revision phase 4 paeds
DESCRIPTION
paediatric contentTRANSCRIPT

Revision Phase 4
5/1/2012

Nephrotic syndrome in childhood
Criteria for diagnosis• Early morning urine protein/creatinine ratio
>200mg/mmol (urine protein loss of >40 mg/m2 H) UPCI
• Hypoalbuminaemia <25 g/L• Oedema• Hypercholestremia +/-

Primary causes• Pos-tinfectious etiologies • Collagen vascular disease (systemic lupus erythematosus,
rheumatoid arthritis, polyarteritis nodosa) • Henoch-Schönlein purpura • Hereditary nephritis • Sickle cell disease • Diabetes mellitus • Amyloidosis • Malignancy (leukemia, lymphoma, Wilms tumor,
pheochromocytoma) • Toxins (bee sting, poison ivy and oak, snake venom) • Medications (probenecid, fenoprofen, captopril, lithium, warfarin,
penicillamine, mercury, gold, trimethadione, paramethadione) • Heroin use

Secondary causes
Related to post-infectious causes :• Group A beta-hemolytic streptococci • Syphilis • Malaria • Tuberculosis • Viral infections (varicella, hepatitis B, HIV type
1, infectious mononucleosis)

Standard definitions in SSNS
• Remission Urine protein dipstick (Albustix) reading 0 or trace for 3 consecutive days
• Relapse Albustix reading 2+ or more 3 consecutive days having previously been in remission
• Frequently relapsing 2 or more relapses within 6 months of initial response or 4 or more within any 12 month period
• Steroid dependent 2 consecutive relapses occurring during corticosteroid treatment or within 14 days after its
cessation• Steroid sensitive Normalization of proteinuria within 4 weeks
after start of standard initial therapy of daily oral prednisolone
• Steroid resistant Failure to achieve remission in spite of 4 weeks of oral prednisolone of 60mg/m2/day to
maximum of 80 mg/day

Complications?
Acute complications• Hypovolaemia• Infection : Peritonitis / Septecemia / cellulitis• Thrombosis: Arteial / venous
Others• Acute renal failure: Prerenal uremia / acute tubular
necrosis• Hyperlipidaemia: Hypercholesterolaemia / increased
plasma LDL and VLDL• Protein malnutrition (cachexia)

Atypical features?
• Age <1 year or > 12 years• Persistent hypertension• Gross haemeturia (microscopic in 25%)• Renal impairment not due to hypovolaemia
(↑plasma creatinine)• ↓Plasma C3

AGN Complications
• Acute renal impairment• Hypertensive encephalopathy• Acute left ventricular failure
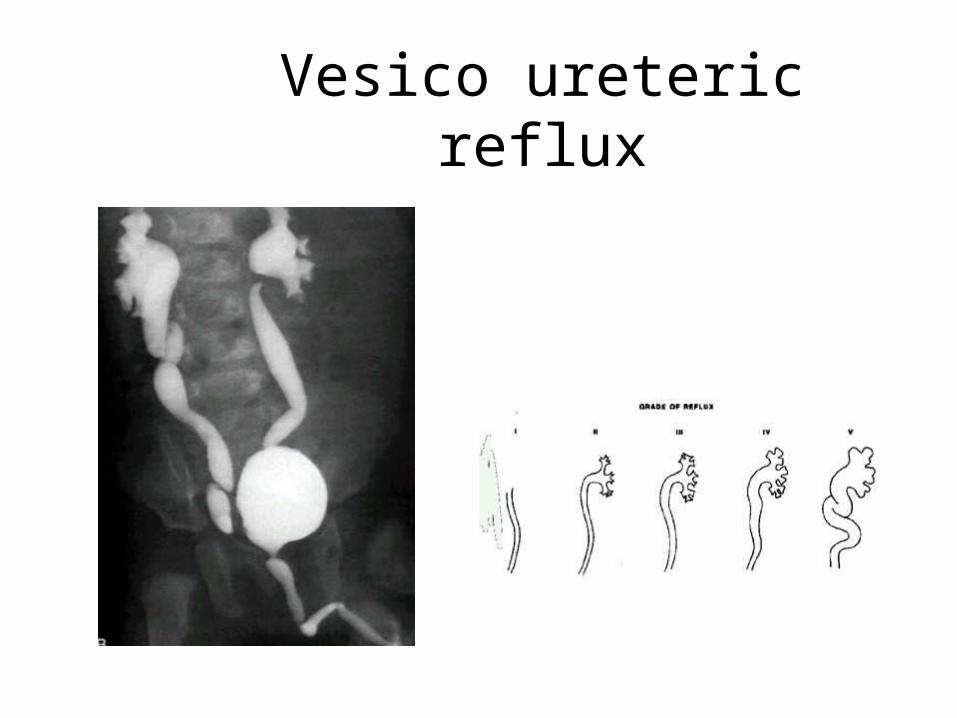
Vesico ureteric reflux

Idiopathic Immune Thrombocytopenia
Extensive petechiae and purpuraon the legs
Conjunctival hemorrhage

Haemarthrosis

Henoch–Schonlein purpuraClassification criteria for HSP:
Palpable purpura (mandatory) in thepresence of at least one of the followingfour features:
– Diffuse abdominal pain– Arthritis (acute) or arthralgia– Renal involvement (any haematuria
and/or proteinuria)– Any biopsy showing predominant IgA
deposition
Palpable purpura often symmetricallydistributed over the extensor,dependent surfaces of the lowerlimbs and buttocks.It may involve the arms, face andears but usually spares the trunk.

Aedes aegypti Mosquito
Dengue Fever andDengue Haemorrhagic Fever

Clinical Case Definition forDengue Hemorrhagic Fever
4 Necessary Criteria:
Usually develops around 3rd –7th day of illness• Fever, or recent history of acute fever• Hemorrhagic manifestations• Low platelet count (100,000/mm3 or less)• Objective evidence of “leaky capillaries:”
– elevated hematocrit (20% or more over baseline)– low albumin– pleural or other effusions

Four Grades of DHF
• Grade 1– Fever and nonspecific constitutional symptoms– Positive tourniquet test is only hemorrhagic manifestation
• Grade 2– Grade 1 manifestations + spontaneous bleeding
• Grade 3– Signs of circulatory failure (rapid/weak pulse, narrow pulse
pressure, hypotension, cold/clammy skin)
• Grade 4– Profound shock (undetectable pulse and BP)

Warning Signs for Dengue Shock
When Patients Develop DSS:• 3 to 6 days after onset of symptoms
When Patients Develop DSS:• 3 to 6 days after onset of symptoms
Initial Warning Signals:• Disappearance of fever• Drop in platelets• Increase in hematocrit
Initial Warning Signals:• Disappearance of fever• Drop in platelets• Increase in hematocrit
Alarm Signals:• Severe abdominal pain• Prolonged vomiting• Abrupt change from fever to hypothermia• Change in level of consciousness (irritability or somnolence)
Alarm Signals:• Severe abdominal pain• Prolonged vomiting• Abrupt change from fever to hypothermia• Change in level of consciousness (irritability or somnolence)
Four Criteria for DHF:• Fever• Hemorrhagic manifestations• Excessive capillary permeability• 100,000/mm3 platelets
Four Criteria for DHF:• Fever• Hemorrhagic manifestations• Excessive capillary permeability• 100,000/mm3 platelets

SEROLOGY
• 10 dengue Infection:– IgM produced by 5th day of symptoms and persists
for 30-60 days.– IgG appears by 14th day and persist for life.
• 20 dengue Infection:– Induces IgM response after 20 days of infection.– IgG rises within 1-2 days after onset of symptoms

Criteria for admission (any of the following) in the presence of suspicion of dengue fever
• Restlessness or lethargy• Cold extremities or circumoral cyanosis• Bleeding in any form• Oliguria or reluctance to drink fluids• Rapid and weak pulse• Capillary refill time > 2 seconds• Narrowing of pulse pressure <20mmHg or hypotension• Haematocrit of 40%, or rising• Platelet count of <100,000• Acute abdomianl pain• Evidence of plasma leakage: pleural effusion, ascitis

Fever
• Enhances immune functioning• Antipyretics
– ↑length of illness and viral shedding– Negative impact on bacterial illness– ↓vaccine antibody response
John Mc Intyre Arch Dis Child 2011;96:1175-1179

Paracetamol
Clinical phases after toxic ingestion.1 Early symptoms (1st day): nausea, vomiting2 Latent phase (1-2days): may have some
improvement over the next 48 hours but liver enlarges and LFT rises
3 Liver failure (3-5 days): enlarged tender liver, jaundice, hypoglycemia, hypotension, varied cardiac arrhythmia and metabolic acidosis, acute haemolytic anaemia and hypothrombinaemia

IronAcute poisoning occurs in stages:
1. Stage I (30 mins-12 hrs)Local toxicity: Acute GIT upsets with epigastric pain, nausea, vomiting, dehydration, haemetemesis and bloody diarrhoea
2. Stage II (8-16 hrs)Systemic toxicity: Signs of acute encephalopathy (severe headache, confusion, delirium, convulsions and coma), acidosis and circulatory collapse and hepatic impairment may occur
3. Stage III (2-5 wks)Late complications: GIT stricture

Salicylate
• Stimulates CNS directly to cause hyperpnoea and produce metabolic derangement with accumulation of organic acids
• Blood pCO2, HCO3 and pH fall progressively• At therapeutic doses interferes with platelet aggregation- >
bleeding time• Toxic doses lowers plasma PT levels by interfering with
utilization of vitamin K in the liver• Gastric mucosal injury and gastric bleeding (presence of
alcohol increases mucosal injury)
• Severe– Severe hyperpnea, coma, cyanosis, oliguria,
uremia, pulmonary oedema, and respiratory failure. Hypoglycemia
• Anaphylactic reaction – Asthmatics should avoid
Clinical features acute poisoning

Salicylate Monogram

Contraindications for lumbar puncture in suspected acute bacterial meningitis
• Signs suggesting raised intracranial pressure– Reduced or fl uctuating level of consciousness (Glasgow coma scale score <9 or a drop of 3 or more)– Relative bradycardia and hypertension– Focal neurological signs– Abnormal posture or posturing– Unequal, dilated, or poorly responsive pupils– Papilloedema– Abnormal ‘doll’s eye’ movements
• Shock• Extensive or spreading purpura• Convulsions• Coagulation abnormalities
– Coagulation results (if obtained) outside the normal range– Platelet count below 100×109/litre– Receiving anticoagulants
• Local superfi cial infection at the lumbar puncture site• Respiratory insuffi ciency

Stridor
• Comfortable position with parent• Oxygen-nasal prong only +
oximetry• Steroid 0.6 mg/im (max 12 mg)
stat, then prednisolone 1 mg/kg 8-12 hourly
• Epinephrine 1/1000, 0.5 ml/kg/dose (max 6 ml) repeat in 2 hours if required (improves in 30 min lasts 2 hours)
• Encourage oral fluids• Intubation and tracheostomy
• Viruses causing croup– PI (commonest), RSV, Inlfuenza virus, measles virus
• Bacterial– Staph, streptococcus– Diphtheria– H. influenza
• FB and inhalation of hot gases• Acute angioneurortic oedema• Expanding mediasternal masses• tetany
Aetiology

Characteristic findings in Bronchiolitis
– Sharp dry cough following coryzal– Cyanosis or pallor– Tachypnoea, apnoea <4mo– Subcoastal, intercostals recession– Hyperinflation of chest
• prominent sternum• Liver displaced downwards
– Auscultation• Fine end-inspiratory crackles• Prolonged expiration

Bronchiolitis treatment
• Oxygen by nasal cannula• Pulse oximetry and apnoea monitor• Nebulised ipratropium, bronchodilator• Fluids by NG or IV• Ventilation 2%• Ribavirin
– Shortens viral excretion and clinical sympoms– In cardiopulmonary disorders, immune deficiency
• Palivizumab- high risk preterms
Observe: colour, RR and pattern of breathing
Oxygen saturation


Acute asthma Mx.
• Give oxygen– Nasal prong/cannula 1-2L/min– Partial rebreathing mask, 10-12L/min-50-60%– Non-rebreathing mask, 10-15L/min-95%– Venturi-type, room air with O2 25-60%
• Monitoring + pulse oximeter• Hydration• Nebulised bronchodilator
– 6-9L of oxygen driven, volume of 4 ml over 20 min and 3X in 1 hour• Steroids
– Oral 1-2 mg/kg/day or IV 4mg/kg hydrocortisone

Agents causing pneumonia in children
• VirusesRSV,PI: infants and young children– Mycoplasma,
commonest in school going children
• Bacteria– Pneumococcus all ages
common– Haemophilus influenza– Staphylococcus aureus

World Health Organization Revised 1990
MANAGEMENT OF THE PATIENT WITH DIARRHOEALoose or watery stool loose stools with blood
FIRST, ASSESS YOUR PATIENT FOR DEHYDRATION
A B C
1.LOOK AT: CONDITION EYES TEARS MOUTH AND TONGUE THIRST
Well, alertNormalPresentMoistDrinks normally not thirsty
Restless, irritableSunkenAbsentDryThirsty, drinks eagerly
Lethargic or unconscious, floppyVery sunken and dryAbsentVery dryDrinks poorly or not able to drink
1.FEEL SKIN PINCH
Goes back quickly Goes back slowly Goes back very slowly
1.DECIDE The patient has NO SIGNS OF DEHYDRATION
If the patient has two or more signs including at least one sign there is SOME DEHYDRATION
If the patient has two or more signs including at least one sign, there is SEVERE DEHYDRATION
1.TREAT Use Treatment Plan A Weigh the patient, if possible, and use Treatment Plan B
Weigh the patient AND USE Treatment Plan C URGENTLY