review of gait, locomotion & lower limbs
TRANSCRIPT

Gait, Locomotion & Lower Limb
Prof. Saeed ShafiSahara Medical College
SAHARA FOR LIFE TRUST






??????
Learning Outcomes

ARTERIES OF LOWER LIMB
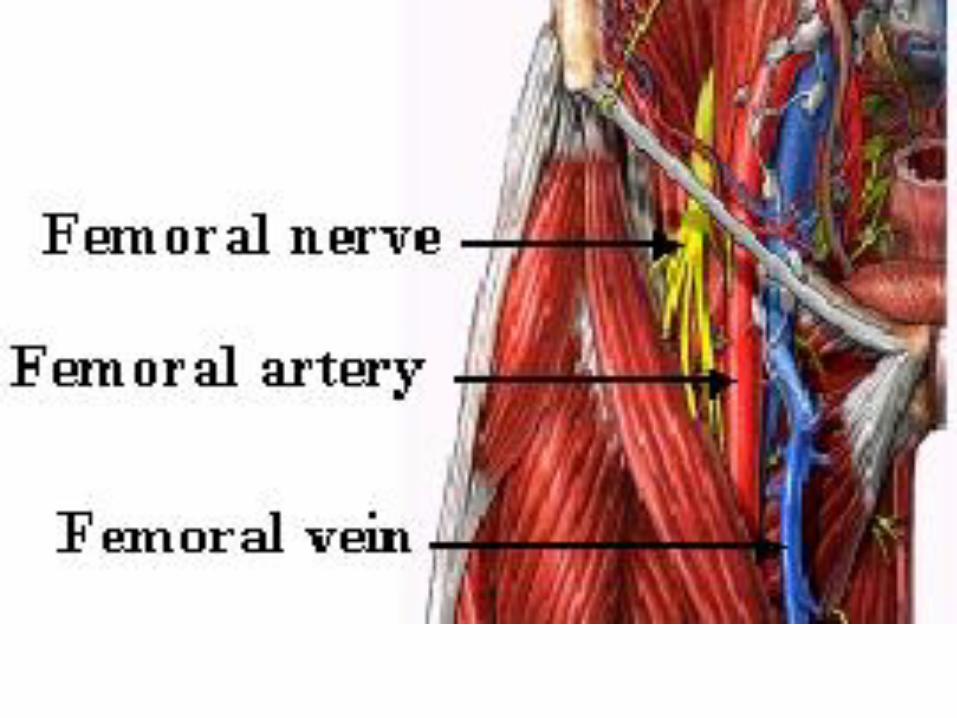
Femoral Artery
Continuation of External iliac artery.
Bisects the femoral triangle, runs deep to
the Sartorius muscle within the adductor
canal.
Leaves the adductor canal through the
tendinous opening in the Adductor
magnus, known as adductor hiatus.



ARTERIES OF LOWER LIMB
• Profanda Femoris Artery
Largest branch of the femoral artery and is the
chief artery to the thigh
Gives off perforating arteries that supply the
adductor magnus and hamstrings
Other branches are medial and lateral
circumflex femoral arteries



Arteries of Gluteal Region• Superior Gluteal Artery
Largest branch of internal iliac artery
Leaves the pelvis through greater sciatic foramen, superior to piriformis muscle
• inferior gluteal artery
Branch of internal iliac artery
Leaves the pelvis through greater sciatic foramen, inferior to piriformis muscle
• Internal pudendal artery
Branch of internal iliac artery
Leaves the pelvis through greater sciatic foramen, inferior to piriformis & enters perineum through lesser sciatic foramen.



ARTERIES OF LOWER LIMB
• Anterior tibial artery
smaller terminal branch of the popliteal artery
Travels in the anterior compartment of the leg from lower border of popliteus muscle upto the ankle joint midway between the two malleoli.
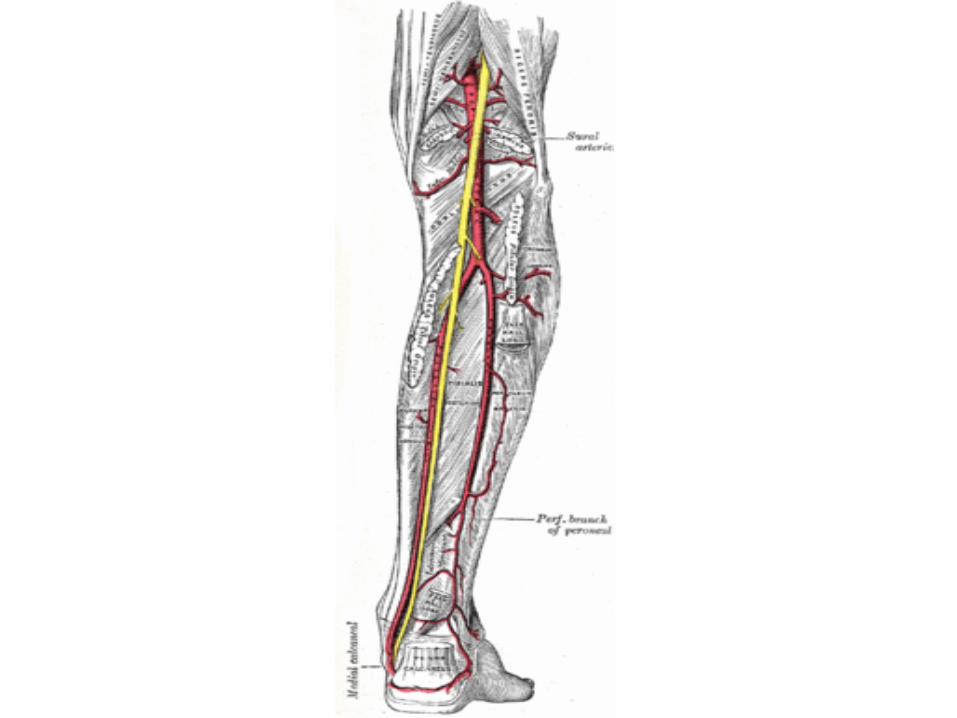
• Posterior tibial artery
larger terminal branch of the popliteal artery
Gives off a branch, the peroneal artery, and travels in the posterior compartment of the leg upto ankle.
ARTERIES OF LOWER LIMB
• Dorsalis pedis artery
Continuation of the anterior tibial artery, begins midway between the two malleoli to the proximal end of the 1st interosseous space
Divides into deep planter artery and arcuate artery and the later forms the dorsal arterial arch
• Lateral plantar artery
• Medial plantar artery
Terminal branches of the posterior tibial artery
Lateral plantar artery forms plantar arterial arch



ARTERIAL ANASTOMOSIS IN
LOWER LIMB
• Trochanteric anastomosis
Main source of blood supply for head of femur
Participating arteries are descending branch of superior
gluteal artey and ascending barnches of both medial and
lateral circumflex femoral arteries and they join near the
trochanteric fossa
• Cruciate anastomosis
Lies at the level of middle of lesser trochanter
Participating arteries are medial and lateral circumflex
femorals, 1st perforating and inferior gluteal areries

ARTERIAL ANASTOMOSIS IN
LOWER LIMB
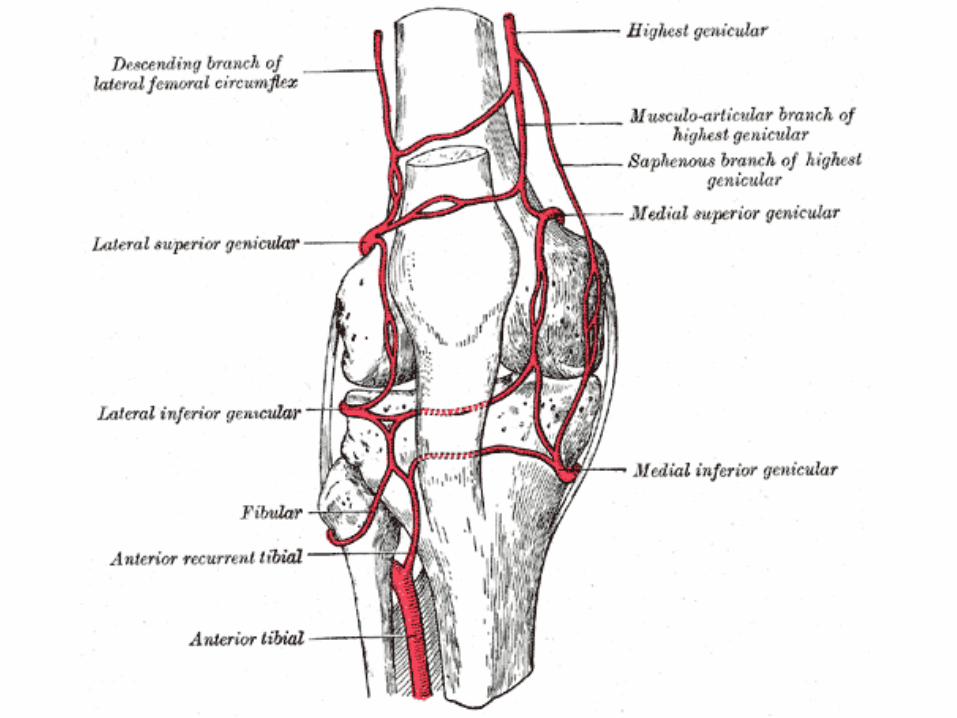
• Genicular anastomosis
• Important network of arterial vessels around the knee
• The two upper genicular branches of poplitealartery anastomose over the front of femur and patella with the descending branch of lateral circumflex femoral artery and the deep branch of descending genicular artery, and , over the front of tibia with the two lower genicular branches of popliteal artery

SUPERFICIAL VEINS OF THE
LOWER LIMB
• Great saphenous vein
• Largest vein the body
• Begins at the medial end of the dorsal venous arch, passes anterior to the medial malleolus of tibia and finally drains into the femoral vein by passing through the saphenous opening
• It is connected to the deep veins by perforating veins
• It has 10 to 12 valves that prevent the reflux of blood distally



SUPERFICIAL VEINS OF THE
LOWER LIMB
• small saphenous vein
• Begins from the lateral part of the dorsal venous
arch and passes posterior to the lateral
malloelus of fibula
• At the lower angle of popliteal fossa it perforates
the deep fascia and joins the popliteal vein


SUPERFICIAL NERVES AND
DERMATOMES OF LOWER LIMB





NERVES OF THE LOWER LIMB
The femoral nerve
• Largest branch of the lumber plexus(L234)
• Forms in the abdomen within the substance of Psoas major
• Passes through the pelvis to the midpoint of inguinal ligament, lateral to the femoral vessels, outside the femoral sheath
• Divides into branches which supply anterior thigh muscles, hip and knee joints and skin on the anteromedial side of the thigh.


NERVES OF THE GLUTEAL REGION
• Superior gluteal nerve
• Inferior gluteal nerve
• Nerve to quadratus femoris
• Nerve to obturator internus
• Pudendal nerve
• Sciatic nerve



NERVES OF THE LOWER LIMB
• The tibial nerve (L4 to S3)
• Medial terminal branch of sciatic nerve and is superficial to artery and vein in popliteal fossa
• Branches are; three genicular nerves to knee joint, muscular branches to calf muscles, and medial sural cutaneous nerve
• Medial sural cutaneous nerve is joined by communicating branch of common peroneal nerve to form sural nerve
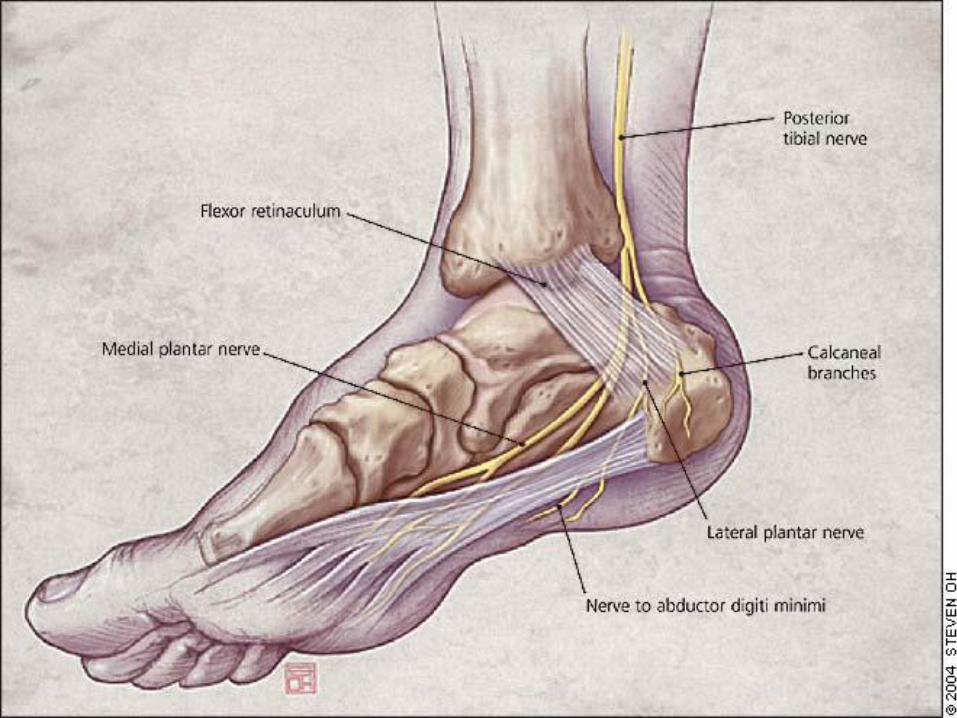
• Divides posterior to the medial malleolus into medial and lateral plantar nerves, which supply muscles and skin of sole

NERVES OF THE LOWER LIMB
• Common peroneal nerve
• Lateral and smaller terminal branch of sciatic
nerve
• Passes over head of fibula and winds around
the neck this bone and divides into superficial
and deep peroneal nerve
• Within the popliteal fossa it gives off genicular
branches to knee joint, lateral sural cutaneous
nerve, and peroneal communicating branch

NERVES OF THE LOWER LIMB
• Deep peroneal nerve
• This nerve of the anterior compartment of the leg is one of the terminal branches of common paeoneal nerve
• Supplies anterior leg muscles, ankle joint and other articulations that it crosses, and skin between the 1st and 2nd digit
• Superficial peroneal nerve
• this nerve of the lateral compartment of the leg is one of the two terminal branches of the common peronealnerve
• Supplies the peroneal muscles and becomes superficial in distal third of the leg

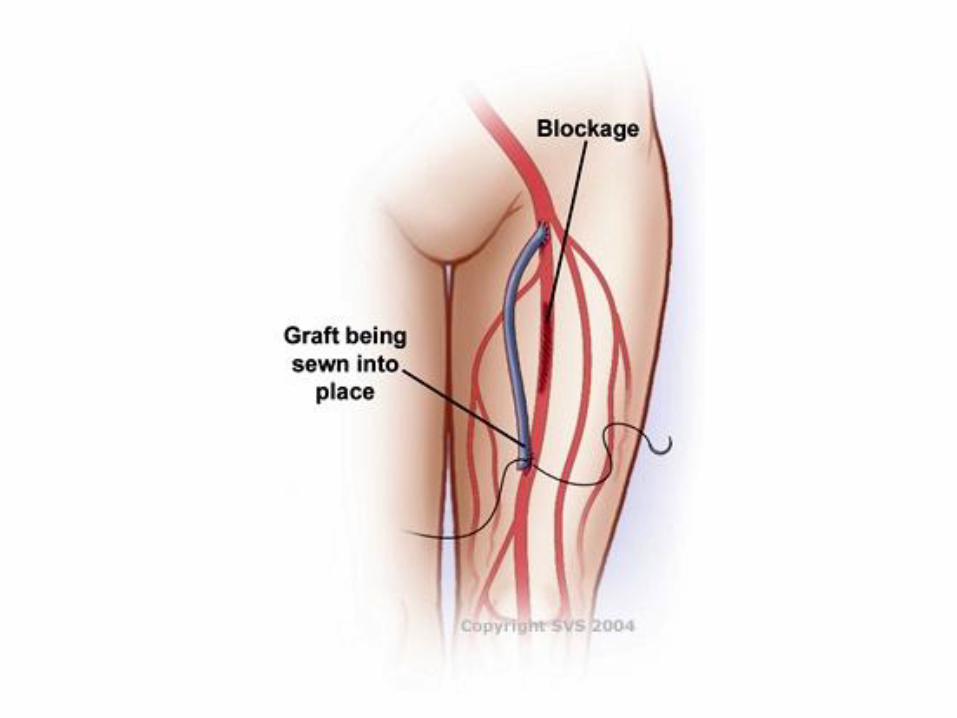



VERICOSE VEINS
• When the valves of the perforating lower limb veins become incompetent( i.e. dilated so that their cusps do not close the veins), contractions of the calf muscles, which normally propel the blood superiorly, cause a reverse flow through the perforating veins (i.e. from deep to superficial veins).
• As a result the perforating and superficial veins become tortuous and dilated
• Treatment consists of tight stockings and surgical ligations in advanced cases

05/10/2010 NAS 54
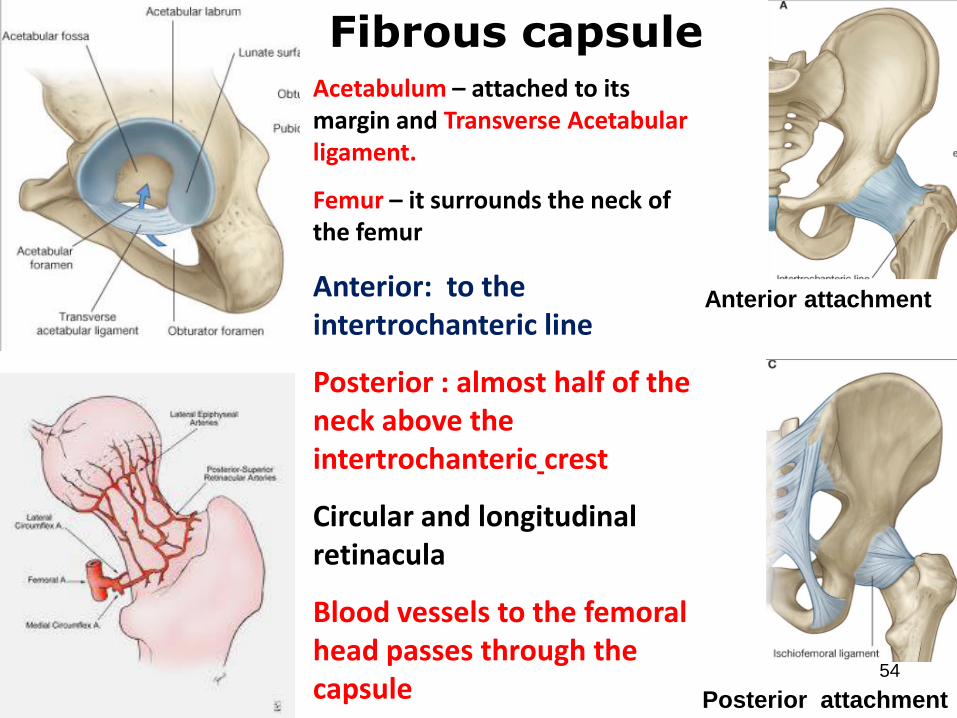
Posterior attachment
Acetabulum – attached to its margin and Transverse Acetabularligament.
Femur – it surrounds the neck of the femur
Anterior: to the intertrochanteric line
Posterior : almost half of the neck above the intertrochanteric crest
Circular and longitudinal retinacula
Blood vessels to the femoral head passes through the capsule
Fibrous capsule
Anterior attachment
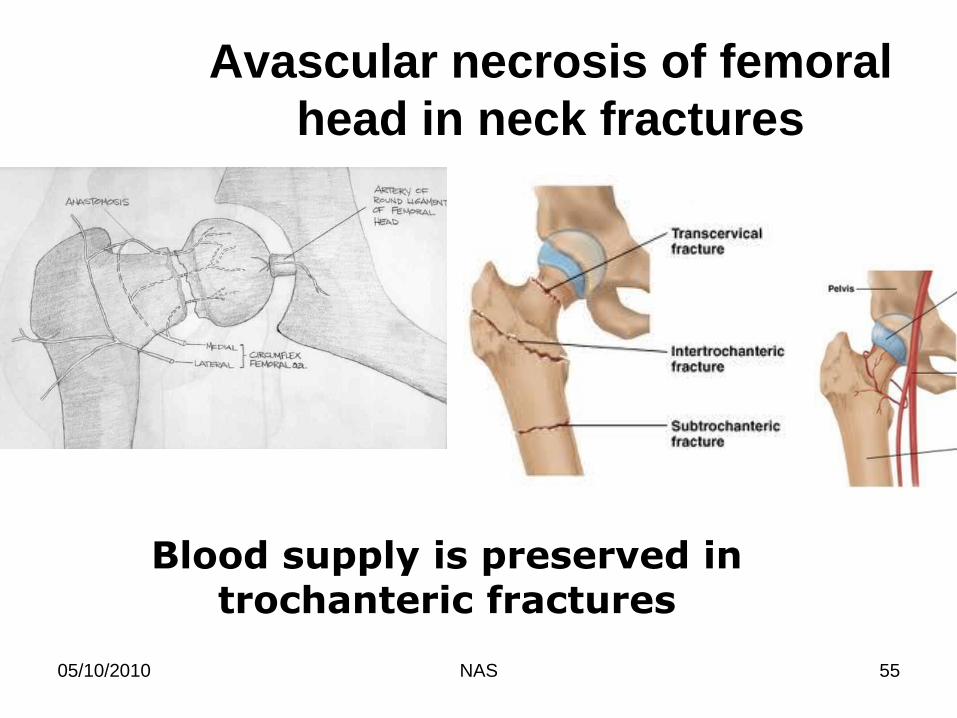
Avascular necrosis of femoral
head in neck fractures
05/10/2010 NAS 55
Blood supply is preserved in trochanteric fractures

05/10/2010 NAS 56
Normal angle of
inclination is about
135
(range 115-140) in
a child & 1350 in the
adult.
Coxa vara
(abnormally
decreased angle of
inclination)
e.g. fracture neck of
femur
Coxa valga
(abnormally increased
angle of inclination)
e.g. congenital
dislocation of the hip
joint
Knee joint and its injuries
17th Oct, 2011
Human structure Course NBAN- 403
Fall- 2011
Dr. Najam SiddiqiMBBS, PhD (Japan) Postdoc (USA)

Objectives: Know the….
• bony , ligamentous and cartilaginous structures that
comprise the knee joint
• proper alignment of the knee
– Be able to distinguish genu valgum from genu varus
• functions of the ligaments and menisci of the knee joint.
• bursas around the joint and their inflammation
• actions, innervations of the muscles acting on the knee
• mechanisms involved with locking and unlocking of the
knee
• the site of appropriate nerve lesion by deficits in knee
movement
• few common diseases of the knee joint
Knee Joint
• Type of the joint
• Articular surfaces
• Factors supporting the knee
• Capsule
• Ligaments
• Menisci
• Bursa
• Relations
• Movements (locking/unlocking)
• Clinical
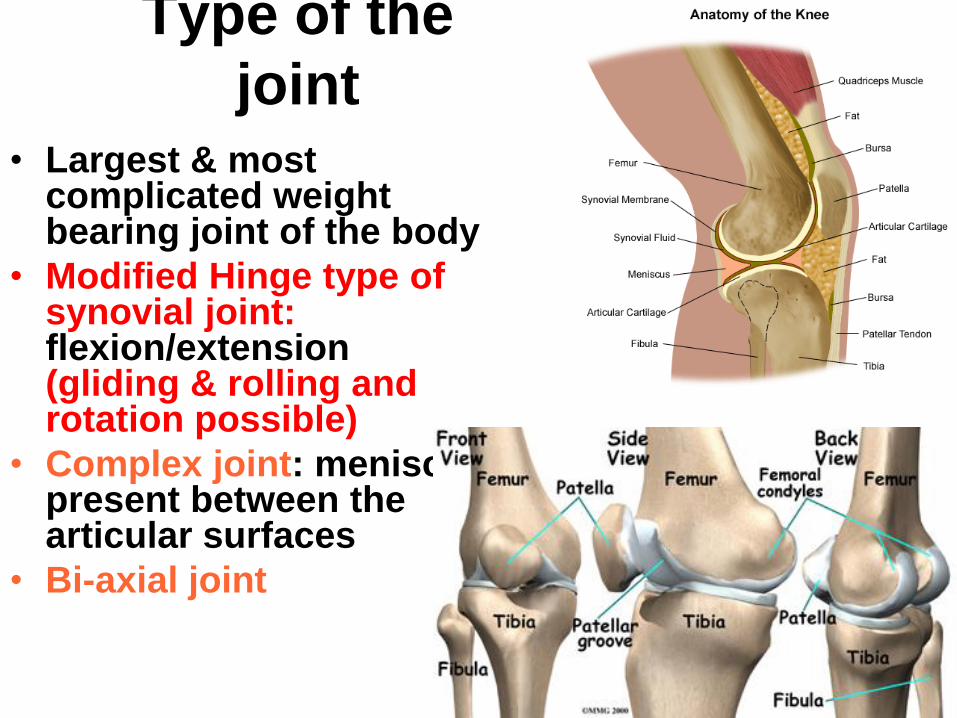
Type of the
joint• Largest & most
complicated weight bearing joint of the body
• Modified Hinge type of synovial joint: flexion/extension (gliding & rolling and rotation possible)
• Complex joint: menisci present between the articular surfaces
• Bi-axial joint
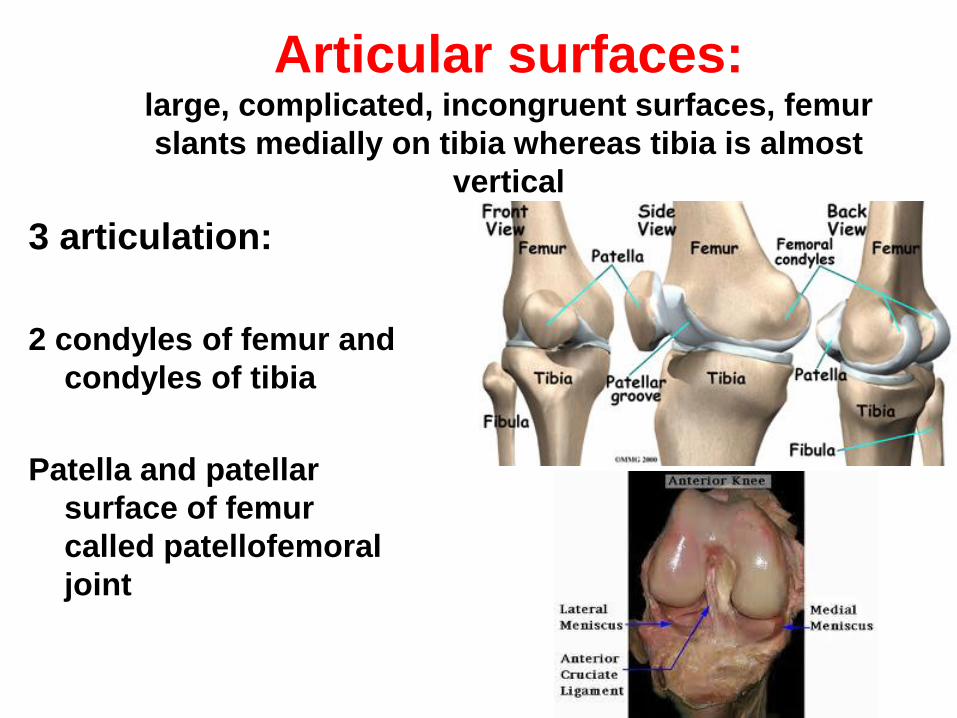
Articular surfaces: large, complicated, incongruent surfaces, femur
slants medially on tibia whereas tibia is almost
vertical
3 articulation:
2 condyles of femur and
condyles of tibia
Patella and patellar
surface of femur
called patellofemoral
joint
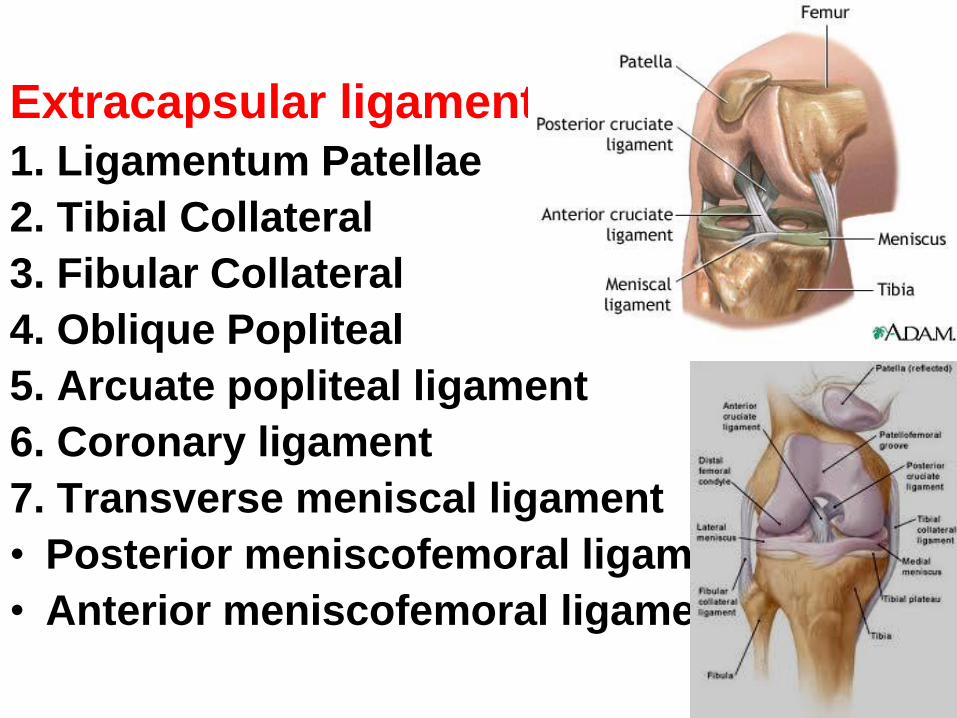
Extracapsular ligaments:
1. Ligamentum Patellae
2. Tibial Collateral
3. Fibular Collateral
4. Oblique Popliteal
5. Arcuate popliteal ligament
6. Coronary ligament
7. Transverse meniscal ligament
• Posterior meniscofemoral ligament
• Anterior meniscofemoral ligament

Extracapsular ligaments
Stabalize the knee
posteriorly
• Oblique Popliteal: tendon of semimembranosuspassing from medial to lateral femoral condyleand attaching to post. capsule
• Arcuate poplitealligament: Arise from fibular head to posterior surface of knee joint over the popliteus muscle

Collateral (Lateral and
medial) ligaments• Lateral collateral
ligament: lateral epicondyle of femur posterior to popliteus tendon to fibular head
• Medial collateral ligament: medial epicondyle of femur to medial tibia

Intracapsular (intra-articular)
ligaments• Anterior cruciate ligament
• Posterior cruciate ligament– refer to tibial attachments
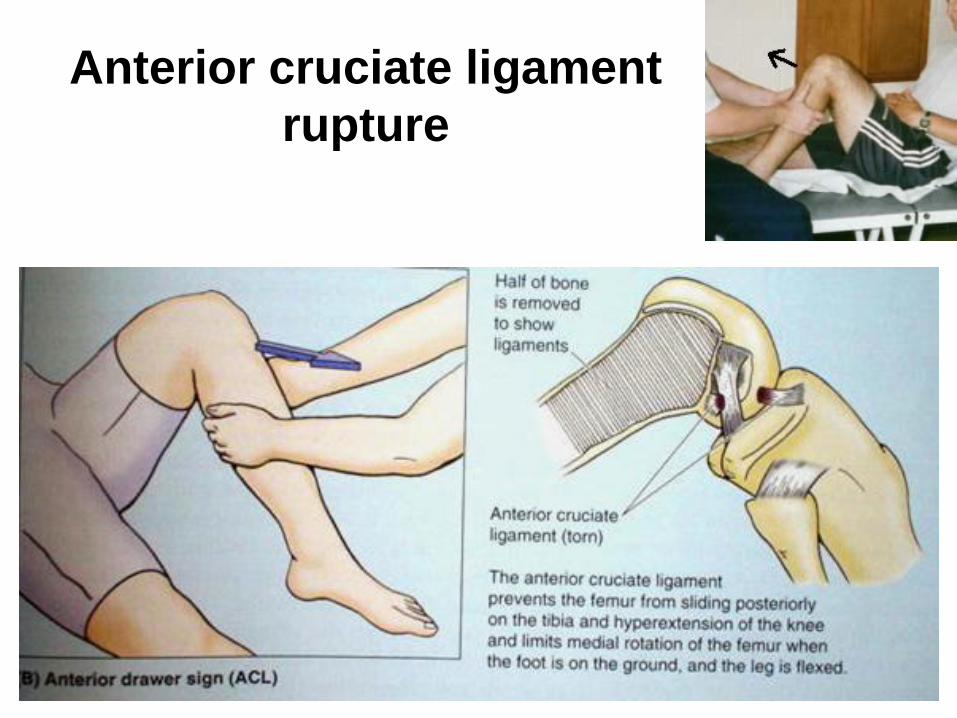
Anterior cruciate ligament
rupture

Posterior cruciate
ligament rupture

Movements
• Flexion
• Extension
• Medial & lateral rotation
• Locking/unlocking
– Locking—During extension medial rotation of femur
– Unlocking—lateral rotation of femur by popliteus

Locking and
unlocking of the knee
•Femur rotates medially on full extension (due to shape of the articularsurfaces)
•Because of rotation of the femur, all the ligaments becomes tight and thus knee locks in extension
•For flexion to begin, the femur must rotate laterally to relax the ligaments, then flexion starts.• Popliteus is the muscle to rotate femur and unlock the knee
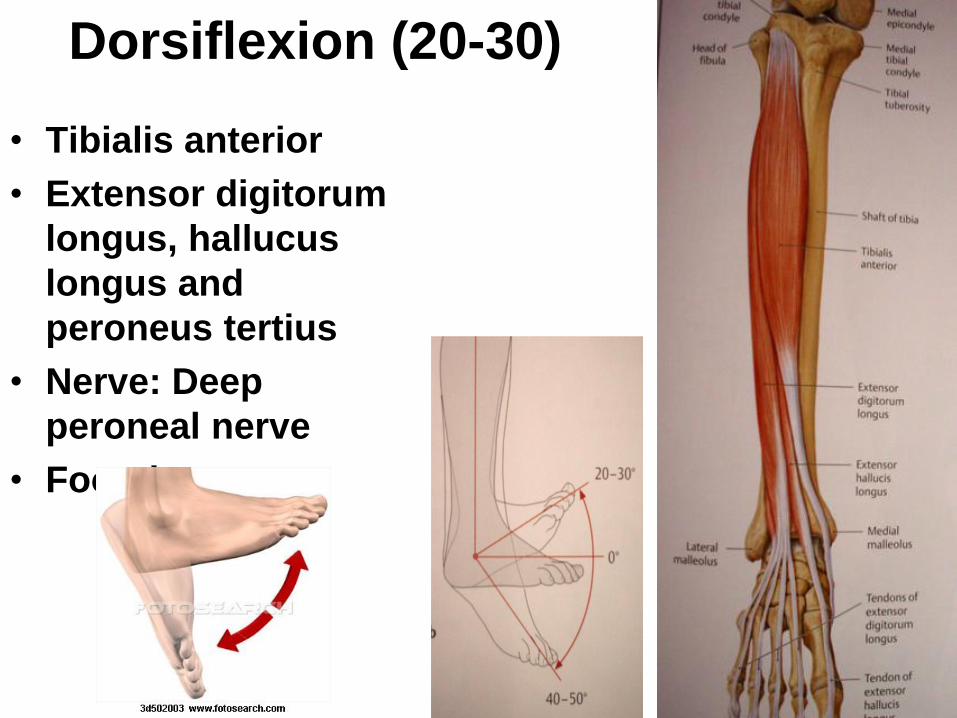
Dorsiflexion (20-30)
• Tibialis anterior
• Extensor digitorum
longus, hallucus
longus and
peroneus tertius
• Nerve: Deep
peroneal nerve
• Foot drop

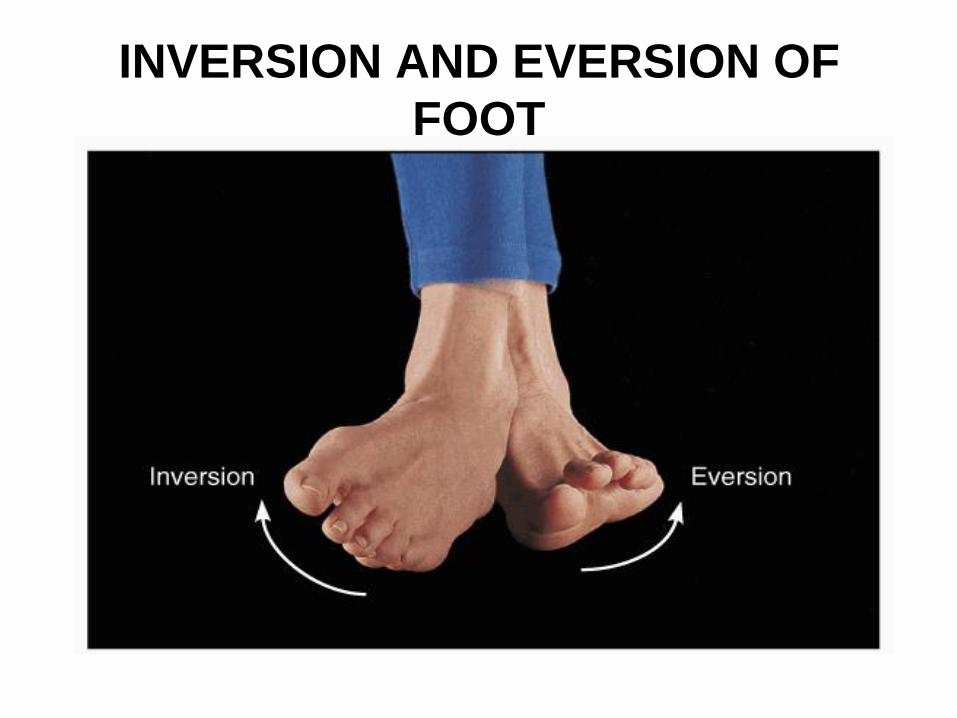
INVERSION AND EVERSION OF
FOOT
• Definitions.
o Inversion.
• Movement of sole of the foot towards the median
plane, e.g. ,when you examine the sole of your
foot.
o Eversion.
• Movement of the sole of the foot away from the
median plane ,e.g. , when the lateral surface of
the foot is raised.
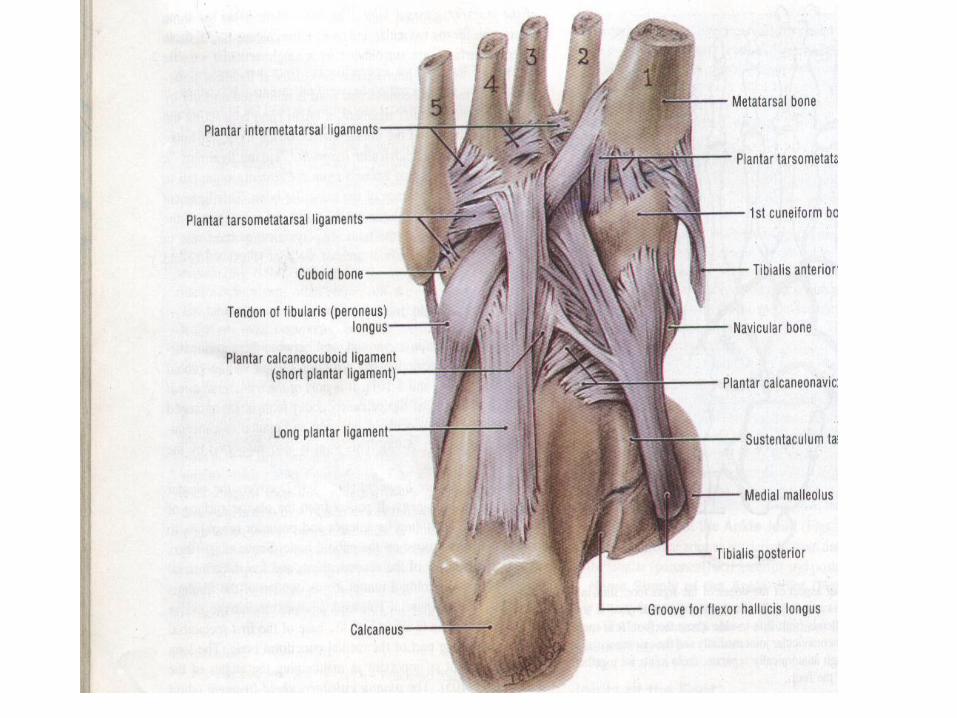
INVERSION AND EVERSION OF
FOOT
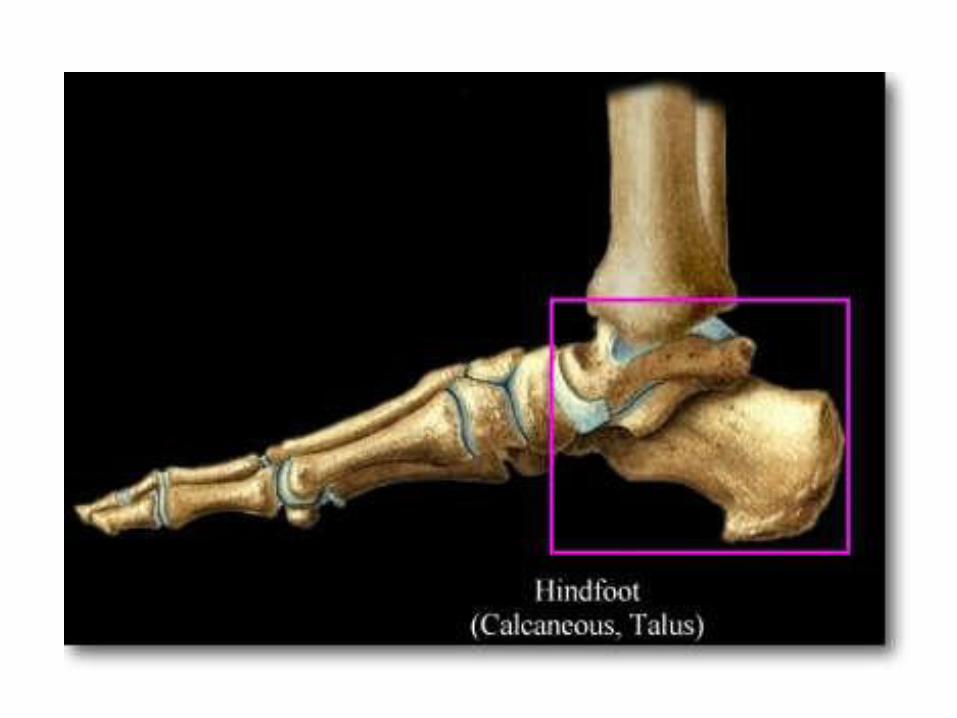

SUBTALAR JOINT
• Synovial joint between inferior surface of
body of talus and the superior surface of
calcaneus
• Surrounded by articular capsule which is
attached to articular margins
• Capsule is supported by medial, lateral
and posterior talocalcaneal ligaments
• Capsule is lined by synovial membrane

MIDTARSAL JOINT OR
TRANSVERSE TARSAL JOINT
• Consists of talocalcaneonavicular and
calcaneocuboid joints
• Movements occuring at this joint are
inversion and eversion


NEED FOR INVERSION AND
EVERSION
• Inversion and eversion give ability to walk
across uneven surfaces.
• These movements are essential in; Turning at speed.
To lean sideways on a foot whose sole is flat on
the ground.

MUSCLES PRODUCING
INVERSION OF FOOT
• Tibialis anterior and Tibialis PosteriorMuscles are responsible, assisted byFlexor and Extensor Hallucis LongusMuscles
• Tibialis Anterior dorsiflexes and TibialisPosterior planterflexes the foot at theankle joint and these opposite effectscancel each other out to produce anuncomplicated inversion of foot


MUSCLES PRODUCING
EVERSION OF FOOT
• Peroneus Longus and Peroneus Brevis
are responsible, assisted by Peroneus
Tertius.
• The former two are plantarflexors, and the
last is dorsiflexors of the ankle joint
• These opposite effects cancel each other
out when the three muscles combine to
produce a simple eversion of foot

SUBTALAR JOINT – Open
Kinematic Chain Motions

BIOMECHANICS OF INVERSION
AND EVERSION
• All the muscles producing inversion and
eversion are attached to fore foot
• Inversion and eversion begins at midtarsal joint
• The rotatory force is than transmitted to the
subtalar joint
• Most of the full range of inversion and eversion
occurs at subtalar joint

BIOMECHANICS OF INVERSION
AND EVERSION
• The axis of inversion - eversion
movement
It is along an oblique line passing from the
lateral tubercle of the calcaneus upwards,
forwards and medially through the neck of the
talus, bisecting the medial part of the tarsal sinus
The lines of pull of the muscles lie at the right
angles to this obliquity, so the muscles act to
best mechanical advantage

BIOMECHANICS OF INVERSION
AND EVERSION
• Mechanically there are four lines of pull
1) Tibialis Anterior, which inverts the foot at tarsal joint and dorsiflexes the foot at ankle joint
2) Peroneus Tertius, which everts the foot at tarsal joints and dorsiflexes the foot at ankle joint
3) Tibialis Posterior, which inverts the foot at the tarsal joints and plantarflexes the foot at the ankle joint
4) Peroneus Longus and Brevis, which evert the foot at tarsal joints and plantarflex the foot at ankle joint

INVERSION AND EVERSION OF
FOOT
• Injuries associated with Inversion and
Eversion of Foot
1) Forced Eversion of the foot
Pott’s Fracture
2) forced inversion of the foot
Ankle Sprain



FORCED EVERSION

Initial Contact Mid Stance Terminal Stance
Pre-Swing Initial Swing Terminal Swing
The Gait Cycle



05/10/2010 NAS 95
Thank you