rpnao 2012 educator’s conference june 4, 2012 - bruton.pdf · rpnao 2012 educator’s conference...
TRANSCRIPT

Alice Cunnington RPNKaren Bruton, RN BScN CETN(C)
RPNAO 2012 EducatorRPNAO 2012 Educator’’s Conference s Conference June 4, 2012June 4, 2012

• To review the implementation of enactment of full scope of practice for RPN’s in a community based hospital setting
• Describe the needs assessment & strategic plan to implement initiative
• Examine the interprofessional model of care• Review the process for education implementation • Identify enablers, supports & tools utilized to support change
• Evaluate & identify strengths & weaknesses
1938 - 6 month practical nurse program initiated1941-45 – 107 trained but then phased out after 5 yrs1946 – 9 mth program, Toronto, Hamilton & Kingston1947 - nurse’s act changed “Certified Nursing Assistant“1955 - 13 training centres and 950 CNA1963 – CNA changed to RNA1967 - RNA education to 35 wks. Now 14,000 RNAs.1975 – 50 educational centres. Now 31,000 RNAs 1993 - RNA program expanded 1.5 years. Called RPN2002 – entry to practice 2 year diploma program

•Community based hospital (100 beds)•Approx 70 RPNs
ER, inpt units, Ambulatory clinics, OR, PACU•4 levels of nursing education
RPN: Certificate/Diploma RN: Diploma/Degree• Feedback from RPNs to increase scope of
practice
•Support enactment of full scope of practice•To provide frontline clinical practice resources at the bedside
•Enhance quality patient care •Enhance quality of the Practice environment

• Community of Practice for health care professionals to address the need for mentorship in role socialization, leadership, research & scholarship
• To facilitate networking & adoption of evidence-based concepts in patient care
• Health professionals who are passionate about improving practice & patient care in their organization
• Through passion for expertise they have organizational and/or unit/program level influence with their peers
• They can provide ongoing resource support for bridging a gap between evidence & practice with strategies to implement specific best practice

•Talked with RN’s, RPN’s, leaders•Surveillance of procedures & practices•Review of policies•Competency survey for all RN’s & RPN’s•Determine gaps in practice•Discussion through committees

• Simultaneously Northumberland Hills Hospital was developing an interprofessional model of care.
• In servicing & input by staff was a priority to ensure all stakeholders had input.
• A full day meeting with all stakeholders was held to develop a model of care.
• A model of care & terms of reference was developed from the input of staff

Once created it was presented hospital wide to all staff for further input

•Supports in place to provide mentoring & leadership
•Budget allocation for implementation
•Identification of technical skills• Scheduling for in-classroom education
•Sustainability of practices

• Approved by Interprofessional Practice Committee• Supported by organization 100%• Two hour in-service for all RPN’s• 5 eLearning modules through NHH eLearning Centre• Self learning package• Ongoing in-services on CNO’s Enactment of Full Scope of Practice all units, staff meetings
• One on one education when required• Sign off check sheets on technical skills

• In-services for all staff on “Enactment of full scope of practice”
• Discussion & questions encouraged
Nurse
EnvironmentPatient

• Promote an environment of openness for sharing perspectives
• Education through staff meetings, Unit Based Council meetings, forums, Committee meetings

•Inservice given regularly throughout NHH •Goal: to increase awareness of strategic plan•Encourage support for initiative by discussion & input from staff•Discussion of strengths, weaknesses & issues that might appear

Throughout implementation, emphasis to develop leadership skills at NHH through:•Interactive learning•Case scenarios•Promote & enhance critical thinking skills•Mentoring & supporting both RNs+RPNs

•Acquiring telephone orders & giving assessments to physicians
•Taking critical results•Checking of orders•Hanging IV medications & added responsibility for IV therapy
MORE………

• Increased responsibility for administration of IM /SQ/Sub-dermal medications including narcotics
• Initiate & check CADD pumps(SQ narcotics) • Checking of blood products
To ensure safety & promote positive To ensure safety & promote positive learning experiences the technical skills learning experiences the technical skills were phased in over several months were phased in over several months
Agenda 2 hr session•CNO’s 3 factor model (Nurse, client & environment)•IV administration presentation with active participation •Interactive learning with case scenario •Identified expectations to complete initiative•Hard copy self learning package

• Adult Learning Theory • Support by colleagues (both RN’s & RPN’s),
Professional Practice Leaders, allied health professionals, managers, directors
• Positive & supportive learning environment • Physicians received a letter explaining expanded
role. Patience & understanding was suggested to promote positive learning

• Brochure developed on “Mentoring& Supporting Colleagues”
• CNO Guidelines “Supporting Learners” posted on each unit to review

Tools developed to support change & Practice•policies & procedures updated•learning packages •Checklists•brochures•SBARD pads at nursing stations•CNO Guide to Support Learners on each floor
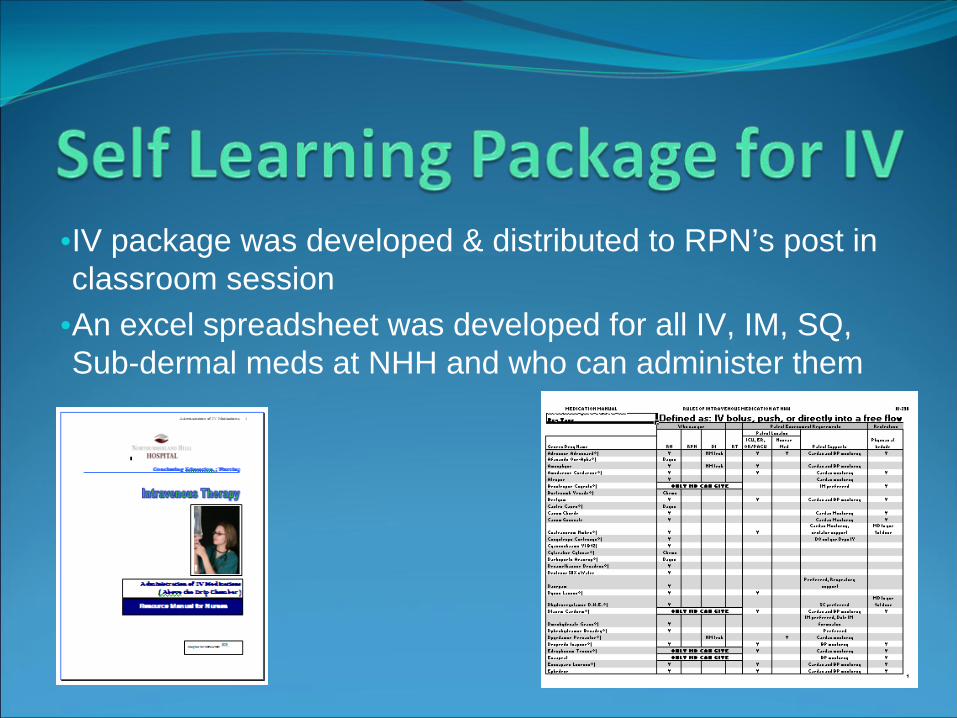
•IV package was developed & distributed to RPN’s post in classroom session
•An excel spreadsheet was developed for all IV, IM, SQ, Sub-dermal meds at NHH and who can administer them

SituationBackgroundAssessmentRecommendationsDocumentation
•Pads on every unit for nurses to use for TOA (change of shift, transferring pt, etc), talking with physicians & colleagues•Left side suggested items to have prepared & the right hand side to use to fill in notes (ie VS, chest sounds)
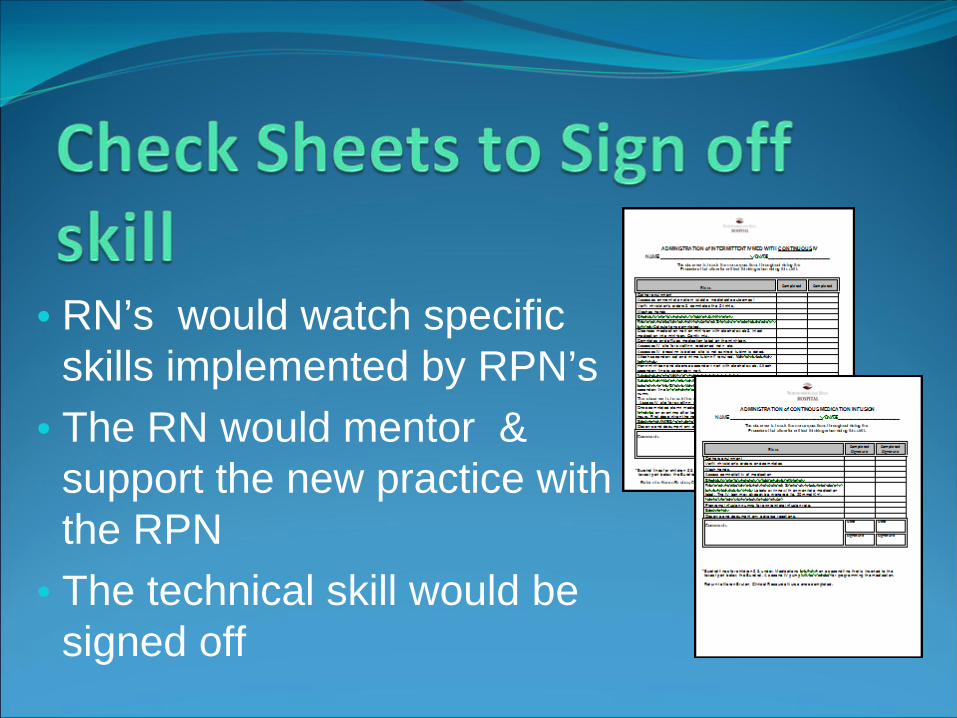
• RN’s would watch specific skills implemented by RPN’s
• The RN would mentor & support the new practice with the RPN
• The technical skill would be signed off

Post in classroom evaluationOne on one commentsInterprofessional Practice CommitteeLeadership committees
Perceptions identified•With any new skills it can be stressful & daunting implementing new practices
•Some fear that they may not be needed as others can do their skills.
OVERALL – Successful implementation!!!

• Biggest Impact to Practice-RPNs doing own MD orders• Improved communication & rapport with physicians &
other health care team members• Most RN’s supported the change especially after in-
servicing which enabled a positive mentoring approach• Nurses dealing with own patient issues reduced potential
mistakes• Patient flow became more efficient • Improved Critical thinking skills• Increased collaboration with interprofessional practice
members

Nurses have a misconception that they are responsible for their colleagues. Education & insight to the CNO standards implemented
“As with any role, once you accept responsibility, you are accountable for
your competence, actions, and decisions. (CNO,2006)
• some RPNs were not ready for the change & didn’t want it
• lack of opportunity for RPNs working in non acute areas to maintain competence with technical skills
• Emergency Department-lack of education of capabilities of RPN’s scope of Practice
• Few of the RN’s were not supportive

• Hiring new staff with different levels of educational backgrounds, skills, experience, competencies and type of past nursing environments
• Being aware of individual needs of new hires

•Nasal gastric tube insertion•Starting of IV’s•Central line care
