reporting of skin cancer using rcpath standards. a regional perspective
DESCRIPTION
Reporting of Skin cancer using RCPath Standards. A regional perspective. Paul Barrett. Aim. Determine if RCPath standards have been adopted Part of network clinical guidelines (Jul13) RCPath Oct12 (revised May14) Pathology can be critical in determining cases to be discussed at MDT - PowerPoint PPT PresentationTRANSCRIPT

Reporting of Skin cancer using RCPath Standards.
A regional perspective.
Paul Barrett

Aim
• Determine if RCPath standards have been adopted– Part of network clinical guidelines (Jul13)– RCPath Oct12 (revised May14)
• Pathology can be critical in determining cases to be discussed at MDT– Excisional intent – High risk– Incompletely excised

• Planned high quality cancer care to just over 3 million people in the North of England
• 8 Foundation and 1 NHSTrusts
• 14 Primary Care Trusts (PCTs)
• 5 localities

Method
• 25 reports requested from 2014 – Each cancer type– Each centre reporting in North East
• Core items in RCPath guidelines assessed
• One centre failed to submit by deadline
• Not all cases suitable
• Not all sites had 25 cases
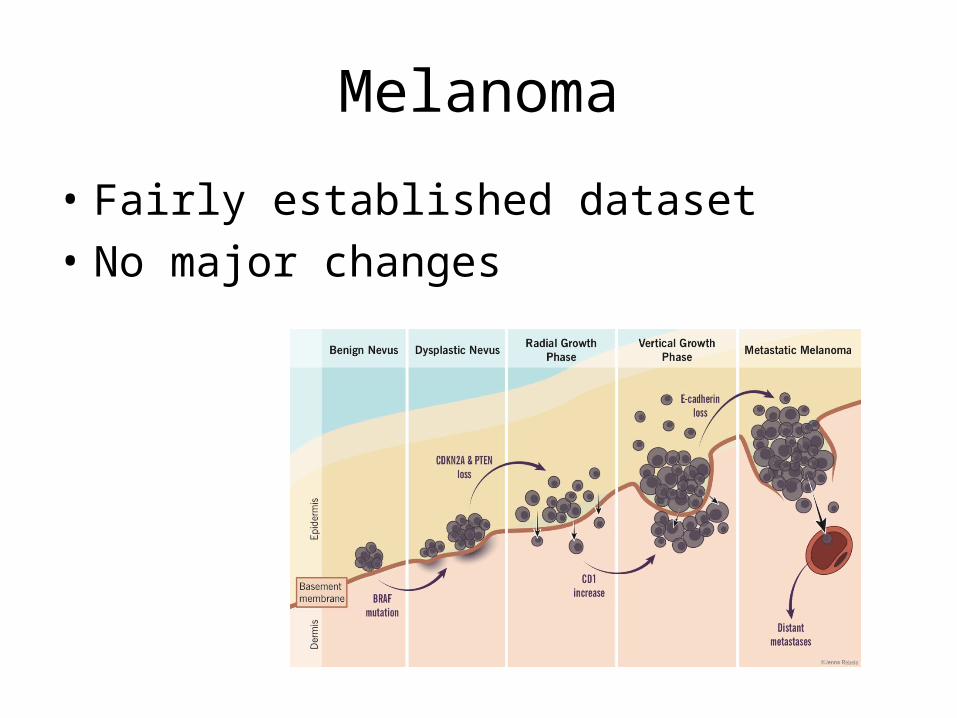
Melanoma
• Fairly established dataset
• No major changes

Results - Melanoma
• 101 cases• Local MDT
– 31
• Proforma – 75
• Non-proforma – 4 central (6%) – 22 local (71%)
Lab Cases
1 25
2 8
3 19
4 4
5 26
6 11
7 8

Results - Melanoma
• All cases– Macroscopic description skin ellipse– Macroscopic description lesion– Excision margins

Results - Melanoma
Critical results
• Breslow 1 (1/0)
• Clark’s 6 (5/1)
• Ulceration 7 (7/0)
• 12 cases do not include vital data
• All destined for review

Results - Melanoma
• LVI 5 (5/0)
• PNI 11 (11/0)
• Microsat 52 (22/30)
• Subtype 13 (12/1)
• Growth phase 9 (9/0)
• Stage 21 (18/3)

Results - Melanoma
• Mitotic rate 2 (2/0)
• Regression 17 (15/2)
• TiL 14 (14/0)
• All data items provided 47 (46%)

SCC
• Significant change around risk status
• Complexity with pT2– Any two of
• Poor differentiation• Into subcutaneous tissue• >2mm• Into reticular dermis

Results - SCC
• 126 cases• Local MDT
– 52 (41%)
• Proforma – 63 (all central)
• Non-proforma – 11 central (17%) – 52 local (82%)
Lab Cases
1 25
2 9
3 25
4 2
5 24
6 20
7 21

Results - SCC
• All cases– Macroscopic description skin ellipse– Macroscopic description lesion– Excision margins

Results - SCC
Critical results
• Grade 8 (8/0)
• Thickness 10 (10/0)
• Level 32 (30/2)

Results - SCC
• LVI 7 (7/0)
• PNI 22 (22/0)
• Subtype 47 (47/0)
• Risk 86 (54/32)
• Stage 65 (41/24)

Results - SCC
• Correct assessment of risk– Recorded in 40
• 3 incorrect• 2 insufficient data in report to assess
• All data items provided 25%• 32 cases (2/30)

BCC
• Established data set
• Is it really cancer?
• Multiple specimens common

Results - BCC
• 159 cases• Local MDT
– 86 (54%)
• Proforma – 65 (all central)
• Non-proforma – 8 central (17%) – 86 local (100%)
Lab Cases
1 25
2 21
3 25
4 25
5 23
6 22
7 18

Results - BCC
• All cases– Macroscopic description skin ellipse– Macroscopic description lesion

Results - BCC
Key results
• Growth pattern 1 (1/0)
• Level 57 (56/1)
• Margins 2 (1/1)

Results - BCC
• LVI 28 (27/1)• PNI 15 (14/1)
• Risk 85 (85/0)• Stage 92 (68/24)
• All data items provided 26%• 41 cases • Combination risk and/or stage absent

Recommendations
• Data could be derived
• Melanoma review centrally
• Confirms value in reporting by proforma– College KPI
• Ensure proforma contains all core items
• Re-audit or audit locally

Clinical
imunosuppression
radiation, burn or chronic inflammation
Site: Specimen type: Curette / Shave / Punch / Incisional ExcisionalSize: Length Width to a depth of
Size of lesion: mm high risk if >20mm Marker & ink: o’clock inked margin-Description:
LLP SH BB Tips: Transverse: SqCC Subtype:
Classic KA-like Verrucous Acantholytic Spindle cell Other:
Grade: Well Moderate Poor Thickness: mm >4mm Stage may increase if >2mm
Adj Bowen’s dis:
No Yes
BCC Subtype:
Superficial Nodular
Infiltrative Micronodular Atypical Sq D: No Yes
Level of invasion:
confined to epidermis into papillary dermis
fills papillary dermis
into reticular dermis*
into subcutaneous fat *possible stage increase for SqCCa
LVI: No Yes PNI: No Yes Margins peripheral: involved clear <1mm clear 1-5mm
clear 5mm+ at unspecified margin/ o’clock deep:
involved clear <1mm clear 1-5mm clear 5mm+
T stage:SCC only
pT1 <=20mm pT2 pT3+ pT2 if 2 of poor diffn, PNI, lip/ear site, into reticular dermis, >2mm thick
Risk status: Low HighMDT discussion: No Yes (excisional, high risk and incomplete)
Comments:
Thickness: mm >4mm Stage may increase if >2mm
Adj Bowen’s dis: No Yes
BCC Subtype: Superficial Nodular
Infiltrative Micronodular
Atypical Sq D: No Yes Level of invasion: confined to epidermis into papillary dermis
fills papillary dermis into reticular dermis*
into subcutaneous fat *possible stage increase for SqCCa
LVI: No Yes PNI: No Yes Margins peripheral: involved clear <1mm clear 1-5mm
clear 5mm+ at unspecified margin/ o’clock deep: involved clear <1mm clear 1-5mm
clear 5mm+
T stage: SCC only
pT1 <=20mm pT2 pT3+ pT2 if 2 of poor diffn, PNI, lip/ear site, into reticular dermis, >2mm thick



Questions?