review of literature and methodologyshodhganga.inflibnet.ac.in/bitstream/10603/15411/9/09_chapter...
TRANSCRIPT

CHAPTER II
Review of Literature and Methodology
Introduction .
Understanding the provision and use of health care services and their determinants, especially
in developing countries like India constitutes a difficult task, especially since the health sector
is not a homogenous entity. However, information regarding the provision, the morbidity
patterns, the access and use of health care services for treatment, and the cost of treatment is
necessary to enable policy decisions for intervention and regulation of the health care sector.
As stated in the introductory chapter, our concern in the present study is the process involved
in the provision, access and utilization of health care services. The existing theoretical and
empirical literature on the health sector, mostly rela~ed to access and utilization are reviewed
here. The approach to the study of these issues and the methodology to be followed would
also be outlined in this chapter.
The chapter is divided into the following sections. In the first section, the issues involved in
understanding questions of access and utilization of the health sector are discussed. Then, the
empirical literature on these issues is reviewed and using this, a conceptual framework for the
analysis is developed, specifying its methodology and the plan for data collection.
2.1 The Specificity of the Health Care Services
The health care sector is different from the other sectors in the economy because of the
distinctive features of 'health care'. Health care is not an output; rather it is an intermediate
good, a process, for achieving health. Nor is health care a homogenous good. Since health
care is thus a commodity totally different in its characteristics from all other commodities,
several scholars have argued that the application of the utility theory of neo-classical
economics in the analysis of the health care sector is of little validity. They have advanced a
large number of reasons in support of the argument, a few of which are mentioned below.
The Absence of a Rational and Informed Consumer: First of all, the rational and informed
consumer of health care is more an ideal than a reality. Health care is a heterogeneous
intermediate commodity and it is not consumed for its own sake. It is people's perception as to
what the levels of health should be that determines the type and extent of health care

consumption. The health care demand increases when individuals' understanding regarding
the health care needs improves. However, since an informed consumer need not necessarily
have a rational perception of health, the neo-classical assumption of a rational consumer is not
valid in the case of the commodity - health care.
Superior Role of Supplier in Decision-making: Secondly, in the health care market, supply or
the supplier) is an important determinant of demand. This is so manifest in health care that
even the normal duality of supply and demand cannot be maintained. The physician often
knows a great deal more than the patient does about the patient's need for various types of
care. Although the supplier induced demand hypothesis is not conclusively and empirically
verified, it emerges from many studies that the increased supply of health care providers,
instead of lowering demand, has normally increased it by increasing the number of surgeries,
the quality of drug consumption, etc. (Auster and Oaxaca; 1981, Green; 1988, Fuchs; 1978).
Additional complications result from the possibility that physicians might shift the nature and
intensity of patients' demand (Sloan and Feldman; 1978, Evans; 1974). Some economists
concede that physicians have the power to shift demand but believe that the power is
sufficiently and uniformly exploited so that the possibility of shifting could be ignored. Others
argue that the amount of shifting varies with exogenouS changes in the physician/population
ratio. This follows from a model in which physicians maximize utility as a function of
income, leisure and "correct practice".
Process More Important; No Knowledge of Possible Outcome: Thirdly, in health care, the
process utility often occupies a more important position than outcome utility. The process
involves decision-making, risk bearing and equity. This is so because decisions are taken
amidst uncertainties of outcome and risk involved in obtaining the outcome. Thus, there is no
guarantee that health care consumption would automatically ensure actual utility gains. In this
situation, the consumer tends to off load responsibility of decision-making on the doctor who
has to bear the moral burden of the decision.
Uncertain Occurrence of Disease: Fourth, because output of health care cannot be stored and
short run supply of health care is relatively inelastic, its productivity is sensitive to changes in
demand. The stochastic nature of the demand for health care results in excess capacity, and the
problem is exacerbated by systematic variation in demand according to days of week and months
7

of year. The problem of measuring output also increases the difficulty of analysing demand for
health care.
Product Uncertainty: Another feature of health care is product uncertainty. Uncertamty as to the
quality of the product is perhaps more intense here than in any other case. Recovery from disease
is as unpredictable as is its incidence. In most commodities, the possibility of learning from own
experience or experience of others is strong because action would be preceded by adequate
number of trials. In the case of severe illnesses, this proposition is not, in general, true;
uncertainty due to inexperience adds on to the intrinsic difficulty of prediction.
Further, there is a special quality to the uncertainty involved; it is very different on the two sides
of the transaction. Because medical knowledge is so complicated, understanding on the part of
the physician as to the consequences and possibilities of treatment is necessarily much greater
than that of the .. patient; or at least it is so believed by both the parties. Further, both parties are
aware of this informational inequality, and their mutual relationship is coloured by this
knowledge.
While these features are peculiar to health care, the commodity itself being of a heterogeneous
character, the features could differ across categories within the health care sector.
Categories of Health Care
The commodity "health care" may be classified according to its categories: - curative care,
preventive cares that is !1atient-related, and promotive care that is not- patient-related. Curative
care category of health care includes personal services (care of patients) and facilities rendered
by health care providers and purchases of medicine. Curative care may be subdivided into "first
contact services" (all outpatient) and "referral services" (inpatient and some outpatient). Patient-
related Preventive care includes services to well patients - particularly infants, mothers and
pregnant women- delivered through maternal and child health clinics at health care facilities and
community health programmes. Typical services are immunization, growth monitoring, and
instruction on improved breast-feeding and weaning practices. Non-patient related promotive
care includes disease control (both vectors control and mass campaigns), sanitation, education
and promotion of health and hygiene, control of pests and zoonotic diseases, and monitoring of
disease patterns. In the case of preventive care services not related to particular patients, no
direct transaction takes place between the supplier of the service and any particular clients. Also
8

the extent of benefit to the beneficiaries is not easy to measure. Therefore, it is not feasible to
charge individuals who benefit from the service. Nor is it possible to think in terms of measuring
the demand and the utilization aspects of these services. Patient-related preventive health care
and curative care renders personal benefits to patients. In the case of the former, it is not only the
patients concerned, but others also, who are benefited by protection from ill health. In the case of
curative care, the benefits are mainly conferred to the direct users.
Public, Private and Merit Good Aspects of Health Care
On the basis of the nature of benefits provided to the society and the nature of provision
required, goods and services are usually classified into public goods and private goods. There
are two important characteristics of a public good which distinguish it from private goods.
The first is the non-excludability characteristic; i.e., it cannot be denied to those who cannot
or will not be paying for its use unlike in the case of. other goods sold in the market. The
second is non-rivalry; i.e., there is no rival character, which means that one individual's
consumption of such goods does not affect other individuals' consumption of the same. Public
goods confer their benefits generally without discrimination to all inhabitants of the relevant
'area. That is, there are general benefits, but no specific benefits to any particular individual.
On the other hand, private goods confer specific benefits to specific individuals while the
society at large may not directly benefit from such services. There are certain services that
provide private, specific and individual benefits and at the same time provide social benefits
also; but the magnitude of the public and the private benefits they render may not be of
comparable magnitudes. Such services are often termed as merit goods.
Health care is a\ product consisting of a variety of services provided by the health personnel,
hospitals, public health programmes, etc., each of which has its own distinctive economic
characteristics. The nature of benefit these services offer differ according to the category of
health care. Non-excludability and non-rival ness of its benefits characterize health care that is
non-patient related. On the other hand, while patient-related health care provides specific or
private benefits to the users, others are also benefited from its use. Curative care, on the other
hand, refers to services, which provide private benefits; they may not provide any for general
social health. Health care services maybe classified into public goods, merit goods and private
goods. Usually, all the non-patient-related preventive care (direct and promotive and educational
aspects of it) is categorized as a public good, while patient-related preventive care is classified as
a merit good. All public health services such as water supply, sewage and refuse disposal,
9
clearing of central sources of infection, etc, come under public goods. Curative care (personal
health services) may be treated as a private good as it provides private benefits and makes no
specific contribution to public health.
The Public- Private Debate in Health Care Provision
The dichotomy between the state and the market has led to polarization of policy positions in the
provision of health care as has been the case with several other economic spheres Charles Allan
(1988) classifies the two positions into paternalists and liberals of health care economics.
Paternalists, believing that health care has unique economic characteristics (of public good,
merit good, etc), which deviate from the basic pre-requisites of competitive market model,
argue in favour of free provision of health care services by the state. Liberals, on the other
hand, claiming that health care is in no significant way different from other economic goods
and services, plead for leaving its provision to the private market l . Donabedian (1971) has
admirably dissected this ideological issue by polarizing these attitudes around two viewpoints,
"libertarian" and "egalitarian". In the libertarian view, access to health care is part of society's
reward system and at the margin at least, people should be able to use their inc~me and wealth to
get more or better health care than what their fellow citizens wish they should. In the egalitarian
view, access to health care is every citizen's right and this ought not to be influenced by income
or wealth.
Some economists argue that public provision of health care is required because of the failure of
markets and the consequent existence of inequality in the health market2. Thus there are two
broad sets of reasons that may justify government activity in the health sector - market
failures and inequality. Examples of market failures in the health care market are imperfect
competition among suppliers, imperfect information among consumers, and externalities.
IThe tenns 'Paternalists' and 'Liberals' were used to denote the supporters of the state and market respectively by Allan (1971). Arrow, Allan, Musgrave, Klannan, Wisbrod, etc advocate the Paternalist position while the two main proponents of the Liberal stand are Buchanan and Lee who belong to the radical liberalism (Libertarianism) of Milton Friedman's variety. 2The point of departure for the theory of market failure is provided by the First theorem o/Welfare Economics. This proposition states that in the absence of external effects and public goods, every competitive eqUilibrium (Le., an allocation in which every consumer maximizes utility and every producer maximizes profit, and the resulting individual plans are compatible) constitutes a Pareto optimum. The significance of a market failure therefore first of all demands proof that at least one of the requirements cited in this main proposition of economics is not fulfilled in the case of health goods. Health goods have the following attributes. # Health goods have the characteristics of public goods; # The consumption of health goods give rise to external effects; # The production of health goods is characterized by increasing returns to scale; #The prerequisites of a perfectly competitive market, that is, market transparency and consumer sovereignty, are not met. (Zweifel and Breyer; 1997, p.128).
10

There are various ways in which markets are perceived to 'fail'. Failure may be split into
demand side failure and supply side failure. On the demand side, a major problem is that of
information asymmetry; i.e., one party. involved in a transaction may have more information
about the transaction than the other. In Pareto terms, it could lead to a trade-taking place
where both the parties believe that they can gain, but subsequently one of them finds that he
or she is worse off.
There may arise a perceived problem of demand in a free market due to inconsistency of
preferences or perhaps even irrationality of choice. Certain forms of government intervention
are at least in part based on this ground. A further problem may emerge -on the demand side,
in certain circumstances, due to the lack of incentive for individuals to reveal their true
preferences. The case of public goods could provide an example of this.
On the supply side, market failure may arise in cases in which private costs of production do
not coincide with social costs of production. One instance of this would be that of under
valuation by the market, of the social value of production. This is the notion of merit goods
(Munday; 1996). Another example would be of social costs of production exceeding private
costs. This is a case of negative externality. A further problem on the supply side may arise
where economies of scale exist. In this case, there will be a tendency towards monopoly (or
at least movement away from competition) as firms have to be large in order to reduce costs.
In this situation, price will be significantly different from marginal cost and firms may lack
the incentive to minimize production costs if they wish to pursue other goals.
Among the numerous kinds of justifications for government intervention, Arrow (1963) had
emphasized the uncertainty elements in the demand for and supply of medical services.
Weisboard (1961) had developed the implications of an option demand characteristic, which
indicates that private provision· of health facilities may be 'sub optimal'. Pauly (1967) had
explored the role of externalities of consumption in the demand for medical care. Lindsay (1969)
had emphasized the apparently universal desire and willingness to "share" - the attitude often
expressed that every one should have "equal access" to the medical resources available - as the
rationale for collective provision of health services. The health sector market lacks the usual
attributes of market forces necessary to become efficient. Khan and Berman (1993) argued that
health care is a commodity that is widely traded in a chaotic private market place where the
consumer often feels helpless and ignorant and therefore government intervention IS
11
indispensable. Libertarians contend that the joint consumption of public health services deviates
from the precepts of the ideal market economy making it inefficient in the allocation of
resources.
Concerns over equity have been seen as the major jl,lstircation for government intervention in
the provision of health services. A private market for health care could be Pareto efficient and
yet provide no services to members of the popUlation who were uninsured and too poor to pay
for these services. Thus, the argument is that the role of government in this context should be
based on considerations of equity and efficiency. The principal rationale for a public health care
system is the reduction of inequality in society. In the case of medical care, equality would mean
that the health care given to an individual depends solely on his medical conditions and
symptoms, not on his ability or willingness to pay. This is what Tobin (1973) called the case for
specific egalitarianism, that certain specific scarce commodities should be distributed less
unequally than the ability to pay for them.
Health care services, which partake of the characteristics of public good, private good and
merit good, could be provided by public or private agencies. However, this characteristic of
health care services raises the question as to who should provide what kind of health care
services and on what basis or for what purpose. There are strong advocates for government
role in the provision while at the same time those who argue for the market's role in deciding
the provision are equally vehement. However, the provision of public goods has remained the
domain of the government sector even in market economies as it was expected that private
providers would shy away from their provision due to lack of incentives, or little scope for
profits, as they cannot charge user fees. Even in the case of merit goods, market is not
considered th~ appropriate dominant provider. Because of this, the 'market-versus-state' debate
as to "who shall provide health care" focuses on the nature of the different categories of the
commodity 'health care', and not on 'good health' or 'health care' as such.
Preventive care comes closer to a public good than curative care does; in a public good,
excludability of customers is rather impossible. Thus, government intervention is considered -,
essential for preventive care. In the case of curative care, the services fall at the other end - in
the broad category of merit goods, or even private goods, since they exhibit features of either
public utilities or even of other normal goods. Curative care has a market since it is possible
to identify beneficiary of such services and to levy a charge on himlher in return for the
12

services. Thus it constitutes a service that a private provider would be interested in providing.
However, there exists the opposite view also that curative care should be provided only by the
public sector. This view is based on considerations of equity and efficiency.
Different Provisions of Health Care
The production and distribution of medical services in a country is determined by decisions made
about the amount of resources to be spent on different types of services, the methods for
producing those services, and the delivery modalities for the provision of health care to the
population (Marquez 1990). Each constituent in the structure would be different from others in
terms of the resources invested in the health infrastructure, the system of payments, degree of
technological sophistication, research capabilities and innovative strategies, location and relation
to the government. In all countries, entry into the profession is restricted by licensing to
guarantee minimum professional quality. The type and the quality of services provided by each
constituent of the health care system would be different yet interdependent and overlapping in
nature. The interdependent and overlapping nature of services accentuates the problem of
identifying the exact role of a particular constituent. Because of these problems, it is also quite
difficult to define a particular segment of the health care system in the totality.
Irrespective of whether health care belongs to the domain of public sector or private sector, it
is expected to serve the society's need optimally. However, such expectation often remains in
the realm of theory; in reality, functioning of the health care system often falls short of
expectations. Allan Williams (1988) tried to capture the theoretical/ ideological debate on
supply of and demand for medical care in the public-private spheres and presented reality in a
nutshell as shown in Table 2.1 and Table 2.2.
13
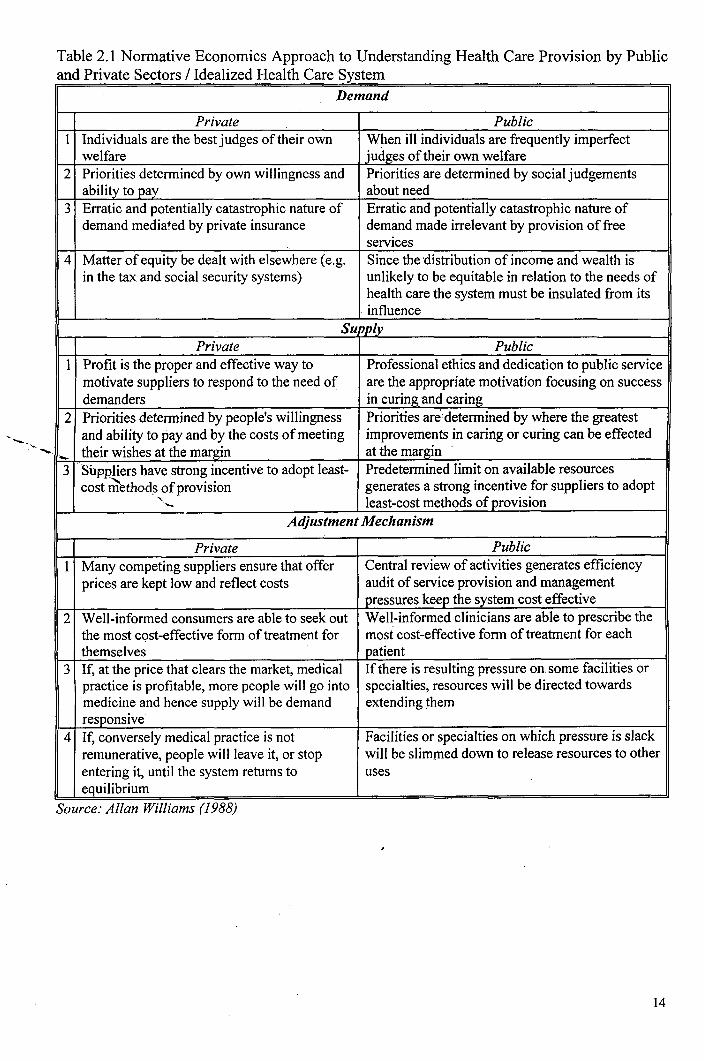
Table 2.1 Normative Economics Approach to Understanding Health Care Provision by Public and Private Sectors / Idealized Health Care System
Demand
Private Public 1 Individuals are the best judges of their own When ill individuals are frequently imperfect
welfare judges of their own welfare 2 Priorities determined by own willingness and Priorities are determined by social judgements
ability to pay about need 3 Erratic and potentially catastrophic nature of Erratic and potentially catastrophic nature of
demand mediated by private insurance demand made irrelevant by provision of free services
4 Matter of equity be dealt with elsewhere (e.g. Since the distribution of income and wealth is in the tax and social security systems) unlikely to be equitable in relation to the needs of
health care the system must be insulated from its influence
Supply Private Public
1 Profit is the proper and effective way to Professional ethics and dedication to public service motivate suppliers to respond to the need of are the appropriate motivation focusing on success demanders in curing and caring
2 Priorities determined by people's willingness Priorities are determined by where the greatest and ability to pay and by the costs of meeting improvements in caring or curing can be effected
- their wishes at the margin at the margin
3 Suppliers have strong incentive to adopt least- Predetermined limit on available resources cost ~thod~ of provision generates a strong incentive for suppliers to adopt
"- least-cost methods of provision - Adjustment Mechanism
Private Public 1 Many competing suppliers ensure that offer Central review of activities generates efficiency
prices are kept low and reflect costs audit of service provision and management pressures keep the system cost effective
2 Well-informed consumers are able to seek out Well-informed clinicians are able to prescribe the the most cQst-effective form of treatment for most cost-effective form of treatment for each themselves patient
3 If, at the price that clears the market, medical If there is resulting pressure on. some facilities or practice is profitable, more people will go into specialties, resources will be directed towards medicine and hence supply will be demand extending them responsive
4 If, conversely medical practice is not Facilities or specialties on which pressure is slack remunerative, people will leave it, or stop will be slimmed down to release resources to other entering it, until the system returns to uses equilibrium
Source: Allan Williams (1988)
14

Table 2.2 Actual Health Care System Demand
Private Public I Doctors act as agents, mediating demand on Doctors act as agents, identifYing need on behalf of patients.
behalf of consumers. 2 Priorities determined by the reimbursement Priorities determined by the doctor's own professional
rules of insurance funds. situation, by his assessment of the patient's condition and the expected trouble-making proclivities of the patient.
3 Because private insurance coverage is itself a Freedom from direct financial contributions at the point of profit seeking activity, some risk rating is service and absence of risk rating enables patients to seek inevitable, hence coverage is incomplete and treatment for trivial or inappropriate conditions. uneven, distorting personal willingness and ability to pay.
4 Attempts to change the distribution of income Attempts to correct inequities in the social and economic and wealth independently are resisted as system by differential compensatory access to health services destroying incentives (one of, which is the leads to resource to health care in circumstances where it is ability to buy better or more medical, care if unlikely to be cost-effective solution to the problem. you are rich).
Supply Private Public
I What is most profitable to suppliers may not be Personal professional dedication and public spirited what is most in the interests of consumers and, motivation Iiktlly to be corroded and degenerate into cynicism since neither consumers nor suppliers may be if others, who' do not share those feelings, are seen to be very clear about what is in the formers interest, doing very well for themselves through blatantly self-seeking this gives suppliers a range of discretion behaviour.
2 Priorities determined by the extent to which Priorities determined by what gives the greatest professional consumers can be induced to part with their satisfaction. money and by the costs of satisfYing the pattern of 'demand'.
3 Profit motive generates a strong incentive Since cost-effectiveness is not accepted as a proper medical towards market segmentation and price responsibility, such pressures merely generate tension discrimination and tie-in agreements with other between the 'professionals' and the 'managers'. professionals.
Adjustment Mechanism Private Public
I Professional ethical rules are used to make Because it does not need elaborate cost data for billing overt competition difficult. purposes, it does not routinely generate much useful
information on costs. 2 Consumers denied information about quality Clinicians know little about costs and have no direct incentive
and competence and if insured, may collude to act on such information as they have and sometimes even with doctors (against the insurance barriers) in quite perverse incentives (Le., cutting costs may make life inflating costs. more difficult or less rewarding for them).
3 Entry into the profess~on made difficult and Very little is known about the relative cost-effectiveness of numbers restricted to maintain profitability. different treatments and, even when it is, doctors are wary of
acting on such information until a general professional consensus emerges.
4 If demand for services falls, doctors extend The phasing out of facilities that have become redundant is range of activities' and push out neighbouring difficult because it often threatens the livelihood of some disciplines. concentrated specialized group and has identifiable people
dependent on it, whereas the beneficiaries are dispersed and can be identified only as 'statistics'.
Source: Allan Williams (1988)
The forgoing facts highlight the divergence between the expected health care practices and
prices and the actual situation. The question of incentive frameworks operating against ethical
considerations in the provision and utilization of health care services becomes relevant. The
15

issue pertains to the provider-user/ agent-user/physician-patientlsupplier-user relationship in
health care sector.
On the supply side are physicians who are the prime players in the provision of health care
services. In fact, most of the theoretical literature looks at the health care sector in an agency
modelled relationship between physicians and patients. As observed by Redisch (1978), it is
the physician who recommends admission, takes responsibility for ordering diagnostic
procedures and therapeutic measures and determines when the patient is fit to leave the hospital.
As Zwifel and Breyer (1997) pointed out, physicians playa key role in the production and
distribution of medical services. The behaviour expected of sellers of medical care is different
from that of businessmen in general. These expectations are relevant because medical care
belongs to the category of commodities for which the product and the activity of production
are identical. In such cases, the customer cannot test the product before consuming it, and
there is an element of trust involved in the relationshi~. A physician's behaviour is supposed
to be governed by a concern for the customer's welfare, which would not be expected of a
seller. There is a 'collectivistic-orientation' that distinguishes medicine and medical
profession from business in which self-interest on the part of participants on both sides is the
accepted norm. Advertising and overt price competition is virtually absent among physicians.
Advice given by physicians on further treatment by him or others is supposed to be
completely divorced from co~siderations of self-interest. Again, it is claimed that treatment is
dictated by the objective needs of the case at hand and not governed by financial
considerations. The physician is relied on as an expert in certifying the existence of illnesses
and injuries for various legal and other purposes. It is socially expected that his concern for
the correct conveying of information will outweigh his desire to please his customers. Hence,
it is obvious that 'the usual market forces do not determine the optimum service, but that the
health care services are supplier (physician) determined.
In most industrialized countries, the medical profession enjoys steadily increasing popularity as
an occupational choice, perhaps more so than any other area. It combines two features that attract
people, viz. the fulfilment of the desire to help other people and the expectation to earn above
average income. However, licensing restricts entry into the profession and thus the supply of
providers.
16

Physician Density and Utilization of Medical Services: Alternative Explanations
The peculiar type of relationship between supplier (physician) and demander (patient) that exists
in the health care sector might playa key role in the creation of supplier-induced demand. The
most striking feature of the physician-patient relationship is the demander's incomplete
information about his true needs. A patient who consults his doctor knows only that he requires
some medical tr~atment (of the diagnostic or therapeutic type) because he is not satisfied with his
health status. Thus he delegates the choice of treatment to the better- infonned doctor while
deciding merely whether or not to follow the doctor's advice and comply with his prescriptions.
Not even in this decision is the patient completely sovereign, as there is a consensus among
physicians and patients that the patient's confidence in the doctor's competence is an important
pre-condition of successful treatment. This means that the demand curve, which depicts the
quantities of planned utilization of medical treatment at alternative prices, predominantly mirrors
the decisions of suppliers, not of demanders of medical care. In the limit, the demand for medical
services is thus totally supplier determined
This relationship does not pose any problem as long as the physician acts as a perfect agent for
the patient, choosing what the patient would have chosen had he possessed the necessary "
technological knowledge. It does become a problem, however, as soon as own interests begin to
influence the doctor's decisions taken on behalf of the patient. Doctors might supply distorted or
inadequate infonnation to their patients systematically consequent on an increase in physician
density in their area of operation, in order to retain or ensure their own full employment; or there
might exist monopoly conditions in the medical market of the locality. In either case, supplier
detennined demand turns into supplier-induced demand.
If it is possible for doctors to boost the demand for their services at their own discretion, then the
very distinction between supply and demand loses its relevance. According to the "supplier
induced demand" hypothesis, the amount of services transacted in the market is exclusively
detennined by supply as desired by the physicians. The "demand" required to match supply is
created artificially through the advice given to patients, whether or not medically appropriate
(Zwiefel and Breyer, 1997, p.205).
Thus due to his superior infonnation, the physician exerts considerable influence on the patient's
demand. "Supplier-induced demand", however, prevails only if physicians act not as perfect
17

agents but according to their own interests, in particular by systematically modifying the
information provided to patients in response to an increase in physician density with the aim of
. ensuring own employment.
"Supplier-induced demand" for medical services explains how utilization of medical services per
capita grows with increasing physician density, even assuming constant prices of medical
services. This explanation is based on the hypothesis that physicians exploit the delegation of
decision-making powers by the patient to their advantage by prescribing medically useless
(ineffective) or economically inappropriate (inefficient) services. However, alternative
explanations of the same empirical phenomenon also exist. Three major explanations advanced
are the following.
Permanent Excess Demand: The observed correlation between physician density and utilization
of medical services may result from permanent excess demand on the market for medical
services, due to price regulation.
Decreasing Indirect Costs; Improved Quality of Treatment: The growth of service volume
associated with increasing physician density could also be the result of demand decisions by
rational patients. The opening of new practice, particularly in rural areas, reduces the average
time and transport costs of consultations. In addition, the average time spent in the waiting room
falls when physicians are less busy. As many diseases get cured without much medical
intervention, an early appointment with the doctor increased the probability of any disease
condition receiving medical treatment. Finally, the average amount oftime devoted by the doctor
per visit by a patient gets longer when the physician becomes less busy. As long as the duration
of a visit is deemed an essential quality characteristic by patients, increasing consultation time
serves the medical care demand at a given price to shift outward at a given price in response to
increased physician density in a locality.
Reversed Causality: - The third explanation for the observed positive statistical correlation
between physician density and per capita utilization refers to a reversed direction of causality.
When choosing a location for his practice, a young doctor would try to determine whether
demand is strong enough to generate a sufficient amount of revenue for him. Regions with high
demand for medical services should thus attract more physicians than those with low demand.
18

Consequently high per capita utilization of medical services leads to high physician density on
average (Zweifel and Breyer, 1997, p 211).
The joint occurrence of rising per capita utilization of medical services with rising physician
density does not conclusively prove that demand is created artificially by physicians. There
are other explanations as well: pre-existing excess demand may have declined, or indirect
costs to patients may have fallen; it is even possible that variations in the physician density
themselves could be the result of variations in the demand for medical care (Zweifel and
Breyer, 1997, P 212). However, the physician is not in a position to control the overall
hospital costs and hence, cost of in-patient treatment. The prices of medicines, overhead costs,
costs of surgery, administrative expenses etc., fall beyond the control of the physician. Hence,
the 'physician dominance' argument seems to be less relevant to overall pricing of health
servIces.
The preceding review of the conceptual and theoretical issues provides the background for a
critical appraisal of the empirical studies in the area.
2.2 Review of Literature
Provision and Physician Behaviour
At the outset it is necessary to mention that there have been hardly any studies in India on the
provision of health care services and physician behaviour patterns. While there do exist some
statistics regarding the number of government medical institutions, doctors and beds, there is
no or little information available on the practice behaviour of the doctors and utilization of
facilities. As a result, most of the studies available for review here are those done in other
countries. However, since the provision of facilities and behaviour and practices of health care
personnel in countries differ from one another due to the differences prevailing in the political
economy conditions and cultural environments, these studies that discuss the country-specific
situations are not adequate for guidance of our study. However, some issues dealt with in
these studies, relevant to our analysis of the provision of health care, are presented here.
These issues include (a) physician career choice, (b) choice of area for practice, (c) choice of
institution/site for practice, (d) practice behaviour in terms of pricing, and ( e) practice
behaviour in term~ of prescribing and treatment aspects; see Table 2.3.
19

Table 2.3 Issues and Outcomes of Empirical Studies in Health Care
Study Ma;orlssue Results 1 Physician Career Choice
1. Zuckerman (1977) Physician career choice Factors that determine the physician career choice are: socio-demographic characteristics, personality traits and institutional (structural) variables.
2. Frenk & Bhashshur Career preferences in Feasibility perception and opportUnity assessment in (1983) medicine terms of type of activity, site and institution are the
determinants IL Area of Practice and Practicinl{ Behaviour
3. Rimlinger Steele Spatial distribution of Patient income levels and the discriminatory pricing (1963) physicians by physicians. 4. Stevens (1989) American hospitals Hospital behaviours are not only determined by
behaviour purely economic considerations, such as output and factor prices, but also by the signals it received from the social environment.
5. Banks (1993) Price variations and The hospitals of same ownership type exhibit hospital behaviours different economic behaviour depending on the
socio-economic environment and the affluence of the area rather than mere urbanization determines the price.behaviour.
III Sector/Site For Practice and Pricing Practices 6. Roemer & Cost of hospital Costs include physician time donated to the hospital Friedman (1971) affiliation restrictions on physician behaviour and costs of
maintaining an acceptable Quality level. 7. Custer (1986) Physician choice of Determinants are the hospital characteristics, also
hospital affiliation and the increase in physician supply reduces their prices physician prices Monetary Returns for additional hours of practice
varied with total hours worked 8.Thornton and Eakin Utility maximization of More monopolistic in nature rather than (1977) single practitioners competitive. 9. Newhouse (1970) Market for physicians' If physicians are unable to maintain a target level of
service demand, they can still maintain a target income by increasing the fees in response to declining demand for their services.
IV. Practicing Behaviour in Terms of Prescription and Treatment 10. Lee (1964& 65) Prescribing behaviour Physicians' practice environment and interactions
of physicians. with pharmaceutical company sales representatives is the determininlZ; factors.
I I Joyce et af'(1968) Drug therapy decision Educations, quality of practice and whole-person making by physicians. orientation are the determinants.
12.Hemminki (1975) Prescribing quality. Time spend on patients affect the prescribing Quality.
13. Ray et al (1976,77 Prescribing behaviour Non-scientific prescribing is correlated with & 80); Becker et al of physicians. physician age, practice site (rural) and number of (1972) patients and type of degrees.
14. Schwartz (1989) Doctors' prescribing Influenced by the nature of demand for their service. behaviour of non-scientific and placebo medicines
20

V. Private-Public mix in Practice 15. Roemer (1993) Private-public mix A substantial proportion of public sector doctors
engage in private practice 16. Ferrinho et al Public doctors' private Switching between public and private practices is a (1998) practice fact due to (or in response to) the inability of the
public sector to sustain a credible system of health care delivery
VI Indian Studies 17. Bhat .R(1993) Role of private sector Regulatory and supportive policy interventions were
inevitable to promote private sector's viable and appropriate development
18. Berman, Peter Private health care Need for rethinking the health care system (1998) provision development strategies to acknowledge and, build
upon the opportunities offered by already extensive NGO health care sector.
19. Yesudian (1994) The private sector The existing regulatory mechanisms inadequate to health market in reduce the inequalities in the medical infrastructure Bombay and manpower, and controlling the rampant unethical
medical practice in private sector.
20. Nandraj and Physical standards in Rampant, unregulated, unplanned and largely Duggal (1996) private health sector in unmonitored growth of the private sector health care
Satara, Maharashtra. resulting in poor and unreliable quality of care and lack of standardization of practice behaviours.
21. Sukanya (1997) Factors influencing the More investment in corporate hospitals, leading to behaviour of private changes in the organizational and ownership hospitals structure of health care services in urban areas.
22. Rama Baru Private health sector in Social bases of privatisation of health care services, (1998) Hyderabad links between public and private complex social
processes through which it is shaped
23. TheICMR Health facilities Most PHCs are over- burdened, accessible only to a study (1991) few and there are regional variations in terms of
area coverage. Also face problems of inadequate drugs and medicine supply, poorly equipped treatment facilities etc.
24. Kabra (1991) Private health facilities Despite increase in size, failure of private sector health care in maintaining the basic minimum standards.
Apart from the above-mentioned studies, a few studies in India .. on the health care sector have
also dealt with selected aspects of the provision of health care. These studies may be broadly
classified under (a) health infrastructure; (b) human resources in health sector and (c)
organizational dynamics in the health care system.
Most of these studies have looked into the government sector III tenns of infrastructure
development and health care activities. The key topir' i functioning
,,-a\ N elJ "-" ,\' ,...-,---. /" \
~y. " :J >~ ""i l ;· ,\.~, I .". '" I). ; )
~~:. dry; / ,,", ~ ;
I 11111111 1111 III 111111 11111 11111 11111 11'1 1111 TH-9411
21

of Primary Health Centres, and Sub centres; location and coverage of various health care
institutions; and performance of the various centrally-sponsored health programmes. The various
health care programmes launched by the government such as government health centres, health
programmes, community health schemes, and health care management, have also formed topics
of discussion in many of them (Mc Pharil et al; 1991, Bhatnagar; 1982, Somanath Roy; 1987
etc.).
Studies on the public health system have brought to light the fact that while government medical
institutions are expected to tackle a full range of health care responsibilities, they are not
equipped with adequate facilities and infrastructure. Most of the studies have suggested the need
for quality improvement of the services provided through these medical institutions (Chauhan et
al; 1985, ICMR; 1991 etc.).
A major chunk of studies in the Indian context have 100K~d at the various aspects related to the
staff of health centres in India. While such studies about staffing in the private health care sector
is grossly inadequate, enquiries made in the NGO sector have examined the role and the
performance of health functionaries with particular emphasis on the aspect of training of health
care personnel. The key topics covered under this group of studies include (a) levels of staff
functioning and performance; (b) nature of work responsibilities; (c) allocation of time for
various activities; (d) adequacy of supervision; and (e) staff motivation. With some exceptions
(like Jesani et. al; 1992) studies on health human-power have approached the issues related to
health staff from an operational, rather than a social or economic point of view. Only a few , studies have looked at the conditions of working for the staff of the private health care
institutions. The study on the earnings of private doctors in New Delhi (Kansal; 1992) makes
mention that the service conditions of the lower level staff in private hospitals and nursing homes
are miserable.
Utilization of Healtlt Care Services
Research conducted on health seeking behaviour (demand for health care) and utilization of
health care services in developing countries is of both theoretical and practical relevance. It
analyses the concepts of the origin and management of illness, provides insights into people's
use or non-use of traditional and/or modem health services available and fmally contributes to
perceptions on health care in particular settings.
22

Since Anderson (1992) and his colleagues did model for health service utilization (which we
shall discuss later), a great deal of research has been carried out hi developed countries on the
factors that influence health service utilization. The issues that were dealt with by such studies
come under ( a) morbidity related issues in utilization of health care, (b) individual characteristics
related issues of utilization, (c) socio-economic and community-related factors in utilization, (d)
access to health care in terms of geographical/spatial proximity related factors in utilization, (e)
access in terms of costs and affordability related factors in utilization, and (f) quality of services
related factors in utilization.
Table 2.4 Factors Determining the Utilization of Health Care Services .~.
Authors of Studies Results Morbidity Related Factors
Heynes (1991) Morbidity differentials are important. Stein and Muir (1986), Sharp et al (1983), Recognition of the illness is important factor in use. Tanner et al (1983) and Zola (1966).
Young (1981), Abbas and Walker (1986), Severity 'of illness is the important factor. Cosminsky and Scrimshaw (1980).
Fassin et al (1988) Cause of illness related factors
Individual Characteristics Acton (1975), Cleary et al (1982), Marcus 7 Role of sex.differentials in utilization behaviour-Siegel (1982), Melnger (1986), Nathansen women tend to be relatively more responsive to price (1977), Sindelar (1982), Verbrugge (1976& changes in the use of health care services. 1985), Wilensky& Cafferata (1983), Hunt- Reasons for gender differences in utilization include McCool et al (1995), Sabir & Ebrahim (1984), factors such as biological differences, differences in Y ohannes & Sstreatfield (1988), Soman et al the preference of care, life style differences and risk (1991), Keonig & D'Souza (1986), Monica aveiting behaviours, and traditional role of women. DasGupta (1987) and Levine (1987). Gabriel (1994), AI-Sekait (1988), Bambang Age asa factor. (1993), Alaka Basu (1990).
Alaka Malwade Basu (1990), Caldwell (1979), Education and Occupation as factors. Cleland & Van Ginneken (1988). Selwyn (1987) Family Size as a factor in utilization
Societal Factors Ashraf et al (1982) Socio-economicstatus of the user Nations MK (1985) Success of the health interventions rests on the ability
to conform to people's life styles Basu AM (1990) Cultural and regional identities had an important
bearing on the knowledge, attitudes and practices relevant to the use of health care facilities.
Brink and Nader (1981) Social class and ethnicityplay roles in utilization
23

Costs & Affordability Factors Asenso-Okyere et al (1998). Cost recovery policies (user fees in public services)
leads to increase In self-medication and other behaviours aimed at cost saving.
Heller (1982), Akin et al (1986) and Hancock Willingness to pay for health care was not (1993). necessarily affected by household's ability to pay. Mwabu (1995), Waddington and Enyimarayew Apart from ability to pay, other socio-demographic (1990) and health related factors also affected households'
willingness to pay for health care.
5. Multiple Factors Determining Health Service Utilization Berkanovic et al (1981). Need (illness level), social structure, organization of
care, general social network pattern and personal believes specific to the symptoms are the factors affecting health service utilization.
Wan and Soifer (1974). Need, cost, health insurance coverage and age are the important factors in utilization of health services.
Anderson and Aday (1978). Main determinants of health service use are the age and level of illness.
Kekki (1980). Use of health services is most influenced by sex, cost of servIce; illness level, socio-economic status and social and societal ne~ork systems.
Access in Terms oj Geographical Proximity Gester and Meade (1988) Distance to the health service more important than
other issues in utilization. Shannon et al (1969 & 1973) and Studnicki Distance and travel time both serve as barriers to (1975). patient movement. Morril et al (1968 & 1970). Patients travel further, on an average to higher order
medical centres, which provide specialized services, than, to smaller, less specialized community hospitals.
Mayer (1983). Distance behaviour of patients varies depending on their particular diagnoses and on the treatment and diagnostic procedures.
Akin and Hutchinson (1999). Bypassing local subsidized public health facility is not very different across income groups and the more severely ill tend to bypass and to travel further for care than do less severely ill.
King M (1973), Van Etten (1972) and lyun B Distance is a significant factor influencing the patient (1972). behaviour, but not every thing depends on distance.
Patients choose the best service (quality) than one near to them.
Adajuylgbe (1980). Patronage of medical establishments is affected by two common factors- distance and community interest.
Egunjobi (1983) A maze of interactions among spatial and non-spatial variables is at work in the choice of hospitals, that linear distance argument is inadequate.
24

Against this background of the international studies in developed as well as developing
countries, we shall attempt a quick survey of the major empirical studies made in India in
recent years.
Studies on Utilization of Health Care Services in India
Most of the research on access and utilization of health care services carried out in India has been
by specialist institutions in Health research, such as NSSO, NIHFW (Delhi), IIHMR (Jaipur),
NCAER (Delhi) or by NGOs such as FRCH (Bombay) and KSSP (Thiruvananthapuram); or ,
. constituted part of baseline surveys for large area projects involving the establishment or .
enhancement of the provision of health care delivery; or formed part of evaluation of such
projects. The two major sources that provide a macro picture are the NSSO and the NCAER
surveys. These studies are based, in general, on household survey, case studies ofPHCs and sub
centres, (for example, the study by DANIDA, 1986) hospital studies (see Purohit, 1992); or local . level secondary data such as PHC or SC records or ·other hospital and district and state level
records which are not published (Murali and Nath; 1985).
Other attempts at exploring the utilization aspect of health services in India have been largely
limited to micro level studies. While they have looked into various aspects, namely, distance of
facility from the patients, type of care, availability of facility, cost of treatment, quality of care,
awareness about existing facilities, as well as other socio-economic aspects of patients in a
particular regional set up, it is not possible to get from them an overall picture at either the state,
the ,regional or the national levels. However, studies focussing exclusively on access and
utilization are few and far in between; much of what exists on these aspects is as part of general
surveys of health.
Most of the survey based studies focused on eliciting information regarding morbidity;
information on the utilization of health care services was only a by-product. Gumber and Berman
(1987) have chronicled the major surveys in India on morbidity patterns and utilization of health
care services; see Table 2.5 and 2.6
25

Table 2.5 Main Focus, Target Population and Area Covered in the Selected Health Surveys Survey/ Study/Area covered Main Focus Target Population
All India (Rural& Urban); NSS Utilization and treatment All population
(1992); Visaria and Gumber expenditure for illness and
(1994); Gumber (1994) injury
NSS (1991); Visaria and Gumber Maternal and Child health Children aged <5 and
(1992) mothers of children aged <1
All India (Rural & Urban) NCAER Morbidity pattern, utilization All Population
(1991); beolalikar and Vashishta & treatment expenditure on
(1992) illness and injury
Rural Madhya Pradesh, Rajasthan Morbidity pattern, utilization All population, children,
and UP; NCAER (1992) and expenditure on health pregnant mothers
care, maternal and child
health, role ofNGOs in
health delivery . Jalgaon in Maharashtra (Rural & Morbidity pattern, utilization All population, children and
urban); Duggal and Amin (1989) and expenditure on health mothers
care, maternal and child
health, births and deaths
Rural Kerala; Kannan et ql (1991) Morbidity pattern, utilization All Population
and expenditure on health
care, childcare, births and
deaths.
Bombay City; Yesudian (1990) Utilization and expenditure All Population
on health care, health
insurance
Madhya Pradesh (Rural and Morbidity pattern, utilization All population
Urban); George et al (1994) and expenditure on illness
and maternity
Rural Haryana;'K,~mtakar et al. Maternal and child health & Poor households having a
(1993); Berman et al. (1994) development, food intake, working mother with
morbidity, activity and children aged <6
employment status of
mothers
Source: Gumber and Berman (1997)
26

Table: 2.6 Main results on Utilization and Costs of treatment in the Selected Health surveys by area/year of survey
Utilization NSSRural- NCAER Rural- NCAER Kerala Rural Jalgaon Bombay Urban 1986-87 Urban 1990 Rural 1991 1987 1987 1989
Untreated 16 (rural) 2.4 (rural) 5-14: 12, Rises 13.7 3.7 (short illness II (urban) 4.7 (urban) Declines in 3 with SES (rural) term); 6.1 including self- Declines by SES Rises by SES district 8.3 (urban) (chronic) medication (%) Declines Declines and by SES Hospitalisation I (rural) NR NR NR 3 (rural) 1.3 (%) 1.5 (urban) 3.9 (urban) Share of public Inpatient: 62 52 (rural) MP: 14 (r)& 26; 12 (rural) 16 (short provider in (rural) & 63 40 (urban); 12 (u) Declines by 18 (urban) term), 32 treatment (%) (urban); Declines by SES UP: 13 (r) & SES Declines (chronic) and by SES Outpatient: 19 13 (u) &47
(rural) &24 RJ:51(r)& (catastrop (urban); Declines 86 (u) hic) b2'SES
Cost of Inpatient: 640 152 (rural), MP:147 (r) 17; Rises 104 92 (short Treatment- Av. (rural), 1053 143 (urban); & 129(u) steeply by (rural), term), . Cost (Rs) (urban); Rises by SES UP: 128 (r) SES 100 596
Outpatient: 71 & 97 (u)..· (urban); (chronic) (rural), 90 RJ: 186 (r) Rises & 1644 (urban); & 152 (u) steeply (catastrop Rises by SES hic);
Rises NR PrivatelPublic Inpatient: 2.57 1.25 (rural), MP: 1.17 (r) NR 1.51 NR Ratio (rural), 4.26 0.86 (urban) & 0.93 (u);
(urban); UP: 1.98 (r) Outpatient: 1.32 & 1.42 (u); (rural), 1.51 RJ: 1.04 (r) (urban) & 1.76 (u)
Medical Cost 100 77 (rural) MP: 75 (r) 67 87 72 (short as % of Total 78 (urban) & 81 (u); term), 90
UP: 76 (r) & (chronic), 67 (u); RJ: 93 69(r)&71 (catastrop (u) hic)
Source: Gumber and Berman (1997)
Though the majority of studies have elicited information on the preferred provider (who in most
cases, is 'the private provider), few have gone into details of the utilization patterns and have tried
to estimate the dimensions of utilization among the various classes of society its distribution in
rural area;;: Several studies stop at the periphery of analysis of the use and the cost of use (for
example, Duggal and Amin; 1989, Kannan et al; 1991, NCAER; 1992, and George et al; 1993.
However, some of these studies have looked into household health expenditure levels. While
George et al (1993) showed that in Madhya Pradesh, the majority get treated in the private
sector, their role at the national level reckoned in terms of locational access, was less (NCAER;
1992). Distance was among the reasons cited for not utilizing government health services
27

(Kannan et al. 1991 and George 1992). The implications of cost and quality on the utilization of
. health care have come out significantly in some other studies (eg. Duggal and Amin; 1989,
Uplekar; 1989, and Yesudian; 1990).
Analyzing the secondary data available for the utilization of health care services such as those
provided by NSSO and NCAER, Purohit and Siddiqui (1994) argued that the pattern of
utilization in India had some desirable outcomes, namely, growing popularity of indigenous,
non-allopathic systems and the growth in private sector involvement in expensive tertiary
care. The existence of an urban bias in tenns of availability and accessibility of health
services was brought out by the study of Visaria and Gumber (1993), which sought to
measure and explain the observed differences in the utilization pattern of primary health care
as between rural and urban populations and across different income groups. It also showed
that lower income groups largely used the public provisions. Krishnan (1992) also talked
about such an urban bias. Nair and Dhingra (1998) made a study of the ability and willingness
to pay for health care in an urban slum in Delhi. They showed' that willingness to pay for
health care was affected by ability.
Utilization of Health Care Services in Kerala
Several studies have gone into the paradox of Kerala's "good health at low cost". Most of them
have, however, examined only have studied some particular aspect or other of the health
development indicators such as birth rate, death rate, infant mortality rate, and increase in life
expectancy (eg. Zachariah and Patel (1982), Zachariah (1983), Nag (1983), Krishnan (1985).
Nag and Krishnan attributed the decline in mortality rates in the state to the widespread
accessibility and high levels of utilization of medical facilities, and wide coverage of preventive
services. UN Study (1975) and Panikar and Soman (1984) brought out the importance of easy
availability of health care as the detenninant factor. These studies were concerned, however,
with health outcdmes and access and utilization factors served only as the possible explanatory
variables. They failed to look into the issue of access and utilization as the processes rather than
as the outcome. However, Kabir and Krishnan (1992) advanced an interesting hypothesis to
explain the complementary development of demand for and the provision of health services,
namely the hypothesis of 'social intennediation in conjunction with the development of health
infrastructure' .
28

The first major study that examined the question of utilization of the health care services in
Kerala was the one by KSSP (Kannan, KP, et al: 1991), referred to already. It found that the state
had one of the highest morbidity rates in the country. Unlike earlier studies, which had
emphasized the role of the government in the health status improvement of the state, this study
brought out the rising role of the private sector and the increasing preference for private sector
utilization across all socio-economic strata as the crucial factor. Since it was based on an
extensive household survey of a general type, rather than an intensive enquiry into micro issues
of access and utilization, it was not able to shed much light on them.
2.3 Determinants of Health Service Utilisation Behaviour
Health seeking behaviour may be defined as any activity undertaken by individuals who perceive
themselves to have a health problem or to be ill, for the purpose of fmding an appropriate
remedy. It should be distinguished from the broader concept of health behaviour, deflned by
Kasl and Cobb as any activity undertaken by individuals' who see themselves as healthy for the
purpose of preventing disease or detecting it in an asymptotic stage. It is hypothesized that the
use of health care services is determined by a combination of factors that include not only
household and individual characteristics,but also illness characteristics as well as provision
characteristics. Following Ward et al (1997), these factors and their analytical orientations may
be summarized as follows. (Table 2.7).
Table 2.7 Analytical Orientations or Approach to Health Seekin~tilization Behaviour The economic In which attention is concentrated on the impact of fmancial barriers .
in health seeking The organizational or In which the focus of attention is on the effects of aspects of health delivery system organization on use of services. The socio- In which emphasis is on the significance of gross characteristics like demographic gender, age and education for utilization The geographic In which the focus of attention is the association between the
geographical proximity of health services and utilization The socio- cultural In which the orientation is towards examining associations between
the values, norms, beliefs, and life-styles of different socio-economic groups and utilization
The social- In which the emphasis is on the link between individual motivation, psychological perception and learning and utilization behaviour
Source: -Helen Ward et al (1997)
On the lines of the above analytical categories, several scholars have tried to develop health care
demand and utilization models. Kroeger (1983) tried to develop conceptual framework for
examining the question of how people enter the sick role and make choices regarding the use or
29

non-use of different health services. His determinants model, based on a more bio-medical and
qualitative approach focused on outlining a set of 'explanatory variables or determinants that are
associated with the choice of different kinds of health service'. Anderson and his colleagues set
out a model for health care utilization, which they claimed to be a structural model for health
care utilization (Anderson and Newman; 1973). In this model, three sets or determinants have
been proposed that could influence health service utilization: See Figure 2.1.
Figure 2.1 Factors Affecting Health Services Utilization According to Anderson's Model
Societal System Determinants of" Determinants
Technology Resources Norms O~anization
INDIVIDUAL DETERMINANTS
Determinants of health service utilization Predisposing factors Enabling factors Illness factors
Demographic Family Level Age, Income, Disability Sex, Insurance Symptoms
Marital Status, (Type of access to care) Diagnoses Social structure, General Health
Education, Community Occupation, Facilities, Evaluation
Religion Cost of service, Mobility etc Region (ruraVurban)
Beliefs Values,
Attitudes;' Knowledge
Source: Anderson (1973)
Almost on the lines of the Anderson model, Kroeger (1983) contributed the following
framework of the following type to analyse the choice of the healer; see figure 2.2.
30

Figure 2.2 Kroeger's (1983) Framework for Analysing Health Seeking Behaviour
Explanatory variables
Dependent Variable
Subject
+ Age Sex
Marital Status Position in Household
Formal Education Occupation Resources
(Land, wealth etc) Interaction with
Family, Community etc
Characteristics of: Disorder
+ Chronic or Acute Severe or Trivial
Etiological Model Expected benefits from
treatment Psychosomatic vs. somatic
Choice of Health Care Resources
/ Traditionall Government!
Modem Healer Private Pharmacist! Drug Seller
Source: Kroeger (1983)
Services
Accessibility Appeal (opinions 7
attitudes toward traditional &modern
healers) Acceptability
Quality Communication
Cost
Self treatment! No treatment
Taking from Anderson's model and modifying Kroeger (1983) model, we can derive the
following framework for our understanding the patterns of utilization of health care services and
the choice of provider in Kerala; see figure 2.3.
The framework for analysing the health care provider seeking behaviour in Kerala in this study is
modelled after the following framework:
31

Figure 2.3 Suggested Framework for Analysing Provider Choice
Household Characteristics Individual Characteristics .. ...
Demand for Health Care
Services ~~----~----~
Need for Health Care
I Illness Characteris1ics ~ ____________ -. __ -r __ ~Ir---~
1 Medical Provider Choice
" System of Medicine
General Practitioner/
Specialist
Provision of Health Care Services in terms of
Accessibility Availability
Affordability (costs) Acceptability
32

2.4 Data Requirements
According to the framework specified, the data requirements for the study fall into two
categories: - one dealing with the provision patterns and the other dealing with the use pattern.
Secondary data were found inadequate to explain the problems taken up in this study. However,
secondary data are used for preparation of the background for the field study and an
understanding of the dimensions of the problem involved. Information on characteristics of the
region and its population as well as on the density and spread of medical facilities are collected
from secondary sources. Also, some details regarding the provision patterns were also available.
However, for the analysis of the use patterns of health care services across the different
categories of provision we have had to rely upon field investigations.
D.ata on Provision Patterns
District-wise data on the supply of health care servIces in Kerala in the public sector are
available for published and unpublished government sources. Information on health care
provision in the government sector for all the three institutionalised bio-medical systems -
Allopathic, Homeopathic and Ayurvedic- is published annually in the Economic Reviews of the
State Planning Board and the annual reports and other publications of the Department of Health
Services of Govt. of Kerala every year. The corresponding data regarding private sector, which
is the dominant sector, is not published by these agencies on a regular periodical basis. Most of
the data that private researchers provide regarding the provision of health care in Kerala (for
that matter, in the whole ofIndia) either do not contain the private sector provision, or leave out
systems other than allopathy.
As far as the government sector in Kerala is concerned, data are available on important items
such as the number of medical institutions, the number of physicians and other health personnel
and the number of patients treated (in-patients as well as out- patients), on an annual basis under
all the three systems of medicines. For private sector health care, similar data are available only
for a few time points in the recent past. Such data for the private sector, however, exclude all
physicians who provide health care services outside medical institutions.
The two major sources of information on the number of private medical institutions in the
different systems of medicine in the state have been (i) the Government surveys of private
33

medical institutions in Kerala conducted in 1986 and 1995; and (ii) the KSSP study of 1987
which gives data on medical institutions, beds, diagnostic labs etc (though it did not mention the
definitions used for classifying medical or paramedical institutions or for even practitioners).
For details regarding the region, its indicators, the socio-economic problems, health problems
and other details regarding the district selected for the study, the sources used are: (i) the Census
(1991) and its Village and Town directory; and (ii) the data collected from the district,
Municipality and Panchayat authorities. For data on the district level provision of health care
services (both public and private) the official source is the survey of Private Medical Institutions
(1985 & 1996), conducted by the Dept of Economics and Statistics, Govt. of Kerala. However,
informal sources such as medical representatives, the Telephone directory and an Ayurveda
Doctors' Directory (1998) published by Academy for Traditional Medicine and Ayurveda
(Thiruvalla, Kerala) were also made use of for obtaining information on the practicing physicians
and medical institutions in the survey area.
However, these sources have limitations too. For example, the Village and Town directory of
the Census gives data regarding area, population, and number of households in each ward, and
medical institutions in the rural areas. However, data of the number of private medical
institutions and practitioners seem unreliable. More over, they do not provide system-wise
details. Similarly, the Kerala government surveys do not give region-wise data within a district,
especially in the 1995 survey. Though they give details of hospitals system-wise and of beds
availability wise, but do not give district-wise information on the size of the medical institutions
and their staff strength. Medical representatives often do not have a complete list of doctors as
they aim at marketing only specific pharmaceutical products, thus targeting the doctors who,
they think, would prescribe them. Often, the lists do not contain names of general practitioners
working in rural areas. The problem with using the list of doctors and hospitals listed in the
telephone directory is that it does not have the names and telephone numbers of fresh graduates,
traditional vaidyans and under-estimates the number of doctors since there would be cases in
which there is more than one doctor in a household. Also, it does not specify the sector or
system of the doctor's practice in most of the cases.
Primary data collection on the provision patterns had to be carried out from the main providers
of the services, i.e., the doctors. A survey of doctors regarding their practice behaviours had to
be preceded by a survey of the institutions, an exercise which was carried out among a
34

randomly selected group of doctors of both public and private sectors, and belonging to
different systems of medicine and working in different institutional set ups in the study area.
Selection of Sample Area and Households
The study area selected was the Alappuzha district. This district was selected taking into
account the fact it has the highest density and spread of health care facilities among the districts
of Kerala. From the Alappuzha district, two localities - one rural and the other urban -were
selected. For the rural area, the Ambalappuzha Panchayat of Ambalappuzha taluk was chosen.
This village consists of 15 wards (1998 figures). These fifteen wards may be broadly classified
into three: coastal wards, wards in the plains and wards in the waterlogged areas. Depending on
these, topographical characteristics, population characteristics vary. For example, the coastal
wards are inhabited by people belonging to the fishermen community whereas the waterlogged
wards are inhabited by backward communities and classes, in the wards in the plains, the
population consists mainly of the upper middle and the high income groups. Three wards were
taken for our study, each ward belonging to one of these three groups so as to facilitate inter
local comparisons. Thus it is a multi-stage cluster random sampling technique that we have
adopted in this study.
The wards selected were 9th, 10th and 14th in the Ambalappuzha panchayat. In each ward,
samples were taken in such a way that at least 10 percent of the total households in the wards
are covered i.~ the sample. Because of the nature of spread of houses in the wards, it was found
difficult to resort to the usual method of choosing every 10th house for the sample. Instead,
from the list of households obtained from the Panchayat records and the voter's list, households
were classified into groups/clusters of 100 households each. From each cluster of 100
households, 10 houses were selected using a random table. A total of 225 rural households were
surveyed.
Following similar methods, two wards from the town area of Alappuzha were selected from
which 120 households were surveyed. The respondents were asked to recall all chronic
morbidity episodes in the past one-year and their treatment details, for acute illnesses, a three
month recall on to the date of interview was fixed.
35
In our data collection exercise through the primary survey, the data collected are the
following:
1. Household profile: - the type of house, wall, drinking water facilities, sanitation facilities,
wastage disposal etc.
2. Household members' profile: - the number of members, adults, children etc, their age, sex,
education, occupation, earning, general health status etc.
3. Morbidity pattern of the households: - Acute, chronic, trivial, serious etc. Episodes lasting
for more than 30 days duration are treated for the purpose of the study as chronic
morbidity episodes while those lasting for less than 30 days are treated as acute morbidity
episodes (Seal, 1971). Acute morbidity is further classified in to (a) minor (less than two
days), (b) Mild (3-6 days) and (c) Moderate (7 to 30 days). This classification refers only
to the duration and not to the seriousness of the episodes. Similarly, chronic morbidities
are classified into (a) very short term (more than 30 days, but less than 6 months (b) short
term (less than a year), (c) medium term (one to thr.ee years), (d) long term (more than '.
three years duration of illness).
4. Type of treatment - whether self-treatment, no treatment or treatment of any of the different
morbidity types.
5. If institutionalised treatment, choice of providers and reasons for the choice, the pattern of
treatment undergone the reasons for choosing particular medical facility, etc.
6. Cost of treatment for different types of illness episo?es: expenditure on consultation,
medicines, injections, IP treatment, hospital charges, lab charges, expenditure on tests,
bribes etc.
7. Burden of treatment on the family's economic position: Family income, nature of income,
cost of treatment, cost of transportation, opportunity cost of forgoing work or leisure for
treatment and visit to medical institutions, the borrowing the family had to make to finance
medical expenditure etc.
Conclusion
In this chapter, we have discussed theoretical issues, reviewed empirical studies, and
developed a framework for analysis in the study. Details regarding area of study, selection of
samples for field investigation, methods of data collection were also discussed. In chapters to
follow, we shall dwell upon the questions of the provision of health facilities, morbidity
patterns, utilization patterns, expenditure and the determinants of utilization.
36

Analysis of theoretical issues showed that health care is different from other commodities and
hence the question as to who should provide them is highly debated. However, actual health
care sector is a mix of private and public provisions. Review of literature showed that more
studies with respect to understanding health care provision and utilisation are needed for
better policy prescriptions. Such an attempt needs a framework which takes care of not only
individual characteristics, but also illness characteristics as well as provision characteristics,
as has been developed for our study.
37