rt arterial blood gas .ppt
DESCRIPTION
ARTERIAL BLOOD GAS lecture and interpretation for every medical students.TRANSCRIPT

ARTERIAL BLOOD GASANALYSIS
Objective
I. Arterial Oxygenation A. Hemoglobin
B. Bohr and Haldane Effects
C. Hemoglobin Dissociation Curve
D. Physiology of Arterial Oxygenation
E. Pathophysiologic Mechanisms of Hypoxemia
F. Cardiopulmonary Compensation for Hypoxemia
Objective
II. Reference Ranges and Interpretative Guidelines
III. Clinical Approach to Interpretation
IV. Hypoxemia and Oxygen Therapy
V. Obtaining Blood Gas Sample
VI. Blood Gas Analyzers
VII. Quality Assurance in Blood Gas Analysis


volume of oxygen carried attached to Hb
vol% of O2 carried attached to Hb
=(Hb content)(1.34)(HbO2% sat.)
• = (PO2)(0.003) + (Hb content)(1.34)(HbO2% sat)
O2 content in vol%
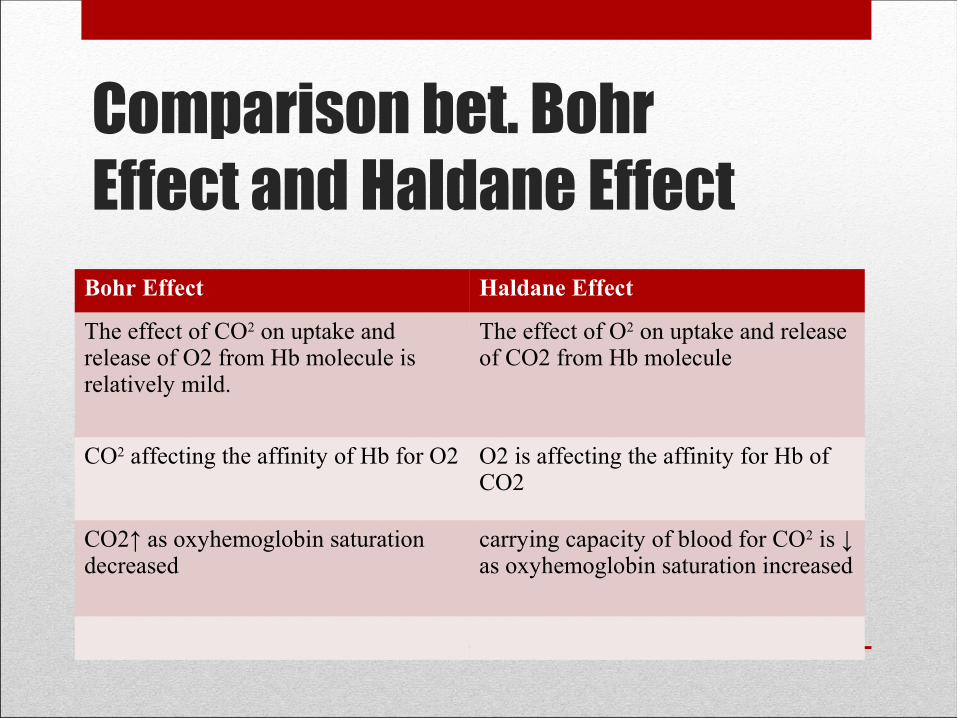
Comparison bet. Bohr Effect and Haldane Effect
Bohr Effect Haldane Effect
The effect of CO2 on uptake and release of O2 from Hb molecule is relatively mild.
The effect of O2 on uptake and release of CO2 from Hb molecule
CO2 affecting the affinity of Hb for O2 O2 is affecting the affinity for Hb of CO2
CO2↑ as oxyhemoglobin saturation decreased
carrying capacity of blood for CO2 is ↓ as oxyhemoglobin saturation increased
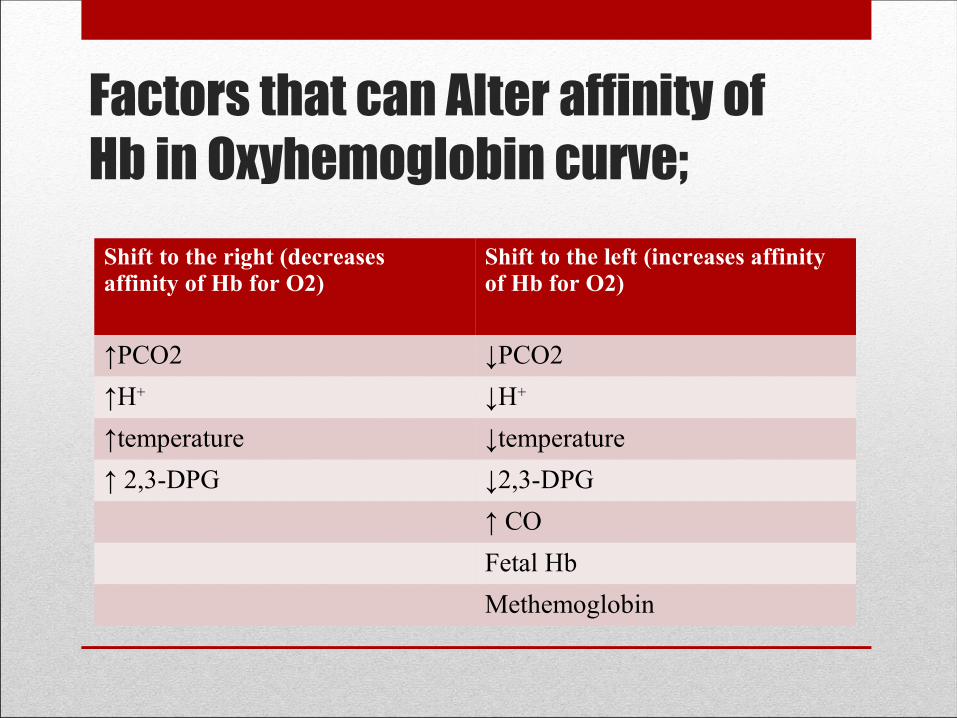
Factors that can Alter affinity of Hb in Oxyhemoglobin curve;
Shift to the right (decreases affinity of Hb for O2)
Shift to the left (increases affinity of Hb for O2)
↑PCO2 ↓PCO2
↑H+ ↓H+
↑temperature ↓temperature
↑ 2,3-DPG ↓2,3-DPG
↑ CO
Fetal Hb
Methemoglobin
pH compensation• The levels of HCO3 and CO2 always change to keep the
pH within normal range.

ABG Interpretation
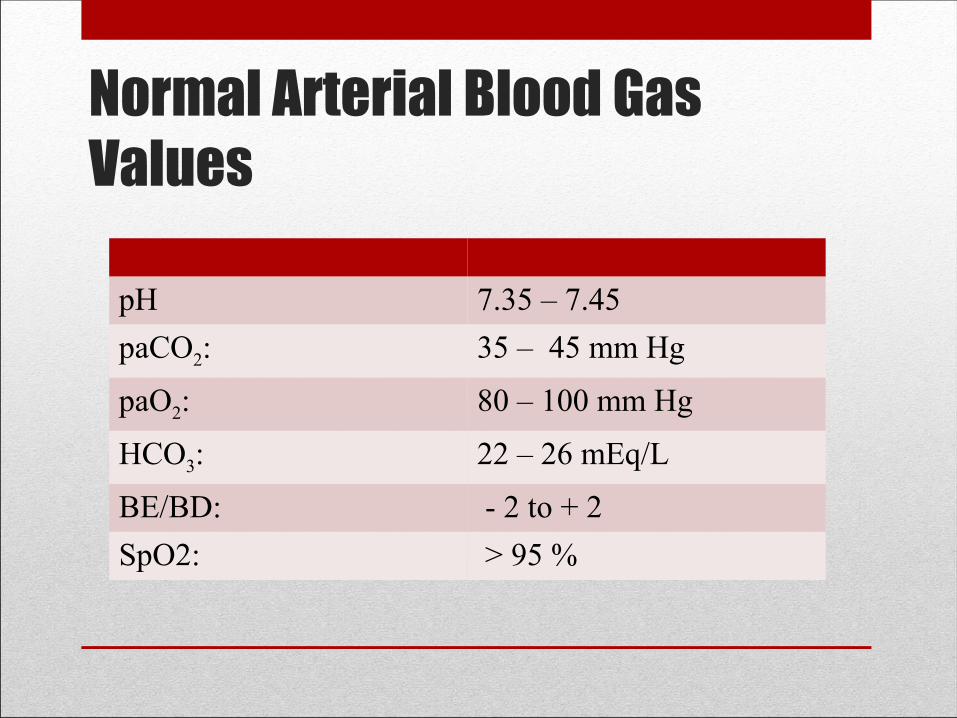
Normal Arterial Blood Gas Values
pH 7.35 – 7.45
paCO2: 35 – 45 mm Hg
paO2: 80 – 100 mm Hg
HCO3: 22 – 26 mEq/L
BE/BD: - 2 to + 2
SpO2: > 95 %
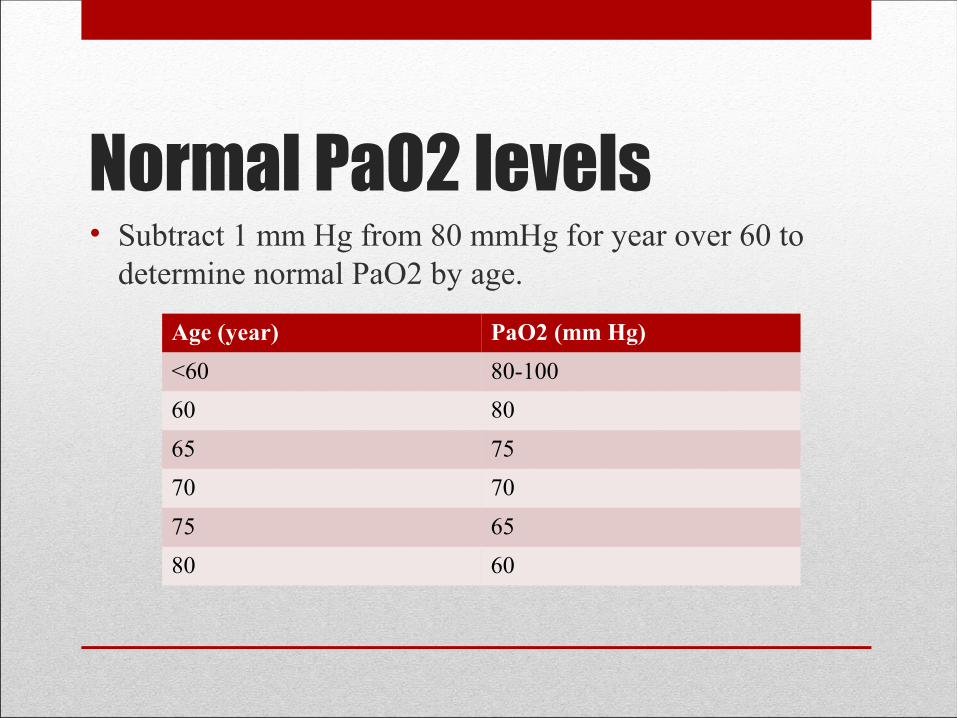
Normal PaO2 levels• Subtract 1 mm Hg from 80 mmHg for year over 60 to
determine normal PaO2 by age.
Age (year) PaO2 (mm Hg)
<60 80-100
60 80
65 75
70 70
75 65
80 60

Levels of hypoxemia
If PaO2 is:
•60 to 79 mm Hg mild hypoxemia
•40 to 59 mm Hg moderate hypoxemia
•<40 mm Hg severe hypoxemia

Assessment of Arterial Oxygenation
Evaluation of Hypoxemia
Room Air (Patient < 60 y/o):
Mild: PaO2 60-79 mmHg
Moderate: PaO2 40-59 mmHg
Severe: PaO2 < 40 mm Hg
On Oxygen Therapy:
• Uncorrected hypoxemia:
PaO2 < 80 mm Hg
• Corrected hypoxemia:
PaO2 = 80 – 100 mm Hg
• Overcorrected hypoxemia:
PaO2 > 100 mm Hg
FiO2 (Fractional InspiredOxygen Concentration)

Inspired Oxygen to PaO2 Relationship
FiO2 Predicted Minimal PaO2
30 % 150
40 % 200
50 % 250
80 % 400
If PaO2 < minimal predicted (FiO2 x 5), the patient can be assumed to be hypoxemic at room air.
Clinically Assess:• Cardiac status
• Peripheral perfusion
• Blood oxygen transport mechanism
Assess 1 and 2 by the vital signs and PE.
If 1 and 2 are adequate, then only 3 can be interfering with proper tissue oxygenation.

Indications for ABG• Sudden dyspnea
• Cyanosis
• Abnormal breath sounds
• Sudden or unexplained tachypnea
• Heavy use of accessory muscles
• Change in ventilator setting
• CPR
• Diffuse infiltrates in c xray

Criteria for choosing site and Technique for obtaining ABG samples must be based on:
• Safety
• Accessibility
• Patient Comfort
Site for ABG
• Brachial Artery
• Radial Artery
• Dorsalis pedis
• Femoral Artery

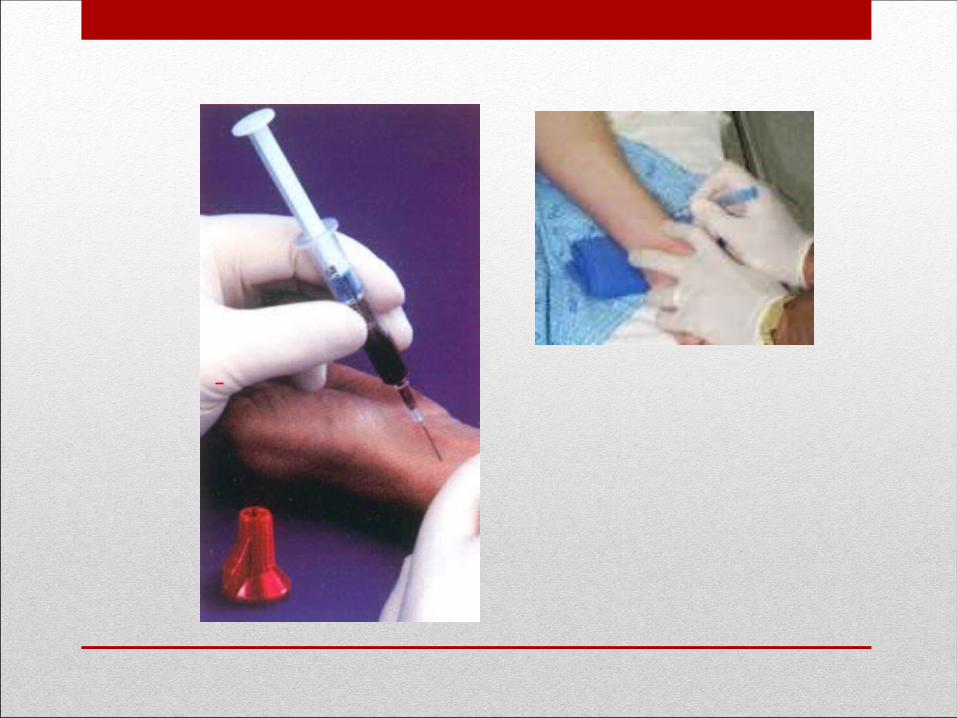
ABG Sampling(radial artery puncture)
1. Explain the procedure to the patient
2. Perform a modified allen’s test
3. Place a folded towel under the patients wrist to keep the wrist hyperextended
4. Clean the puncture site with isopropyl alcohol (70%)
5. The practitioner must wear gloves for this procedure
6. Aspirate 0.5ml of 1:1000 solution of heparin into the syringe using gauge needle. Pull the plunger of the syringe back and forth so that the entire portion of the syringe is exposed to the heparin

ABG Sampling(radial artery puncture)7. With the needle/ syringe in one hand, palpate the artery with the other. The needle should enter the skin at a 45° angle with bevel pointed up. The needle should be advanced until blood is pulsating into the syringe
8. After 2 to 4 ml of blood has been obtained a sterile gauze pad should be applied with pressure over the puncture sithe for 3 to 5 minutes until bleeding has stopped.
9. Air bubbles should be removed from the syringe, since they affect the blood gas levels. Air in the blood causes increased PaO2 levels and decreased PaCo2 levels.
10. A cap or rubber stopper should then be placed over the needle.to prevent air from entering the syringe.
ABG Sampling(radial artery puncture)11. The syringe is then placed on ice to slow the metabolism and keep the ABG levels accurate.
12. The practitioner should record the ff:
a) patients name and room number
b)Fio2 level
c)If patient is on ventilator, record
d)Fio2, Vt, RR, Mode, PEEP,


Parameters Excessive Heparin Air bubbles
pH ↓ or remain the same ↑
PCO2 ↓ ↓
PO2 May altered May altered
HbO2% sat May altered May altered
HbCO2% sat Will not altered Will not altered
Hb content ↓ Is not altered
HCO3 ↓ ↓
Base Excess ↓ ↓
Oxygen content May be altered Maybe altered
Blood gas contaminants
Blood gas contaminants*If insufficient heparin levels are used;
• Machine clotting is very likely;
• Results are questionable
*Saline and other IV solutions alter blood gas values in a manner similar to that of heparin except that the pH may also increase.
Significant Problems• Arteriospasm
• Air or clotted blood emboli
• Anaphylaxis
• Patient or sampler contamination
• Hematoma
• Hemorrhage
• Trauma to the vessel
• Arterial occlusion
• Vasovagal response
• Pain

Recommended Equipment for Percutaneous Arterial Blood Sampling• Standard precautions barrier protection (gloves, safety goggles)
• Anticoagulant(liquid sodium, lithium heparin, or dry lyophilized heparin)
• Sterile glass or low-diffusibility plastic syringe(1 to 5 mL)
• Short-bevel 20 to 22-gauge needle with a clear hub(23 to 25 gauge for children and infants)
• Patient/sample label
• Isopropyl alcohol (70%) or providone-iodine (Betadine) swabs (check patients for iodine sensitivity)
• Sterile gauze squares, tape, bandages
• Puncture-resistant container
• Ice slush (if specimen will not be analyzed within 15 minutes)
• Towels
• Sharps container
• Local anesthetic (0.5% lidocaine)*
• Hypodermic needle(25 to 26 gauge)
• Needle capping device
Blood gas analyzersI. Oxygen Analyzers
• Analyzers that use the thermal conductiity of oxygen
• Analyzers that use Pauling’s principle of paramagnetic susceptability of oxygen (Beckman D-2)
• Analyzers operating on the polarographic principle (Clark electrode)
• Analyzers using galvanic cell

Blood gas analyzers
II. pH (Sanz) electrode
III. PCO2 (Severinghaus Electrode)
IV. Transcutaneous PO2 (TCPO2) and PCO” (TCPCO2) monitoring
V. Spectrophotometric Analyzers
Blood gas analyzers
Type of units commonly used Spectrophotometric analyzers are ;
• pulse oximeters
• CO oximeter
• Flame Photometer
• Capnography (end-tidal CO2 monitoring)

Blood gas analyzers• Currently, blood gas analyzers have the following
capabilities
• 1. accurate measurement of pH, PCO2 and PO2
• 2. self calibration
• 3. accurate measurement of base excess or deficit
• 4.accurate measurement of plasma bicarbonate (HCO3)
• 5. correction for temperature
• 6. self troubleshooting abilities
• 7. automated blood gas interpretation
references• Egan’s fundamentals of respiratory care 9th edition,
Mosby, 2009
• The essentials of respiratory care third edition, kackmarek9

THE END…