research article quality improvement …downloads.hindawi.com/journals/bmri/2016/5625364.pdfresearch...
TRANSCRIPT

Research ArticleQuality Improvement Interventions for Early HIV InfantDiagnosis in Northeastern Uganda
Jonathan Izudi,1 Agnes Akot,2 Grace Paul Kisitu,3
Pauline Amuge,3 and Adeodata Kekitiinwa3
1Baylor College of Medicine Children’s Foundation-Uganda, Mulago Regional Referral Hospital, Block-Clock Tower,P.O. Box 72052, Karamoja Region, Kampala, Uganda2Kaabong District Local Government, Kaabong District Hospital, ANC Clinic, Kaabong, Uganda3Baylor College of Medicine Children’s Foundation-Uganda, Clinical Center of Excellence, Mulago Regional Referral Hospital,Block-Clock Tower, P.O. Box 72052, Kampala, Uganda
Correspondence should be addressed to Jonathan Izudi; [email protected]
Received 9 September 2016; Revised 22 November 2016; Accepted 5 December 2016
Academic Editor: Lucia Lopalco
Copyright © 2016 Jonathan Izudi et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction. Early infant diagnosis (EID) of human immunodeficiency virus (HIV) ensures prompt treatment and infant survival.In Kaabong Hospital, 20% of HIV exposed infants (HEIs) had access to HIV diagnosis by eight weeks. We aimed to improve EIDof HIV by deoxyribonucleic acid-polymerase chain reaction (DNA-PCR) testing by eight weeks from 20 to 100% between June2014 and November 2015.Method. In this quality improvement (QI) project, EID data was reviewed, gaps prioritized using themematrix selection, root causes analyzed using fishbone tool, and improvement changes were selected using counter measures matrixbut implemented using Plan-Do-Study-Act cycle. Root causes of low first DNA-PCR testing included maternal EID ignorance,absent lost mother-baby pairs (LMBP) tracking system, and no EID performance reviews. Health education, Continuous MedicalEducation (CMEs), and integration of laboratory and EID services were initial improvement changes used. Results. DNA-PCRtesting increased from 20 to 100% between June 2014 and July 2015 and was sustained at 100% until February 2016. Two declines,67% in September 2014 and 75% in June 2015, due to LMBP were addressed using expert clients and peer mothers, respectively.Conclusion. Formation ofWIT, laboratory service integration atMBCP, and task shifting alongEID cascade improvedEIDoutcomesat 6 weeks.
1. The Problem
Globally, human immunodeficiency virus (HIV) exposedinfants (HEIs) have delayed access to early infant diagnosis ofHIV (EID) [1]. Although new HIV infections have reduced[2], efforts towards “zero-new infections” and having 80%HIV-infected infants started on antiretroviral therapy (ART)may be reversed if EID is delayed [3]. According to theWorldHealth Organization (WHO), three in every four HEIs havedelayed access to EID services leading to high HIV-relatedchildhood deaths in Sub-Saharan Africa despite the availabil-ity of antiretroviral therapy (ART).
EID is hence a critical facilitator of early access to ART.In doing so, it ensures optimal viral suppression, reducedincidences of opportunistic infections, and improved quality
of life of HIV-positive children [4]. Conversely, EID alsohas critical implications for infant survival. Previous studiessuggested a 76% reduced risk of infant mortality within thefirst 3 months of life [5, 6] and 75% reduced HIV progressionto Acquired Immunodeficiency Syndrome (AIDS) [6] withearly ART initiation. Given the aggressive course of pediatricHIV with an estimated 20% infant mortality before sixmonths [7] and 35–40% mortality before 12 months of age[7, 8], the role of EID in early ART initiation cannot be under-estimated [8].
Uganda adopted Option-B plus that mandates initiationof ART in HIV-positive pregnant and lactating mothersirrespective of WHO clinical staging and immune status inorder to eliminate mother to child transmission of HIV (e-MTCT).
Hindawi Publishing CorporationBioMed Research InternationalVolume 2016, Article ID 5625364, 8 pageshttp://dx.doi.org/10.1155/2016/5625364

2 BioMed Research International
This is implemented through a provider initiated testingand counseling (PITCT). In PITCT, all pregnant mothers aretested for HIV during antenatal care (ANC) visits, labor, anddelivery and postpartummothers are tested during postnatal-care visits. Consequently, those found HIV-positive arestarted on ART and cotrimoxazole prophylaxis [2].
After delivery, HEIs are started on daily Nevirapine syrupadjusted according to weight and age bands until six weeks ofage. At six weeks of age, daily Nevirapine syrup is stoppedand daily cotrimoxazole syrup is started but adjusted overtime according to weight/age bands until 18 months of age.In terms of breast feeding, HEIs are exclusively breastfedduring the first six months of life; complementary feedingcommences thereafter and breastfeeding ceases at 1 year [1, 2].
From birth to 18 months, HEIs undergo routine testingfor HIV.The first test is by deoxyribonucleic acid-polymerasechain reaction (DNA-PCR) at six weeks of age, then a secondDNA-PCR test is at six weeks after cessation of breastfeeding,and a final rapid HIV antibody test is at 18 months of age[9]. Should a HEI turn positive during these three HIVtesting times, ART is initiated and subsequent monitoringcontinued concurrently with cotrimoxazole prophylaxis. Forthe HIV-positive pregnant or lactating mother, ART and cot-rimoxazole are continued for life while monitoring virologicsuppression. Despite these recommendations, EID by DNA-PCR tests among HEIs within two months of birth (firstDNA-PCR) in Uganda remains low at 40.2% [10].
This has led to late ART initiation and unfavorable pedi-atric HIV outcomes [4]. Second, loss to follow-up of HIV-positive mothers and HEIs continues to retard EID services.According to Uganda National Pediatric HIV Support data,70% of HEIs are either lost to follow-up or have no finalHIV antibody test at 18 months [11]. To resolve these poorEID outcomes, Uganda introduced the concept of Mother-Baby Care Point (MBCP), a service delivery model withinthe maternal child health clinic where HIV-positive mothersand HEIs are paired, cared for together, and retained until 18months postpartum or beyond [11].
In KaabongHospital, substantial proportion ofHEIs havedelayed access to EID by first DNA-PCR test. In June 2014,EID data analysis indicated only one in every five (20.0%)HEIs had access to EID by first DNA-PCR test.The precedingmonths (March–May 2014) equally had low proportion ofHEIs tested by DNA-PCR at 6 weeks. Maternal and healthservices related factors contributed to this low first DNA-PCR testing. In Uganda, all HEIs are expected to have theirfirst DNA-PCR test between 6 and 8 weeks of age. Our aimwas therefore to increase first DNA-PCR testing from 20 to100% between June 2014 and November 2015 using qualityimprovement (QI) interventions.
2. Background
Quality of healthcare gained huge recognition in Ugandalately [12, 13]. Quality improvement (QI) defined as clos-ing gaps between current and expected performance usingappropriate measures as defined by standards is relatively anew concept in Uganda.
Uganda launched the first QI strategic framework in 2010.This was followed by establishment of QI committees atvarious levels of healthcare (national, regional, district, healthsubdistrict, hospitals and its departments, and health centers)[13]. The goal was to provide high quality health services andcontribute to attainment of good quality of life andwell-beingat all levels of healthcare [12, 14].
Quality of healthcare is an important mediator betweenthe sixWHObuilding blocks of health systems strengthening(service delivery, health work force, health information,health financing, leadership and medical products, vaccines,and technologies) and health outcomes (effectiveness, effi-ciency, responsiveness, and social and financial risk protec-tion) [13].
This QI project was conducted at Kaabong General Hos-pital in Karamoja region, Northeastern Uganda. Karamojaregion (a rural and remote setting) has poor transportnetwork and frequent intraclan and cross-border armed raidsamong others.The region has limited access to health servicesand health information and suffers from inadequate humanresources for health (below average staffing levels and highturnover) to handle the increasing burden of HIV/AIDS. Inthe past, Karamoja region was known for its conservativecultural practices and isolation from the rest of Uganda (dualfactors that accounted for low HIV prevalence). However,in recent years, HIV prevalence increased from 3.5% in2005 to 5.3% in 2011 due to improved security allowing freemovement of people and urbanization [15].
The region has poor EID quality of care indicators. ByMarch 2016, merely 61% (126/206) of HEIs received an HIVtest by 6–8 weeks. Similarly, 49% (100/206) were startedon cotrimoxazole prophylaxis within 2 months of birth.However, there was marked progress in reducing the regionalHIV positivity rate among HEIs from 17% in 2012 to 2% byJune 2016. In contrast, 7.4% of women in Karamoja regionuse modern family planning (FP) methods and 20.5% haveunmet FP need [16].
Kaabong district is one of the seven districts of Karamojaregion and it is among the 15 bottom performing districtsin Uganda. It was ranked 105th out of 112 districts in healthperformance indicators [14]. Kaabong Hospital located inKaabong district is owned by the Republic of Uganda and liesapproximately 709 kilometers in the Northeast of Kampala,the Capital City of Uganda. It serves 27 lower health facilitiesof which one is level four, five are level three, and 21 arelevel two health centers. In addition, it is a referral center forpatients from the bordering districts (Kitgum and Kotido)and countries (Southern Sudan and Kenya) [17].The hospitalprovides generalmedical, surgical, pediatric, obstetric, ortho-pedic, nursing, HIV/ART, e-MTCT, EID, TB, ophthalmic,and dental services [17].
3. Baseline Measurement
In June 2014, the MBCP Work Improvement Team (WIT),a departmental QI team at the ANC unit of KaabongHospital, abstracted EIDdata for the periodMarch–June 2014using standardized Ministry of Health (MoH)-Uganda dataabstraction form.

BioMed Research International 3
Table 1: Theme matrix selection for prioritization of EID quality of care gaps.
Themes CustomersImpact oncustomerscore (𝐴)
Need toimprovescore (𝐵)
Overall score(A × B)
Remark onselection
20% first DNA-PCRtesting
HEIs andcaregivers 4 5 20 Selected
55% secondDNA-PCR testing
HEIs andcaregivers 2 5 10 Not selected
75% HIV antibodytesting at 18 months
HEIs andcaregivers 5 3 15 Not selected
60% EID result givento caregivers
HEIs andcaregivers 3 3 9 Not selected
The EID data was then summarized into frequencies andpercentages to intentionally identify quality of care gaps.
Of data abstracted from all eligible HEIs, major EIDgaps identified were as follows: only five out of 25 (20.0%)had first DNA-PCR tests at 6 weeks, two out of three(66.7.0%) had second DNA-PCR test 6 weeks after cessationof breastfeeding, five out of seven (71.4%) had HIV antibodytest at 18 months, and six out of ten (60.0%) EID results weregiven to caregivers/mothers.TheMBCPWIT discussed theseperformance indicators and prioritized them for improve-ment using the theme matrix selection. In the theme matrixselection, performance indicators were prioritized based onthe potential negative impacts on HEIs and HIV-positivelactating mother and the urgency of the need to tackle. Aranking score of 1–5 for both the potential negative impactand urgency to tackle was used. Highest score was assignedto a performance indicator that had high negative impactand high need to solve. The overall score was the productof the rank-scores of the two measures in the theme matrixselection (Table 1). The first DNA-PCR testing scored 20,second DNA-PCR testing scored 10, HIV-serological testingat 18 months scored 15, and EID result given to caregivers ormothers scored nine. So, improving first DNA-PCR testingwas prioritized for QI (Table 1).
4. Design
First, Baylor College of Medicine Children’s Foundation-Uganda (Baylor-Uganda) conducted a two-day QI men-torship at Kaabong general hospital during which selectedhealthcare workers from all departments were orientedon Uganda National QI Framework 2010/2011–2014/2015through 1-hour Continuous Medical Education (CME) onbasic QI concepts (introduction to QI, dimensions of quality,quality grid, steps in QI, principles of QI, data use in QI, QItools for problem identification, and analysis among others).After the CME, a Hospital QI team consisting of multidis-ciplinary team members, clinical, nursing, laboratory, andenvironmental health professionals and two community rep-resentatives, was formed. At each department (Tuberculosis,ART, MBCP, laboratory, and ART), WITs were formed toaddress quality of health care performance gaps.
5. Strategy
The MBCP WIT started a QI project using four principlesof QI: identification of EID quality of care gap (problemidentification), analysis of the root causes of the EID gap,development of evidence based improvement changes (solu-tions), and the testing and implementation of developedsolutions using the Plan-Do-Study-Act (PDSA) cycle [18].
5.1. Analysis of EID Quality of Care Gaps. The fishbone tool[19] was used to analyze potential root causes of low firstDNA-PCR testing. During this analytical process, the Why-Why-Why approach for each identified root cause of lowfirst DNA-PCR testing was used to systematically identifyunderlying causes until no further causes were identified [19].
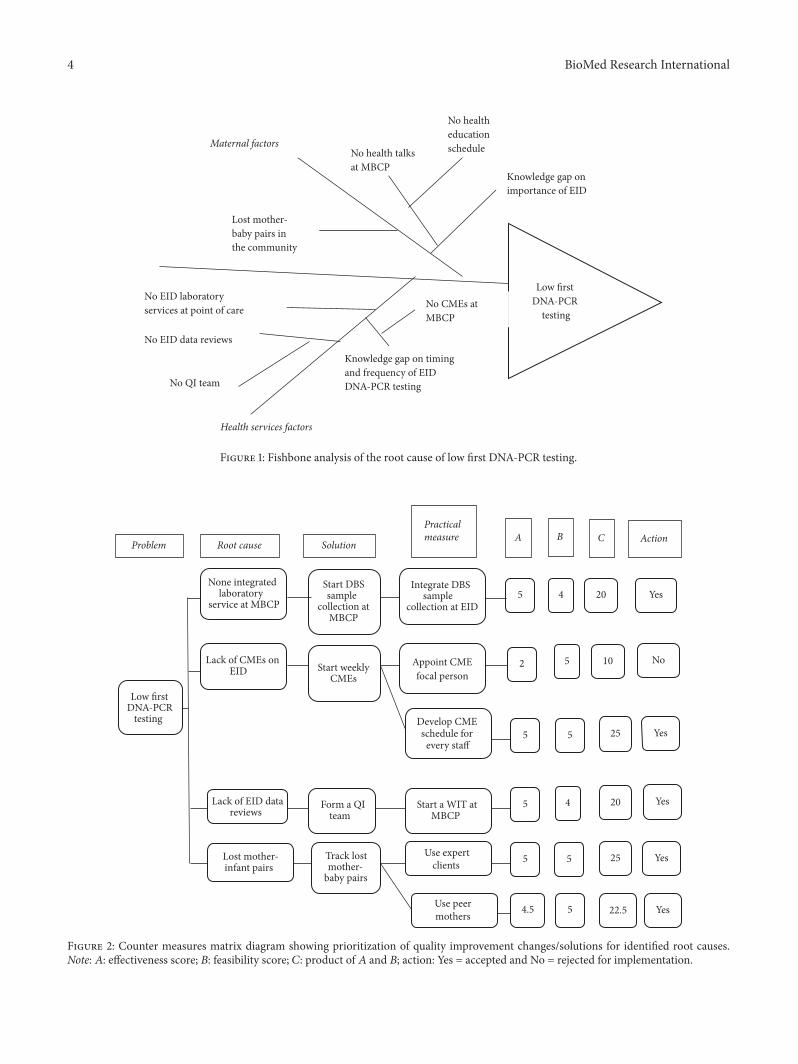
The root cause were summarized and categorized asmaternal and health services factors. The maternal factorsincluded lack of knowledge on EID importance and lostmother-infant pairs in the community. Conversely, healthservices related factors encompassed nonintegrated labora-tory services for dry blood spot (DBS) sample collection attheMBCP, health provider knowledge gap on the timing, andfrequency of DNA-PCR tests due to lack of CMEs and lack ofroutine EID data reviews due to absence of WIT (Figure 1).
5.2. Development of Improvement Changes and Prioritization.The WIT developed QI solutions (improvement changes)according to identified root causes. They used the countermeasures matrix to prioritize improvement changes based onfeasibility and effectiveness ranking scores of 1–5 (Figure 2).Highest score was assigned to an improvement change thatwas highly feasible and highly effective. Using this approach,priority was given to an improvement changewith the highestoverall score obtained by the product of feasibility andeffectiveness scores [20]. Consequently, conduct ofCMEs andintegration of laboratory services for DBS sample collectionat the MBCP and health education talks at the MBCPwere initially prioritized. Afterwards, expert clients and peermothers were introduced to address gaps in lost mother-babypairs.
5.3. Implementation of Improvement Changes. We used thePlan-Do-Study-Act (PDSA) cycle to implement the QI
4 BioMed Research International
Maternal factors
Low first DNA-PCR
testing
No health education scheduleNo health talks
at MBCPKnowledge gap on importance of EID
Lost mother-baby pairs in the community
No EID laboratory services at point of care
No EID data reviews
Knowledge gap on timing and frequency of EID DNA-PCR testing
No CMEs at MBCP
Health services factors
No QI team
Figure 1: Fishbone analysis of the root cause of low first DNA-PCR testing.
Low first DNA-PCR
testing
None integrated laboratory
service at MBCP
Lack of CMEs on EID
Lack of EID datareviews
Lost mother-infant pairs
Start DBS sample
collection at MBCP
Start weekly CMEs
Integrate DBS sample
collection at EID
Appoint CME focal person
Develop CME schedule for
every staff
5 4 20 Yes
2 5 10 No
5 5 25 Yes
Form a QI team
Track lost mother-
baby pairs
Start a WIT at MBCP
5 4 20 Yes
Use expert clients
Use peer mothers
5 5 25 Yes
4.5 5 22.5 Yes
Problem Root cause Solution
Practical measure A B C Action
Figure 2: Counter measures matrix diagram showing prioritization of quality improvement changes/solutions for identified root causes.Note: 𝐴: effectiveness score; 𝐵: feasibility score; 𝐶: product of 𝐴 and 𝐵; action: Yes = accepted and No = rejected for implementation.

BioMed Research International 5
Mar
-14
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4D
ec-1
4Ja
n-15
Feb-
15M
ar-1
5Ap
r-15
May
-15
Jun-
15Ju
l-15
Aug-
15Se
p-15
Oct
-15
Nov
-15
Dec
-15
Jan-
16Fe
b-16
Perc
enta
ge o
f firs
t D
NA-
PCR
tests
(%)
CME, EID integration
& health talk
Use of expert clients
Use of peer mothers
Lost mother-baby pairs
0102030405060708090
100
Figure 3: Trend of first (6–8 weeks) DNA-PCR testing among HIV exposed infants at Kaabong Hospital.
project [21]. The PDSA Cycle ensured a step-by-step imple-mentation, monitoring and evaluation, and formulation ofnew QI changes or modification of current changes [22].During implementation, a QI change that never yielded anincrease in the performance indicator was dropped and newchange(s) developed or existing ones were modified.
5.4. Documentation of QI Process. A QI journal consisting ofstart and end dates of the QI project, improvement objective,indicator, problem statement, QI solutions (changes), a linegraph with annotations, and f lessons learnt was used todocument theQI process.The set QI objective was to increasethe testing of HEIs at six weeks of age by DNA-PCR fromtwenty percent to hundred percent between June 2014 andNovember 2015. The indicator was the percentage of HEIswith a DNA-PCR test within eight weeks of age. In ourindicator, the numerator was the number of HEIs between 6and 8 weeks with a documentedDNA-PCR test result and thedenominator was the number of all HEIs 6–8 weeks of age atthe MBCP, Kaabong Hospital.
On monthly basis, the MBCP QI focal person reviewedEID clinical charts, abstracted data on firstDNA-PCR testing,computed frequencies and percentages, and updated thedocumentation journal. EID performance indicators wereshared with the rest of the WIT members at monthly QImeetings.
6. Results
Of eligible HEIs for first DNA-PCR (6–8 weeks) testing,testing of HEIs improved from five out of 25 (20.0%) in June2014 to nine out of 10 (90%) in July 2014 when CMEs forhealthcare workers and health education talks to caregiverson the importance of EID and DBS sample collection wereintegrated at the MBCP. However, two declines in first DNA-PCR testing, two out of three (67.0%) in September 2014 andthree out of four (75.0%) in June 2015, were recorded.
The initial decline in September 2014 was due to loss ofmother-baby pairs in the community and this was addressedby use of expert clients to track lost mother-infant babypairs in the community. The second decline in June 2015was due to repeat loss of mother-baby pairs in the com-munity as well and was tackled by use of peer mothersto track lost mother-infant baby pairs in the communities
(Figure 3). Other than these declines, the overall first DNA-PCR testing was sustained at 100% between June 2014 andJanuary 2016 (Supplementary Material S1 available online athttp://dx.doi.org/10.1155/2016/5625364).
7. Lessons Learnt
This QI project improved EID by first DNA-PCR testing atKaabong Hospital. The introduction of CMEs, point of careDBS sample collection through integration of EID laboratoryservices at the MBCP, patient health education, and use ofexpert clients and peer mothers led to significant improve-ments in firstDNA-PCR testing.The integration of laboratoryservices at the MBCP increased first DNA-PCR testing.Earlier, WHO advised health facilities to conduct onsite DBSsample collection for DNA-PCR testing in order to scale upaccess and coverage of PMTCT and follow-up services [23].
Our EID results obtained by point of care DBS samplecollection was similar to those obtained by conventionalmethods. In Tanzania, similar results were reported [24]. InKwazulu-Natal, South Africa, the integration of EID servicesat an immunization clinic was highly accepted by caregiversand led to increased access to EID services by HEIs at sixweeks of age [25]. Similarly, in this QI project, caregiversembraced the approach and reported it to be time saving andconvenient.
So onsite mentorship is essential in improving coverageand quality of EID services. In agreement with past resultsfrom Botswana, training of healthcare workers on EID DBSsample collection improved EID quality of care indicators[26].
To us, health facility based CMEs and patient healtheducation were critical interventions. CMEs kept healthworkers up-to-date with EID clinical knowledge. Provisionof adequate health education and counseling to caregivers onimportance of EID improved self-efficacy in health matters.Health facilities providing EID services must enforce CMEsto enhance healthcare worker knowledge and improve EIDquality of care. We suggest the inclusion of CME attendancesas a performance appraisal indicator to improve compliance.
Identification ofHEIs remains the first critical step in pro-viding EID services and linkage to care [27]. InMozambique,75% of HIV-infected women never returned HEIs for EIDservices [8]. One of the biggest challenges to EID success in

6 BioMed Research International
our setting was the high loss to follow-up. We tackled thischallenge by use of expert clients and peer mothers. In thepast, Uganda introduced expert clients for scaling up ARTaccess, particularly, to ensure greater involvement of personswith HIV and to address human resource crisis [28]. In ourintervention, an expert client was an HIV-positive adult withdemonstrated substantial compliance to medical advice andimproved clinical, physical, and immunological response toART. He or she was willing to engage in supporting theEID program and community members for improved servicedelivery and is viewed as a role model by other HIV-positivepersons.
Expert clients are therefore HIV-positive persons viewedby people living with HIV as motivating, influential, accept-able, appropriate, trustworthy, respectable, and morallyupright to handle health matters. They voluntarily and rou-tinely participate in health facility activities such as triaging,patient recording, health education, and counseling of diffi-cult clients among others. In this intervention, expert clientsused lostmother-baby pair sociodemographic details (village,parish, and subcounty) provided by theMBCP Focal Personsto confidentially track the pairs in the community. Uponidentification, the mothers were counseled on importance ofDNA-PCR tests by expert clients while in the community andphysically linked to the MBCP for DNA-PCR testing.
To our surprise, the use of expert clients to track lostmother-infant pairs from the communities and their linkageto the MBCP resulted in substantial increase in DNA-PCR testing because they were accessible, appropriate, andacceptable by HIV-positive mothers.
Also, Uganda introduced the concept of Family SupportGroups (FSGs) as a pathway to extend HIV care, treatment,and support to familymembers ofHIV-positive pregnant andlactatingmothers. FSGs consist ofHIV-positive pregnant andlactating mothers, HIV-positive children under five years,spouses to HIV-positive pregnant or lactating mothers, preg-nant and lactating mothers in serodiscordant relationships,and caregivers of under 5-year-old HIV-positive children.FSGs are vital in reducing stigma at community level, offeringpeer support, improving group confidence, and fightingexternal stigma [29]. Because they are embedded in the com-munities, they play a great role in community engagementsand this forms a critical catalyst in elimination of mother tochild transmission (e-MTCT) of HIV success. Peer supportpractices improve demand for e-MTCT services, generatelocal solutions, and drive community sociobehavioral change[30].
In our setting, peer mothers were groups of womencreated from HIV-positive mothers within FSGs but witha HIV-negative child. This proves their compliance to e-MTCT services and ability to be change agents. It is thereforenot surprising that the use of peer mothers equally led toimproved firstDNA-PCR testing. Peermotherswere reportedto be friendly, approachable, and open minded with clearEIDmessages compared to health workers and expert clients.To us, these acceptability differences are attributable to pastexperiences of peer mothers in the context of e-MTCT.Peer mothers experienced similar circumstances currentlyconfronting HIV-positive lactating mothers in caring for
HEIs compared to expert clients. They are therefore morelikely to package clearer and specific HIV messages thanexpert clients and healthcare workers.
8. Conclusion
The integration of EID laboratory services at MBCP, patienthealth education on importance of EID, regular EID CMEsfor health workers, and use of community structures (expertclients and peer mothers) significantly improved EID out-comes and quality.
9. Recommendation
We recommendDBS sample collection in EID clinics, regularEID CMEs to health workers, and health education talksto HIV-positive lactating mothers in improving EID qual-ity of care indictors. In addition, expert clients and peermothers are very useful in improving EID coverage andoutcomes. However, we noted that most health facilities inKaramoja region neglect EID. Our experience calls for activeimplementation of QI and adoption of these QI changesby both the public and the private healthcare settings tobetter EID quality of care. We strongly advice adherence toroutine EID data reviews, analysis of EID quality of care gaps,generation of evidence based solutions, andmultidisciplinaryteam composition for success.
Overall, to improve quality of health care, strongermeasures in supportive supervision by multidisciplinaryteams, staff motivation, continuous learning, adherence toprofessional code of conduct, improved logistical support toensure adequate supplies of drugs/diagnostics, and timelypayment of staff stipends when indicated are very central.
10. Limitations
Our QI initiative was the first systematically conducted andrigorous project in Karamoja region, Northeast Uganda. Weexperienced major challenges in missing EID data. In addi-tion, the lack of qualitative information from HIV-positivelactating mothers to explain dynamics and lived experiencesin EID service utilization may be limiting. Secondly, the lownumbers of HEIs resulted in large variations in percentages.However, these are the total numbers of all eligible HEIs forDNA-PCR test at 6 weeks.
It was not possible to have numbers larger than thoseobserved. In our setting, there are fewer HEIs because of lowHIV prevalence in general. Also, stigma and discriminationof HIV-positive persons hinder access to and continuationwith HIV care among HIV-positive mothers. The combina-tion of these factors accounts for the low numbers of HEIs incare.
Despite these limitations, this QI project proved thatsimple, cost-effective, and evidence-oriented approaches canclose gaps between current and expected performances asdefined by standards.

BioMed Research International 7
Abbreviations
AIDS: Acquired Immunodeficiency SyndromeART: Antiretroviral therapyCME: Continuous Medical EducationDNA: Deoxyribonucleic acidEID: Early infant diagnosisE-MTCT: Elimination of mother to child
transmission of HIVFSGs: Family Support GroupsHAART: Highly active antiretroviral therapyHEI: HIV exposed infantsHIV: Human immunodeficiency virusMBCP: Mother-baby care pointPCR: Polymerase chain reactionPMTCT: Prevention of mother to child
transmission of HIVPOC: Point of careQI: Quality improvementWHO: World Health OrganizationWIT: Work improvement team.
Consent
All participants enrolled in HIV care at Kaabong Hospitalgave written informed consent prior to enrollment in HIVcare.
Competing Interests
The authors declare no competing interests.
Authors’ Contributions
Jonathan Izudi and Agnes Akot initiated, monitored, andevaluated theQI project. Jonathan Izudi, Agnes Akot, PaulineAmuge, Grace Paul Kisitu, and Agnes Akot equally con-tributed in writing this manuscript. Jonathan Izudi is firstauthor and Agnes Akot, Pauline Amuge, Grace Paul Kisitu,Grace Paul Kisitu, and Adeodata Kekitiinwa are co-authors.
Acknowledgments
The authors recognize the great quality improvement lead-erships of Dr. Andrew Katawera and Dr. Calvin Epidu, theregional laboratory qualitymanagement support by SolomonOkot Paul, and countless support from Kaabong DistrictHealth Office by Dr. Nalibe Shalif.
References
[1] E. T. Katabira, M. R. Kamya, I. Kalyesubula, and A. Namale,National Antiretroviral Treatment Guidelines for Adults, Ado-lescents, and Children, Ministry of Health, Kampala, Uganda,2009.
[2] E. T. Katabira, Ed., The Integrated National Guidelines forAntiretroviral Therapy, Prevention of Mother to Child Transmis-sion of HIV and Infant & Young Child Feeding, Ministry ofHealth-Uganda, Kampala, Uganda, 1st edition, 2011.
[3] Joint United Nations Program on HIV/AIDS (UNAIDS), 90-90-90 An Ambitious Treatment Target to Help End the AIDSEpidemic, WHO & UNAIDS, Geneva, Switzerland, 2014.
[4] A. S. Hassan, E.M. Sakwa, H.M.Nabwera et al., “Dynamics andconstraints of early infant diagnosis of HIV infection in ruralKenya,” AIDS and Behavior, vol. 16, no. 1, pp. 5–12, 2012.
[5] C. Motswere-Chirwa, A. Voetsch, L. Lu et al., “Follow-up ofinfants diagnosed with HIV-early infant diagnosis program,Francistown, Botswana, 2005–2012,” Morbidity and MortalityWeekly Report, vol. 63, no. 7, pp. 158–160, 2014.
[6] A. Violari, M. F. Cotton, D. M. Gibb et al., “Early antiretroviraltherapy and mortality among HIV-infected infants,” The NewEngland Journal of Medicine, vol. 359, no. 21, pp. 2233–2244,2008.
[7] A. H. Mirkuzie, S. Hinderaker, M. Sisay, K. Moland, and O.Mørkve, “Current status of medication adherence and infantfollowup in the prevention ofmother to childHIV transmissionprogramme in Addis Ababa: a cohort study,” Journal of theInternational AIDS Society, vol. 14, no. 1, article 50, 2011.
[8] R. E. Cook, P. J. Ciampa,M. Sidat et al., “Predictors of successfulearly infant diagnosis of HIV in a rural district hospital inZambezia, Mozambique,” Journal of Acquired Immune Defi-ciency Syndromes, vol. 56, no. 4, pp. e104–e109, 2011.
[9] Ministry of Health-Uganda, “The 2014 integrated guidelines forHIV/AIDS management,” in Kampala AIDS Control Program,pp. 45–47, 2014.
[10] Ministry of Health-Uganda, Uganda HIV/AIDS Country Pro-gress Report, Ministry of Health, Kampala, Uganda, 2014.
[11] AIDS Treatment and Information Center, Infectious DiseasesInstitute, and Makerere University, “AIDS Treatment Informa-tion Center newsletter,” in Quarterly Newsletter of the AIDSTreatment Information Center, Infectious Diseases Institute,Makerere University, vol. 11, 1, 3, 5, AIDS Treatment Informa-tion Center, Infectious Diseases Institute, Makerere University,Kampala, Uganda, 2014.
[12] The Republic of Uganda, The Quality Improvement Methods:A Mannual for Health Workers in Uganda, The Republic ofUganda, Kampala, Uganda, 2015.
[13] The Republic of Uganda, Health Sector Quality ImprovementFramework and Strategic Plan 2010/2011–2014/2015, vol. 9, TheRepublic of Uganda, Kampala, Uganda, 2011.
[14] The Republic of Uganda, Annual Health Sector PerformanceReport for Financial Year 2014/2015,Ministry ofHealth-Uganda,Kampala, Uganda, 2015.
[15] Uganda AIDS Commission, National HIV Prevention Strategy2011–2015: Expanding and Doing HIV Prevention Better, AIDSCommission, Kampala, Uganda, 2011.
[16] Republic of Uganda, The State of Uganda Population Report2014: Harnessing Uganda’s Demographic Dividend for Socioeco-nomic Transformation, Republic of Uganda, Kampala, Uganda,2014.
[17] Kaabong general hospital profile, http://www.sustainuganda.org/content/kaabong-general-hospital-profile.
[18] Ministry of Health Uganda, A Competence Based TrainingManual for Health Workers in the Management of Tuberculosisin Children, National TB Leprosy Program, Kampala, Uganda,2015.
[19] Fish bone template diagram in excel, https://www.qimacros.com/fishbone-diagram-template/.
[20] Counter Measures Matrix, https://www.qimacros.com/quality-tools/solution/.

8 BioMed Research International
[21] P. Walley and B. Gowland, “Completing the circle: from PD toPDSA,” International Journal of Health Care Quality Assurance,vol. 17, no. 6, pp. 349–358, 2004.
[22] Minnesota Department of Health, PDSA: Plan-Do-Study-Act,2014.
[23] World Health Organization, WHO Recommendations on theDiagnosis of HIV Infection in Infants and Children, 2010.
[24] S. M. Lofgren, A. B. Morrissey, C. C. Chevallier et al., “Eval-uation of a dried blood spot HIV-1 RNA program for earlyinfant diagnosis and viral load monitoring at rural and remotehealthcare facilities,” AIDS, vol. 23, no. 18, pp. 2459–2466, 2009.
[25] N. Rollins, S. Mzolo, T. Moodley, T. Esterhuizen, and H. vanRooyen, “Universal HIV testing of infants at immunizationclinics: an acceptable and feasible approach for early infant diag-nosis in high HIV prevalence settings,”AIDS, vol. 23, no. 14, pp.1851–1857, 2009.
[26] T. Creek, A. Tanuri, M. Smith et al., “Early diagnosis of humanimmunodeficiency virus in infants using polymerase chainreaction on dried blood spots in Botswana’s national programfor prevention of mother-to-child transmission,” The PediatricInfectious Disease Journal, vol. 27, no. 1, pp. 22–26, 2008.
[27] S. A.Woldesenbet, D. Jackson, A. E. Goga et al., “Missed oppor-tunities for early infant HIV diagnosis: results of a nationalstudy in South Africa,” Journal of Acquired Immune DeficiencySyndromes, vol. 68, no. 3, pp. e26–e32, 2015.
[28] P. Brown-Peterside, C. A. Redding, L. Ren, and B. A. Koblin,“Acceptability of a stage-matched expert system interventionto increase condom use among women at high risk of HIVinfection in New York City,” AIDS Education and Prevention,vol. 12, no. 2, pp. 171–181, 2000.
[29] G.Mburu,M.Ram,M. Skovdal et al., “Resisting and challengingstigma in Uganda: the role of support groups of people livingwith HIV,” Journal of the International AIDS Society, vol. 16, no.3, Article ID 18636, 2013.
[30] L. A. Gulaid and K. Kiragu, “Lessons learnt from promisingpractices in community engagement for the elimination of newHIV infections in children by 2015 and keeping their mothersalive: summary of a desk review,” Journal of the InternationalAIDS Society, vol. 15, supplement 2, Article ID 17390, 2012.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com