root fracture in primary teeth - jdor journal 12 issue 1 2016/7_prahlad.pdfroot fracture in primary...
TRANSCRIPT
Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 33
CASE REPORT
ROOT FRACTURE IN PRIMARY TEETH Prahlad.Gadicherla1*, M. Mala Devi2,
*Corresponding Author Email: [email protected]
Contributors:
1,Reader, Department of
Pedodontics & Preventive
Dentistry,Faculty of Dental
Sciences,M.S.Ramaiah University
of Applied Sciences, Bangalore-54.
2,P.G.Student, , Department of
Pedodontics & Preventive
Dentistry,Faculty of Dental
Sciences,M.S.Ramaiah University
of Applied Sciences, Bangalore-54.
.
ABSTRACT
Dental traumatic injuries are not uncommon in children. When addressing
problems involved with trauma to the primary dentition, we as Pediatric dentist not
only have the responsibility of only looking in to the trauma to tooth but also to
comfort the child and parents in the acute state, to avoid inducing dental fear and
anxiety in young children who may be experiencing their first dental problem, and
to minimize the risk of further damage to the permanent teeth. We present a case of
3.5 year old reported to our OPD experiencing pain in her maxillary central incisors
following traumatic injury after a fall.
Keywords: primary incisor, root fracture, diagnostic dilemma
INTRODUCTION
Radicular fracture involves dentin, cementum and pulp
that may be present either in the radicular apparatus only
or involves coronal portion of the tooth (crown root
fracture). Maxillary central incisors are more commonly
involved with incidence reported being 80% in the
permanent dentition 1. These sorts of root fractures are
relatively uncommon among dental traumas, comprising
0.5–7% of the injuries affecting the permanent dentition
where as in the primary dentition, root fractures are as rare
as about 2–4%, due to the plasticity of the developing
alveolar bone 2.
The occurrence of root fracture is most frequent at the age
of 3–4 years where physiologic root resorption has begun,
thereby weakening the root 1. Diagnosis of root fractures
always presents a formidable challenge for the clinicians
because most of the root fractures remain asymptomatic.
A young child is often difficult to examine and treat due
to lack of co-operation because of fear. The situation is
distressing to both the parent and the child. A child’s
maturity and ability to cope with the emergency situation,
the time for shedding of the injured tooth and the
occlusion, are all important factors that influence
treatment 3.
CASE REPORT:
A 3.5-year-old girl reported to the out-patient
Department of Pedodontics and Preventive Dentistry,
Faculty of Dental Sciences, M S Ramaiah University of
Applied Sciences, Bangalore, with the chief complaint of
a broken tooth in upper front tooth region since three days.
Medical history and Dental history was nothing in
particular. Childs’ father gave the history of fall while
playing 2 days back and the tooth got fractured. The child
was conscious with no signs of vomiting or any change in
behaviour. The child started having pain after a day in that
fractured tooth and the pain was not relieved in any
medication.
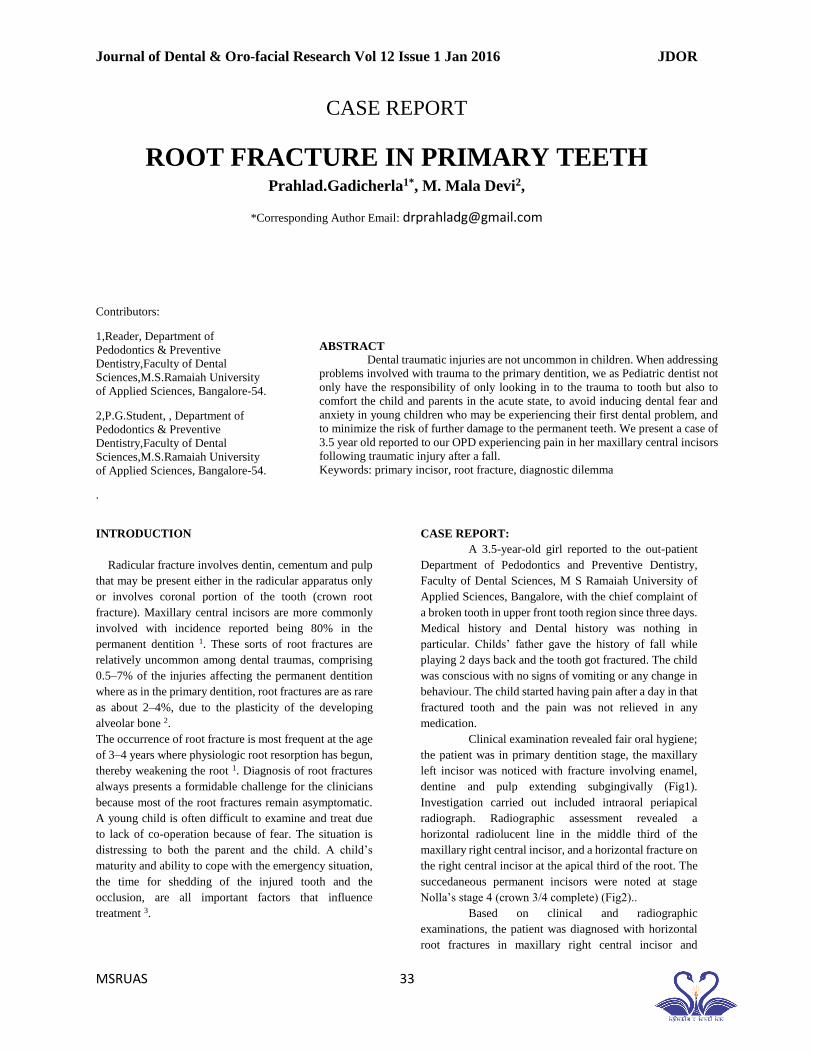
Clinical examination revealed fair oral hygiene;
the patient was in primary dentition stage, the maxillary
left incisor was noticed with fracture involving enamel,
dentine and pulp extending subgingivally (Fig1).
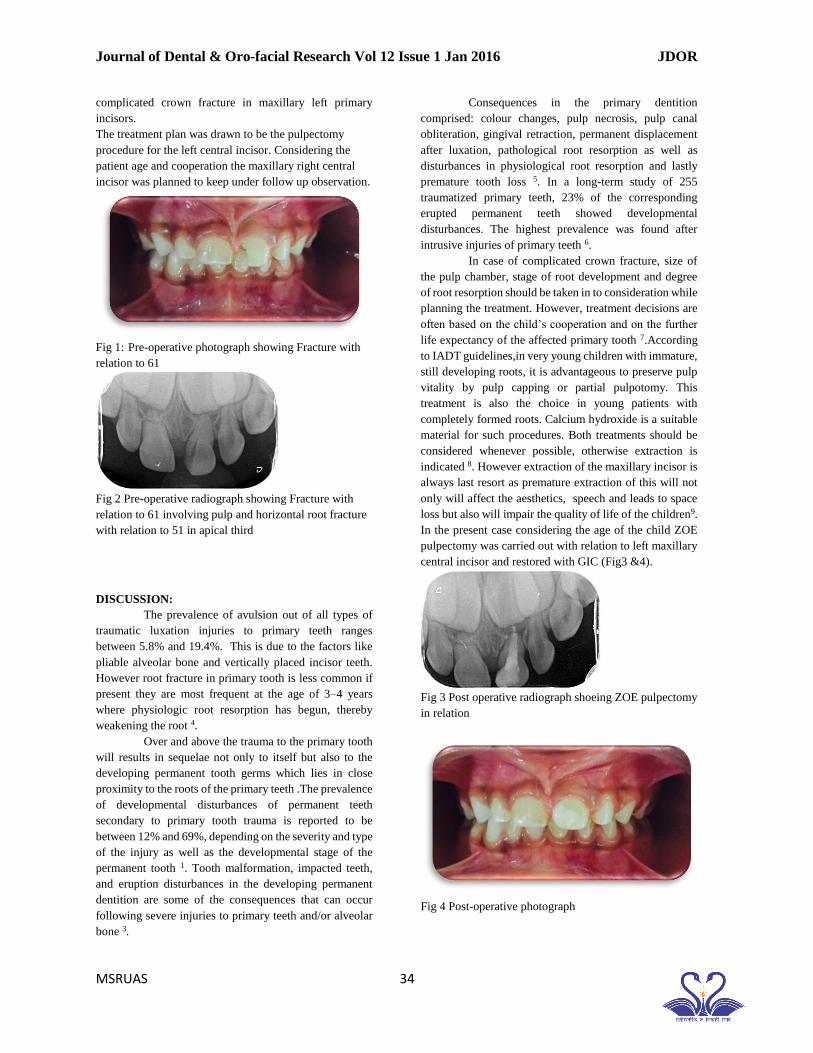
Investigation carried out included intraoral periapical
radiograph. Radiographic assessment revealed a
horizontal radiolucent line in the middle third of the
maxillary right central incisor, and a horizontal fracture on
the right central incisor at the apical third of the root. The
succedaneous permanent incisors were noted at stage
Nolla’s stage 4 (crown 3/4 complete) (Fig2)..
Based on clinical and radiographic
examinations, the patient was diagnosed with horizontal
root fractures in maxillary right central incisor and
Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 34
complicated crown fracture in maxillary left primary
incisors.
The treatment plan was drawn to be the pulpectomy
procedure for the left central incisor. Considering the
patient age and cooperation the maxillary right central
incisor was planned to keep under follow up observation.
Fig 1: Pre-operative photograph showing Fracture with
relation to 61
Fig 2 Pre-operative radiograph showing Fracture with
relation to 61 involving pulp and horizontal root fracture
with relation to 51 in apical third
DISCUSSION:
The prevalence of avulsion out of all types of
traumatic luxation injuries to primary teeth ranges
between 5.8% and 19.4%. This is due to the factors like
pliable alveolar bone and vertically placed incisor teeth.
However root fracture in primary tooth is less common if
present they are most frequent at the age of 3–4 years
where physiologic root resorption has begun, thereby
weakening the root 4.
Over and above the trauma to the primary tooth
will results in sequelae not only to itself but also to the
developing permanent tooth germs which lies in close
proximity to the roots of the primary teeth .The prevalence
of developmental disturbances of permanent teeth
secondary to primary tooth trauma is reported to be
between 12% and 69%, depending on the severity and type
of the injury as well as the developmental stage of the
permanent tooth 1. Tooth malformation, impacted teeth,
and eruption disturbances in the developing permanent
dentition are some of the consequences that can occur
following severe injuries to primary teeth and/or alveolar
bone 3.
Consequences in the primary dentition
comprised: colour changes, pulp necrosis, pulp canal
obliteration, gingival retraction, permanent displacement
after luxation, pathological root resorption as well as
disturbances in physiological root resorption and lastly
premature tooth loss 5. In a long-term study of 255
traumatized primary teeth, 23% of the corresponding
erupted permanent teeth showed developmental
disturbances. The highest prevalence was found after
intrusive injuries of primary teeth 6.
In case of complicated crown fracture, size of
the pulp chamber, stage of root development and degree
of root resorption should be taken in to consideration while
planning the treatment. However, treatment decisions are
often based on the child’s cooperation and on the further
life expectancy of the affected primary tooth 7.According
to IADT guidelines,in very young children with immature,
still developing roots, it is advantageous to preserve pulp
vitality by pulp capping or partial pulpotomy. This
treatment is also the choice in young patients with
completely formed roots. Calcium hydroxide is a suitable
material for such procedures. Both treatments should be
considered whenever possible, otherwise extraction is
indicated 8. However extraction of the maxillary incisor is
always last resort as premature extraction of this will not
only will affect the aesthetics, speech and leads to space
loss but also will impair the quality of life of the children9.
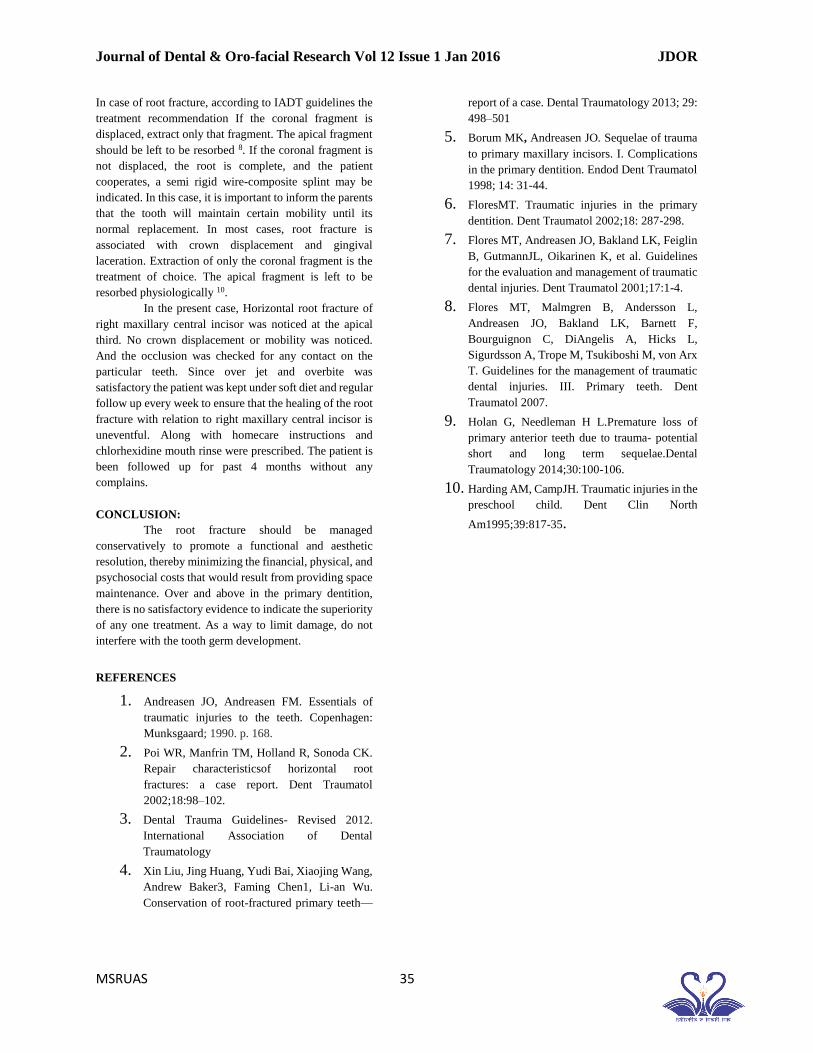
In the present case considering the age of the child ZOE
pulpectomy was carried out with relation to left maxillary
central incisor and restored with GIC (Fig3 &4).
Fig 3 Post operative radiograph shoeing ZOE pulpectomy
in relation
Fig 4 Post-operative photograph
Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 35
In case of root fracture, according to IADT guidelines the
treatment recommendation If the coronal fragment is
displaced, extract only that fragment. The apical fragment
should be left to be resorbed 8. If the coronal fragment is
not displaced, the root is complete, and the patient
cooperates, a semi rigid wire-composite splint may be
indicated. In this case, it is important to inform the parents
that the tooth will maintain certain mobility until its
normal replacement. In most cases, root fracture is
associated with crown displacement and gingival
laceration. Extraction of only the coronal fragment is the
treatment of choice. The apical fragment is left to be
resorbed physiologically 10.
In the present case, Horizontal root fracture of
right maxillary central incisor was noticed at the apical
third. No crown displacement or mobility was noticed.
And the occlusion was checked for any contact on the
particular teeth. Since over jet and overbite was
satisfactory the patient was kept under soft diet and regular
follow up every week to ensure that the healing of the root
fracture with relation to right maxillary central incisor is
uneventful. Along with homecare instructions and
chlorhexidine mouth rinse were prescribed. The patient is
been followed up for past 4 months without any
complains.
CONCLUSION:
The root fracture should be managed
conservatively to promote a functional and aesthetic
resolution, thereby minimizing the financial, physical, and
psychosocial costs that would result from providing space
maintenance. Over and above in the primary dentition,
there is no satisfactory evidence to indicate the superiority
of any one treatment. As a way to limit damage, do not
interfere with the tooth germ development.
REFERENCES
1. Andreasen JO, Andreasen FM. Essentials of
traumatic injuries to the teeth. Copenhagen:
Munksgaard; 1990. p. 168.
2. Poi WR, Manfrin TM, Holland R, Sonoda CK.
Repair characteristicsof horizontal root
fractures: a case report. Dent Traumatol
2002;18:98–102.
3. Dental Trauma Guidelines- Revised 2012.
International Association of Dental
Traumatology
4. Xin Liu, Jing Huang, Yudi Bai, Xiaojing Wang,
Andrew Baker3, Faming Chen1, Li-an Wu.
Conservation of root-fractured primary teeth—
report of a case. Dental Traumatology 2013; 29:
498–501
5. Borum MK, Andreasen JO. Sequelae of trauma
to primary maxillary incisors. I. Complications
in the primary dentition. Endod Dent Traumatol
1998; 14: 31-44.
6. FloresMT. Traumatic injuries in the primary
dentition. Dent Traumatol 2002;18: 287-298.
7. Flores MT, Andreasen JO, Bakland LK, Feiglin
B, GutmannJL, Oikarinen K, et al. Guidelines
for the evaluation and management of traumatic
dental injuries. Dent Traumatol 2001;17:1-4.
8. Flores MT, Malmgren B, Andersson L,
Andreasen JO, Bakland LK, Barnett F,
Bourguignon C, DiAngelis A, Hicks L,
Sigurdsson A, Trope M, Tsukiboshi M, von Arx
T. Guidelines for the management of traumatic
dental injuries. III. Primary teeth. Dent
Traumatol 2007.
9. Holan G, Needleman H L.Premature loss of
primary anterior teeth due to trauma- potential
short and long term sequelae.Dental
Traumatology 2014;30:100-106.
10. Harding AM, CampJH. Traumatic injuries in the
preschool child. Dent Clin North
Am1995;39:817-35.