results - shodhgangashodhganga.inflibnet.ac.in/bitstream/10603/26672/12/12_chapter 5.pdffindings of...
TRANSCRIPT
RESULTS

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 95 University of Delhi, Delhi
Results
On the basis of detailed history, the study subjects (400 infertile females fulfilling
inclusion criteria) were categorized with regard to their demographic profile, type of
infertility and duration of married life. Patients were also categorized according to their
gynecological symptoms, menstrual disturbance, history of contact or past history of
TB and history suggestive of active disease. Findings of molecular tests (DNA PCR,
mRNA-based RT-PCR, real-time and gene fingerprinting for mutation monitoring in
the drug resistant genes) were correlated with a cascade of clinical profile/laparoscopic
findings and pregnancy outcome following diagnosis and anti-tubercular treatment.
Demographic profile of study subjects
Socioeconomic status
When the educational and professional/economical background of the patients was
compared, it was found that maximum patients (43%) belonged to middle strata of the
society while 37% and 20% patients belonged to lower and higher strata of the society
as shown in fig 15 (110).
Fig 15: Pie diagram depicting socioeconomic status of the study subjects.
State-wise geographic distribution
Maximum patients visiting the infertility clinic were from Delhi (276/400) followed by
Uttar Pradesh (68/400), Haryana (48/400) and other states (8/400). The geographic
distribution of patients among various states is shown in fig 16.
37%
43%
20%
Socioeconomic Status
lower middle high

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 96 University of Delhi, Delhi
Fig 16: Graph depicting the state distribution among the study subjects
Details of Study subjects & healthy fertile Controls
The patients in the study group were between the age group 18 and 40 years. The
mean age of the patients was 27.8 years with a standard deviation of 4.7 years.
Table 19: Age distribution of study subjects.
Age (years) No. of cases Percentage
18-25 98 24.5%
26-30 160 40%
31-35 107 26.75%
36-40 39 9.75%
Total 400
Fig 17: Graph showing age distribution among the study subjects.
0%
20%
40%
60%
80%
Delhi Haryana Uttar Pradesh
Others
69%
12% 17%2%
Geographic distribution
24.5%
40%
26.8%
9.8%
0
10
20
30
40
50
18-25 yrs 26-30 yrs 31-35 yrs 36-40 yrs
Age Distribution
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 97 University of Delhi, Delhi
Table 20: Age distribution among fertile controls.
On analysis, we found that maximum number of Study subjects (40%) belonged to the
age group 26-30 years suggesting that female genital tuberculosis affects females in
their early reproductive age.
Duration of marital life
The duration of marital life ranged between 1.5 years and 17 years. The mean duration
of marital life was 7.2 years with a standard deviation of 3.5 years.
Type of infertility
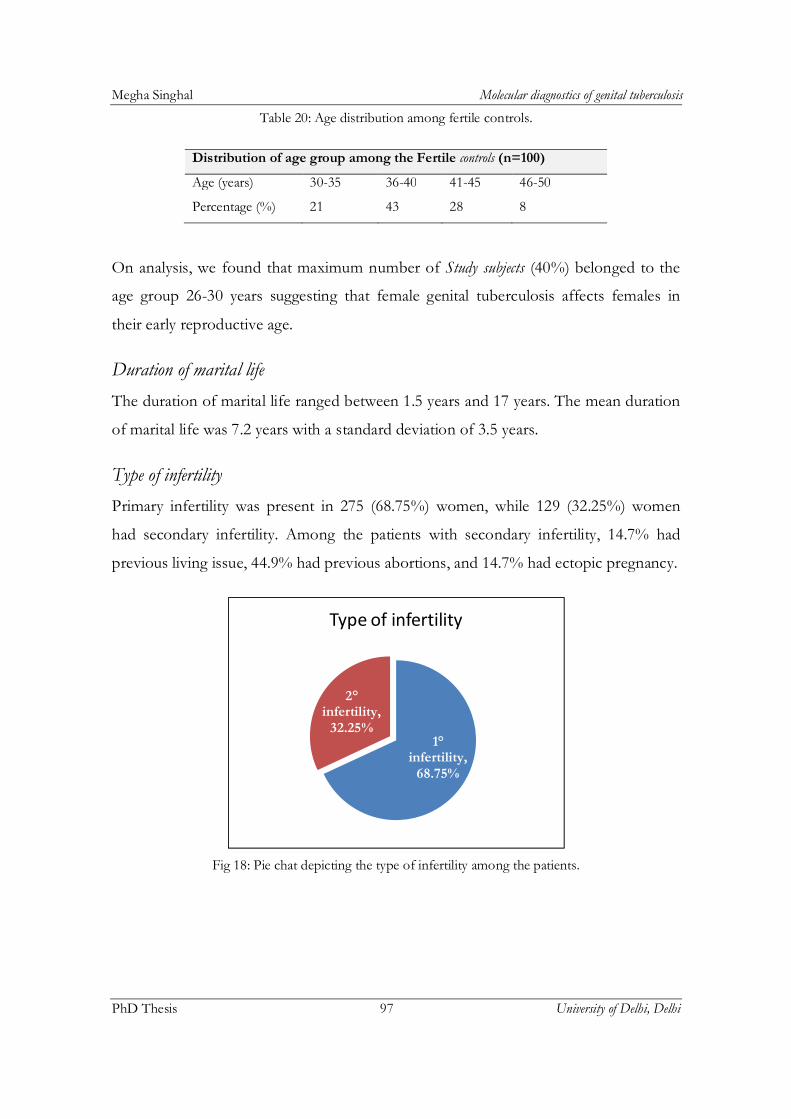
Primary infertility was present in 275 (68.75%) women, while 129 (32.25%) women
had secondary infertility. Among the patients with secondary infertility, 14.7% had
previous living issue, 44.9% had previous abortions, and 14.7% had ectopic pregnancy.
Fig 18: Pie chat depicting the type of infertility among the patients.
1°infertility,
68.75%
2°infertility,
32.25%
Type of infertility
Distribution of age group among the Fertile controls (n=100)
Age (years) 30-35 36-40 41-45 46-50
Percentage (%) 21 43 28 8
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 98 University of Delhi, Delhi
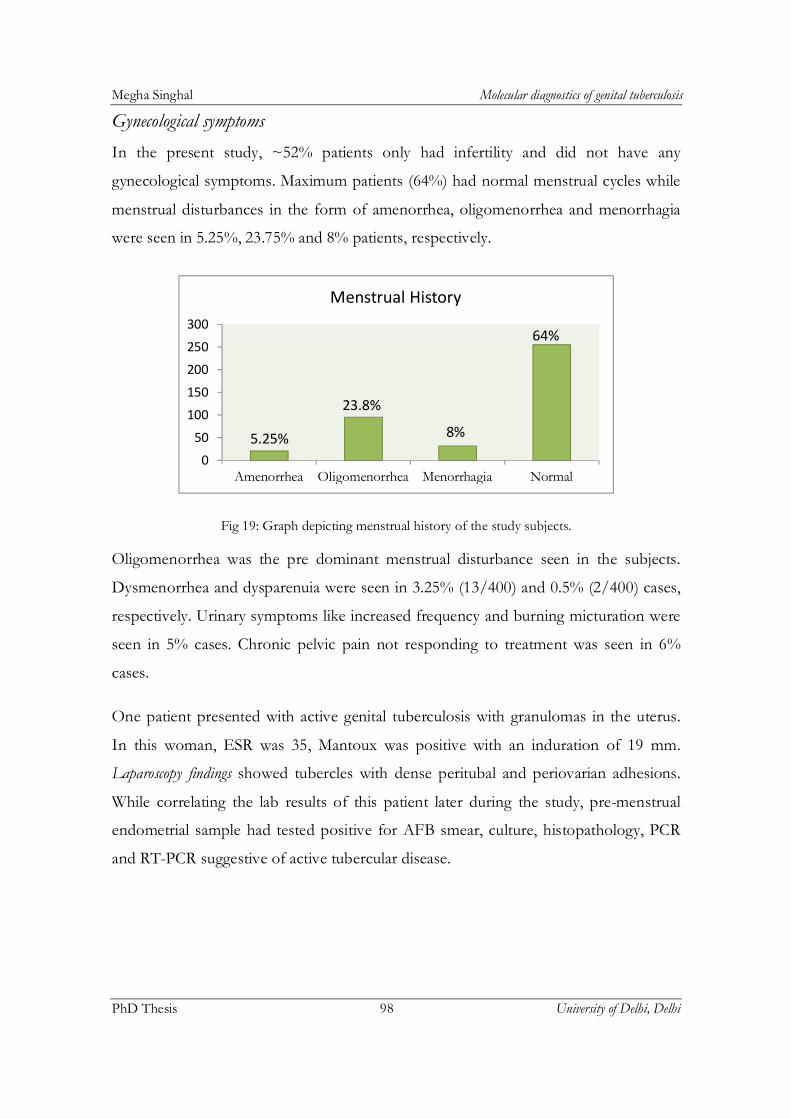
Gynecological symptoms
In the present study, ~52% patients only had infertility and did not have any
gynecological symptoms. Maximum patients (64%) had normal menstrual cycles while
menstrual disturbances in the form of amenorrhea, oligomenorrhea and menorrhagia
were seen in 5.25%, 23.75% and 8% patients, respectively.
Fig 19: Graph depicting menstrual history of the study subjects.
Oligomenorrhea was the pre dominant menstrual disturbance seen in the subjects.
Dysmenorrhea and dysparenuia were seen in 3.25% (13/400) and 0.5% (2/400) cases,
respectively. Urinary symptoms like increased frequency and burning micturation were
seen in 5% cases. Chronic pelvic pain not responding to treatment was seen in 6%
cases.
One patient presented with active genital tuberculosis with granulomas in the uterus.
In this woman, ESR was 35, Mantoux was positive with an induration of 19 mm.
Laparoscopy findings showed tubercles with dense peritubal and periovarian adhesions.
While correlating the lab results of this patient later during the study, pre-menstrual
endometrial sample had tested positive for AFB smear, culture, histopathology, PCR
and RT-PCR suggestive of active tubercular disease.
5.25%
23.8%
8%
64%
0
50
100
150
200
250
300
Amenorrhea Oligomenorrhea Menorrhagia Normal
Menstrual History

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 99 University of Delhi, Delhi
Table 21: Gynecological symptoms observed among 400 study subjects.
Symptoms Number % age
No symptom other than infertility 208 52%
Menstrual disturbance 146 36%
Dysmenorrhea 13 3.25%
Dysparenuia 3 0.75
Chronic pelvic pain 24 6%
Vaginal Discharge 32 8%
Urinary Symptom 20 5%
Previous history of tuberculosis
Nearly 30% (121/400) patients had a past history of tuberculosis. This included
patients affected with pulmonary as well as extra pulmonary cases (such as lymph
node, recurrent uveitis, cervical lymphadenopathy, abdominal, spine and bone
tuberculosis). All these patients adequately received anti-tubercular therapy (ATT) for 9
months to 1.5 years as per the Revised National Tuberculosis Control Programme
(RNTCP).
Among the patients with past history of tuberculosis, 18.2% (22/121) were found be
positive in DNA PCR, 14.8%, (18/121) had suggestive laparoscopic findings while
2.48% (3/121), 5.79% (7/121) and 1.65% (2/121) were positive in smear, culture and
histopathology respectively.
Fig 20: Pie chart showing the past history of tuberculosis among the patients.
Present30%
Absent70%
Past history of Tuberculosis

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 100 University of Delhi, Delhi
Table 22: Positivity by each parameter among the patients (121) with past history of tuberculosis.
AFB smear AFB culture HPE DNA PCR Laparoscopy
Positive 3 7 2 22 18
Negative 118 114 119 99 103
Findings of Mantoux and HIV Test Results
The total leucocyte count (TLC) ranged between 7-11 109/l and the differential
leucocyte count (DLC) was within normal limits for all the subjects including the cases
which tested positive for genital tuberculosis.
Mantoux test (Mx)
Result of Mantoux test was available on 336 study subjects. A positive tuberculin
induration was defined as induration size equal to or greater than 10 mm. In our study,
tuberculin >10 mm was seen 21.4% (72/336) subjects. Out of these 72 Mantoux
positive cases however, only 29 (40.2%) showed corroborative evidence of tuberculosis
from other tests of our study; whereas the remaining 43 cases were not positive in any
other test carried-out in this study.
HIV status
Tuberculosis and HIV have a synergistic relationship, as tuberculosis being an
opportunistic infection may suppress the immune status in AIDS patients. Therefore,
all subjects and their partners were tested for the presence of HIV infection; but all
were negative for HIV.
Findings of Chest X-ray
In the present study, chest radiography (poster anterior view) was done in 330 cases.
The findings were normal except in 7 cases with findings of opacified cavities,
heterogenous cavities and ill defined opacities suggesting healed lesions with fibrous
scars. As none of the cases had symptoms pertaining to respiratory system, sputum for
AFB was not done in these cases.

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 101 University of Delhi, Delhi
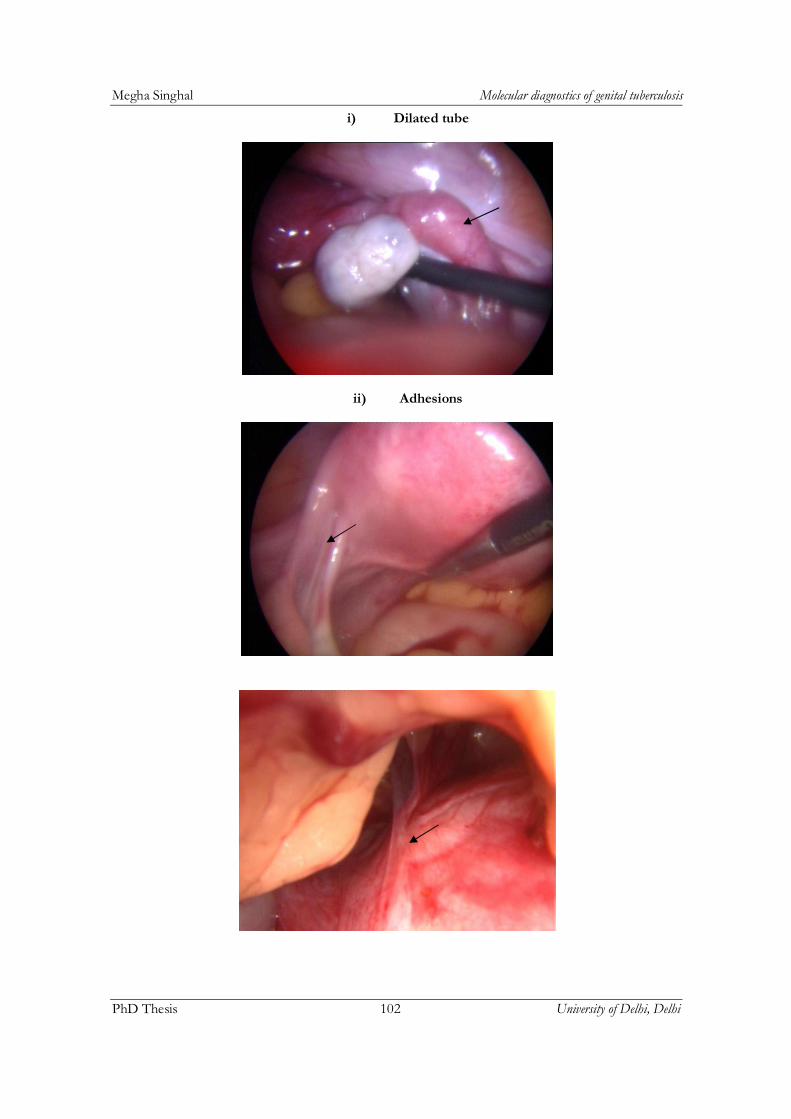
Findings of Laparoscopy
Results from diagnostic endoscopy (Laparoscopy) were obtained from all the subjects.
A systemic and thorough evaluation of pelvis and abdominal cavity was carried out for
evidence of TB and findings such as granulomas, caseation, calcification, tubercles and
loculated ascites were looked for. The fallopian tubes were also evaluated for the
presence of proximal and distal blocks and hydrosalpinx. Presence of adhesions was
also noted. Pelvis and peritoneal cavity were also evaluated for presence of other
pathology. Presence of fluid in Pouch of Douglas (POD) was also noted. Pelvic
pathology like fibroid uterus, endometriosis, and polycystic ovaries was seen as
incidental findings. Table 23 shows the laparoscopic findings among the study subjects.
The laparoscopic findings were subdivided into:
Group A: This group included findings suggestive of tuberculosis.
Suggestive findings, which included:
Affirmative findings (presence of tubercles, peritubal and/or periovarian
adhesions, tubo-ovarian mass, beaded tubes, cornual blockage)
Suspicious findings (hydrosalpinx, sacculated tubes, signs of chronic inflammation,
pelvic inflammatory disease, and mild adhesions)
*More than one positive finding (tubercle/adhesions/beaded tubes/blockage)
was considered as being suggestive for tuberculosis in laparoscopy.
Group B: This included findings other than tuberculosis or normal findings.
Normal findings: This included findings other than tuberculosis like normal pelvic
findings, endometriosis, fibroid uterus etc.
Suggestive of Tuberculosis: 38/400
- Affirmative: 26/38 - Suspicious: 12/38
Not suggestive: 362/400
Fig 21: Laparoscopic findings of the patients
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 102 University of Delhi, Delhi
i) Dilated tube
ii) Adhesions
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 103 University of Delhi, Delhi
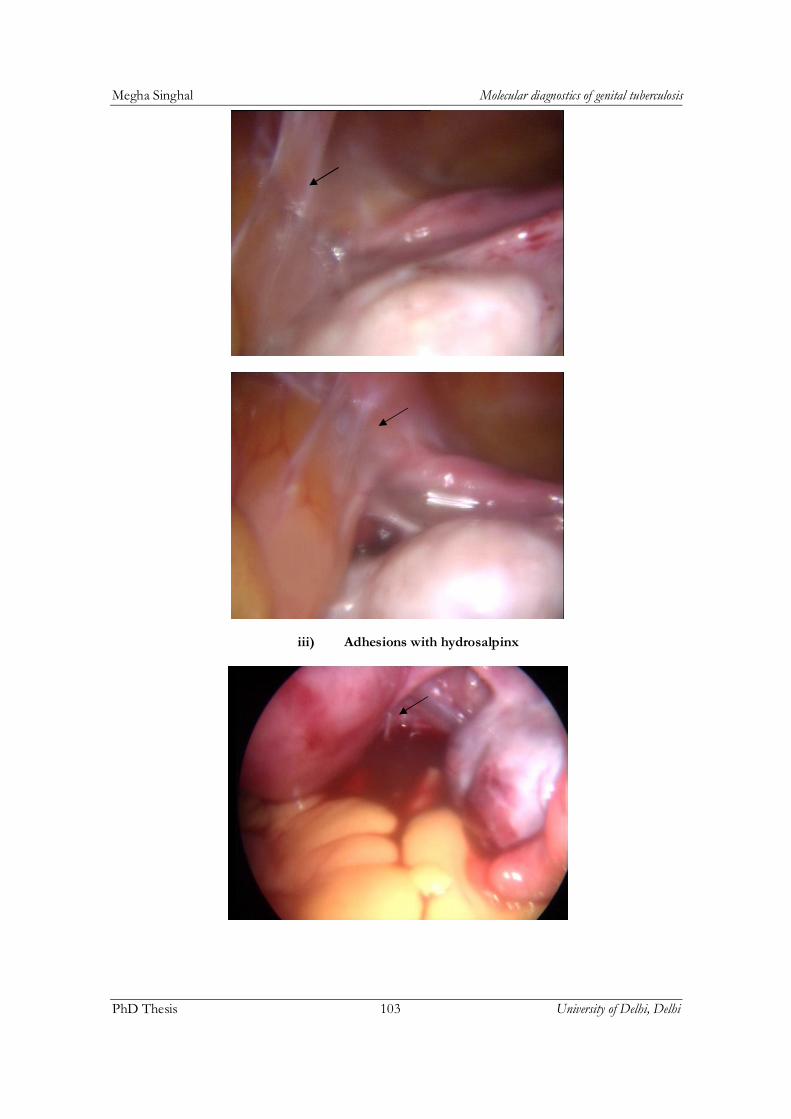
iii) Adhesions with hydrosalpinx
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 104 University of Delhi, Delhi
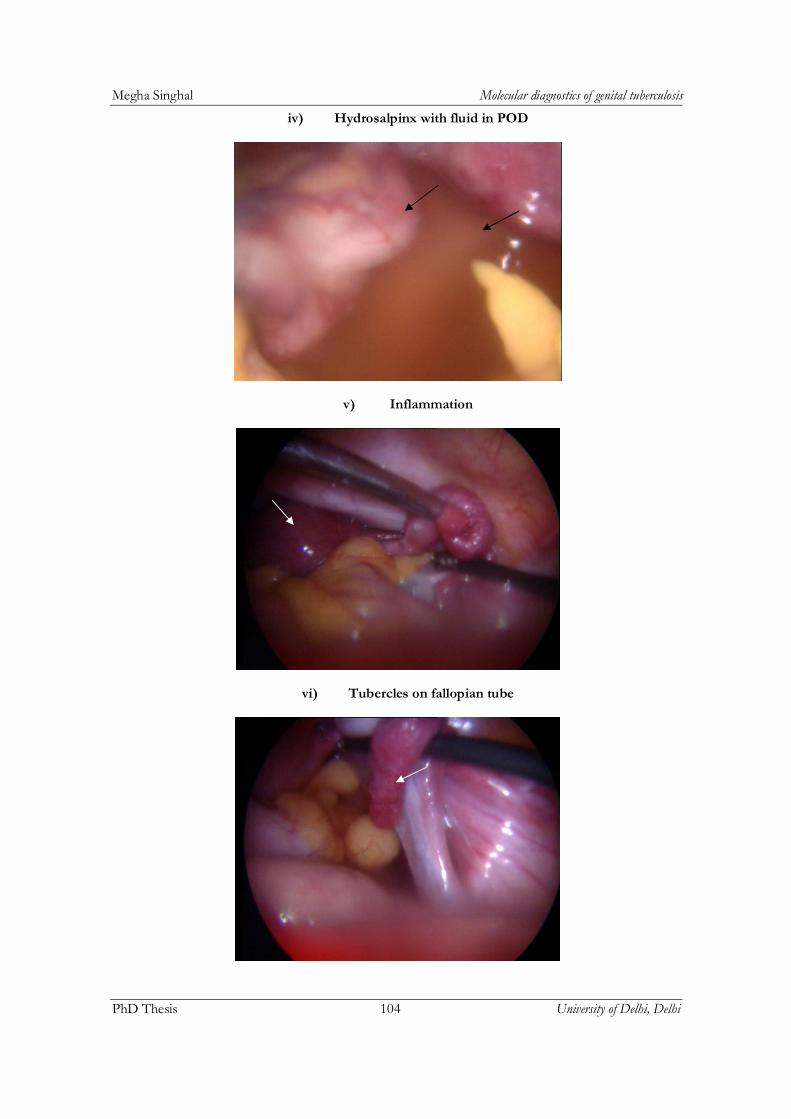
iv) Hydrosalpinx with fluid in POD
v) Inflammation
vi) Tubercles on fallopian tube

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 105 University of Delhi, Delhi
Table 23: Laparoscopy findings among study subjects
Laparoscopic findings No. of patients
Adhesions (Peritoneal/Pelvic/POD)
36
Beaded tube appearance 4 Tubo-ovarian mass 8 Tubal block (uni) 49 Tubal block (bi) 32
Tube absent 8 Hydrosalpinx 10 Frozen Pelvis 7 Tubercles 4 Fluid in POD 3 Caseous granuloma 5 Endometriosis 11 Calcification 1 PID 5
PCOS 21
While correlating the results, it was observed that all the 38 laparoscopy positives
were also DNA PCR positive during the present study.
Findings of Conventional Laboratory Tests
Findings of histopathological examination (HPE)
Pre-menstrual endometrial biopsy samples were taken and sent for histopathology.
Out of the 400 women, 1.25% (5/400) samples showed positive for tuberculosis. In
these cases, the histology showed sub epithelial tissue shows multiple caseating
granulomas with langerhans giant cells and diffuse and dense inflammatory infiltrate
comprising lymphocytes, plasma cells and neutrophils. The impression was said to be
as granulomatous highly suggestive of tuberculosis. Another 14 patients showed signs
of non tubercular endometritis (fig 23).
Secretory endometrium was seen in 81.2% (325/400) patients while proliferative
endometrium was seen in 13.2% (53/400) patients. Hyperplastic endometrium was
observed in 3 (0.75%) women (table 24). In one case which presented as active genital
tuberculosis, the histology showed tubercular salpingitis and clear evidence of
tuberculosis were also seen in laparoscopy. Among the patients in control group, no

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 106 University of Delhi, Delhi
sample was found to be positive for tuberculosis in histopathology. All patients
positive in histopathology were also positive in Laparoscopy and DNA PCR.
Fig 22: Histopathological findings among the infertile patients
Table 24: Various results in histopathology in the study group
Result of HPE Number Percentage
Study group (n=400) Tubercular endometritis Chronic endometritis Proliferative phase Secretory phase Hyperplastic endometrium Control group (n=100) Tubercular etiology
5 14 53 325 3 0
1.25% 3.5%
13.25% 81.2% 0.75%
0
Smear and Culture
Smears were prepared from all the study and control subjects and examined by Ziehl-
Neelsen method. Out of the 400 samples in the study group, AFB Smear detected
1.75% (7/400) cases. In the control group however, none of the samples was found to
be positive.
1.25% 3.5%
13.25%
81.20%
Histopathological findings
Tubercular endometritis
Chronic endometritis
Proliferative phase
Secretory phase

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 107 University of Delhi, Delhi
Fig 23: Results of AFB culture in the study group.
Culture by BACTEC 460 TB systems was done in all the samples. Since these extra
pulmonary samples are paucibacillary in nature their processing included milder
decontamination. The reading on the BACTEC machine was taken every alternate day.
Table 25: Positivity in AFB smear/culture among the study and control groups.
Endometrial biopsy Smear* %% tage Culture* % tage
Study subjects (n=400) 7 1.75% 11 2.75%
Controls (n=100) 0 0 0 0
*All AFB smear and culture positive were also positive in DNA PCR.
Culture for acid-fast bacilli using BACTEC 460 TB systems detected 2.75% (11/400)
cases (fig 23). The cultures were identified as positive within 12 days and were
identified as MTB on the basis of NAP test. Apart from this, 6 cultures got
contaminated. However none of the contaminated sample was positive in AFB smear
or PCR.
2.75%
95.75%
1.50%
Results of AFB culture in study group
Positive
Negative
Contaminated
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 108 University of Delhi, Delhi
Molecular Diagnostic Tests
Findings of Objective 1:
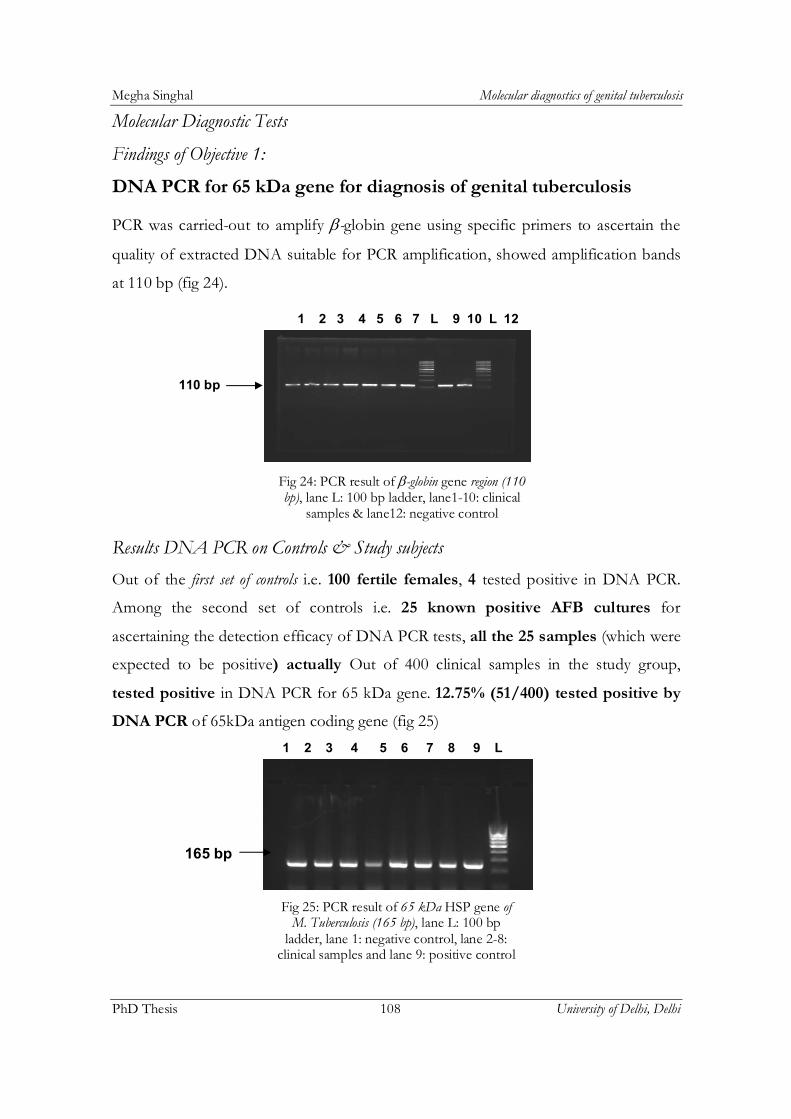
DNA PCR for 65 kDa gene for diagnosis of genital tuberculosis
PCR was carried-out to amplify -globin gene using specific primers to ascertain the
quality of extracted DNA suitable for PCR amplification, showed amplification bands
at 110 bp (fig 24).
Fig 24: PCR result of -globin gene region (110 bp), lane L: 100 bp ladder, lane1-10: clinical
samples & lane12: negative control
Results DNA PCR on Controls & Study subjects
Out of the first set of controls i.e. 100 fertile females, 4 tested positive in DNA PCR.
Among the second set of controls i.e. 25 known positive AFB cultures for
ascertaining the detection efficacy of DNA PCR tests, all the 25 samples (which were
expected to be positive) actually Out of 400 clinical samples in the study group,
tested positive in DNA PCR for 65 kDa gene. 12.75% (51/400) tested positive by
DNA PCR of 65kDa antigen coding gene (fig 25)
Fig 25: PCR result of 65 kDa HSP gene of M. Tuberculosis (165 bp), lane L: 100 bp
ladder, lane 1: negative control, lane 2-8: clinical samples and lane 9: positive control
1 2 3 4 5 6 7 L 9 10 L 12
110 bp
1 2 3 4 5 6 7 8 9 L
165 bp

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 109 University of Delhi, Delhi
Comparative analysis of DNA PCR result with Other tests and Laparoscopy
Comparative analysis of DNA PCR results with other tests is tabulated was carried out
with previous tests. The results are shown in table 26 and fig 26.
Table 26: Comparative analysis of DNA PCR with conventional tests and laparoscopy
Tests Histopath Smear Culture Laparo DNA PCR
Positivity
5/400 7/400 11/400 38*/400 51*^/400
*Of 38 laparoscopy positives, 4 which initially tested negative or doubtful in DNA PCR turned positive in repeat PCR after spiking; later confirmed with DNA sequence homology for 65 kDa gene. ^All these 51 PCR positive samples were confirmed to be true positives by gene sequence analysis of the PCR products.
Fig 26: Positivity by different parameters in the diagnosis of female genital tuberculosis.
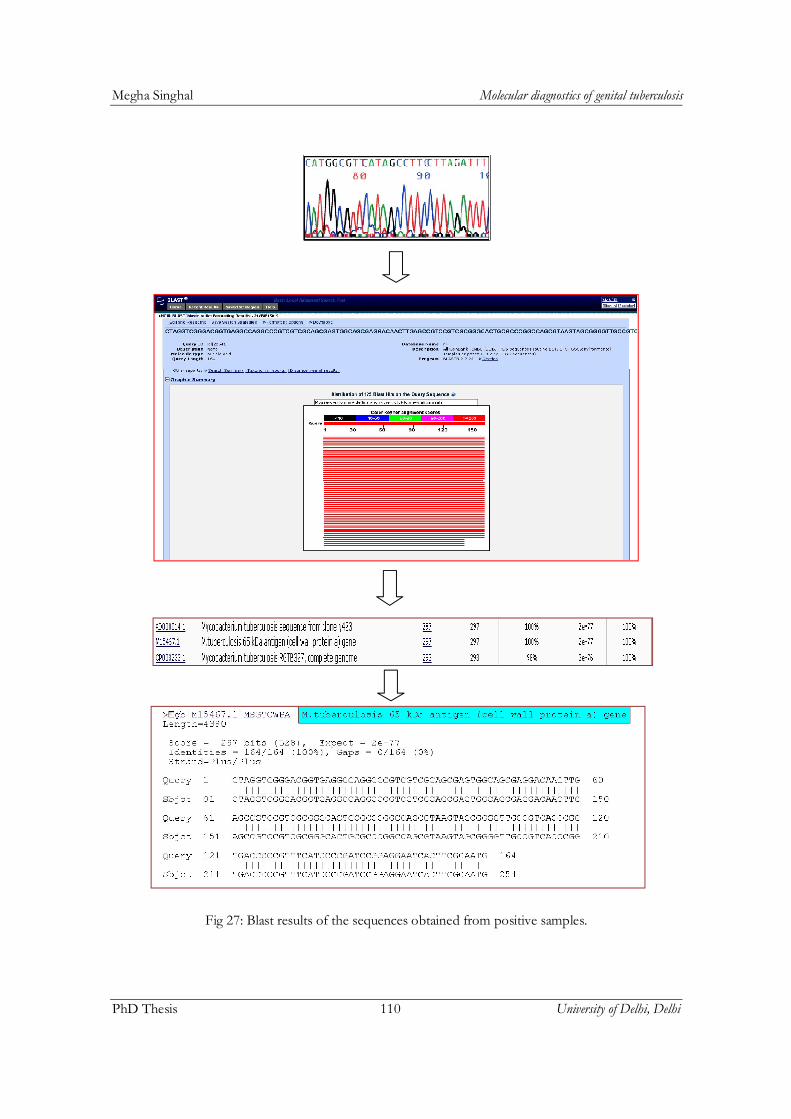
Confirmation of DNA PCR positivity by Gene sequencing/BLAST search
Gene signatures of 165 bp region of 65kDa gene of M. tuberculosis
The samples that tested positive for 65 kDa gene were analyzed by partial nucleotide
sequencing (fig 27). The sequences were subjected to BLAST search to confirm DNA
sequence homology with 65 kDa gene of M. tuberculosis. The blast results showed 100%
identity with the 65 kDa gene of M. tuberculosis suggesting it to be M. tuberculosis and
thus no false amplification was seen. Following is the 165 bp sequence of 65kDa gene
of M. tuberculosis.
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
AFB Smear AFB Culture Histopathology Laparoscopy DNA PCR
1.75%2.50%
1.25%
9.50%
12.75%
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 110 University of Delhi, Delhi
Fig 27: Blast results of the sequences obtained from positive samples.

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 111 University of Delhi, Delhi
> M.tuberculosis - 65 kDa antigen (cell wall protein a) gene
Homology of reference sequences of 65kDa gene with gene sequences of our study subjects. All the 51 DNA-positives had identical sequences.
Findings of Objective 2:
Utility of mRNA RT-PCR to detect active cases of genital TB
mRNA-based RT-PCR for detection of 85B antigen gene for viability of M. tuberculosis
Nested RT-PCR carried out to amplify 216 bp region of 85B antigen gene of M.
tuberculosis using specific primers. Gel picture of the standardized PCR is shown below
(fig 28):
Fig 28: Nested RT-PCR result of 85B antigen gene region (216 bp), lane L: 100 bp
ladder, lane 8: positive control, lane1-4,6,7: clinical samples and lane5: negative control
Out of the 51 DNA PCR positive patients in the study group, 31.3% (16/51) patients tested positive for mRNA-based RT-PCR.
1 2 3 4 5 6 7 8 L
216 bp
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 112 University of Delhi, Delhi
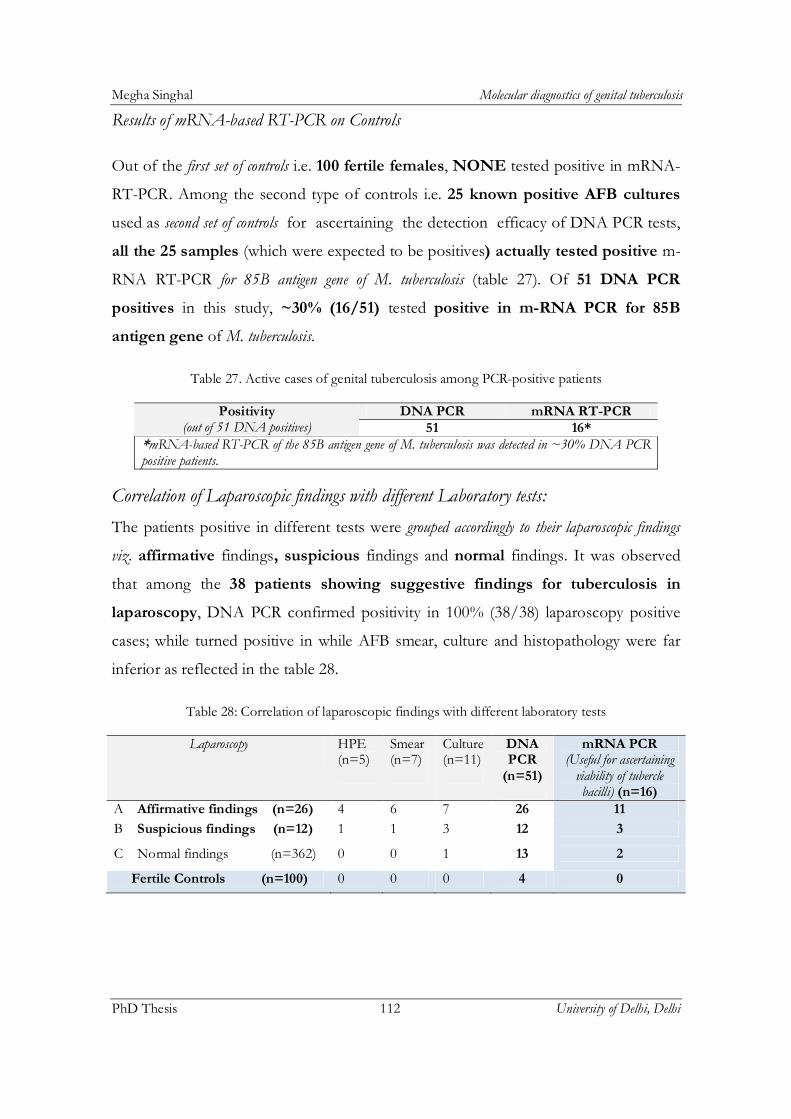
Results of mRNA-based RT-PCR on Controls
Out of the first set of controls i.e. 100 fertile females, NONE tested positive in mRNA-
RT-PCR. Among the second type of controls i.e. 25 known positive AFB cultures
used as second set of controls for ascertaining the detection efficacy of DNA PCR tests,
all the 25 samples (which were expected to be positives) actually tested positive m-
RNA RT-PCR for 85B antigen gene of M. tuberculosis (table 27). Of 51 DNA PCR
positives in this study, ~30% (16/51) tested positive in m-RNA PCR for 85B
antigen gene of M. tuberculosis.
Table 27. Active cases of genital tuberculosis among PCR-positive patients
Positivity (out of 51 DNA positives)
DNA PCR mRNA RT-PCR 51 16*
*mRNA-based RT-PCR of the 85B antigen gene of M. tuberculosis was detected in ~30% DNA PCR positive patients.
Correlation of Laparoscopic findings with different Laboratory tests:
The patients positive in different tests were grouped accordingly to their laparoscopic findings
viz. affirmative findings, suspicious findings and normal findings. It was observed
that among the 38 patients showing suggestive findings for tuberculosis in
laparoscopy, DNA PCR confirmed positivity in 100% (38/38) laparoscopy positive
cases; while turned positive in while AFB smear, culture and histopathology were far
inferior as reflected in the table 28.
Table 28: Correlation of laparoscopic findings with different laboratory tests
Laparoscopy HPE (n=5)
Smear (n=7)
Culture (n=11)
DNA PCR
(n=51)
mRNA PCR (Useful for ascertaining
viability of tubercle bacilli) (n=16)
A Affirmative findings (n=26) 4 6 7 26 11
B Suspicious findings (n=12) 1 1 3 12 3
C Normal findings (n=362) 0 0 1 13 2
Fertile Controls (n=100) 0 0 0 4 0

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 113 University of Delhi, Delhi
Confirmation mRNA results by gene sequencing of 216bp product of 85B antigen gene
The samples that tested positive by 85B antigen gene amplification were analyzed by
partial nucleotide sequencing. The results of sequencing were blasted onto the global
genome data bank (NCBI website) to confirm the presence of 85B antigen gene of M.
tuberculosis.
Blast search result of 216 bp sequence of 85B antigen gene of M. tuberculosis showing 100%
identity of our sequences with the 216 bp 85B antigen gene sequence of the standard M.
tuberculosis strain Rv1886c (gene) >Rv1886c, suggesting that our RT-PCR products were
true positives (fig 29).
Fig 29: Blast results of the sequences obtained from positive samples.
Homology of in-silico deduced amino acid reference sequences of 85B antigen gene of M. tuberculosis with amino acid sequences of our study subjects. All the 16 mRNA-positives had identical sequences.
Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 114 University of Delhi, Delhi
Sequence relatedness between the 85B antigen gene sequences from study subjects and controls
Fig 30: Sequence diversity between the study and control group.

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 115 University of Delhi, Delhi
Structure of the active site: 85B antigen gene
Using m-fold web server, the structure of active site was drawn out of the sequences
of 85B antigen gene from our study and control groups, but no difference was found in
the binding site; yet again confirming that our mRNA PCR positives were true
positives (fig 31).
dG= -79.64 [initially -89.30] dG= -82.36 [initially -88.40]
Fig 31. Structure of active site of 85B antigen gene from Study Subjects and AFB culture controls
Deduced amino acid sequence from our 85 B antigen gene sequence
ERMTTQDVEAITPQTLINIRPVVAAIKEFFGTSQLSQFMDQNNPLSGLTHKR
RLSALGPGGLSRERAGLEVRDVHPSHYGRMCPIETPEGPNIGLIGSLSVYARV
NPFRVHRNAVP
Findings of Taqman real-time PCR using our ‘self in-silico designed’ novel target for mRNA-based Taqman Real-time PCR for mRNA
A total of 19 out of 51 DNA confirmed positives (i.e. 37.25%) were positive in our
developed TaqMan assay as against only 16 detected by conventional RT-PCR for
mRNA of 85B antigen gene of M. tuberculosis to differentiate between active and latent

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 116 University of Delhi, Delhi
cases of genital tuberculosis. Real-time PCR was carried-out in the ABI 7900 HT
machine using the novel targets depicted in table 29. The amplification plot is shown in
fig 32.
Fig 32. TaqMan Real-time PCR standardized using novel target. It depicts one positive control, one negative control
along with two samples that tested positive for 146 bp region of 85B antigen gene of M. tuberculosis.
Table 29. Primers and probe along with annealing temperatures for novel targets
Name Sequence Position Orientation No. (nt) Anneal temp C 85B_F (primer)
GTTCGTAGCAGCAACCTGAA
817 forward 20 59.08
85B_R (primer)
GAACTCTGCAGGTCACCCTT
943 reverse 20 59.3
Probe CCAGGATGCGTACAACGCCG
840 forward 20 69.06

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 117 University of Delhi, Delhi
Comparative efficacy of Conventional RT-PCR vs Novel Real-time RT-PCR:
Table 30 compares the detection rates by conventional RT-PCR and novel real-time PCR.
Table 30: Detection rates by conventional RT-PCR and novel real-time PCR
By conventional RT-PCR 16/51 DNA PCR positives
By Novel TaqMan Real-time PCR 19*/51 DNA PCR positives
*The three extra positives detected by real-time PCR could not be confirmed through sequence analysis. Hence it is only indicative of the marginal superiority of the technique.
Findings of Objective 3:
Findings on drug-resistance genes (rpo B, kat G and inh A)
Detection of rpo B, kat G and inh A genes in 51 DNA PCR-positive infertile females
For mutation analysis, DNA from all 51 samples was subjected to amplification of
partial region of rpoB, katG and inhA genes associated with multidrug resistance. Table
31 shows the primer sequences used for the multidrug resistant genes along with their
annealing temperature, nucleotide position and amplicon size (bp). Primer sequences
and corresponding Gel pictures of PCR amplification of 350 bp rpoB, 620 bp katG and
248 bp inhA genes are shown in figures 33, 34 and 35:
Table 31: Primer sequences used for the multidrug resistant genes along with their annealing temperature, nucleotide position and amplicon size (bp)
Gene Sequence Anneal temp C Position(nt) Amplicon size
rpoB
F- GGGAGCGGATGACCACCC 60 2266 350 bp R- GCGGTACGGCGTTTCGATGAAC
2615
katG F- AGCTCGTATGGCACCGGAAC 60 904 620 bp
R- TTGACCTCCCACCCGACTTG 1523 inhA F- CCTCGCTGCCCAGAAAGGGA 45 Upstream
of inhA gene 248 bp
R- ATC CCC CGG TTT CCT CCG GT

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 118 University of Delhi, Delhi
Fig 33: PCR result of rpoB gene region (350 bp), lane L: 100bp ladder, lane 3:
negative control, lane 1, 2 and 4: clinical samples
Fig 34: PCR result of katG gene region (620 bp), lane L: 100bp ladder, lane 2-
6: clinical samples
Fig 35: PCR result of inhA gene region (248 bp), lane L: 100bp ladder, lane 3:
negative control, lane 1, 2 and 4: clinical samples
Analysis of DNA sequences to unveil new mutation(s), if any in the rpo B, kat G and inh A genes from 51 DNA PCR-positive cases for drug resistance to Rifampicin & Isoniazid
Sequencing was carried-our as per the protocol mentioned earlier for sequencing of
DNA PCR positive amplicons. The sequences were subjected to BLAST search base
(NCBI website); and subsequent mutation analysis by comparison with the previously
reported sequences.
350 bp
1 2 3 L 4
L 2 3 4 5 6
248 bp
1 2 3 4 L
620 bp

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 119 University of Delhi, Delhi
Gene signatures of 350 bp region of rpoB gene
Samples that amplified the 350 bp, 620 bp and 248 bp region of rpoB, katG and inhA
genes were analyzed by partial nucleotide sequencing. The results of sequencing were
blasted onto the global genome data bank (NCBI website) to search for the reference
sequence of M. tuberculosis.
After the blast results, reference sequence was selected and mutation analysis was
carried out using various softwares like Mega v4.1, BioEdit v7.0.5.3 and SeqScape® v2.7
(Applied Biosystems). All the sequences were submitted to global NCBI GenBank.
BLAST search results:
The following figure shows the blast results obtained for positive samples (fig 36).
Fig 36: Blast results of the sequences obtained from positive samples.

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 120 University of Delhi, Delhi
Mutation analysis of drug resistance genes in DNA PCR positives
Mutation analysis was carried out in the drug resistance genes. The drug resistance
analysis results for rpoB gene are shown in table 32. Figure 37 depicts the point of
mutation on the rifampicin resistance determining region (RRDR).
Fig 37: Rifampicin resistance determining region (RRDR) showing mutations at two codon positions
Table 32: Mutations in the rpoB gene
Codon no. Mutation Position of Mutation
516 GACTAC (AspTyr) T replaces G at first position
531 TCGTTG (SerPhe) T replaces C at first position
TCGTGG (SerTrp) G replaces at second position
572 ATCTTC (IlePhe) T replaces A at first position
584 TTCTTT C (PhePhe) Insertion of T at the third position
Accession no.: JF268583 to JF268611 (NCBI, Gene Bank)
Fig 38: Multiple Sequence alignment depicting mutations in rpoB gene

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 121 University of Delhi, Delhi
Fig: 39: Amino acid alignment of the partial region of rpoB gene of M. tuberculosis depicting differences in amino acid at various positions.

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 122 University of Delhi, Delhi
Mutations in the katG gene
Only 2 mutations at codon position 315 and 463 already reported previously in other
forms of tuberculosis were also found in the amplicon sequences of katG gene from
our study subjects.
Table 33: Mutations in the katG gene of M. tuberculosis.
Codon no. Mutation Position of Mutation 315 AGCACC (Ser315Thr) C replaces G at second position
463 CGGCTG (Arg463Leu) T replaces G at second position
*Codon 463 is a polymorphic site. This substitution was seen in almost all samples. It has been shown to be associated not with resistance but with evolutionary genetics.
Mutations in the inh A gene
No mutation was seen in the promoter region of inhA gene of M. tuberculosis.
Profile of 51 DNA PCR confirmed cases of genital tuberculosis of our study
After compiling the results from various tests, it was found that a total of 51 samples
tested positive for genital tuberculosis by various parameters. The clinical profile of the
positive patients is shown in table 34:
Table 34: Showing profile of 51 DNA PCR confirmed cases of genital tuberculosis of our study
Age (years)
18-25 26-30 31-35 36-40
12 22 14 3
Type of Infertility
Primary (1) Secondary (2)
35 16
History of TB
Present Absent
22 29
Menstrual History
Amenorrhea Oligomenorrhea Menorrhagia Normal
2 21 4 24

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 123 University of Delhi, Delhi
Comparison of results between female genital TB positive and negative patients
Various parameters were compared between genital TB positive and negative patients.
Oligomennorhea was found to have a significant correlation between the two groups.
Table 35 shows the comparison of various characteristics between the two groups.
Table 35. Clinical characteristics of positive and negative patients.
Clinical feature Positive patients (%) Negative patients (%) p-value
Amenorrhea 3.9 5.4 0.6448
Oligomenorrhea 41.2 21.2 0.0017
Menorrhagia 7.8 8.02 0.9647
1 infertility 68.6 68.6 0.9838
H/O TB 43.1 28.4 0.319
Comparison of results between mRNA-positive and mRNA-negative patients
Comparison of various clinical characteristics between the patients who were DNA
positive-mRNA positive and those who were DNA positive-mRNA negative did
not reveal any significant difference in any parameter between the two groups (table
36).
Table 36: Comparison of clinical features between mRNA-positive & negative patients
Clinical Features mRNA-positive patients (16/51)
mRNA-negative patients (35/51)
p-value
Amenorrhea 0 2 0.329
Oligomenorrhea 4 10 0.79
Menorrhagia 2 3 0.661
1 infertility 27 8 0.052
H/o TB 9 13 0.201

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 124 University of Delhi, Delhi
Profile of 13 FGTB positive-laparoscopy negative patients
The clinical features of 13 female genital tuberculosis positive-laparoscopy negative
patients were analyzed. They are presented in table 37.
Table 37: Profile of 13 FGTB positive-laparoscopy negative patients
Parameter Findings
Type of infertility Seven (53.8%) patients had 1 infertility while six (46.1%) had
2 infertility.
Menstrual cycle 23.07% had Oligomenorrhea, 7.7% had Menorrhagia while 61.5% had normal cycles
H/o TB Three patients (30.7%) had a previous history of TB (pulmonary and abdominal tuberculosis).
Smear and Histopathology None of the patients were positive by smear and histopathology
Culture One patient (7.7%) had a positive culture
mRNA -based RT-PCR Two patients (15.3%) had a positive RT-PCR
Follow-up of Study Subjects and Pregnancy Outcome
Among the 400 subjects, a total of 51 subjects tested positive for M. tuberculosis by
different parameters. All the subjects were put on anti-tubercular therapy using the
standard regimen. Patients with multidrug resistant endometrial tuberculosis were put
on second line anti-tubercular drug regimen as per the revised tuberculosis control
program for multidrug-resistant tuberculosis.
Table 38: Showing the number of patients who conceived after treatment.
Number of patients put on ATT as per Laparoscopy and/or DNA PCR results of this study
Conceived=7
Not conceived even after treatment=6
Still under treatment
Lost interest
Lost to follow-up
IUI IVF Spontaneous IUI IVF
3 1 3 4 2 19 12 7

Megha Singhal Molecular diagnostics of genital tuberculosis
PhD Thesis 125 University of Delhi, Delhi
Seven (7/51; 13.72%) patients conceived post-ATT. These included one patient from
group A with positive DNA-PCR and RT-PCR; one patient from group B, with a
positive DNA-PCR and culture and five patients from group C, all with positive
DNA-PCR, one of which had a positive RT-PCR (table 38).