role of benzodiazepines in...
TRANSCRIPT

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 1
Role of Benzodiazepines in Treatment
Barbara J Limandri, PhD, PMHNP, BC
Portland Dialectical Behavior Therapy Institute
Portland, Oregon
Disclosures: I have no financial conflicts of interest to disclose

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 2
Learning Outcomes
• Explain the issues of prescribing patterns of benzodiazepines in the United States.
• Review the mechanisms of action of benzodiazepines in relation to treatment outcomes
• Discuss protocols for benzodiazepine withdrawal and discontinuation.
Prescribing Patterns of Benzodiazepines
• Between 1996 and 2013 number of adults filling a BZD prescription increased 67% from 8.1 million to 13.5 million
• In 2013 BZDs prescribed for:• Anxiety disorders 56.1%
• Mood disorders 12.1%
• Unclassified (including insomnia) 12.0%
(Bachhuber, Hennessy, Cunningham, Starrels, 2016)
• In 2012 prescribers wrote 82.5 opioid prescriptions and 37.6 BZD prescriptions per 100 persons in US(Paulozzi, Mack, Hockenberry, 2014)

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 3
Benzodiazepine Use in the US
• In 2008 5.2% of US adults aged 18‐80 years used BZDs• Those 18‐35 yrs 2.6%
• Those 36‐50 yrs 5.4%
• Those 51‐64 yrs 7.4%
• Those 65‐80 yrs 8.7%
• Nearly twice as prevalent in women as men
• About 25% of those receiving BZDs involved long‐acting
(Olfson, King, Schoenbaum, 2014)
Benzodiazepines and Opioids
• During 2004‐09, 27% of veterans who received opioid analgesics also received BZDs
• Women 33%; men 26%
• More likely to be middle‐aged, white, and live in wealthier areas
• More likely to have had recent hospitalization for substance use disorder
• Death from drug overdose 49% with concurrent opioid and BZD prescriptions
• Deaths were higher when BZDs prescribed regularly vs as needed
(Park, Saitz, Ganoczy, Ilgen, Bohnert, 2015)
Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 4
Long‐Term Use of Benzodiazepines
• Adults 65‐80 who used BZDs, 31.4% used for more than 120 days
• Adults 18‐35 14.7% used for more than 120 days
•Women 65‐80 yo 10% were prescribed BZDs and 30% were long term use
•Most prescriptions written by non‐psychiatrists(NIMH Press Release, Dec. 17, 2014)
Use of BZDs
• Anxiety Disorders
• Generalized Anxiety Disorder
• Panic Disorder
• Social Anxiety Disorder
• Obsessive Compulsive Disorder
• Major Depressive Disorder
• Trauma and Stress Related Disorders (PTSD, Adjustment Disorders)
• Dementia Disorders
• Cluster B Personality Disorders

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 5
Target Actions and Adverse Responses
• Sedative
•Hypnotic
• Anxiolytic
• Anticonvulsant
•Muscle relaxant
• Anterograde amnesia
•Dissociation
• Cognitive impairment
• Paradoxical anxiety
• Behavioral disinhibition
•Dependence & tolerance
Mechanism of Action of BZDs
• Gamma aminobutyric acid neurotransmitter (GABA), neuroinhibitory
• GABA receptors
• GABAA
• GABAB
• Chloride channel

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 6
GABA‐A Receptor
BZD Action on GABA‐A Receptor
Ashton Manual: benzo.org.uk

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 7
BZD binding to GABA
BZD Pharmacokinetics
Drug Half‐life (Active metabolite)
Approx Dose Equivalentto Diazepam 10 mg
Alprazoam (Xanax) 6‐12 hrs 0.5 mg
Chlordiazepoxide (Librium) 5‐30 (36‐200) hrs 5‐6 mg
Clonazepam (Klonopin) 18‐50 hrs 0.5 mg
Chlorazepate (Tranxene) (36‐200) hrs 15 mg
Diazepam (Valium) 20‐100 (36‐200) hrs 10 mg
Lorazepam (Ativan) 10‐20 hrs 1 mg
Oxazepam (Serax) 4‐15 hrs 20 mg
Prazepam (Centrax) (36‐200) hrs 10‐20 mg

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 8
Reasons for BZD Withdrawal
• Long term unwanted effects
• Memory loss and impaired learning
• Cognitive dulling
• Emotional blunting
• Depression
• Loss of efficacy over time
Withdrawal Process from BZDs
• Begin with detailed review of BZD use, reason for initiation, reason for continuation, change in dosage, observed effects
• Frank, non judgmental discussion of pros and cons of continuation vs withdrawal
• Commitment from both client and provider
• Adequate social and emotional support
• Discussion of use of protocol designed for slow and safe withdrawal
• Written agreement of protocol and limits of agreement (e.g., loss of prescription, limited prescriptions, appointments)

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 9
Withdrawal Principles
• Dosage tapering to avoid risk of:
• Convulsions
• Psychotic reactions
• Acute anxiety exacerbation
• Switching to long‐acting benzodiazepine of similar potency
• Using appropriate formulations to achieve dosage (e.g., tablet, liquid)
Designing Withdrawal Schedule
• Schedule around client’s symptoms (i.e., insomnia, morning inertia)
• Change one dose at a time, usually start with night time dose
• Less often taking dose, less focus on the drug
• The larger the initial dose, the greater the decrement (i.e., first decrease may be 25%)
• Plan first several decrements to determine tolerability of plan and permit slowing down or increasing rate of decrements
• Never go backwards in dosage taper
• Watch for compensation by increasing OTC drugs, alcohol, street drugs
• If not successful with first effort at withdrawal, try again when stress is lower

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 10
Example Withdrawal Schedule(Starting dosage alprazolam 6 mg daily. Alz = alprazolam, Dzp = diazepam.)
MORNING MID DAY EVENING DAILY DIAZEPAMEQUIVALENT
Week 1 Alz 2 mg Alz 2 mg Alz 1.5 mg + dzp 10 mg
120 mg
Week 2 Alz 2 mg Alz 2 mg Alz 1 mg + dzp20 mg
120 mg
Week 3 Alz 1.5 mg + dzp 10 mg
Alz 2 mg Alz 1 mg + dzp20 mg
120 mg
Week 4 Alz 1 mg + dzp20 mg
Alz 2 mg Alz 1 mg + dzp20mg
120 mg
Week 5‐6 Alz 1 mg + dzp20 mg
Alz 1 mg + dzp10 mg
Alz 1 mg + dzp20 mg
110 mg
Example Withdrawal Schedule(Starting dosage alprazolam 6 mg daily. Alz = alprazolam, Dzp = diazepam.)
MORNING MID DAY EVENING DAILY DIAZEPAM EQUIVALENT
Weeks 7‐8 Alz 1 mg + dzp20 mg
Alz 1 mg + dzp10 mg
Alz 0.5 mg + dzp20 mg
100 mg
Weeks 9‐10 Alz 1 mg + dzp20 mg
Alz 1 mg + dzp10 mg
D/C alzDzp 20 mg
90 mg
Weeks 11‐12 Alz 0.5 mg + dzp 20 mg
Alz 1mg + dzp10 mg
Dzp 20 mg 80 mg
Weeks 13‐14 Alz 0.5 mg + dzp 20 mg
Alz 1 mg + dzp10 mg
Dzp 20 mg 80 mg
Weeks 15‐16 Alz 0.5 mg + dzp 20 mg
D/C alzDzp 10 mg
Dzp 20 mg 60 mg
Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 11
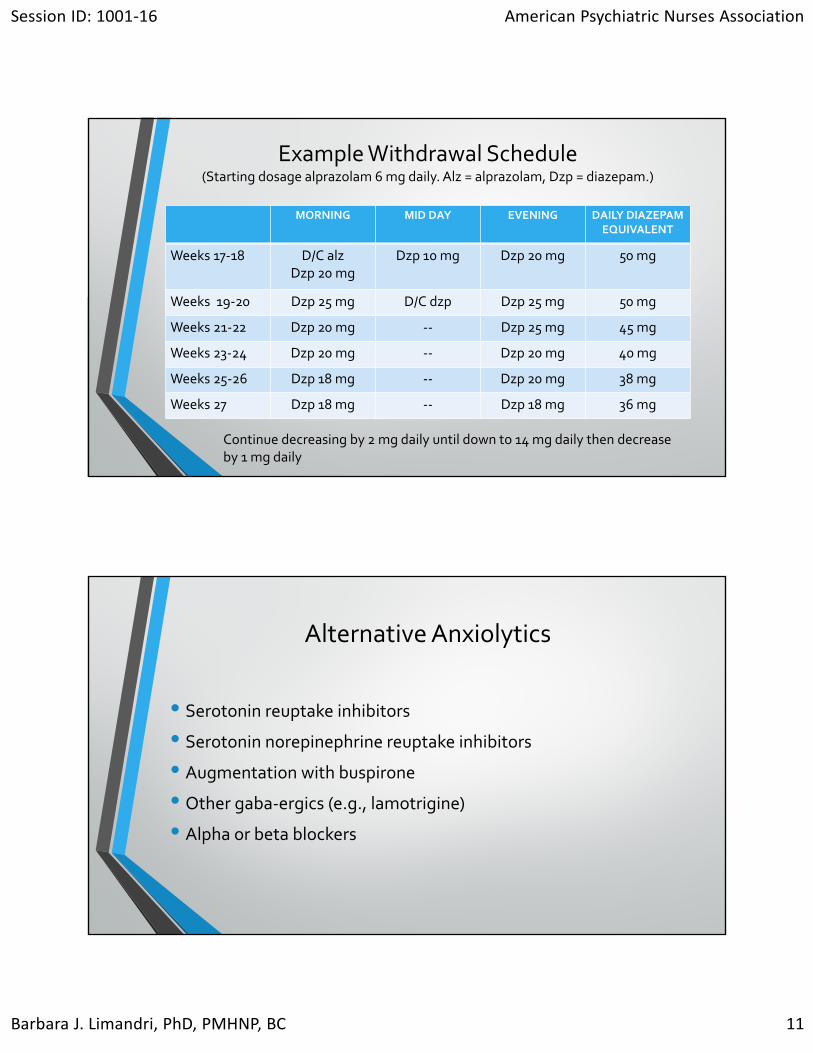
Example Withdrawal Schedule(Starting dosage alprazolam 6 mg daily. Alz = alprazolam, Dzp = diazepam.)
MORNING MID DAY EVENING DAILY DIAZEPAMEQUIVALENT
Weeks 17‐18 D/C alzDzp 20 mg
Dzp 10 mg Dzp 20 mg 50 mg
Weeks 19‐20 Dzp 25 mg D/C dzp Dzp 25 mg 50 mg
Weeks 21‐22 Dzp 20 mg ‐‐ Dzp 25 mg 45 mg
Weeks 23‐24 Dzp 20 mg ‐‐ Dzp 20 mg 40 mg
Weeks 25‐26 Dzp 18 mg ‐‐ Dzp 20 mg 38 mg
Weeks 27 Dzp 18 mg ‐‐ Dzp 18 mg 36 mg
Continue decreasing by 2 mg daily until down to 14 mg daily then decrease by 1 mg daily
Alternative Anxiolytics
• Serotonin reuptake inhibitors
• Serotonin norepinephrine reuptake inhibitors
• Augmentation with buspirone
• Other gaba‐ergics (e.g., lamotrigine)
• Alpha or beta blockers

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 12
Alternative Anxiety Reduction Strategies
• Progressive relaxation
• Mindfulness practice
• Distress tolerance skills
Summary
• Benzodiazepines used for short term only (2‐4 wks)
• Avoid use with older clients, esp with mobility problems
• Can be used as interim while other medications initiated (e.g., SRIs)
• Require careful and crystal clear explanation to client with specific limitations
• Withdrawal should be slow and using established written protocol that client agrees to adhere to
• Non adherence needs to have consequences established initially in writing

Session ID: 1001‐16 American Psychiatric Nurses Association
Barbara J. Limandri, PhD, PMHNP, BC 13
References
• Boeuf‐Cazou, O, Bongue, B., Anslau, D., Marquie, J‐C, Lapeyre‐Mestre, M. (2011). Impact of long‐term benzodiazepine use on cognitive functioning in young adults: the VISAT cohort. European Journal of Pharmacology, 67: 1045‐1052.
• Deckersbach, T, Mshier, S.J., Tuschen‐Caffier, B, Otto, M.W. (2011). Memory dysfunction in panic disorder: An investigation of the role of chronic benzodiazepine use. Depression and Anxiety, 28: 999‐1007.
• Dell’osso, B, Lader, M. (2013). Do benzodiazepines still deserve a major role in the treatment of psychiatric disorders? A critical reappraisal. European Psychiatry: The Journal Of The Association Of European Psychiatrists. 28: 7‐20.
• deGier, NA, Gorgels, WJ, Lucassen, PL, Oude Voshaar, R, Mulder, J, Zitman, F (2011). Discontinuation of long‐term benzodiazepine use: 10‐year follow‐up. Family Practice. 28: 253‐9.
• Gallager, H.C. (2013). Addressing the issue of chronic, inappropriate benzodiazepine use: How can pharmacists play a role? Pharmacy, 1: 65‐93.
References• Hawkins, EJ, Malte, CA, Imel, ZE, Sason, AJ, Kiviahan, DR (2012). Prevalence
and trends of benzodiazepine use among Veterans Affairs patients with posttraumatic stress disorder, 2003‐2010. Drug And Alcohol Dependence 124:154‐61.
• National Health Service (2008). Guidance for Prescribing & Withdrawal of Benzodiazepines & Hypnotics in General Practice. www.benzo.org.uk/amisc/bzgrampian.pdf
• NIMH (2014) Press release: Despite risks, benzodiazepine use highest in older people. http://www.nimh.nih.gov/news/science‐news/2014/despite‐rsks‐benzodiazepine‐use‐highest in‐older people. shtml.
• Olfson, M., King, M., Schoenbaum, M. (2015). Benzodiazepine use in the United States. JAMA Psychiatry, 72: 136‐142.