rheumatology diagnostics 101
TRANSCRIPT
Rheumatology Diagnostics 101
Planning the Diagnostic Work-up for suspected
Rheumatic Disease
Evelyn O. Salido, MD, MScAssociate Professor
Division of Rheumatology
UP College of Medicine

Objectives
Given a patient with arthritis, the
participants will be able to:
• Create an appropriate diagnostic plan.
• Interpret the results of common tests.
Most common tests for patients
with arthritis (my experience)
• Serum uric acid
• ESR + CRP
• Joint x-ray
• Rheumatoid factor
• ASO
Diagnostic steps for a patient
with joint pains
TREATMENT
LABORATORY TESTS
DIAGNOSIS
PHYSICAL EXAM
HISTORY
Why we do diagnostic tests
NEW PATIENTS
• Confirm diagnosis
• Rheumatic disease
• Comorbidities
• Establish prognosis
FOLLOW-UP PATIENTS
In addition--
• Determine effects of
treatment
• Disease activity
• Adverse drug effects
TREATMENT
Case 1

Renato, 65/M, L knee pain
• Chronic (10 years)
• Progressive
• Use-related pain
TREATMENT
LABORATORY TESTS
DIAGNOSIS
PHYSICAL EXAM
HISTORY
65/M, L knee pain
• chronic & progressive use-related pain, NRS 5-6/10
• NSAID-use, acid reflux, HPN
History
• Bilateral genu varus, crepitus, no tenderness
Physical Exam
• Confirm rheumatologic diagnosis: knee apl, bilateral?
• Establish prognosis: ?
• Check comorbidities: Hgb, urinalysis, crea, SGPT, albumin
Diagnostic tests
OSTEOARTHRITIS
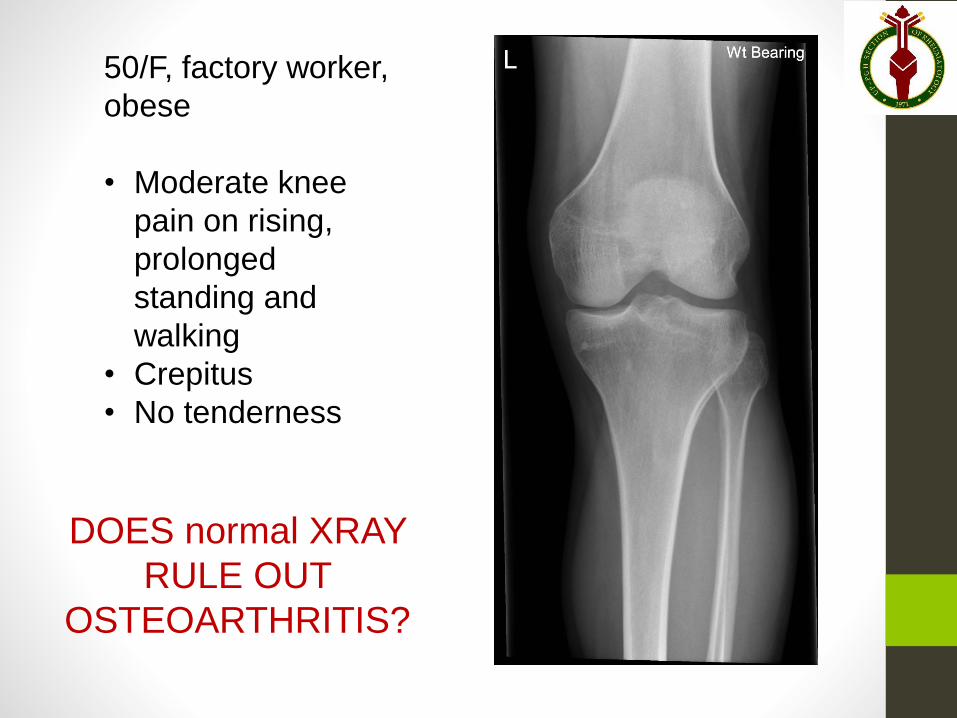
50/F, factory worker,
obese
• Moderate knee
pain on rising,
prolonged
standing and
walking
• Crepitus
• No tenderness
DOES normal XRAY
RULE OUT
OSTEOARTHRITIS?
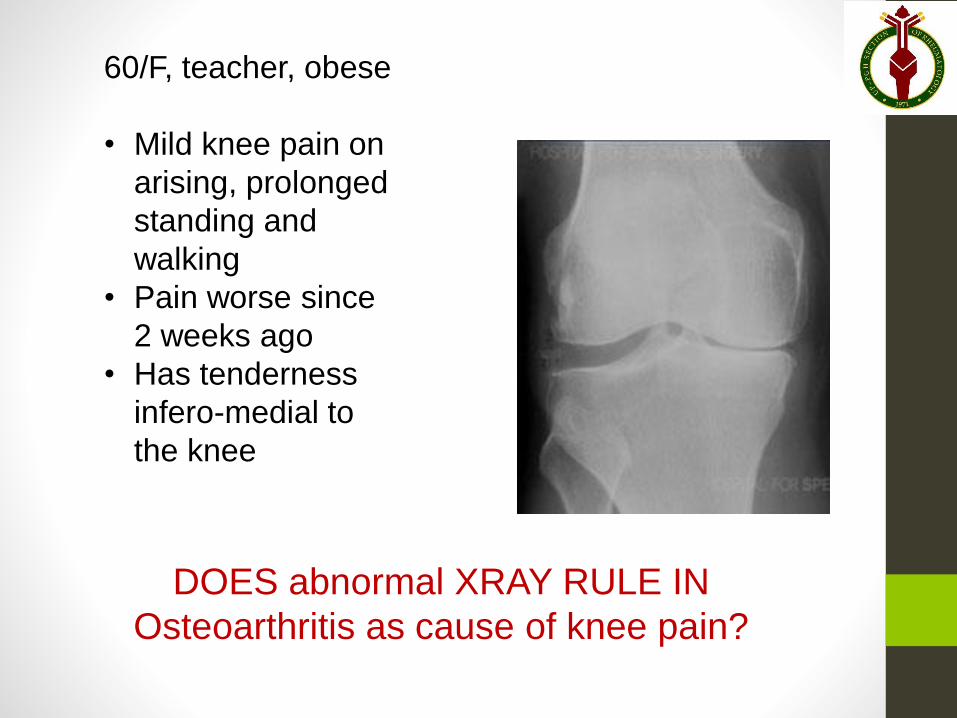
60/F, teacher, obese
• Mild knee pain on
arising, prolonged
standing and
walking
• Pain worse since
2 weeks ago
• Has tenderness
infero-medial to
the knee
DOES abnormal XRAY RULE IN
Osteoarthritis as cause of knee pain?
Joint radiograph
• Useful in assessing integrity of bony
structures
• May or may not be needed in diagnosis
of arthritis
• Physician must have clear expectation
of how it will aid management
• Clinical correlation is a must
When is plain radiograph most useful
in diagnosis of joint pain?
• Suspected OA of unusual sites
• History of trauma
• History of cancer
• Chronic inflammatory arthritis of
peripheral and axial joints
• Pain extends beyond the joint along
bony areas
Case 1: OAJudicious use of joint radiographs
• Indication
• Choice of joints to image
• Clinical correlation
Case 2
Olivia,42/F, hand pain
• chronic & progressive rest-related pain and stiffness (“morning stiffness”)
• Prn NSAID almost daily for a month
History
• Swelling, tenderness, increased warmth at joints- shoulders, elbows, wrists, fingers, knees, ankles, toes
Physical Exam
RHEUMATOID ARTHRITIS
42/F, pain at hands
• Chronic (4 months) and Progressive
• Rest-related pain (inflammatory)
• Symmetrical polyarthritis
Rheumatoid Arthritis (ACR-EULAR 6)
• Confirm rheumatologic diagnosis and determine prognosis
• ESR, CRP, RF, ACPA, joint xray, MRI (atypical)
• Check comorbidities
• Hgb, urinalysis, crea, SGPT, albumin, Hbs ag, CXR, PPD
Diagnostic tests
Erythrocyte Sedimentation Rate
• Rate of sedimentation of RBC in 1 hr
• Normal Rate 20 mm/hr
• Inflammation: increase in proteins
(fibrinogen) that make red blood cells
clump together
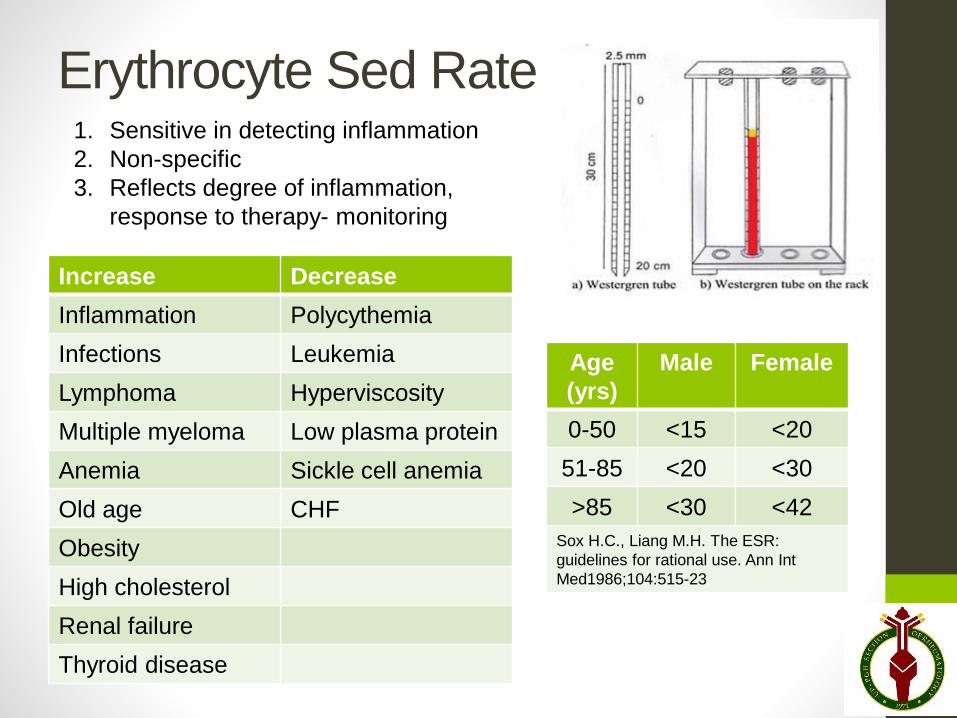
Erythrocyte Sed Rate
Increase Decrease
Inflammation Polycythemia
Infections Leukemia
Lymphoma Hyperviscosity
Multiple myeloma Low plasma protein
Anemia Sickle cell anemia
Old age CHF
Obesity
High cholesterol
Renal failure
Thyroid disease
Age
(yrs)
Male Female
0-50 <15 <20
51-85 <20 <30
>85 <30 <42
Sox H.C., Liang M.H. The ESR:
guidelines for rational use. Ann Int
Med1986;104:515-23
1. Sensitive in detecting inflammation
2. Non-specific
3. Reflects degree of inflammation,
response to therapy- monitoring
C-reactive protein
• Protein produced by liver
• Binds to surface of dead/dying cells, activates complement
and promotes their clearance
• Starts to rise by 4-6 hrs, peaks at 48 hrs, t½ 19 hrs
• Returns to normal more quickly than ESR
INTERPRETATION
Normal 0.8 -10 mg/L
Viral Infections 10-40 mg/L
Bacterial infection 40-200 mg/L
Severe bacterial infections, Burn >200 mg/L
High in malignancy, allergy, older age, late pregnancy
Autoantibodies: Rheumatoid factor
• Antibody for Fc portion of IgG
• Laboratory techniques
• ELISA- iu/ml
• Latex fixation- +/- (1:80)
• Diagnosis of RA
• Low positive- <3x ULN
• High positive- >3x ULN
• RA: + in 50% during 1st 6 mos
+ in 85% during 1st 2 yrs
• Prognosis of RA
• Higher titer- more erosive
disease, poorer prognosis
Positive RF
• IE
• TB
• Hepatitis C
• SLE
• Sjogren’s
syndrome
• Primary biliary
cirrhosis
• Post-vaccination
arthropathy
• Old age
Autoantibodies: ACPA
anti-citrullinated protein antibody
• Antibody against citrullinated peptides
• Measured in serum through ELISA
• Diagnosis of RA• Low positive- <3x ULN
• High positive- >3x ULN
• Detected as early as 10 years before onset
of symptoms of RA
• Not increased during infections
• May be positive in 15% of PsA, SLE, MCTD
• Prognosis: Marker of severe RA disease
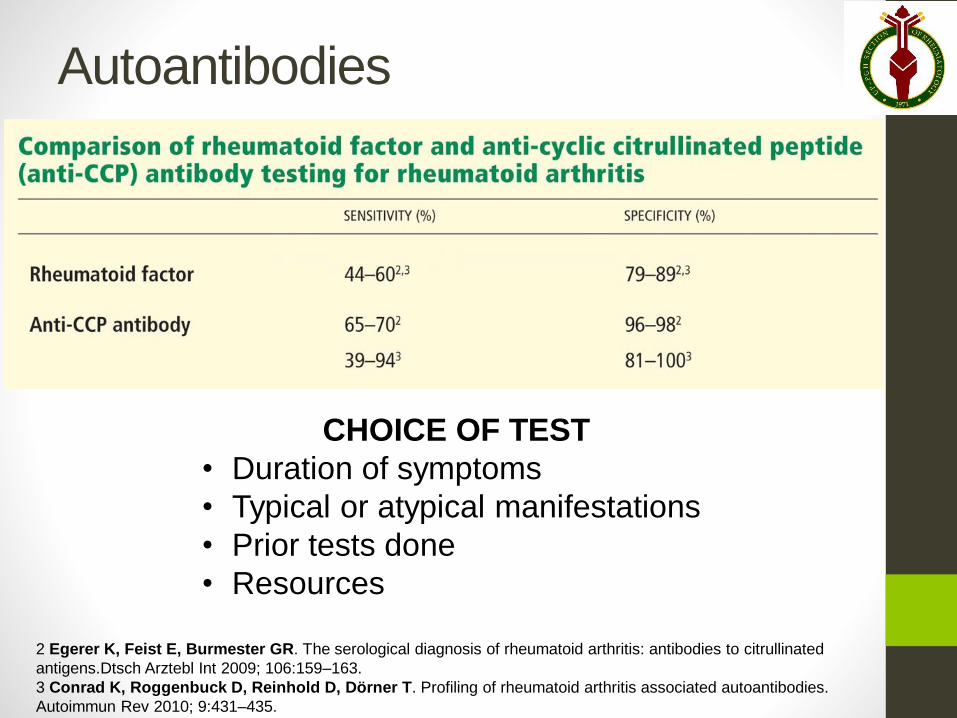
2 Egerer K, Feist E, Burmester GR. The serological diagnosis of rheumatoid arthritis: antibodies to citrullinated
antigens.Dtsch Arztebl Int 2009; 106:159–163.
3 Conrad K, Roggenbuck D, Reinhold D, Dörner T. Profiling of rheumatoid arthritis associated autoantibodies.
Autoimmun Rev 2010; 9:431–435.
Autoantibodies
CHOICE OF TEST
• Duration of symptoms
• Typical or atypical manifestations
• Prior tests done
• Resources
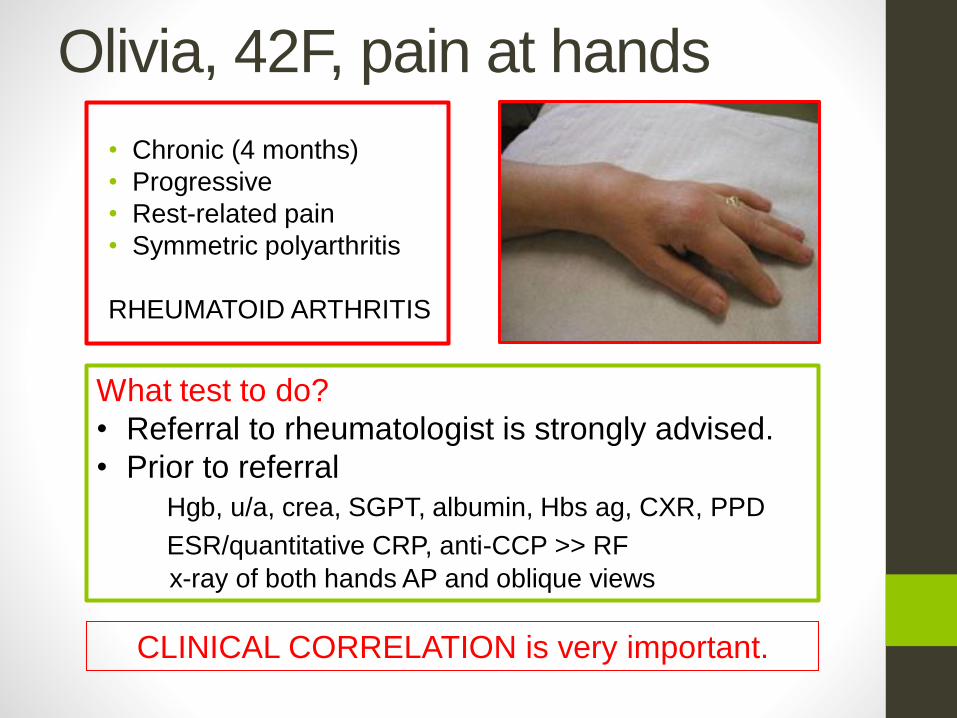
Olivia, 42F, pain at hands
• Chronic (4 months)
• Progressive
• Rest-related pain
• Symmetric polyarthritis
RHEUMATOID ARTHRITIS
What test to do?
• Referral to rheumatologist is strongly advised.
• Prior to referral
Hgb, u/a, crea, SGPT, albumin, Hbs ag, CXR, PPD
ESR/quantitative CRP, anti-CCP >> RF
x-ray of both hands AP and oblique views
CLINICAL CORRELATION is very important.
Case 2: RA• Acute phase reactants (ESR, CRP) are non-
specific markers of inflammation & more
useful for monitoring.
• Autoantibodies are more specific (RF, ACPA)
• Tests for general health, latent infections
Case 3
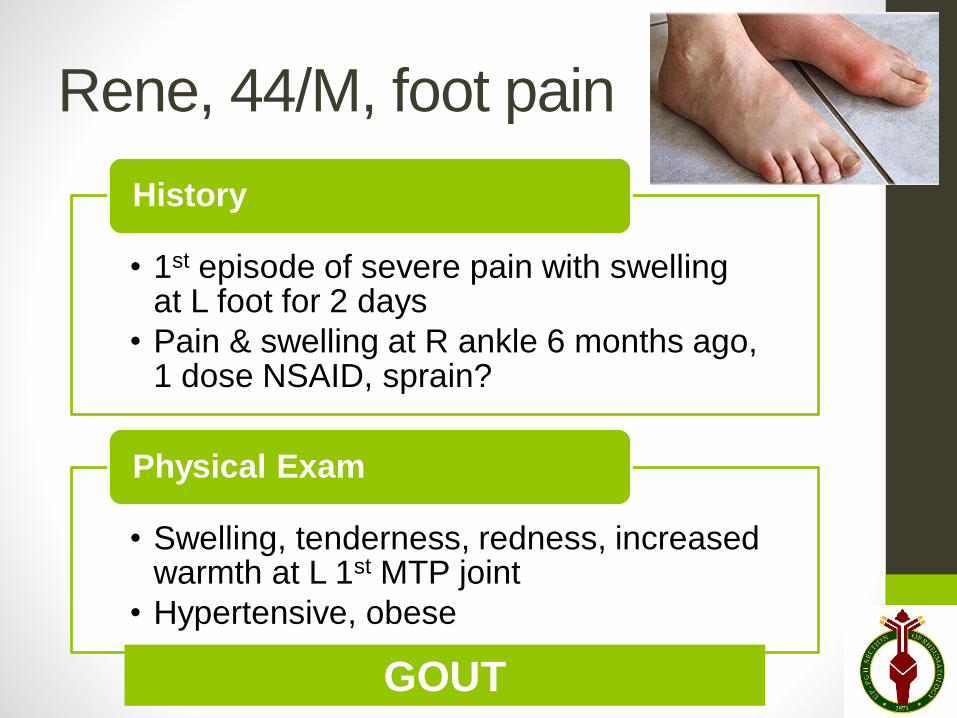
Rene, 44/M, foot pain
• 1st episode of severe pain with swelling at L foot for 2 days
• Pain & swelling at R ankle 6 months ago, 1 dose NSAID, sprain?
History
• Swelling, tenderness, redness, increased warmth at L 1st MTP joint
• Hypertensive, obese
Physical Exam
GOUT
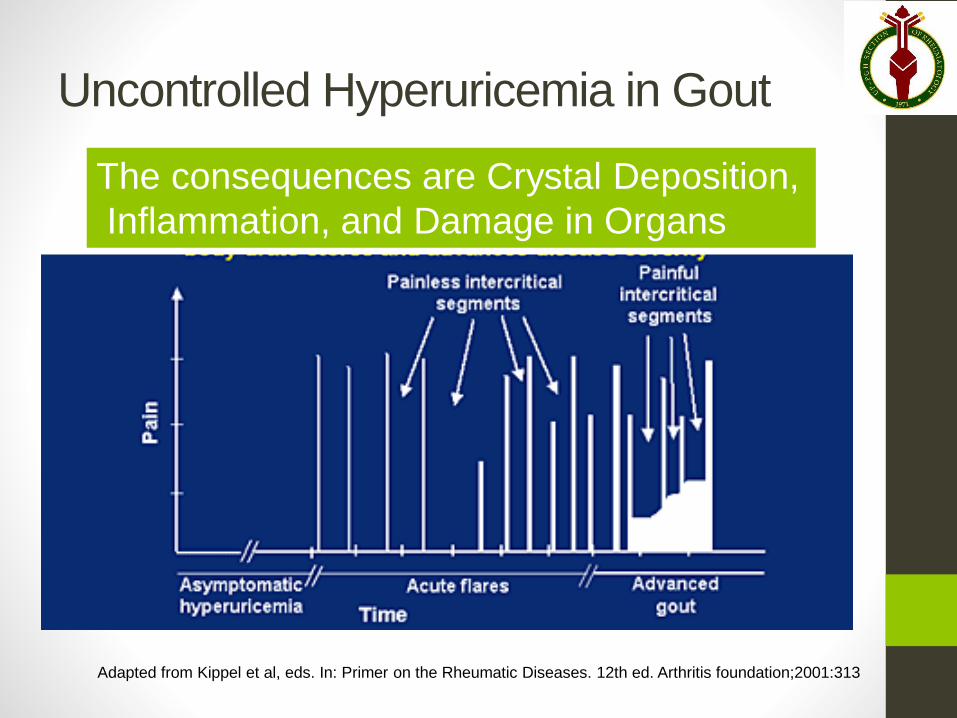
Uncontrolled Hyperuricemia in Gout
The consequences are Crystal Deposition,
Inflammation, and Damage in Organs
Adapted from Kippel et al, eds. In: Primer on the Rheumatic Diseases. 12th ed. Arthritis foundation;2001:313
Serum uric acid
• Source: By-product of cell breakdown (80%); Diet (20%)
• Excretion: urine (80%), feces (20%)
• Normal values
• Males 7 mg/dl, Females 6 mg/dl
• Determinants
• Genetics>>diet
• Intrinsic factors- sex, age, weight
• Diseases with increased cell turnover
• Medications
Serum uric acid in gout
• Elevated in blood and in tissues
• Poor correlation between serum levels
and symptoms
• May be low during acute gout arthritis due to
uricosuric effects of some inflammatory
cytokines or intake of urate-lowering drug
• May be high in the absence of gout:
asymptomatic hyperuricemia
• An obese menopausal woman with knee pain
from Osteoarthritis
• Symptomatology + SUA level = Gout DX
Rene, 44/M
• 2 episodes of acute inflammatory monoarthritis at the foot, the first resolved after 3 days, no apparent renal disease but with metabolic syndrome
Diagnosis: Gout
• Confirm rheumatologic diagnosis
• Uric acid- serum, synovial fluid
• Kidney structure & function tests
• Check comorbidities
• Hgb, urinalysis, crea, SGPT, FBS, lipids
Do tests? Consider stage of gout
Case 3: Gout• Serum uric acid does not always reflect total
body pool (blood & tissue deposits) of urate
• Check renal function & metabolic syndrome.
• Monitor SUA to achieve optimal level for
dissolution of deposited crystals.
Case 4
Cristina, 32/F, hand pain
• 4 months- pains, stiffness, and swelling (elbows, wrists, fingers, knees, ankles)
• 2 weeks- facial rashes, fever & weakness
History
• Macules at cheeks, forehead, neck
• Pale, tachypneic, tachycardic, with Gr I bipedal pitting edema
• Swollen, tender, warm joints
Physical Exam
Multisystemic disease- SLE?
Cristina, 32/F
• Inflammatory polyarthritis
• Malar rashes, pallor
• Fever, pedal edema
SLE or other AICTD
• Extent of organs involvement
• Serologic tests
• Comorbidities
Do tests?
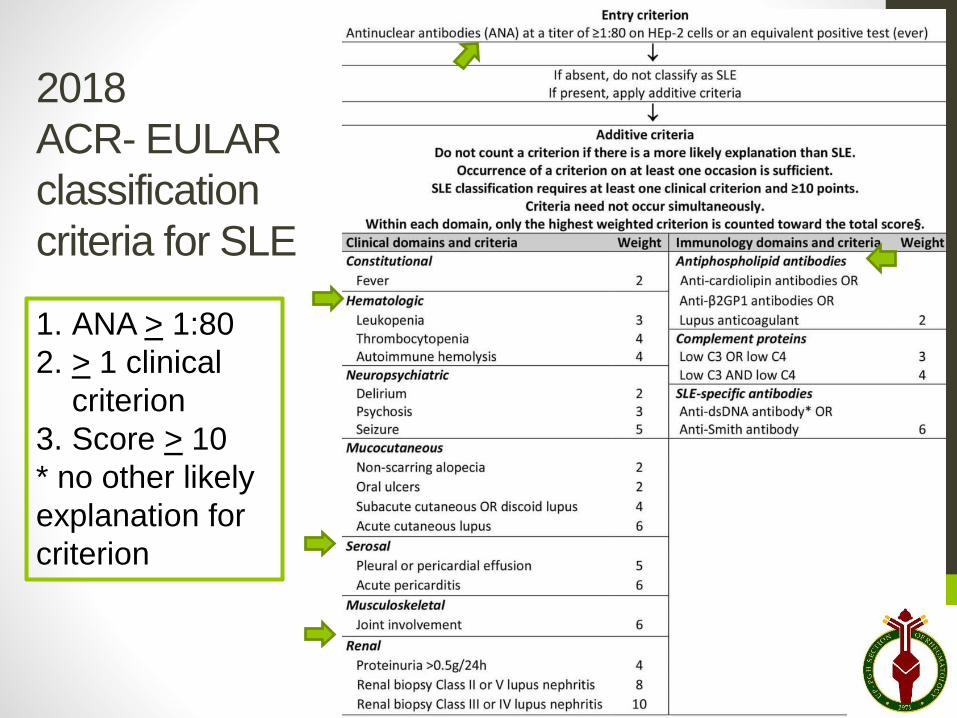
2018
ACR- EULAR
classification
criteria for SLE
1. ANA > 1:80
2. > 1 clinical
criterion
3. Score > 10
* no other likely
explanation for
criterion
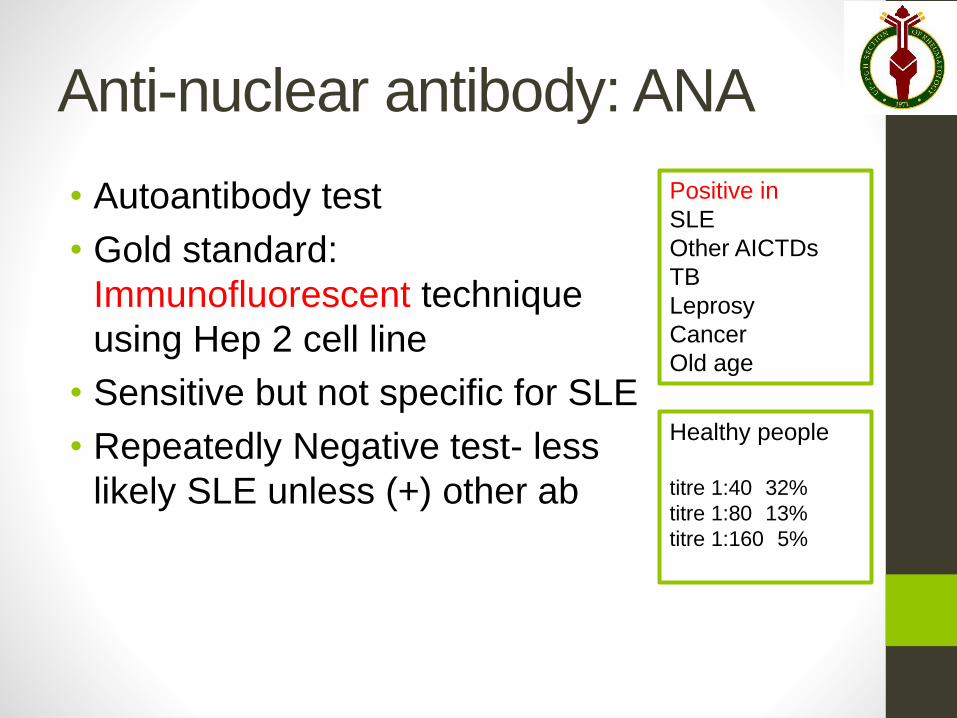
Anti-nuclear antibody: ANA
• Autoantibody test
• Gold standard:
Immunofluorescent technique
using Hep 2 cell line
• Sensitive but not specific for SLE
• Repeatedly Negative test- less
likely SLE unless (+) other ab
Positive in
SLE
Other AICTDs
TB
Leprosy
Cancer
Old age
Healthy people
titre 1:40 32%
titre 1:80 13%
titre 1:160 5%
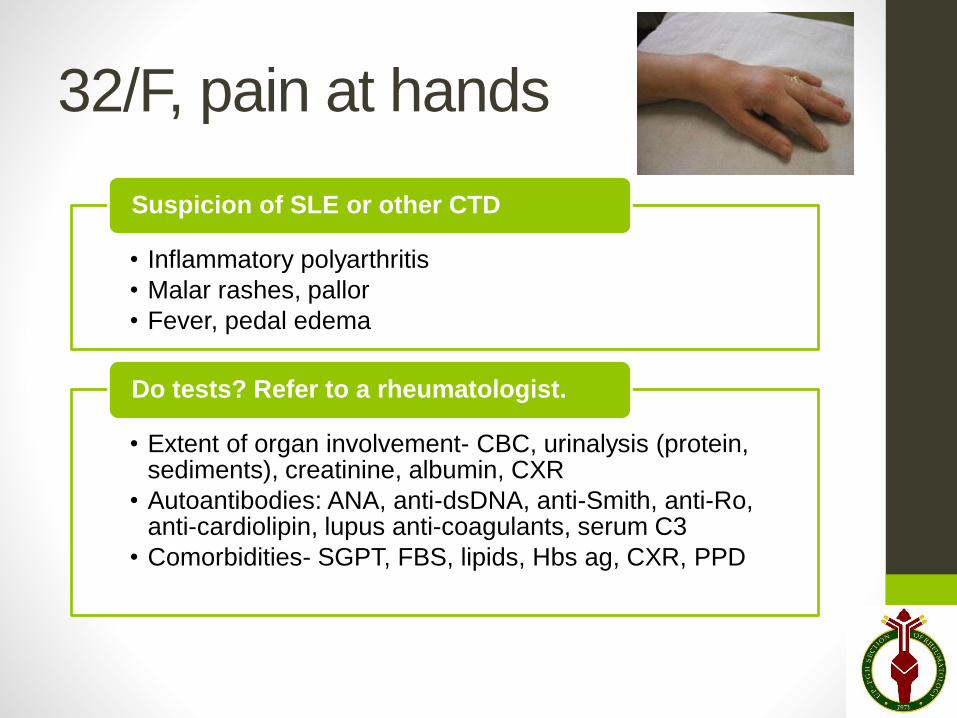
32/F, pain at hands
• Inflammatory polyarthritis
• Malar rashes, pallor
• Fever, pedal edema
Suspicion of SLE or other CTD
• Extent of organ involvement- CBC, urinalysis (protein, sediments), creatinine, albumin, CXR
• Autoantibodies: ANA, anti-dsDNA, anti-Smith, anti-Ro, anti-cardiolipin, lupus anti-coagulants, serum C3
• Comorbidities- SGPT, FBS, lipids, Hbs ag, CXR, PPD
Do tests? Refer to a rheumatologist.
Case 4: SLE• Establish + multisystemic disease
• CBC, urinalysis, creatinine, SGPT, CXR, Hbs
ag, ANA-IF
When planning diagnostic work-up for
suspected rheumatic disease
• Detailed history & thorough PE
• Working impression and differentials
• Have a clear rationale for ordering
each test
• Anticipate what the results will show
and the corresponding planned action.
• There is no de cajon “rheuma package”
Thank you