request for change in family income in income (new).pdf · change of family composition request ......
TRANSCRIPT
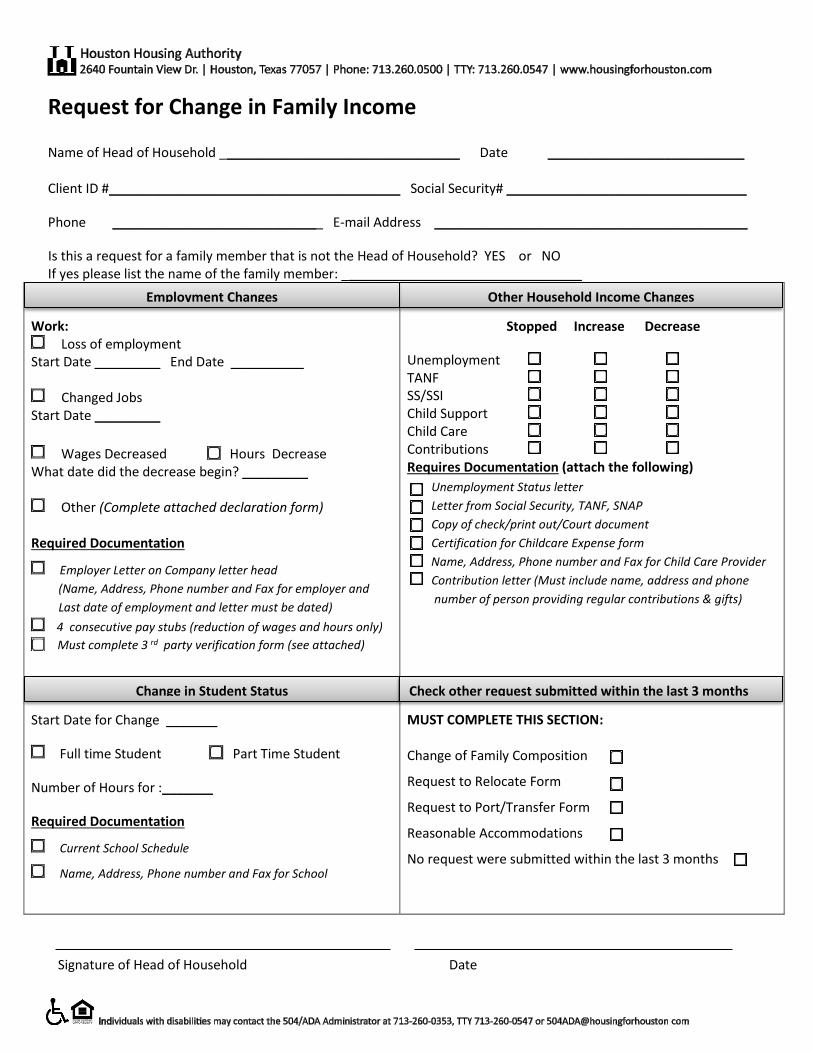
Request for Change in Family Income
Name of Head of Household _________________________________ Date ___________________________ Client ID #________________________________________ Social Security# _________________________________
Phone ____________________________ E-mail Address ___________________________________________
Is this a request for a family member that is not the Head of Household? YES or NO If yes please list the name of the family member: _________________________________
Work: Loss of employment
Start Date _________ End Date __________
Changed Jobs Start Date _________
Wages Decreased Hours Decrease What date did the decrease begin? _________
Other (Complete attached declaration form) Required Documentation
Employer Letter on Company letter head
(Name, Address, Phone number and Fax for employer and
Last date of employment and letter must be dated)
4 consecutive pay stubs (reduction of wages and hours only)
Must complete 3 rd
party verification form (see attached)
S
Stopped Increase Decrease
Unemployment TANF SS/SSI Child Support Child Care Contributions Requires Documentation (attach the following)
Unemployment Status letter
Letter from Social Security, TANF, SNAP
Copy of check/print out/Court document
Certification for Childcare Expense form
Name, Address, Phone number and Fax for Child Care Provider
Contribution letter (Must include name, address and phone
number of person providing regular contributions & gifts)
Start Date for Change _______
Full time Student Part Time Student
Number of Hours for :_______
Required Documentation
Current School Schedule
Name, Address, Phone number and Fax for School
MUST COMPLETE THIS SECTION: Change of Family Composition
Request to Relocate Form
Request to Port/Transfer Form
Reasonable Accommodations
No request were submitted within the last 3 months
Signature of Head of Household Date
Other Household Income Changes
Change in Student Status
Check other request submitted within the last 3 months
Employment Changes
Dear Client:
We are committed to processing your Interim Change in Family Income request in a timely manner. However, all of the required documentation to support the change must be submitted with the request. Change request forms must be complete, signed, and legible. We cannot accept requests that are incomplete. Interim Change Request Packets can be submitted in person or by mail. If mailing, send only copies, and do not include original documents. Due to processing constraints, we can only provide a status on interim changes that have been submitted at least 30 days prior. Status request can be submitted via email to [email protected], and we will provide a
status via email within 3 business days (not including weekends or holidays). Don’t forget to check your spam mailbox.
It is your responsibility to continue to pay your portion of the rent until the interim change is effective. If you are approved for a change of income, a rent change notification letter will be mailed to you and to the landlord. If your request has been denied, a denial letter will be mailed to you within 30 days. HHA Interim Change Request Forms and Required Documents:
1. Change of Income Packet returned with all pages. 2. Request for Change in Family Income Form must be signed and returned. 3. Houston Housing Authority Required Forms
o HUD Authorization to Release of Information – 9886 (Must be signed by head of household and anyone in household 18 and older)
o 3rd Party Income Verification Form o Unemployment Benefit (if receiving or applied for UEB must submit proof of benefits from Texas Work Source
Commission - www.twc.state.tx.us/ui/unemployment-benefits-services) o Non Income Affidavit (A &B if the is no income of any source for household) o Contribution and Gifts Letter o Household Assets Self Certification Form o Authorization for Release of Information (Must be signed by head of household and anyone in household 18 and
older) o Declaration Form o School Verification Form (If Applicable. Must be filled out by the school with the students schedule included) o Child Care Expenses Verification Form (If Applicable. Must be filled out by the child care provider)
Client must attach: 1. All Supporting Documentation 2. Request for Change in Family Income Packet and Form 3. Houston Housing Authority Required Forms
Thank you, HHA staff
Housing Choice Voucher Program DECLARATIONS
(Please Print)
Client’s Name: _____________________
Social Security #: _______________________
I would like to declare the following: _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ _____________________________ _________________________________ Your Signature Date _____________________________ Your address _____________________________ Your phone # _____________________________ Email
2640 Fountain View Drive Houston, Texas 77057 | 713.260.0600 P| 713.260.0547 TTY| www.housingforhouston.com
A Fair Housing and Equal Opportunity Agency
For assistance: Individuals with disabilities may contact the 504/ADA Administrator
at 713-260-0528, TTY 713-260-0547 or [email protected].
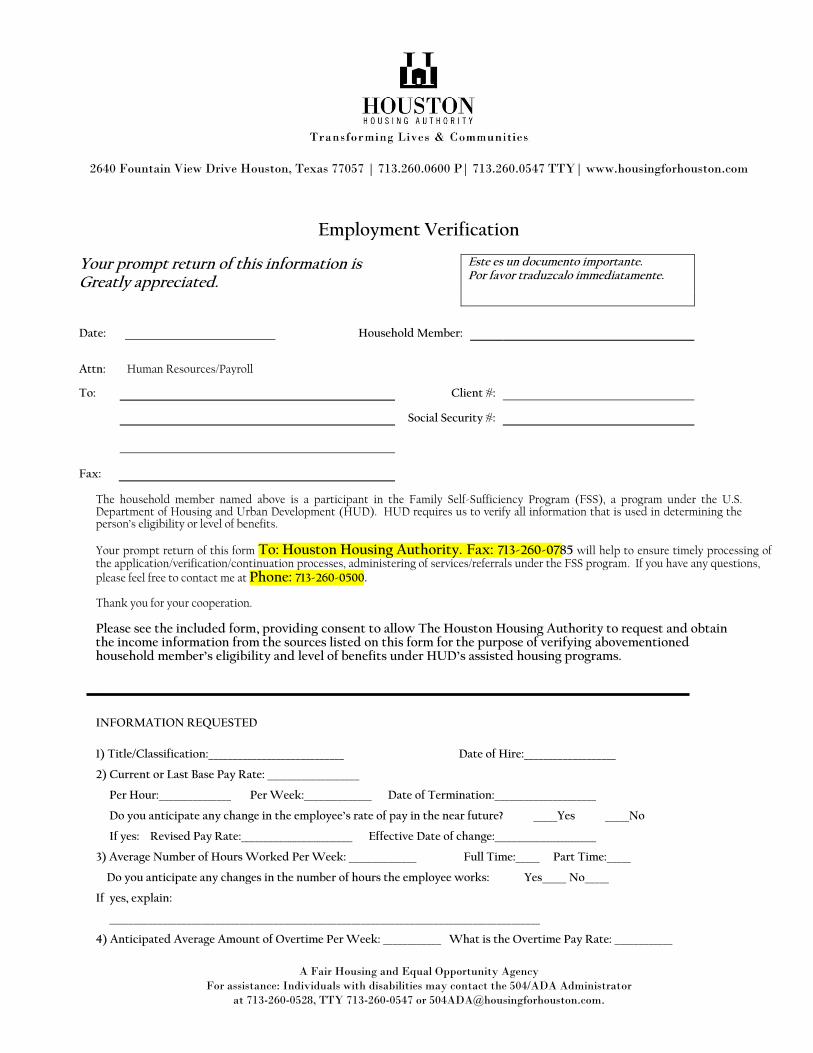
Employment Verification
Your prompt return of this information is Greatly appreciated.
Este es un documento importante. Por favor traduzcalo immediatamente.
Date: Household Member:
Attn: Human Resources/Payroll
To: Client #:
Social Security #:
Fax: The household member named above is a participant in the Family Self-Sufficiency Program (FSS), a program under the U.S. Department of Housing and Urban Development (HUD). HUD requires us to verify all information that is used in determining the person’s eligibility or level of benefits. Your prompt return of this form To: Houston Housing Authority. Fax: 713-260-0785 will help to ensure timely processing of the application/verification/continuation processes, administering of services/referrals under the FSS program. If you have any questions, please feel free to contact me at Phone: 713-260-0500. Thank you for your cooperation. Please see the included form, providing consent to allow The Houston Housing Authority to request and obtain the income information from the sources listed on this form for the purpose of verifying abovementioned household member’s eligibility and level of benefits under HUD’s assisted housing programs.
-
INFORMATION REQUESTED
1) Title/Classification:____________________________ Date of Hire:___________________
2) Current or Last Base Pay Rate: ___________________
Per Hour:_______________ Per Week:______________ Date of Termination:_____________________
Do you anticipate any change in the employee’s rate of pay in the near future? _____Yes _____No
If yes: Revised Pay Rate:_______________________ Effective Date of change:_____________________
3) Average Number of Hours Worked Per Week: ______________ Full Time:_____ Part Time:_____
Do you anticipate any changes in the number of hours the employee works: Yes_____ No_____
If yes, explain:
_________________________________________________________________________________________
4) Anticipated Average Amount of Overtime Per Week: ____________ What is the Overtime Pay Rate: ____________
Houston Housing Authority
Page 2 of 2
A Fair Housing and Equal Opportunity Agency
For assistance: Individuals with disabilities may contact the 504/ADA Administrator
at 713-260-0528, TTY 713-260-0547 or [email protected].
5) How often is Employee Paid: ____Weekly ____Bi-Weekly ____ Semi-Monthly ____ Monthly
6) Is Employee on: ______Piecework Timework ______Seasonal
If the employee’s work is seasonal or sporadic, indicate lay –off period: ______________________________
7) Is Employee currently on: ___ Medical Leave ___Maternity ____ Military ____ Other
Effective Date:_______________________ Anticipated End Date:___________________________ Will employee be entitled to Workman’s Compensation ____ Yes ____No
What is the percentage, or amount of pay employee will receive while on leave of absence: _______% / $________
8) Gross annual earnings you anticipate for this employee for the next twelve months. (Gross amount including all tips, bonuses, overtime, commissions.) Effective date of anticipated earnings?___________________ 9) Anticipated Tips, Commissions, Bonuses $ 10) Does this employee receive vacation? Yes No With Pay? Yes No 11) Amount deducted for medical coverage $ _________________ per _________________ 12) Is employee paid on a 9 month _____ or a 12 month ______ cycle? (School Districts Only) _____________________________________ ______________________________ Print Name & Title of Official: Date: _____________________________________ ______________________________ Signature: Telephone Number: Company Stamp (if applicable):
Family Income -- 3rd Party Verification Contact Information This form must be completed Employment (If applicable) check one: Previous or Current Corporate Company Name: ______________________________________________________________ Corporate Company Address: ____________________________________________________________ Phone number#: __________________________________ Fax#_______________________________ Address of actual work location: __________________________________________________________ Contributions (If applicable) Contributors Name: ____________________________________________________________________ Contributors Address: __________________________________________________________________ Phone#: _____________________________________ Fax#____________________________________ School Verification (If applicable - 18 and older) Name of School: _______________________________________________________________________ School address: _______________________________________________________________________ Phone#: _____________________________________Fax#_____________________________________ Child Care Provider (If applicable) Name of Child Care Provider: _____________________________________________________________ Child Care Providers address: _____________________________________________________________ Phone#: ______________________________________Fax#____________________________________ Child Support (all filed child support orders, regardless of whether payment is received and proof of payment) Cause# _______________________________________________________________________________ CIN#_________________________________________________________________________________ Unemployment Benefits (If applicable) Did you apply for unemployment benefits?
Yes (Attach status letter) No (Must apply and provide proof)
Start Date: _________________________________ End Date: __________________________________ Weekly Benefit Amount: ______________________
2 of 2
Certification of Information
WARNING: TITLE 18, SECTION 1001 OF THE UNITED STATES CODE STATES THAT A PERSON IS GUILTY OF A FELONY FOR KNOWINGLY AND WILLINGLY MAKING FALSE OR FRAUDULENT STATEMENTS TO ANY DEPARTMENT OR
AGENCY OF THE UNITED STATES AND SHALL BE FINED NOT MORE THAN $10,000 OR IMPRISONED FOR NOT MORE THAN FIVE YEARS OR BOTH.
I hereby certify that all of the information I have provided on this reexamination form is true and complete.
Signature of Head of Household Date
Signature of Spouse or Co-head Date
Current Phone Number
Name & Phone Number of an Emergency Contact
Email Address
Page 1 of 2
AUTHORIZATION FOR RELEASE OF INFORMATION CONSENT I authorize and direct any federal, state or local agency, organization, business, or individual to release to the Houston Housing Authority any information or materials needed to complete and verify my application for housing assistance and/or to maintain my continued occupancy of housing furnished by or through the Housing Authority. I understand and agree that this authorization or the information obtained with its use may be given to and used by the Housing Authority in administering and enforcing program rules and policies. I also consent for HUD or the Housing Authority to release information from my participant file related to my rental history to credit bureaus, collections agencies and/or future landlords. This includes records on my payment history, and any violations of my lease or PHA policies. I authorize the Houston Housing Authority to release to any entity or person any information relating to me if the Houston Housing Authority determines that releasing such information might lead to additional assistance being provided to me. INFORMATION COVERED I understand that, depending on program policies and requirements, previous or current information regarding my household or me may be requested; this includes but is not limited to: Identity and Marital Status Residences and Rental Activity Income Medical or Child Care Allowances Credit and Criminal Activity Employment, Income, and Assets I understand that this authorization cannot be used to obtain any information about me that is not pertinent to my eligibility and continued participation in a housing assistance program. GROUPS OR INDIVIDUALS THAT MAY BE ASKED The groups or individuals that may be asked to release the above information (depending on program requirements) includes, but not limited to: Previous Landlords (including Veteran’s Administration Retirement/Pensions Public Housing Agencies) Welfare Agencies Courts and Post Offices Law Enforcement Agencies Schools and Colleges Social Security Support and Alimony Providers Credit Bureaus and Providers Administration Utility Companies Mortgage Companies Lending Institutions Medical and Child Care Providers
COMPUTER MATCHING NOTICE AND CONSENT I understand and agree that the Housing Authority may conduct computer-matching programs to verify the information supplied for my application or re-examination. If a computer match is done, I understand that I have a right to notification of any adverse information found and a chance to disprove incorrect information. HUD or the Housing Authority may, in the course of its duties exchange such automated information with other federal, state, or local agencies, including but not limited to State Employment Security agencies; Department of Defense; Office of Personnel Management; U.S. Postal Services; Social Security Agency; and State Welfare and food stamp agencies.
Page 2 of 2
CONDITIONS I agree that a photocopy of this authorization may be used for the purposes stated above. The original of this authorization is on file with the PHA and will stay in effect for a year and three months from the date signed. I understand I have a right to review my file and correct any information that I can prove is incorrect. Signature(s) Printed Name Date
Head of Household
Spouse/Co-Head
Adult Member NOTE: This general consent may not be used to request a copy of a tax return. If a copy of a tax return is needed, IRS Form 4506, “Request for a copy of a tax form” must be prepared and signed separately.

Authorization for the Release of Information/ Privacy Act Notice to the U.S. Department of Housing and Urban Development(HUD)
and the Housing Agency/Authority (HA) PHA requesting release of information; (Cross out space if none) (Full address, name of contact person, and date)
Houston Housing Authority
2640 Fountain View Suite 100
Houston, TX 77057
Authority: Section 904 of the Stewart B. McKinney Homeless
Assistance Amendments Act of 1988, as amended by Section 903
of the Housing and Community Development Act of 1992 and
Section 3003 of the Omnibus Budget Reconciliation Act of 1993.
This law is found at 42 U.S.C. 3544.
This law requires that you sign a consent form authorizing: (1)
HUD and the Housing Agency/Authority (HA) to request verifi-
cation of salary and wages from current or previous employers; (2)
HUD and the HA to request wage and unemployment compensa-
tion claim information from the state agency responsible for
keeping that information; (3) HUD to request certain tax return
information from the U.S. Social Security Administration and the
U.S. Internal Revenue Service. The law also requires independent
verification of income information. Therefore, HUD or the HA
may request information from financial institutions to verify your
eligibility and level of benefits.
Purpose: In signing this consent form, you are authorizing HUD
and the above-named HA to request income information from the
sources listed on the form. HUD and the HA need this information
to verify your household’s income, in order to ensure that you are
eligible for assisted housing benefits and that these benefits are set
at the correct level. HUD and the HA may participate in computer
matching programs with these sources in order to verify your
eligibility and level of benefits.
Uses of Information to be Obtained: HUD is required to protect
the income information it obtains in accordance with the Privacy
Act of 1974, 5 U.S.C. 552a. HUD may disclose information
(other than tax return information) for certain routine uses, such as
to other government agencies for law enforcement purposes, to
Federal agencies for employment suitability purposes and to HAs
for the purpose of determining housing assistance. The HA is also
required to protect the income information it obtains in accordance
with any applicable State privacy law. HUD and HA employees
may be subject to penalties for unauthorized disclosures or im-
proper uses of the income information that is obtained based on the
consent form. Private owners may not request or receive
information authorized by this form.
Who Must Sign the Consent Form: Each member of your
household who is 18 years of age or older must sign the consent
form. Additional signatures must be obtained from new adult
members joining the household or whenever members of the
household become 18 years of age.
U.S. Department of Housing and Urban Development Office of Public and Indian Housing OMB CONTROL NUMBER: 2501-0014 IHA Requesting Release of information of information:(Cross out space if none) (full address, name of contact person, and date)
Persons who apply for or receive assistance under the following
programs are required to sign this consent form:
PHA-owned rental public housing
Turnkey III Homeownership Opportunities
Mutual Help Homeownership Opportunity
Section 23 and 19(c) leased housing
Section 23 Housing Assistance Payments
HA-owned rental Indian housing
Section 8 Rental Certificate
Section 8 Rental Voucher
Section 8 Moderate Rehabilitation
Failure to Sign Consent Form: Your failure to sign the consent
form may result in the denial of eligibility or termination of
assisted housing benefits, or both. Denial of eligibility or termi-
nation of benefits is subject to the HA’s grievance procedures and
Section 8 informal hearing procedures.
Sources of Information To Be Obtained
State Wage Information Collection Agencies. (This consent is
limited to wages and unemployment compensation I have re-
ceived during period(s) within the last 5 years when I have
received assisted housing benefits.)
U.S. Social Security Administration (HUD only) (This consent is
limited to the wage and self employment information and pay-
ments of retirement income as referenced at Section 61
03(l)(7)(A) of the Internal Revenue Code.)
U.S. Internal Revenue Service (HUD only) (This consent is
limited to unearned income [i.e., interest and dividends].)
Information may also be obtained directly from: (a) current and
former employers concerning salary and wages and (b) financial
institutions concerning unearned income (i.e., interest and divi-
dends). I understand that income information obtained from these
sources will be used to verify information that I provide in
determining eligibility for assisted housing programs and the
level of benefits. Therefore, this consent form only authorizes
release directly from employers and financial institutions of
information regarding any period(s) within the last 5 years
when I have received assisted housing benefits.
Consent: I consent to allow HUD or the HA to request and obtain income information from the sources listed on this form for the
purpose of verifying my eligibility and level of benefits under HUD’s assisted housing programs. I understand that HAs that receive
income information under this consent form cannot use it to deny, reduce or terminate assistance without first independently
verifying what the amount was, whether I actually had access to the funds and when the funds were received. In addition, I must be
given an opportunity to contest those determinations.
This consent form expires 15 months after signed.
Signatures:
Head of Household Date
Social Security Number (if any) of Head of Household Other Family Member over age 18 Date
Spouse Date Other Family Member over age 18 Date
Other Family Member over age 18 Date Other Family Member over age 18 Date
Other Family Member over age 18 Date Other Family Member over age 18 Date
Privacy Act Notice. Authority: The Department of Housing and Urban Development (HUD) is authorized to collect this information by
the U.S. Housing Act of 1937 (42 U.S.C. 1437 et. seq.), Title VI of the Civil Rights Act of 1964 (42 U.S.C. 2000d), and by the Fair Housing
Act (42 U.S.C. 3601-19). The Housing and Community Development Act of 1987 (42 U.S.C. 3543) requires applicants and participants to
submit the Social Security Number of each household member who is six years old or older. Purpose: Your income and other information are
being collected by HUD to determine your eligibility, the appropriate bedroom size, and the amount your family will pay toward rent and
utilities. Other Uses: HUD uses your family income and other information to assist in managing and monitoring HUD-assisted housing programs,
to protect the Government’s financial interest, and to verify the accuracy of the information you provide. This information may be released to
appropriate Federal, State, and local agencies, when relevant, and to civil, criminal, or regulatory investigators and prosecutors. However, the
information will not be otherwise disclosed or released outside of HUD, except as permitted or required by law. Penalty: You must provide
all of the information requested by the HA, including all Social Security Numbers you, and all other household members age six years and
older, have and use. Giving the Social Security Numbers of all household members six years of age and older is mandatory, and not
providing the Social Security Numbers will affect your eligibility. Failure to provide any of the requested information may result in a delay
or rejection of your eligibility approval.
Penalties for Misusing this Consent:
HUD, the HA and any owner (or any employee of HUD, the HA or the owner) may be subject to penalties for unauthorized disclosu res or improper uses of information collected based on the consent form.
Use of the information collected based on the form HUD 9886 is restricted to the purposes cited on the form HUD 9886. Any per son who knowingly or willfully requests, obtains or discloses any information under false pretenses concerning an appl icant or participant may be subject to a misdemeanor and fined not more than $5,000.
Any applicant or participant affected by negligent disclosure of information may bring civil action for damages, and seek oth er relief, as may be appropriate,
against the officer or employee of HUD, the HA or the owner responsible for the unauthorized disclosure or improper use.
Original is retained by the requesting organization. ref. Handbooks 7420.7, 7420.8, & 7465.1 form HUD-9886 (7/94)
Change of Income Interim FAQ Q1. I am no longer employed. What type of proof do I need to provide?
A. Employer letter on company letter head with dates the employment began and ended.
Or
Go to Work Source and request a print out of Benefits and Initial Claims – Current Claim status.
Also apply for unemployment and submit proof you applied for Unemployment Benefits
www.twcstate.tx.us/ui/unemployment
Q2. My hours and or wages have been reduced. What proof do I need to provide?
A. 2 – 4 consecutive pay stubs
Q3. I am on an approved leave with my employer and will not get paid during this time. What proof do I need to provide?
A. Employer letter on company letter head with date the change will begin. B. 2-4 consecutive pay stubs. C. Employer verification form
Q4. I am on a temporary leave with my employer and receiving workers compensation. What proof do I need to provide?
A. Employer letter on company letter head with date leave began, must include details about compensation. B. 2-4 consecutive pay stubs C. Proof of workers comp. D. Employer verification form
Q5. I am still employed with the same employer but have not received hours or pay while waiting for reassignment? What proof do I need to provide? A . Employer letter on company letter head with date the assignment ended. Must include status of reassignment. B. 2-4 consecutive paystubs Q6. I am currently receiving contributions and the amount I receive has changed? What proof do I need to provide?
A. Contribution form B. If the person providing contributions has changed, provide a letter from old provider.
Q7. I am not the head of household and have a change in student status. What proof do I need to provide?
A. School Verification form (college or technical) B. Financial aid award letter C. School scheduled showing full time status
Q8. I have a decrease of TANF, Social Security or Social Security Disability. What proof do I need to provide?
A. Please provide all pages of the award letter.
Q9. I have a decrease in Child Support and missed 4 consecutive payments. What proof do I need to provide?
A. Child support payments history letter from the office that handles the case B. Child support Case# and CIN# if filed in Texas. For cases filed outside of Texas we need a payment status letter from the office
that handles your case.
Interim Forms FAQ, cont’d Q10. Why is it important to sign the 9886 HUD Authorization to Release?
A. This forms allows HUD and the Houston Housing Authority to request income information from various agencies to determine
your eligibility. All household members age 18 and older must sign.
Q11. Should the Child Care Provider form be completed by the HCVP Participant or the Child Care provider?
A. The HCVP participant should fill out the first page and sign and the child care provider must complete the second page.
B. This form must be submitted with the change of income packet.
Q14. Why are you requesting an Employer letter on company letter head instead of using my last paystubs for my change of income?
A. There are details needed about your employment status that cannot be determined by your pay stub such as your start date, last day of employment, rate of pay and hours. Some company stubs are not detailed enough and do not even show the name of the company a person works for or company address.
B. The inconsistency of information on your paystub would require HHA to send a employer verification. Some employers respond to our verifications in a timely manner and some do not. We ask you to provide the letter to prevent delay in processing your request.
Q15. What happens if I am unable to provide all of the documents of proof needed to support my request for change of income?
A. If all information is not provided at the time of the request, your request will not be accepted. It is your responsibility to provide the required documents in order to process your request in a timely manner.
Q12. When Should a Zero income Checklist form be provided?
A. Anytime there is a change of income that would result in no income for the participating family.
Example: No Employment, No Unemployment, No Contributions, No TANF, No Social Security or Disability, No Child Support.
The head of household must complete the Zero Income checklist and provide copies of bills and receipts for the past 2
months.
Q13. I am waiting for the change to process and I am unable to pay my portion of the rent. What can I do?
A. During the wait period HCVP participant is still responsible for their portion of the rent? If unable to pay please contact your community resources such as 211 United Way Helpline, Harris County Social Services, Gulf Coast Community Services, American Red Cross, Salvation Army.
Q16. I have submitted my request with all documents of proof required. How long will it take to process?
A. Your request for change will be processed within 60-90 business days. There is no need to contact us during this time. If the assigned specialist needs any addition documents you will be notified by final notice. You can request the status by e-mail only at [email protected] after 30 days from the time the request was submitted.
B. Confidentiality is important and for protection of your personal information we cannot provide the status of your change of
income request to your Landlord or Property Manager. However we can provide them with the change of income process, timeframe to complete, and what to accept once it is complete. You can show your Landlord a copy of your receipt as proof your request for a change was submitted.
Q17. How will I know the change of income request is complete?
A. If approved you and your landlord will receive a Rent Change Letter by mail. If Denied you will receive a denial letter by mail.