review of struma.doc
DESCRIPTION
refrat tentang strumaTRANSCRIPT

REVIEW OF STRUMA
PREPARED BY:
Stefano Leatemia
11.2012.031
SURGERY CLERKSHIP
AIR FORCE HOSPITAL OF DR.ESNAWAN ANTARIKSA
FACULTY OF MEDICINE UKRIDA
PERIOD MAY 6th – JULY 13th 2013
1

TABLE OF CONTENTS
Preface ……...................................................................................................................................i
Content ..........................................................................................................................................1
CHAPTER I Introduction ……………………………………………………………………….3
CHAPTER II Anatomy and Physiology of Thyroid .....................................................................4
CHAPTER III
3.1 Struma Difusa ……………………………………………………………………....9
3.2 Struma Nodosa Toxic ………………………….......................................................10
3.3 Struma Difusa ……………………………………………………………………...11
3.4 Struma Nodosa Non Toxic ………………………………………………………..12
3.5 Carcinoma …………………………………………………………………………14
3.6 Enforcement Measures Struma Diagnosis ...............................................................18
CHAPTER IV Conclusion …………………………………………………………………….. 22
REFERENCES ……………………………………………………………………………….. .23
2

CHAPTER I
INTRODUCTION
Struma is the enlargement of the thyroid gland caused by the addition of thyroid gland
tissue itself. Enlargement of the thyroid gland that causes changes in the body's functions and
some that did not affect function. Struma is a disease common day-to-day, with a history and a
thorough physical examination, struma with or without metabolic dysfunction can be diagnosed
accurately.
Epidemiological Survey for struma endemik often found in mountainous regions such as
the Alps, Himalayas, Bukit Barisan and other mountain areas. For toxic struma prevalence is 10
times more common in women than men. In the case of a woman found 1,000 women 20-27,
while the men 1-5 of 1,000 men.
3

CHAPTER II
Thyroid Gland Anatomy and physiology
To understand disease and thyroid disorders, to remember back about the anatomy of the
thyroid. Anatomy and normal physiologic must be known and remembered back before the
change of anatomy and physiology that may progress to a disease or disorder.
2.1 Anatomy of the Thyroid
The thyroid gland consists of three lobes, which dextra lobe, the left lobe and the
isthmus which lies in the middle. It can sometimes be found all four parts namely the pyramidal
lobe is located on the isthmus slightly to the left of the center line. This lobe is residual thyroid
tissue that remains embryonic.
The thyroid gland has a weight of about 25-30 grams and is located between the thyroid
and sixth tracheal rings. The entire thyroid tissue wrapped by a layer called the true capsule.
4
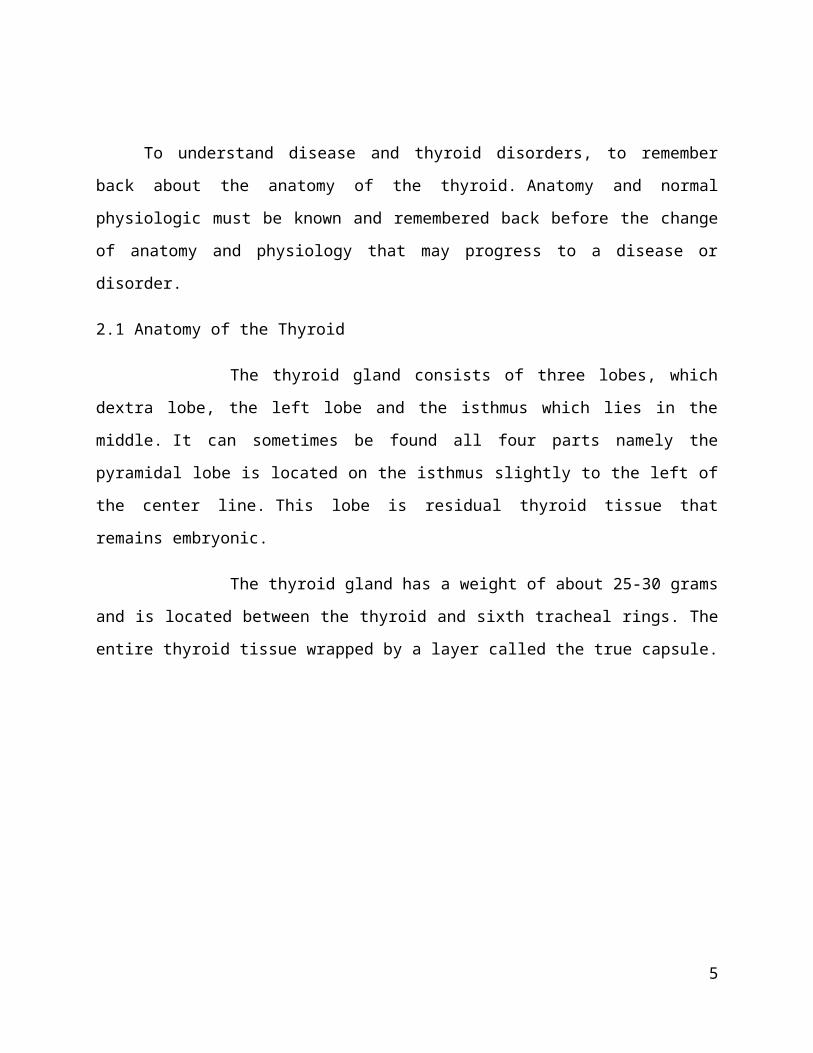
Vascularity of the thyroid gland derived from:
. 1) A. Superior thyroid which is a branch of A. Carotid externa
2) A. Inferior thyroid which is a branch of A. Subclavian
3) A. Ima thyroid which is a branch of the Arcus Aorta
Nerve that passes through the thyroid is the recurrent nerve. It is located in the dorsal
neural thyroid before entering the larynx.
5

2.2 Physiology of Thyroid
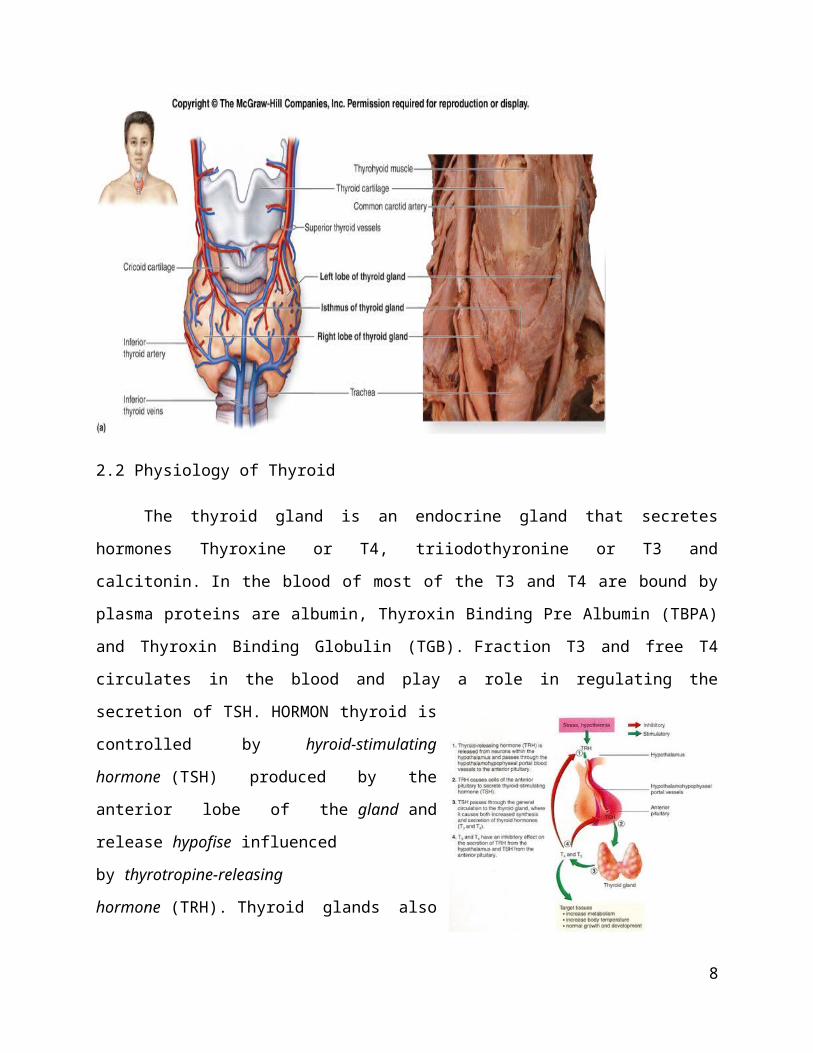
The thyroid gland is an endocrine gland that secretes hormones Thyroxine or T4,
triiodothyronine or T3 and calcitonin. In the blood of most of the T3 and T4 are bound by plasma
proteins are albumin, Thyroxin Binding Pre Albumin (TBPA) and Thyroxin Binding Globulin
(TGB). Fraction T3 and free T4 circulates in the blood and play a role in regulating the secretion
of TSH. HORMON thyroid is controlled by hyroid-stimulating hormone (TSH) produced by the
anterior lobe of the gland and release hypofise influenced by thyrotropine-releasing
hormone (TRH). Thyroid glands also secrete calcitonin of parafolicular cell, which can lower
serum calcium affect bone.
Thyroid hormone function, among others:
1) increase the metabolic rate
2) cardiogenic effects
3) simpatogenik
4) growth and nervous system
6

CHAPTER III
DISCUSSION
Enlargement of the thyroid gland or struma classified according to its physiological effects
clinical, and changes in shape that occur. Struma can be divided into:
1) Toxic struma, struma which raises the clinical symptoms in the body, based on
changes in shape can be subdivided into
a. Diffusa, ie if the enlargement of the thyroid gland covering the entire lobe, like those found
in Grave's disease.
b. Nodosa, ie if the enlargement of the thyroid gland only on one lobe, like those found in
Plummer's disease.
2) Nontoxic struma, the struma that does not cause clinical symptoms in the body, based on the
change in shape can be subdivided into
a. Diffusa, such as those found in endemic struma
b. Nodosa, such as those found in thyroid malignancy
Enlargement of the thyroid gland can be caused by:
1) Hyperplasia and hypertrophy
Each organ is triggered when the work will have to compensate by increasing the
number of cells and multiply. Likewise, when the thyroid gland will be encouraged to
work pertumnuhan produce the hormone thyroxine and will have m embesar, such as
puberty and pregnancy.
2) Inflammation or infection
Processes such as inflammation of the thyroid gland in acute thyroiditis, subacute
thyroiditis (de Quervain) and chronic thyroiditis (Hashimoto)
7
3) Neoplasms
Benign and malignant
Struma cause clinical symptoms caused by changes in thyroid hormone levels in
the blood. The thyroid gland can result in excessive levels of thyroid hormone or
commonly called hyperthyroidism and in levels of normal or less than normal is called
hypothyroidism. Symptoms in hyperthyroidism are:
Increased appetite and weight loss
Can not stand the heat and hyperhidrosis
Palpitations, high systolic and diastolic pressure is low resulting in a high pulse
(pulsus celler) and in the long term could be atrial fibrillation
Tremor
Diarrhea
Infertility, amenorrhae in women and testicular atrophy in men
Exophtalmus
Symptoms in hypothyroidism is the opposite of hyperthyroidism:
Decreased appetite and weight gain
Can not stand the cold and dry scaly skin
Bradycardia, low systolic pressure and pulse pressure are weak
Gestures become sluggish and edema of the face, eyelids and limbs
8

3.1 Difusa Toxic Struma
3.1.1 Definition
Difusa toxic struma can be found in Grave's Disease. The disease is also called
Basedow. Trias Basedow include diffuse enlargement of the thyroid gland, and eksoftalmus
hipertiroidi. Disease is more common in younger people with symptoms such as excessive
sweating, hand tremors, decreased heat tolerance terhafap, weight loss, emotional instability,
menstrual disorders such as amenorrhea, and polidefekasi (often defecation). Clinical often
found in the thyroid gland enlargement, sometimes there is also a manifestation of the eye and
miopatia exophthalmus ekstrabulbi. Although the etiology of Graves' disease is not known for
sure, it seems there is a role of an antibody that can be captured TSH receptor, leading to
increased thyroid hormone stimulus. The disease is also characterized by increased absorption of
radioactive iodine by the thyroid gland.
Image: Graves disease
3.1.2 Pathophysiology
Grave's Disease is a disease caused by abnormalities in the body's immune system,
where there is a substance called Thyroid Receptor Antibodies. This substance occupies TSH
9

receptor in thyroid cells and stimulate them in berlebiham, so it can not occupy the TSH receptor
and thyroid hormone levels in the body is increased.
3.1.3 Clinical Symptoms
Symptoms and signs that arise is a manifestation of increased metabolism in all body
systems and organs that may be clinically apparent. Increased metabolism causes increased
caloric needs, and often intake (intake) insufficient caloric needs, causing drastic weight loss.
Increased metabolism in the cardiovascular system visible in the form of an increase in
blood circulation, among others, with an increase in cardiac output / cardiac output up to two-
three times normal, and also in a resting state. Rhythm pulse rise and pulse pressure increases, so
be pulsus Celer; patients will experience tachycardia and palpitations. Burden on myocardial,
and autonomic nerve stimulation can result in a heart rhythm disorder ektrasistol, atrial
fibrillation, and ventricular fibrillation.
Gastrointestinal secretion and peristalsis increases often resulting polidefekasi and
diarrhea.
Hipermetabolisme nervous system usually causes tremors, sleeplessness sufferers, often
waking in the night. Patients experience emotional instability, anxiety, thought disorder, and
unwarranted fear that very disturbing.
In the airways, causing dyspnea and tachypnea hipermetabolisme are not too
distracting. Muscle weakness mainly proximal muscles, usually quite disturbing and often appear
suddenly. This is caused by electrolyte disturbances triggered by the hipertiroidi.
Menstrual disorders can be secondary amenorrhoea or metrorhagia. Eye disorders
caused by an autoimmune reaction in the form of antibodies binding to receptors on muscle and
connective tissue in the eye socket ekstrabulbi. Connective tissue and fat tissue to hyperplastic so
eyeball pushed to the outer eye muscles and pinched. The result is eksoftalmus which can cause
eye damage due to keratitis. Impaired muscle movement will cause strabismus.
10

Figure: Schematic pathogenesis of Graves' disease
3.1.4 Treatment
Graves disease therapy aimed at controlling the state tirotoksisitas / hipertiroidi with
antithyroid administration, such as propyl-tiourasil (PTU) or karbimazol. Definitive therapy can
be selected between anti-thyroid medication long-term, detachments with radioactive iodine, or
thyroidectomy. Surgery of the Thyroid with hipertiroidi done especially if treatment with the
thyroid gland fails medikamentosa great.Surgery usually provides a good permanent cure
although sometimes encountered the hipotiroidi and minimal complications.
3.2 Struma Nodosa Toxic
3.2.1 Definition
Nodosa toxic struma is an enlarged thyroid gland on one lobe is accompanied by
signs of hyperthyroidism. Nodular enlargement occurs in young adulthood as a nontoxic
11

goiter. When untreated, in 15-20 years can be toxic. Was first distinguished from Grave's
disease by Plummer, then known as Plummer's disease.
3.2.2 Pathophysiology
The disease begins with the onset of nodular enlargement of the thyroid gland that
does not cause symptoms of toxicity, but if not treated immediately, within 15-20 years
can cause hyperthyroidism. The factors that affect the change of nontoxic be toxic
include these nodules turn out to be its own autonomous (associated with autoimmune
diseases), thyroid hormone from the outside, as the radioactive iodine treatment.
3.2.3 Clinical Symptoms
When history, it is difficult to distinguish between Grave's disease with
Plummer's disease because both showed symptoms of hyperthyroidism. The difference is
when a physical examination at the time of palpation where we can feel the enlargement
affects only one lobe.
3.2.4 Treatment
Therapy given to Plummer's Disease Grave's also the same as that aimed at
controlling the state tirotoksisitas / hipertiroidi with antithyroid administration, such as
propyl-tiourasil (PTU) or karbimazol. Definitive therapy can be selected between anti-
thyroid medication long-term, detachments with radioactive iodine, or
thyroidectomy. Surgery of the Thyroid with hipertiroidi done especially if treatment with
the thyroid gland fails medikamentosa great. Surgery usually provides a good permanent
cure although sometimes encountered the hipotiroidi and minimal complications.
3.3 Struma Difusa nontoxic
3.3.1 Definition
12

Endemic goitre endemic goitre is a disease that i signed with ti roid gland
enlargement that occurs in a population, and is expected to relate to deficiencies in the
daily diet. Endemic goiter epidemiology is estimated there are approximately 5% in a
population of primary school children / preadolescent (6-12 years), as is evident from
several studies. Endemic goitre occurs due to deficiency of iodine in the diet.Frequent
incidence of endemic goiter in derah pegnungan, such as in the Himalayas, alpens, areas
with the availability of natural iodine and iodine additional coverage has not done well
3.3.2 Pathophysiology
Generally, the mechanism of occurrence of goiter caused by a
deficiency intake iodine by the body. In addition, goiter can also be caused by
congenital abnormalities of thyroid hormone synthesis or goitrogen (goiter-causing
agents such as intake Excessive calcium and Brassica family vegetables). Lack of
iodine causes a lack of thyroid hormone can be synthesized. This will lead to an increase
in the release of TSH (thyroid-stimulating hormone) into the blood as kompensatoriknya
effect. The effect causes hypertrophy and hyperplasia of thyroid follicular cells, resulting
in enlargement of the thyroid macroscopically. This enlargement can normalize body of
work, because on the kompensatorik effects of thyroid hormone needs are met. However,
in some cases, such as iodine deficiency is endemic, this enlargement will not be able to
compensate for the existing disease. The condition known as goiter hypothyroidism. The
degree of enlargement of the thyroid following levels and duration of thyroid hormone
deficiency that occurs in a person.
Diffuse Goiter
Diffuse Goiter is a form like piece that forms a visible enlargement without forming
nodules. Form is usually found with non-toxic properties (normal thyroid function), hence this
form is also called simple goiter. Can also be referred to as colloid goiter due to an enlarged
follicle cells are generally met by colloidal proficiency level. This disorder appears in endemic
and sporadic goiter.
13
Endemic goiter appeared in a soil, water, and food supply contains less iodine, so the
iodine deficiency is widespread in the area teresebut. Examples region is mountainous Alps, the
Andes or Himalayas.
Meanwhile, sporadic goiter appeared less frequently and can be caused by many things,
the consumption of which inhibit the synthesis of thyroid hormones or enzymes for impaired
thyroid hormone synthesis dropped hereditary.
On simple goiter, there are two phases of evolution, namely hyperplastic and colloid
involution. In the hyperplastic phase, the thyroid gland is diffusely enlarged and symmetrical,
although not too large magnifying power (up to 100-150 grams). Follicle-folikelnya coated by
columnar cells are numerous and crowded. Accumulation of these cells is not the same in the
whole gland. If after the consumption of iodine the body needs increased or decreased thyroid
hormone, follicle epithelial cell involution occurs, forming large follicles filled with
colloid. Thyroid would normally macroscopically visible brown and translucent, while
histologically will be seen that the follicles filled with colloid and epitelnya flattened and
cuboidal cells.
3.3.3 Clinical Symptoms
Most of the clinical manifestations associated with enlargement of the thyroid
gland. Most patients remained euthyroid state shows, but some circumstances having
hypothyroidism. Hypothyroidism is more common in children with biosynthetic defect as the
cause, including defects in the transfer of iodine.
3.3.4 Procedures
The goal of treatment is to shrink the goitre endemic goitre and hypothyroidism resolve
possible, namely by giving SoL Lugoli for 4-6 months. If there is improvement, treatment was
continued until a year and then tapering off in 4 weeks. When the 6 months after treatment of
goitre is not also shrink the medical treatment is not successful and should be operative action.
3.4 Struma nodosa nontoxic
14

3.4.1 Definition
Goitre nodosa is non toxic ti roid gland enlargement to the clinically palpable nodules
without one or more signs hypertiroidisme. The term struma nodosa indicates the existence of a
process, either physiological or pathological cause asymmetrical enlargement of the thyroid
gland. Because it is not accompanied by signs of toxicity in the body, it is referred to as
asymmetric enlargement nodosa nontoxic goiter.This disorder is very common everyday, and to
watch out for signs of possible malignancy.
3.4.2 Pathophysiology
SNNT can also be referred to as sporadic goiter. If endemic goitre occurs 10% of the
population in areas with iodine deficiency, the sporadic goiter occurs in someone who does not
live in an area endemic low iodine. The cause is as yet unknown, there can be interference
enzyme important in the synthesis of thyroid hormones or consumption of drugs containing
lithium, propiltiourasil, fenilbutazone, or aminoglutatimid.
3.4.3 Clinical Symptoms
In general, non-toxic struma nodosa had no complaints because there was no hypo-or
hyperthyroidism. SNNT diagnosis is important in the absence of toxic symptoms caused by
changes in thyroid hormone levels, and felt on palpation of the enlarged thyroid gland on one
lobe. Usually thyroid began to swell at a young age and developed into multinodular in
adulthood. Due to gradual growth, goitre may be asymptomatic unless large lump in the neck.
majority of patients with struma nodosa can live with strumanya without complaint.
Although most of struma nodosa does not interfere with breathing due to jut forward, others can
cause narrowing of the trachea when bilateral enlargement. Goitre nodosa unilateral
stimulation can lead the way into contra lateral direction. Thus may not lead to the promotion of
respiratory disorders. Significant narrowing cause respiratory until finally happened with stridor
inspiratoar dispn ea.
Complaints that there is a sense of weight in the neck. Trachea during swallowing to cover up the
15

larynx and epiglottis so heavy because fixed to the trachea.
3.4.4 Treatment
Operative action is still the main option on SNNT. Various techniques of operations
include:
a. Lobectomy, which is the lobe lift, when the gland is left subtotal weighing 3 grams
b. Isthmolobektomi, the removal of one lobe followed by the isthmus
c. Total thyroidectomy, which is removal of the entire thyroid gland
d. Bilateral subtotal thyroidectomy, the partial removal of the right lobe and the left part,
the rest of the network in the posterior 2-4 grams taken to prevent damage to the
parathyroid glands or N.Recurrent Laryngeus
3.5 Carcinoma of the Thyroid
3.5.1 Definition
Thyroid carcinoma is a malignancy (uncontrolled growth of cells) that occur in the
thyroid gland. Cancer is a depressing thyroid malignancy in thyroid which has 4 types:
papillary, follicular, medullary and anaplastic. Thyroid cancer rarely causes enlargement of the
gland, often causing small growth (nodule) in the gland. The majority of thyroid nodules are
benign, thyroid cancer usually can be cured
Thyroid Cancer often limit the ability to absorb iodine and limit the ability to produce
thyroid hormone, but sometimes produce enough thyroid hormone, causing hyperthyroidism.
3.5.2 Classification of thyroid carcinoma
2) Papillary carcinoma, This carcinomas derived from thyroid cells and is the most common
type of thyroid carcinoma. More often found in children and young adults and is more
common in females. Exposed to radiation during childhood helped to cause this
malignancy. First appeared in the form of a palpable lump in the thyroid gland as enlarged
16
lymph nodes or neck area. Metastases may occur via the lymph to other areas in the thyroid
or, in some cases, to the lungs.
3) Follicular carcinoma, carcinoma is derived from follicular cells and is 20-25% of thyroid
carcinoma. Follicular carcinoma primarily affects on age above 40 tahun.Karsinoma
follicular also attacked 2 women up to 3 times more often than men. Exposure to X-rays
during childhood increases the risk of this type of malignancy. This type is more invasive
than the papillary type.
4) Anaplastic carcinoma, This highly malignant carcinoma and constitute 10% of thyroid
cancers. Slightly more often in women than men. Metastasis occurs in rapid, early around
it and then other parts of the body. At first people were just complaining about the presence of
thyroid tumor area. With this cancer infiltration around, arising hoarseness, stridor, and
difficulty swallowing. Life expectancy after diagnosis is established, usually only a few
months.
5) Parafolikular carcinoma, carcinoma parafolikular or medul l er is unique among thyroid
cancer. This carcinoma more commonly in women than men and is most often over 50 years.
Carcinoma is rapidly metastasize, often to the place much like the lungs, bones, and liver. His
trademark is his ability to secrete calcitonin because of origin. Carcinoma is often said to be
hereditary.
3.5.3 Differences Benign and Malignant Thyroid Nodules
Approximately 5% had malignant struma nodosa. In the clinic should be differentiated
thyroid nodules are benign and malignant nodules that have these characteristics:
1. Consistency hard on some parts or the whole nodules and hard-driven, although malignant
nodules may undergo cystic degeneration and then become soft.
2. In contrast to the consistency of soft nodules more often benign, although calcified
nodules can be found in adenomatous hyperplasia longstanding.
3. Infiltration into the surrounding tissue nodules merupaka sign of malignancy, although not
always malignant nodules infiltrating. If found ptosis, miosis, and enoftalmus a sign of
infiltration into surrounding tissue
17
4. 20% are malignant solitary nodules whereas multiple nodules are rarely malignant.
5. Nodules that appear suddenly or rapidly growing needs, especially malignant suspicion
that is not accompanied by pain. Or nodules old suddenly enlarged progressively
6. Suspected malignant nodules when accompanied by regional lymph node enlargement or
change in voice became hoarse.
7. Carotid artery pulsation is palpable from the rear edge of the sternocleidomastoid
muscular enlargement due to pressure nodules (Berry's Sign)
3.6 Enforcement Measures Diagnosis Struma
3. 5. 1 Anamnesis
On history, major complaints expressed by the patient may be a lump in the neck that
has lasted a long time, and the symptoms of hyperthyroidism or hipotiroidnya. If the patient
complained of a lump in the neck, then it should be further explored whether or progressive
enlargement occurs very slowly, accompanied with swallowing disorders, impaired breathing
and voice changes. After that asked whether or not there symptoms of hyper and hypofunction of
thyroid kelenjer. Need a place to stay were also asked patients and salt intake to see if there are
trends towards endemic goitre. Conversely, if patients present with symptoms towards hyper or
hypofunction of the thyroid, should be explored further to hyper or hypo and whether there is a
lump in the neck.
3. 5. 2 Physical Examination
On physical examination localist status at the anterior region coli, the most first carried
out an inspection, symmetrical enlargement seen whether or not, arise respiratory signs or not,
part moves while swallowing or not.
On palpation it is important to determine whether the right is bejolan thyroid gland or
lymph nodes. The difference was at the time the patient is asked to swallow. If true then enlarged
thyroid lumps will also move when swallowing, while if not moving then to think about the
possibility of enlarged cervical lymph nodes. Palpable enlargement should be described:
Location: right lobe, left lobos, isthmus
18

Size: in centimeters, length diameter
The number of nodules: one (uninodosa) or more than one (multinodosa)
Consistency: cystic, soft, chewy, hard
Pain: there is pain or not at the time of palpation
Mobility: no or no attachment to the trachea, muscular sternokleidomastoidea
Lymph nodes around the thyroid: no enlargement or not
3.5.3 Examination Support
Laboratory tests used in the diagnosis of thyroid disease is divided into:
1. Examination to measure thyroid function. Examination to determine levels
of T3 and T4 and TSH most often using radioimmunoassay technique (RIA)
and ELISA in serum or blood plasma. Normal levels of total T4 in adults is
50-120 ng / dl. Normal levels of T3 in adults is 0.65 to 1.7 ng / dl.
2. Examination to indicate the cause of thyroid disorders. Antibodies to various
thyroid antigens found in the serum of patients with autoimmune thyroid
disease. Such as thyroglobulin antibodies and thyroid stimulating hormone
antibodies
3. Radiological examination
X-rays can clarify the deviation of the trachea or retrosternal goitre
enlargement is generally clinically was to be expected. X-ray neck AP and
lateral position is usually an option.
Thyroid ultrasound is useful to determine the number of nodules,
differentiate between solid and cystic lesions, detect the presence of
cancerous tissue that does not capture iodine and can be seen by scanning
the thyroid.
Thyroid scanning is essentially a presentation of I 131 uptake thyroid
distributed. Uptake can be determined from the impression the size, shape
19

and location of the main parts is thyroid function (distribution within the
gland). Normal uptake of 15-40% within 24 hours. From the results of
thyroid scanning can distinguish three forms, namely cold nodule uptake
when nil or less than normal compared with the surrounding region, this
suggests that the function of low and often occurs in neoplasms. The second
form is when uptakenya warm nodule with surrounding, showing the
function of the thyroid nodule with other parts. If the latter is the hot nodule
uptake more than normal, meaning excessive activity and rarely in
neoplasms.
4. FNAB. Histopathologic examination of 80% accuracy. It is worth
remembering that not to determine the only definitive therapy based
on the results of FNAB alone.
3.5.4 Measures Surgery
Indications operations on goitre is:
1. Toxic diffuse goiter who fail to medical therapy
2. Struma uni or multinodosa with the possibility of malignancy
3. Struma with compression disorders
4. Cosmetics
Contraindicated in goiter surgery:
1. Struma toksika that have not prepared in advance
2. Goitre with cardiac decompensation and other systemic diseases that have not
been controlled
3. Large goitre which cling tightly to the neck tissues that are normally difficult
to move because of carcinoma. Such carcinomas are usually of poor prognosis
anaplastic type. Attachment to the trachea or larynx or trachea may well
20

dilakukanreseksi laringektomi, but attachment with extensive soft tissue neck
excision is difficult to do well.
First clinical examination for menentuka n whether the suspected malignant
thyroid nodules or suspected to be benign. When the suspected malignant nodules, it is
distinguished whether the case is operable or inoperable.
When the case at hand is inoperable then performed an act of incisional biopsy for
histopathological examination purposes. Debulking followed by action and external
radiation or chemoradiotherapy. When suspected malignant thyroid nodules or suspected
benign operable can be taken isthmolobektomi or lobectomy. If after the PA results prove
that the lesion is benign then the operation is complete, but if malignant it must be
determined beforehand which type of carcinoma occurred.
Complications of thyroid surgery:
a. Bleeding from A. Superior thyroid
b. Dispneu
c. Paralysis N. Recurrent Laryngeus. Consequently oto-laryngeal muscle
weakness occurs
d. Paralysis N. Laryngeus Superior. As a result, patients become lenih
sound weak and difficult to control the high pitch sound, due to the
shortening of the vocal cords due to relaxation of
M. Cricothyroid. Possibility terligasi nerve during surgery
21

CHAPTER IV
CONCLUSION
Goitre is a disease that often we encounter daily. It's important to do a history and
physical examination are thorough and meticulous to determine the presence or absence of signs
of toxicity caused by changes in thyroid hormone levels in the body. So also with signs of
malignancy that can be detected in time.
Next is to determine the appropriate tests to determine the exact diagnosis of the
existing types of goitre. With a definite diagnosis then we can mnentukkan appropriate for
treatment of goitre experienced by pasie. Does it require surgery, or simply given treatment
within a certain period.
22

REFERENCES
1. Widjosono, Garitno, Endocrine System: Textbook of Surgery. Editor Syamsuhidayat
R.Jong WB, Revised Edition, EGC, Jakarta, 1997: 925-952.
2. Kariadi KS Sri Hartini, Sumual A., Struma nodosa Non Toxic & Hyperthyroidism:
Textbook of Pneyakit In, Keiga Edition, Publisher Faculty of Medicine, Jakarta,
1996: 757-778.
3. Schteingert David E., Thyroid Disease, Pathophysiology, Fourth Edition, Book Two,
EGC, Jakarta, 1995: 1071-1078.
4. Liberty Kim H, Thyroid Glands: Textbook of Surgery, Volume One, Publisher
Binarupa script, Jakarta, 1997: 15-19.
23