revisiting the therapeutic potential of leptin david litzinger, phd director, pharmaceutical...
TRANSCRIPT

Revisiting the Therapeutic Potential of LeptinRevisiting the Therapeutic Potential of Leptin
David Litzinger, PhD
Director, Pharmaceutical Sciences
Amylin Pharmaceuticals, Inc.
2011 AAPS National Biotechnology Conference
San Francisco, CA
2
Leptin HistoryLeptin History
• 1950 Obese mice appear randomly in a colony at Jackson Laboratory.
• 1994 Dr. Jeffrey Friedman and colleagues at Rockefeller University discover the ob gene and protein, and explore their role in body weight regulation, appetite, and metabolism.
• 1997 Amgen begins clinical trials of leptin for obesity.
• 1999 Amgen publishes disappointing obesity trial results.
• 2007 Amylin conducts clinical POC test of leptin/pramlintide combination; reduces bodyweight on average by 12.7% over 24 weeks.
• 2009 A 28-week pramlintide/leptin clinical study, followed by a 52-week extension study, showed sustained and robust weight-loss.
• 2010 Amylin submits the initial sections of a rolling submission for a BLA for the use of leptin to treat patients with rare forms of
lipodystrophy.
• 2011 Amylin and JDRF announce that they entered into a research collaboration agreement to provide financial support for a clinical
POC study to investigate leptin in patients with type 1 diabetes.

3
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body Weight
Amylin
Question: Why aren’t anti-obesity drugs more effective?
Adapted from Badman M.K. and Flier J.S. Science 2005; 307: 1909-1914.
GI tract
Adipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents

4
Pramlintide (25,28,29Pro-h-amylin)Pramlintide (25,28,29Pro-h-amylin)
• 3949.4 Da, 37 amino acids
• Isoelectric point 5.3
• Single disulfide bond, C-term amidated
• No free cysteines
• Limited solubility at neutral pH (<0.5 mg/mL), higher at lower pH
5
0 2 4 6 8 10 12-10
-8
-6
-4
-2
0
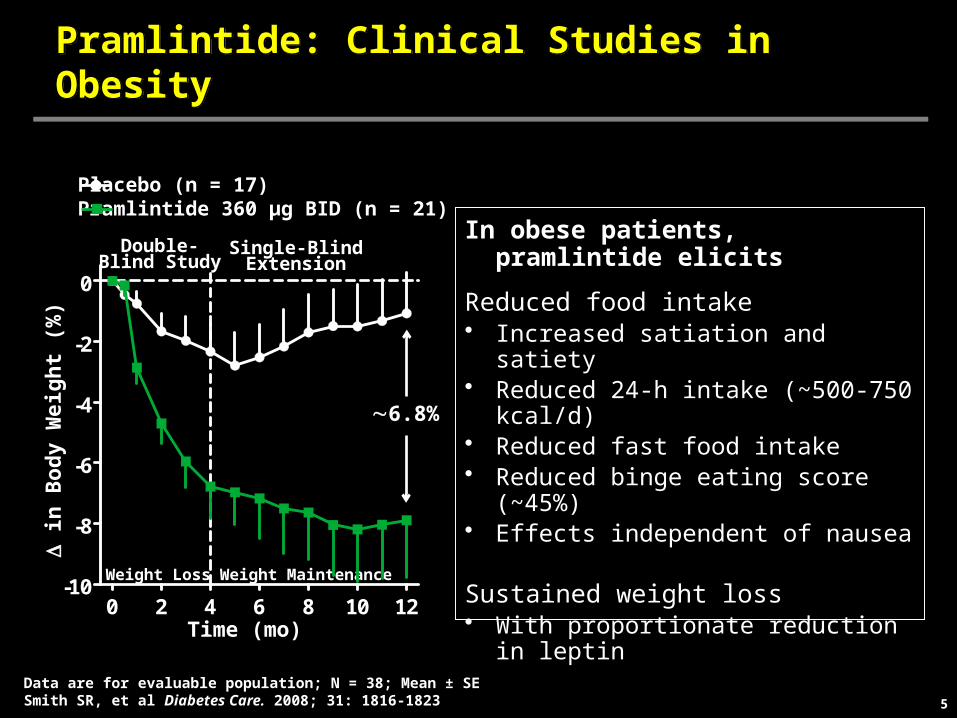
Pramlintide: Clinical Studies in ObesityPramlintide: Clinical Studies in Obesity
Time (mo)
D in
Bo
dy
Wei
gh
t (%
)
6.8%
Weight Loss Weight Maintenance
In obese patients, pramlintide elicits
Reduced food intake• Increased satiation and satiety• Reduced 24-h intake (~500-750 kcal/d)• Reduced fast food intake• Reduced binge eating score (~45%)• Effects independent of nausea
Sustained weight loss• With proportionate reduction in leptin
Placebo (n = 17)Pramlintide 360 µg BID (n = 21)
Data are for evaluable population; N = 38; Mean ± SESmith SR, et al Diabetes Care. 2008; 31: 1816-1823
Double-Blind Study
Single-BlindExtension

6
• 16.2 kDa, 147 amino acids, (native leptin 146 AA)
• Isoelectric point 6.1
• Single disulfide bond
• No free cysteines
• Limited solubility at neutral pH (2-3 mg/mL), higher at lower pH
• Four helix bundle tertiary structure
Metreleptin (r-metHuLeptin)Metreleptin (r-metHuLeptin)
7
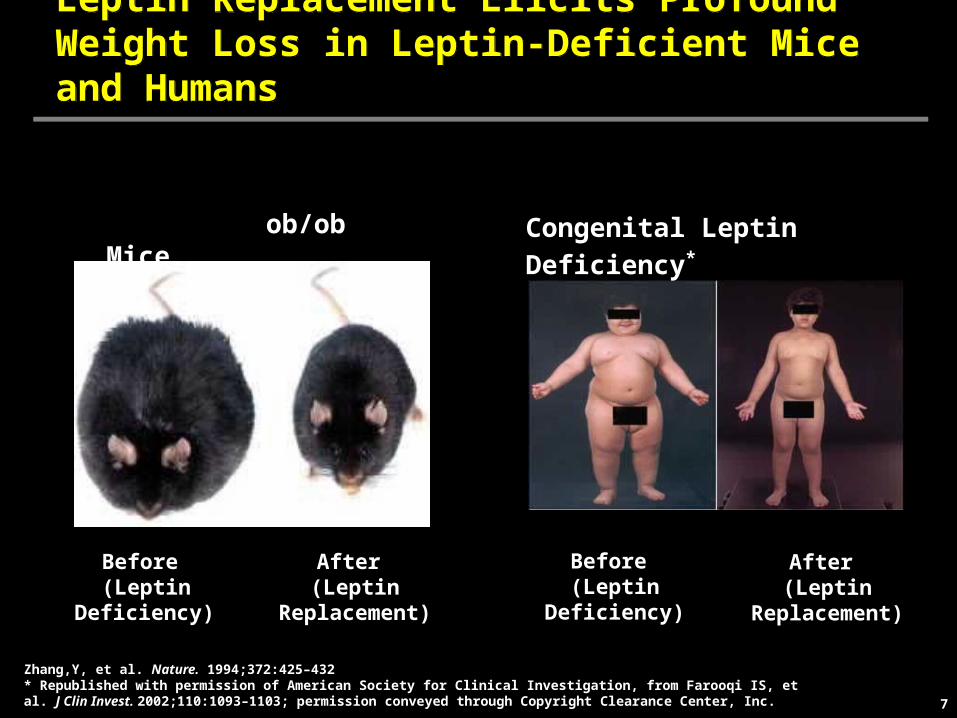
Leptin Replacement Elicits Profound Weight Loss in Leptin-Deficient Mice and HumansLeptin Replacement Elicits Profound Weight Loss in Leptin-Deficient Mice and Humans
ob/ob Mice
Before (Leptin Deficiency)
After (Leptin Replacement)
Congenital Leptin Deficiency*
Before (Leptin Deficiency)
After (Leptin Replacement)
Zhang,Y, et al. Nature. 1994;372:425–432* Republished with permission of American Society for Clinical Investigation, from Farooqi IS, et al. J Clin Invest. 2002;110:1093–1103; permission conveyed through Copyright Clearance Center, Inc.
8
-3 0 3 6 9 12-5
-4
-3
-2
-1
0
1
2
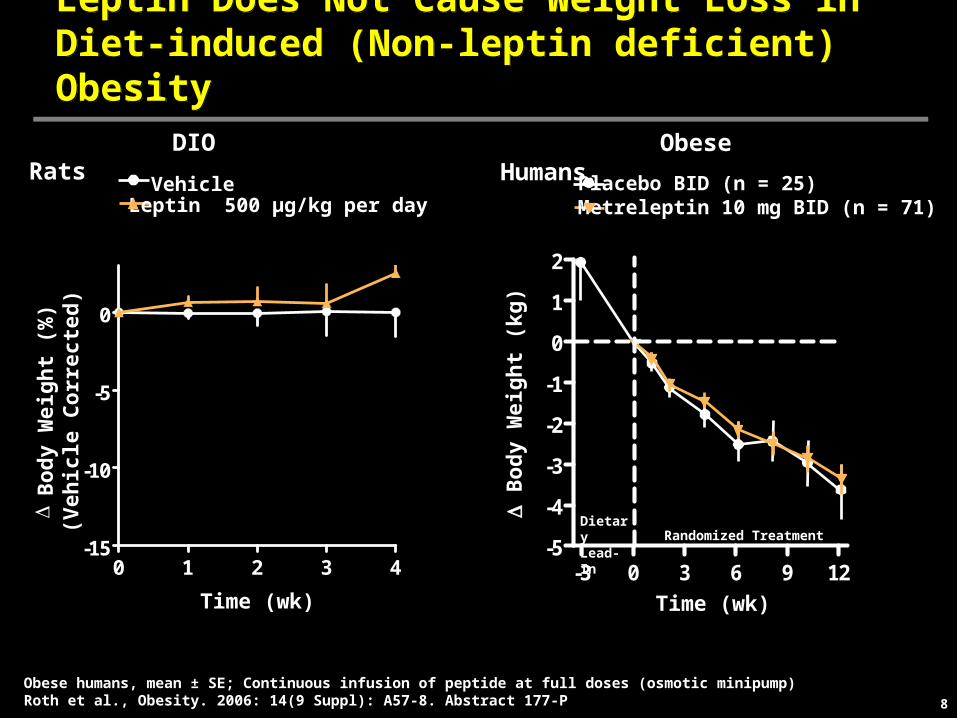
Leptin Does Not Cause Weight Loss in Diet-induced (Non-leptin deficient) ObesityLeptin Does Not Cause Weight Loss in Diet-induced (Non-leptin deficient) Obesity
Obese Humans
Time (wk)
D B
od
y W
eig
ht
(kg
)
Obese humans, mean ± SE; Continuous infusion of peptide at full doses (osmotic minipump) Roth et al., Obesity. 2006: 14(9 Suppl): A57-8. Abstract 177-P
Placebo BID (n = 25)Metreleptin 10 mg BID (n = 71)
Dietary Lead-In Randomized Treatment
DIO Rats
0 1 2 3 4-15
-10
-5
0
DB
od
y W
eig
ht
(%)
(Veh
icle
Co
rrec
ted
)
Time (wk)
VehicleLeptin 500 µg/kg per day

9
0 3 6 9 120
50
100
150
200
250
Roth JD, et al. Proc Natl Acad Sci USA. 2008;105:7257–7262.
Food Intake
Cu
mu
lati
ve F
oo
d In
take
(g
ram
s)
*
*p<0.05 compared to all groupsDiet-induced obesity prone rats (CRL; N=7/group).
Amylin+Leptin Synergy for Weight Loss is not Explained by the Anorexigenic Effect of AmylinAmylin+Leptin Synergy for Weight Loss is not Explained by the Anorexigenic Effect of Amylin
Amylin+Leptin
VehicleLeptin 500 µg/kg/d
Amylin 100 µg/kg/d
(Pairfed-Amylin)+Leptin
Time (Days)
0 3 6 9 12-14
-12
-10
-8
-6
-4
-2
0
2 Body Weight
% C
han
ge
in B
od
y W
eig
ht
(Veh
icle
-Co
rrec
ted
)*
Time (Days)

10
Veh A+LPF
AdiposeTissue(H&E)
Amylin/Leptin Induced Greater Fat Loss and Prevented Counter Regulatory AdaptationsAmylin/Leptin Induced Greater Fat Loss and Prevented Counter Regulatory Adaptations
Trevaskis JL et al. Endocrinology. 2008; 149(11):5679-87
• Amylin + Leptin treated DIO rats lost nearly 2-fold greater fat mass than pair-fed control*
• Amylin + Leptin prevented metabolic counter-regulatory adaptations
− No decrease in energy expenditure as was seen in pair-fed controls (oxygen consumption results)
− Fat utilized throughout study whereas pair-fed controls initially showed fat followed by carbohydrate utilization (respiratory quotient results)
*Pair-fed control: no leptin or amylin
11
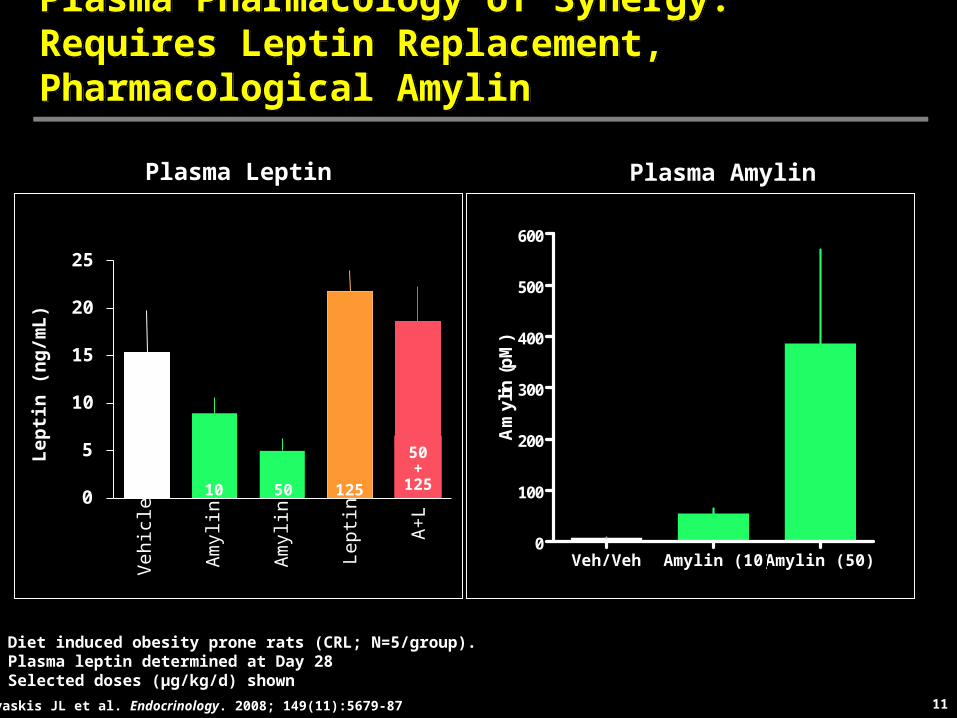
Plasma Pharmacology of Synergy: Requires Leptin Replacement, Pharmacological AmylinPlasma Pharmacology of Synergy: Requires Leptin Replacement, Pharmacological Amylin
0
5
10
15
20
25
Lep
tin
(n
g/m
L)
10 50 125
50+
125
Lep
tin
A+
L
Am
ylin
Am
ylin
Veh
icle
Diet induced obesity prone rats (CRL; N=5/group).Plasma leptin determined at Day 28Selected doses (µg/kg/d) shown
Trevaskis JL et al. Endocrinology. 2008; 149(11):5679-87
Plasma Leptin
Veh/Veh Amylin (10) Amylin (50)0
100
200
300
400
500
600
Am
ylin
(p
M)
Plasma Amylin

12
Amylin Upregulated pSTAT3 Signaling in the Ventromedial Hypothalamus in DIO RatsAmylin Upregulated pSTAT3 Signaling in the Ventromedial Hypothalamus in DIO Rats
Ventromedial Hypothalamus
Lean Vehicle PF Amylin0
100
200
300
400
500
*, **
DIO Rats
pS
TA
T3-
Act
ivat
ed C
ells
(n
)
Lean Harlan Sprague Dawley rats or DIO-prone rats; Mean ± SE; *P<0.05 vs vehicle controls; **P<0.05 vs PF(amylin) Roth JD, et al. Proc Natl Acad Sci U S A. 2008;105:7257–7262
Vehicle ControlsLeptin 15 mg/kg i.p.
Lean DIO–Vehicle
DIO–PF DIO–Amylin
Leptin-Stimulated pSTAT3 Shown

13
– Design: Randomized, double-blind, controlled, multicenter– Study population: Overweight or obese subjects (BMI 27-35 kg/m2)– Treatment: 4-week lead-in requiring 2-8% weight loss followed by 20
weeks randomized treatment 2:2:1 pramlintide: pramlintide/metreleptin: metreleptin
– Primary efficacy endpoint: Weight loss in pramlintide vs pramlintide/metreleptin
Pramlintide/Metreleptin: Phase 2 Clinical Proof-of-Concept StudyPramlintide/Metreleptin: Phase 2 Clinical Proof-of-Concept Study
Placebo-P + Metreleptin 5 mg BID
Pramlintide 360 µg BID + Placebo-M
Pramlintide 360 µg BID + Metreleptin 5 mg BID36
0 µ
g B
IDP
ram
lin
tid
e
18
0 µ
g B
IDP
ram
lin
tid
e
40% kcal deficit 20% kcal deficit
Lead-in Randomized Treatment
Day 1Screen -4 161 4 8 12 20-2
Roth JD et al Proc Natl Acad Sci USA. 2008; 105: 7257-7262.
Time (wk)
14
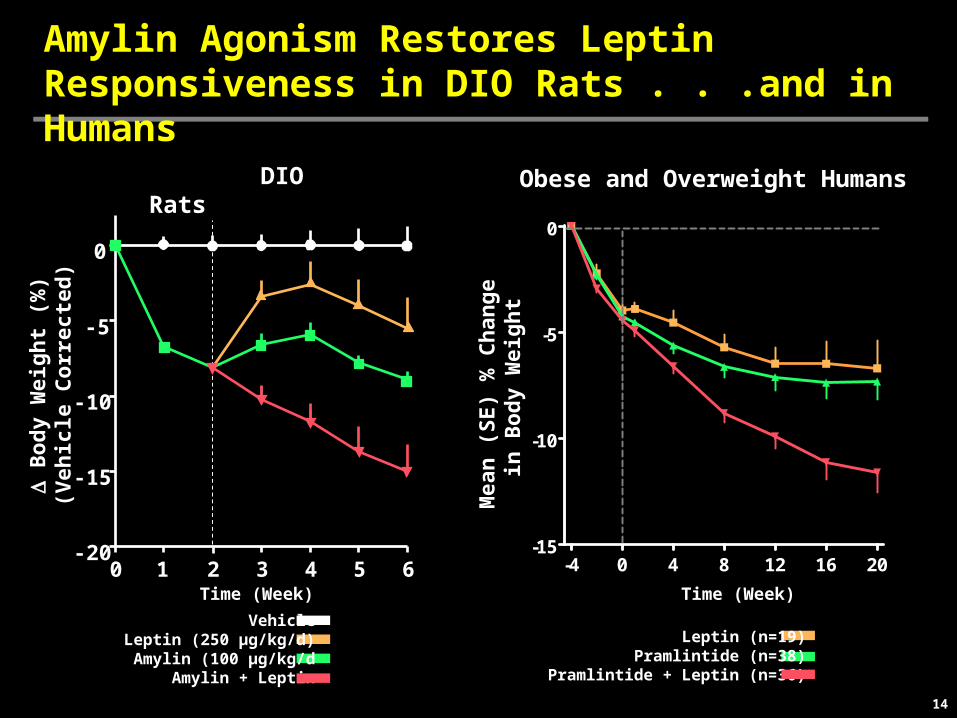
Amylin Agonism Restores Leptin Responsiveness in DIO Rats . . .and in Humans
Obese and Overweight Humans DIO Rats
Time (Week)
-4 0 4 8 12 16 20-15
-10
-5
0
Time (Week)
Mea
n (
SE
) %
Ch
ang
e in
Bo
dy
Wei
gh
t
Leptin (n=19)Pramlintide (n=38)
Pramlintide + Leptin (n=36)
VehicleLeptin (250 µg/kg/d)Amylin (100 µg/kg/d
Amylin + Leptin
0 3 4 5 61 2-20
-15
-10
-5
0
D B
od
y W
eig
ht
(%)
(Veh
icle
Co
rrec
ted
)
15
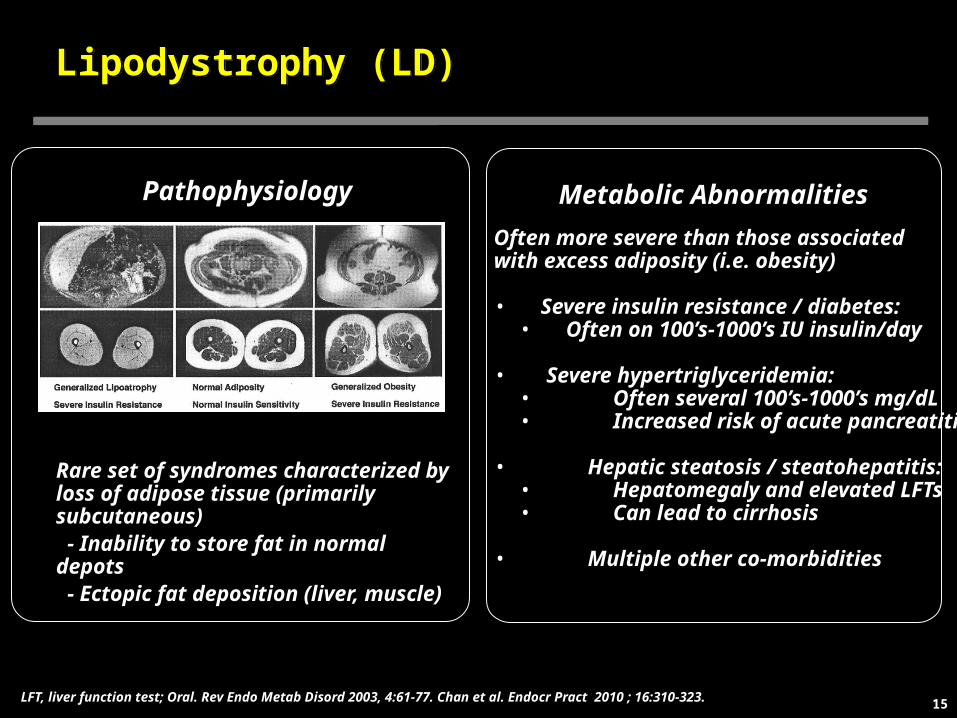
Lipodystrophy (LD)Lipodystrophy (LD)
Pathophysiology
Rare set of syndromes characterized by loss of adipose tissue (primarily subcutaneous) - Inability to store fat in normal depots - Ectopic fat deposition (liver, muscle)
Often more severe than those associated with excess adiposity (i.e. obesity)
• Severe insulin resistance / diabetes:• Often on 100’s-1000’s IU insulin/day
• Severe hypertriglyceridemia: • Often several 100’s-1000’s mg/dL • Increased risk of acute pancreatitis
• Hepatic steatosis / steatohepatitis: • Hepatomegaly and elevated LFTs• Can lead to cirrhosis
• Multiple other co-morbidities
Metabolic Abnormalities
LFT, liver function test; Oral. Rev Endo Metab Disord 2003, 4:61-77. Chan et al. Endocr Pract 2010 ; 16:310-323.
16
0 4 8 1280
100
120
140
160
180
200
55 40 43 39
Number of Patients
Time (months)
Me
an
(S
E)
FP
G (
mg
/dL
)
0 4 8 125
6
7
8
9
10
54 40 41 38
Number of Patients
Time (months)
Me
an
(S
E)
Hb
A1
c (
%)
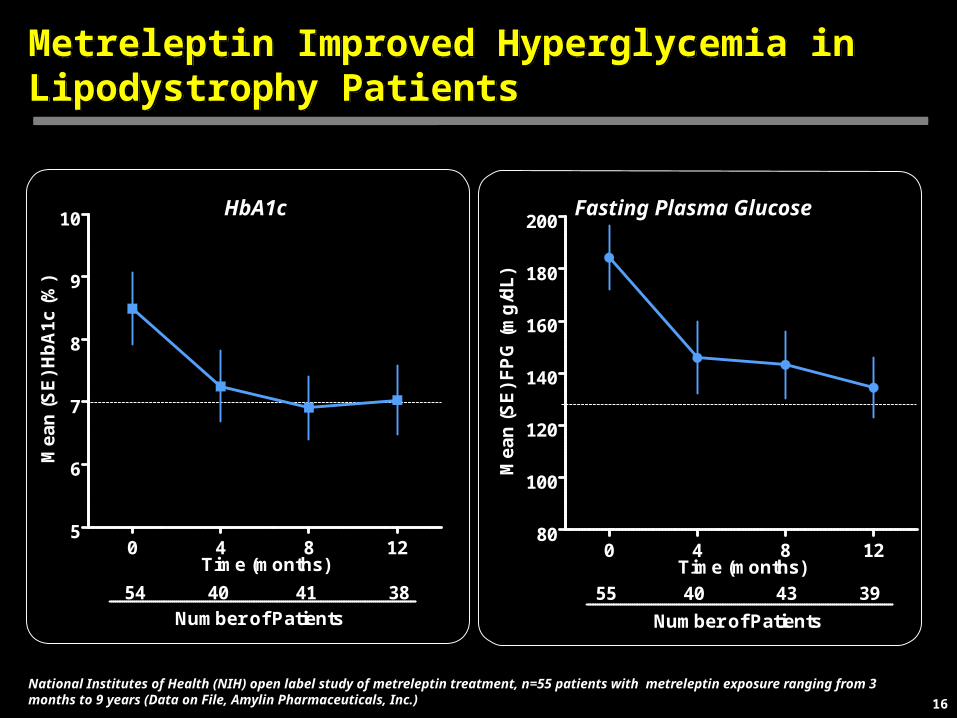
Metreleptin Improved Hyperglycemia in Lipodystrophy PatientsMetreleptin Improved Hyperglycemia in Lipodystrophy Patients
HbA1c Fasting Plasma Glucose
National Institutes of Health (NIH) open label study of metreleptin treatment, n=55 patients with metreleptin exposure ranging from 3 months to 9 years (Data on File, Amylin Pharmaceuticals, Inc.)

17
Metreleptin Improved Hypertriglyceridemia inLipodystrophy PatientsMetreleptin Improved Hypertriglyceridemia inLipodystrophy Patients
Mean Triglycerides Median Triglycerides
0 4 8 120
100
200
300
400
500
54 40 42 39
Number of Patients
Time (months)
Me
dia
n T
rig
lyc
eri
de
s (
mg
/dL
)
0 4 8 120
250
500
750
1000
1250
1500
1750
54 40 42 39
Number of Patients
Time (months)
Me
an
(S
E)
Tri
gly
ce
rid
es
(m
g/d
L)
National Institutes of Health (NIH) open label study of metreleptin treatment, n=55 patients with metreleptin exposure ranging from 3 months to 9 years (Data on File, Amylin Pharmaceuticals, Inc.)

18
Effect of Metreleptin on LipodystrophyEffect of Metreleptin on Lipodystrophy
• Unique therapy that directly addresses underlying pathophysiology
• Corrects relative leptin deficiency and associated hyperphagia, which exacerbates metabolic abnormalities as patients are driven to consume more
• Stimulates breakdown of fat in liver and muscle and reduces high triglyceride levels
• Improves insulin sensitivity and reduces hyperglycemia
Oral et al. Endocr Pract 2010; 16:324-333.
19
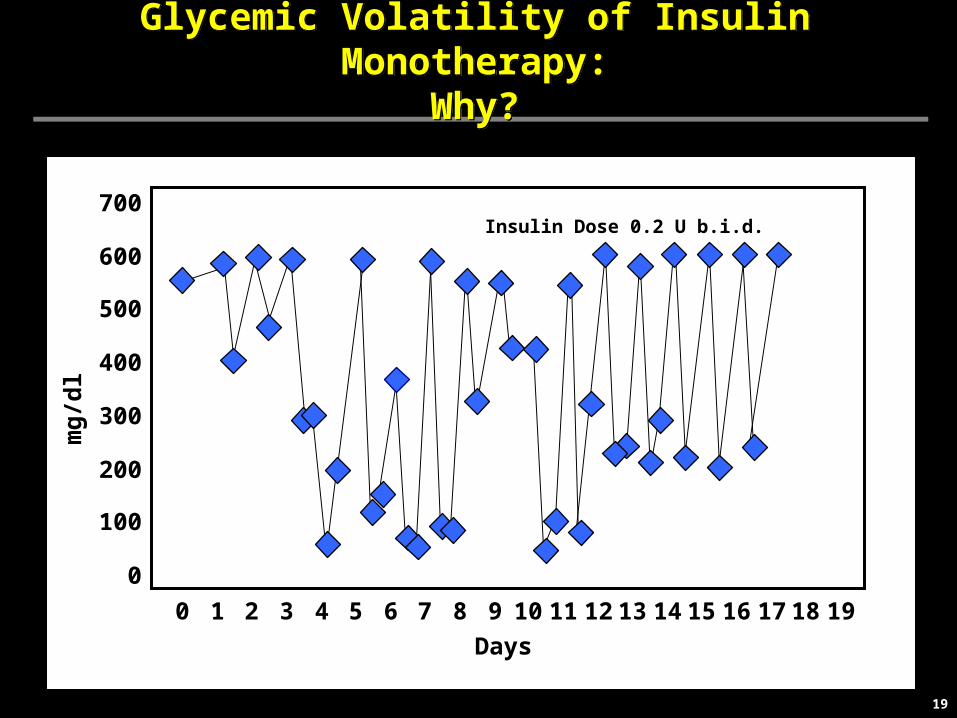
Glycemic Volatility of Insulin Monotherapy:Why?
Glycemic Volatility of Insulin Monotherapy:Why?
Insulin Dose 0.2 U b.i.d.
0
100
200
300
400
500
600
700
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
mg
/dl
Days
20
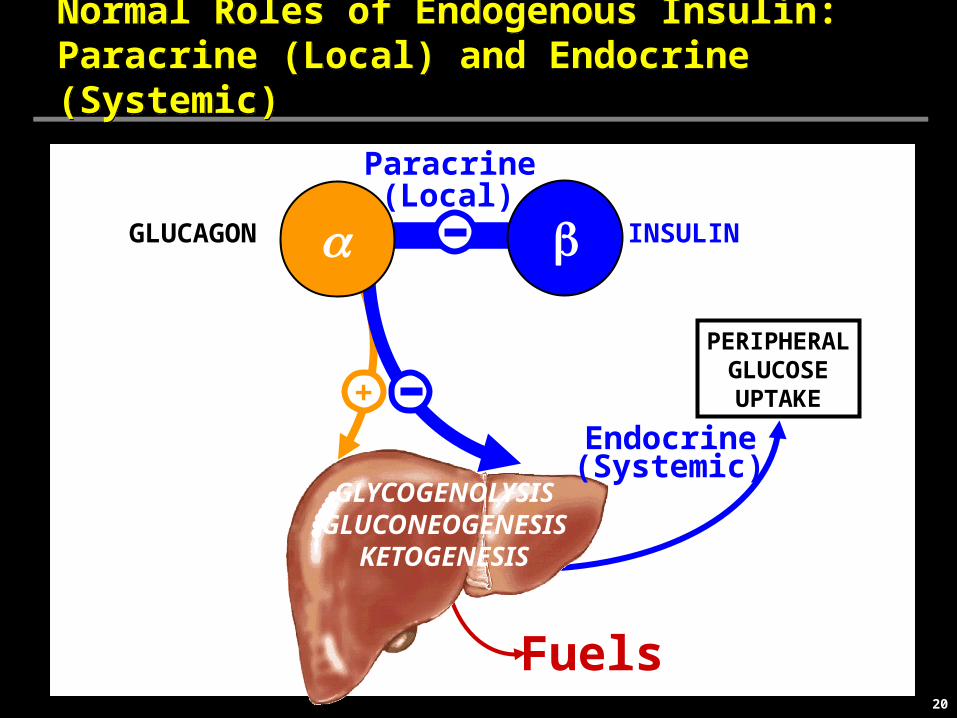
Normal Roles of Endogenous Insulin:Paracrine (Local) and Endocrine (Systemic) Normal Roles of Endogenous Insulin:Paracrine (Local) and Endocrine (Systemic)
GLUCAGON INSULIN
+
GLYCOGENOLYSISGLUCONEOGENESIS
KETOGENESIS
a b
PERIPHERALGLUCOSEUPTAKE
Fuels
Paracrine
Endocrine(Systemic)
(Local)

21
STRATEGY: Since injected insulin cannot approach paracrine levels in normal islets -cells, let leptin suppress glucagon.STRATEGY: Since injected insulin cannot approach paracrine levels in normal islets -cells, let leptin suppress glucagon.
GLUCAGON INSULIN
GLYCOGENOLYSISGLUCONEOGENESIS
KETOGENESIS
b
PERIPHERALGLUCOSEUPTAKE
Fuels
XInsulin
Suppressora X
+

22
Glycemic Volatility of Insulin Monotherapy is Eliminated by LeptinGlycemic Volatility of Insulin Monotherapy is Eliminated by Leptin
Insulin Dose 0.2 U b.i.d.
0
100
200
300
400
500
600
700
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
mg
/dl
Days
Leptin + Low Dose Insulin (0.02 U b.i.d.)
23
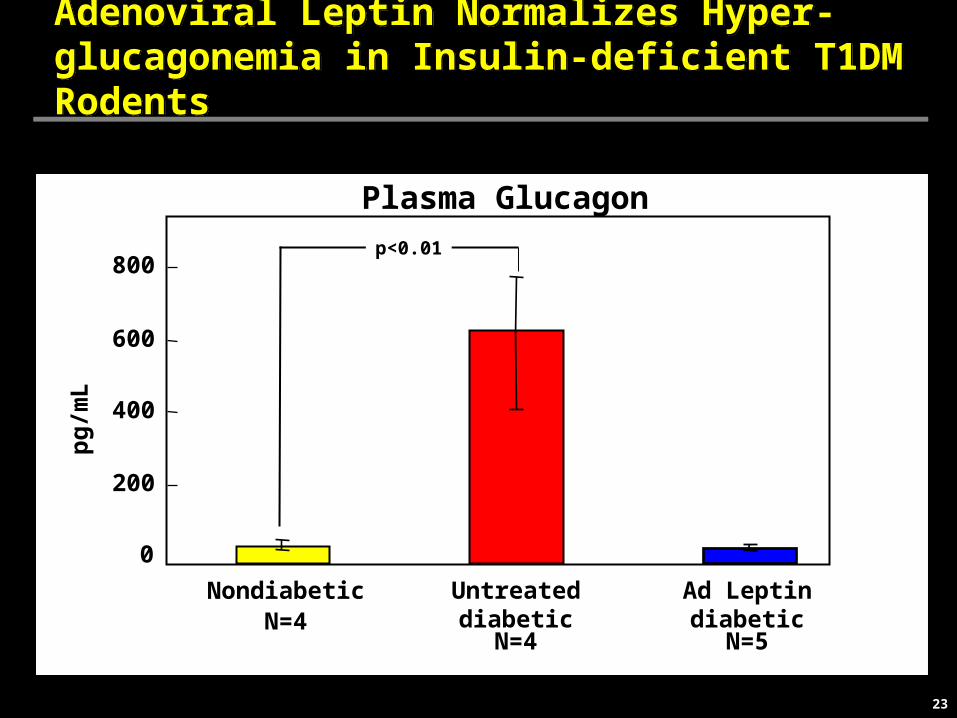
Adenoviral Leptin Normalizes Hyper-glucagonemia in Insulin-deficient T1DM RodentsAdenoviral Leptin Normalizes Hyper-glucagonemia in Insulin-deficient T1DM Rodents
L Plasma Glucagon
0
200
400
600
800
Untreateddiabetic
Ad Leptindiabetic
Nondiabetic
p<0.01
N=4N=4 N=5
pg
/mL

24
Product DevelopmentProduct Presentation/Patient ComplianceProduct DevelopmentProduct Presentation/Patient Compliance
• Co-Formulation
− Both API’s in single formulation for administration
• Sustained-Release Formulations
− Extend duration of release from injection site
− Extend duration of activity, reduce injection frequency
• Second Generation Compounds
− Reduce clearance and extend circulation
− Extended duration of activity, reduce injection frequency
− Improve pharmaceutical properties
• Other
− Devices
25
SummarySummary
• Weight loss with leptin can be restored by amylin/pram – a potential drug for obesity
• Leptin markedly improves the metabolic pathology of LD - a potential drug for LD
• Leptin normalizes diabetes in preclinical models - a potential drug for Type 1 diabetes
• SR formulations, Second Generation molecules, and devices in development for optimal product presentation and patient compliance

26
AcknowledgementsAcknowledgements
• In Vivo Pharmacology– Jonathan Roth– James Trevaskis– Victoria Turek– Christine Mack– Carrie Wittmer– Chunli Lei– Calvin Vu– Pete Griffin– David Parkes
• Functional Imaging– Barbara Roland– Rebecca Cole– Guibao Gu
•Research– Soumitra Ghosh
• Clinical Research– Alain Baron– Christian Weyer– Joy Koda– Amy Halseth– Larry Shen
• Biometrics– Todd Coffey– Colleen Burns
•R&D Strategic Relations– Elaine Chiquette
• Collaborators– Barry Levin
•Roger Unger and Group