review - blood transfusion · review. blood transfus 2016; 14: ... is a rare bleeding disorder...
TRANSCRIPT

© SIMTI S
ervizi
Srl
255
Review
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15© SIMTI Servizi Srl
The anti-CD20 monoclonal antibody rituximab to treat acquired haemophilia A
Giovanni D'Arena1, Elvira Grandone2, Matteo N.D. Di Minno3,4, Pellegrino Musto5, Giovanni Di Minno3
1Haematology and Stem Cell Transplantation Unit, IRCCS Cancer Referral Centre of Basilicata, Rionero in Vulture; 2Haemostasis and Thrombosis Unit, IRCCS "Casa Sollievo della Sofferenza" Hospital, San Giovanni Rotondo; 3Department of Clinical Medicine and Surgery, Regional Reference Centre for Coagulation Disorders, Federico II University, Naples; 4Unit of Cell and Molecular Biology in Cardiovascular Diseases. Monzino Cardiology Centre, IRCCS, Milan; 5Scientific Direction, IRCCS Cancer Referral Centre of Basilicata, Rionero in Vulture, Italy
Background. Acquired haemophilia A (AHA) is a rare bleeding disorder caused by the development of specific autoantibodies against naturally occurring factor VIII (FVIII). Although about half of cases are idiopathic, AHA may be associated with several non-neoplastic conditions, autoimmune disorders, as well as haematological malignancies, such as chronic lymphocytic leukaemia and lymphoma. The long-term suppression of inhibitors is one of the mainstays of the treatment of AHA. Apart from standard immunosuppressive treatments, rituximab has been proven to be effective in AHA.
Materials and methods. The aim of this review is to provide a systematic description of data available in the literature on this topic. To do so, we performed a search using the indexed online database Medline/PubMed, without temporal limits, matching the words "rituximab" and "acquired h(a)emophilia". Furthermore, additional published studies were identified in the reference list of the publications found in PubMed.
Results. The review of the literature confirms that rituximab may be a safe and useful treatment for AHA.
Discussion. Although rituximab is not a standard therapy for AHA, it may be useful in resistant cases. However, the definitive place of this monoclonal antibody in the therapeutic strategy for AHA (first or second-line, alone or in combination with other drugs) remains to be determined more precisely and warrants further investigation.
Keywords: acquired haemophilia, inhibitors, rituximab, cancer, B-cell malignancies.
IntroductionRituximab, a chimeric human/murine monoclonal
antibody targeting the CD20 antigen on the surface of B cells, is used extensively to treat CD20-positive haematological cancers and is now being increasingly employed to treat several autoimmune disorders1. Acquired haemophilia A (AHA) is a rare bleeding disorder caused by the development of specific autoantibodies (inhibitors) against naturally occurring factor VIII (FVIII)2.
The treatment of AHA is focused on the need to stop potentially life-threatening bleeding and to gain a long-term suppression of the inhibitors3. In detail, the inhibitors are usually eradicated by standard immunosuppressive treatments, such as steroids and cyclophosphamide. More recently, rituximab has also been used, generally as second-line treatment4.
The first experiences with rituximab in AHA were described in 2001 and several patients have been treated with this specific approach since then5. The aim of this
review is to provide a systematic description of data available in the literature on this topic. To do so, we searched the indexed online database Medline/PubMed, without temporal limits, matching the words "rituximab" and "acquired h(a)emophilia". Additional published studies were identified in the reference lists of the publications found in PubMed.
Incidence and pathogenesis of acquired haemophilia A
AHA is a rare bleeding disorder. First described in 19406, it is due to the development of autoantibodies against FVIII. The incidence of AHA has been estimated to be 0.2-1.0 cases per million population per year, although it is probably higher because not all affected patients are reported7. The median age of patients at presentation is 60 to 70 years and the condition occurs with similar frequency in males and females. However, females are younger than males, probably because of the risk of post-partum inhibitors.
All rights reserved - For personal use only No other use without premission

© SIMTI S
ervizi
Srl
256
D'Arena G et al
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
Bleeding manifestations are often severe and may occur spontaneously or after minor trauma. In addition, patients usually experience soft tissue bleeding other than haemarthroses, which are more commonly seen in the congenital form of haemophilia.
Although the development of inhibitors is idiopathic in approximately half of patients, various conditions associated with FVIII inhibitor development, including connective tissue and inflammatory bowel diseases, puerperium, malignancies, and dermatological disorders, are currently known. In this setting, the database of the European Acquired Haemophilia (EACH2) registry, which has collected data on 501 patients from 117 centres in 13 European countries, showed that among the 482 patients who bled (96.2% of all registered patients), the underlying medical condition was as follows: autoimmune disorder (14.1%), malignancy (11.5%), pregnancy (8.9%), drug-induced (3.3%), transfusion, dermatological, infection, monoclonal gammopathy of undetermined significance or others (7.8%)8. No associated medical condition was identified (the so-called idiopathic forms) in 54.4%, while no information was reported for 22 patients (4.6%) (Figure 1).
Acquired haemophilia A associated with haematological malignancies
Autoimmune phenomena may complicate the clinical course of several haematological malignancies, in particular B-cell lymphoproliferative disorders9.
The association of AHA with several haematological cancers has been reported and was first reviewed by Sperr et al.10 More recently, Franchini et al. showed that lymphoproliferative neoplasms, such as chronic lymphocytic leukaemia and lymphomas, are the blood malignancies most frequently associated with AHA (70% of cases). Moreover, muco-cutaneous haemorrhages were the most frequently observed type of bleeding (63% of cases)11 (Figure 2). The relationship between inhibitor production and the underlying haematological disease was demonstrated by the disappearance of the inhibitor when cancer treatment was given successfully. Sallah et al. proposed different pathogenic mechanisms explaining this association: alterations of the FVIII molecule, disturbances in the antigen-presenting cell process and alterations in the function/interaction of B and T cells12.
Finally, immunomodulatory drugs, such as fludarabine and interferon, have been reported to be associated with the appearance of FVIII inhibitors, probably due to the immune disturbance caused by these agents in patients with a disease involving the immune system11.
Figure 1 - Medical conditions that can underlie AHA. Data are expressed as percentages from 482 bleeding
patients from 117 centres in 13 European countries, according to the database of the EACH2 registry8. "Others" means: transfusion, dermatological conditions, infection, monoclonal gammopathy of undetermined significance or other medical conditions.
AHA: acquired haemophilia A.
Figure 2 - Haematological malignancies that can underlie acquired haemophilia A (AHA).
Data are expressed as percentages from 30 patients with AHA and haematological malignancies, according to the review of Franchini et al.11
CML: chronic myeloid leukaemia; MF: idiopathic myelofibrosis; CLL: chronic lymphocytic leukaemia; WM: Waldenstrom's macroglobulinaemia; AML: acute myeloid leukaemia; MM: multiple myeloma; MDS: myelodysplatic syndromes.
All rights reserved - For personal use only No other use without premission

© SIMTI S
ervizi
Srl
257
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
Rituximab to treat acquired haemophilia A
Diagnosis and managementThe presence of FVIII inhibitors must be suspected
when an unexplained prolongation of the activated partial thromboplastin time (aPTT) is not corrected by the in vitro addition of normal plasma (mixing test). Several other conditions may cause prolongation of the aPTT: lupus anticoagulant, heparins and other anticoagulants (i.e., vitamin K antagonists and direct oral anticoagulants) and acquired von Willebrand syndrome. For this reason, these conditions must be ruled out. In AHA the FVIII level is reduced, although rarely to less than 2%, and the Bethesda assay demonstrates the presence of an inhibitor. Table I summarises the differential diagnosis of a prolonged aPTT. The diagnostic work-up of AHA was recently reviewed by Tiede et al.13 Finally, an underlying concomitant disorder triggering AHA should be searched for and, if found, removed with appropriate therapeutic measures.
The treatment of AHA is aimed at immediate stopping the acute bleeding and long-term suppression of the inhibitor. In general, bypassing inhibitor agents, such as the recombinant activated FVII (rFVIIa) and activated prothrombin complex concentrate (APCC), are used to control the bleeding. Human FVIII concentrate, recombinant porcine FVIII concentrate and desmopressin are also employed. Furthermore, immunosuppression is required to eradicate the inhibitor. Glucocorticoids combined with cyclophosphamide are frequently given. This approach is able to eradicate inhibitors in approximately 70% of patients with AHA3.
As showed by a very recent report published by Tiede et al., predictors of a positive response are a low inhibitor level and a short interval between the appearance of the inhibitor and the start of therapy14. Moreover, FVIII ≥1 IU/dL and inhibitor level <20 Bestheda units (BU)/mL were independent predictors of overall survival and define a subgroup of patients with better prognosis.
Rituximab to eradicate inhibitorsThe monoclonal antibody rituximab, a chimeric
antibody targeting CD20 antigen on B-cell surface15,
was first reported to be effective in eradicating the inhibitors in AHA in 20014. To date, 160 patients with this condition treated with rituximab have been described16-49. Published studies, including several cases reported only in abstract form, describing the use of rituximab in acquired haemophilia have been previously reviewed by Barcellini and Franchini5,7,11 and are updated in the present review.
As shown in Table II, rituximab has been used alone or in combination with other immunosuppressive drugs, such as steroids and cyclophosphamide, as salvage or first line-therapy. Overall, a high rate of response was observed, with 123 patients (77%) achieving complete response. A complete response is usually defined as normalisation of the FVIII level and an inhibitor that is no longer detectable or <1 BU, while a partial response is defined as a >50% decrease in inhibitor titre, a FVIII level >25% and no further bleeding5. However, it should be noted that the criteria for complete or partial response are not identical in all reports. This may explain why the response rate was quite high in this review compared to other studies45 in which more stringent response criteria were used. In addition, several cases were reported only as case reports with a tendency to describe only responding patients. Consequently, the outcome data should be evaluated with caution.
The dose of rituximab infused in almost all cases was 375 mg/m2, the standard dose used in the treatment of lymphoma. However, a lower dose (100 mg) has also been used16. The number of courses of rituximab was very variable, ranging from a single, low dose to 12 standard doses. The time to response was also heterogeneous, ranging from 1 week to more than 1 year. Re-treatment with rituximab was generally effective. Overall, the administration of rituximab in AHA was well tolerated with very few early or late side effects of the infusion; no infectious complications have been reported so far.
In eight patients with AHA treated with rituximab, Aggarwal et al.17 found that the best results to standard treatments were achieved in cases with low inhibitor
Table I - Differential diagnosis of a prolonged aPTT.
aPTT PT Thrombin time Fibrinogen levels Platelet count
Acquired haemophilia ↑ N↓ N N N
FVIII, FIX, FXI, FXII deficiency ↑ N N N N
Heparin therapy ↑ N ↑ N N
Fibrinolytic treatment ↑ ↓ ↑ ↓ N
DIC ↑ ↑ ↑ ↓ ↓
von Willebrand's disease N/↑ N N N N
Acquired von Willebrand's disease ↑ N N N N
aPTT: activated partial thromboplastin time; PT: prothrombin time; N: normal; FVIII: factor VIII; FIX: factor IX; FXI: factor XI; FXII: factor XII; DIC: disseminated intravascular coagulation.
All rights reserved - For personal use only No other use without premission

© SIMTI S
ervizi
Srl
258
D'Arena G et al
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
Table II - Updated results of the published studies on rituximab treatment of idiopathic and secondary AHA.
References N. of patients treated
Age (years)
Sex (M/F)
N. of rituximab doses
to maximum benefit
Response to rituximab
Time to the bestresponse (week)
Duration of response(months)
Karwal et al.4 3 73-79 1/2 4 1 CR, 1 PR, 1 No R 8-56 3+ to 6+
Tamponi et al.5,7,11 2 41, 72 1/1 1-4 2 CR 4 NR
Wiestner et al.22 4 38-79 3/1 2-4 4 CR 3-12 36+ to 38+
Kain et al.23 1 28 1/0 4 1 CR 12 7+
Marietta et al.24 1 71 0/4 2 1 PR 17 1
Fisher et al.25 1 71 1/0 2 No R - -
Jy et al.26 1 81 0/1 4 1 PR 2 6
Low et al.5,7,11 1 32 0/1 11 1 CR 106 11
Mazj et al.5,7,11 4 24-70 1/3 2-4 4 CR 2-3 1-12
Stasi et al.27 10 27-78 5/5 4 8 CR, 2 PR 3-12 2-42
Grimley et al.5,7,11 2 31, 83 0/2 4 2 CR 16, 20 3, 4
Riess5,7,11 2 60, 72 2/2 4 2 CR 4, 8 14, 24
Krause et al.5,7,11 4 70-81 2/2 4 4 CR 4-32 NA
Aggarwal et al.17 4 60-81 2/2 4-8 3 CR, 1 PR 2 -35 3-10
Abdallah et al.28 2 47, 80 0/2 4 2 CR 10, 65 18, 30
Herman et al.29 1 53 1/0 8 1CR 22 NA
Holme et al.30 2 64, 94 1/1 4 1CR 13 NA
Maruscak et al.5,7,11 1 59 1/0 4 1 CR 4 21
Hut-Kuhne et al.5,7,11 2 47, 70 0/2 4 2 CR 4, 15 NA
Malato et al.5,7,11 1 NR NR 4 1 CR 32 8
Maillard et al.31 1 18 0/1 4 1 CR 48 12
Clatworthy & Jayne 32 1 48 1/0 2 1 CR 1 3
Berezné et al.33 2 74, 81 2/0 4 2 CR 38, 43 9, 10
Onitilo et al.34 6 24-76 2 /4 3-9 6 CR 1-52 4-36
Teitel5,7,11 1 18 0/1 4 1 CR 12 NA
Theodossiades et al.5,7,11 1 66 0/1 4 1 CR 12 NA
Oliveira et al.35 1 61 0/1 4 1 CR 2 12
Field et al.5,7,11 4 40-71 1/3 4 4 PR 6-11 5-14
Santoro et al.5,7,11 1 25 0/1 4 1 CR 39 29
Alvarado et al.36 2 61, 73 0/1 4 2 CR 6-35 3, 24
Millet et al.37 2 30, 68 0/2 4 2 CR 12, 16 12, 32
Machado et al.38 2 40, 59 1/1 12, 4 2 CR 12, 4 20, 24
Cretel et al.39 1 88 0/1 4 1 CR 7 18
Dedeken et al.40 3 25-56 0/3 1-4 3 CR 2-3 8-24
Ichikawa et al.41 1 63 0/1 4 1 CR 8 6
Wermke et al.16 1 66 1/0 1 (low dose) 1 CR 3 10
Braunert et al.5,7,11 1 76 1/0 4 1 CR NA 6
Boles et al.42 15 19-81 8/7 4 14 CR, 1 PR 4-83 2-60
Singh et al.43 8 39-88 2/6 4-6 7 CR 4-40 6-82
Collins et al.44 51 5-78 30/ 21 4 31 CR 4-21 NR
Imashuku et al.45 1 80 1/0 4 1 CR 6 5
Conte et al.46 1 54 1/0 4 1 CR 20 67+
de Palencia Espinosa et al.47 1 63 1/0 4 1 CR 8 12+
Daikeler et al.48 2 NR NR NR 1 CR, 1 No R NR NR
D'Arena et al.49 1 60 1/0 8 1 CR 6 12
AHA: acquired haemophilia A; CR: complete remission; PR: partial remission; No R: no response; NR: not reported; NA: not applicable.
All rights reserved - For personal use only No other use without premission
© SIMTI S
ervizi
Srl
259
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
Rituximab to treat acquired haemophilia A
titres, while patients with high titres had a good response to rituximab. In light of this, Aggarwal et al. proposed an algorithm for the treatment of AHA on the basis of which, patients with a low inhibition titres (<5 BU/mL) and minimal bleeding should be treated only with prednisone, while patients with higher inhibitor titres should also receive rituximab (if titre <30 BU/mL or there is serious bleeding) or rituximab plus cyclophosphamide (if titre ≥30 BU/mL).
Subsequently, Collins et al. reported on 15 patients with AHA identified in 23 Haemophilia Centres in the United Kingdom and reported an overall response to rituximab in 47% of patients, despite only 14% of them obtaining a durable response18. None of the three patients treated with rituximab without adding FVIII responded. The same authors performed a systematic review of the literature and found 28 additional cases treated with rituximab. Inhibitor negativity was achieved in a higher number of patients (56%) than those reported in the English study, while the proportion of patients with a sustained response was similar. Finally, these authors suggested that rituximab combined with FVIII is potentially useful in haemophilia patients with inhibitors resistant to standard immunosuppressive therapy.
Franchini et al. performed a systematic review and a meta-analysis including 49 cases of AHA in which a durable complete remission (i.e., no inhibitor recurrence during follow-up) was obtained in 53% of the patients treated with rituximab19. On the basis of a multivariate analysis, rituximab appeared to be more effective in mild-to-moderate disease than in severe disease and when concomitantly administered
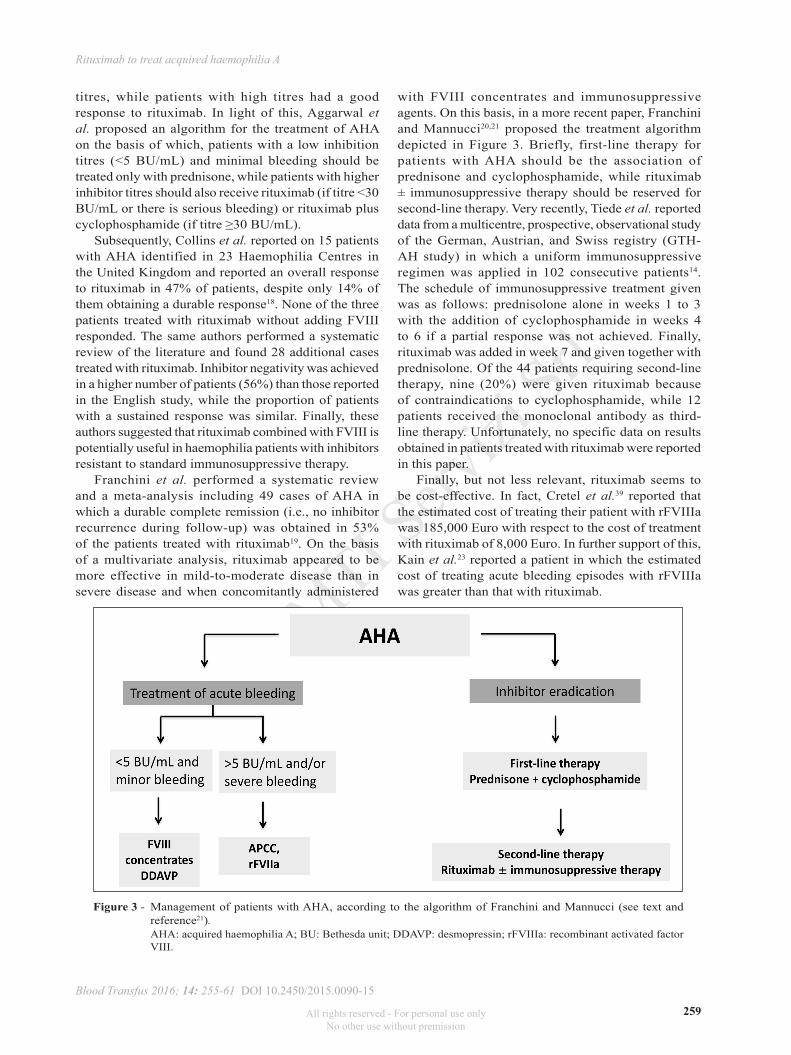
with FVIII concentrates and immunosuppressive agents. On this basis, in a more recent paper, Franchini and Mannucci20,21 proposed the treatment algorithm depicted in Figure 3. Briefly, first-line therapy for patients with AHA should be the association of prednisone and cyclophosphamide, while rituximab ± immunosuppressive therapy should be reserved for second-line therapy. Very recently, Tiede et al. reported data from a multicentre, prospective, observational study of the German, Austrian, and Swiss registry (GTH-AH study) in which a uniform immunosuppressive regimen was applied in 102 consecutive patients14. The schedule of immunosuppressive treatment given was as follows: prednisolone alone in weeks 1 to 3 with the addition of cyclophosphamide in weeks 4 to 6 if a partial response was not achieved. Finally, rituximab was added in week 7 and given together with prednisolone. Of the 44 patients requiring second-line therapy, nine (20%) were given rituximab because of contraindications to cyclophosphamide, while 12 patients received the monoclonal antibody as third-line therapy. Unfortunately, no specific data on results obtained in patients treated with rituximab were reported in this paper.
Finally, but not less relevant, rituximab seems to be cost-effective. In fact, Cretel et al.39 reported that the estimated cost of treating their patient with rFVIIIa was 185,000 Euro with respect to the cost of treatment with rituximab of 8,000 Euro. In further support of this, Kain et al.23 reported a patient in which the estimated cost of treating acute bleeding episodes with rFVIIIa was greater than that with rituximab.
Figure 3 - Management of patients with AHA, according to the algorithm of Franchini and Mannucci (see text and reference21).
AHA: acquired haemophilia A; BU: Bethesda unit; DDAVP: desmopressin; rFVIIIa: recombinant activated factor VIII.
All rights reserved - For personal use only No other use without premission

© SIMTI S
ervizi
Srl
260
D'Arena G et al
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
ConclusionsIn the last years, the anti-CD20 monoclonal
antibody rituximab has gained a role in the treatment of autoimmune disorders and its use is rapidly increasing1. Notably, rituximab also seems to be beneficial in AHA. However, its definitive role in inhibitor eradication (first or second-line therapy, high or low inhibitor titres, older and/or frail patients for whom corticosteroid and cytotoxic therapy are unsuitable) still requires further evaluation. Unfortunately, it is difficult to design randomised controlled trials in AHA because of the rarity of this disorder. Notwithstanding, though additional data need to be acquired in order to optimise the use and to compare the efficacy of this drug to that of other treatments, current evidence confirms that rituximab should now be considered as part of the therapeutic armamentarium of AHA, despite reserving it to second line-therapy.
AcknowledgementsThis work is dedicated to the memory of Prof.
Giuseppe (Pino) Maiese. He lives on in our hearts.
Disclosure of conflicts of interestPM received onoraria from Roche, the manufacturer of rituximab. All other Authors declare no conflicts of interest.
References1) Gurcan HM, Keskin DB, Stern JNH, et al. A review of
the current use of rituximab in autoimmune diseases. Int Immunopharmacol 2009; 9: 10-25.
2) Ma AD, Carrizosa D. Acquired factor VIII inhibitors: pathophysiology and treatment. Hematol Am Soc Hematol Educ Program 2006; 432-7.
3) Collins PW. Therapeutic challenges in acquired factor VIII deficiency. Hematol Am Soc Hematol Educ Program 2012; 2012: 369-74.
4) Karwal MW, Schlueter AJ, Zenz DW, Davis R. Treatment of acquired factor VIII deficiency with rituximab. Blood 2001; 98: 533.
5) Barcellini W, Zanella A. Rituximab therapy for autoimmune haematological disease. Eur J Int Med 2011; 22: 220-9.
6) Lozier EL. Hemorragic diathesis with prolonged coagulation time associated with a circulating anticoagulant. Am J Med Sci 1940; 199: 318-27.
7) Cohen AJ, Kessler CM. Acquired inhibitors. Bailleres Clin Hematol 1996; 9: 331-54.
8) Baudo F, Collins P, Huth-Kuhne A, et al. Management of bleeding in acquired hemophilia A: results from the European Acquired Haemophilia (EACH2) Registry. Blood 2012; 120: 39-46.
9) D'Arena G, Guariglia R, La Rocca F, et al. Autoimmune cytopenias in chronic lymphocytic leukemia. Clin Dev Immunol 2013; 2013: 730131.
10) Sperr WR, Lechner K, Pabinger I. Rituximab for the treatment of acquired antibodies to factor VIII. Haematologica 2007; 92: 66-71.
11) Franchini M, Targher G, Manzato F, Lippi G. Acquired factor VIII inhibitors in oncohematology: a systematic review. Crit Rev Oncol Hematol 2008; 66: 194-9.
12) Sallah S, Nguian NP, Abdallah JM, Hourahan LR. Acquired hemophilia in patients with hematologic malignancies. Arch Pathol Lab Med 2000; 124: 730-4.
13) Tiede A, Werwitzke S, Scharf RE. Laboratory diagnosis of acquired hemophilia A: limitations, consequences, and challenges. Semin Thromb Hemost 2014; 40: 803-11.
14) Tiede A, Klemorth R, Scharf RE, et al. prognostic factors for remission of and survival in acquired hemophilia A (AHA): results from the GTH-AH 01/2010 study. Blood 2015; 125: 1091-7.
15) Weiner GJ. Rituximab: mechanism of action. Semin Hematol 2010; 47: 115-23.
16) Wermke M, von Bonin M, Gehrisch S, et al. Successful eradication of acquired factor-VIII-inhibitor using single low-dose rituximab. Haematologica 2010; 95: 521-2.
17) Aggarwal A, Grewal R, Green RJ, et al. Rituximab for autoimmune haemophilia: a proposed treatment algorithm. Haemophilia 2005; 11: 13-9.
18) Collins PW, Mathias M, Hanley J, et al. Rituximab and immune tolerance in severe haemophilia A: a consecutive national cohort. J Thromb Haemost 2009; 7: 787-94.
19) Franchini M, Mengoli C, Lippi G, et al. Immune tolerance with rituximab in congenital haemophilia with inhibitors: a systematic literature review based on individual patients' analysis. Haemophilia 2008; 14: 903-12.
20) Franchini M. Rituximab in the treatment of adult hemophilia A: a systematic review. Crit Rev Onc Hematol 2007; 63: 47-52.
21) Franchini M, Mannucci PM. Inhibitor eradication with rituximab in haemophilia: where do we stand? Br J Haematol 2014; 165: 600-8.
22) Wiestner A, Cho HJ, Asch AS, et al. Rituximab in the treatment of acquired factor VIII inhibitors. Blood 2002; 100: 3426-8.
23) Kain S, Copeland TS, Leahy NF. Treatment of refractory autoimmune (acquired) haemophilia with anti-CD20 (rituximab). Br J Haematol 2002; 119: 578.
24) Marietta M, Pozzi S, Luppi M, et al. Acquired haemophilia in HIV negative, HHV-8 positive multicentric Castelman's disease: a case report. Eur J Haematol 2003; 70: 181-2.
25) Fischer KG, Deschler B, Lubbert M. Acquired high-titer factor VIII inhibitor: fatal bleeding despite multimodal treatment including rituximab preceded by plasmaphereses. Blood 2003; 101: 3753-4.
26) Jy W, Gagliano-DeCesare T, Kett DH, et al. Life-threatening bleeding from refractory acquired FVIII inhibitor successfully treated with rituximab. Acta Haematol 2003; 109: 206-8.
27) Stasi R, Brunetti M, Stipa E, Amadori S. Selective B-cell depletion with rituximab for the treatment of patients with acquired hemophilia. Blood 2004; 103: 4424-8.
28) Abdallah A, Coghlan DW, Duncan EM, et al. Rituximab-induced long-term remission in patients with refractory acquired hemophilia. J Thromb Haemost 2005; 3: 2589-90.
29) Herman C, Boggio L, Green D. Factor VIII inhibitor associated with peginterferon. Haemophilia 2005; 11: 408-10.
30) Holme PA, Brosstad F, Tjonnfjord GE. Acquired haemophilia: management of bleeds and immune therapy to eradicate autoantibodies. Haemophilia 2005; 11: 510-5.
31) Maillard H, Launay D, Hachulla E, et al. Rituximab in postpartum-related acquired hemophilia. Am J Med 2006; 119: 86-8.
32) Clatworthy MR, Jayne DR. Acquired hemophilia in association with ANCA-associated vasculitis: response to rituximab. Am J Kidney Dis 2006; 47: 680-2.
33) Berezné A, Stieltjes N, Le-Guern V, et al. Rituximab alone or in association with cortcosteroids in the treatment of acquired factor VIII inhibitors: report of two cases. Transfus Med 2006; 16: 209-12.
34) Onitilo A, Skorupa A, Lal A, et al. Rituximab in the treatment of acquired factor VIII inhibitors. Thromb Haemost 2006; 96: 84-7.
All rights reserved - For personal use only No other use without premission
© SIMTI S
ervizi
Srl
261
Blood Transfus 2016; 14: 255-61 DOI 10.2450/2015.0090-15
Rituximab to treat acquired haemophilia A
35) Oliveira B, Arkfeld DG, Weitz IC, et al. Successful rituximab therapy of acquired factor VIII inhibitor in a patient with rheumatoid arthritis. J Clin Rheumatol 2007; 13: 89-91.
36) Alvarado Y, Yao X, Jumper C, et al. Acquired hemophilia: a case report of 2 patients with acquired factor VIII inhibitor treated with rituximab plus a short course of steroid and review of the literature. Clin App Thromb Hemost 2007; 13: 443-8.
37) Millet A, Decaux O, Bareau B, et al. Efficiency of rituximab in acquired hemophilia: report of two cases and review of literature. Rev Med Int 2007; 28: 862-5.
38) Machado P, Raya JM, Martin T, et al. Successful response to rituximab in two cases of acquired haemophilia refractory to standard-therapy. Int J Hematol 2008; 87: 545-9.
39) Cretel E, Jean R, Chiche L, Durant JM. Successful treatment with rituximab in an elderly patient with acquired factor VIII inhibitor. Geriatr Gerontol Int 2009; 9: 197-9.
40) Dedeken L, St-Louis J, Demers C, et al. Postpartum acquired haemophilia: a single centre experience with rituximab. Haemophilia 2009; 15: 1166-8.
41) Ichikawa S, Kohata K, Okitsu Y, et al. Acquired hemophilia A with sigmoid colon cancer: successful treatment with rituximab followed by sigmoidectomy. In J Hematol 2009; 90: 33-6.
42) Boles JC, Key NS, Kasthuri R, Ma AD. Single-center experience with rituximab as first-line immunosuppression for acquired hemophilia. J Thromb Haemost 2011; 9: 1429-31.
43) Singh AG, Hamarneh IS, Karwal MW, Lentz SR. Durable responses to rituximab in acquired factor VIII deficiency. Thromb Haemost 2011; 106: 172-4.
44) Collins P, Baudo F, Knoebl P, et al. Immunosuppression for acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2). Blood 2012; 120: 47-55.
45) Imashuku S, Kudo N, Kubo K, et al. Rituximab for managing acquired hemophilia A in a case of chronic neutrophilica leukemia with the JAK2 kinase V617F mutation. J Blood Med 2012; 3: 157-61.
46) Conte GL, Figuero GM, Aravena PR, et al. Acquired hemophilia A treated with rituximab. Report of one case. Rev Med Chile 139: 357-61.
47) Daikeler T, Labopin M, Di Gioia M, et al. Secondary autoimmune diseases occurring after HSCT for an autoimmune disease: a retrospective study of the EBMT autoimmune disease working party. Blood 2011; 118: 1693-8.
48) de Palencia Espinosa MAF, Casan VA, Corro y A de la Rubia Nieto BG. Acquired haemophilia A in a patient with chronic hepatitis C virus infection receiving treatment with pegylated interferon plus ribavirin: role of rituximab. Farm Hosp 2013; 37: 494-8.
49) D'Arena G, Grandone E, Di Minno MN, et al. Acquired hemophilia A successfully treated with rituximab. Mediterr J Hematol Infect Dis 2015, 7 (1): 12015024.
Arrived: 8 April 2015 - Revision accepted: 17 June 2015Correspondence: Giovanni D'ArenaHaematology and Stem Cell Transplantation UnitIRCCS, Centro di Riferimento Oncologico della Basilicata Via Padre Pio 185028 Rionero in Vulture, Italye-mail: [email protected]
All rights reserved - For personal use only No other use without premission