respiratory system chapter 22. organs of the respiratory tract upper respiratory tract –located...
TRANSCRIPT

Respiratory SystemChapter 22

Organs of the Respiratory Tract
• Upper respiratory tract– Located outside of the thoracic cavity– Include nose/ nasal cavity, pharynx, larynx
and upper trachea
• Lower respiratory tract– Located within the thoracic cavity– Includes lower trachea, bronchi,
bronchioles, alveoli and lungs; also includes pleural cavity and muscles of respiration
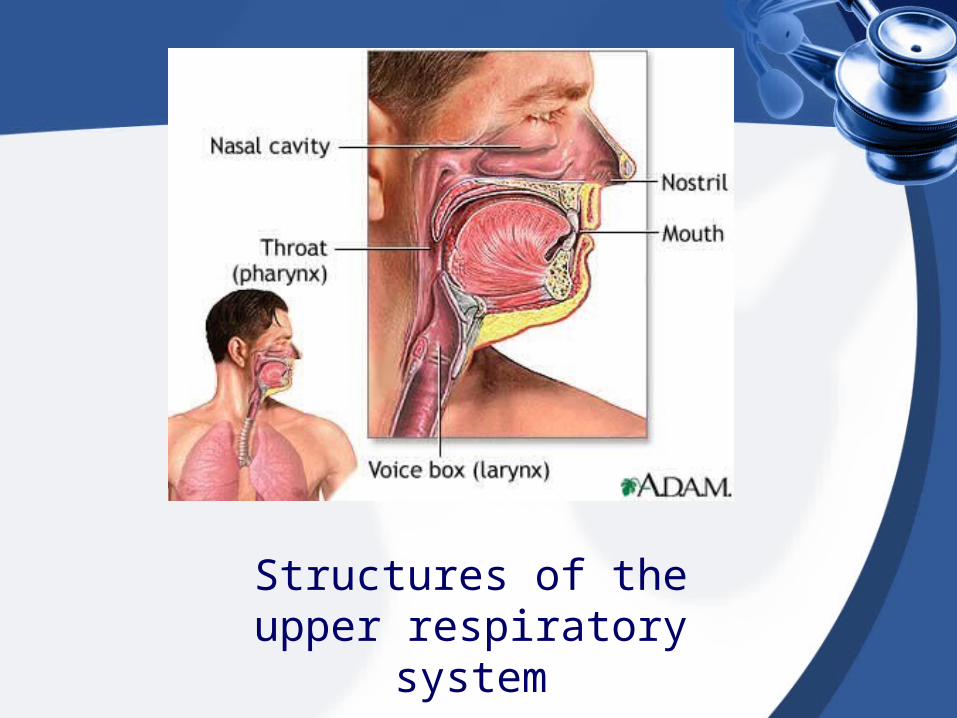
Structures of the upper respiratory system

Structures of the lower respiratory system

Respiratory Organs
• Concerned with conduction (movement) of air through the respiratory passages
• Alveoli are tiny air sacs located at the ends of the respiratory passages– Concerned with the exchange of oxygen
and carbon dioxide

Structures of the Upper Tract
• Nose– Nasal cavities (inner portion) separated by
the nasal septum– Openings to entrance of nose called
nares; contain hairs to filter large particles and dust; contains smell receptors
– Nasal conchae are bony projections on the lateral walls; contains blood vessels and mucus to warm air and trap particles

Figure 22-2 A, Organs of the upper respiratory tract. B, Larynx showing the thyroid cartilage (Adam's apple). C, Vocal cords and glottis (closed). D, Vocal cords and glottis (open).
Elsevier items and derived items © 2007, 2003, 2000 by Saunders, an imprint of Elsevier Inc.

Structures of the Upper Tract
• Pharynx– Commonly called the throat– Divided into nasopharynx, oropharynx and
laryngopharynx– Part of the digestive and respiratory
system

Structures of the Upper Tract
• Larynx– Commonly called the voicebox– Three functions: passageway for air during
breathing; produces sound; prevents food and foreign substances from entering the airways
– Composed of cartilage (thyroid cartilage), muscles and ligaments
– Epiglottis is cartilage flap that covers the entrance to the larynx

Structures of the Upper Tract
• Larynx– Contains vocal cords; folds of tissue
composed of muscle and elastic ligaments– The glottis is the space between the vocal
cords– True vocal cords
• Produce sound
– False vocal cords• Do not produce sound

Normal larynx showing true and false cords and cartilage rings of trachea

Structures of the Upper Tract
• Larynx– Loudness of voice depends on the force of
air passing over the true vocal cords– Sounds are formed using pharynx, oral
cavity, tongue and lips– Sound resonates in nasal cavities, sinuses
and pharynx

Structures of the Upper Tract
• Larynx– Food or other foreign material (emesis) is
normally kept out of the larynx by closure of the epiglottis
– During swallowing, the larynx moves upward and forward and the epiglottis moves downward
– Patients who have difficulty swallowing are at high risk for aspiration
Structures of the Upper Tract
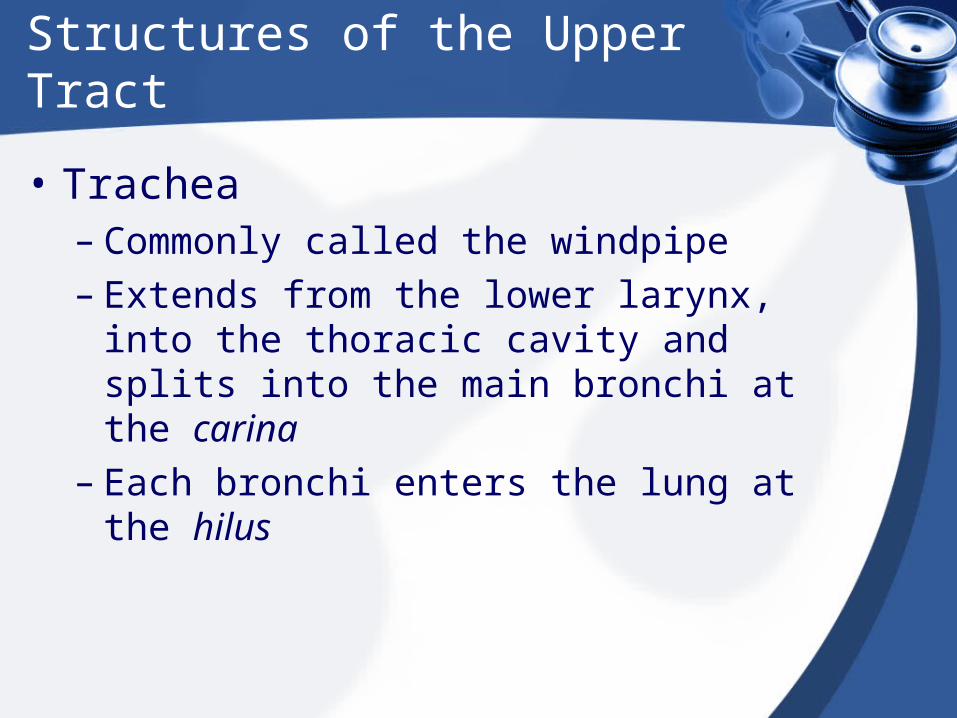
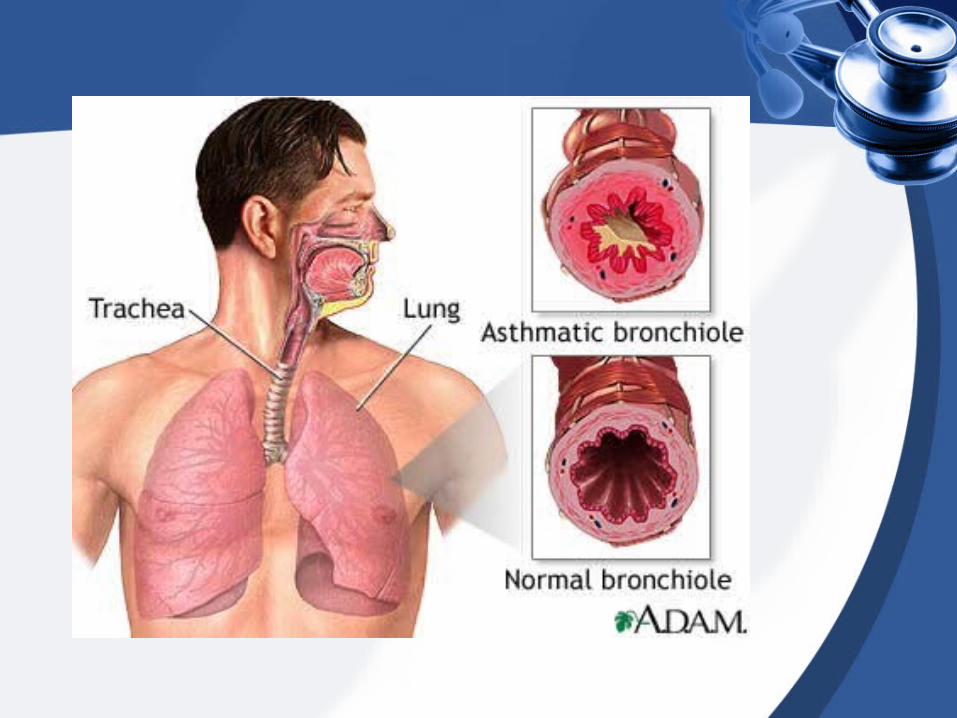
• Trachea– Commonly called the windpipe– Extends from the lower larynx, into the
thoracic cavity and splits into the main bronchi at the carina
– Each bronchi enters the lung at the hilus

Structures of the Upper Tract
• Trachea– Lies anterior to the esophagus– Supported by C-shaped rings of cartilage;
important to keep trachea open

Carina

Tracheostomy

Structures of the Lower Tract
• Bronchi– Trachea splits into right and left mainstem, or
primary, bronchi (singular bronchus)– Each primary bronchus branches into
secondary bronchi; these in turn branch into smaller tertiary bronchi; upper bronchi contain cartilage which eventually disappears in lower branches
– The right bronchus is shorter, wider and more vertical; most aspirations and pneumonias occur here


Structures of the Lower Tract
• Bronchioles– Bronchi divide into smaller and smaller
branches called bronchioles– Contain smooth muscle, no cartilage;
constriction causes reduced air flow– Asthma: involves constriction of
bronchioles; patient will complain of tightness in chest, difficulty breathing, cough; wheezing is the sound of air moving through narrow passageways

Structures of the Lower Tract
• Bronchioles– Asthma: patient needs to be treated with
bronchodilators to increase airflow
– Bronchioles contain beta2- adrenergic receptors; stimulation causes relaxation of the smooth muscle and therefore bronchodilation
• Albuterol is a beta2-adrenergic agonist

Structures of the Lower Tract
• Alveoli– Bronchioles end in clusters of tiny air sacs
called alveoli (singular alveolus)– A pulmonary capillary surrounds each
alveolus– Function is to exchange oxygen and
carbon dioxide across the membrane between the alveoli and the capillaries
– Atelectasis refers to collapsed alveoli

Structure of terminal air passages.


Structures of the Lower Tract
• Lungs– Right and left lungs located in the pleural
cavities– Divided into lobes; right lung has three
lobes (upper, middle and lower), left lung has two lobes (upper and lower)
– Upper part of the lung is the apex; lower part of the lung is the base


External surface of a normal lung illustrating lobes and fissues.The faint cobblestonelike pattern of the pleural surface defines the individual lung
lobules.

Bronchogram illustrating normal branching of bronchi and bronchioles that are normal in caliber and appearance.

Structures of the Lower Tract
• Pleural Membranes– Serous membranes line the outer portion
of each lung and inner portion of the chest wall
– Visceral pleura lines the outer portion of the lung
– Parietal pleural lines the inner chest wall– Space between the two is called the
pleural cavity or intrapleural space– Pleural membranes secrete pleural fluid
for lubrication

Structures of the Lower Tract
• Pleural Membrane– Under normal circumstances, pleural fluid
provides lubrication and reduces friction– Certain diseases and conditions cause
blood, air or excess fluid to enter the pleural cavity
– Pleural effusion– Empyema– Pneumothorax/ hemothorax


Collapsed & Expanded Lungs
• Lungs can collapse because of the principles of elastic recoil and surface tension
• If the thoracic cavity is entered (trauma, surgery etc.) the lungs will collapse

Collapsed & Expanded Lungs
• Elastic Recoil– Stretchy fibers in the lungs stretch in
response to a volume of air– Theses fibers will remain stretched as long
as air is present in the lungs– When the air is allowed to escape, the
lung fibers will collapse (recoil) into their unstretched position


Collapsed & Expanded Lungs
• Compliance– Measure of elastic recoil– Decreased compliance results in stiff
lungs- difficult to inflate (ARDS, pulmonary edema, pulmonary fibrosis)
– Increased compliance results in limp, over-stretched lungs; air cannot be expelled completely (emphysema, COPD)


X-Ray showing hyperinflated lungs in a patient with COPD

Collapsed & Expanded Lungs
• Surface Tension– Each alveolus is lined with a thin layer of
water molecules– Remember water is a polar molecule; the
positive end of one molecule is attracted to the negative end of another molecule
– This attraction between molecules causes the alveoli to shrink or collapse
• So why don’t the alveoli all collapse??

Collapsed & Expanded Lungs
• Surface Tension– Specialized lung cells secrete surfactants
(specialized proteins)– Surfactants decrease (not eliminate)
surface tension by interfering with the electrical attraction between water molecules
– Every few breaths a person takes a large breath (sigh); causes an increased stretch of the alveoli and promotes the secretion of surfactants



Collapsed & Expanded Lungs
• Why Lungs Expand…
• Lung expansion depends on pressures within the intrapleural space and in the thoracic cavity
• Intrapulmonic pressure (within the lungs)
• Intrapleural pressure (within the pleural space)
• Atmospheric pressure (pressure in the room)


Collapsed & Expanded Lungs
• Lungs remain expanded because the intrapleural pressure is negative – Pressure within the lung (intrapulmonic)
and outside of the chest (atmospheric) is greater than the pressure in the pleural space

Visceral and Parietal separate and cause the lung to collapse

Collapsed & Expanded Lungs
• Pneumothorax– Surgical, trauma, spontaneous
• Hemothorax
• Hemopneumothorax

A, Normal relation of lung to chest wall. B, Pneumothorax caused by a perforating injury of lung.


Typical chest tube placement

Normal chest X-ray
Normal Chest X-ray (CXR)

PneumothoraxWhite arrow indicates collapsed lung
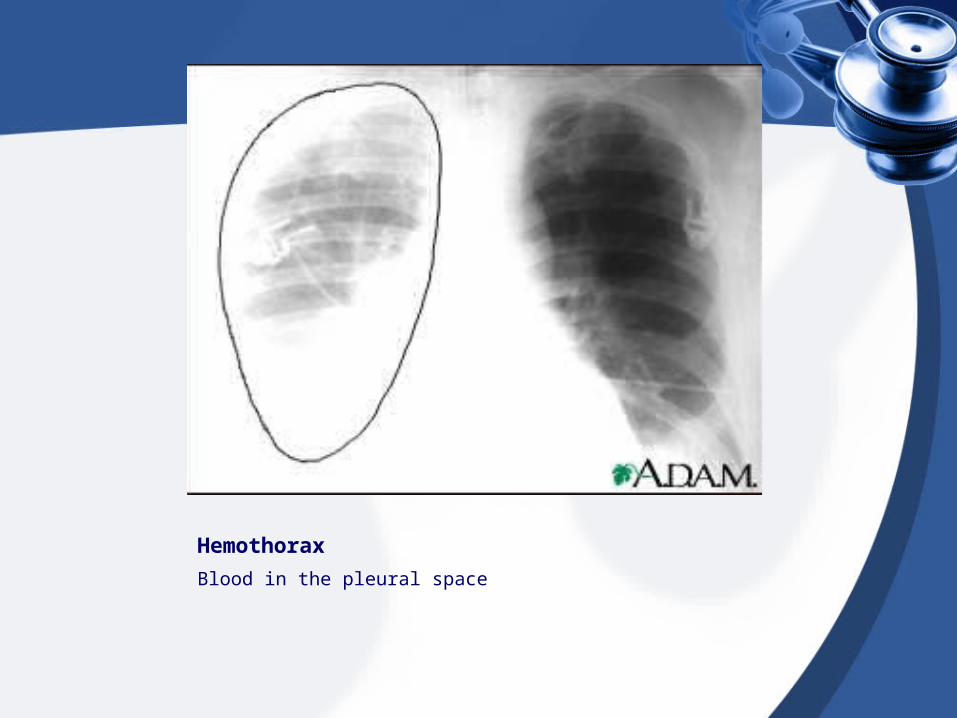
Hemothorax
Blood in the pleural space
Respiratory Function
• Includes three steps:
• Ventilation (or, breathing)
• Exchange of oxygen or carbon dioxide
• Transport of oxygen and carbon dioxide by the blood

Ventilation (Breathing)
• Movement of air into and out of the lungs
• Two phases– Inhalation (inspiration)– Exhalation (expiration)
• Respiratory cycle is one inhalation and one exhalation

Ventilation (Breathing)
• Air flows in response to changes in pressure
• Inspiration– Ribs move upward and outward…increase
volume of thoracic cavity/ lungs…decreases pressure in thoracic cavity…air rushes in
• Expiration– Ribs/diaphragm relax…volume decreases
and pressure increases…air is pushed out

Ventilation (Breathing)
• The relationship between pressure and volume is the basis for Boyle’s law
• Inhalation– Associated with an increase in thoracic
volume
• Expiration– Associated with a decrease in thoracic
volume

Boyle’s law

Ventilation (Breathing)
• Muscles of respiration– Diaphragm
• Chief muscle of inspiration• Contraction of diaphragm flattens it and pulls it
down toward the abdomen (lengthens)
– Intercostal muscles• External and internal intercostals; between the
ribs• Contraction of external muscles cause the ribs
to move up and out (widens)

Ventilation (Breathing)
• Muscles of respiration– Accessory muscles include abdominal and
internal intercostals– Assist with forced exhalation


Ventilation (Breathing)
• Inhalation is an active process; it requires ATP to fuel the muscles as they contract
• Exhalation is a passive process; it occurs when the muscles relax, so there is no ATP used
• During exercise or with some lung diseases (COPD), exhalation becomes an active process because accessory muscles must be used

Innervation
• Phrenic nerve and intercostal nerves cause the skeletal muscles of respiration to contract
• Phrenic nerve exits the spinal cord at the level of C4
Gas Exchange
• Exchange of oxygen and carbon dioxide occurs in the lungs and at the cellular level
• Lungs (alveoli)– Large surface area (millions of alveoli in
each lung)– Thin walls of alveoli and pulmonary
capillaries– Closeness of alveoli and pulmonary
capillaries (ensures high rate of diffusion)

Diffusion of Gases
• The amount of each gas creates a pressure, called a partial pressure– Room air contains 78% Nitrogen (not used
by the body), 21% oxygen (PO2) 0.04% carbon dioxide (PCO2)
• Higher pressure, diffusion occurs more easily; gases move from high pressure to low pressure

Gas Exchange
• Oxygen– Artery has more O2 than the cells, so O2
leaves the blood and moves into the cells
– The blood has supplied the cells with O2
• Carbon dioxide– Cells have more CO2 than blood, so CO2
moves from the cells into the blood
– The blood has removed CO2 waste from the cells

Lung Volumes
• Respiration can be altered to meet the needs of the body
• The amount or volume of air inhaled can vary

Lung Volumes
• Tidal volume– Amount of air moved in and out with each breath
• Inspiratory reserve volume– Additional amount of air able to be inhaled
• Expiratory reserve volume– Additional amount of air able to be exhaled
• Residual volume– Amount of air left in lungs after forced exhalation
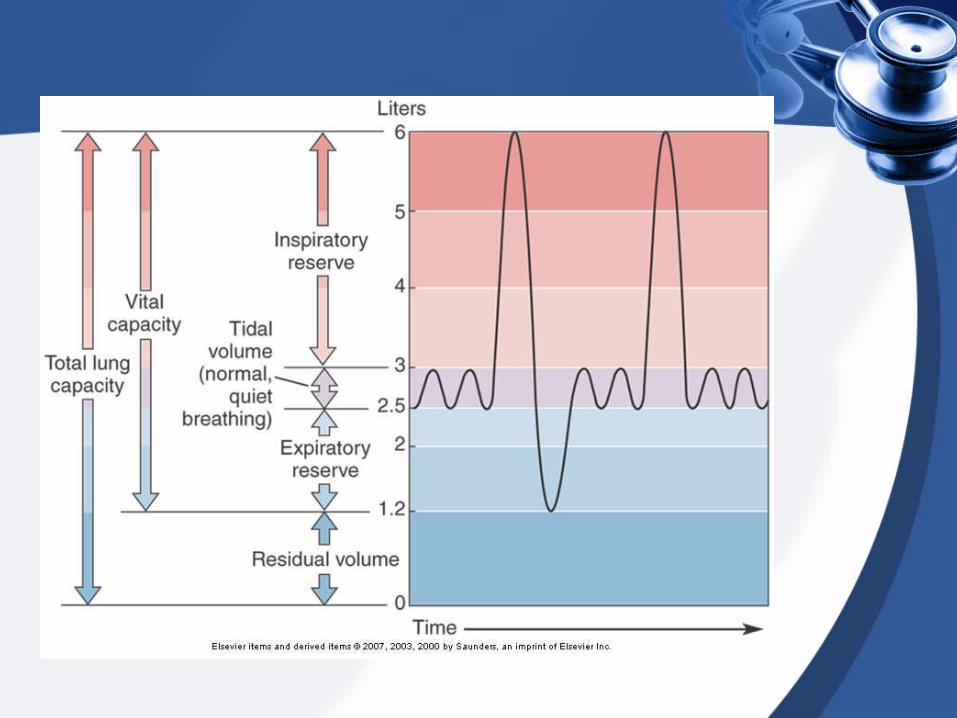
Lung Capacities
• Pulmonary capacity refers to combinations of lung volumes
• Vital capacity– Tidal volume, inspiratory & expiratory
reserves– Used to measure pulmonary function
• Total lung capacity– Vital capacity plus residual volume

Lung Capacities
• Anatomical dead space– Amount of air left in the respiratory system
at the end of inhalation– Does not reach the alveoli, so it is not
involved in gas exchange– Includes air in the mouth, nose, pharynx,
larynx, trachea and bronchial tree

Control of Breathing
• Normal respiration– Rhythmic– Involuntary– Can voluntarily alter rate and depth– Normal rate?
• 12 to 20 breaths per minute for adults• 20 to 40 breaths per minute for infants and
children

Control of Breathing
• Breathing is controlled by nervous system and chemical mechanisms
• Medullary respiratory control center– Located in the medulla– Sets breathing rhythm– Sends nerve impulses to the phrenic
nerve- cause alternating contraction and relaxation
– Very sensitive to narcotics (opioids)

Control of Breathing
• Other centers located in the pons help modify and control breathing patterns
• Pneumotaxic center
• Apneustic center

Control of Breathing
• Chemoreceptors in the body respond to different chemicals that affect respiration
• Central chemoreceptors– Located within the central nervous system
– Respond to altered levels of CO2 and H+
• Peripheral chemoreceptors– Located outside of the central nervous
system
– Respond to altered levels of H+ and O2

Control of Breathing
• Note:– The main regulator of breathing is CO2
levels, not O2
– The body responds to altered levels of CO2 very quickly; oxygen levels must be very low in order to elicit a response
– Patients with COPD alter their physiology so that oxygen becomes the driving force of respiration

Variations of Respiration
• Hyperventilation– Increased rate and depth of respirations
– Causes excessive loss of CO2 (hypocapnia)
– Anxiety, acidosis, pulmonary edema, asthma• Hypoventilation
– Decreased rate and depth of respirations
– Causes increased levels of CO2 (hypercapnia) and decreased levels of O2
– Respiratory obstruction, depression, trauma

Variations of Respiration
• Dyspnea
• Tachypnea
• Eupnea
• Orthopnea
• Hypopnea
• Cheyne-Stokes
• Kussmaul breathing


Respiratory Abnormalities


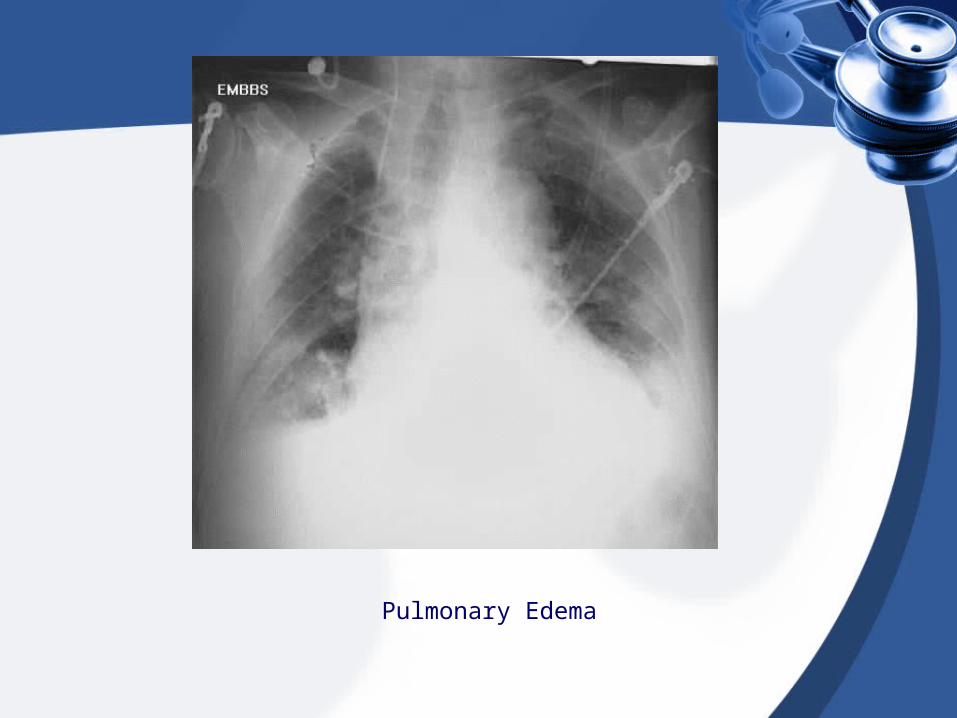
Pulmonary Edema

Pneumonia
