role ofretrograde his purkinje block in...
TRANSCRIPT
Role of Retrograde His Purkinje Block in theInitiation of Supraventricular Tachycardia byVentricular Premature Stimulation in theWolff-Parkinson-White Syndrome
MASOODAKHTAR, MOHAMMADSHENASA, and DONALDH. SCHMIDT,Natalie and Norman Soref and Family Electrophysiology Laboratory,University of Wisconsin Mount Sinai Medical Center,Milwaukee, Wisconsin 53201
A B S T R A C T The precise mechanisms for paroxys-mal reentrant supraventricular tachycardia (PSVT) ini-tiation during right ventricular premature stimulation(V2 method) were analyzed in 14 consecutive patientswith Wolff-Parkinson-White Syndrome in whom thePSVT was inducible during retrograde refractoryperiod studies. 9 patients had left-sided and the remain-ing 5 of 14 had right-sided ventriculo-atrial (VA) acces-sory pathway (AP). At the basic cycle lengths (V,V1)ranging from 550 to 900 ms (mean, 657.1+139.5), closelycoupled V2 (mean V,V2, 357.3+59.2 ms, range 320-500)produced retrograde His bundle (H2) activation via thebundle branches and retrograde atrial (A2) activation viathe AP. As the V1V2 were further shortened, the V2showed a retrograde block in the His Purkinje system(HPS) and conducted to the atria via AP in 9 of 14 cases.Subsequently, the A2 impulse conducted anterogradeover the atrioventricular node-HPS to initiate a PSVToran atrial echo response in all nine cases. In none of thepatients was a PSVT induced by V2 when the latterproduced retrograde H2 activation via the bundlebranches. In 10 of 14 cases, however, the retrograde H2was followed by a V3, due to macroreentry in the HPS.The V3 in turn blocked retrogradely in the HPS whileproducing A3 via the AP to initiate a PSVT or an atrialecho response in 9 of 10 cases. Retrograde block of V2and/or V3 in the HPSresulted in PSVTinitiation in 13 of14 cases, whereas in the remaining 1 case the exactmechanism was not clear. In none of the patients in thisseries was the PSVT initiated with a retrograde block of
Address reprint requests to Dr. Masood Akhtar, Cardio-vascular Disease Section, Mount Sinai Medical Center, POBox 342, Milwaukee, Wisc. 53201.
Received for publication 22 August 1980 and in revisedform 7 November 1980.
V2 in the atrioventricular node with or withoutconcomitant retrograde A2 activation via the AP. Weconclude that within the ranges of cycle lengths tested,a retrograde block of V2 and/or V3 in the HPSis the mostcommon mechanism for initiation of PSVT duringventricular premature stimulation in patients with theWolff-Parkinson-White Syndrome.
INTRODUCTION
Paroxysmal reentrant supraventricular tachycardia(PSVT),' utilizing atrioventricular (AV) node and HisPurkinje system (HPS) anterogradely, and an accessorypathway (AP) in the retrograde direction, is relativelycommon in patients with the Wolff-Parkinson-White(WPW) Syndrome (1-4). Several studies have demon-strated that PSVTin these patients can be initiated withatrial as well as ventricular premature beats. It has alsobeen previously demonstrated that during ventricularpremature stimulation, the ability or inability to inducePSVT depends upon the various patterns of ven-triculo-atrial (VA) conduction along the normal and theAP (5-8). Although addressing themselves to the VAconduction along the normal pathway in patients withthe WPWSyndrome, studies to date have not made aclear distinction between conduction along the HPSvs.the AV node, the two components of normal pathway.Since the HPSand AVnode have different electrophys-iological properties and therapeutic responses, a clearunderstanding of the role of retrograde conduction in
'Abbreviations used in this paper: Ae, atrial echo; AP,accessory pathway; AV, atrioventricular; ERP, effective re-fractory period; HPS, His Purkinje system; PSVT, paroxysmalrentrant supraventricular tachycardia; VA, ventriculo-atrial;WPW,Wolff-Parkinson-White.
1047J. Clin. Invest. (© The American Society for Clinical Investigation, Inc. * 0021-9738/81104/1047/09 $1.00Volume 67 April 1981 1047-1055
the HPS and the AV node in the initiation of PSVT isdesirable. This report demonstrates the role of retro-grade block within the HPS in the initiation of PSVTduring right ventricular premature stimulation in 14patients with the WPWSyndrome.
METHODSRight heart catheterization was performed in a post absorptive,nonsedated state, using local anesthesia. The nature of the pro-cedure was explained to all patients and signed consents wereobtained. Quadripolar electrode catheters were percutane-ously inserted into peripheral veins and positioned in theregion of the high right atrium, AV junction, coronary sinus,and right ventricle. The catheters were used for local bipolarelectrogram recordings and/or electrical stimulation usingtechniques previously described (9). Surface electrocardio-gram Leads I, II, and VI, intracardiac electrograms, and timelines were simultaneously displayed on a multichannel oscil-loscope and recorded on a frequency-modulated tape. Therecords were subsequently retrieved for analysis at a paperspeed of 100-150 mm/s. Intracardiac stimulation was per-formed using digital stimulator capable of delivering rectangularimpulses with adjustable voltage and duration. During theconduct of these studies, patient isolation existed and allequipment was carefully grounded.
Retrograde refractory period studies were performed usingventricular extrastimulus method. Premature stimuli wereintroduced after eight ventricular paced beats of predeter-mined constant cycle length. The coupling intervals weregradually reduced by 10-20 ms until ventricular muscle re-fractoriness was encountered.
Definition of terms. A complete set of definitions foranterograde and retrograde conduction and refractory periodstudies has been previously published (9). Pertinent defini-tions repeatedly used in this text will be outlined here.
The A-H interval was measured from the onset of low atrialelectrogram to the beginning of His bundle potential. TheH-V and RB-V intervals were measured from the onset of Hisand right bundle branch deflections to the earliest detectableventricular activity, either on the surface electrocardiogramor the local intracardiac tracings.
Atrial echo (Ae) response represents spontaneous retrogradeexcitation of the atrium exclusively via the accessory pathwayoccurring during nonpaced beats.
For an easier comprehension some of the terms used andelectrophysiologic parameters measured during retrograderefractory period studies are graphically depicted in Fig. 1.The S,, V1, and A1 represent stimulus artifact, ventricular, andretrograde atrial deflections, respectively, during the basicdrive, whereas S2, V2, H2, and A2 represent stimulus artifact,ventricular, His bundle, and atrial deflections following thepremature beat.
The retrqgrade activation in response to V2 of the H2 via thebundle branches and the A2 via AP is shown in panel A. Exclu-sive VA conduction via the AP during both V, and V2 is sug-gested by the sequence of atrial activation and its lack ofchange following V2 despite significant delay along the normalpathway (V2H2 interval).
The effective refractory period (ERP) of AP (panel B) is thelongest V1V2 where V2 blocks in the AP.
The ERP-AVnode (panel C) is the longest V,H2 where H2 isnot followed by A2. V,H2 is taken in lieu of retrograde H1H2since H1 is generally not visible during the basic drive, and itis assumed that V1H1 interval is constant (9). It should be notedthat ERP-AV node can only be deterrnined after retrogradeERPof AP pathway is encountered.
ERP-HPS (panel D) is longest V1V2 where V2 blocks belowthe His bundle recording site (i.e., HPS).
RESULTS
Anterograde and retrograde conduction and refractoryperiod studies were performed in 22 consecutive pa-tients with WPWSyndrome who had symptomaticPSVT. In only 14 of 22 patients was the PSVTinducibleduring right ventricular premature stimulation, andfindings in these 14 cases form the basis of this report.In the remaining 8 of 22 cases, PSVT could not beelicited during ventricular premature stimulation forthe reasons previously published (7). 12 of the 14 hadventricular preexcitation during sinus rhythm, whereasthe remaining two (patients 5 and 8) had electrocardio-graphically concealed left sided AP. The pertinentclinical and electrophysiologic data are summarized inTable I. At the time of study all were in sinus rhythmand were not taking any cardioactive medications. Twopatients had associated arteriosclerotic heart disease,and another two had mitral valve prolapse, whereas theremaining cases did not have clinically detectablestructural heart disease. Although two or more basicventricular cycle lengths were scanned in 10 of 14 pa-tients, to simplify presentation of the results only thedata from the shortest available cycle lengths in eachcase will be presented in detail.
Retrograde refractory period studies. Ventricularpremature stimulation was initiated at V1V2 intervalswhich measured 50-100 ms less than the basic drive,and the coupling intervals were progressively short-ened. During the basic drive (V,) six patients (patients2, 3, 5, 7, 10, and 13; Table I) demonstrated retrogradeatrial depolarization exclusively via the AP, whereasfusion retrograde atrial activation was observed in theothers (10). In the latter cases a change from fusionatrial activation to exclusive activation via the AP wasnoted as the V1V2 were further shortened. This changein retrograde atrial activation was noted at V1V2 inter-vals which had not yet produced emergence of a Hisdeflection from the V2 electrogram. At the basic cyclelength range of 550-900 ms (Table I), the His bundledeflection first emerged from V2 at V,V2 intervalsranging from 320-500 ms. Since in patients with retro-gradely functioning AP the His bundle deflection fol-lowing V2 could result from either retrograde conduc-tion via the bundle branches or anterograde depolariza-tion via the AV node following A2 activation over theAP, the behavior of His bundle activation was closelyanalyzed (11). In all nine patients with left-sided (cases1-9, Table I) and 2 of 5 cases (patients 11 and 12) withright-sided VAAP, the separation of retrograde A2 fromV2 deflection (on the His bundle electrogram tracing)was sufficient to provide a clear segment where thepresence of a His deflection could be identified. In all
1048 M. Akhtar, M. Shenasa, and D. H. Schmidt
A
V1,- V~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~lRA ! iV1A1 A
CS _Ii.11 ViAiziVAi 100
A
~~Al V2 A2
HBI4
550 300
V2A2=175
V2A2=100 a
V2A2145 4
V2H2-125
C
A1 Ai m,lbM_ A
A1 A
mu9RSmm_mmm.WS ; V J~~~~~~~~~~~~~~~~
f qY''- - SlAV!2"'S' w'550 280
ERP-AVNVl H2
B
4-A- A!- 2 V22=335
9¶~~~~49~~l 4 VA2295
Vi A VA2 VL!IL~~~~1~~21J\~ V2A2=295
550 20 VH2=140OERP-AP
D ~~~~VlV2
I LI
V2H2=140" 1U'
A1h1
2701 1
ERP-HPSV1V2
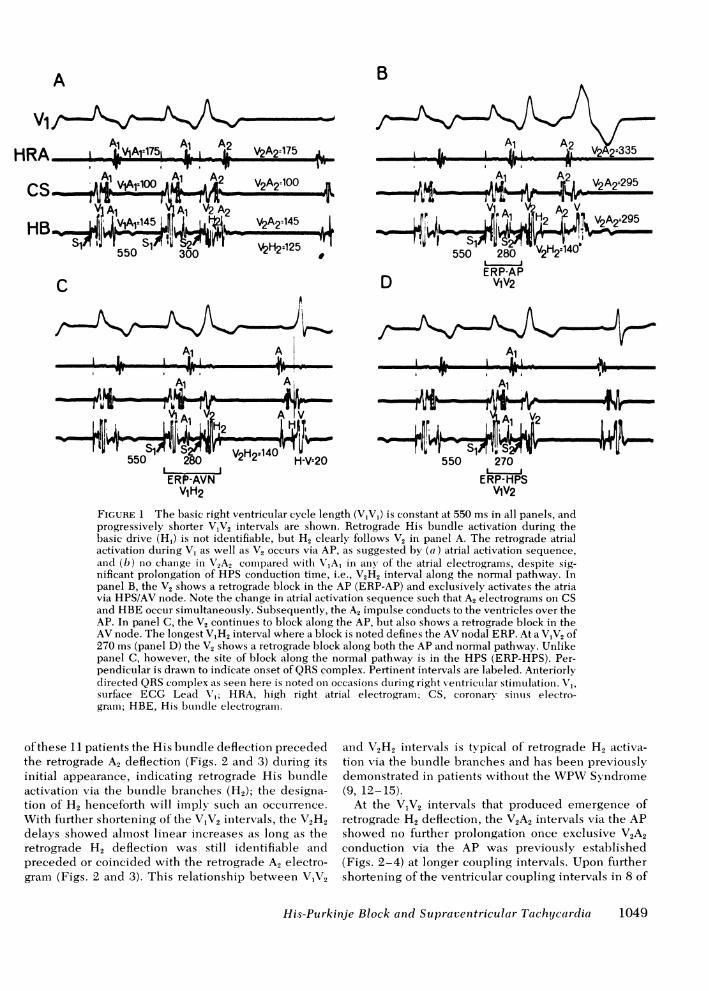
FIGURE 1 The basic right ventricular cycle length (V,Vl) is constant at 550 ms in all panels, andprogressively shorter V1V2 intervals are shown. Retrograde His bundle activation during thebasic drive (H1) is not identifiable, but H2 clearly follows V2 in panel A. The retrograde atrialactivation during V1 as well as V2 occurs via AP, as suggested by (a) atrial activation sequence,and (b) no change in V"2A2 compare(d with NVA1 in any of the atrial electrograms, despite sig-nificant prolongation of HPS conduction time, i.e., V2H2 interval along the normal pathway. Inpanel B, the V2 shows a retrograde block in the AP (ERP-AP) and exclusively activates the atriavia HPS/AV node. Note the change in atrial activation sequence such that A2 electrograms on CSand HBEoccur simultaneously. Subsequently, the A2 impulse conducts to the ventricles over theAP. In panel C, the V2 continues to block along the AP, but also shows a retrograde block in theAVnode. The longest V1H2 interval where a block is noted defines the AVnodal ERP. At a V1V2 of270 ms (panel D) the V2 shows a retrograde block along both the AP and normal pathway. Unlikepanel C, however, the site of block along the normal pathway is in the HPS (ERP-HPS). Per-pendicular is drawn to indicate onset of QRScomplex. Pertinent intervals are labeled. Anteriorlydirected QRScomplex as seeni here is noted on occasions duiring right veentricular stimuilation. V1,sturface ECG Lead V'1; HRA, high right atrial electrogram; CS, coronary sinuiIs electro-graim; HBE, His btundle electrogram.
of these 11 patients the His bundle deflection precededthe retrograde A2 deflection (Figs. 2 and 3) during itsinitial appearance, indicating retrograde His bundleactivation via the bundle branches (H2); the designa-tion of H2 henceforth will imply such an occurrence.With further shortening of the V,V2 intervals, the V2H2delays showed almost linear increases as long as theretrograde H2 deflection was still identifiable andpreceded or coincided with the retrograde A2 electro-gram (Figs. 2 and 3). This relationship between VIV2
and V2H2 intervals is tvpical of retrograde H2 activa-tion via the bundle branches and has been previouslydemonstrated in patients withouit the WPWVSyndrome(9, 12-15).
At the VIV2 intervals that produced emergence ofretrograde H2 deflection, the V2A2 intervals via the APshowed no further prolongation once exclusive V2A2conduction via the AP was previously established(Figs. 2-4) at longer coupling intervals. Upon furthershortening of the ventricular coupling intervals in 8 of
His-Purkinje Block and Supraventricular Tachycardia
I I Ra- I A
VW - -vn 7- "IT O"IT,
1049

cn cn cn cnP- P- P. PL4x z xP6 .6 I6
+ + +
+ + +I I + + +
01i 00 00_F F
10 04
10
+ + + +
ct (c4 (A (A cn zP. P. .- .~ >
m m m m m<0.4 04 04 04:>
+ + + + Oi+
V
+ + + + + +
+ + + + + +
o oc- c0
4 o-_4 _
0) 0 00 0cli _- cli cs c-
10 10 10001 -4 - (0o ocs _ b s cs~~~~~~~
+
+
0
(.0
+ + + C-
0.40.4F x_ _
0.4+ = 0*4
+ m
I0 01 r to
00 0 00 00COOl - - 0_ coCO CO CO CO CO CO CO
0 0 0 0 0 0Ot, It 10 (.0 (0 00 10
01't
01 01 0 0S C C CQC-Vv
P.4 0.4
-0-4- 0-
000.4
0z
+ ± + + +
O co
C)00cli
010 C10i 0-1
C.
0 0 0 0 0 010 1F (0 00 O~
to o- ovo01 01 01 01 01
v (0 1Cto 00Cl Cl NC 010
v
00000 0 0 0 0 00 000000 010toC)t 0 0 00 0(0 t- (0 0m 10 t~- t- (0 (0 (0 1- (.0
) Q p0, ) 0 ) 00 Z > Z Z Z00 0 0 0 00z z ~ zz z <C
0O - 0 00_ Cl co 'It Co
0.4 (L Q 01)> 0 0 0 0
z z zO
0 0O 0(0 -
0 C0
0 0-o t- 1 10_CO 10 (c t4 t 01 sr
m 1c t- 00 -- 01C CO I'_- -_ _ _ _
z 0rA C.)
0
z1=
.^.
CdC
>
O Q)
o "0
_ Q
CCU>
Cd Q) Cdc
>. Lo
0^ -
b b4
0 r 0
0 b
Z C)
< >. = C
u"0
> ~0
. d>.r
i>b4 ° '1u0 Cd
0 0
.Q o -b1X
0 - 0"40" 04
a) 0~
C. > >
.Q X,Q,,,u
.4 . .
0"=< F
1050 M. Akhtar, M. Shenasa, and D. H. Schmidt
> .z
C C
C)100: s
;>4
>4eco> co
P0C r.
0
r
1.4
3c0tos
* t
*--EO~cu)
rt3Qr1
-..I
024z
0
Q( 0_ _._
C0
E .4>I coE .t .Cd >q -
4 -E
x
CA
A B1
Vl_Al A1l A
RA .±.
HB 4-# 5 a .
HB_IVRB LA- . IIAJT.,!_'I__ -1l-l1-1 .1
A
V2A2-180 H
V2H2N170 h
H-RBa3V2RB2.180 F
n-i I_L 1-1!_,
/~~~~~~A Ae Ae
~~~.1~ ~ ~ i
h~~~VA-8 Ae H AeV9;
tB --60 X310,,W44u49fr 4
c
A2 V2A2.180V, 1 V21H2'190
"H-t-t_g*xr hRB2 V R 200 j~~~~ II-2301A
Dm _w__~~~~~A.~
o RK _ _~~~~A---
.UI ,C'*11 III
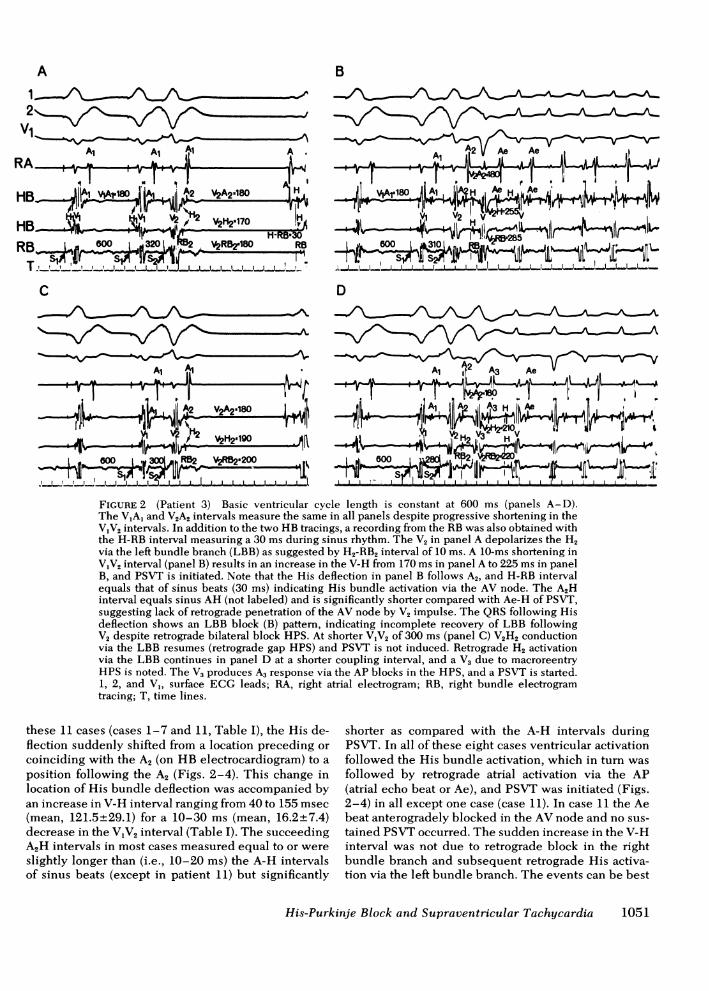
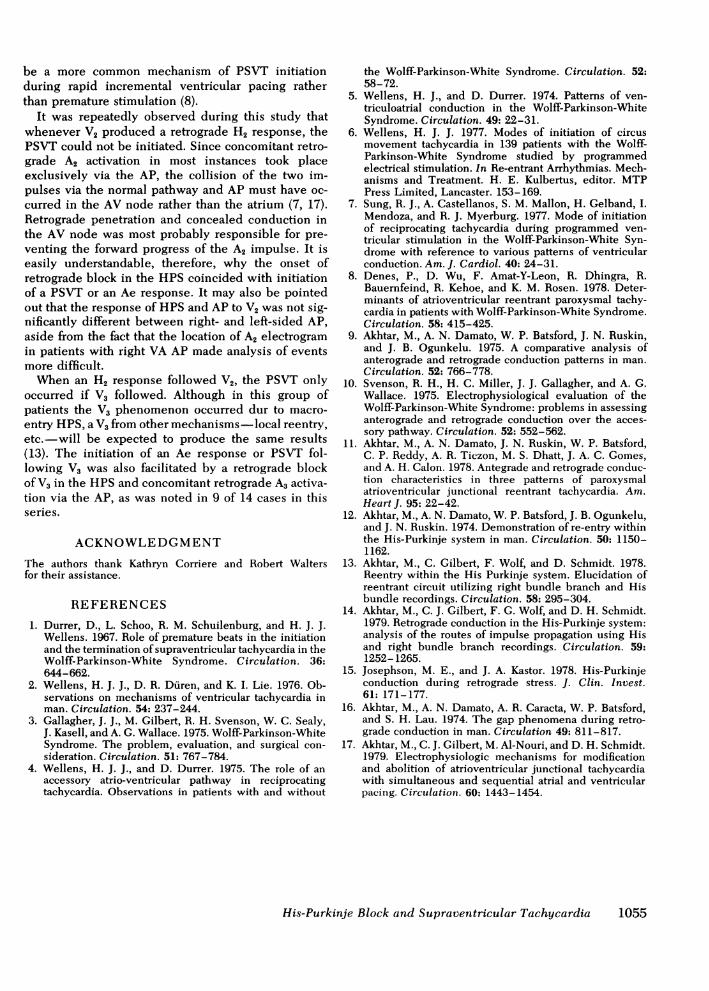
.,7FIGURE 2 (Patient 3) Basic ventricular cycle length is constant at 600 ms (panels A-D).The VIA, and V2A2 intervals measure the same in all panels despite progressive shortening in theV1V2 intervals. In addition to the two HB tracings, a recording from the RBwas also obtained withthe H-RB interval measuring a 30 ms during sinus rhythm. The V2 in panel A depolarizes the H2via the left bundle branch (LBB) as suggested by H2-RB2 interval of 10 ms. A 10-ms shortening inV1V2 interval (panel B) results in an increase in the V-H from 170 ms in panel A to 225 ms in panelB, and PSVT is initiated. Note that the His deflection in panel B follows A2, and H-RB intervalequals that of sinus beats (30 ms) indicating His bundle activation via the AV node. The A2Hinterval equals sinus AH (not labeled) and is significantly shorter compared with Ae-H of PSVT,suggesting lack of retrograde penetration of the AV node by V2 impulse. The QRSfollowing Hisdeflection shows an LBB block (B) pattern, indicating incomplete recovery of LBB followingV2 despite retrograde bilateral block HPS. At shorter V1V2 of 300 ms (panel C) V2H2 conductionvia the LBB resumes (retrograde gap HPS) and PSVT is not induced. Retrograde H2 activationvia the LBB continues in panel D at a shorter coupling interval, and a V3 due to macroreentryHPS is noted. The V3 produces A3 response via the AP blocks in the HPS, and a PSVT is started.1, 2, and V1, surface ECG leads; RA, right atrial electrogram; RB, right bundle electrogramtracing; T, time lines.
these 11 cases (cases 1-7 and 11, Table I), the His de-flection suddenly shifted from a location preceding orcoinciding with the A2 (on HB electrocardiogram) to aposition following the A2 (Figs. 2-4). This change inlocation of His bundle deflection was accompanied byan increase in V-H interval ranging from 40 to 155 msec(mean, 121.5+29.1) for a 10-30 ms (mean, 16.2+7.4)decrease in the V1V2 interval (Table I). The succeedingA2H intervals in most cases measured equal to or wereslightly longer than (i.e., 10-20 ms) the A-H intervalsof sinus beats (except in patient 11) but significantly
shorter as compared with the A-H intervals duringPSVT. In all of these eight cases ventricular activationfollowed the His bundle activation, which in turn wasfollowed by retrograde atrial activation via the AP(atrial echo beat or Ae), and PSVTwas initiated (Figs.2-4) in all except one case (case 11). In case 11 the Aebeat anterogradely blocked in the AVnode and no sus-tained PSVToccurred. The sudden increase in the V-Hinterval was not due to retrograde block in the rightbundle branch and subsequent retrograde His activa-tion via the left bundle branch. The events can be best
His-Purkinje Block and Supraventricular Tachycardia 1051
A
2
RA .- --I -- , .l2l 2|r< v5A'AA233JIb IAIb IV A2b
V1 l,A2 -33CAHB T I. -.i,I .
RV !I
C
550 1'_330 V2H2-110
it H-V-45
11# 550 r, .F, V2H29155i' SiY S2WSi'' S29'
*PA1A2.3OV AT V A"'",ft ,
O^ Ae -VAe' v
_ -1 k- Ii_-II#; -I-. -Tra-fX*19 TXl*-vsww riA1A2'300.1 Al1\V2 Ae V Ae
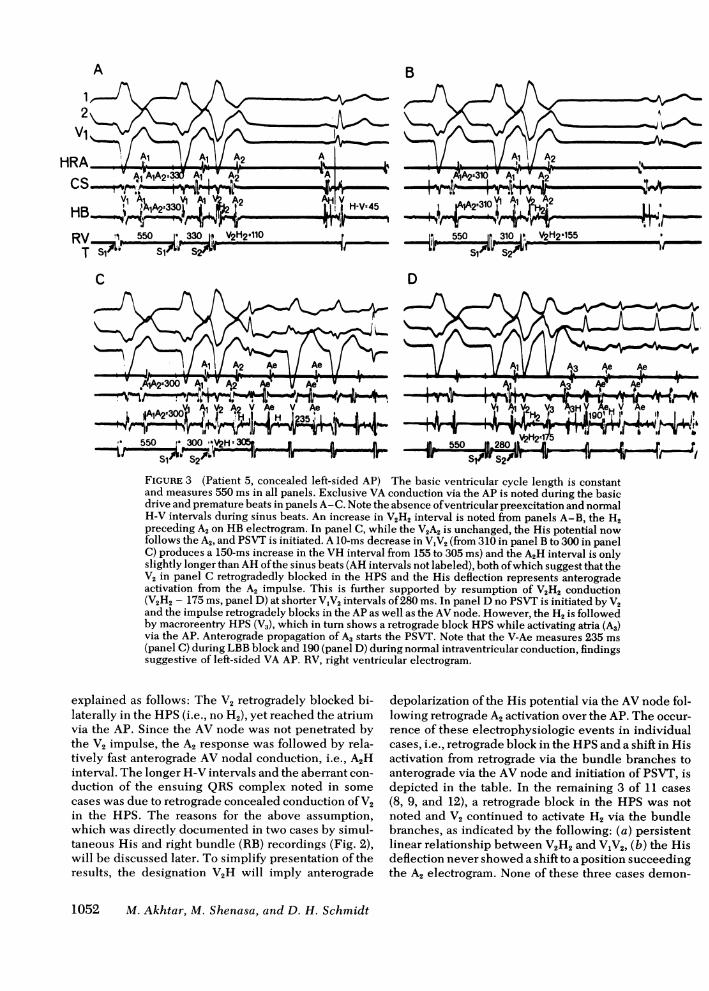
.550.300 H 5509~~~~~ ~~~-AFIGURE 3 (Patient 5, concealed left-sided AP) The basic ventricular cycle length is constantand measures 550 ms in all panels. Exclusive VA conduction via the AP is noted during the basicdrive and premature beats in panels A-C. Note the absence of ventricular preexcitation and normalH-V intervals during sinus beats. An increase in V2H2 interval is noted from panels A-B, the H2preceding A2 on HBelectrogram. In panel C, while the V2A2 is unchanged, the His potential nowfollows the A2, and PSVT is initiated. A 10-ms decrease in V1V2 (from 310 in panel B to 300 in panelC) produces a 150-ms increase in the VH interval from 155 to 305 ms) and the A2H interval is onlyslightly longer than AHof the sinus beats (AH intervals not labeled), both of which suggest that theV2 in panel C retrogradedly blocked in the HPS and the His deflection represents anterogradeactivation from the A2 impulse. This is further supported by resumption of V2H2 conduction(V2H2 - 175 ms, panel D) at shorter V1V2 intervals of 280 ms. In panel Dno PSVT is initiated by V2and the impulse retrogradely blocks in the APas well as the AVnode. However, the H2 is followedby macroreentry HPS (V3), which in turn shows a retrograde block HPSwhile activating atria (A3)via the AP. Anterograde propagation of A3 starts the PSVT. Note that the V-Ae measures 235 ms(panel C) during LBB block and 190 (panel D) during normal intraventricular conduction, findingssuggestive of left-sided VA AP. RV, right ventricular electrogram.
explained as follows: The V2 retrogradely blocked bi-laterally in the HPS(i.e., no H2), yet reached the atriumvia the AP. Since the AV node was not penetrated bythe V2 impulse, the A2 response was followed by rela-tively fast anterograde AV nodal conduction, i.e., A2Hinterval. The longer H-V intervals and the aberrant con-
duction of the ensuing QRScomplex noted in some
cases was due to retrograde concealed conduction of V2in the HPS. The reasons for the above assumption,which was directly documented in two cases by simul-taneous His and right bundle (RB) recordings (Fig. 2),will be discussed later. To simplify presentation of theresults, the designation V2H will imply anterograde
depolarization of the His potential via the AVnode fol-lowing retrograde A2 activation over the AP. The occur-
rence of these electrophysiologic events in individualcases, i.e., retrograde block in the HPSand a shift in Hisactivation from retrograde via the bundle branches toanterograde via the AV node and initiation of PSVT, isdepicted in the table. In the remaining 3 of 11 cases(8, 9, and 12), a retrograde block in the HPS was notnoted and V2 continued to activate H2 via the bundlebranches, as indicated by the following: (a) persistentlinear relationship between V2H2 and V1V2, (b) the Hisdeflection never showed a shift to a position succeedingthe A2 electrogram. None of these three cases demon-
1052 M. Akhtar, M. Shenasa, and D. H. Schmidt
B
HI'A
'p
D
,_,~~~~~~%Nw1mL---AlL
- 4
AIi! A1. I? OIL
300 I-
275 I-
250 1-
225 I
200,ms)
175
ERP-VM
150 I-
125 I
100 F75
a V2A2 CS* V2A2 HBo V2 A2 HRA* V2H2 or V2HO PSVT with V2O PSVT with V3
inL--j~~~
block&..
gap retHPS blc
gapHIPS
250 275 300 325 350 375 400 425 450V1 V2 (m s)
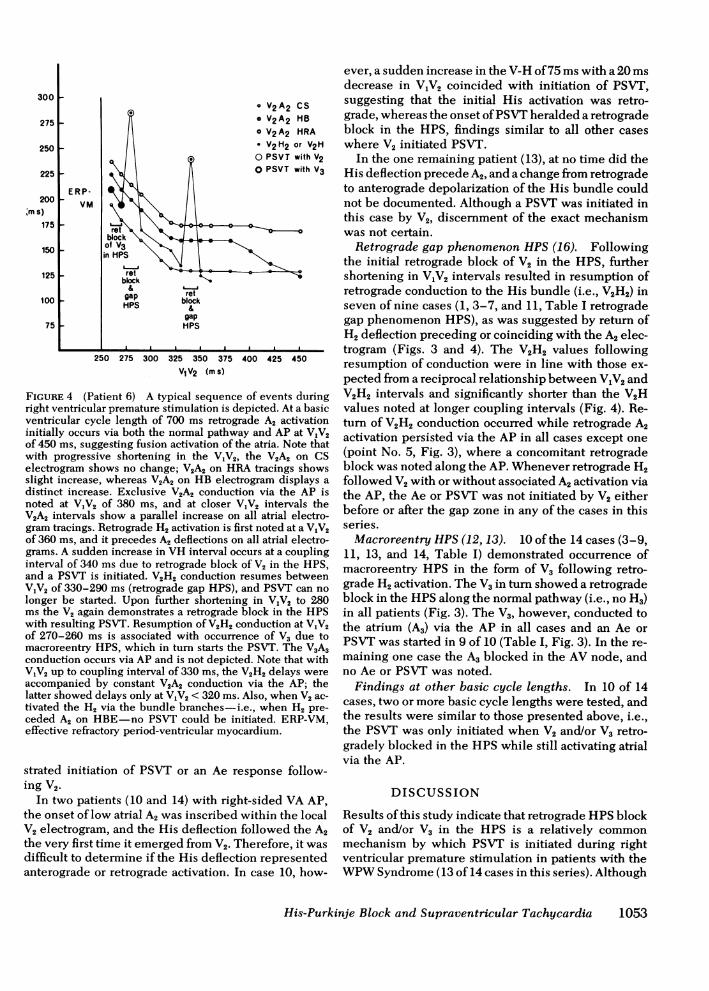
FIGURE 4 (Patient 6) A typical sequence of events duringright ventricular premature stimulation is depicted. At a basicventricular cycle length of 700 ms retrograde A2 activationinitially occurs via both the normal pathway and AP at V1V2of 450 ms, suggesting fusion activation of the atria. Note thatwith progressive shortening in the V,V2, the V2A2 on CSelectrogram shows no change; V2A2 on HRAtracings showsslight increase, whereas V2A2 on HB electrogram displays adistinct increase. Exclusive V2A2 conduction via the AP isnoted at V1V2 of 380 ms, and at closer V,V2 intervals theV2A2 intervals show a parallel increase on all atrial electro-gram tracings. Retrograde H2 activation is first noted at a V1V2of 360 ms, and it precedes A2 deflections on all atrial electro-grams. A sudden increase in VH interval occurs at a couplinginterval of 340 ms due to retrograde block of V2 in the HPS,and a PSVT is initiated. V2H2 conduction resumes betweenV1V2 of 330-290 ms (retrograde gap HPS), and PSVT can nolonger be started. Upon further shortening in V1V2 to 280ms the V2 again demonstrates a retrograde block in the HPSwith resulting PSVT. Resumption of V2H2 conduction at V1V2of 270-260 ms is associated with occurrence of V3 due tomacroreentry HPS, which in turn starts the PSVT. The V3A3conduction occurs via AP and is not depicted. Note that withV1V2 up to coupling interval of 330 ms, the V2H2 delays wereaccompanied by constant V2A2 conduction via the AP; thelatter showed delays only at V1V2 < 320 ms. Also, when V2 ac-tivated the H2 via the bundle branches-i.e., when H2 pre-ceded A2 on HBE-no PSVT could be initiated. ERP-VM,effective refractory period-ventricular myocardium.
strated initiation of PSVT or an Ae response follow-ing V2.
In two patients (10 and 14) with right-sided VA AP,the onset of low atrial A2 was inscribed within the localV2 electrogram, and the His deflection followed the A2the very first time it emerged from V2. Therefore, it wasdifficult to determine if the His deflection representedanterograde or retrograde activation. In case 10, how-
ever, a sudden increase in the V-H of 75 ms with a 20 msdecrease in V1V2 coincided with initiation of PSVT,suggesting that the initial His activation was retro-grade, whereas the onset of PSVTheralded a retrogradeblock in the HPS, findings similar to all other caseswhere V2 initiated PSVT.
In the one remaining patient (13), at no time did theHis deflection precede A2, and a change from retrogradeto anterograde depolarization of the His bundle couldnot be documented. Although a PSVT was initiated inthis case by V2, discernment of the exact mechanismwas not certain.
Retrograde gap phenomenon HPS (16). Followingthe initial retrograde block of V2 in the HPS, furthershortening in VjV2 intervals resulted in resumption ofretrograde conduction to the His bundle (i.e., V2H2) inseven of nine cases (1, 3-7, and 11, Table I retrogradegap phenomenon HPS), as was suggested by return ofH2 deflection preceding or coinciding with the A2 elec-trogram (Figs. 3 and 4). The V2H2 values followingresumption of conduction were in line with those ex-pected from a reciprocal relationship between V1V2 andV2H2 intervals and significantly shorter than the V2Hvalues noted at longer coupling intervals (Fig. 4). Re-turn of V2H2 conduction occurred while retrograde A2activation persisted via the AP in all cases except one(point No. 5, Fig. 3), where a concomitant retrogradeblock was noted along the AP. Whenever retrograde H2followed V2 with or without associated A2 activation viathe AP, the Ae or PSVT was not initiated by V2 eitherbefore or after the gap zone in any of the cases in thisseries.
Macroreentry HPS(12, 13). 10 of the 14 cases (3-9,11, 13, and 14, Table I) demonstrated occurrence ofmacroreentry HPS in the form of V3 following retro-grade H2 activation. The V3 in turn showed a retrogradeblock in the HPSalong the normal pathway (i.e., no H3)in all patients (Fig. 3). The V3, however, conducted tothe atrium (A3) via the AP in all cases and an Ae orPSVTwas started in 9 of 10 (Table I, Fig. 3). In the re-maining one case the A3 blocked in the AV node, andno Ae or PSVTwas noted.
Findings at other basic cycle lengths. In 10 of 14cases, two or more basic cycle lengths were tested, andthe results were similar to those presented above, i.e.,the PSVT was only initiated when V2 and/or V3 retro-gradely blocked in the HPSwhile still activating atrialvia the AP.
DISCUSSION
Results of this study indicate that retrograde HPSblockof V2 and/or V3 in the HPS is a relatively commonmechanism by which PSVT is initiated during rightventricular premature stimulation in patients with theWPWSyndrome (13 of 14 cases in this series). Although
His-Purkinje Block and Supraventricular Tachycardia 1053

the induced V2 may initiate PSVT by other mecha-nisms, present data suggest that other mechanisms areless commonly responsible for PSVT initiation duringventricular premature stimulation. In a series with 139cases of WPWSyndrome reported by Wellens (6) it wasnoted that, during ventricular premature stimulation,a PSVT was most commonly initiated when V2 retro-gradely blocked along the normal pathway (30 of 139cases) or by V3 (9 of 139 cases) when the latter wasinducible, and by other mechanisms in only 11 of 139cases. The exact site of retrograde block (HPS vs. AVnode) of V2 or V3 was not demonstrated, and it cannotbe stated with certainty whether the findings in the re-port by Wellens and the present study are comparable.A recent study showed that in patients with ventricularpreexcitation, programmed ventricular extrastimuli didnot initiate PSVT if there was no VA conduction andthere was persistent retrograde atrial fusion activationvia both the APand normal pathway (7). A narrow QRSPSVT could be elicited with V2 when VA conductionwas intact, V2A2 conduction occurred exclusively viathe AP, and normal pathway was less deeply pene-trated (7). In that report it was indicated, however,that the level or site of retrograde block along the nor-mal pathway could not be determined.
Regular narrow QRS complex PSVT is the mostcommon arrhythmia elicited by programmed atrial aswell as ventricular premature stimulation in patientswith the WPWSyndrome (3, 4). During prematureatrial stimulation (A2), the premature impulse blocks inthe AP, activates the ventricles over the AVnode-HPS,and returns to the atria via the AP to start the PSVT.Induction of the same PSVTwith V2, on the other hand,will be more likely if V2A2 conduction occurred via theAPand subsequent anterograde propagation took placealong the AV node-HPS. The latter occurrence willobviously be facilitated by a retrograde block of V2 inthe normal pathway. A retrograde block of V2 abovethe His bundle (AV node), however, may not permitinitiation of PSVTeven if accompanied by concomitantretrograde A2 activation via the AP, because of effect ofretrograde concealed conduction in the AV node.Under the following circumstances, however, V2 maystart PSVT despite AV nodal penetration (a) whenV2 produces only a partial penetration of the AV nodewith resultant rapid recovery of excitability, (b)initiates intranodal reciprocation, (c) conducts withlong V2A2 via AP sufficient to allow recovery of AVnodal excitability. A retrograde block of V2 in the HPS,on the other hand, would permit unhindered progressof A2 impulse through the AV node, since the priorAV nodal depolarization is during the last V,.
A support for the preceding hypothesis is provided inthe present study by demonstration that the PSVTinitiation did coincide with the occurrence of retro-
grade block of V2 in the HPS. That the site of retro-grade block of V2 was indeed in the HPS rather thanthe AV node is suggested by the following obser-vations: (A) A sudden increase in the V-H values (amean increase of 121.8 ms from V2H2 to V2H, for a16.2 ms mean decrease) in V1V2 intervals, a behaviorunlike that of retrograde H2 activation via the bundlebranches and therefore suggesting a shift from retro-grade to anterograde activation of the His bundle (Figs.2-4). (B) A return of H2 deflection at shorter V1V2,producing V2H2 values less than V2H values (retro-grade gap phenomenon HPS) noted at longer V1V2,and concomitant abolition of PSVT (Figs. 3 and 4). (C)Direct demonstration of the shift from a retrograde toanterograde activation of the His bundle when both Hisand RB recordings were available (two cases, Fig. 2).(D) The occurrence of macroreentry HPS after retro-grade H2 activation and its disappearance despitelonger V-H intervals, coinciding with the shift of Hisdeflection to a location succeeding the A2 (Fig. 3). (E)A consistent relationship between the A2 and thesucceeding His deflection with values approximatingthe sinus A-H values. This suggests that the occurrenceof His deflection after A2 was not an independentphenomenon (retrograde via bundle branches) but itsoccurrence was directly related to and in fact de-pendent upon the preceding A2 activation (Figs. 2and 3).
It seems reasonable to conclude, therefore, that theHis deflection following the A2 was due to anterogradedepolarization via the AV node. Despite the abovereasoning, questions can be raised as to whether the V2might still have blocked in the AV node rather thanHPS, and whether the H2 deflection was either notidentifiable for some reason or was obscured by thelocal V2 electrogram. These questions can be dismissedfor the following reasons: (a) Once the retrograde H2deflection emerges, the V2H2 intervals generallylengthen (rather than shorten) at shorter V1V2 (9, 12, 14,15). (b) The occurrence of gap phenomenon in mostcases suggests retrograde H2 was recordable when-ever the His bundle was depolarized. (c) At the V2Hinterval ranges noted in these cases, the His bundleactivation will have to occur twice (first retrogradelyand then anterogradely) within a period of 300 ms, anunlikely occurrence. In the event the V2 retrogradelypenetrates the AV node, the subsequent A2H inter-vals will be expected to be much longer than thesinus beats (retrograde concealed conduction in theAV node). Such a mechanism of PSVT initiation wasnot noted in the present series but has been pre-viously described, and may operate more frequentlyat shorter cycle lengths due to abbreviation in therefractoriness of the His. For similar reasons a retro-grade AV nodal block of ventricular impulse may also
1054 M. Akhtar, M. Shenasa, and D. H. Schmidt
be a more common mechanism of PSVT initiationduring rapid incremental ventricular pacing ratherthan premature stimulation (8).
It was repeatedly observed during this study thatwhenever V2 produced a retrograde H2 response, thePSVT could not be initiated. Since concomitant retro-grade A2 activation in most instances took placeexclusively via the AP, the collision of the two im-pulses via the normal pathway and AP must have oc-curred in the AV node rather than the atrium (7, 17).Retrograde penetration and concealed conduction inthe AV node was most probably responsible for pre-venting the forward progress of the A2 impulse. It iseasily understandable, therefore, why the onset ofretrograde block in the HPS coincided with initiationof a PSVT or an Ae response. It may also be pointedout that the response of HPSand AP to V2 was not sig-nificantly different between right- and left-sided AP,aside from the fact that the location of A2 electrogramin patients with right VA AP made analysis of eventsmore difficult.
When an H2 response followed V2, the PSVT onlyoccurred if V3 followed. Although in this group ofpatients the V3 phenomenon occurred dur to macro-entry HPS, a V3 from other mechanisms-local reentry,etc.-will be expected to produce the same results(13). The initiation of an Ae response or PSVT fol-lowing V3 was also facilitated by a retrograde blockof V3 in the HPSand concomitant retrograde A3 activa-tion via the AP, as was noted in 9 of 14 cases in thisseries.
ACKNOWLEDGMENT
The authors thank Kathryn Corriere and Robert Waltersfor their assistance.
REFERENCES
1. Durrer, D., L. Schoo, R. M. Schuilenburg, and H. J. J.Wellens. 1967. Role of premature beats in the initiationand the termination of supraventricular tachycardia in theWolff-Parkinson-White Syndrome. Circulation. 36:644-662.
2. Wellens, H. J. J., D. R. Duren, and K. I. Lie. 1976. Ob-servations on mechanisms of ventricular tachycardia inman. Circulation. 54: 237-244.
3. Gallagher, J. J., M. Gilbert, R. H. Svenson, W. C. Sealy,J. Kasell, and A. G. Wallace. 1975. Wolff-Parkinson-WhiteSyndrome. The problem, evaluation, and surgical con-sideration. Circulation. 51: 767-784.
4. Wellens, H. J. J., and D. Durrer. 1975. The role of anaccessory atrio-ventricular pathway in reciprocatingtachycardia. Observations in patients with and without
the Wolff-Parkinson-White Syndrome. Circulation. 52:58-72.
5. Wellens, H. J., and D. Durrer. 1974. Patterns of ven-triculoatrial conduction in the Wolff-Parkinson-WhiteSyndrome. Circulation. 49: 22-31.
6. Wellens, H. J. J. 1977. Modes of initiation of circusmovement tachycardia in 139 patients with the Wolff-Parkinson-White Syndrome studied by programmedelectrical stimulation. In Re-entrant Arrhythmias. Mech-anisms and Treatment. H. E. Kulbertus, editor. MTPPress Limited, Lancaster. 153-169.
7. Sung, R. J., A. Castellanos, S. M. Mallon, H. Gelband, I.Mendoza, and R. J. Myerburg. 1977. Mode of initiationof reciprocating tachycardia during programmed ven-tricular stimulation in the Wolff-Parkinson-White Syn-drome with reference to various patterns of ventricularconduction. Am. J. Cardiol. 40: 24-31.
8. Denes, P., D. Wu, F. Amat-Y-Leon, R. Dhingra, R.Bauernfeind, R. Kehoe, and K. M. Rosen. 1978. Deter-minants of atrioventricular reentrant paroxysmal tachy-cardia in patients with Wolff-Parkinson-White Syndrome.Circulation. 58: 415-425.
9. Akhtar, M., A. N. Damato, W. P. Batsford, J. N. Ruskin,and J. B. Ogunkelu. 1975. A comparative analysis ofanterograde and retrograde conduction patterns in man.Circulation. 52: 766-778.
10. Svenson, R. H., H. C. Miller, J. J. Gallagher, and A. G.Wallace. 1975. Electrophysiological evaluation of theWolff-Parkinson-White Syndrome: problems in assessinganterograde and retrograde conduction over the acces-sory pathway. Circulation. 52: 552-562.
11. Akhtar, M., A. N. Damato, J. N. Ruskin, W. P. Batsford,C. P. Reddy, A. R. Ticzon, M. S. Dhatt, J. A. C. Gomes,and A. H. Calon. 1978. Antegrade and retrograde conduc-tion characteristics in three patterns of paroxysmalatrioventricular junctional reentrant tachycardia. Am.Heart J. 95: 22-42.
12. Akhtar, M., A. N. Damato, W. P. Batsford, J. B. Ogunkelu,and J. N. Ruskin. 1974. Demonstration of re-entry withinthe His-Purkinje system in man. Circulation. 50: 1150-1162.
13. Akhtar, M., C. Gilbert, F. Wolf, and D. Schmidt. 1978.Reentry within the His Purkinje system. Elucidation ofreentrant circuit utilizing right bundle branch and Hisbundle recordings. Circulation. 58: 295-304.
14. Akhtar, M., C. J. Gilbert, F. G. Wolf, and D. H. Schmidt.1979. Retrograde conduction in the His-Purkinje system:analysis of the routes of impulse propagation using Hisand right bundle branch recordings. Circulation. 59:1252-1265.
15. Josephson, M. E., and J. A. Kastor. 1978. His-Purkinjeconduction during retrograde stress. J. Clin. Invest.61: 171-177.
16. Akhtar, M., A. N. Damato, A. R. Caracta, W. P. Batsford,and S. H. Lau. 1974. The gap phenomena during retro-grade conduction in man. Circulation 49: 811-817.
17. Akhtar, M., C. J. Gilbert, M. Al-Nouri, and D. H. Schmidt.1979. Electrophysiologic mechanisms for modificationand abolition of atrioventricular junctional tachycardiawith simultaneous and sequential atrial and ventricularpacing. Circulation. 60: 1443-1454.
His-Purkinje Block and Supraventricular Tachycardia 1055