role of mdct in blunt abdominal trauma dr. muhammad bin zulfiqar
TRANSCRIPT

Role Of MDCT in Blunt Abdominal Trauma
DR MUHAMMAD BIN ZULFIQARPGR III FCPS Services institute of Medical
Sciences/ Services Hospital Lahore
Very Special Thanks to Dr. Bushra Ujala & Radiology Assistant

OBJECTIVES
• Initial evaluation of– Blunt trauma– Penetrating trauma
• Follow up of non-operative management• Rule out injury

INTRODUCTION
• Trauma: leading cause of death under 40• Abdominal trauma: 10%
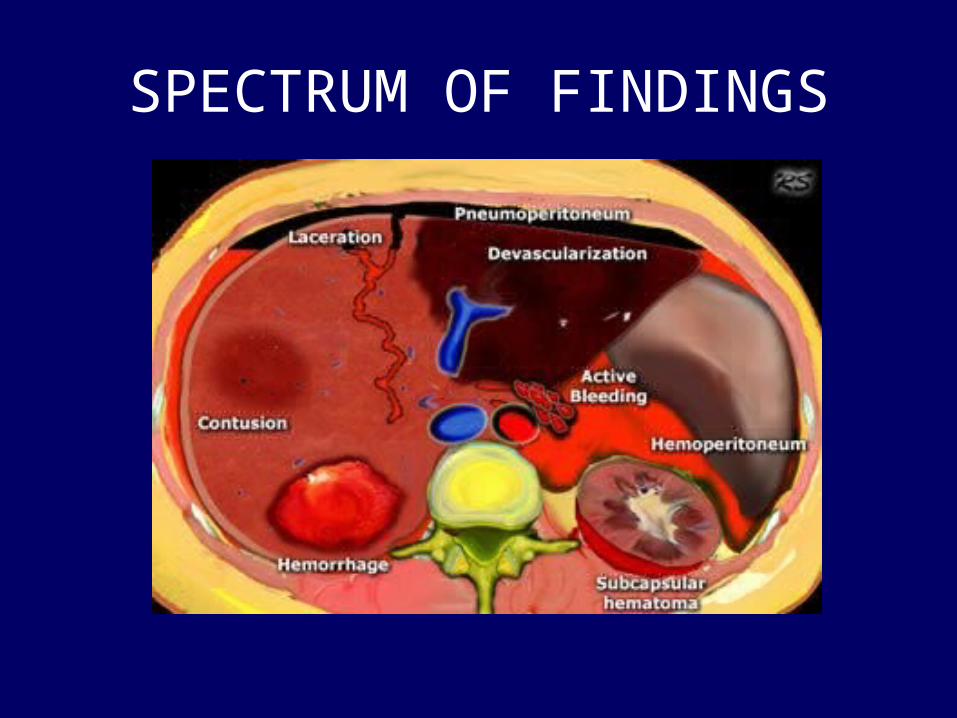
SPECTRUM OF FINDINGS

ABDOMINAL TRAUMA PROTOCOL
• Blunt injury:– deceleration, crush, weapon(e.g bat)• Venous phase ~ 70 seconds• Delayed scan if injury present; ~ 3-5 minutes
• Penetrating injury: – knives, gun• Same as blunt• Additional scan after rectal contrast material

SPLEEN
• MOST COMMONLY INJURED SOLID ORGAN(25%)

SPLENIC CT INJURY GRADING SCALE ( AAST)
Grade 1– Laceration(s) < 1cm deep– Subcapsular hematoma < 1cm diameter
Grade 2– Laceration(s) 1-3 cm deep– Subcapsular or central hematoma 1-3cm diam
Grade 3– Laceration(s) 3-10 cm deep– Subcapsular or central hematoma 3-10 cm dia
Grade 4– Laceration(s) >10 cm deep– Subcapsular or central hematoma > 10 cm diam
Grade 5– Splenic tissue maceration or devascularization

A CASE OF SPLENIC INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

SPLENIC INJURY-ANOTHER CASE
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

SPLENIC INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
A 22 yr male 3 hr after a snowboarding accident with LUQ & Lt shoulder pain.

SPLENIC INJURY- CONTRAST BLUSH
• 82% failure rate for NOM• 9.2 x more require intervention• Managed with embolization / splenectomy
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

LIVER
• 2ND MOST COMMONLY INVOLVED ORGAN

LIVER INJURY
Liver injury. The arrows indicate different types of injury.
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
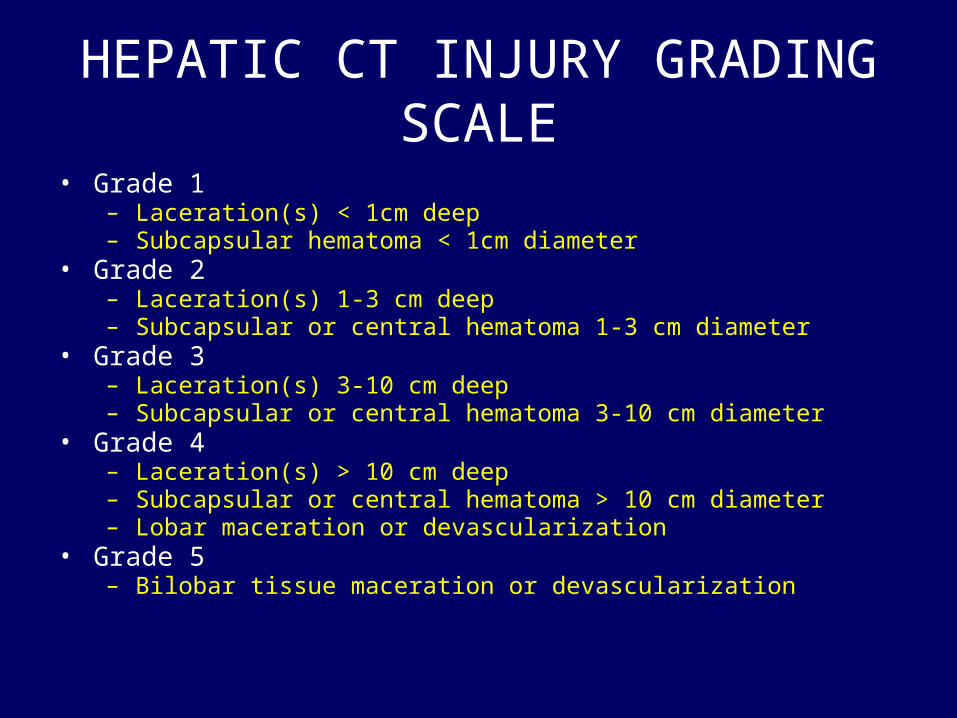
HEPATIC CT INJURY GRADING SCALE• Grade 1
– Laceration(s) < 1cm deep– Subcapsular hematoma < 1cm diameter
• Grade 2– Laceration(s) 1-3 cm deep– Subcapsular or central hematoma 1-3 cm diameter
• Grade 3– Laceration(s) 3-10 cm deep– Subcapsular or central hematoma 3-10 cm diameter
• Grade 4– Laceration(s) > 10 cm deep– Subcapsular or central hematoma > 10 cm diameter– Lobar maceration or devascularization
• Grade 5– Bilobar tissue maceration or devascularization

LIVER INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
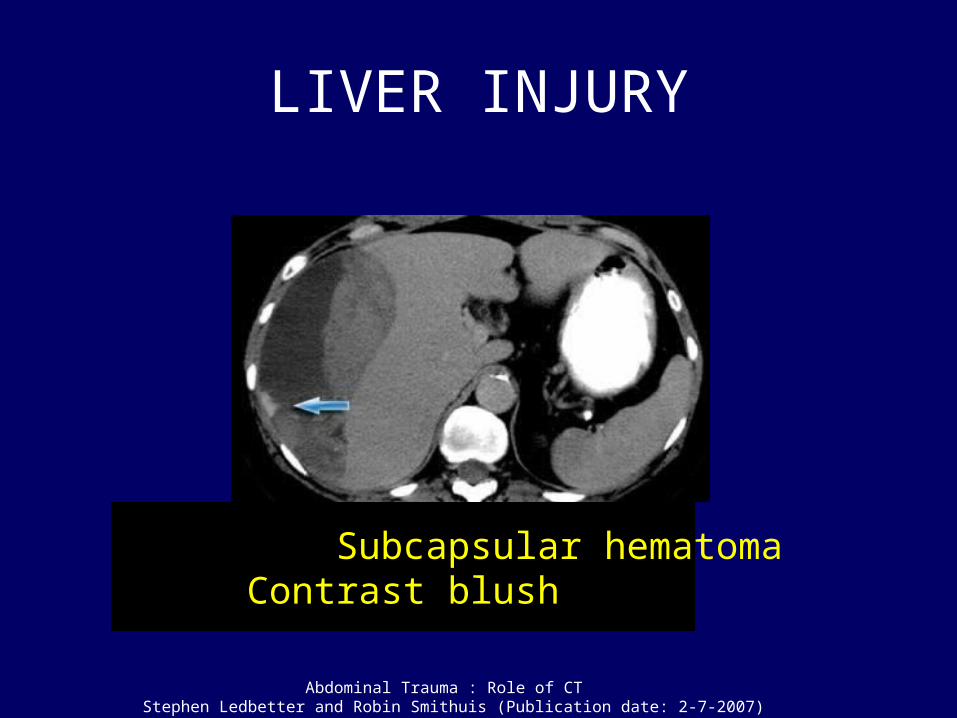
LIVER INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Subcapsular hematomaContrast blush

LIVER LACERATIONS
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

LIVER INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Avulsed Rt hepatic vein

RENAL INJURY
• 90% due to blunt trauma- 10% penetrating• 3rd most common involved organ in adults– 10% of solid visceral injury
• Most common injured organ in children • Evaluation for– Parenchymal injuries– Vascular injuries– Collecting system injuries

RENAL-PENETRATING INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

RENAL INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Knife stab in the Rt flank.

RENAL INJURY SCALE (AAST)• Grade 1
– Contusion / Subcapsular hematoma– No parenchymal laceration
• Grade 2– Laceration < 1cm depth of renal cortex– No urinary extravasation
• Grade 3– Laceration > 1cm depth of renal cortex– No urinary extravasation
• Grade 4– Laceration extending through the renal cortex, medulla and into collecting
system– Minor renal artery or vein injury with contained hematoma
• Grade 5– Shattered kidney– Devascularized kidney, hilar avulsion

RENAL INJURY-BLUNT TRAUMA
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

CATEGORIES OF RENAL INJURIES
Introduced by Michael Federle

BLADDER INJURY
• X-ray of a 65 yr male struck by a car travelling at moderate speed.
• Loss of consciousness for 2 min.
• Foley catheter was passed & there was gross hematuria.
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

BLADDER INJURY
Images of the routine trauma.
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

BLADDER INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Pre-cystogram Post-cystogram

BADDER INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Sagittal Coronal
Reconstruction

ARTERIAL BLEEDING IN PELVIC INJURY
Pre-cystogram image
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

PANCREATIC INJURY
• Uncommon- 0.4%• 1.1% penetrating
trauma• 0.2% blunt trauma• Isolated injury-Rare• Part of `package injury`

VECTORS OF FORCE- TRAUMA ``PACKAGES``
Right-sided Midline Left-sided
R hepatic lobe Left hepatic lobe SpleenR kidney Pancreatic body L kidneyDiaphragm Aorta DiaphragmPancreatic head Transverse colon Pancreatic tailDuodenum DuodenumIVC Small bowel

PANCREATIC TAIL INJURY-LT SIDED PACKAGE INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
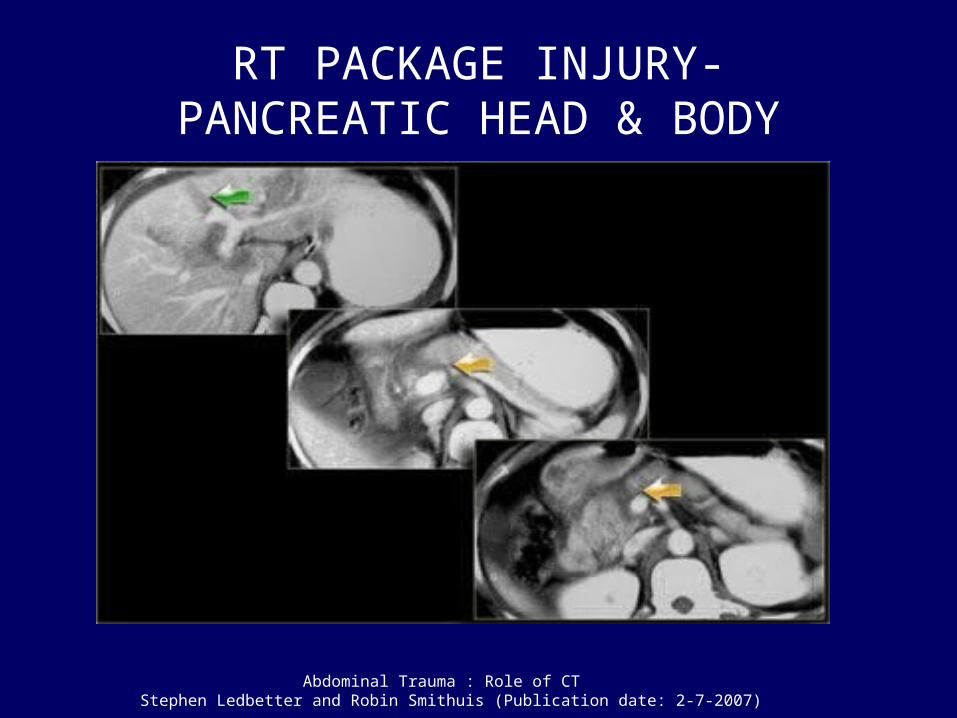
RT PACKAGE INJURY-PANCREATIC HEAD & BODY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
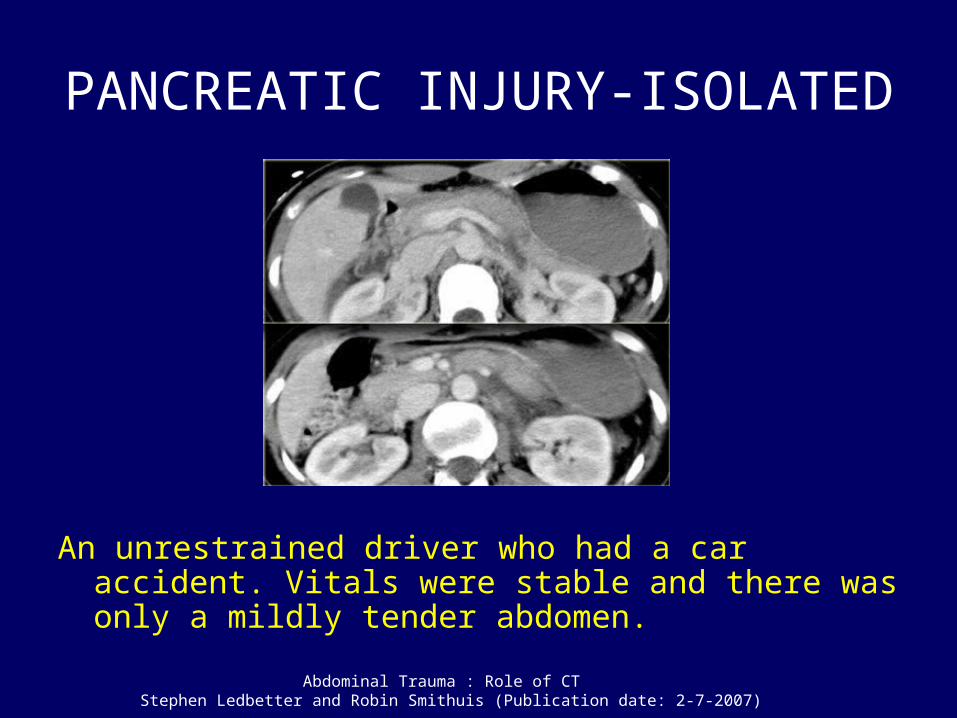
PANCREATIC INJURY-ISOLATED
An unrestrained driver who had a car accident. Vitals were stable and there was only a mildly tender abdomen.
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
DIAPHRAGMATIC INJURY
• Incidence: – 1-6% of blunt trauma patients– Penetrating 2x > blunt
• Frequently other injuries (75-100%)• Left > Right– Blunt 75%– Penetrating 56%
• Bilateral 1-5% of cases• Posterolateral : most frequent site

DIAPHRAGMATIC INJURY
• Specific signs– Herniation of abdominal viscera into thorax– CT ``collar`` sign
• Non-specific signs– Discontinuity of the crus– Thickening of the diaphragm– ``dependent viscera `` sign
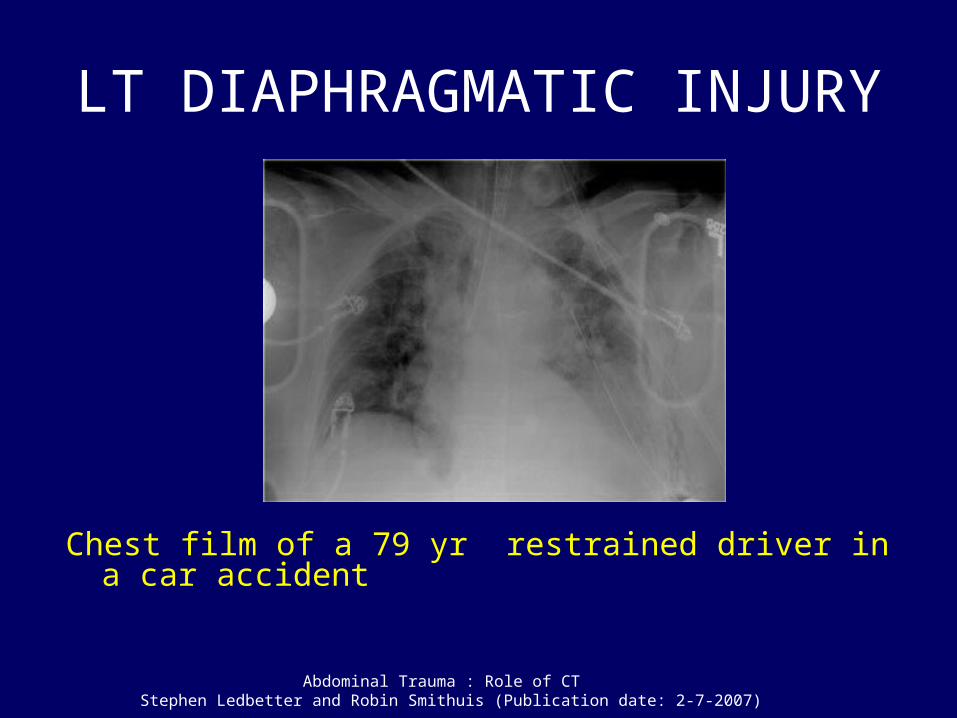
LT DIAPHRAGMATIC INJURY
Chest film of a 79 yr restrained driver in a car accident
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
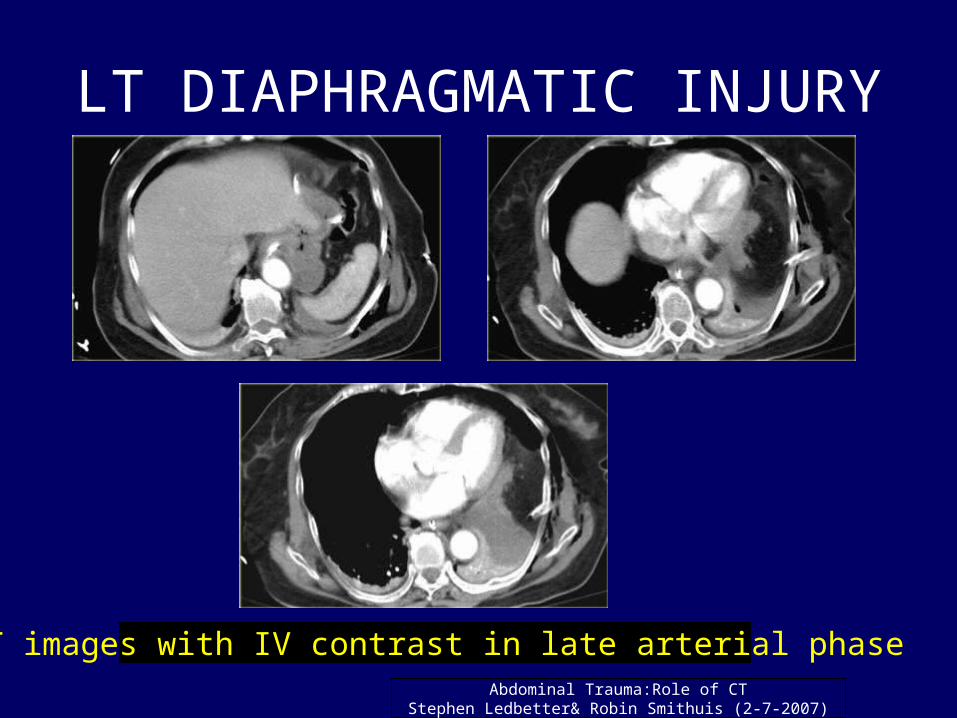
LT DIAPHRAGMATIC INJURY
CT images with IV contrast in late arterial phaseAbdominal Trauma:Role of CT
Stephen Ledbetter& Robin Smithuis (2-7-2007)

LT DIAPHRAGMATIC INJURY
CT findings in same pt. ( oral contrast )
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

CT `COLLAR` SIGN
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Coronal reconstruction

`DEPENDENT VISCERA` SIGN
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

RT DIAPHRAGMATIC INJURY
Chest film in a pt. with right sided injury
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

`COLLAR` SIGN –RT SIDED DIAPHRAGMATIC RUPTURE
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
Axial image Sagittal MPR

AORTIC INJURY
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
An unrestrained 22 yr male involved in a high speed motor vehicle accident

AORTIC INJURY
Consecutive images of the aorta at the level of the diaphragm.
Abdominal Trauma : Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)
BOWEL INJURY
• Direct Findings:– Bowel wall disruption– Oral contrast extravasation
• Indirect Findings:– Free intraperitoneal / retroperitoneal air– Free intraperitoneal / retroperitoneal fluid– Focal area of bowel wall thickening– Abnormal bowel wall enhanement.

BOWEL INJURY-CONTRAST EXTRAVASATION
Abdominal Trauma: Role of CT Stephen Ledbetter and Robin Smithuis (Publication date: 2-7-2007)

BOWEL INJURY
15 yr boy with blunt trauma to abdomen and a perforated stomach.
Bowel, Trauma: Multimedia;Raul N Uppot, MD, Updated: sep 2, 2005.

BOWEL INJURY
Female with blunt abdominal trauma and duodenal perforation.
Bowel, Trauma: Multimedia; Raul N Uppot, MDUpdated:Sep 2, 2005
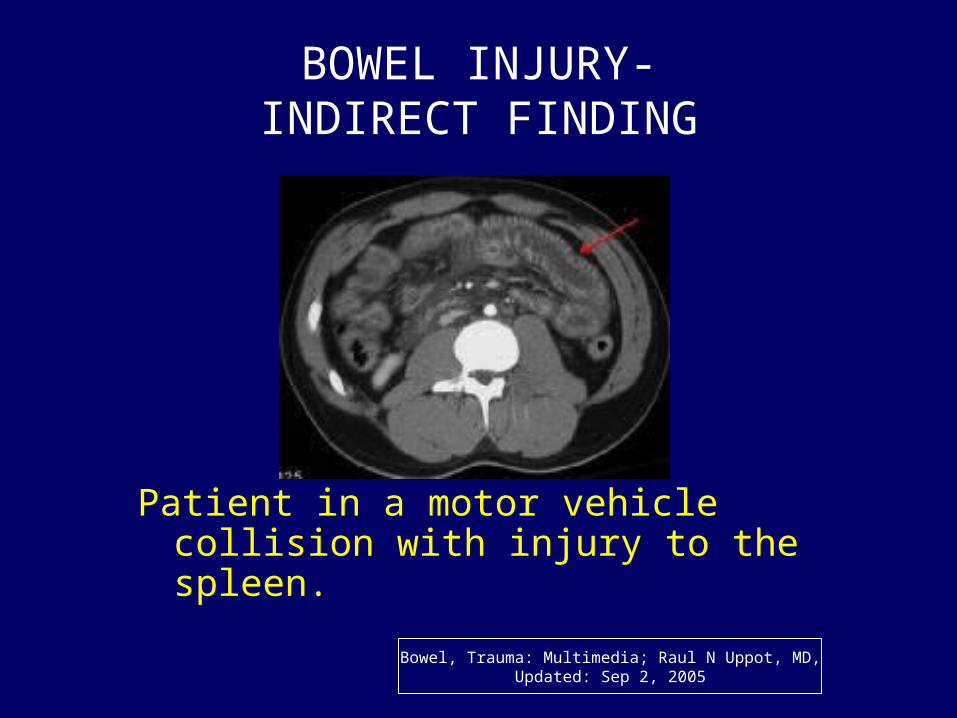
BOWEL INJURY-INDIRECT FINDING
Patient in a motor vehicle collision with injury to the spleen.
Bowel, Trauma: Multimedia; Raul N Uppot, MD,Updated: Sep 2, 2005

Take Home Message
• By using MDCT we can evaluate blunt abdominal trauma patients and help surgeons in management.
• We can confidently suggest Whether surgical intervention is mandatory or not.

REFERENCES
• Imaging of Renal Trauma: A Comprehensive Reviewby Akira Kawashima, MD, Carl M. Sandler, MD, Frank M. Corl, MS, O. Clark West, MD, Eric P. Tamm, MD, Elliot K. Fishman, MD and Stanford M. Goldman, MDRadiographics. 2001;21:557-574
• PDF format: American College of Radiology, ACR Appropriateness Criteria® for Blunt Abdominal Trauma This review considers the issue of blunt abdominal trauma in adults. A continued trend is noted for detection of specific findings that do predict the need for therapeutic surgery or for angiographic embolization or that predict a period of close observation is needed for an injured patient. This trend in imaging parallels a strong trend in trauma therapy toward nonoperative management of injuries of the spleen, liver, and kidney even when hemoperitoneum is present.
• Optimization of Selection for Nonoperative Management of Blunt Splenic Injury: Comparison of MDCT Grading Systems by Helen Marmery et al. AJR 2007; 189:1421-1427
