robert f. storey senior lecturer and honorary consultant in cardiology, university of sheffield,...
TRANSCRIPT

Robert F. Storey
Senior Lecturer and Honorary Consultant in Cardiology, University of Sheffield,
Sheffield, UK
Stent thrombosisFuture directions

Disclosures
RF Storey has received research grant support and/or consultancy fees from AstraZeneca, Lilly, The Medicines Company, Merck Sharp & Dohme, Sanofi Aventis, and Bristol Myers Squibb

Platelet Activation Mechanisms
Storey RF. Current Pharmaceutical Design 2006
Thrombin
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR1
PAR4
Densegranule
Thrombingeneration
Shapechange
IIb3
IIb3
FibrinogenIIb3
Aggregation
AmplificationAmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TP
Coagulation
GPVI
Collagen
ATPATP
P2X1
ASPIRIN
xCLOPIDOGRELPRASUGREL
ACTIVE METABOLITE
x AZD6140 CANGRELOR
GPIIB/IIIA ANTAGONISTS
x

On chronic ASA 7 days post ASA Post ASA 300 mg0
20
40
60
80
100
% a
gg
reg
ati
on
Arachidonic acid-induced platelet aggregation in 190 IHD patients
Compliance rather than aspirin resistance
Schwartz et al. Am J Cardiol 2005

Storey RF et al. Platelets 2002; 13: 407-413
Variable response to clopidogrel with incomplete P2Y12 receptor blockadeFinal response to 20 µM ADP before and after clopidogrel 300 mg followed by 75 mg daily for 4-7 days in patients undergoing PCI +/- 150 nM cangrelor added in vitro
0
20
40
60
80
100
Baseline PostClopidogrel
PostClopidogrel+ cangrelor
Mea
n %
Pla
tele
t A
ggre
gatio
n
*
*
* P<0.05
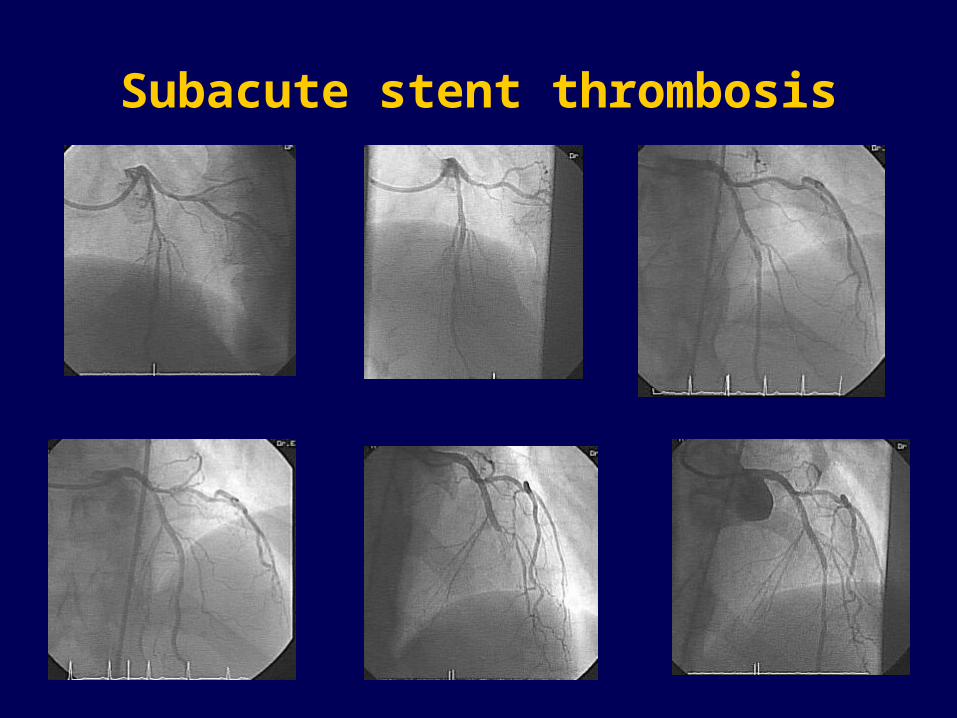
Subacute stent thrombosis

Platelet aggregation before and 4 hours after clopidogrel 600 mg in patients undergoing PCIWhole blood single platelet counting in response to ADP 10 uM
Baseline Post clopidogrel0
20
40
60
80
100
% a
gg
reg
ati
on
Patient with subacute stentthrombosis
Smith SMG et al. Platelets 2006; 17: 250-258

Prasugrel
• Novel thienopyridine (CS-747) in phase III development (PCI in ACS patients)
• Different pathways of metabolism to clopidogrel and higher potency probably related to more efficient production of active metabolite

Prasugrel 5-20 mg daily vs clopidogrel 75 mg daily in healthy volunteers – inhibition of ADP induced platelet
aggregation at 10 days
0
20
40
60
80
100
Prasugrel 5 mg
Prasugrel10 mg
Prasugrel20 mg
Clopidogrel75 mg
JA Jakubowski et al. ACC Annual Scientific Session 2005.

Clinical Target Vessel Thrombosis
0.4%0.6%
1.0%0.5%
2.4%
0.0%
2.0%
4.0%
6.0%
Clop Pras 40/7.5 60/10 60/15
P= NS
Target Vessel Revasc or Documented Total Occlusion
RR=0.25 [0.1, 0.9]
P = 0.03
Prasugrel LD/MDTreatment Group

Significant Non-CABG Bleeding 30 d (%)
(TIMI Major + Minor) – Primary Endpoint
1.6%1.7% 1.5%2.0%
1.2%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Clop Pras 40/7.5 60/10 60/15
P= NSP = 0.77
Prasugrel LD/MDTreatment Group

TRITON – TIMI 38TRITON – TIMI 38
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCIACS (STEMI or UA/NSTEMI) & Planned PCI
ASA
PRASUGRELPRASUGREL CLOPIDOGRELCLOPIDOGREL
11oo endpoint: endpoint: CV death, MI, StrokeCV death, MI, Stroke22oo endpoints: endpoints: CV death, MI, Stroke, Re-ischemiaCV death, MI, Stroke, Re-ischemia
CV death, MI, UTVRCV death, MI, UTVR
Median duration of therapy - 12 months
N= 13,000

AZD6140
• Class: CPTP* (non-thienopyridine)
• Reversible platelet P2Y12 receptor antagonist
• Orally active
• Rapid onset of action (2 h) with or without a loading dose
• Acts directly (no metabolic activation required)
• Plasma t½ ~12 h
*cyclo-pentyl-triazolo-pyrimidine

Comparison of clopidogrel 300 mg loading dose vs AZD6140 90-270 mg
loading doses in ACS patients
0 2 4 6 8 10 120
25
50
75
100
Clopidogrel
AZD6140 90mg
AZD6140 180mg
AZD6140 270mg
Time post dose (h)
Mea
n %
in
hib
tio
n
Inhibition of platelet aggregation induced by ADP 20 M
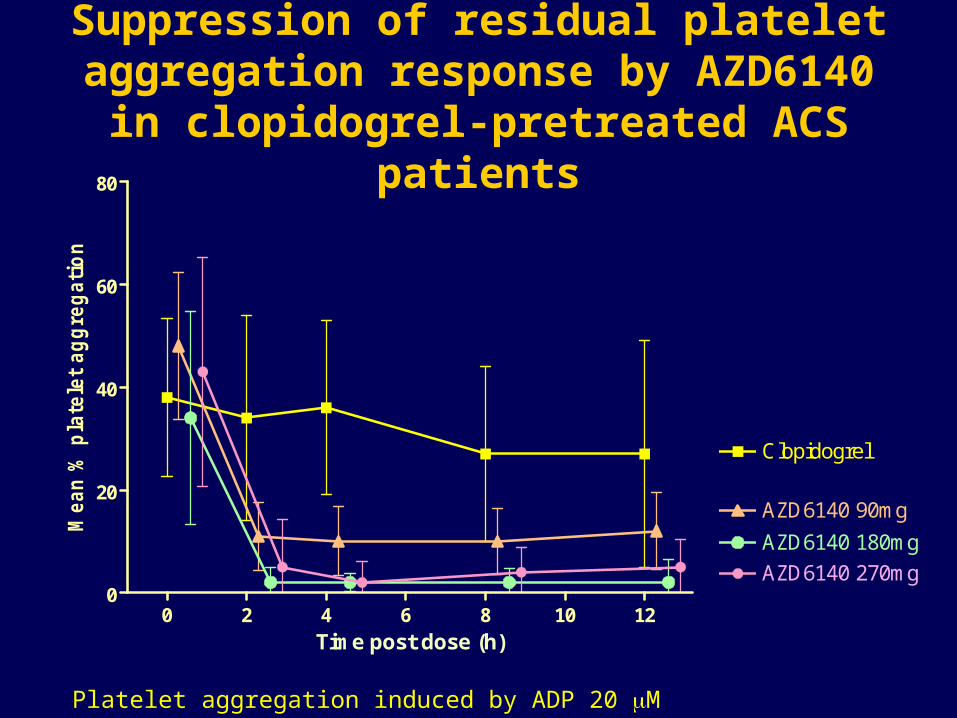
Suppression of residual platelet aggregation response by AZD6140 in clopidogrel-pretreated ACS patients
0 2 4 6 8 10 120
20
40
60
80
Clopidogrel
AZD6140 90mg
AZD6140 180mg
AZD6140 270mg
Time post dose (h)
Mea
n %
pla
tele
t ag
gre
gat
ion
Platelet aggregation induced by ADP 20 M
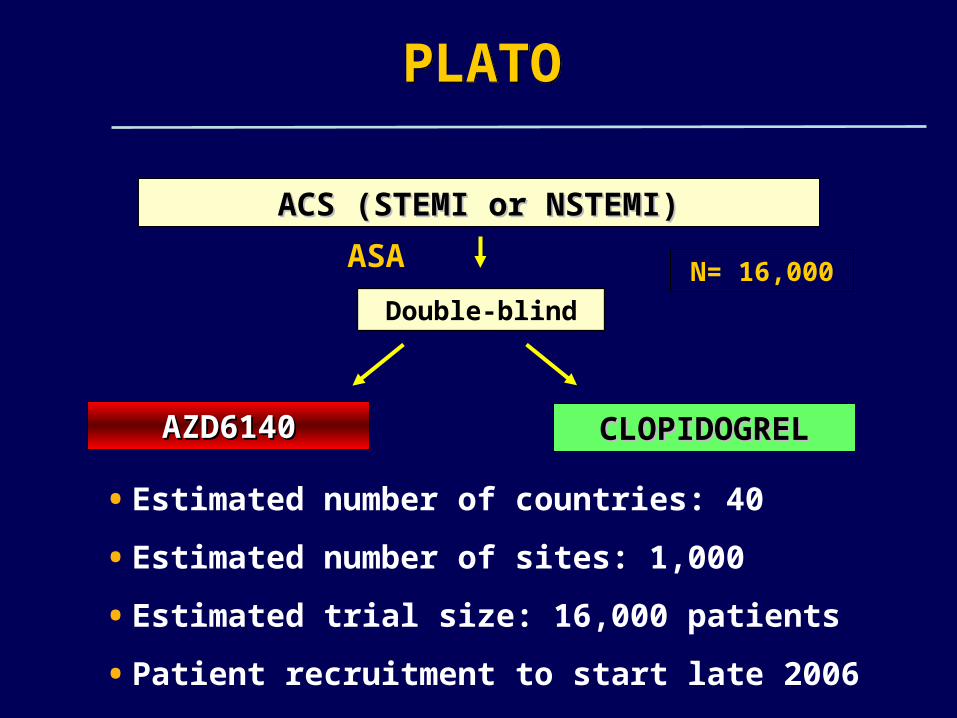
PLATOPLATO
Double-blind
ACS (STEMI or NSTEMI)ACS (STEMI or NSTEMI)
ASA
AZD6140AZD6140 CLOPIDOGRELCLOPIDOGREL
N= 16,000
• Estimated number of countries: 40
• Estimated number of sites: 1,000
• Estimated trial size: 16,000 patients
• Patient recruitment to start late 2006

Cangrelor
• Stabilised ATP analogue
• Reversible platelet P2Y12 receptor antagonist
• Intravenous use only
• Onset of action within minutes
• Acts directly (no metabolic activation required)
• Plasma t½ < 9 minutes
• Phase 3 studies - CHAMPION

Higher incidence of late stent thrombosis seen with DES in BASKET-LATE study and in follow up studies of Taxus and Cypher stents
Heparin coated stents – no convincing evidence of clinical benefit
Stem cells – under investigation to assess whether they can be used to promote endothelialisation
Need for new agents, either systemic or stent coated, that reduce neointima formation without impairing endothelialisation
Stent coatings

CONCLUSIONS (1)
True aspirin resistance is rare
Compliance is important – patients should be advised of the reasons for antiplatelet therapy, intended duration of treatment and risks of poor compliance

CONCLUSIONS (2)
Inadequate P2Y12 receptor blockade by clopidogrel in some patients is probably a major risk factor for stent thrombosis and 3 new P2Y12 antagonists are in phase 3 development to address this:
Prasugrel (oral thienopyridine)
AZD6140 (oral reversible antagonist)
Cangrelor (short-acting iv antagonist)

CONCLUSIONS (3)
DES appear to increase the risk of late stent thrombosis and further work is required to establish whether novel stent coatings or systemic agents can reduce subacute and late thrombosis risk