review l treatment implant surgery ocal …eprints.bice.rm.cnr.it/4671/1/portiere.pdflocal...
TRANSCRIPT
review
ORAL & Implantology - Anno I - N. 1/2008
The diverse methods and terminology used in theliterature regarding accidents and complicationscall for descriptive criteria that may be universal-ly accepted irrespective of the different focus ofsingle studies. The proposed classification (Tab.1). considers the timing of events and is based ona distinction between the terms accident andcomplication. Accidents are events that occurduring surgery and complications are all theconditions that appear postoperatively. Early-stage complications appear in the immediatepostoperative period and interfere with healing,
and late-stage complications arise during theprocess of osseointegration.
Early-stage complications
Early-stage complications may involve the max-illary sinus or the mandibular bone, soft tissuesand nerve trunks adjacent to the implant site. Notall the mechanisms responsible for these compli-cations are known but the most common causes
LOCAL COMPLICATIONS IN DENTALIMPLANT SURGERY: PREVENTION ANDTREATMENTS. ANNIBALI, M. RIPARI, G. LA MONACA, F. TONOLI, M.P. CRISTALLI
University of Rome “Sapienza”Department of Oral Surgery, School of Dentistry
SUMMARYLocal complications in dental implant surgery: preven-tion and treatmentThere are many detailed articles regarding accidents andlocal complications in dental implantation. Comparison ofthe data they report is not always easy because differentcriteria have been followed in the various classificationsand there is confusion between the terms accident andcomplication. The aim of this paper is to propose a classi-fication that considers the timing of the events and makesa distinction between the two terms. Accidents are eventsthat occur during surgery and complications are all thepathological conditions that appear postoperatively. Theproper diagnostic procedures and surgical techniques forcomplications prevention and treatment are also de-scribed.
Key words: complications, failures, prevention, treatment,osseointegrated implants.
RIASSUNTOComplicanze locali in chirurgia implantare: prevenzio-ne e trattamentoLe pubblicazioni relative agli incidenti e alle complicanze lo-cali in chirurgia implantare sono numerose e dettagliate, an-che se i dati non sempre sono di facile confronto sia per ladiversità dei criteri adottati nell’elaborare le classificazioni,sia per la confusione esistente tra i termini di incidente ecomplicanza. Scopo del presente lavoro è quello di propor-re una classificazione che tenga in considerazione la cro-nologia degli eventi e si basi sulla differenza esistente trai due termini, per cui si devono considerare incidenti glieventi che si verificano durante l’intervento e complicanzetutte le condizioni patologiche che si manifestano nel pe-riodo successivo alla fase chirurgica. Vengono descrittiinoltre le procedure diagnostiche e gli accorgimenti di tec-nica operatoria necessari alla loro prevenzione e al lorotrattamento.
Parole chiave: complicanze, fallimenti, prevenzione, trat-tamento, impianti osteointegrati.
21
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

ORAL & Implantology - Anno I - N. 1/2008
revi
ew
22
are an excessively traumatic surgical approach,bone overheating during osteotomy, and bacteri-al contamination of the host site.
Infection
Infections arising during the first few postopera-tive days present with edema, exudate and pain.They are caused by bacterial contamination dur-ing surgery either directly via accidental contactwith the implants or indirectly from gloves or in-struments. The risks of such a complication maybe reduced by following the surgical principlesof asepsis (1, 2). This measure is advisable eventhough a retrospective analysis by Scharf andTarnow (3) comparing 273 implants inserted un-der “sterile” conditions and 113 implants placedunder “clean” conditions showed no statisticallysignificant differences in the success rates of thetwo groups.Besides a sterile working area and a clean envi-ronment, an aseptic protocol includes disinfec-tion of the perioral skin with solutions containingpovidone-iodine and alcohol, disinfection of theoral mucosa with 0.2% chlorhexidine (which sig-nificantly reduces the bacterial count in the sali-va for over 4 hours), and cleansing of surgicalgloves in sterile saline to remove dust or contam-inants. Further preventive measures are the ad-
ministration of antibiotic therapy before and afterthe procedure and the prescription of proper oralhygiene at home with mouthwashes containing0.12% chlorhexidine during the first two weeksafter the procedure. A recent study reported thatthe use of chlorhexidine was associated with sig-nificant reductions in infections showing a 4.1%decrease in the test group and 8.7 % reduction inthe control group (4).
Edema
Edema is the accumulation of excess plasma flu-id (transudate) in the interstitial spaces (at least a10% increase). It is correlated to the extent ofsurgical trauma and to the duration of surgery.Edema is a complication when there is a consid-erable accumulation of fluid because this maynegatively affect healing and create discomfort tothe patient during food intake and oral hygienemaintenance (Fig. 1). Atraumatic surgical tech-
Figure 1Postoperative edema.
Table 1 - Local complications in dental implant sur-gery.
Early-stage complications• Infection• Edema• Ecchymoses and haematomas• Emphysema• Bleeding• Flap dehiscence • Sensory disorders
Late complications• Perforation of the mucoperiosteum• Maxillary sinusitis• Mandibular fractures• Failed osseointegration• Bony defects• Periapical implant lesion
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 23
niques minimizing tissue damage, the applicationof ice packs and the administration of corticos-teroids will prevent or limit edema after implantsurgery.
Ecchymoses and haematomas
Blood effusions infiltrating surface tissues (ec-chymoses) and circumscribed blood collections(hematomas) are not common after implant sur-gery. Particularly long and complex procedures,lack of patient compliance with the instructionsreceived for the immediate postoperative period(application of ice packs, compression and tam-ponade, and cold liquid diet), vessel fragility, es-pecially typical in elderly patients, and failure todiscontinue antiplatelet therapy before surgery(5) may favor the appearance of ecchymoses andhematomas (Fig. 2).
Although they are associated with a greater riskof infection, ecchymoses and hematomas do notgenerally require any particular treatment. Topi-cal skin applications of heparin-containing med-ications will help them resorb. If there is a recenthematoma between the bone and the mucope-riosteal flap, it should be drained and externalcompression will be applied on the soft tissues toavoid relapses (6).
Emphysema
Emphysema is a very rare complication resultingfrom a sudden rise of the intraoral pressure. Thismay occur when a patient sneezes and air isforced through the mucoperiosteal tissue of a notperfectly approximated flap and into the muscu-lar interstices at the interface between the muscu-lar fascia and soft tissues (6). Clinically it pres-ents with swelling of half of the face, extendingat times to the neck and thorax. A characteristiccrackling sound is evinced upon palpation.Massages and compression with ice packs willhelp resorb the air entrapped in the tissues thusleading to fast and spontaneous regression of theemphysema.Measures for preventing this complication in-clude avoiding the use of high-velocity instru-ments to prepare the bone bed or irrigation of thewound with hydrogen peroxide and ensuring aperfect approximation of incised edges when su-turing. Patients will be instructed blow their nosegently and avoid sneezing during the first fewdays after surgery.
Bleeding
Failure to stabilize the flap, tearing of soft tissuescaused by tight or sharp suture material, mastica-tory trauma and traumas resulting from earlytemporization or an inappropriately modifiedtemporary prosthesis are all causes of postopera-tive bleeding. Treatment will consist of eliminat-
Figure 2Ecchymose and haematoma.
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

ORAL & Implantology - Anno I - N. 1/2008
revi
ew
24
ing the causes of bleeding and implementing thenormal procedures to promote hemostasis (com-pression and tamponade with surgical gauzessoaked in tranexamic acid). If the bleeding doesnot stop, the flap will be re-elevated, the clottedblood removed and new sutures applied to fullyimmobilize the soft tissues and promote clot for-mation and stabilization.
Flap dehiscence
Dehiscence is opening of the surgical woundedges exposing part or all of the implant headand/or surrounding bony tissues. Etiologically,flap dehiscence may result from a number ofcausative factors: a very thin mucosa; failure toensure passive reapproximation and closure ofthe flap margins, that will thus be unable tocounter the intramural mechanical stress due tomuscle/bone interaction; presence of large ede-ma or hematomas; insufficient or excessive ten-sion on the suture, causing soft tissue necrosisdue to impaired blood supply; functional move-ments, such as mastication, phonation or deglu-tition; previous prosthodontic surgery or radia-tion therapy affecting the vascularity of the flap;sudden trauma of edentulous segments by theopposing dentition; premature use of a remov-able denture; incomplete tightening of the coverscrew, often as a result of the presence of bloodresidues inside the implant; bone débris pro-duced during osteotomy or implant insertion andtrapped under the periosteum; cigarette smokingand the local effects of nicotine (presence of cy-totoxic and vasoactive substances) as well as itssystemic effects (altered granulocytes and Tcells, impaired production of antibodies and va-somotor substances) (Fig. 3) (5, 7, 8).Treatment will vary based on the extent of expo-sure. If it is small, no surgical correction is re-quired because the granulation tissue that formswill promote healing by secondary intention. Agranulation tissue formation process lasting overtwo weeks may require refreshing the epithelialwound margins with a diamond bur. A large de-
hiscence will be treated by removing the suturesand resuturing.Dehiscences may be prevented by 1) careful pre-operative assessment of the soft tissues to meas-ure the amount of keratinized mucosa presentand planning of augmentation procedures as ap-propriate; 2) minimally invasive flap elevationand reflection with careful removal of any bonedébris beneath; 3) proper suturing; 4) sensibletemporization with appropriate modifications,rebasing and relining; and 5) delaying the use ofremovable dentures until two weeks after sur-gery.
Sensory disorders
Temporary or permanent sensory impairmentmay result from injuries to nerve trunks during
Figure 3Flap dehiscence one week after surgery.
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 25
implant surgery. Quantitatively, sensory disor-ders may entail enhanced perception of a stimu-lus (hyperesthesia), reduced sensitivity (hypoes-thesia) or no sensation (anesthesia). Qualitative-ly, disorders are distinguished based on the per-ception of a different stimulus from the one ap-plied (paresthesia or dysesthesia).Patients may express the changes they subjec-tively perceive with a variety of words and ways(9). After a self-administered questionnaire wascompleted by 266 patients treated with osseointe-grated mandibular implants, Ellies reported thatsymptoms included numbness, tingling, hot andcold, pain, swelling, hardening, burning, loss ofsaliva, prickling, tickle, electrical shock sensa-tion (54-64%), itch and effects on phonation, onthe intake of solid or liquid foods, on deglutition,and on taste. The lower jaw was more affectedand the most common sites were the lower lip(54-64%), chin (46-58%), gum tissues (32-45%),and the tongue (11-16%) (10-12). Sensory alterations prevail in the mandible (thereis a lesser likelihood of sensory impairment inthe maxilla) with values ranging from 1.7 to43.5% for temporary alterations and from 5% to15% for permanent alterations over one year af-ter surgery (11 ).Establishing the prognosis is not simple. Themain factor affecting duration and reversibility isthe nature of the damage. Reversible conditionscomprise compression by edema or hematomasand excessive stretching of the mental nerve dur-ing flap reflection, as long as stretching is not toosudden and the 8% elastic limit is not exceeded(9). The outcome of disorders caused by implantplacement close to the inferior alveolar nerve isvariable since immediate implant removal oftenleads to sensory recovery. By contrast, injuries tothe inferior alveolar nerve or to the mental nerveduring osteotomy produce permanent sensory al-teration with the occurrence of hyperalgesia (13).Diagnosis of a nerve injury is performed in twostages. The early-stage diagnosis will take placeimmediately after the injury occurs while late-stage diagnosis will include more thorough in-vestigations. In the early stage, the symptoms re-ported by the patient will be assessed and
panorex x-rays performed to identify any patho-logical changes that may be associated with theinjury (e.g. penetration of an implant into themandibular canal). If such changes are not radi-ographically visible, a wait and see attitude is ad-visable since the paresthesia and/or hypoesthesiareported by the patient may result from a“stunned nerve syndrome” (neuropraxia). Bycontrast, if the injury is observed intraoperative-ly and/or symptoms persist or worsen, clinicaland laboratory tests will be required. Clinical in-vestigations include mechanoceptive, thermal,electric, nociceptive, and chemical tests that willbe repeated monthly starting from the first monthafter the accident to assess changes in the func-tion of the affected nerve. Investigations of thelingual nerve will be supplemented with gustato-ry sensitivity tests.Laboratory tests include electrophysiologicalmeasurements (somato-sensory evoked poten-tials - TSEP) the Blink Reflex test, and advancedimaging techniques (computerized tomographyand nuclear magnetic resonance). Nerve trunk injuries may be treated medically orsurgically depending on the extent of the patho-logical alterations and the neurological symp-toms reported by the patient. In the immediatepostoperative period combination drug therapieswith NSAIDs, cortisones, proteoliyic enzymes,antibiotics, and vitamins (C and E) are adminis-tered to reduce compression of the nerve trunk byedema or hematomas, to prevent the develop-ment of infections and to block fibrous tissuescarring. In the first month after implant surgery,the aim of treatment is to promote nerve regener-ation. Hence, vitamins C and D, vasodilators(naftidrofuryl) and ozone therapy will be admin-istered to prevent ischemia due to an increasedblood supply demand during the regenerationprocess. Physical therapy, with magnetotherapy,low level laser therapy, and transcutaneous elec-tric nerve stimulation (TENS) will be ensured.Should these therapeutic regimens fail, drug ther-apy will be administered with anticonvulsants(carbamazepine, diphenylhydantoin, valproicacid) or associations of tricyclic antidepressantsand psychotropic drugs (phenotiazine) to control
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI
ORAL & Implantology - Anno I - N. 1/2008
revi
ew
26
central pain induced by cortical hyperactivity.Surgical therapy (microneurosurgery) may be re-quired to restore integrity of the injured nervetrunk and of nerve function. Three techniqueshave been described in the literature for nerve re-construction: 1) neurorrhaphy or direct end-to-end anastomosis with an epineural or interfascic-ular suture; 2) grafting of autologous nerve tissuetaken from various sites; and 3) tubulization ofthe nerve stumps.
Late complications
Late-stage complications are the result of nox-ious events occurring during surgery or healing.They mainly concern osseointegrating implantsand the surrounding bone tissue and havecausative mechanisms that often remain obscure.
Perforation of the mucoperiosteum
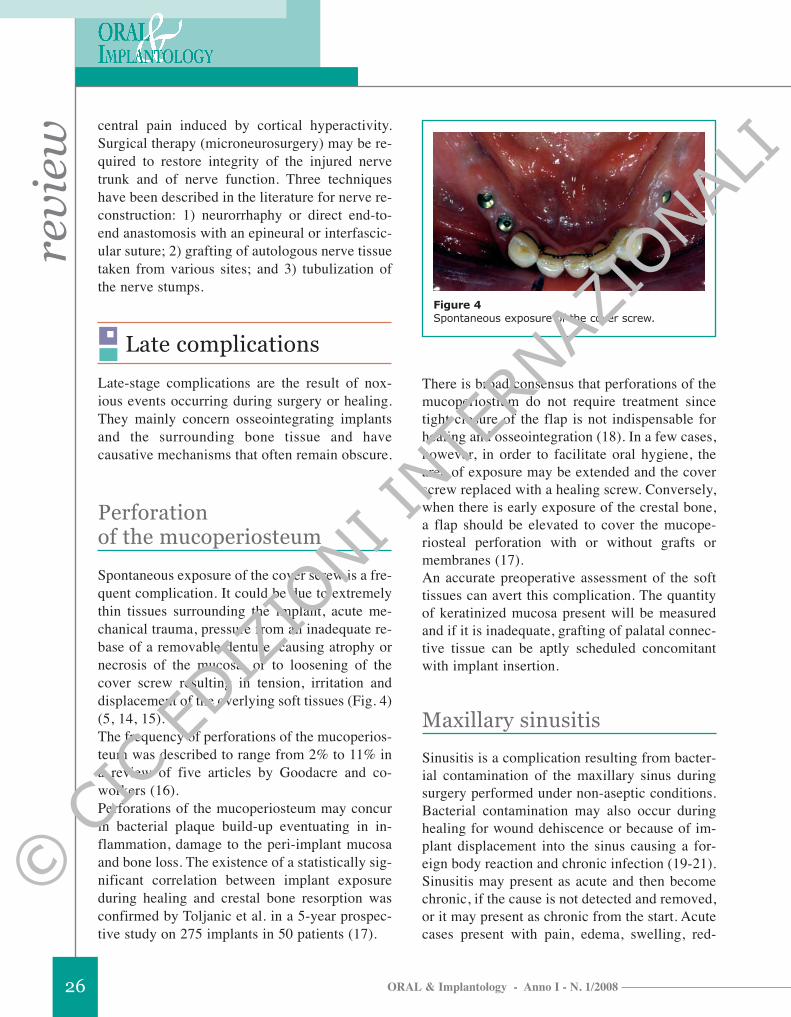
Spontaneous exposure of the cover screw is a fre-quent complication. It could be due to extremelythin tissues surrounding the implant, acute me-chanical trauma, pressure from an inadequate re-base of a removable denture, causing atrophy ornecrosis of the mucosa, or to loosening of thecover screw resulting in tension, irritation anddisplacement of the overlying soft tissues (Fig. 4)(5, 14, 15).The frequency of perforations of the mucoperios-teum was described to range from 2% to 11% ina review of five articles by Goodacre and co-workers (16). Perforations of the mucoperiosteum may concurin bacterial plaque build-up eventuating in in-flammation, damage to the peri-implant mucosaand bone loss. The existence of a statistically sig-nificant correlation between implant exposureduring healing and crestal bone resorption wasconfirmed by Toljanic et al. in a 5-year prospec-tive study on 275 implants in 50 patients (17).
There is broad consensus that perforations of themucoperiostium do not require treatment sincetight closure of the flap is not indispensable forhealing and osseointegration (18). In a few cases,however, in order to facilitate oral hygiene, thearea of exposure may be extended and the coverscrew replaced with a healing screw. Conversely,when there is early exposure of the crestal bone,a flap should be elevated to cover the mucope-riosteal perforation with or without grafts ormembranes (17).An accurate preoperative assessment of the softtissues can avert this complication. The quantityof keratinized mucosa present will be measuredand if it is inadequate, grafting of palatal connec-tive tissue can be aptly scheduled concomitantwith implant insertion.
Maxillary sinusitis
Sinusitis is a complication resulting from bacter-ial contamination of the maxillary sinus duringsurgery performed under non-aseptic conditions.Bacterial contamination may also occur duringhealing for wound dehiscence or because of im-plant displacement into the sinus causing a for-eign body reaction and chronic infection (19-21).Sinusitis may present as acute and then becomechronic, if the cause is not detected and removed,or it may present as chronic from the start. Acutecases present with pain, edema, swelling, red-
Figure 4Spontaneous exposure of the cover screw.
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 27
dened soft tissues overlying the involved sinusand purulent drainage through the homolateralnasal cavity (19-20). In chronic cases, there isless exudates but more massive proliferation ofmucosa, thickening of the membrane and meta-plasia of the epithelium; polypoid masses maypartially fill the sinus leading to exudate reten-tion. Air in the sinus will decrease considerablyand the antral content will become progressivelyradiopaque until it is completely and permanent-ly opacified.Treatment of sinusitis includes systemic therapywith antibiotics, chlorhexidine mouthwashes, ir-rigations with saline through the nasal orifice,and the use of nasal decongestants. If the infec-tion worsens or a dislodged implant is in the si-nus, radical revision surgery of the maxillary si-nus will be required and the antral mucosa com-pletely removed (Fig. 5a-5b) (19-21).Maxillary sinusitis may be prevented by careful-ly screening patients before implant surgery toidentify individuals with sinusitis or predispos-
ing factors, administering prophylactic antibiotictherapy and strictly observing the surgical princi-ples of asepsis.
Mandibular fractures
Mandibular fractures are rare complicationswhich may occur during osseointegration (beforethe implants are uncovered and loaded), afterrestoration (for the removal of non-osseointegrat-ed implants) or as the result of a trauma (16, 22-24). The cases reported in the literature regardonly endosseous implants placed in severely re-sorbed crests.The exact mechanism through which mandibularfractures occur is unknown, but the consistentfinding of fracture lines passing through implantsites strongly suggests that this is the weakestand most susceptible area during osseointegra-tion where stresses converge and the greatest lossof bone density occurs. This is why it has often
Figure 5a-bMaxillary sinusitis for implant displacement into the sinus.
A B© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

ORAL & Implantology - Anno I - N. 1/2008
revi
ew
28
been hypothesized that there may be a correlationbetween the occurrence of mandibular fracturesand metabolic or bone remodeling disorders,such as osteoporosis and osteomalacia (22).The clinical signs of mandibular fractures arepain, swelling, impaired function and fistulae inthe fracture area (23, 24).Diagnosis consists of clinical and radiographicexamination of the patient. During the clinicalevaluation, small movements of bony fragments,crackling sounds, and signs of infection will beidentified. Radiographs will characteristicallyshow a radiolucent area through the implant site(25). This is not always easy to identify and oftenrequires more enhanced investigations, such ashigh resolution CT and technetium 99m-methyl-ene diphosphonate bone scans, as suggested byRothman and co-workers (23).Aligned fractures with only numbness of thefractured area will be treated with antibiotictherapy and a soft diet. The patient will be keptunder observation since healing is usually un-eventful. Malaligned fractures require reductionand immobilization of the fractured segment torestore mandibular shape and function, especial-ly in view of future prosthodontic rehabilitation.There is no need to remove the implant to ensureeffective healing and osseointegration if there isno inflammation or implant loosening and thefractured fragments can be stabilized and fixedadequately (25, 26). It is not easy to predict theoutcome of highly resorbed malalignedmandibular fractures because of the reducedblood supply and the poor bone regeneration po-tential. Adequate precautions need to be taken beforeand during implantation surgery and during heal-ing to prevent mandibular fractures. The boneshould be at least 7 mm in height and 6 mm inwidth (24) and if this is not the case, proceduresfor ridge expansion or augmentation must be per-formed. During surgery, preparation of multiplebone beds is to be avoided. At least 5 mm of hardtissue should be left between one site and the oth-er to permit an adequate distribution of forces(24). After preparing the implant sites, the sur-geon should ensure that a few millimeters of buc-
cal and oral cortical bone remain. Finally, over-screwing of the implant into the bone is to beavoided. During healing the patient will be in-structed to keep the mandible at rest to protect itfrom stress.
Failed osseointegration
Lack of osseointegration is diagnosed at phase IIsurgery or restoration when the implant is loaded.It is one of the worst complications since it in-evitably results in loss of the implant (Fig. 6a-6b)(27).The main causes for lack of osseointegration in-clude reduced healing capacity, occlusal loadingduring osseointegration, failure to follow theplanned protocol, technical errors during surgery(such as accidental contamination of the implantsurface) (5-7), and especially bone overheatingduring implant site preparation. When a temper-ature of over 47°C is reached for 1 minute in-traosseous blood vessels coagulate and extendednecrotic areas are formed which become radi-ographically visible after 2-4 weeks (6).Clinically, lack of osseointegration is diagnosedwhen the implant has loosened and a muffledsound is heard upon percussion. Radiographicevidence consists of a small radiolucent marginaround the implant indicating that there is no di-rect contact between the bone and the implant(27-29).Treatment will require removal of the loose im-plant and accurate debridement of the area in-volved so that a new implant may be inserted af-ter healing has taken place.
Bony defects
A horizontal or vertical bony defect around animplant is a complication that may be observedon assessing the bone-implant interface at thetime of phase II surgery (Fig. 7).The causes that may lead to bone defects are:
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 29
1) direct trauma to the bone or an insult to the pe-riosteum reducing vascularity, 2) decreased bonedensity, 3) implant placement into fresh extrac-tion sockets, 4) wrong inclination of the implant,5) excessive torque during insertion, 6) the pres-
ence of a bone dehiscence not treated at phase Isurgery, 7) an extremely thin alveolar crest, 8)wound dehiscence during healing, 9) perforationof the mucoperiosteum, 10) postoperative infec-tion, 11) excessive loading by the temporaryprosthesis, or 12) the patient’s bad habits (17,30).Bony defects are not easy to identify since thepatients are asymptomatic. Hence the crestalbone-implant interface should always be exam-ined radiographically before connecting the abut-ment. If a bone defect is suspected, it is recom-mended to incise and elevate a flap to directlyevaluate the size of the defect after curetting anyepithelial tissue present .Treatment will differ based on the type and ex-tent of bone loss. Hence, in the presence of:– a vertical defect of less than 2 mm, horizontalosteoplasty can be performed to reduce the defectwithout compromising the restorations or thecosmetic result; – a vertical defect of more than 2 mm involving
Figure 7A vertical bony defect around two implants at the ti-me of phase II surgery.
Figure 6a-bLoss of the implant for lack of osseointegration.
A B
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

ORAL & Implantology - Anno I - N. 1/2008
revi
ew
30
less than half of the implant, autologous bonetaken from an intraoral site may be grafted.When the bone loss is greater than 25% of thecircumference of the implant, grafting may becombined with a membrane. Uncovering of theimplants will be postponed by 2-4 months;– a small horizontal defect, apical repositioningof the soft tissues will be performed with clean-ing of the exposed threads to avoid plaque build-up;– a larger horizontal defect, a graft of autologousbone will be performed and a membrane posi-tioned after accurate curettage of the area to helprestore blood supply and promote new bone for-mation. Uncovering of the implants will be post-poned by 3-4 months;– a vertical or horizontal defect deeper than halfthe length of the implant, the implant will have tobe removed because of inadequate stability andcosmetics.Bone defects may be prevented by identifyingand avoiding all the conditions that may engen-der the risk of such an event. Hence, treatmentplanning will take into account the quantity andquality of bone present. Proper surgical tech-niques will be performed and careful postopera-tive management ensured to protect the surgicalwound from excessive stress.
Periapical implant lesion
“Periapical implant lesion” designates a patho-logical area of osteolysis at the apex of an os-seointegrated implant (27, 31-33). The incidenceof periapical implant lesions has been reported toincrease when implant therapy was extended tocases of partial edentulism (31-35). The most frequent cause is contamination of theapical portion of an implant by microbial florafrom adjacent endodontically or periodontallyinvolved teeth. Other causes include: 1) acciden-tal sectioning of the neurovascular bundle ofneighboring teeth, 2) pre-existing bone infec-tions, 3) the presence of foreign bodies (en-dodontic material, fractured instruments in the
canals, etc.) or root fragments, 4) sinus infec-tions, 5) contamination of the implant surfaceduring manufacturing or insertion and 6) com-pression of bone débris on the bottom of the im-plant site by excessively forceful implant inser-tion causing ischemia, necrosis and bone seques-tration (31-35).Periapical implant lesions are “inactive” if nosymptoms are present and “infected” when signsof acute inflammation or a fistula are present. In-active lesions are similar to bone scars aroundthe apex of a tooth. They require no therapy, butonly careful clinical and radiographic follow-up.By contrast, infected lesions must be treated sur-gically and the procedure will vary based on theextension of the lesion. Conservative surgerywill be performed for small lesions. The infect-ed site will be accessed to entirely remove theinflammatory tissue around the apex of the im-plant. Some cases may also require removal ofpart of the implant (36). A more radical surgicalapproach will be necessary when osseointegra-tion is compromised or localized osteomyelitisis present. In this case the implant will be re-moved together with the infected tissue (31-35).Adjacent teeth with affected pulp or periodontaldisease will also be treated and the apical seal ofdevitalized teeth checked for leakage.Periapical implant lesions may be preventedthrough a careful preoperative examination of theperiodontal and endodontic conditions of the pa-tient and eradication of any microbial foci. Thisapproach might not suffice since bacteria havebeen shown to exist around the apex of pulpec-tomized teeth without any signs or symptoms. Fi-nally, surgery should be as minimally invasive aspossible and care will be taken to remove anybone débris from the bottom of the implant sitebefore implantation.
Infection
The main cause of late-stage infection is con-tamination of recently inserted implants by thepathogenic microflora of natural teeth. Contam-
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 31
ination of the implants may be favored by thepresence of necrotic and traumatized bony tis-sue and/or an impaired host defense mecha-nisms (7, 37). Characteristic clinical featuresare edema, swelling, purulent exudate, pain onpalpation or fistulae (Fig. 8a-8b). Relativelymarked bone resorption may be found on radi-ographs (38).If there is no bone involvement, a flap will beelevated and reflected to drain the abscess or re-move the granulation tissue. Sterile saline willbe used to irrigate the area and local antibiotictreatment with a tetracycline solution will beadministered. If there is bone resorption a guid-ed bone regeneration protocol will be followed.Postoperative antibiotic therapy in both caseswill consist of amoxillicin + clavulanic acid 2 gdaily and metronidazole 750 mg daily. The pa-tient will be instructed to maintain accurate oralhygiene with 0.12% chlorhexidine rinses.
Conclusions
Local complications arising during implant sur-gery may be the main determinants of the outcomeof the entire rehabilitation program. Hence, theprevention of complications is a priority objectivefor the surgeon. Careful clinical and radiographicexamination of each case, accurate planning ofprocedures, the use of proper surgical techniquesand appropriate instruments and the correct man-agement of healing and osseointegration all con-cur in preventing such events.
References
11. Friberg B. Sterile operating conditions for the place-ment of intraoral implants. J Oral Maxillofac Surg1996; 54: 1334-1336.
Figure 8a. Infection at the time of phase II surgery, characterized from edema and purulent exudates. b. A flap has been elevated to drain the abscess.
A B
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

ORAL & Implantology - Anno I - N. 1/2008
revi
ew
32
12. Kraut RA. Clean operating conditions for the place-ment of intraoral implants. J Oral Maxillofac Surg1996; 54: 1337-1338.
13. Sharf DR, Tarnow DP. Success rates of osseointegra-tion for implants placet under sterile versus clean con-ditions. J Periodontol 1993; 64 (10); 954-956.
14. Lambert PM, Morris HF, Ochi S. The influence of0.12% chlorexidine digluconate rinses on the incidenceof infectious complications and implant success. J OralMaxillofac Surg 1997; 55 (suppl 5): 25-30.
15. Worthington P, Bolender CL, Taylor TD. The swedishsystem of osseointegrated implants: problems andcomplications encountered during a 4- year trial peri-od. Int J Oral Maxillof Implants, 1987; 2: 77-84.
16. Lauc T, Kobler P. Early post-operative complicationsin oral implantology. Coll Antropol 1998; 22: 251-257.
17. Esposito M, Hirsch JM, Lekholm U, Thomsen P. Bi-ological factors contributing to failures of osseointe-grated oral implants: (II) Etiophatogenesis. Eur J OralSci 1998; 106: 721-764.
18. Haas R, Haimbock W, Mailath G, Watzek G. The re-lationship of smoking on peri-implant tissue: a retro-spective study. J Prosthet Dent 1996; 76: 592-596.
19. Dao T, Mellor A. Sensory disturbances associatedwith implant surgery. Int J Prosthodont 1998; 11: 462-469.
10. Ellies L. Altered sensation following mandibular im-plant surgery: a retrospective study. J Prosthet Dent1992; 68: 664-671.
11. Ellies LG, Hawker PB. The prevalence of altered sen-sation associated with implant surgery. Int J OralMaxillofac Implants 1993; 8: 674-679.
12. Ellies LG. The incidence of altered sensation of themental nerve after mandibular implant placement. JOral Maxillofac Surg 1999; 57: 1410-1412.
13. Wismeijer D, van Waas MA, Vermeeren JI, Kalk W.Patients’ perception of sensory disturbances of themental nerve before and after implant surgery: aprospective study of 110 patients. Br J Oral Maxillo-fac Surg 1997; 35 (4): 254-9.
14. Jemt T, Laney WR, Herris D, Henry PJ, Krogh PH,Polizzi G. Osteointegrated implants for single toothreplacement: a 1-year report from a multicenterprospective study. Int J Oral Maxillof Impl 1991; 6:29-36.
15. Tal H. Spontaneus early exposure of submerged im-plants: classification and clinical observations. J Peri-odontal 1999; 70: 213-219.
16. Goodacre C, Kan J Rungcharassaeng K. Clinicalcomplications of osseointegrated implants. J ProsthetDent 1999; 81: 537- 552.
17. Toljanic J, Banakis M, Willes L, Graham L. Soft tis-sue exposure of endosseous implants between stage I
and stage II surgery as a potential indicator of earlycrestal bone loss. Int J Oral Maxillof Implants 1999;14: 436-441.
18. Buser D, Bragger U, Lang NP, Nyman S. Regenera-tion and anlargement of jaw bone guided tissue regen-eration. Clin Oral Impl Res 1990; 1: 22-32.
19. Ueda M, Kaneda T. Maxillary sinusitis caused bydental implants: report of two cases. J Oral MaxillofSurg 1992; 50: 285-287.
20. Quiney RE, Brimble E, Hodge M. Maxillary sinusitisfrom dental osseointegrated implants. J Laryng Otol1990; 104: 333-334.
21. Regev E, Smith RA, Perrott DH, Pogrel MA. Maxil-lary sinus complications related to endosseous im-plants. J Oral Maxillofac Surg 1995; 10: 451-461.
22. Mason M, Triplett G, Van Sickels J, Parel S.Mandibular fractures through endosseous cylinderimplants: report of cases and review. J Oral Maxillo-fac Surg 1990; 48: 311-317.
23. Rothman SLG, Schwarz MS, Chafetz NI. High-reso-lution computerized tomography and nuclear bonescanning in the diagnosis of postoperative stress frac-tures of the mandible: a clinical report. Int J OralMaxillofac Implants 1995; 10: 765-768.
24. Raghoebar GM, Stellingsma K, Batenburg RH,Vissink A. Etiology and management of mandibularfractures associated with endosteal implants in the at-rophic mandible. Oral Surg Oral Med Oral PatholOral Radiol Endod 2000; 89: 553-9.
25. Shonberg DC, Stith HD, Jameson LM, Chai JY.Mandibular Fracture Through an Endosseous Im-plant. Int J Oral Maxillofac Implants 1992; 7: 401-404.
26. Eyrich G, Gratz K, Sailer H. Surgical treatment offractures of the edentulous mandible. J Oral Maxillo-fac Surg 1997; 55: 1081-1087.
27. Esposito M, Thomsen P, Ericson L, Lekholm U.Histopathologic observations on early oral implantfailures. Int J Oral Maxillof Implants, 1999; 14: 798-810.
28. Esposito M, Hirsch JM, Lekholm U, Thomsen P. Bi-ological factors contributing to failures of osseointe-grated oral implants: (I) Success criteria and epidemi-ology. Eur J Oral Sci 1998; 106: 527-551.
29. Schmid J. Pathogenesis of implant failures. Periodon-tology 2000; 1994; 4: 127-138.
30. Block MS, Kent JN. Factors associated with soft-and hard-tissue compromise of endosseous im-plants. J Oral Maxillofac Surg 1990 Nov; 48 (11):1153-60.
31. Piattelli A, Scarano A, Balleri P, Favero G. Clinicaland histologic evaluation of an active implant periapi-cal lesion: a case report. Int J Oral Maxillofac Impl1998; 13: 713-716.
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI

review
ORAL & Implantology - Anno I - N. 1/2008 33
32. Piattelli A, Scarano A, Piattelli M, Podda G. Implantperiapical lesions: clinical, histologic and histochem-ical aspects. A case report. Int J Periodont Rest Dent1998; 18: 181-187.
33. Piattelli A, Scarano A, Piattelli M. Abscess formationaround the apex of a maxillary root form implant:clinical and microscopical aspects. A case report. JPeriodontol 1995; 66 (10): 899-903.
34. Shaffer MD, Juruaz DA, Haggerty PC. The effect ofperiradicular endodontic pathosis on the apical regionof adjacent implants. Oral Surg Oral Med Oral PatholOral Radiol Endod 1998; 86 (5): 578-81.
35. Chaffee NR, Lowden K, Tiffee JC, Cooper LF. Peri-
apical abscess formation and resolution adjacent todental implants: a clinical report. J Prosthet Dent2001; 85 (2): 109-12.
36. Reiser GM, Nevins M. The implant periapical lesion:etiology, prevention, and treatment. Compend ContinEduc Dent 1995; 16 (8): 768, 770, 772 passim.
37. Rosenberg ES, Torosian JP, Slots J. Microbial differ-ences in 2 clinically distinct types of failures of osseoin-tegrated implants. Clin Oral Impl Res 1991; 2: 135-144.
38. Lehmann B, Bragger U, Hammerle CHF, FourmousisI, Lang NP. Treatment of an early implant failure ac-cording to the principles of guided tissue regeneration(GTR). Clin Oral Impl Res 1992; 3: 42-48.
Correspondence: Prof. Susanna AnnibaliDepartment of Oral Surgery, School of Dental MedicineUniversity of Rome “Sapienza”Via Caserta, 7 - 00189 RomeFax +39-6-49918142E-mail: [email protected]
© C
IC EDIZ
IONI I
NTERN
AZIO
NALI