“risky states” optimizing icu safety through patient engagement, system science and information...
TRANSCRIPT

“Risky States” Optimizing ICU Safety Through Patient Engagement, System Science and Information Technology
Beth Israel Deaconess Medical Center; MIT; Aptima
Abstract
Objective
Methods
Results
Conclusions
Collaborators
Funded by the generosity of the Gordon and Betty Moore Foundation
• We used existing data and expert analysis to identify fundamental risky states (risk events/event drivers) in the ICU environment, system and people in the system that impact the likelihood of risky events or actual harm to occur.
• We identified corresponding harm outcomes during and following these “risky states” and will use them to inform the development of new holistic mitigation strategies
• Acquired and reviewed 2 years of retrospective data
• Analyzed retrospective data and develop model
• Designed application to display real time information to ICU staff about risky level
• It was impossible to create a working list of MD’s and RN’s assigned to care for each ICU patient at any point in time from existing electronic data sources
•It will be important to capture “drivers” that we have not considered in the first analysis of retrospective data
Environment Predictors - Drivers
AcuitySOFA ScoreTISS-28Unplanned ProceduresLength of Unit StayLength of Hospital StayPts in first 24 hrs
ExperienceFloat Nurse New Nurse <1 yearTraveling NurseRare Unit ProcedureInexperience with ProcedureCare TeamBoarding Patient
Other EventsReadmission"ED Critical"Admission with no Past HistoryAdmission from outside HospitalNight vs DayWeekend vs WeekdaySpecial EventNational Conference
UtilizationHours of CareBed UtilizationResource Nurse AssignmentsAdmissionsDischarges
“ Total Burden of Harm”
Preventable HarmsCLABSIVAC/IVAC/PossVAP/ProbVAPHigh Tidal VolumeVTE-PEICU-Acquired DeliriumDecrease in Function Mobility *FallsMedication EventsCAUTI
Potentially Preventable HarmsICU-Acquired Pressure UlcerPTT > 100 while on HeparinINR > 6 while on WarfarinHypoglycemina while on Heparin InfusionOversedationOversedation requiring NaloxoneIatrogenic PneumothoraxReintubation./Unplanned extubationReadmission to ICUPositive C. Diff and Blood Culture
…
Potential HarmsBleedingLab Specimen ErrorsIdentification ErrorsReintubation and Unplanned ExtubationAdministering NaloxoneAdministering Vitamin KBUN or Creatinine Doubled Baseline
1. Identified drivers through retrospective review of root cause analyses
2. Identified harms (voluntary reports, billing data, IHI ICU global triggers tool
3. Analyzed 2 years of retrospective data for all ICU patients 2012 – 2014
“ICU Intensity Index” Dashboard
Team
• Dustin Boone• Tricia Bourie• Christina Cain • Michael Cocchi• Jane Foley • Agnes Hu (MIT)• Retsef Levi (MIT) • Lisa Lucia (Aptima, Inc.)• Yiyin Ma (MIT)• Ariel Mueller • Sharon O’Donoghue• Kristin O’Reilly• Jeremy Richards• Adam Traina (MIT) • Donna Williams• Kathryn Zieja
• Nurse Consultants– Juliann Corey– Lynn Mackinson– Veronica Kelly
PI’s• Danny Talmor• Ken Sands

Environment Predictors - Drivers
AcuitySOFA ScoreTISS-28Unplanned ProceduresLength of Unit StayLength of Hospital StayPts in first 24 hrs
ExperienceFloat Nurse New Nurse <1 yearTraveling NurseRare Unit ProcedureInexperience with ProcedureCare TeamBoarding Patient
Other EventsReadmission"ED Critical"Admission with no Past HistoryAdmission from outside HospitalNight vs DayWeekend vs WeekdaySpecial EventNational Conference
UtilizationHours of CareBed UtilizationResource Nurse AssignmentsAdmissionsDischarges

“ Total Burden of Harm”
Preventable HarmsCLABSIVAC/IVAC/PossVAP/ProbVAPHigh Tidal VolumeVTE-PEICU-Acquired DeliriumDecrease in Function Mobility *FallsMedication EventsCAUTI
Potentially Preventable HarmsICU-Acquired Pressure UlcerPTT > 100 while on HeparinINR > 6 while on WarfarinHypoglycemina while on Heparin InfusionOversedationOversedation requiring NaloxoneIatrogenic PneumothoraxReintubation./Unplanned extubationReadmission to ICUPositive C. Diff and Blood Culture
…
Potential HarmsBleedingLab Specimen ErrorsIdentification ErrorsReintubation and Unplanned ExtubationAdministering NaloxoneAdministering Vitamin KBUN or Creatinine Doubled Baseline

Moderate Risk State

High Risk State
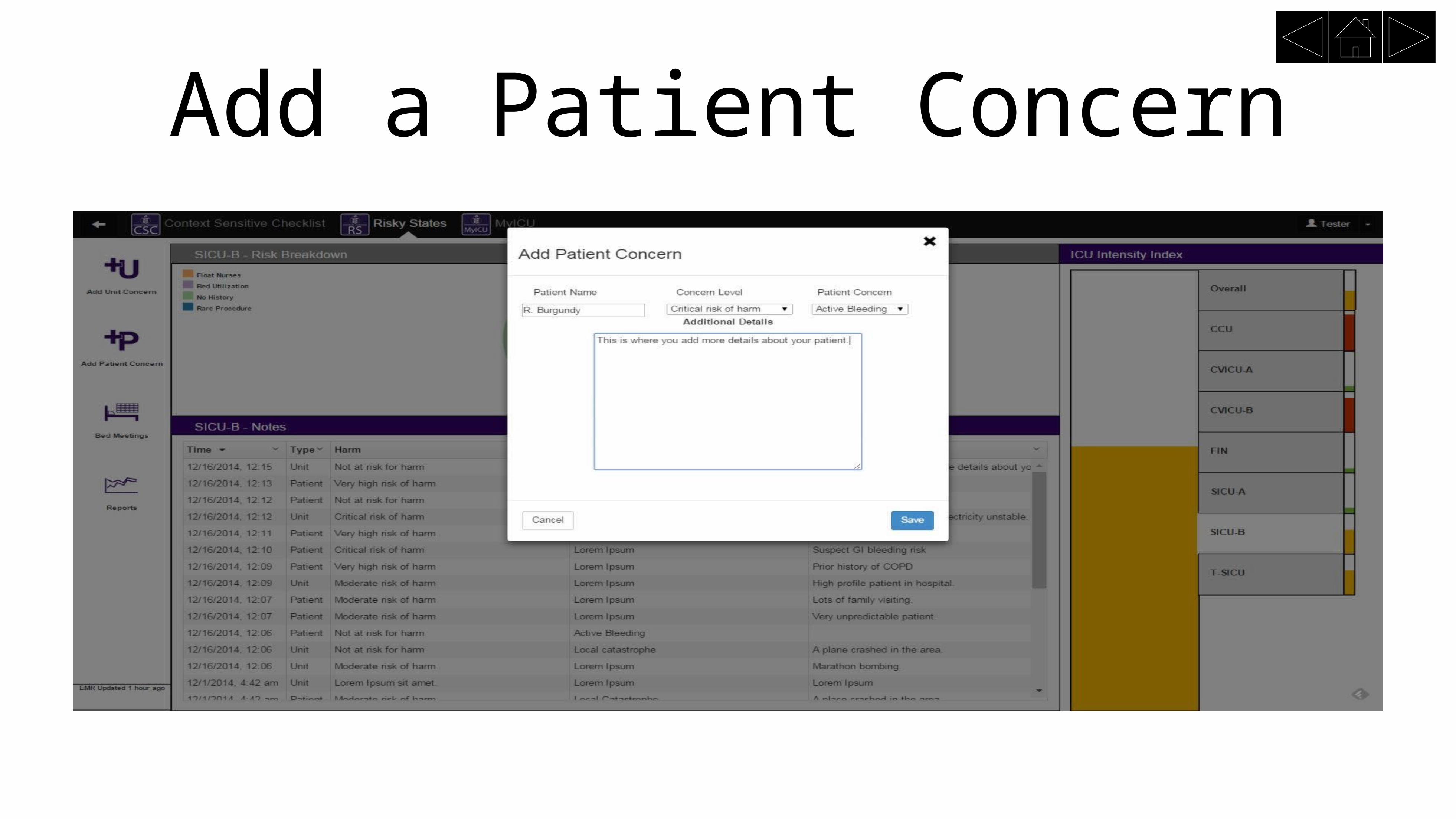
Add a Patient Concern

Add a Unit Concern