respiratory muscle activity during rapid (rem) sleep ... · ods ofhypopnoea occurduring rapid eye...
TRANSCRIPT

Thorax 1995;50:376-382
Respiratory muscle activity during rapid eye
movement (REM) sleep in patients withchronic obstructive pulmonary disease
J E S White, M J Drinnan, A J Smithson, C J Griffiths, G J Gibson
AbstractBackground - In patients with chronic ob-structive pulmonary disease (COPD) peri-ods of hypopnoea occur during rapid eyemovement (REM) sleep, but the mech-anisms involved are not clear.Methods - Ten patients with stable COPDwere studied during nocturnal sleep. De-tailed measurements were made ofsurfaceelectromyographic (EMG) activity of sev-eral respiratory muscle groups and theaccompanying chest wall motion usingmagnetometers.Results - Hypopnoea occurred in as-sociation with eye movements duringphasic rapid eye movement (pREM) sleep.During pREM sleep there were reductionsin EMG activity of the intercostal, dia-phragm, and upper airway muscles com-pared with non-REM sleep. Episodichypopnoea due to partial upper airwayocclusion ("obstructive" hypopnoea) wasseen consistently in four subjects while theothers showed the pattern of "central"hypopnoea accompanied by an overall re-duction in inspiratory muscle activity. Al-though activity of the intercostal muscleswas reduced relatively more than that ofthe diaphragm, lateral rib cage paradox(Hoover's sign) was less obvious duringpREM-related hypopnoea than duringwakefulness or non-REM sleep.Conclusions - Hypopnoea during REMsleep in patients with COPD is associatedwith reduced inspiratory muscle activity.The pattern of hypopnoea may be either"obstructive" or "central" and is generallyconsistent within an individual. Relativelyunopposed action ofthe diaphragm on therib cage during REM sleep is not ac-companied by greater lateral inspiratoryparadox.(Thorax 1995;50:376-382)
Keywords: REM sleep, chronic obstructive pulmonarydisease, respiratory muscle activity, hypopnoea.
Ventilation during rapid eye movement (REM)sleep is characterised by its variability bothwithin and between subjects."2 In patientswith chronic obstructive pulmonary disease(COPD) periods of hypopnoea in REM sleepresult in hypoxaemia, but the precise mech-anisms are uncertain. In healthy subjects re-duced respiratory muscle activity has beenshown in REM sleep3-5; this is generally most
marked in those respiratory muscles which alsohave a postural function, with activity of thediaphragm being relatively spared or even in-creasing. Patients with airways obstruction dueto COPD,"8 have been reported to show asimilar pattern during REM sleep, but theresults have been variable and the numbers ofpatients studied in detail are few.One potential consequence of discoordinate
inspiratory muscle action is recurrent upperairway narrowing or occlusion. Although earlywork on nocturnal hypoxaemia in patients withCOPD suggested that obstructive apnoea wasfrequently present,9 the population studied washighly selected and later work appeared torefute this conclusion.'0 It has subsequentlybeen shown, however, that the clinical featuresassociated with the obstructive sleep apnoeasyndrome can be seen with obstructive hypo-pnoea rather than complete apnoea." Inpatients with COPD it is not clear to whatextent diminished activity of the upper airwaymuscles in REM sleep may result in obstructivehypopnoea and consequent arterial de-saturation.Many patients with COPD, airways ob-
struction, and hyperinflation have abnormalrib cage motion when awake. In particular,a commonly recognised feature is inspiratoryparadox ofthe lateral rib cage margin (Hoover'ssign) due to indrawing by a flattened dia-phragm.'2 We postulated that, in such patients,relative sparing of the activity of the diaphragmduringREM sleep with suppression ofthe otherrespiratory muscles might further impair ribcage motion and therefore exacerbate oxygendesaturation.We studied a group of patients with COPD
to elucidate further the patterns of respiratorymuscle activity in REM sleep and the ways inwhich these may result in hypopnoea.
MethodsTen men with severe COPD and mild to mod-erate hypoxaemia were studied (table 1). Theywere middle aged or elderly and of normalbuild, and all but one had hyperinflation (de-fined as increased functional residual capacity).None was a regular heavy drinker and all ab-stained from alcohol for 24 hours before thestudy. Four subjects (nos 1-4) showed obviouslateral rib cage paradox (Hoover's sign) whenexamined in the semi-recumbent posture whileawake. All subjects gave informed consent priorto participation in the study which was ap-proved by the local ethics committee.
Department ofRespiratory MedicineJ E S WhiteG J Gibson
Department ofMedical PhysicsM J DrinnanA J SmithsonC J Griffiths
Freeman Hospital,Newcastle upon TyneNE7 7DN, UK
Reprint requests to:Dr J E S White.Received 7 April 1994Returned to authors16 June 1994Revised version received23 November 1994Accepted for publication4 January 1995
376
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from

Respiratory muscle activity during REM sleep in COPD
Table 1 Subject characteristics, pulmonary function and daytime arterial blood gas tensions
Patient Age BMI Motion FEV, FRC RV Pao2 Paco2 Sao2no. (years) (kg/rM2) awake (%o predicted) (Go predicted) (%o predicted) (kPa) (kPa) (Go)
1 53 19-5 LP 8 243 277 8-3 5-4 912 76 23-5 LP 24 172 260 8-8 6-1 933 69 28-0 LP 30 197 222 7 2 6-2 874 69 19 9 LP 23 210 240 8-1 6-1 905 60 21-8 Normal 27 236 294 10 9 5 4 946 61 24-5 Normal 46 137 202 - - 907 74 21-5 Normal 41 106 309 12-2 2 5 958 48 19 2 Normal 11 243 309 7 9 7-7 899 53 17-9 Normal 10 279 384 9 0 5-6 9410 70 18-0 Normal 18 275 111 7 9 4 5 91Mean 63 21-4 24 210 261 8-9 5-5 91-4
BMI = body mass index; normal = qualitatively normal motion of the lateral rib cage; LP =lateral paradox; FEV, =forced expiratory volume in one second; FRC =functional residual capacity; RV =residual volume; Pao2= arterial partial pressure of oxygen; Paco, =arterial partial pressure of carbon dioxide; Sao, =oxygensaturation.
Standard sleep study signals were recordedthroughout a night in hospital following oneacclimatisation night. Arterial oxygen sat-uration (Sao2) was recorded by a pulse oximeterusing a finger probe (Biox 3700e, Ohmeda,Louisville, USA), and airflow by thermistors atthe mouth and nose (Oxford Medical, Oxford,UK). Posteroanterior (RCPA) and lateral(RCLAT) rib cage motion and posteroanteriorabdominal motion (ABPA) were obtained usingpairs of magnetometers.'3 Transmitter mag-netometers were positioned in the midline overthe xiphisternum and just above the umbilicusfor RCPA and ABPA, respectively, and overthe left lower costal margin in the mid axillaryline for RCLAT; receiver magnetometers werepositioned at the same horizontal level on theback or in the mid axillary line. A single channelelectroencephalogram (EEG) Cz/Oz was re-corded and an electrooculogram (EOG) fromleft and right eyes was combined as a singlechannel as previously validated.'4 In addition,for the purpose of the present study, surfaceelectromyographic (EMG) activity was re-corded from selected respiratory muscles using9 mm diameter silver/silver chloride cup elec-trodes (SLE, Croydon, Surrey, UK) applied tocarefully cleaned and abraded skin with animpedance of less than 1 kQ. Electrodes wereplaced at least 2 cm apart over five groupsof respiratory muscles: (1) the "genioglossusgroup" (EMGGe), placed 1 cm to each side ofthe midline midway between the chin and thehyoid bone; (2) the parasternal intercostal(EMGI,t) muscles lateral to the sternum in thesecond intercostal space; (3) the diaphragm(EMGDi) in the seventh or eighth intercostalspace in the anterior axillary line, on the rightto reduce cardiac artefact; (4) the rectus ab-dominis (EMGRA) muscle 2 cm lateral to theumbilicus; and the external oblique (EMGEXOb)muscle midway between the inferior costal mar-gin and the iliac crest in the mid clavicular line.Signals were amplified, filtered at 40-1000 Hz,rectified, and integrated using a first order lowpass filter with a time constant of 50 ms. Bothintegrated and "raw" EMG data were recordedon digital tape (EDR 128, Earthdata, South-ampton, UK). The posture of the subject wasrecorded with a low light camera (Panasonic,Japan) and an infrared light using a three hourVHS videotape (NV-GI8 Panasonic, Japan)running at half normal speed to give a studyduration of six hours. Synchronisation wasachieved by superimposition of waveforms on
the video image and by placing a clock in viewof the camera.'5 The subject was allowed toadopt his preferred posture and left to sleep inthe darkened room.Epochs of wakefulness, non-REM and REM
sleep, as assessed by standard criteria afterRechtschaffen and Kales,'6 were identified froma hard copy of the whole study replayed usinga chart recorder (TA4000 Gould, Ilford, UK).REM sleep was further divided into phasic(pREM) and tonic (tREM) periods dependingon the presence or absence of eye movementsusing a method similar to that described byWiegand et al.5 Only periods of sleep with stablesignals and with the subject in his preferredsleeping posture were analysed. Sixteen suchperiods of REM sleep were identified (rangeper subject 1-3), together with 29 adjacentperiods of non-REM sleep (range per subject1-4). The data from these periods were trans-ferred to a personal computer using an analogueto digital converter (Dash- 16, Metrabyte,Taunton, MA, USA). The periods analysedincluded mean (SD) numbers of consecutivebreaths of 59 (23) and 64 (18) during non-REM and REM sleep, respectively. The ana-lysis was performed using specifically de-veloped software which calculated the peaklevel of integrated EMG activity above elec-trical zero, recorded from each muscle for eachbreath and for the captured section as a whole. 7Results ofpeakEMG activity in each individualwere expressed as ratios between REM andnon-REM sleep. Apnoea was defined as ces-sation of airflow and hypopnoea as a reductionin rib cage excursion of at least 50%, both forat least 10 seconds. Apnoeas or hypopnoeaswere classified as "obstructive" when (1) ribcage motion in the posteroanterior dimensionwas paradoxical relative to abdominal motion,and (2) a large increase was seen in EMGGe atthe termination of the event, together withEEG evidence of arousal. Events were definedas "central" when there was an overall decreasein muscle activity accompanied neither by post-eroanterior paradox nor snoring.
Statistical comparisons of the magnitude ofEMG activity were performed by paired t testafter logarithmic transformation of the ratiosof activity in REM and non-REM sleep.
ResultsThe subjects generally slept poorly with mean(SD) sleep efficiency of 45 (20)%. All subjects
377
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from

White, Drinnan, Smithson, Griffiths, Gibson
2.0 -
1.8- __Intercostal
1.6- Diaphragm
1.4 Geriog Iossils T
12-1.0-.
0.8-
0-6-
0.4
0.2
1 2 3 5ti 7 8 9 10Figure 1 Mean (SD) ratios ofpeak EMG activity during phasic REM and non-REMsleep recorded from intercostal, diaphragm, and genioglossus muscle groups in nine subjects(subject no. 6 had no pREM sleep). The reductions in intercostal and diaphragmaticactivity in pREM sleep were significant (p<0-002 and p<0 001, respectively) andintercostal activity was more reduced than that of the diaphragm (p<002). Nosatisfactory recordings of EMGG, were obtained from subject no. 10 in REM sleep.
Table 2 Mean (SD) ratios ofEMG activity duringREM and non-REM sleep
Ratio Ge Int Di
tREM/non-REM 1-08 (0 8) 0-69 (0 3)* 0-86 (0 3)pREM/non-REM 0-56 (0 2)t 0-36 (01)4I 0 55 (0 2)4Difference between NS p<001 p<0005tREM and pREM
Ge = genioglossus; Int = intercostal; Di = diaphragm muscles;NS = not significant.* p<005 different from unity.t p<0002 different from unity.: p<0001 different from unity.
had at least one epoch of REM sleep but noperiods ofphasic eye movements were observedin one subject (no. 10).No attempt was made to measure levels of
tonic EMG activity. Phasic inspiratory EMGI,tand EMGDi activity was seen in all stages ofwakefulness and sleep. Phasic EMGGe activitywas usually detectable during wakefulness, al-though in some subjects this was obscured byhigh levels of tonic activity. Phasic EMGG,activity was seen in all subjects during sleep.The magnitude ofmean peak inspiratory EMGactivity during tREM sleep was similar to thatduring non-REM sleep for EMGGe and EMGDi,while peak EMGI,t activity was less in tREMthan in non-REM sleep (p<005, table 2).During pREM sleep peak activity of all threemuscle groups was markedly suppressed com-pared with non-REM sleep (table 2). The pro-portional reduction in EMGInt activity in pREMsleep was significantly greater than that ofEMGDi (p<0-02, fig 1). EMGI,t and EMGDiactivity were both significantly more reducedin pREM than in tREM sleep (p<0 001, table2). EMGGe activity during pREM sleep wasalso significantly suppressed in comparisonwith non-REM sleep (p<0 002).
Figure 2 shows an example of the reductionin EMGInt activity associated with phasic eyemovements in a subject with qualitatively nor-mal rib cage motion and fig 3 shows a similarpattern in a subject who had paradoxical lateralrib cage motion both when awake and asleep.The episodes of reduced EMG activityillustrated in figs 2 and 3 fit the criteria for"central" hypopnoeas. REM-related hypo-pnoeas of this type were seen in five of the ninesubjects (nos 2, 5, 7, 8, and 10) in whompREM sleep was recorded.
Figure 2 Recordings from subject no. 7 with normal lateral rib cage motion during non-REM andpREM sleep. Therecordings are in order from the top: airflow (V); posteroanterior rib cage motion (RCPA); posteroanterior abdominalmotion (ABPA); lateral rib cage motion (RCLAT); genioglossus group EMG (EMGG,); intercostal EMG (EMGind;diaphragmatic EMG (EMGDd); electrooculogram (EOG). Note considerably reduced intercostal activity and slightlyreduced diaphragmatic activity in association with phasic eye movements during REM sleep compared with non-REMsleep.
C.Cc
0.0
378
I XIz~l V161
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from
Respiratory muscle activity during REM sleep in COPD
Non-REM
RCPA
ABPA
EMGGe
EMGlnt
EMGDi
EOG
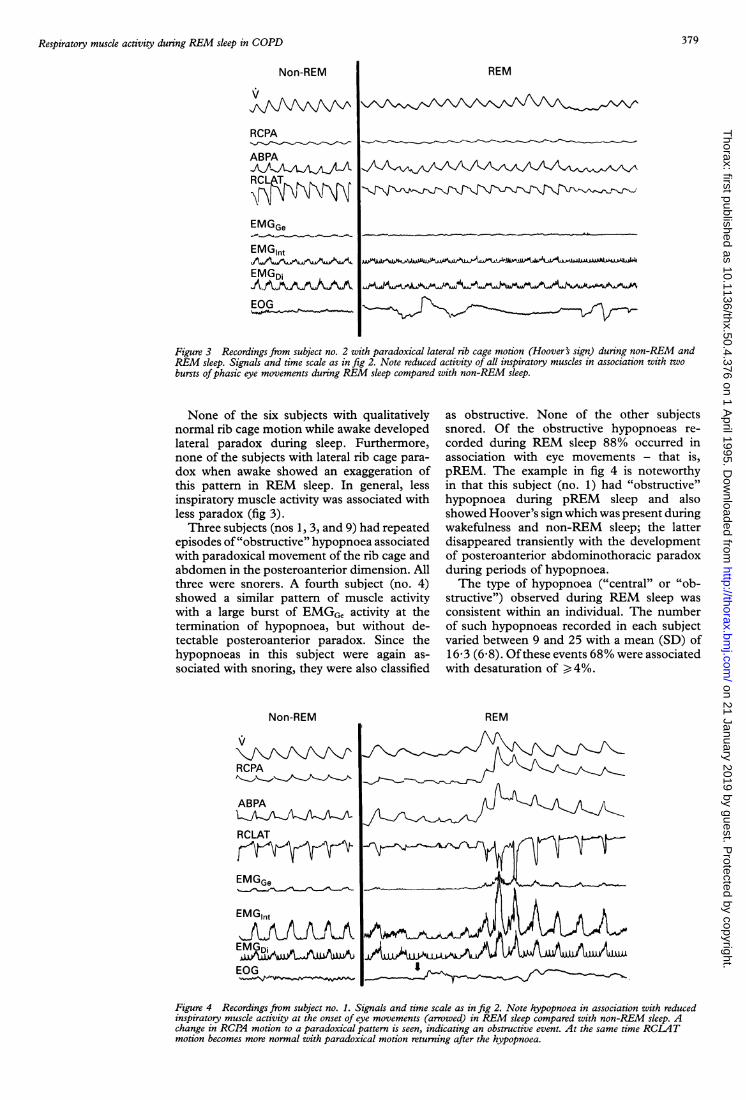
Figure 3 Recordings from subject no. 2 with paradoxical lateral rib cage motion (Hoover's sign) during non-REM andREM sleep. Signals and time scale as in fig 2. Note reduced activity of all inspiratory muscles in association with twobursts ofphasic eye movements during REM sleep compared with non-REM sleep.
None of the six subjects with qualitativelynormal rib cage motion while awake developedlateral paradox during sleep. Furthermore,none of the subjects with lateral rib cage para-dox when awake showed an exaggeration ofthis pattern in REM sleep. In general, lessinspiratory muscle activity was associated withless paradox (fig 3).Three subjects (nos 1, 3, and 9) had repeated
episodes of"obstructive" hypopnoea associatedwith paradoxical movement of the rib cage andabdomen in the posteroanterior dimension. Allthree were snorers. A fourth subject (no. 4)showed a similar pattern of muscle activitywith a large burst of EMGGe activity at thetermination of hypopnoea, but without de-tectable posteroanterior paradox. Since thehypopnoeas in this subject were again as-sociated with snoring, they were also classified
Non-REM
(I
RCPA
ABPA
RCLAT
EMGGe
EMGlnt
EOG
as obstructive. None of the other subjectssnored. Of the obstructive hypopnoeas re-
corded during REM sleep 88% occurred inassociation with eye movements - that is,pREM. The example in fig 4 is noteworthyin that this subject (no. 1) had "obstructive"hypopnoea during pREM sleep and alsoshowed Hoover's sign which was present duringwakefulness and non-REM sleep; the latterdisappeared transiently with the developmentof posteroanterior abdominothoracic paradoxduring periods of hypopnoea.The type of hypopnoea ("central" or "ob-
structive") observed during REM sleep was
consistent within an individual. The numberof such hypopnoeas recorded in each subjectvaried between 9 and 25 with a mean (SD) of16-3 (6 8). Ofthese events 68% were associatedwith desaturation of ) 4%.
REM
Figure 4 Recordings from subject no. 1. Signals and time scale as in fig 2. Note hypopnoea in association with reducedinspiratory muscle activity at the onset of eye movements (arrowed) in REM sleep compared with non-REM sleep. Achange in RCPA motion to a paradoxical pattern is seen, indicating an obstructive event. At the same time RCLATmotion becomes more normal with paradoxical motion returning after the hypopnoea.
REM
379
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from

White, Drinnan, Smithson, Griffiths, Gibson
Expiratory abdominal muscle activity (pre-dominantly in EMGaob) was recorded in theawake state in only two individuals and in nonewas such activity detected during sleep.
DiscussionVentilation during REM sleep shows con-siderable variation within and between in-dividuals and this is reflected in the differentresults of published studies. Such variation fol-lows largely from the variability of REM sleepitself, which is not a homogeneous state butconsists of two distinct subtypes: so-calledphasic REM (pREM) characterised by rapideye movements and myoclonic twitches, andtonic REM (tREM) characterised by muscleatonia and desynchronised EEG.'8 In healthysubjects reductions in ventilation during REMsleep are of variable extent and duration andoccur particularly in relation to periods of eyemovements - that is, pREM.'2 Similar findingswere reported in patients with COPD byGeorge and colleagues'9 who found that fallsin Sao2 were closely related to the density ofeye movements. They found an overall fall inventilation during pREM sleep but the mech-anism of this hypoventilation was not in-vestigated.Few studies of the electrical activity of the
inspiratory muscles during sleep have been re-ported, even in normal subjects. In healthyindividuals a considerable decrease in inter-costal muscle activity is seen while dia-phragmatic activity has been reported to beincreased3 or suppressed.4 Episodes of hypo-pnoea are seen particularly in association witheye movements,4 and inspiratory activity of theupper airway muscles has also been shown tobe reduced in association with eye movementsin normal subjects.'
In patients with COPD Hudgel et al' showedthat diaphragmatic EMG activity decreased inmost cases during REM sleep but it increasedin two of 13 patients; intercostal EMG activitydecreased in the one patient in whom it wasrecorded. No differentiation was made betweentREM and pREM sleep. Johnson et al6 studiedthe activity of the scalene and stemomastoidmuscles in patients with COPD and showedconsistent reductions in EMG activity in as-sociation with pREM, but activity of otherinspiratory muscles was not reported.
Despite an acclimatisation night to minimisethe "first night effect", our subjects slept poorly.Others have encountered a similar problem inpatients with COPD.20 We did, however, obtaingood quality recordings during pREM sleep innine of the 10 subjects. The amount of dataavailable for analysis was further limited byrestricting measurements to those obtained ina constant posture.
Surface EMG recordings have the dis-advantage ofreduced specificity compared withthose obtained using needle electrodes. Theelectrode placements used were, however,chosen to reflect EMG activity of the relevantmuscles with least contamination from othermuscles. Moreover, previous work has shownEMG activity from transmandibular electrodes
to be qualitatively similar to signals from genio-glossus intramuscular electrodes,21 and surfacediaphragmatic EMG recordings are qual-itatively similar to signals obtained from oes-ophageal electrodes even during changes inlung volume.22 In patients with COPD it hasbeen shown that the surface diaphragmaticEMG correlates well with transdiaphragmaticpressure.7 We found no evidence of abdominalmuscle activity during sleep, but cutaneouselectrodes are probably less sensitive for de-tection of expiratory activity as recent work hasshown that the most frequently active ex-piratory muscle in awake subjects with COPDis transversus abdominis, which is the leastaccessible to surface recording.23 We classifiedas "central" those events where an overall re-duction in inspiratory EMG activity alone wasobserved; "obstructive" events were thosewhere abdominothoracic paradox, a large in-crease in EMGGe at the termination of hypo-pnoea, and EEG evidence of arousal wereobserved in the presence of snoring. One sub-ject (no. 4) who was categorised as havingobstructive hypopnoea had no detectable ab-dominothoracic paradox during these events.As has been pointed out previously, this doesnot exclude obstructive events as no accountis taken of motion in the craniocaudal di-mension.24 Confident identification of theseevents would require measurement of oes-ophageal pressure which was not obtained,but the association with snoring and arousalsupports the classification as "obstructive".We have confirmed and extended previous
observations on the important association be-tween phasic eye movements duringREM sleepand suppression of activity of the inspiratorymuscles in patients with COPD. Our resultshelp to explain the mechanisms of several pre-vious observations in REM sleep - namely,hypoventilation in pREM,' reduced con-tribution of rib cage to ventilation,7 decreasein oxygen utilisation by the respiratory muscles,8and oxygen desaturation in patients withCOPD related to the density of eye move-ments.'8 The limited data available from thisand other studies suggest that the inhibitoryeffects of pREM sleep in patients with COPDand normal subjects are similar. The con-sequences for oxygenation, however, are likelyto be greater in patients with COPD, par-ticularly in those of the "blue bloater" typewho show more marked arterial desaturationduring sleep.25
MECHANISMS OF HYPOPNOEAThe relative degrees of inhibition of the variousinspiratory muscle groups during pREM sleepvaried between individuals, but the pattern wasconsistent within an individual, as has also beenobserved in normal subjects by Neilly et al.26Intercostal muscle activity was proportionallymore suppressed than that of the diaphragmin all but one of our subjects. The degree ofreduction in EMGG, was more variable thanthat of EMGlnt or EMGDi. The differentialsuppression of inspiratory muscle groups as-sociated with pREM sleep has clear im-
380
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from

Respiratory muscle activity during REM sleep in COPD
plications for the mechanism(s) of hypopnoeaand consequent oxygen desaturation. In allcases in the present study such events werecharacterised by hypopnoea rather than com-plete apnoea. Of the nine subjects studied inpREM sleep, the pattern of hypopnoea wasclassified as "central" in five and "obstructive"in four. A study of patients with the sleepapnoea syndrome suggested that an importantdetermination of whether an event is classifiedas "central" or "obstructive" is the balance ofactivity between the upper airway muscles andthe inspiratory "pump" muscles.27 A similarbalance may be relevant to the genesis ofhypo-pnoeas in some patients with COPD. Thus,overall reduction in activity of the various in-spiratory muscles (fig 3, right) results in a"central" hypopnoea whilst disproportionatereduction in EMGGe activity produces an "ob-structive" hypopnoea even though activity ofother inspiratory muscles is also reduced (fig4, right). However, greater reduction in peakactivity of the upper airway muscles than inthat of the inspiratory "pump" muscles duringpREM sleep was seen in only one ofthe subjects(no. 1). Clearly, upper airway anatomy andcompliance also contribute to the pathogenesisof narrowing or collapse of the airway, andhence to whether or not an hypopnoea (orapnoea) appears "obstructive" or "central".The calibre of the upper airway is reducedin some subjects with COPD,27 and alcoholconsumption has been suggested as a con-tributory factor to obstructive events in thesepatients.28 We did not obtain a complete alcoholhistory in all our subjects, but subject no. 1was a non-drinker and none of the subjectsdrank alcohol within 24 hours of the study.The pattern of hypopnoea between individualswas not related to the posture in which eachwas studied.
Guilleminault et al9 suggested that de-saturation in patients with COPD was com-monly due to obstructive apnoea but the studypopulation was highly selected. Subsequently,a prospective study of patients with COPDby Catterall and colleaguesl' concluded thatREM-related desaturation in COPD was notdue to obstructive sleep apnoea. Although theynoted frequent periods of hypopnoea, themechanism was not investigated. It is, however,now accepted that the full blown clinical pictureassociated with the obstructive sleep apnoeasyndrome can result from frequent obstructivehypopnoea without complete airway oc-clusion." Although apnoea may be infrequentin patients with COPD, our data suggest thatobstructive hypopnoea may be quite common.This conclusion is also supported by the studyby Littner et al29 which suggested that un-expected partial upper airway obstruction, asassessed by intrathoracic pressure measure-ment, contributed to nocturnal desaturation inthree of nine patients with COPD.
DISCOORDINATE CHEST WALL MOTIONReduced expansion and, occasionally, para-doxical motion of the rib cage during REM
sleep have been described in previous studiesin patients with COPD and related to inhibitionof respiratory muscle EMG activity,67 but thestudies concentrated on volume changes of therib cage compartment as a whole rather thanmotion in a particular dimension. Sevenpatients studied by Hudgel et al7 showed para-doxical motion of the rib cage compartmentduring REM sleep, with five exhibiting thispattern only in the hypopnoeic periods ofREMsleep, but the relation to specific inspiratorymuscle activity was not clear. Johnson andRemmers6 reported paradoxical motion of therib cage compartment in association with re-duced EMG activity of the scalenus anteriormuscle during pREM sleep, but no data weregiven on intercostal or diaphragmatic activity;abdominal excursion increased but only by asmall amount. Since, however, similar com-partmental paradox occurs with hypo-ventilation due to narrowing of the upperairway, "central" and "obstructive" hypo-pnoea cannot be distinguished using this cri-terion alone.2We are unaware of any previous studies
which have assessed lateral rib cage paradox(Hoover's sign) during sleep. Although ourseries included only four subjects with Hoover'ssign while awake, we found consistently thatlateral paradox became less, rather than more,evident during pREM-related hypopnoeas.Classically, Hoover's sign is associated with alow flat diaphragm and the proposed mech-anism involves abnormal traction on the lateralrib cage via its insertional effect. 2 We hy-pothesised that loss of intercostal muscle ac-tivity and relative preservation ofdiaphragmaticactivity during REM sleep might exaggeratethe distortion, but clearly this was not thecase. However, a change in magnitude of theintegrated EMG activity may not be relateddirectly to the force of muscle contraction andthere is some evidence that, during REM sleep,electromechanical coupling of the diaphragmbecomes less efficient.30 Such an effect mightcounter the greater rib cage distortion whichwould be expected from relatively unopposeddiaphragmatic contraction. Alternatively, thedegree of lateral rib cage paradox in subjectswith hyperinflation may depend simply on thestrength of diaphragmatic contraction, ir-respective of any potential stabilising effect ofintercostal muscle activity.
We thank the Chest, Heart and Stroke Association and theBreathe North branch of the British Lung Foundation forfinancial support for this project.
1 Gould GA, Gugger M, Molloy J, Tsara V, Shapiro CM,Douglas NJ. Breathing pattern and eye movement densityduring REM sleep in humans. Am Rev Respir Dis 1988;138:874-7.
2 Millman RP, Knight H, Kline LR, Shore ET, Chung D-CC, Pack AI. Changes in compartmental ventilation inassociation with eye movements during REM sleep.JApplPhysiol 1988;65: 1196-202.
3 Tabachnik E, Muller NL, Bryan AC, Levison H. Changesin ventilation and chest wall mechanics during sleep innormal adolescents. JAppl Physiol: Respirat Environ 1981;51:557-64.
4 Muller NL, Francis PW, Gurwitz D, Levison, Bryan CA.Mechanism of haemoglobin desaturation during rapid-eye-movement sleep in normal subjects and in patientswith cystic fibrosis. Am Rev Respir Dis 1980;121:463-9.
5 Wiegand L, Zwillich CW, Wiegand D, White DP. Changes
381
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from

White, Drinnan, Smithson, Griffiths, Gibson
in upper airway muscle activation and ventilation duringphasic REM sleep in normal men. J Appl Physiol 1991;71:488-97.
6 JohnsonMW, Remmers JE. Accessory muscle activity duringsleep in chronic obstructive pulmonary disease. Jf ApplPhysiol: Respirat Environ 1984;57: 1011-7.
7 Hudgel DW, Martin RJ, Capehart M, Johnson B, Hill P.Contribution of hypoventilation to sleep oxygen de-saturation in chronic obstructive pulmonary disease. J.Appl Physiol: Respirat Environ 1983;55:669-77.
8 Fletcher EC, Gray BA, Levin DC. Nonapneic mechanismsof arterial oxygen desaturation during rapid-eye-move-ment sleep.JApplPhysiol: Respirat Environ 1983;54:632-9.
9 Guilleminault C. Cummiskey J, Motta J. Chronic ob-structive airways disease and sleep studies. Am Rev RespirDis 1980;122:397-406.
10 Catterall JR, Douglas NJ, Calverley PMA, Shapiro CM,Brezinova V, Brash HM, et al. Transient hypoxaemiaduring sleep in chronic obstructive airways is not a sleepapnoea syndrome. Am Rev Respir Dis 1983;128:24-9.
11 Gould GA, Whyte KF, Rhind GB, Airlie MAA, CatterallJR, Shapiro CM, et al. The sleep hypopnoea syndrome.Am Rev Respir Dis 1988;137:895-900.
12 Gilmartin JJ, Gibson GJ. Mechanisms of paradoxical ribcage motion in parents with chronic obstructive pulmonarydisease. Am Rev Respir Dis 1986;134:683-7.
13 Griffiths CJ, Gilmartin JJ, Gibson GJ, Murray A. Measure-ment of chest wall movement; design, performance andclinical use of a four channel magnetometer instrument.Clin Phys Physiol Meas 1983;4:363-71.
14 Wells DT, Allen RP, Wagman AMI. A single channel systemfor recording eye movements. Psychophysiology 1977;14:73-4.
15 Griffiths CJ, Cooper BG, Gibson GJ. A video systemfor investigating breathing disorders during sleep. Thorax1991;46:136-40.
16 Rechtshaffen A, Kales A, eds. A manual of standardisedterminology, techniques and scoring system for sleep stages ofhuman subjects. Bethesda, MD: National Institute ofHealth (Publication No. 204), 1968.
17 Drinnan MJ, Murray A, White JES, Smithson AJ, GibsonGJ, Griffiths CJ. Automated measurement of the cyclicactivity of the respiratory muscles. Med Eng Phys 1994;16:477-83.
18 Sullivan CE, Murphy E, Kozar LF, Phillipson EA. Ventil-
atory responses to CO2 and lung inflation in tonic versusphasic REM sleep. J Appl Physiol: Respirat Environ 1979;47:1304-10.
19 George CF, West P, Kryger MH. Oxygenation and breathingpattern during phasic and tonic REM in patients withchronic obstructive pulmonary disease. Sleep 1987;10:234-43.
20 Leitch AG, Clancy LJ, Leggett RJE, Tweedale P, DawsonP, Evans JI. Arterial blood gas tensions, hydrogen ion,and electroencephalogram during sleep in patients withchronic ventilatory failure. Thorax 1976;31 :730-5.
21 Sauerland EK, Sauerland BAT, Orr WC, Hairston LE.Noninvasive electromyography of human genioglossal(tongue) activity. Electromyogr Clin Neurophysiol 1981 ;21:279-86.
22 Benzett RB, Inbar GF, Brown R, Goldman M, Rossier A,Mead J. Diaphragm electrical activity during negativelower torso pressure in quadriplegic men. J Appl Physiol1981;51:654-9.
23 Ninane V, Rypens F, Yernault J-C, de Troyer A. Abdominalmuscle use during breathing in patients with chronicairflow obstruction. Am Rev Respir Dis 1992;146:15-21.
24 Staats BA, Bonekat HW, Harris CD, Offord KP. Chest wallmotion in sleep apnoea. Am Rev Respir Dis 1984;130:59-63.
25 Douglas NJ, Calverley PMA, Leggett RJE, Brash HM,Flenley DC, Brezinova V. Transient hypoxaemia duringsleep in chronic bronchitis and emphysema. Lancet 1979;i:1-4.
26 Neilly JB, Gaipa EA, Maislin G, Pack AI. Ventilation in earlyand late rapid-eye-movement sleep in normal humans. JAppl Physiol 1991;71:1201-15.
27 Block AJ, Faulkner JA, Hughes RL, Remmers JE, ThachB. Factors influencing upper airway closure. Chest 1984;86:114-22.
28 Chan CS, Grunstein RR, Bye PTP, Woolcock AT, SullivanCE. Obstructive sleep apnoea with severe chronic airflowlimitation. Am Rev Respir Dis 1989;140:1274-8.
29 Littner MR, McGinty DJ, Arand DL. Determinants ofoxygen desaturation in the course of ventilation duringsleep in chronic obstructive pulmonary disease. Am RevRespir Dis 1980;122:849-57.
30 Hendricks JC, Kline LR. Differential activation within costaldiaphragm during rapid-eye-movement sleep in cats. JAppl Physiol 1991;70:1194-200.
382
on 21 January 2019 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.50.4.376 on 1 April 1995. D
ownloaded from