riding the rapids of payment reform: downstream effects of quality reporting on revenue capture
TRANSCRIPT

Riding the Rapids of Payment Reform?
Downstream Effects of Quality Reporting on Revenue Capture

Introductions
• Jodi Frei, PT MSMIIT, Northwestern Medical Center
• William Presley, Vice President , Acmeware

Audience Poll
• CIOs?
• Providers?
• IT Informatacists?
• Quality Nurses?
• Others?

Session Agenda
• Background on Quality Programs
• 2017 Quality Programs: VBP, MIPS, APM
• Reporting, Scoring
• Reimbursement, Financial Impact
• Challenges and Opportunities
• Infrastructure Considerations
• Future Insights

Riding the Rapids
“…often done on whitewater or different degrees of rough water, and generally represents a new and challenging environment for participants. Dealing with risk and the need for teamwork is often a part of the experience. “
Wikipedia
Sounds familiar?

Background: Quality Measurement Programs
Hospital Quality
• EHR Incentive Program
• Hospital Value-Based Purchasing
• Inpatient Psychiatric Facilities
• Inpatient Quality Reporting
• HAC payment reduction program
• Readmission reduction program
• Outpatient Quality Reporting
• Ambulatory Surgical Centers
• The Joint Commission (TJC)
Physician Quality
• EHR Incentive Program
• Physician Quality Reporting System (PQRS)
• Value-Based Payment Modifier (VM)
• eRX Quality Reporting
Payment Model
• Bundled Payments
• Accountable Care Organizations (ACO)
• Medicare Shared Savings Program
• Patient Centered Medical Homes (PCMH)
Programs Driving Performance Based Reimbursement
Hospital Quality• Value Based Purchasing (VBP)• Inpatient Quality Program (IQR) and MU• Hospital-Acquired Conditions (HAC)• Hospital Readmission Reduction (HRRP)
Physician Quality
• Merit-based Incentive Payment System (MIPS)
Payment Model
• Alternative Payment Model (APM)
• Comprehensive Primary Care (CPC+)
Revenue at Risk

Details Behind 2017 Quality Programs: MIPS
MACRA
• Bipartisan legislation signed into law on April 16, 2015
• Repealed Sustainable Growth Rate Formula
• Rewards providers for quality versus quantity
• Combines existing quality programs into one
• Participants: Part B Eligible Professionals
MIPS Overview
• Combines components of PQRS, Value Modifier, and MU into one program
• One composite performance score, 0-100 points, determined through 3 weighted categories
• Budget neutral program rewarding quality performance
• 2017 performance impacts 2019 payment

Current Physician Quality Programs

Merit-Based Incentive Program (MIPS)
Quality
Resource Use
Advancing Care
Clinical Practice
Composite Scoring
1 - 100

2017

MIPS Participants
2017: Medicare Part B Eligible
• Physicians
• PAs
• NPs
• Clinical nurse specialists
• Certified registered nurse anesthetists
2019: Opened to other clinicians
• PTs, OTs, SLPs
• Nurse Midwives
• Clinical Social Workers
• Dietitians
• Clinical Psychologists

MIPS Eligibility
EC EC EC EC EC
Hospitalist ED Provider Ortho Practice Family Practice
EC
Private Practice
Acute Ambulatory

MIPS Participation Options
Pick your pace
• Option 1: Test the System by submitting partial data
No negative, no positive 2019 adjustment
• Option 2: Participate for Part of the Year
Small positive 2019 adjustment available
• Option 3: Participate Full Calendar Year
Modest payment adjustment available
• Option 4: Participate in APM
5% incentive payment available

MIPS Scoring: QUALITY DOMAIN
Selection of 6 Measures;
Reduced from PQRS 9,
Minimum case requirement
One Crosscutting
Measure; One Outcome or High Priority
2-3 Claims Based
Population Measures
1-10 Points per measure, based on historical
benchmark
Additional Points for Reporting Additional Measures
Converting Performance To Points
CMS will create 10 deciles per measure based on national benchmarks of baseline period, 2 years prior
1-10 points assigned based on the decile within which the EP performs

MIPS Quality Performance Scorecard
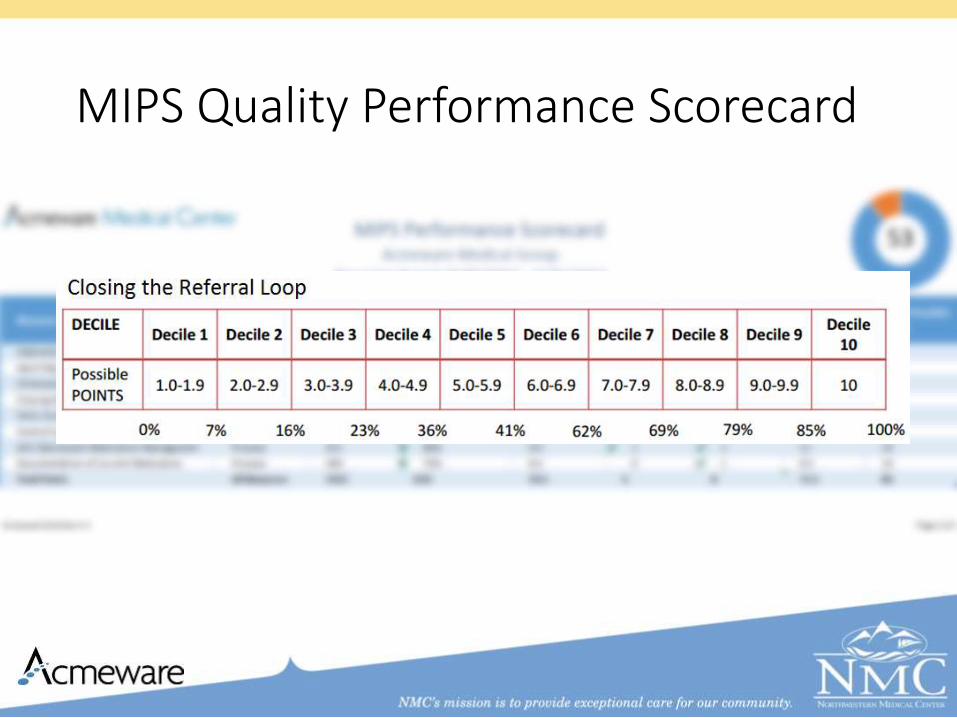
MIPS Quality Performance Scorecard

Advancing Care
25% total MIPS score
5 measures required
Extra points for reporting of additional measures

Meaningful Use vs Advancing Care
Meaningful Use
• Strict Reporting Requirement
• Labor Intensive
• Misaligned with Other Quality programs
Advancing Care
• Flexible Reporting
• Streamlined
• Aligned with Other Quality Programs

Summary of Advancing Care Measures
Required Objective Measures:
• Security Risk Analysis
• e-Prescribing
• Provide Patient Access
• Send Summary of Care
• Request/Accept Summary of Care
For bonus credit, you can:
• Report up to 4 additional measures
• Report Public Health and Clinical Data Registry Reporting measures
• Use certified EHR technology to complete certain improvement activities in the improvement activities performance category

Improvement Activities
15% of Total MIPS Score
Maximum Score of 40 points
Credit for involvement in Medical Home and APMs
90 available to accommodate specialists

Description of Improvement Activities
90 available aligned with:
• Care Coordination
• Beneficiary Engagement
• Patient Safety
• Expanded Practice Access
• Population Management
• Emergency Preparedness
• Achieving Health Equity
• Participation in APM

Improvement Activities: Scoring
Scoring based on weighting
• Up to 20 points for highly weighted activities
• Medical Home, transformation of the clinic, public health priorities
• Examples: Patient experience ratings, timely access for Medicaid patients
• Up to 10 points for all other activities, considered medium weight. Most options are of medium weight
Total high weight points + total medium points/total possible points (40) = % of Improvement Activities Score
Improvement Activities: Reporting
Individual clinicians, groups or designated 3rd party vendors must designate Yes/No to each chosen activity
Reporting Options:
• Attestation
• QCDR
• Qualified Registry Reporting
• EHR
• Claims (If feasible, no other reporting necessary)
• Groups of 25 or greater also have option of reporting via CMS Web Interface

Cost Catagory
0% of total MIPS score
Replaces Value Modifier
Claims based reporting
*No additional reporting requirements
Scoring is based on comparison to others
*Those that provide the most efficient, effective care will receive greater scores

Cost Category: Measures
40 Episode Specific Measures
*Specialty specific measures exist
Up to 10 points are available per measure
*Patient volumes per measure, typically 20, are required in order to qualify for measure
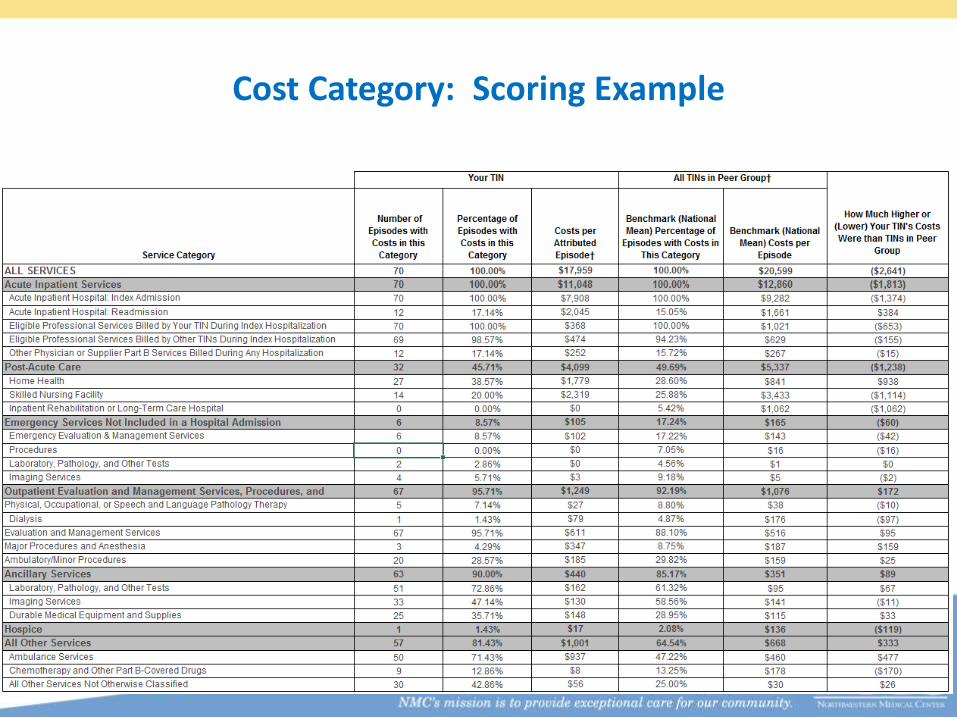
Cost Category: Scoring Example

Total Performance Score
SubmissionCategory Scoring
Composite Performance
Score Calculation
Comparison to
Performance Benchmark
Payment Adjustment Calculation
and Application
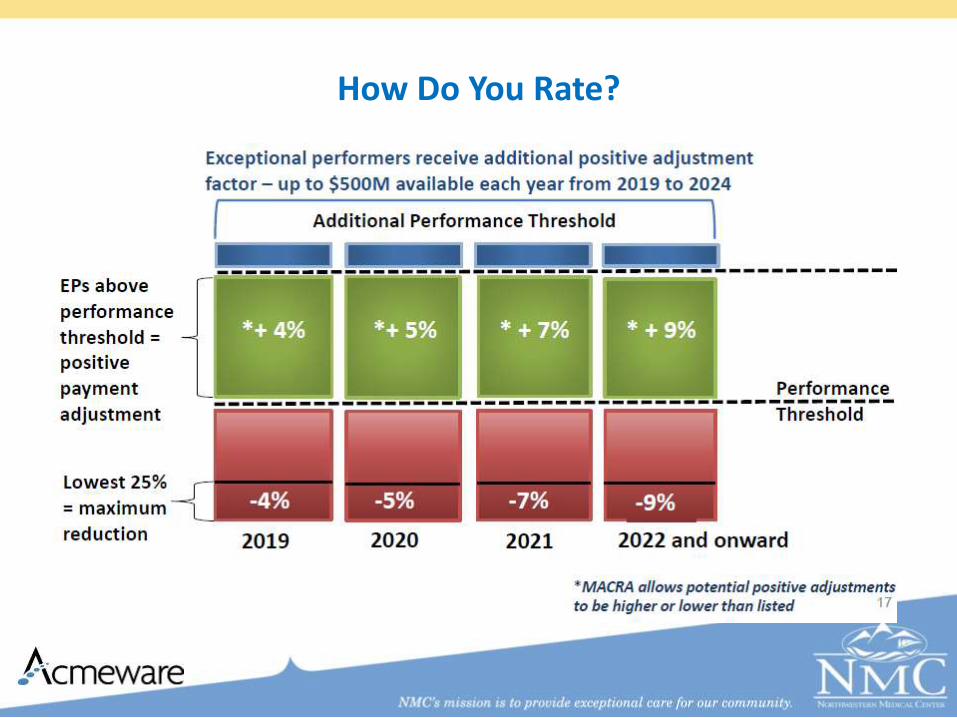
How Do You Rate?

Revenue at Risk

Physician Revenue at Risk

Details Behind 2017 Quality Programs: APM

Advanced APMs
• Clinicians who are involved with qualified ACOs, Medical Homes, etc
• ACO must base payment on quality measures
• Must meet patient volume and financial risk thresholds
• In order to determine APM eligibility, all clinicians report through MIPs in 2017
• APM clinicians avoid MIPS reporting requirements and payment adjustments
• Receive 5% APM incentive payment
• Does not change how APMs reward value

Advanced APMs Criteria

ACO Reporting
• Measures, means and frequency vary per ACO
• Vermont:
• Three ACOs coming under one umbrella - VCO
• Data flowing from EMRs through HIE to ACO Data Repository Workbench One
• PMPM Analyzer
• ACO Explorer
• Manual annual reporting process will phase out
• Importance of thoroughly and accurately diagnosis and comorbidities

Details Behind 2017 Quality Programs: VBP
VBP Program Background
• Funded by reductions from Diagnosis-Related Group (DRG) payments; Budget Neutral
• Built on the Hospital Inpatient Quality Reporting (IQR) measure reporting infrastructure
• Measures collected through the Hospital IQR Program infrastructure
• Reimbursements based on either national benchmarks or internal improvements

VBP Program Domains and Measures

VBP Program Domains and Measures

VBP Program Domains and Measures

VBP Program Domains and Measures

VBP Program Domains and Measures

Value Based Purchasing Scoring
• Scores for all measures generate total performance score
• Types of points awarded
• Achievement points
• 0-10 based on comparison to all hospitals’ baseline period rates
• Improvement points
• 0-9 based on comparison to same hospital’s baseline period rates
• Consistency points
• 0-20 based on hospital’s HCAHPS scores compared to all hospitals’ baseline period rates

Financial Impact
• Total amount of value-based incentive payments must equal the total amount withheld across all hospitals in the program.
• For FY18 payment (2016 performance): 2% withhold
• Value-based incentive payments = Sum of all hospital’s base-operating DRG*0.02 (withhold)

Revenue at Risk
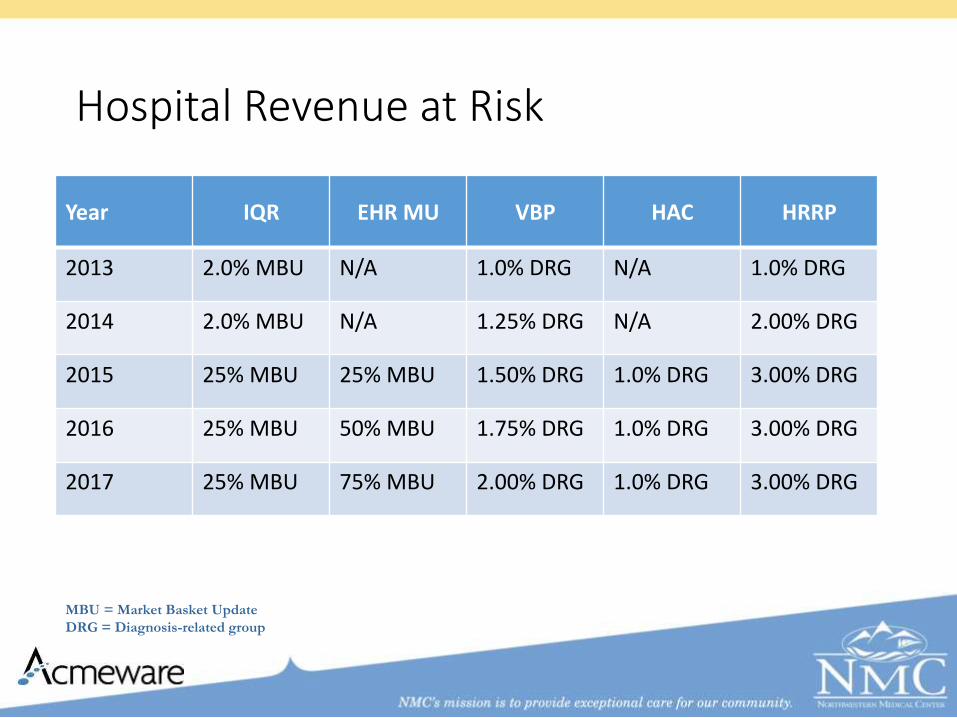
Hospital Revenue at Risk
Year IQR EHR MU VBP HAC HRRP
2013 2.0% MBU N/A 1.0% DRG N/A 1.0% DRG
2014 2.0% MBU N/A 1.25% DRG N/A 2.00% DRG
2015 25% MBU 25% MBU 1.50% DRG 1.0% DRG 3.00% DRG
2016 25% MBU 50% MBU 1.75% DRG 1.0% DRG 3.00% DRG
2017 25% MBU 75% MBU 2.00% DRG 1.0% DRG 3.00% DRG
MBU = Market Basket Update
DRG = Diagnosis-related group

Hospital Revenue at Risk
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
2013 2014 2015 2016 2017
IQR EHR VBP HAC HRRP
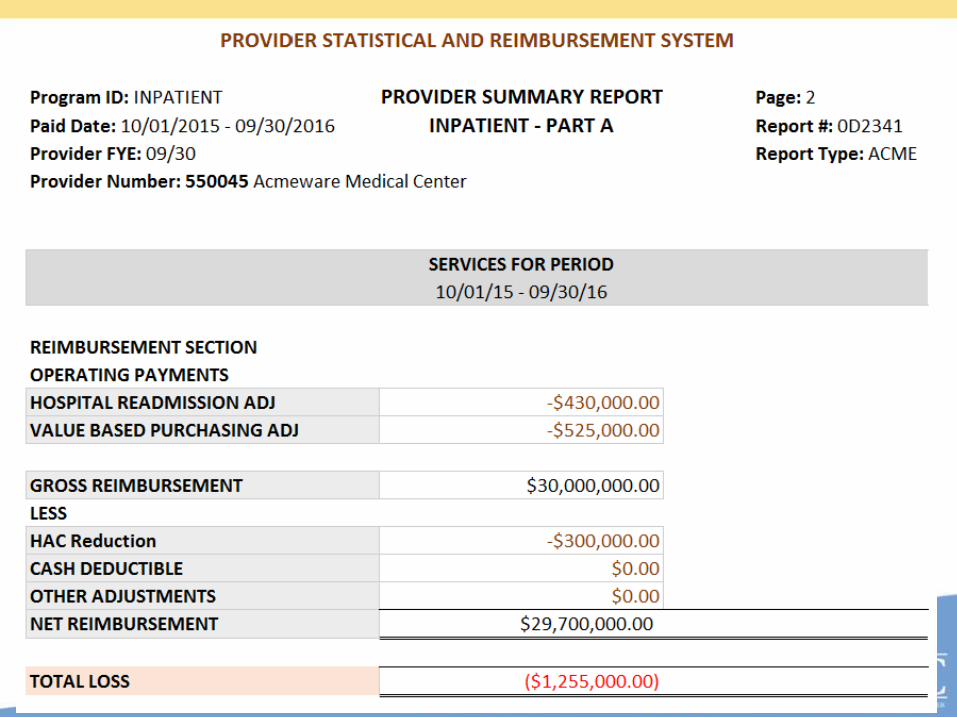
Financial Impact
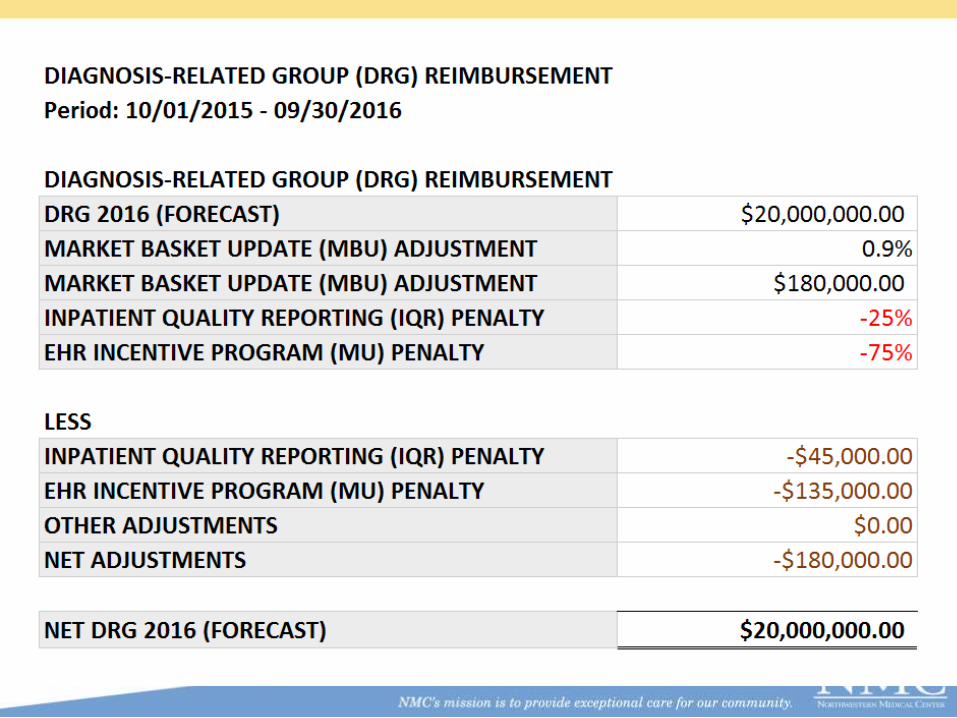
Financial Impact

Infrastructure Considerations
Infrastructure and Integration
• EHR 2015 Edition (Stage 3) Upgrades for 2018
• Acute and Ambulatory EHR Integration
• Data Warehouse Design
• Quality Reporting Metrics and Alerting

Measurement Validation

Enhanced Oversight and Accountability
ONC expands role of oversight
Attest to cooperation with certain authorized IT surveillance and oversight activities
Clinicians required to give access to their EHR
No restriction of data sharing and interoperability

Challenges
• Disparate Systems
• Difficult to assess performance across settings
• Creation of Clinical Alerts
• Coding occurs post discharge
• Understanding workflow required by eCQMs
• Transition from free text and customized reporting

Conclusion
• CMS is transitioning to what the they call "a new and more responsive regulatory framework." This new framework is based on the landmark bipartisan legislation called MACRA
• As organizations transition from volume to value based reimbursement, both in the inpatient and outpatient realms, increased attention to quality outcomes is necessary
• This involves focus on:
• Standardized Workflow
• Performance Reporting with Clinical Alerts
• Clinical Surveillance Across Settings
• Data Sharing - TOC
Questions
• Jodi Frei, PT MSMIIT Northwestern Medical Center
• William Presley, Vice President Acmeware

References• Physician Quality, Path to Value,
http://www.acmeware.com/products.aspx
• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/MACRA-MIPS-and-APMs.html
• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/NPRM-QPP-Fact-Sheet.pdf
• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/MIPS-Scoring-Methodology-slide-deck.pdf
• https://www.acog.org/-/media/Departments/Payment-Reform/ProposedCrosscuttingQualityMeasures.pdf?dmc=1&ts=20160802T0014121685
• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/CPIA-Performance-Category-slide-deck.pdf
• https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Hospital_VBPurchasing_Fact_Sheet_ICN907664.pdf
• http://www.himss.org/news/cms-previews-quality-payment-program-changes-fy-2017-performance-year-allows-clinicians-pick-their
• https://qpp.cms.gov
• https://www.cms.gov/medicare/medicare-fee-for-service-payment/physicianfeedbackprogram/valuebasedpaymentmodifier.html
• https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Advancing-Care-Information-Fact-Sheet.pdf