review on gout disease and their treatment
TRANSCRIPT

www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
540
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
REVIEW ON GOUT DISEASE AND THEIR TREATMENT
Sandhya Gorakh Bansode*, Prof. K. N. Tarkase, Sagar Babasaheb Khedkar, Disha
Vikas Kamble, Akshay Nagnath Bhalekar
Dr. Vithalrao Vikhe Patil Foundation, College of Pharmacy, Viladghat, Ahmednagar.
ABSTRACT
Gout is a paiful condition that occurs when uric acid produced by the
body is stored as crystals in the joints and soft tissues. It is a
disturbance of uric acid in the body. Gout is a disorder of purine
metabolism, and occurs when it final metabolite, uric acid, crystallizes
in the form of monosodium urate, precipitating and forming deposits
(tophi) in joints, on tendons, and in the surrounding tissues. It is a
important to recognize that it is a systematic disorder caused by either
overproduction or underexcretion of uric acid. High serum uric acid, or
hyperuricemia, is the causative agent in gout; however, hyperuricemia
is not pathomnemonic of gout. Affecting factors – such as alcohol
abuse, obesity, and genetics determine a predisposition to developing a gout. There are
different types of gout such as Asymptomatic gout, Acute gout, Interval gout, Chronic gout
and Pseudogout. Alcohol consumption, age, postmenoupausal, diet, dehydration, kidney and
thyroid disorders, diuretics and cyclosporines intake, etc are the reasons of causes gout.
People with gout can develop more severe conditions, such as: Recurrent gout, Advanced
gout and kidney stone. Joint fluid test, blood test, x-ray imaging, ultrasound, dual- energy
computerized tomography (DECT) these test are help to identifying the characterization of
gout. Other important points in its management includes patient education, diet and life style
changes, as well as the drug used in the treatment of gout attack.
KEYWORDS: Gout, Hyperuricemia, Uric acid, Monosodium urate crystals, Purine
metabiltes, Pathophysiology of gout, Allopurinol.
INTRODUCTION
Gout is a painful condition that occurs when uric acid produced by the body is stored as
crystals in the joints and / or soft tissues. Located in the joints, these uric acid crystals
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 8, 540-551 Review Article ISSN 2278 – 4357
*Corresponding Author
Sandhya Gorakh Bansode
Dr. Vithalrao Vikhe Patil
Foundation, College of
Pharmacy, Viladghat,
Ahmednagar.
Article Received on
27 May 2021,
Revised on 16 June 2021,
Accepted on 06 July 2021,
DOI: 10.20959/wjpps20218-19496

www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
541
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
precipitate, causing inflammatory arthritis, which, in turn, cause swelling, redness, heat
sensation, pain and functional impotence at the articular level. Although gout is a disease
with a long history (with the description of the syndrome as "pruning" first described by the
ancient Egyptians and later by Hippocrates), the relationship between the disease and uric
acid was only demonstrated in the 19th century by Sir Alfred Baring Garrod, while only in
1909 the gout was assimilated by Sir Archibald Garrod to the acquired metabolic disorders.
Gout, referred to as "disease queen" and "disease of the kings," is a chronic condition, closely
linked to high-value uric acid metabolism, which can form monosodium urate crystals,
identified by Mc Carthy and Hollander in synovial fluid in inflamed joints, becoming gold
standard in the diagnosis of gout, crystals are deposited in the joints, causing joint
inflammation episodic or persistent, having key role in understanding of the disease.
Consecutively has instead increased local temperature, pain and tenderness in the joints
increased (most or at the joint of the hallucus), associated with a very intense night pain. Gout
is not just a metabolic disease in which uric acid is deposited in the joints or tissues, it can,
over time, cause diabetes, atherosclerosis, but also kidney complications. Unfortunately, it is
an invalidating disease, because the deposition at the level of the uric acid causes the joint to
be affected, which changes its appearance and becomes dysfunctional. The increased
production of uric acid is usually determined by purine-rich diets, high-fructose foods or by
increased alcohol consumption. Causes of increased uric acid are increased production,
decreased renal clearance, or a combination of these two mechanisms. The appearance of
gout is influenced by factors such as: sex (men make gout more often than women), age (the
risk increases after age 65); race, nutrition. Some lymph and myeloproliferative
haematological diseases, hemolytic anemia, cutaneous psoriasis, characterized by marked
cellular degradation, are associated with hyperuricemia and gout. Gene mutations of some
enzymes involved in the metabolism of purines (hypoxanthinguanine-phosphoribosyl-
transferase deficiency or increased phosphoribosylpyrophosphate-synthetase activity) are
known genetic causes, but fortunately, rare, hyperuricemia and gout. The elimination of uric
acid from the body is largely by renal elimination, which involves several processes, initially
glomerular filtration, then proximal tubular reabsorption, secretion and finally a new
postsecretory reabsorption.
There are three periods of disease evolution: the period of asymptomatic hyperuricemia - the
crystalline uric acid deposition takes place at the tissue level; acute attacks - the crystals
deposited in the joints cause inflammation, usually at the veil of a single joint; chronic gout -
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
542
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
manifests with persistent joint pain and swelling, uric acid deposits in the soft tissues, called
tofi, usually located intra or periarticularly at the elbows, fingers and toes or at the ears. In
addition to joint manifestations and tofu formation, renal impairment is one of the most
common complications of hyperuricemia.
Gout is a heterogeneous group of sufferers sufferers characterized by hyperuricemia,
recurrent attacks of arthritis (in which synovial fluid contains monosodium urate crystals, and
in leukocytes phagocytosis occurs), tofu formation, especially around the extremity joints
(which sometimes lead to deformities and mutilation) or on the ear flag, parenchymal renal
disease affecting the renal interstitium, nephrons and vessels, uric renal lithiasis. In more than
half of the patients, the metatarsal-phalangeal joint of the hallucinus is damaged. The onset is
usually abrupt, the most frequent at night. Fever is preceded by chills. In chronic form, gouty
stews are almost characteristic. All these symptoms are a major clinical manifestation of
purine metabolism, which increases the amount of uric acid in the body (over 7 mg% in
serum).
Gout is also called as gouty arthritis. A form of arthritis characterized by severe pain, redness
and tenderness. Gout is a general term for a variety of conditions caused by a buildup of uric
acid. This buildup easily affects on feet. Gout is a form of inflammatory arthritis
characterized by recurrent attack of red, tender, hot, and swollen joint. Pain typically comes
on rapidly, reaching, maximal intensity in less than 12 hours. The joint at the base of big toe
is affected in half cases. It may also result in tophi, kidney stones, or kidney damage. Gout is
due to persistently elevated levels of uric acid in the blood. This occurs from a combination
of diet, other health problems, and genetic factors. At high levels, uric acid crystallizes and
the crystals deposit in joints, tendons, and surrounding tissues, resulting in an attack of gout.
Gout occurs more commonly in those who regularly drink beer or sugar-sweetened beverages
or who eat foods that are high purines such as liver, shellfish, or anchovies, or are
overweight. Diagnosis of gout may be confirmed by the presence of crystals in the joint fluid
or in a deposit outside the joint. Blood uric acid levels may be normal during an attack.
Pathophysiology and Treatment of gout
Gout is a disorder of purine metabolism, and occurs when it final metabolite, uric acid,
crystallizes in the form of monosodium urate, precipitating and forming deposits (tophi) in
joints, on tendons, and in the surrounding tissues. Although gout affects peripheral joint, it is
a important to recognize that it is a systematic disorder caused by either overproduction or
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
543
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
underexcretion of uric acid. High serum uric acid, or hyperuricemia, is the causative agent in
gout; however, hyperuricemia is not pathomnemonic of gout. According to studies, 60-95%
of individuals with hyperuricemia do not progress to gout. Therefore researcher posit that
other factors – such as alcohol abuse, obesity, and genetics determine a predisposition to
developing a gout. Additionally many patients with gout will not present with hyperuricemia
in the clinic. It is a important to reiterate, however, that all individual with gout must have
had hyperuricemia at some point in order to develop the disease.
As stated earlier, uric acid is a normal byproduct of purine metabolism. The purine
nucleotides AMP and GMP are broken down into hypoxanthine and xanthine respectively.
Xanthine is converted directly to uric acid by the action of xanthine oxidase (xo). Treatment
of gout target the enzyme xanthine oxidase by inhibiting its production of uric acid, and thus
raising the concentrations of more soluble uric acid precursors, which can be excreted. The
major drug is used to treat gout is Allopurinol, a structural analogue of hypoxanthine. The
action of allopurinol at XO is via another molecule, alloxanthine. Alloxanthine is a structural
analogue of xanthine made by a reaction between allopurinol and XO. Alloxanthine is a
active agent that act as a competitive inhibitor on the XO active site.
There are two principle ways that an individual can achieve hyperurecemia.
Overproduction or underexcreting uric acid. Uric acid is a normal metabolite of purine
catabolism. If purines such as AMP, GMP, or adenine are overproduced, uric acid level rise
consequently. Purine synthesis begins with ribose-5-phosphate and contains many steps that
are highly feedback regulated by purine end products. PRPP synthetase and PRPP
amidotransferase are the major rate determining enzymes of purine biosynthesis, and
consequently, they are high regulated. Mutations in either of thesetwo enzymes could lead to
a loss of feedback control, and thus cause overproduction of purines and eventually uric acid.
Deficiency of other enzymes in the purine synthetic pathway can cause hyperuricemia.
Hypoxanthine-guanine phoshoribosytransferase (HGPRT), for example, is an enzyme that “
salvages” excess purine byproducts and covert them back into nucleotides by the following
reactions:
Hypoxanthine + PRPP ↔ IMP + PPi
If HGPRT is deficient, the body is unable to recycle hypoxanthine back into purine
nucleotides. As a result, hypoxanthine levels build up and forms uric acid. Uderexcretion of
uric acid is other causative factor for hyperucicemia, and therefore gout. Underexcretion of
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
544
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
uric acid typically occurs secondary to kidney disease and accouns for the minority of gout
cases. The vast majority of gout is caused by overoroduction of uric acid by the mechanisms
outlined above.
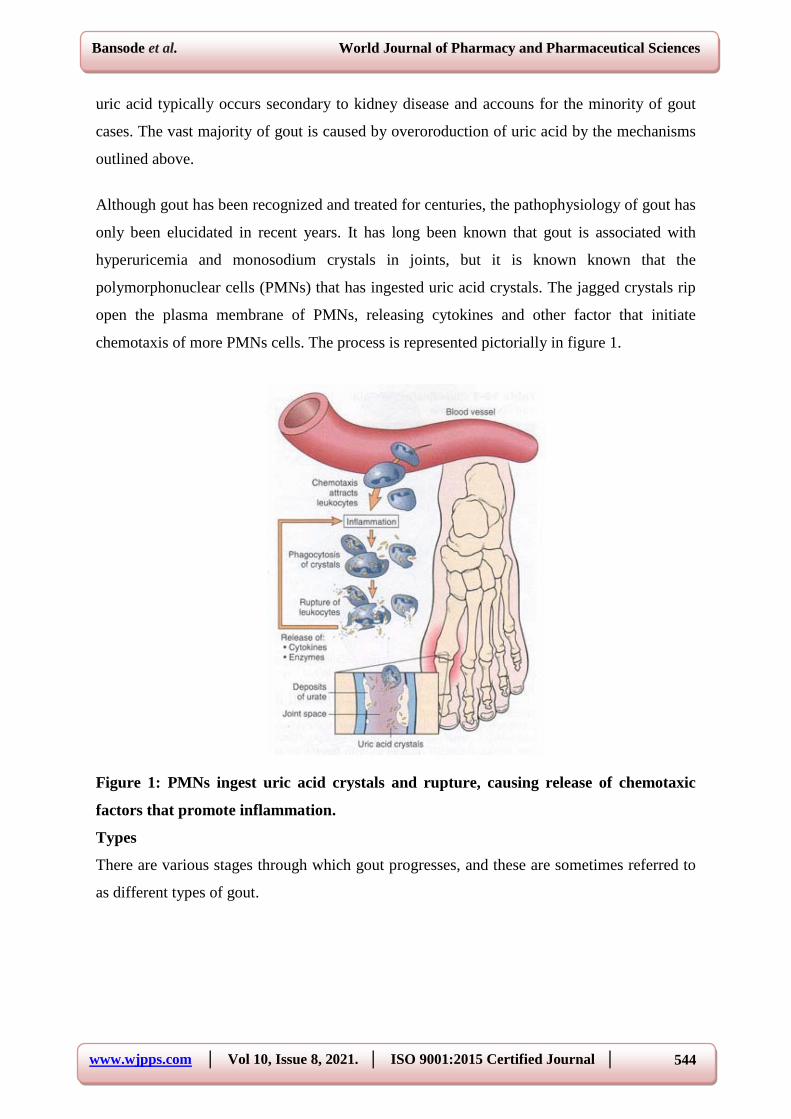
Although gout has been recognized and treated for centuries, the pathophysiology of gout has
only been elucidated in recent years. It has long been known that gout is associated with
hyperuricemia and monosodium crystals in joints, but it is known known that the
polymorphonuclear cells (PMNs) that has ingested uric acid crystals. The jagged crystals rip
open the plasma membrane of PMNs, releasing cytokines and other factor that initiate
chemotaxis of more PMNs cells. The process is represented pictorially in figure 1.
Figure 1: PMNs ingest uric acid crystals and rupture, causing release of chemotaxic
factors that promote inflammation.
Types
There are various stages through which gout progresses, and these are sometimes referred to
as different types of gout.

www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
545
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
Asymptomatic hyperuricemia
It is possible for a person to have elevated uric acid levels without any outward symptoms. At
this stage, treatment is not required, though urate crystals may deposit in tissue and cause
slight damage.
People with asymptomatic hyperuricemia may be advised to take steps to address any
possible factors contributing to uric acid build-up.
Acute gout
This stage occurs when the urate crystals that have been deposited suddenly cause acute
inflammation and intense pain. This sudden attack is referred to as a “flare” and will normally
subside within 3 to 10 days. Flares can sometimes be triggered by stressful events, alcohol
and drugs, as well as cold weather.
Interval or intercritical gout
This stage is the period in between attacks of acute gout. Subsequent flares may not occur for
months or years, though if not treated, over time, they can last longer and occur more
frequently. During this interval, further urate crystals are being deposited in tissue.
Chronic tophaceous gout
Chronic tophaceous gout is the most debilitating type of gout. Permanent damage may have
occurred in the joints and the kidneys. The patient can suffer from chronic arthritis and
develop tophi, big lumps of urate crystals, in cooler areas of the body such as the joints of the
fingers.
It takes a long time without treatment to reach the stage of chronic tophaceous gout – around
10 years. It is very unlikely that a patient receiving proper treatment would progress to this
stage.
Pseudogout
One condition that is easily confused with gout is pseudogout. The symptoms of pseudogout
are very similar to those of gout, although thr flare-ups are usually less severe.
The major difference between gout and pseudogout is that the joints are irritated
by Calcium pyrophosphate crystals rather than urate crystals. Pseudogout requires different
treatment to gout.
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
546
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
Symptoms
The signs and symptoms of gout almost always occur suddenly, and often at night. They
include.
1) Intense joint pain – Gout usually affects the big toe, but it can occurs in any joint. Other
commonly affected joints include the ankles, knees, elbows, wrists and fingers. The pain is
likely to be most severe within the 4 to 12 hours after it begins.
2) Lingering discomfort – After the most severe pain subsides, some joint discomfort may
last from a few days to a few weeks. Later attacks are likely to last longer and affect more
joints.
3)Inflammation and redness – The affected joint or joints become swollen, tender, warm and
red.
4) Limited range of motion – As gout progresses, then may not be able to move joints
normally.
Causes of gout
1. The buildup of uric acid in the blood from breakdown of purines causes gout.
2. Certain conditions, such as blood and metabolism disorders or dehydration, make a body
produce too much uric acid.
3. A kidney or thyroid problems, or an inherited disorders, can make it harder for body to
remove excess uric acid.
4. More likely to get gout if:
a) A middle aged man or postmenopausal woman
b) Have a parents, siblings, or other family members with gout
c) More consumption of alcohol
d) Take medications such as diuretics and cyclosporine
5. Have a condition like high blood pressure, kidney disease, thyroid disease, diabetes, or
sleep apnea also causes a gout.
Risk Factors
More likely to develop gout if high level of uric acid in a body, Factors that increases the uric
acid in a body includes:
1. Diet: Eating a diet rich in red meat and shellfish and drinking beverages sweetened with
fruit sugar (fructose) increase levels of uric acid, which increase the risk of gout. Alcohol
consumption especially of beer, also increases the risk of gout.

www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
547
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. Weight: If overweight, then body produces more uric acid and then kidney have more
difficult time eliminating uric acid.
3. Medical conditions: Certain disease and conditions increase the risk of gout. These include
untreated high blood pressure and chronic conditions such as diabetes, obesity, metabolic
syndrome, and heart and kidney diseases.
4. Certain medications: Low dose aspirin and some medications used to control hypertension-
including thiazide diuretics, angiotensin-converting enzyme (ACE) inhibitors and Beta
blockers- also can increase uric acid levels. So can the use of anti-rejection drugs prescribed
for people who have undergone an organ transplant.
5. Family history of gout: If other member of family have had gout, then more likely to
develop the disease.
6. Age and Sex: Gout occurs more often in men, primarily because women tend to have a
lower uric acid levels. After menopause, however, women’s uric acid levels approach those
of men. Men are also more likely to develop gout earlier usually between the ages of 30 and
50 whereas women generally develop signs and symptoms after menopause.
7. Recent surgery or trauma: Experiencing recent surgery or trauma can sometimes trigger a
gout attack. In some people, receiving a vaccination can trigger a gout flare.
Complications
People with gout can develop more severe conditions, such as.
1. Recurrent gout : Some people may never experience gout signs and symptoms again. Other
may experience gout several times each year. Medications may help to prevent gout attack in
people with recurrent gout. If left untreated gout can cause erosion and destruction of a joint.
2. Advanced gout: Untreated gout may cause a deposits of urate cryatals to form under the
skin in nodules called tophi (TOE- fie). Tophi can develop in several areas, such as fingers,
hands, feet, elbows or Achilles tendons along the backs of ankles. Tophi usually are not
painful, but they can become swollen and tender during gout attacks.
3. Kidney stones : Urate crystals may collect in the urinary tracts of people with gout, causing
kidney stones. Medications can help reduce the risk of kidney stones.
Diagnosis
Doctors usually diagnose gout based on the symptoms and the appearance of the affected
joint. Tests to help diagnose gout may include.
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
548
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
Joint fluid test. Your doctor may use a needle to draw fluid from your affected joint.
Urate crystals may be visible when the fluid is examined under a microscope.
Blood test. Your doctor may recommend a blood test to measure the levels of uric acid in
your blood. Blood test results can be misleading, though. Some people have high uric
acid levels, but never experience gout. And some people have signs and symptoms of
gout, but don't have unusual levels of uric acid in their blood.
X-ray imaging. Joint X-rays can be helpful to rule out other causes of joint inflammation.
Ultrasound. This test uses sound waves to detect urate crystals in joints or in tophi.
Dual-energy computerized tomography (DECT). This test combines X-ray images
taken from many different angles to visualize urate crystals in joints.
Treatment of gout
1. If left untreated, gout can eventually lead to arthritis. This painful condition cal leave a
joint permanently damaged and swollen.
2. The treatment plan recommends will depends on the stages and severity of gout.
3. Medications to treat gout work in one of two ways.
Relieve pain and bring down inflammation
b) Or prevent future gout attacks by lowering uric acid levels.
a) Drugs to relieve gout pain include:
(1) Nonsteroidal anti-inflammatory drugs(NSAIDs), such as aspirin(Bufferin),
ibuprofen(advil, Motrin), and naproxen(Aleve)
(2) Colchicines(Colcrys, Mitigare)
(3) Corticosteroids
b) Drugs that prevent gout attacks include:
(1) Xanthine oxidase inhibitors, such as Allopurinol (Lopurin, Zyloprim) and febuxostat
(Uloric).
(2)Probenecid (Probalan).
4. Along with medications, lifestyle changes to help manage a symptoms and reduce the risk
of future Attacks. For example, reduce the alcohol intake, lose weight, quit smoking, etc.
medications and lifestyle are not the only way to manage gout. A few alternative therapies
have also shown promise.
CONCLUSION
The appearance of gout is favoured by a food containing large amount of nucleic, alcohol and
lead poisoning, probably due to the fact that all these substances have a harmful influence on
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
549
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
renal function. A clear diagnosis is the first step for a correct therapeutic approach. The
diagnosis of gout is made by identifying the monosodium urate crystals at the articular level
and based on the specific clinical signs and hyperurecemia.
REFERENCES
1. Dalbeth N, Merriman TR, Stamp LK. Gout Lancet, 2016; 388(10055): 2039–52.
2. Emmerson BT. The management of gout. New Engl J Med, 1996; 334(7): 445–51.
3. Pascual E, Sivera F. Time required for disappearance of urate crystals from synovial fluid
after successful hypouricaemic treatment relates to the duration of gout. Ann Rheum Dis,
2007; 66(8): 1056–8.
4. Singh JA. Challenges faced by patients in gout treatment: a qualitative study. J Clin
Rheumatol: Practical Rep Rheum Musculoskelet Dis, 2014; 20(3): 172–4.
5. Kuo CF, Grainge MJ, Zhang W, Doherty M. Global epidemiology of gout: prevalence,
incidence and risk factors. Nat Rev Rheumatol, 2015; 11(11): 649–62.
6. McCarty DJ, Hollander JL. Identification of urate crystals in gouty synovial fluid. Ann
Intern Med, 1961; 54: 452–60.
7. Mandal AK, Mount DB. The molecular physiology of uric acid homeostasis. Annu Rev
Physiol, 2015; 77: 323–45.
8. Kamei K, Konta T, Hirayama A, Suzuki K, Ichikawa K, Fujimoto S, et al. A slight
increase within the normal range of serum uric acid and the decline in renal function:
associations in a community-based population. Nephrol, Dialysis, Transplant: official
publication of the European Dialysis and Transplant Association – European Renal
Association, 2014; 29(12): 2286–92.
9. Durcan L, Grainger R, Keen HI, Taylor WJ, Dalbeth N. Imaging as a potentialoutcome
measure in gout studies: A systematic literature review. Semin Arthritis Rheum, 2016;
45(5): 570–9.
10. Dalbeth N, Clark B, McQueen F, Doyle A, Taylor W. Validation of a radiographic
damage index in chronic gout. Arthritis Rheum, 2007; 57(6): 1067–73.
11. Nestorova R, Fodor D. Crystal-induced arthritis. In: El Miedany Y,
editor.Musculoskeletal ultrasonography in rheumatic diseases. Cham: Springer
International Publishing, 2015; 137–67.
12. Grassi W, Gutierrez M, Filippucci E. Chapter 16 - crystal-associated synovitis A2 –
Wakefield, Richard J. In: D’Agostino MA, editor. Essential applications of
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
550
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
musculoskeletal ultrasound in rheumatology. Philadelphia: Content Repository Only!,
2010; 187–97.
13. Filippucci E, Di Geso L, Grassi W. Tips and tricks to recognize microcrystalline arthritis.
Rheumatol (Oxford, England), 2012; 51(Suppl 7): vii18–21.
14. Gutierrez M, Smith W, Thiele R, Keen H, Kaeley G, Naredo E, et al. Defining elementary
ultrasound lesions in gout. Preliminary results of Delphi consensus and web-exercise
reliability. Ann Rheum Dis, 2014; 73(Suppl 2): 302.
15. Wright SA, Filippucci E, McVeigh C, Grey A, McCarron M, Grassi W, et al. High-
resolution ultrasonography of the first metatarsal phalangeal joint in gout: a controlled
study. Ann Rheum Dis, 2007; 66(7): 859–64.
16. Filippucci E, Riveros MG, Georgescu D, Salaffi F, Grassi W. Hyaline cartilage
involvement in patients with gout and calcium pyrophosphate deposition disease. An
ultrasound study. Osteoarthr Cartilage, 2009; 17(2): 178-81.
17. Nicolaou S. Invited commentary. Radio Graph, 2011; 31(5): 1376–7.
18. Huppertz A, Hermann KG, Diekhoff T, Wagner M, Hamm B, Schmidt WA. Systemic
staging for urate crystal deposits with dual-energy CT and ultrasound in patients with
suspected gout. Rheumatol Int, 2014; 34(6): 763–71.
19. Bongartz T, Glazebrook KN, Kavros SJ, Murthy NS, Merry SP, Franz 3rd WB, et al.
Dual-energy CT for the diagnosis of gout: an accuracy and diagnostic yield study. Ann
Rheum Dis, 2015; 74(6): 1072–7.
20. Melzer R, Pauli C, Treumann T, Krauss B. Gout tophus detection-a comparison of dual-
energy CT (DECT) and histology. Semin Arthritis Rheum, 2014; 43(5): 662–5.
21. McQueen FM, Doyle AJ, Reeves Q, Gamble GD, Dalbeth N. DECT urate deposits: now
you see them, now you don’t. Ann Rheum Dis, 2013; 72(3): 458–9.
22. Glazebrook KN, Guimaraes LS, Murthy NS, Black DF, Bongartz T, Manek NJ, et al.
Identification of intraarticular and periarticular uric acid crystals with dual-energy CT:
initial evaluation. Radiology, 2011; 261(2): 516–24.
23. Chowalloor PV, Siew TK, Keen HI. Imaging in gout: A review of the recent
developments. Therap Adv Musculoskelet Dis, 2014; 6(4): 131–43.
24. Toprover M, Krasnokutsky S, Pillinger MH. Gout in the spine: imaging, diagnosis, and
outcomes. Curr Rheumatol Rep, 2015; 17(12): 70.
25. Zheng ZF, Shi HL, Xing Y, Li D, Jia JY, Lin S. Thoracic cord compression due to
ligamentum flavum gouty tophus: a case report and literature review. Spinal Cord, 2015;
53(12): 881–6.
www.wjpps.com │ Vol 10, Issue 8, 2021. │ ISO 9001:2015 Certified Journal │
551
Bansode et al. World Journal of Pharmacy and Pharmaceutical Sciences
26. Nunes EA, Rosseti Jr AG, Ribeiro DS, Santiago M. Gout initially mimicking rheumatoid
arthritis and later cervical spine involvement. Case Rep Rheumatol, 2014; 2014: 357826.
27. Ahmad I, Tejada JG. Spinal gout: a great mimicker. A case report and literature review.
Neuroradiol J, 2012; 25(5): 621–5.
28. Nygaard HB, Shenoi S, Shukla S. Lower back pain caused by tophaceous gout of the
spine. Neurology, 2009; 73(5): 404.
29. Hsu CY, Shih TT, Huang KM, Chen PQ, Sheu JJ, Li YW. Tophaceous gout of the spine:
MR imaging features. Clin Radiol, 2002; 57(10): 919–25.
30. Gongidi P, Gough-Fibkins S. Spondyloarthritis: a gouty display. J Radiol Case Rep,
2010; 4(5): 13–8.
31. Zhao Z, Wang Y, Jin J, Deng X, Huang F. An analysis of abnormal magnetic resonance
imaging of sacroiliac joints in patients misdiagnosed as spondyloarthritis. Zhonghua nei
ke za zhi, 2014; 53(9): 724–9.
32. Kang HJ, Jung SH, Yoon HK, Hahn SB, Kim SJ. Carpal tunnel syndrome caused by
space occupying lesions. Yonsei Med J, 2009; 50(2): 257–61.
33. Chen CK, Chung CB, Yeh L, Pan HB, Yang CF, Lai PH, et al. Carpal tunnel syndrome
caused by tophaceous gout: CT and MR imaging features in 20 patients. AJR Am J
Roentgenol, 2000; 175(3): 655–9.
34. Godfrin-Valnet M, Godfrin G, Godard J, Prati C, Toussirot E, Michel F, et al.Eighteen
cases of crowned dens syndrome: Presentation and diagnosis. Neurochirurgie, 2013;
59(3): 115–20.
35. Udayakumar D, Kteleh T, Alfata S, Bali T, Joseph A. Spinal gout mimicking paraspinal
abscess: A case report. J Radiol Case Rep, 2010; 4(6): 15-20.