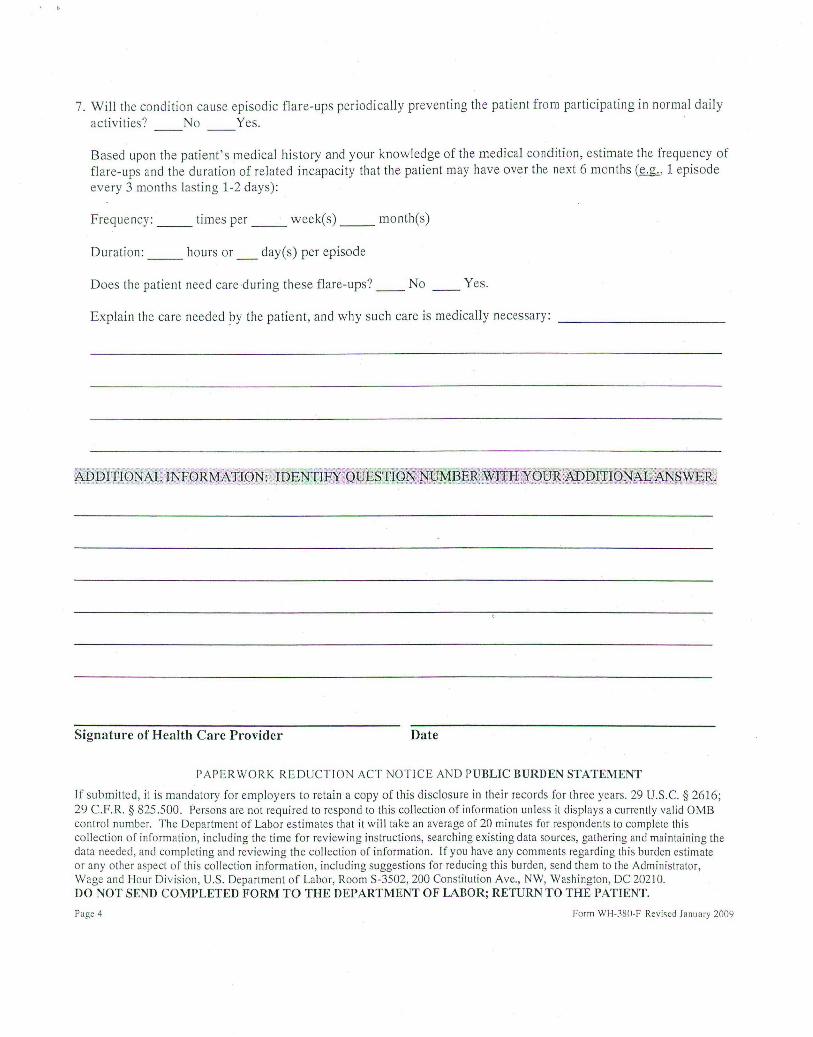
7. Will the condition cause episodic flare -ups periodically preventing th e patient from participating in normal daily
activities? No Yes.
Based upon the patient's medical hi story and your knowledge of the medical condition, estimate the frequency of
flare-ups and the duration of related incapacity that the patient may have over the next 6 months (~, 1 episode
every 3 months lasting 1-2 days):
Freque ncy: _ _ times per _ _ weekes) __ month(s)
Duration: _ _ hours or _ day(s) per episode
Does th e patient need care during th ese flare-ups? __ No Yes.
Explain the care needed by th e patient, and why such care is medically necessary: __________ _
Signature of Health Care Provider Date
PAPERWORK REDUCTION ACT NOTICE AND PUBLIC BURDEN STATEMENT
If submitted, it is mandatory for employers to retain a copy of this disclosure in their records for three years. 29 U.S.c. § 2616; 29 C.F.R. § 825.500. Persons are not required to respond to this collection of information unl ess it displays a currently valid OMB contro l number. The Department of Labor estimates th at it wi ll take an average of 20 minutes for responden ts to complete this collection of information, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. If you have any comments regarding this burden estimate or any other aspect of this col lection information, including suggestions for reducing this burden, send them to the Administrator, Wage and !-lour Division, U.S. Department of Labor, Room S-3502, 200 Constitution Ave., NW, Washington, DC 202]0. DO NOT SEND COMPLETED FORM TO THE DEPARTMENT OF LABOR; RETURN TO THE PATIENT.
Page 4 Form WH-~8n·F Revised January 200t)
Notice of Eligibility and Rights & Responsibilities
U.S. Department of Labor Employment Standards Administration Wage and Hour Division
~w: HII' ~, ' W (~_~mny .C:lnd Medi~_al Leave Act)
OMB ControIN~~ber: 1215 -oi~i Expires: 12/31/2011
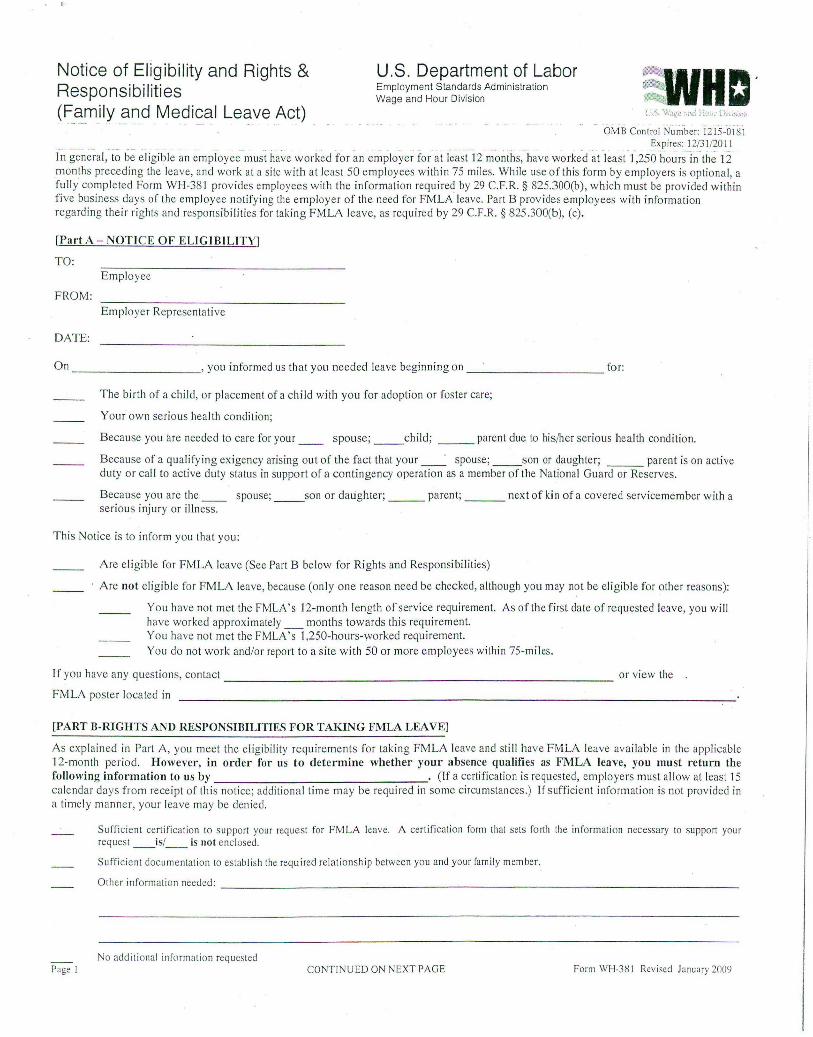
f~ gene'~al, to be eligible an employee-must have worked for an employer for at least 12 ~-onths,-have wo rked at least 1 ,250 hoursi~- the 12 m onths preceding the leave, and work at a site with at leas t 50 employees within 75 miles, While use of this form by employers is optiona l, a fully completed Form WH-381 provides employees with the information req ui red by 29 C.F.R. § 825.300(b) , which must be provided within five business days of the employee notifying the employer of the need for FMLA leave. Part B provides employees with information regarding their rights and responsibilities for tak in g FMLA leave, as required by 29 C.F.R. § 825.300(b), (c).
[Part A - NOTICE OF ELIGIBILITY]
TO: Employee
FROM: Employer Representati ve
DATE:
On __________ , you informed us that you needed leave beginning on _ ____ ___ __ for:
The birth of a ch ild, or placement of a child with you for adoption or foster care;
Your own serious hea lth cond ition;
Because you are needed to care for your __ spouse; __ child; _ __ parent due to his/her serious health condition.
Because of a qu alifying exigency aTising out of the fact that your _ _ . spouse; _ _ son or daughter; ___ parent is on active duty or cal l to ac tive duty status in support of a contingency operation as a member of the Nationa l Guard or Reserves.
Because you are the __ spouse; _ _ son or daughter; _ _ _ parent; _ __ next of kin of a covered servicemember with a serious injury or illness.
Th is Notice is to inform you th at you:
Are eligible for FMLA leave (See Part B below for Ri ghts and Responsibilities)
Are not eligible for FMLA leave, because (only one reason need be checked, although you may not be el igible for other reasons):
You have not met the FMLA's 12-mol1th length of servi ce requirement. As of the firs t date of requested leave, you wi ll have worked approximately _ months towards th is requirement. You have not met the FMLA's 1 ,250-hours-worked requirement. You do not work and/or report to a site with 50 or more employees within 75-miles.
I f you have any questions, contact or view the . ------------- ------------------------FMLA poster located in
[PART B-RIGHTS AND RESPONSIBILITIES FOR TAKING FMLA LEAVE]
As explained in Part A, you meet the eligibili ty req ui rements for taking FMLA leave and st ill have FMLA leave available in the appl icable 12-month period. However , in ordel' for us to determine whether your absence qualifies as FMLA leave, you must return the following information to us by . (If a certification is requested, employers must all ow at least 15 calendar days from receipt of this notice; additiona l time may be requi red in some circumstances.) If s ufficient information is not provided in a timely manner, your leave may be denied .
Page I
Sufficient certification to support your request for FMLA leave. A cert ification form that sets forth the information necessary to support your request _ _ is/ _ _ is 1I0t enclosed.
Sufficient documentat ion to establish the required relationship between you and your family member.
Othcrin~rmmionneeded: _ _ ___ ~ _ _ ____ _ ~ _ _ _ ~ _ _ _______ ___ _______ _ _
No add itional informntion requested CONTINUED ON NEXT PAGE Form WH·3H 1 Revised January 200'1

If your leave does qualify as FMLA leave you will have the foll owing r esponsibilities while on FMLA leave (only checked blanks apply):
Contact at to make arrangements to continue to make your share of the premium payments on yo ur health insu rance to maintain health benefi ts while you are on leave . You have a minimum 3D-day (or, ind icate lon£er period, if appl icabl e) grace period in wh ich to make premium payments. If payment is not made timely, your group health insurance may be cancelled, provid ed we not ify you in writing at least 15 days before the date that your health coverage will lapse, or, at ou r option, we may pay your share of the prem iums during FMLA leave, and recover these payments from you upon your return to work.
You will be required to use your available pa id ___ sick, ___ vacation, and/or other leave during your FMLA absence, This means that you will receive your paid leave and the leave wi ll also be considered protected FMLA leave and counted aga ins t yo ur FMLA leave entitlement.
Due to yo ur status wit hin the com pany, you are considered a "key employee" as defined in the FMLA. As a " key employee," restorat ion to
employment may be denied following FMLA leave on the grounds that such restoration will cause substantial and grievo us economic injury to us. We _have/ __ have not determined that restoring you to employment at the conclusion of FMLA leave will cause substantial and grievous economic harm to us.
Whil e on leave you w ill be required to furnish us with periodic reports of your status and intent to return to work every _ _ ___ ...,-___ _ (Indicate interval of per iod ic reports, as appropriate for the particular leave situat ion).
If the circumstances of your leave change, and you are able to return to work earlier than the date indicated on the reverse side of this form, you will be required to notify us at least two workdays prior to the date you intend to report for work.
If your leave does qualify as FMLA leave you wi ll have the foll owing rights whil e on FMLA leave:
You have a right under the FMLA for up to 12 weeks of unpaid leave in a 12-month period calculated as:
the calendar year (J anuary - December).
a fixed leave year based on _ _ _ _ ____ ___ ___ _ _ ______ ____ ___ _ _ _ ______ _
the 12-month period measured forw ard from the date of your first FMLA leave u sage.
a "rol ling" 12-month period measured backward from the date of any FMLA leave usage.
You have a right under the FMLA for up to 26 weeks of unpaid leave in a single 12-month period to care for a covered servicemember with a serious
injury or illness. T his single 12-month period commenced on _____ _ _ _________ _____ ___________ _ _
Your health benefit s must be maintained during any period of unpaid leave under the same conditions as if you continued to wo rk. You must be reinstated to the same or an equivalent job with the sam e pay, benefits, and terms and condit ions of employment on your return from FMLA-protected leave . (If your leave extends beyond the end of your FMLA ent itlement, you do not have return rights under FMLA.) If you do not return to work foll owing FM LA leave fo r a reason other than: 1) the continuation, recurrence, or onset of a ser ious health condition which wou ld enti tle you to FMLA leave; 2) the continuation, recurrence, or onset of a covered servicemember's serious injury or illness which would entitle yo u to FMLA leave; or 3) other c ircumstances beyond your contro l, you may be required to reimburse us for our share of health insurance premiums pa id on your behalf during your FMLA leave. If we have not informed you above that you must use accrued paid leave while taking your unpai d FMLA leave entitlement, you have the right to have __ sick, __ vacation, and/or _ other leave run concurrently with your unpaid leave entitlement, provided yo u meet any applicable requirements of the leave policy . Applicable conditions related to the substitution of paid leave are referenced or set fort h below. If you do not meet the requirements for tak ing paid leave, you remain entitled to take unpaid FMLA leave.
__ For a copy of conditions applicable to sick/vacation/other leave usage please refer to ______ ava ilable at: _ __________ _ _
__ Applicable condit ions for use of paid leave: ____ ________ ___ _ ____________________ _
Once we obtain the information from you as specified above, we will inform you, within 5 business days, whether your leave will be designated as FMLA leave and count tOWaI'ds your FMLA leave entitlement. If you have any questions, please do not hes itate to conL1ct:
_ __________________________ ______ ~at ______________________________ _
PAPERWoi{K REDUCTION ACT NOTICE AND PUBLIC BURDEN STATEMENT It i, mandatory for employers to provide employees with noti ce of their eligibility for FMLA protection and their rights and respons ibilities. 29 U.s.c. * 261 7; 29 C.F.R. § 82S.300(b), (c). It is mandatory for employers to retain a copy of this disc losure in their records fo r th ree years. 29 U.s.C. § 201 0; 29 C.F.R. § 825.500. Per,ons are not required to re,pond to this collection of information unless it di,plays a currently valid OMB control number. The Department of Labor estimates that it will take an average of 10 minutes fo r respondents to complete this collection of informati on, including the time for reviewing instructions, searching ex isting data source" gather ing and maintaining the data needed, and completing and reviewing the collection of information. If you have any comments regarding this burden e,timate or any other aspect of this collection information, including suggest ions for reducing this burden, send them to the Administrator, Wage and Hour Division, U.S. Department of Labor, Room S-3502, 200 Constitution Ave., NW, Washington, DC 20210. DO NOT SEND THE COMPLETED FORM TO THE WAGE AND HOUR DIVISION. . Page 2 Form WH:381 R~vised January 2009
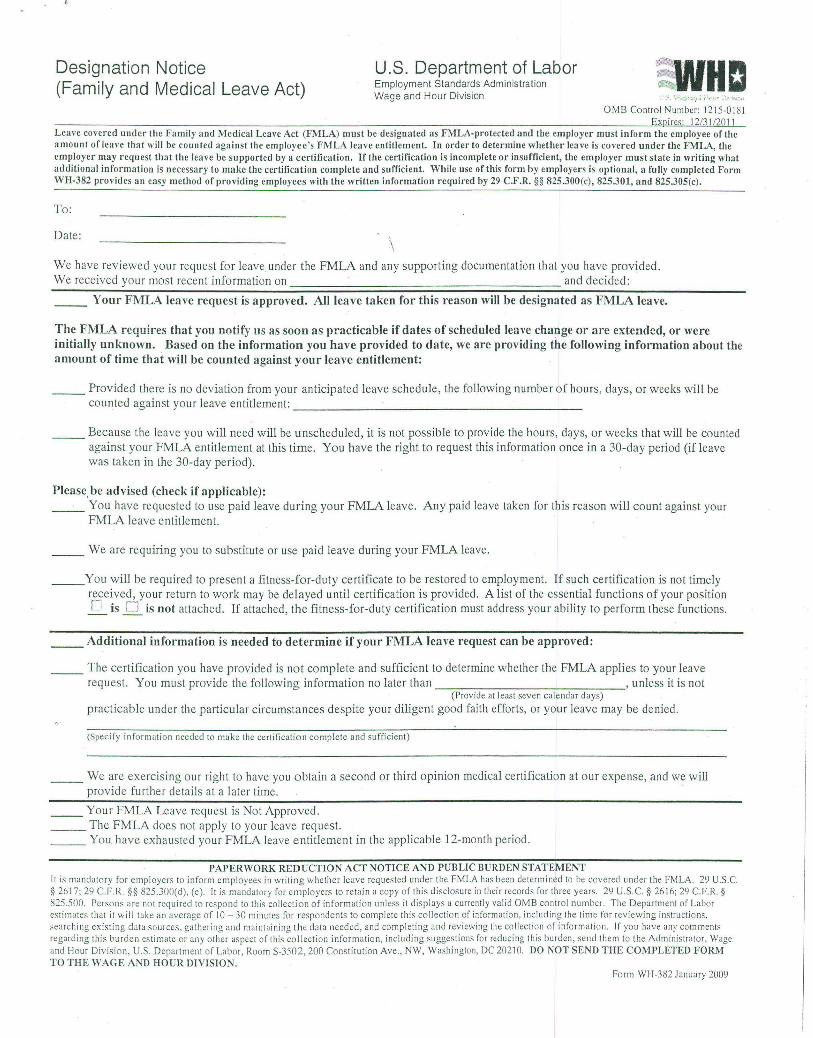
Designation Notice (Family and Medical Leave Act)
U.S. Department of Labor Employment Standards Administration Wage and Hour Division
SWHa OMS Control Number: 12 15-01~1
Expires: 12/3 1/2011 Leave covered under the Family and Medical Leave Act (FMLA) must be designated as FMLA-protected and the employer must inform the employee of the a mount of leave thnt will be counted against the employee 's FMLA leave entitlement. In order to determine whether leave is cover-ed under the FMLA, the employer may reqnest that the leave be supported by a certification. If the certification is incomplete or insufficient, the employer must state in writing what additional information is necessary to make the certification complete and sufficient. While nse of this form by employers is optional, a fully completed Form WH-382 provides an easy method of providing employees with the written information required by 29 C .F.R. §§ 825.300 (c) , 825.301, and 825.305(c).
To:
Date:
" \
We have reviewed your request for leave und er the FMLA and any supporting documentation that you have provided. We received your most recent information on and decided:
__ Your FMLA leave request is approved. All leave taken for this reason will be designated as FMLA leave.
The FMLA requires that you notify us as soon as practicable if dates of scheduled leave change or are extended, or were initially unknown. Based on the information you have provided to date, we are providing the following information about the amount of time that will be counted against your leave entitlement:
_ _ Provided there is no deviation from your anticipated leave schedule, the following number of hours, days, or weeks will be counted against yo ur leave entitlement: ______________________ _
_ _ Because the leave you will need will be unscheduled, it is not possible to provide the hours, days, or weeks that will be counted against your FMLA entitlement at this time. You have the right to request this information once in a 30-day period (if leave was taken in the 30-day period).
Please, be advised (check if applicable): _ __ You have requested to use paid leave during your FMLA leave. Any paid leave taken for this reason will count against your
FMLA leave entitlement.
__ We are requiring you to substitute or use paid leave during your FMLA leave _
__ You will be required to present a fitness-far-duty certificate to be restored to employment. If such certification is not timely r~eived , your return to work may be delayed until certification is provided. A list of the essential functions of your position L is [) is not attached. If attached, the fitness -for-duty certification must address your ability to perform these functions,
__ Additional information is needed to determine if your FMLA leave request can be approved:
_ _ The certification you have provided is not complete and sufficient to determine whether the FMLA applies to your leave request. You must provide the following information no later than , unless it is not
(Provide at least seven calendar days)
practicable under the particular circumstances despite your diligent good faith efforts, or your leave may be denied,
(Specify information needed to make the certification complete and su ffic ient)
___ We are exercising our righ t to have you obtain a second or third opinion medical certification at our expense, and we will provide further details at a later time. '
__ Your FMLA Leave request is Not Approved. __ The FMLA does not apply to your leave request. ___ You have exhausted your FMLA leave entitlement in the applicable 12-month period.
PAPERWORK REDUCTION ACT NOTICE AND PUBLIC BURDEN STATEMENT It is mandatory for employers to inform employees in writing whether leave requested under the FMl.A has been determined to be covered under the FMLA. 29 U.S.c. § 2617; 29 C.F.R. §§ 825.300(d), (e). It is mandatory for employers to retain a copy of this disclos ure in their records for three years. 29 U.S.c. § 21i Iii; 29 C.F.R. § 825.500. Persons are not required to res pond to this collect ion of information unless it displays a currently valid OMB control number. The Department of l.abor estimates that it will tak e an average of 10 - 30 minutes for respondents to complete this collection of information, including the time for reviewing instructions. searching existing data sources, gathering and maintaining the data needed , and completing and reviewing the collection of in formation . If you have any comments regarding this burden estimate or any other aspect of this collection information, including suggestions for reducing this burden, send them to the Administrator, Wage and Hour Division, U.S. Departmen t of Labor, Room S-3502, 200 Constitution Ave .. NW, Wash ington, DC 20210. DO NOT SEND THE COMl'LETED FORM TO THE WAGE AND HOUR DIVISION,
Form WH-382 January 2009
POLICE DEPARTMENT CITY OF NEW YORK
Report Under P. G.205-21 P. G. 205-28
Subject: LEAVE OF ABSENCE WITHOUT PAY FOR THIRTY (30) CALENDAR DAYS OR MORE FOR THE PURPOSE OF HARDSHIP, EDUCATION, CHILD CARE, FMLA, ETC.
"I have requested an extended leave of absence for thirty days or more for the purpose of
---------------------- and not for other full time employment. I am aware that full time employment is any employment requiring over twenty (20) hours a week per the General Municipal Law, Section 208D. I agree if this leave is approved, that I will not accept other employment while on this leave without the Department's prior approval, obtained through the Military and Extended Leave Desk. Failure to obtain such approval may be cause for termination of my employment with the Police Department."
NOTARY STAMP/SEAL
State of ----------------------County of --------------------City of ___ _____ __ -----::-On this day of ----------------
__ ~---------------- 20 Before me personally came
to me known and known to me to be the individual described herein and who executed the foregoing instrument, and duly acknowledged to me that he/she executed the same.
Notary Public/Commissioner of Deeds
Signature Date
7
PURPOSE
PROCEDURE
UNIFORMED MEMBER OF THE SERVICE
NOTE
PATROL SUPERVISOR
PATROL GUIDE Section: Command Operations Procedure No: 212-32
OFF DUTY INCIDENTS INVOLVING UNIFORMED MEMBERS OF THE SERVICE
DATE ISSUED: I DATE EFFECfIVE: I REVISION NUMBER: I PAGE: 07/27/07 08/03/07 07-04 10fl
To facilita te the preliminary investigation of off duty incidents involving uniformed members of the service.
When an off duty unifo rmed member of the service is at an unusual police occurrence to w hich the uniformed member of the servite is either a participant or a witness:
1.
2.
Remain at the scene of incident when feasible and consistent with personal safety. Request response of patrol supervisor, precinct of occurrence.
For purposes of this p rocedure an unusual police occurrence shall include family disputes and other incidents of domestic violence in which the officer is either a participant or a witness. When remaining at the scene is inappropriate, the uniformed member of the service concerned may leave the scene; however, said member must promptly notify the desk officer, precinct of occurrence, and be guided by the desk officer's instructions. If incident occurs outside of the City the uniformed member of the service concerned will promptly notify the Operations Unit. The Operations Unit will notify the appropriate patrol borough responsible for conducting investigations in the residence county, or the appropriate authority if outside residence counties.
3. 4.
Respond to scene and assess situation. Notify desk officer of available details.
DESK OFFICER 5. 6.
COMMANDING 7. OFFICER! COUNTERPART
Conduct investigation and take appropriate action.
NOTE
RELATED PROCEDURES
Any investigation of a police incident or unusual occurrence, including domestic violence and family disputes, which involve an off duty uniformed member of the service as a participant or witness will benefit from that uniformed member's presence.
I nterrogation of M embers of the S ervice (P.G. 206-13) Unusual Occurrence Reports (P.G. 212-09)
NEW • YORK • CITY • POLICE • DEPARTMENT

'SAl~LE SAMPLE SAMPLE
tNSTRUCTIONS: All Copies Should Accompany Member of the SeNice Appearing at the NYC Police Pension Fund
Rank
PROPERTY RECEIPT - DISCONTINUANCE OF SER VICE PD 520·013 (Rev. 05·09)
Command
Last Four Digits Of Soc. Sec. No.
Tax Reg. No.
Member is 0 SERVICE RETIREMENT 0 DISABILITY RETIREMENT 0 VESTED INTEREST Applying For: 0 RESIGNATION 0 EXTENDED LEAVE OF ABSENCE (30 days or more) 0 WITHOUT PAY
DEPARTMENT EQUIP M ENT DISPOSITION (Use Boxes 13-15 For Equipment Returned Not Listed Be /ow) ITE M
1. SHIELD
2. 1.0. CARD
3. O.C. PEPPER SPRAY NUMBER:
4 . HELMET
5. NEW YORK CITY TRANSIT POUCE PASS METRO CARD
6. LlRR POLICE PASS
7, METRO·NORTH RR ( POLICE PASS
~
RECEIVED B Y (Printed) SIGNATURE C OMM A ND
~ ~ r--- ,---
\ I \ I \ 8, DEPARTMENT n CELL PHONE I \ n
ommunications ivision. elecommunicatio s Unit, , __ -'
ne Police Plaza. Room 91 PB ..
9, RESTRICTED/HQ ANN8X
~ I \ J PARKING PERMIT
10, NYPD VEHICLE 0\ \ I \ \ \I i IDENTIFICATION PLATE
11, DEPARTMENT RADIO h\ I L-J \ ~ I 12, LAPTOP COMPUTER U I \ I (CAPTAINS AND ABO E)
13, ) I Il \ I 14, '\~ L-J L--.J '-- ILJ '--- ~
15,
Unused Summonses Returned? D YES 0 NO Charges Pending? 0 YES 0 NO Next Scheduled Tour After Leaves, Except Terminal Leave:
ISignature of Commanding Officer
FOR NYC POLICE P=NSION FUND USE ONLY ;',>,:;,/". / Date Filed T,L. Begins
LW Begins Ends
O P I I Disposition Of Firearms If Not Delivered To Property Clerk
WAIVER TO
BEGIN T.L.
Remarks:
o APPROVE D
o DISAPPROVED
PREPAR ED RanklTitle BY:
Rank, Name, Command
Name Printed
ReI. Date Date
Date Property To Be Turned In:
I Signature
l
I
TO:
PERSONNEL BUREAJ MEMO
DATE ISSUED: June 15,2009 I NUMBER: 44
ALL COMMANDS I
SUBJECT: NEW MILITARY AND EXTENDED LEAVE DESK (MELD) INTERNET . WEBSITE
1 . The Department has recently created a new Military and Extended Leave Desk (MELD) Internet Website, which can be accessed from the Finest Health website. The MELD website is designed to provide access to uniformed and civilian members of the servic~ to obtain MELD forms, Department bulletins, special announcements, and other helpful website links.
2. Members may access the MELD website via the Internet by entering www.nyc.gov/nypd. Once at the homepage, select "Employees" which is located on the left hand side under "Find Services," Click on link to "Finest Health" website. Login as follows:
Username: finesthealth Password: s,tayhealthy (must be lowercase)
The link to the MELD website is located on the upper right corner of the Finest Health webpage.
3. The Department will continually update the MELD Internet Website as new information becomes available. The Department encourages its members to offer feedback by contacting the Military and Extended Leave Desk at (646) 610-5513 or via e-mail: [email protected].
4. In addition, members are reminded they may also access the Military and Extended Leave Desk (MELD) website via the Department Intranet as follows:
1. Log onto the NYPD intranet homepage. 2. Select "Benefits". 3. Select "Military and Extended Leave Desk" to access the website.