root cause analysis (rca) - american … cause analysis (rca) • retrospective analysis •...
TRANSCRIPT

Root Cause Analysis (RCA)
Grace Gwe-Ya Kim, Ph.D.

Learning Objectives - RCA
• To understand the basics of Root Cause Analysis (RCA)
• To learn about the techniques to implement RCA
• To be able to analyze the causes and contributing factors for an incident

Outline - RCA
• Definitions
• Description & Tenet / Overview
• Background
• Conducting an RCA
• Example

Operational Definitions - RCA• Sentinel event – an unexpected occurrence
involving death or serious physical or psychological injury, or risk thereof
• Error – failure to complete a planned action as intended or the use of an incorrect plan of action to achieve a given aim.
• Near miss – an event or situation that could have resulted in an accident, injury or illness but did not either by chance or through timely intervention. Also known as a close call, good catch or near hit.

Operational Definitions - RCA• Safety Culture – the shared commitment of
leadership, management and employees to ensure the safety of the work environment [for staff and patients]
• Active error – error that occurs at the point of human interface with a complex system
• Latent error – errors due to failures of system design

Root Cause Analysis (RCA)• Retrospective analysis• Serious, adverse events (and near misses)
with rare occurrences• Identify underlying problems that increase
likelihood errors• RCA is a “systems analysis”
– Examine relationships between different layers & other aspects of systems design
• Impartial analysis (Culture of Safety)

Human RootsInappropriate Human intervention
Physical RootsSymptoms
Latent RootsDeficiencies in Process
Failure of Analysis
“Witch Hunting”
RCA
Three Levels of Root Cause
Muhamed Faizal Mohd Karin, 5 Whys Analysis, Leanapplied.com, Oct. 2012
Causes from all of these areas are important in RCA

Background - RCA• Originated in engineering (1960s)
– Rare error events (e.g., industrial, airline accidents)• Industrial psychology & human factors engineering
RCA Approaches (“Schools”)
Field(s) or Scope
Production-based ManufacturingProcess-based Expanded to include business processesFailure-based Engineering
MaintenanceSafety-based Accident analysis
Occupational Safety & HealthSystems-based Amalgamation - adds in change
management, risk management & systems analysis

Background - RCA• Healthcare
– TJC sentinel event standards 1999• RCA and corrective action plan is expected• Encourage but not require self-reporting
– U.S. Department of Veterans Affairs (VA) Administration National Center for Patient Safety (NCPS) (est. 1999)
• RCA process required for VA radiotherapy medical events; findings shared as “lessons”

RCA Overview
1. Collect information (What happed?)
2. Identify causes (Why it happened?)
3. Recommendations for remediation
4. Implement and Monitor

RCA Step 1: What happened?
• Focus on “what” rather than “why”- A narrative can be helpful
• Helpful tools- Process Mapping- Ask questions and listen
- Let the interviewee ‘connect the dots’

RCA Step 2: Why it happened?
• Identify causes– Focus on the “whys”
• Helpful tools– Brainstorming– 5-Whys: force and in-depth analysis– Cause & Effect (Fishbone) Diagram

Brainstorming• A method for a group of people
to generate a large number of ideas in a short period of time
• Designate a note taker & moderator (separate people)
• Start with a statement of the problem
• No bad ideas, all ideas recorded– Criticizing or discussing the ideas is
not allowed

The 5 Whys• Simple procedure of asking
‘why’ 4 or 5 times as to the cause of an error or near-miss to force an in-depth analysis
• At each successive ‘why’ question, the group probes deeper
• Results are recorded for use in the RCA

Cause & Effect Diagram
Start of event Error
Reason #1
#1.2
#1.1
Reason #2
#2.2
#2.1
Reason #3
#1.2
.1
#3.1
aka: Ishikawa or Fishbone Diagram
#1.1
.1#1.1.1.1

RCA Step 3: Recommendations• Requires domain experts
• Low cost, high impact• Focus on sphere of influence• Cost-benefit analysis
• Examples– Checklists– No interruption zone– Time out– Intuition Cost
Impa
ct
A
BC
Outside of your control
/influence
What you can
influence
What you can control

RCA Step 4: Implement & Monitoring• Monitoring System
- National reporting system: RO-ILS
- Department reporting system
• For a RCA to be useful it has to encompass: - Corrective Actions- Learning- Follow-up

When to conduct an RCA• Any single obviously serious event
– Federal or state level investigation– Institutional level investigation– Departmental level investigation
• Systematic events– Equipment failure, process failure, etc.
• High frequency sporadic events- Human error, etc.

Other Analysis Techniques• Re-enactment (people, computer
simulation)
• Re-construction (reassemble debris for clues)
• Barrier analysis (process industries)
• Bayesian inference

Other Analysis Techniques• Failure mode and effects analysis (FMEA)
• Fault tree analysis (FTA)
• Why-because analysis
• Pareto analysis (“80/20 rule”)
• RPR Problem Diagnosis (IT)

RCA – Key to Success
• Leadership & involved persons participation
• Internally consistent
• Consider relevant literature, experience
• Investigate soon after incident

RCA Systems• US RCA Approach
– U.S. Department of Veterans Affairs (VA) National Center for Patient Safety (NCPS)
http://www.patientsafety.va.gov/professionals/publications/handbook.asp
• UK RCA Approachhttp://www.nrls.npsa.nhs.uk/resources/collections/root-cause-analysis/
• Canadian RCA Approachhttp://www.patientsafetyinstitute.ca/English/toolsResources/IncidentAnalysis/Pages/Tools.aspx

• Event Reported
Example - Event Reported
You are the agent for the chipmunks
First time or recurrent?
Awesome StudioStudio A
Incident
Chipmunks were out of control and injured
Agent

What Happened
https://www.youtube.com/watch?v=CvfINIM87iI

• Narrative• In the recording studio, the chipmunks were
tired so they couldn’t sing• Manager decided to give them coffee• Manager brought the large coffee with
caramel and whip cream.• Chipmunks finished the coffee• Chipmunks were out of control and injured
after drinking coffee
RCA Step 1: What happened?

• Process Map
RCA Step 1: What happened?
Chipmunks were tired with cont. recording
Manager decided to give them
coffee
Manager brought coffee
Chipmunks finished coffee
Chipmunks were out of control and
injured
Incident

• The 5 Whys
RCA Step 2: Why it happened?
Q1. Why were the Chipmunks out of control and injured?A1. They drank coffee
Q2. Why did they drink coffee?A2. The manager asked them to
Q3. Why did the manager ask the to drink coffee?A3. So they could keep recording
Q4. Why did they need to keep recording?A4. They only had the studio for one more hour

Cause & Effect Diagram
Studio singing
Chipmunk injured
Drank coffee
LOVE coffee
Manager asked
Kid
s lo
ve
swee
t stu
ff
aka: Ishikawa or Fishbone Diagram
To k
eep
reco
rdin
g
Limited record time
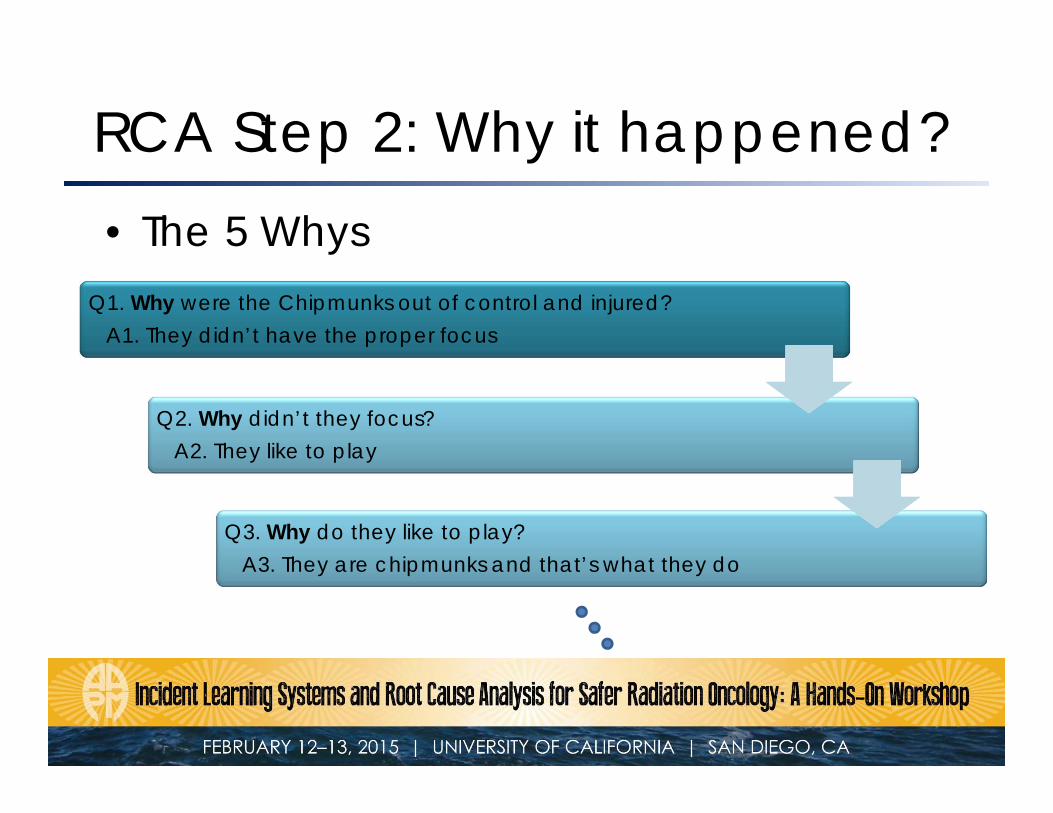
• The 5 Whys
RCA Step 2: Why it happened?
Q1. Why were the Chipmunks out of control and injured?A1. They didn’t have the proper focus
Q2. Why didn’t they focus?A2. They like to play
Q3. Why do they like to play?A3. They are chipmunks and that’s what they do

Cause & Effect Diagram
Studio singing
Chipmunk injured
No focus
That’s what they do
Like to play
Reason #3
#3.1
aka: Ishikawa or Fishbone Diagram
Drank coffee
LOVE coffee
Manager asked
Kid
s lo
ve
swee
t stu
ff
To k
eep
reco
rdin
g
Limited record time

• Don’t record chipmunks any longer• Don’t give chipmunks coffee
– What if chipmunks LOVE coffee?
• Recommend a new manager that better understands chipmunks – not ideal (no direct control, only a recommendation (weak))
• Work in padded recording studio• Make sure there is enough recording time for breaks• Order small coffee / decaf only?• Make sure chipmunks play before recording
RCA Step 3: Recommendations

• Choose and always use the proper size cup for Chipmunks
• Give play time before recording
• Keep tracking record time and break time
RCA Step 4: Implement & Monitoring

1. Which statement is true for the RCA?
20%
20%
20%
20%
20% 1. It is a prospective analysis2. It is systems analysis3. It focuses on high occurrence events4. It determines incident severity5. It identifies potential failure modes
10
Answer: 2. It is systems analysisRef ) Towards Safer Radiotherapy, BIR/IPEM/NPSA/SCR/RCR, The Royal College of Radiologists, 2008

2. Which technique is not used for RCA?
20%
20%
20%
20%
20% 1. Cause & Effect Diagram2. Re-construction3. Barrier Analysis4. 5 Whys5. FMEA
10
Answer: 5. FMEARef ) Duke Okes, Root Cause Analysis (The Core of Problem Solving and Corrective Action), ASQ Quality Press, 2009

3. When do we stop asking Why?
20%
20%
20%
20%
20%1. After identification of direct cause2. After asking Why 5 times3. After identification of 5th symptom4. After identification of actionable root cause5. After 5 process steps
10
Answer: 4. After identification of actionable root cause
Ref ) Michael L. George, John Maxey, The Lean Six Sigma Pocket Toolbook