respiratory examination slides of dr jm nel department critical care dr scarpa schoeman – dept...
TRANSCRIPT

Respiratory Examination
Slides of Dr JM NelDepartment Critical Care
Dr Scarpa Schoeman – Dept Internal Medicine

Respiratory Examination
1. Positioning of the patient
2. General Appearance
3. The hands
4. The face
5. The trachea
6. The chest
7. The heart
8. The abdomen
9. Other

Positioning of the patient
Undress to waist
Sitting position
Acutely ill– Lying down
General appearance
1. Dyspnoea– Signs of dyspnoea at rest– RR: 16- 25/min
2. Cyanosis– Central cyanosis: tongue
3. Cough character

General appearance
4. Sputum– Colour/volume/type– Hemoptysis
5. Stridor– Loudest on inspiration
6. Hoarseness
The hands
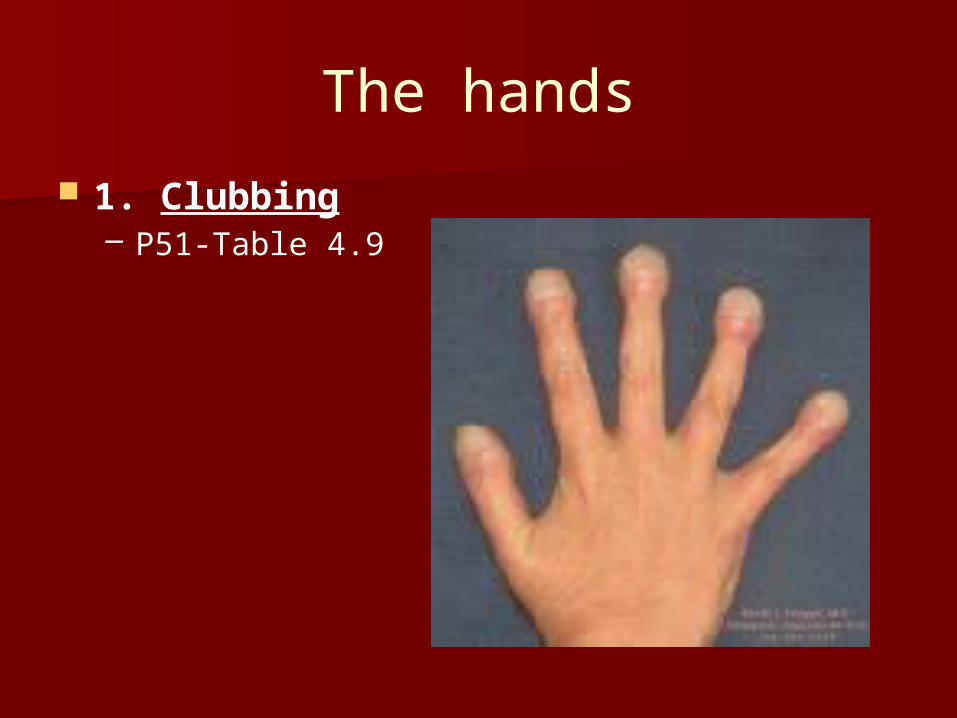
1. Clubbing– P51-Table 4.9

The hands Clubbing
– Cardiovascular Congenital cyanotic heart disease Infective endocarditis
– Respiratory (80% the cause) Lung carcinoma Chronic pulmonary suppuration Idiopathic lung fibrosis Cystic fibrosis Asbestosis Pleural mesothelioma
– Gastrointestinal Cirrhosis Inflammatory bowel disease Coeliac disease
COPD/TB does not give clubbing

The hands
HPO
Periosteal inflammation Clubbing marked Distal end of long
bones,wrists,metacarpal,metatarsal bones, knees, ankles
Swelling/Tenderness

The hands
2. Staining– Cigarette smoking
3. Wasting and weakness
– Wasting small muscles– Weakness abduction– Infiltration of brachial plexus by lung CA

The hands
4. Pulse rate
– Pulse rate– Pulsus paradoxus
Systolic BP drop > 10mmHg
5. Flapping tremor(Asterixis)
– Dorsiflex hands– CO2 retention (COPD)

The face
1. Horner’s syndrome
– Constricted pupil– Partial ptosis– Loss of sweating
– Apical lung tumour– Compression of sympathetic nerves

The face
2. Skin changes– Connective tissue diseases

The face
3. URTI– Look inside mouth
4. Sinuses– Look inside mouth
5. SVC obstruction– Facial plethora or cyanosis

The trachea
Position
Tracheal tug– COPD
The chest
Inspection
Palpation
Percussion
Auscultation

The chest: Inspection
1. Shape and symmetry of chest shape
– Barrel- shaped chest
– Pigeon chest
– Funnel chest
– Harrison’s sulcus
– Kyphosis, scoliosis, kyphoscoliosis
– Lesions of chest wall
– Movement of chest wall

The chest: Inspection
Barrel- shaped chest– Increased AP diameter– Severe asthma/COPD– Normal elderly people

The chest: Inspection
Pigeon chest(pectus carinatum)– Outward bowing sternum/costal
cartilages– Chronic childhood resp infectons– Rickets
Funnel chest(pectus excavatum)– Developmental defect– Depression lower end of sternum– Severe: decreased lung capacity

The chest: Inspection
Harrison’s sulcus
– Linear depression lower ribs just above costal margins
– Severe asthma in childhood– Rickets

The chest: Inspection
Kyphosis, scoliosis, kyphoscoliosis
– Severe: reduced lung capacity

The chest: Inspection
Lesions of chest wall– Scars
Previous surgery Previous ICD
– Radiotherapy Erythema
– Subcutaneous emphysema– Prominent veins
SVC obstruction

The chest: Inspection Movement of chest wall
– Expansion Upper lobes
– From behind– Look down at clavicles
Lower lobes– From behind– Unilateral
Localized fibrosis, consolidation, collapse, pleural effusion
– Bilateral COPD, diffuse pulmonary fibrosis

The chest: Inspection
Movement of chest wall
–Asymmetry–Paradoxical inward movement
abdomen during inspiration Diaphragm paralysis

The chest: Palpation
1. Chest expansion– Thumbs move symmetrical 5cm on
inspiration– Lower lobe
From back– Upper lobe
From front

The chest: Palpation
2. Apex beat– Displacement
Towards side of lesion– Collapse lower lobe– Localized fibrosis
Away from lesion– Pleural effusion– Tension pneumothorax
– Impalpable COPD: hyperinflation

The chest: Palpation
3. Vocal fremitus– Palm of hand– “99”– Differences– Increased: Consolidation– Same as vocal resonance
4. Ribs– Localized pain
Trauma, metastases, prolonged coughing

The chest: Percussion

The chest: Percussion
1. Symmetrical– Ant/Post/Lat– Supraclavicular fossa over lung apex– Clavicle with finger

The chest: Percussion

The chest: Percussion
2. Interpretation– Resonant
Normal
– Dull Solid structure (liver) Consolidation
– Stony dull Fluid- filled area (pleural effusion)
– Hyperresonant Over hollow structures
– Bowel, pneumothorax

The chest: Percussion
3. Liver dullness
– Upper level 5th / 6th rib MCL If lower: hyperinflation
4. Cardiac dullness
– Decreased COPD Asthma

The chest: Auscultation
1. Breath sounds
2. Vocal resonance

The chest: Auscultation
1. Breath sounds– General
– Quality of breath sounds
– Intensity of breath sounds
– Added sounds

The chest: Auscultation(Breath sounds)
General
– Diaphragm of stethoscope– Compare sides– Axilla– Bell of stethoscope above clavicles
Lung apices

The chest: Auscultation(Breath sounds)
Quality of breath sounds p125– Normal breath sounds (vesicular)
– Bronchial breath sounds
– Amphoric breath sounds

The chest: Auscultation(Breath sounds)
Normal breath sounds (vesicular)
– Most of chest– Breath through mouth– Inspiration
Longer and louder than expiration– No gap between inspiration and
expiration

The chest: Auscultation(Breath sounds)
Bronchial breathing– Hollow, blowing sound– Audible in expiration– Gap between inspiration and expiration– Expiration
Higher intensity than inspiratory– Normal posteriorly over upper chest
– CONSOLIDATION

The chest: Auscultation(Breath sounds)
Amphoric breathing– Exaggerated bronchial quality– Very hollow (blowing over bottle)
– LARGE CAVITY

The chest: Auscultation(Breath sounds)
Intensity of breath sounds– Normal or reduced
– Reduced COPD Pleural effusion Pneumothorax Pneumonia Large neoplasm Pulmonary collapse

The chest: Auscultation(Breath sounds)
Added sounds– Continuous sounds (wheezes)
– Interrupted sounds (crackles)

The chest: Auscultation(Breath sounds)
Continuous sounds (wheezes)– Musical– Inspiration +/- expiration– Airway narrowing– High pitched
Smaller bronchi Asthma
– Low pitched Larger bronchi COPD
– Monophonic Localized Bronhial obstruction (Lung CA)
– Stridor Louder over trachea Inspiratory

The chest: Auscultation(Breath sounds)
Interrupted sounds (crackles)
– Non-musical– Early inspiratory
Small airway disease COPD Medium coarseness
– Late/pan-inspiratory Disease in alveoli Fine
– Pulmonary fibrosis Medium
– LV failure
Coarse– Bronchiectasis– Retention of secretions

The chest: Auscultation(Breath sounds)
Pleural friction rub Thickened pleural surfaces rub together Grating sound Causes
– Pleurisy Secondary to pulmonary infarction
– Pneumonia– Malignant involvement of pleura– Spontaneous pneumothorax

The chest: Auscultation
2. Vocal resonance– Auscultation while patient speaks– Ability of lung to transmit sounds– Normal– Consolidation
Can hear “99” Aegophony
– Bee becomes bay Whispering pectoriloquy
– Can hear when whispers

The chest: Signs

The chest: Signs

The chest: Signs

The chest: Signs

The chest: Signs
Hyperinflation– Increased AP diameter– Trageal tug– Apex not palpable– Hyperressonant percussion– Liver displaced downwards– No cardiac dullness– Soft heart sounds

The Heart
Measure JVP– Increased in RV failure
Listen to P2– Loud in pulmonary hypertension
The Abdomen
Liver examination– Displaced downward in hyperinflation– Enlarged in metastases (Lung CA)

Other
Pemberton’s sign– Lift arms over head one minute– SVC obstruction
Facial plethora Cyanosis Inspiratory stridor Non-pulsatile elevation of JVP

Other
Feet– Oedema
Cor pulmonale
– DVT PE
