running head: craniopharyngioma and immune response · ma. elena hc, et al. running head:...
TRANSCRIPT
iMedPub Journalshttp://www.imedpub.com
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
2015Vol. 6 No. 3:31
1
© Under License of Creative Commons Attribution 3.0 License Find this article in: www.jneuro.com
© Under License of Creative Commons Attribution 3.0 License | This article is available in: www.jneuro.com
Research Article
DOI: 10.21767/2171-6625.100031
Martha Lilia TS1,2, Citlaltepelt SL1,Ma. Elena HC2, Carlos SG1 and Manuel CL3
1 NationalInstituteofNeurologyandNeurosurgery,MexicoCity,Mexico
2 MedicineSchool,sessionofpostgradestudies,atPolithechnicalNationalInstitute,MexicoCity,Mexico
3 Epidemiologyandepidemiologicalsurveillancedepartment,NationalInstituteofRespiratorydisease,MexicoCity,Mexico
Corresponding author:MarthaTena-Suck
Departamento de Neuropatología Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Av. Insurgentes Sur No. 3788 Col. La fama, Delegación Tlalpan C.P. 14269. México, D.F., México.
Tel:(525)56063822,(525)56062008
Citation: LiliaTSM,CitlaltepeltSL,Ma.ElenaHC,etal.RunningHead:CraniopharyngiomaandImmuneResponse.JNeurolNeurosci.2016,6:3.
Running Head: Craniopharyngioma and Immune Response
AbstractBackground: Craniopharyngioma is a rare tumor and accounts for 5-10% ofchildhoodtumorsand,despiteofthebenignhistologicalfeatures,fewstudiesoninflammatorycellsandresponseincraniopharyngiomahavebeenpublished.
The aimof thiswordwas to knownabout inflammation and immunoresponcein Craniopharyngiomas, which were evaluated thought immunohistochemistry.HIF1a, IFI16, TNF-α, TNF- λ, HMC-2, interleukins 6, CD4, CD20, CD68, CD57,Fascin,plasmacellswereused.Tumorsweredividedbetweenrecurrencevsnorecurrenceandbraininfiltration.
Methods and materials: We retrospectively evaluated clinico-pathologicalfindingsin56patientswithcraniopharyngioma(CP).Basedonhistopathologicaland immunohistochemicalfindingsandonclinicalpresentation, tumorsizeandfollow-updatawerecorrelatedwithemphasisintheinflammatoryresponse.
Results: 45wereadamantinomatouscraniopharyngiomasand11werepapillarycraniopharyngiomas. Inflammation was higher in the adamantinomatous typethaninthepapillarytypeandwasassociatedwithgliosis,dystrophiccalcification,andwetkeratinformation,aswellastumoursizeandthedurationofpatients’follow-up.Therewasastatisticallysignificantcorrelationbetweeninflammationin craniopharyngioma and CD4 (p=0.041), CD20 (Phi=0.652, p=0.000), CD68(Phi=0.493, p=0.000), NK (Phi=0.456, p=0.040) MHC-II (Phi=0.476, p=0.014),andIFI-16(Phi=0.436,p=0.031).However,therewasnocorrelationbetweenIL-6immunoexpressionandinflammation.Caseswithmoresevereinflammationwereassociatedwithashorterfollow-upperiodthancasesinwhichnoinflammationwaspresent(LogRanktextp=0.07,IC95%).
Conclusions: Thesedata suggest thatmacrophagesand inflammatory responsemayactasactivatorsincraniopharyngiomas.Thismaybeinvolvedintumorcellproliferation and malignant transformation. Understanding the mechanism ofthesedifferencesmaybecriticalinthedevelopmentofnovelimmunotherapiesforCP,asatreatmentstrategyforCPandtoillustratepossiblephysiologicalpathwaysresponsibleforthetherapeuticbenefitobserved.Furtherstudiesareneeded.
Keywords: Craniopharyngioma; Inflammation; Immune response;Immunohistochemical;Recurrence;Interleukin6,12and4;CD68;Fascin;Plasmacells;CD4;CD8
Abbreviations: CPs: Craniopharyngiomas; Ada: Adamantinomatous form; Paform: Papillary form; SR: Stellate Reticulum; WK: Wet keratin; DC: DystrophicCalcification;GC:GiantCells;CC:CholesterolClefts;FLI:Finger”-LikeInterdigitation;RF:RosenthalFibers; IFI16: Interferonfactor inducible;NFκB:NuclearfactorκB;TNF-α andTNF- λ: Tumornecrosis factorα and tumornecrosis factor λ;GFAP:Glial Fibrillary Acidic Protein; MIF: Macrophage Migration Inhibiting Factor;CNS: CentralNervous System;BBB: Blood-Brain Barrier; TILs: Tumor InfiltratingLymphocytes; PSGL-1: P-Selectin Glycoprotein Ligand-1; NK cells: Natural killercells;HIF-1α:Hypoxiainduciblefactor-1alpha;VEGF:Vascularendothelialgrowthfactor; CA9: Carbonic Adhydrase 9; MVD: Microvessel Density; TAMs: Tumor-associatedmacrophages
Received: August22,2015; Accepted: November10,2015;Published: November14,2015
2
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
This article is available in: www.jneuro.com
IntroductionCraniopharyngiomas (CPs) account for 1.2% to 4% of all braintumors and 6 to 9% of all childhood tumors [1]. They are themost commonnon-glial tumors in childhood [2], andoriginatefrom the embryonic remains of squamous cells through thehypophyseal-pharyngeal duct [1-3]. The pathology of cystformation, inflammation and immune response have beenalwaysquestioned[4].ThecysticportionoftheCPisfilledwithsecretedfluid,cholesterolcrystals,andepithelialcells.Moreover,its presence is associatedwith amajor risk of recurrence, andthus suggesting a proliferative appliance in its genesis andgrowth, rupture, and inflammatory and immune response.Indeed, the cyst fluid recurs aftermultiple aspirations and theepithelium of the cyst is the actively proliferating componentduetothepresenceofsecretorysquamouscellsandofzymogengranules[4].Duetothesecretivepropertiesofthisepithelium,most part of PC has a cystic portion containing secreted fluid,cholesterolcrystals,andepithelialcells[1].Chemicalmeningitisis a rare phenomenon due to rupture of a craniopharyngiomacyst; it develops because of presenceof cholesterol crystals incystfluidsecretedbythesquamousepitheliumliningofthecyst[5].Spontaneousruptureofthecystdescribedmainly inadultsmay present with or without meningitis, depending upon thecholesterolcontentsofcysticfluidoftumor[6,7].Themechanismofruptureofacraniopharyngiomacystmaydependonweaknessofthecystwallcausedbycystexpansioninducingdegenerationofcystwall [8,9].Chemicalmeningitis inCPs issupposedtobecausedby the cholesterol crystals contained in the cysticfluid.Chemical meningitis is therefore strong possibility in operatedcases of residual or recurrent CP though the occurrence ofmeningitis depends on a leak and contents of cholesterol inparticularforacystofCPs[7,8].
Theaimofthisworkwastoevaluatetheimmuneresponseintheboundaryofthecraniopharyngioma.Aclinicalpathologicalandimmunohistochemistryapproach.
Material and MethodClinical casesCraniopharyngiomas were retrieved from the files of thedepartment of Neuropathology at the National Institute ofNeurology and Neurosurgery in Mexico City. The review wasconductedduringthe2000-2007period.Clinicalinformationandfollow-updatawereavailablefor56cases.Age,gender,locationandsizeoftumor,timeofonsetofsymptoms,surgicalexeresis,recurrenceandfollow-upwererecorded.
All tumours analyzed in the study were obtained from a firstsurgery.Histologicalsubtypes/gradeswereclassifiedaccordingtotheguidelinesgivenbytheWorldHealthOrganization(WHO)[1].
Surgically removed specimens were fixed immediately in 10%formalinandsubsequentlyparaffin-embeddedandhematoxylin-eosin-stained. Four pathologists without previous knowledgeof the specimen’s source independently carried out themorphologicalanalysis.
PathologySurgical and biopsy specimens from 56 patients with CP werereviewed. 35 adaCps and 15 pCPs. All biopsies were fixedovernightin4%formalinandroutinelyprocessedintoembeddedparaffin.Sectionswerecutevery4μm.Alltumorsanalysedinthestudywereobtainedfromthefirstsurgicalprocedure,andwereassignedtotwocategories,accordingtothepresence(group1)orabsence(group2)ofbraininvasion.
The criteria to declare brain invasion included the presenceofcohesivecellsformingnestorcompactlyarrangedasa“finger”-like interdigitation, single cells, nests, cords in the form ofwet keratin, ghost cells, and dystrophic calcification in brainparenchyma as well as inflammatory response; macrophages,plasmacells,hemosiderophages.Inaddition,wetkeratin,ghostcellsandcalcificationsonthetumorboundarieswereevaluated.Ruptureofexternalepithelium,tumoralcellsproliferation,stellatereticulumdensity,presenceofoilmachineryfluid,inflammation,granuloma formation, cholesterol cleft macrophages, gliosis,reactive astrocytes, Rosenthal fibers and vessel proliferationwere also considered, paying attention to their characteristicsfor each case. Chronic Inflammation (presence of lymphocytesandplasmacellsinfiltration)andmacrophageswereevaluatedinsurroundingandadjacentbraintissue.
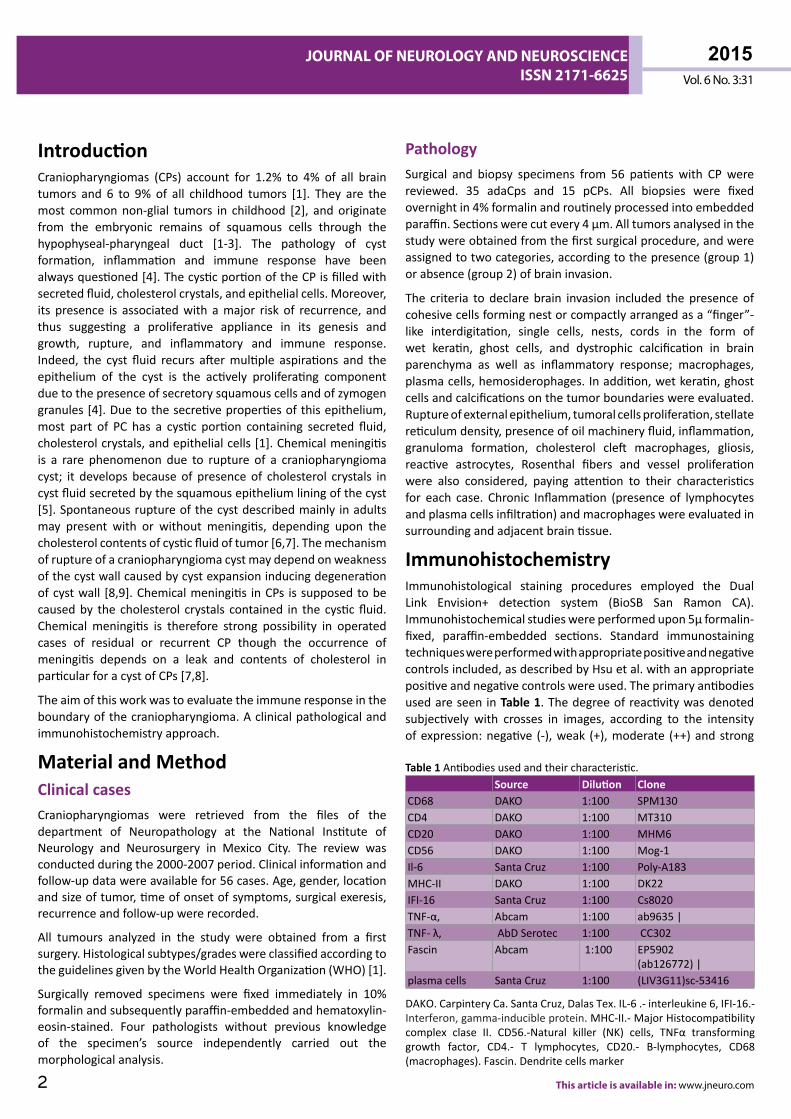
ImmunohistochemistryImmunohistological staining procedures employed the DualLink Envision+ detection system (BioSB San Ramon CA).Immunohistochemicalstudieswereperformedupon5μformalin-fixed, paraffin-embedded sections. Standard immunostainingtechniqueswereperformedwithappropriatepositiveandnegativecontrolsincluded,asdescribedbyHsuetal. withanappropriatepositiveandnegativecontrolswereused.TheprimaryantibodiesusedareseeninTable 1.Thedegreeofreactivitywasdenotedsubjectively with crosses in images, according to the intensityofexpression:negative (-),weak (+),moderate (++)andstrong
Table 1Antibodiesusedandtheircharacteristic.Source Dilution Clone
CD68 DAKO 1:100 SPM130CD4 DAKO 1:100 MT310CD20 DAKO 1:100 MHM6CD56 DAKO 1:100 Mog-1Il-6 SantaCruz 1:100 Poly-A183MHC-II DAKO 1:100 DK22IFI-16 SantaCruz 1:100 Cs8020TNF-α, Abcam 1:100 ab9635|TNF-λ, AbDSerotec 1:100 CC302Fascin Abcam 1:100 EP5902
(ab126772)|plasmacells SantaCruz 1:100 (LIV3G11)sc-53416
DAKO.CarpinteryCa.SantaCruz,DalasTex.IL-6.-interleukine6,IFI-16.-Interferon,gamma-inducibleprotein.MHC-II.-MajorHistocompatibilitycomplex clase II. CD56.-Natural killer (NK) cells, TNFα transforminggrowth factor, CD4.- T lymphocytes, CD20.- B-lymphocytes, CD68(macrophages).Fascin.Dendritecellsmarker
3
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
© Under License of Creative Commons Attribution 3.0 License
craniopharyngiomas (ACF) and eleven (19.6%) were papillarycraniopharyngiomas (PCF) (p=0.005). Twenty-nine (51.8%)samples were from female subjects and twenty-eight (48.2%)from male subjects. Age ranged from 23 to 87 years (mean49.89).Timeelapsedfromonsetofsymptomswas3-24months(mean10.89mo).
Location: Twenty-four of these neoplasms (41.1%) weresuprasellar in location, eighteen (32.1%) infrasellar, andfifteen(27.8%) involved both suprasellar and infrasellar regions. Totalexeresis was attained in thirty-six (64.3%) cases and partialexeresisintwentycases(35.7%).Recurrencewasseenintwenty-seven(48.2%)casesanddeathconfirmedineight(14.3%).
Tumorsize ranged from23to49mm(mean34.5).The follow-upperiodforthepatientsrangedfrom12to56months(mean35.50).
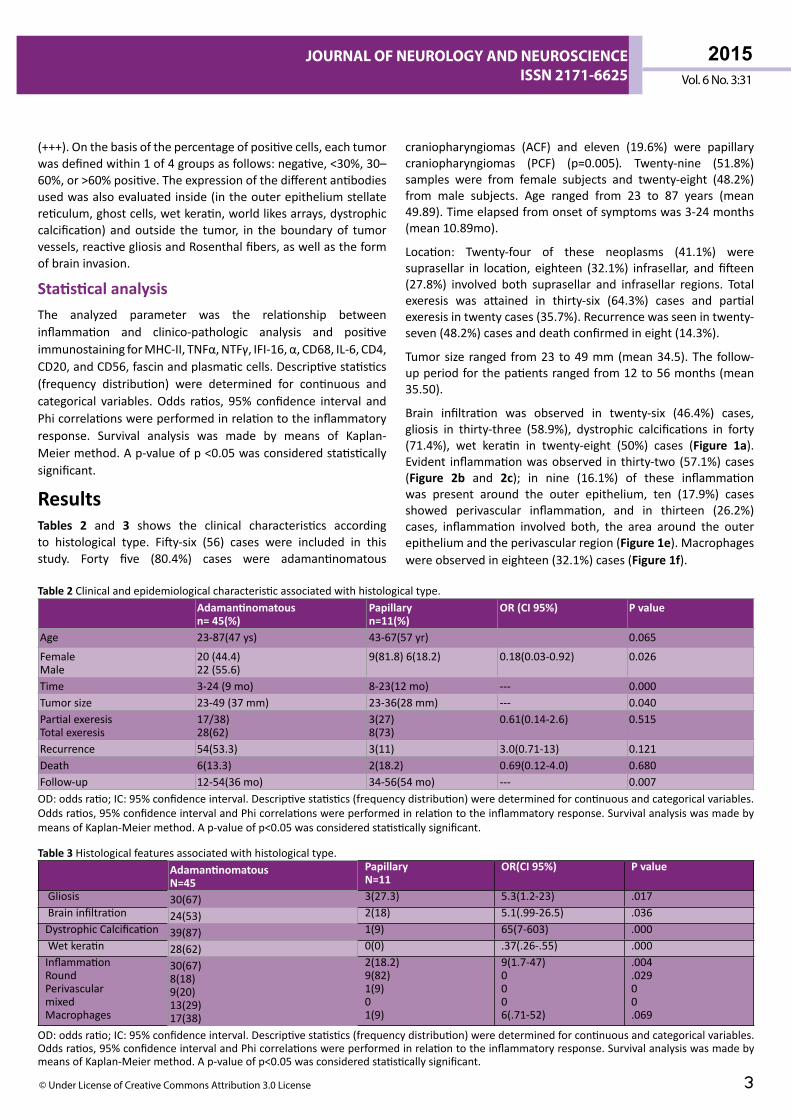
Brain infiltration was observed in twenty-six (46.4%) cases,gliosis in thirty-three (58.9%), dystrophic calcifications in forty(71.4%), wet keratin in twenty-eight (50%) cases (Figure 1a).Evident inflammationwasobserved in thirty-two (57.1%)cases(Figure 2b and 2c); in nine (16.1%) of these inflammationwas present around the outer epithelium, ten (17.9%) casesshowed perivascular inflammation, and in thirteen (26.2%)cases, inflammation involved both, the area around the outerepitheliumandtheperivascularregion(Figure 1e).Macrophageswereobservedineighteen(32.1%)cases(Figure 1f).
(+++).Onthebasisofthepercentageofpositivecells,eachtumorwasdefinedwithin1of4groupsasfollows:negative,<30%,30–60%,or>60%positive.Theexpressionofthedifferentantibodiesusedwasalsoevaluatedinside(intheouterepitheliumstellatereticulum,ghostcells,wetkeratin,worldlikesarrays,dystrophiccalcification) andoutside the tumor, in theboundaryof tumorvessels,reactivegliosisandRosenthalfibers,aswellastheformofbraininvasion.
Statistical analysisThe analyzed parameter was the relationship betweeninflammation and clinico-pathologic analysis and positiveimmunostainingforMHC-II,TNFα,NTFγ,IFI-16,α,CD68,IL-6,CD4,CD20,andCD56,fascinandplasmaticcells.Descriptivestatistics(frequency distribution) were determined for continuous andcategorical variables.Odds ratios, 95% confidence interval andPhicorrelationswereperformedinrelationtotheinflammatoryresponse. Survival analysis was made by means of Kaplan-Meiermethod.Ap-valueofp<0.05wasconsideredstatisticallysignificant.
ResultsTables 2 and 3 shows the clinical characteristics accordingto histological type. Fifty-six (56) cases were included in thisstudy. Forty five (80.4%) cases were adamantinomatous
Table 2 Clinicalandepidemiologicalcharacteristicassociatedwithhistologicaltype.Adamantinomatousn= 45(%)
Papillaryn=11(%)
OR (CI 95%) P value
Age 23-87(47ys) 43-67(57yr) 0.065
FemaleMale
20(44.4)22(55.6)
9(81.8)6(18.2) 0.18(0.03-0.92) 0.026
Time 3-24(9mo) 8-23(12mo) --- 0.000Tumorsize 23-49(37mm) 23-36(28mm) --- 0.040PartialexeresisTotalexeresis
17/38)28(62)
3(27)8(73)
0.61(0.14-2.6) 0.515
Recurrence 54(53.3) 3(11) 3.0(0.71-13) 0.121Death 6(13.3) 2(18.2) 0.69(0.12-4.0) 0.680Follow-up 12-54(36mo) 34-56(54mo) --- 0.007OD:oddsratio;IC:95%confidenceinterval.Descriptivestatistics(frequencydistribution)weredeterminedforcontinuousandcategoricalvariables.Oddsratios,95%confidenceintervalandPhicorrelationswereperformedinrelationtotheinflammatoryresponse.SurvivalanalysiswasmadebymeansofKaplan-Meiermethod.Ap-valueofp<0.05wasconsideredstatisticallysignificant.
Table 3 Histologicalfeaturesassociatedwithhistologicaltype.AdamantinomatousN=45
PapillaryN=11
OR(CI 95%) P value
Gliosis 30(67) 3(27.3) 5.3(1.2-23) .017Braininfiltration 24(53) 2(18) 5.1(.99-26.5) .036DystrophicCalcification 39(87) 1(9) 65(7-603) .000Wetkeratin 28(62) 0(0) .37(.26-.55) .000InflammationRoundPerivascularmixedMacrophages
30(67)8(18)9(20)13(29)17(38)
2(18.2)9(82)1(9)01(9)
9(1.7-47)0006(.71-52)
.004
.02900.069
OD:oddsratio;IC:95%confidenceinterval.Descriptivestatistics(frequencydistribution)weredeterminedforcontinuousandcategoricalvariables.Oddsratios,95%confidenceintervalandPhicorrelationswereperformedinrelationtotheinflammatoryresponse.SurvivalanalysiswasmadebymeansofKaplan-Meiermethod.Ap-valueofp<0.05wasconsideredstatisticallysignificant.
4
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
This article is available in: www.jneuro.com
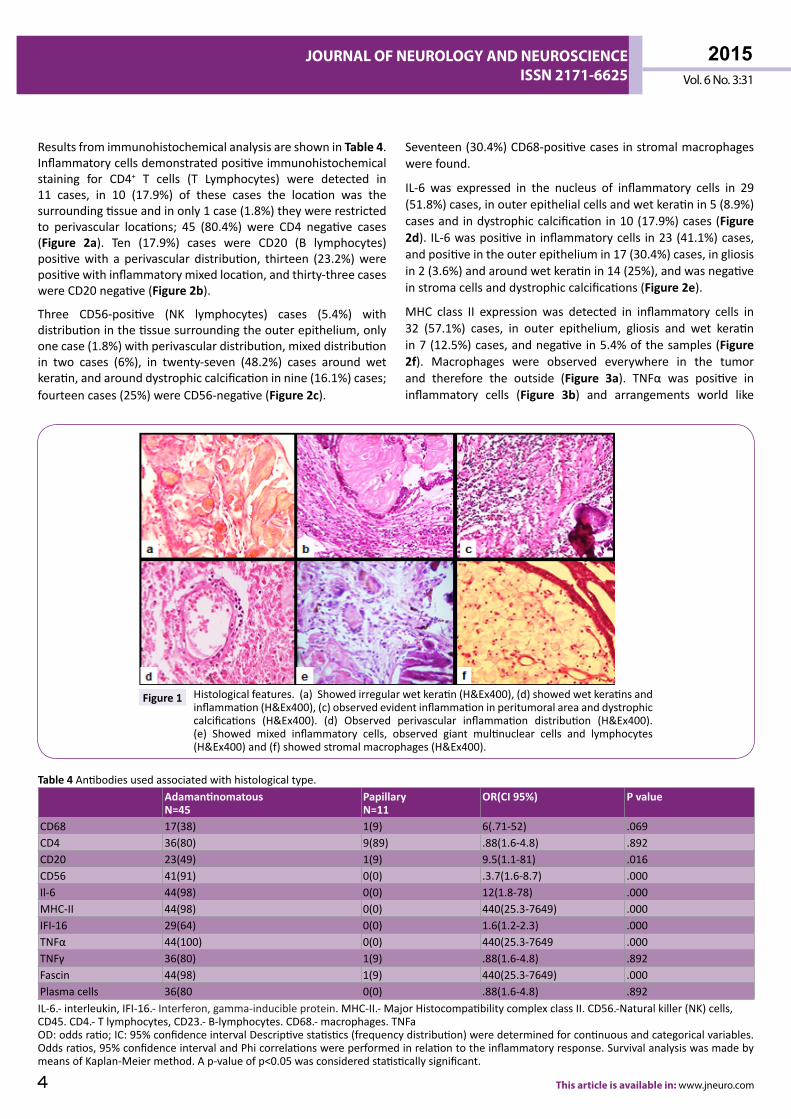
ResultsfromimmunohistochemicalanalysisareshowninTable 4.Inflammatorycellsdemonstratedpositiveimmunohistochemicalstaining for CD4+ T cells (T Lymphocytes) were detected in11 cases, in 10 (17.9%) of these cases the location was thesurroundingtissueandinonly1case(1.8%)theywererestrictedto perivascular locations; 45 (80.4%) were CD4 negative cases(Figure 2a). Ten (17.9%) cases were CD20 (B lymphocytes)positivewith a perivascular distribution, thirteen (23.2%)werepositivewithinflammatorymixedlocation,andthirty-threecaseswereCD20negative(Figure 2b).
Three CD56-positive (NK lymphocytes) cases (5.4%) withdistributioninthetissuesurroundingtheouterepithelium,onlyonecase(1.8%)withperivasculardistribution,mixeddistributionin two cases (6%), in twenty-seven (48.2%) cases around wetkeratin,andarounddystrophiccalcificationinnine(16.1%)cases;fourteencases(25%)wereCD56-negative(Figure 2c).
Seventeen(30.4%)CD68-positivecasesinstromalmacrophageswerefound.
IL-6 was expressed in the nucleus of inflammatory cells in 29(51.8%)cases,inouterepithelialcellsandwetkeratinin5(8.9%)casesandindystrophiccalcificationin10(17.9%)cases(Figure 2d). IL-6waspositivein inflammatorycells in23(41.1%)cases,andpositiveintheouterepitheliumin17(30.4%)cases,ingliosisin2(3.6%)andaroundwetkeratinin14(25%),andwasnegativeinstromacellsanddystrophiccalcifications(Figure 2e).
MHC class II expression was detected in inflammatory cells in32 (57.1%) cases, in outer epithelium, gliosis and wet keratinin7(12.5%)cases,andnegativein5.4%ofthesamples(Figure 2f). Macrophages were observed everywhere in the tumorand therefore the outside (Figure 3a). TNFα was positive ininflammatory cells (Figure 3b) and arrangements world like
Figure 1 Histologicalfeatures.(a)Showedirregularwetkeratin(H&Ex400),(d)showedwetkeratinsandinflammation(H&Ex400),(c)observedevidentinflammationinperitumoralareaanddystrophiccalcifications (H&Ex400). (d) Observed perivascular inflammation distribution (H&Ex400).(e) Showed mixed inflammatory cells, observed giant multinuclear cells and lymphocytes(H&Ex400)and(f)showedstromalmacrophages(H&Ex400).
Table 4 Antibodiesusedassociatedwithhistologicaltype.AdamantinomatousN=45
PapillaryN=11
OR(CI 95%) P value
CD68 17(38) 1(9) 6(.71-52) .069CD4 36(80) 9(89) .88(1.6-4.8) .892CD20 23(49) 1(9) 9.5(1.1-81) .016CD56 41(91) 0(0) .3.7(1.6-8.7) .000Il-6 44(98) 0(0) 12(1.8-78) .000MHC-II 44(98) 0(0) 440(25.3-7649) .000IFI-16 29(64) 0(0) 1.6(1.2-2.3) .000TNFα 44(100) 0(0) 440(25.3-7649 .000TNFγ 36(80) 1(9) .88(1.6-4.8) .892Fascin 44(98) 1(9) 440(25.3-7649) .000Plasmacells 36(80 0(0) .88(1.6-4.8) .892IL-6.-interleukin,IFI-16.-Interferon,gamma-inducibleprotein.MHC-II.-MajorHistocompatibilitycomplexclassII.CD56.-Naturalkiller(NK)cells,CD45.CD4.-Tlymphocytes,CD23.-B-lymphocytes.CD68.-macrophages.TNFaOD:oddsratio;IC:95%confidenceintervalDescriptivestatistics(frequencydistribution)weredeterminedforcontinuousandcategoricalvariables.Oddsratios,95%confidenceintervalandPhicorrelationswereperformedinrelationtotheinflammatoryresponse.SurvivalanalysiswasmadebymeansofKaplan-Meiermethod.Ap-valueofp<0.05wasconsideredstatisticallysignificant.
5
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
© Under License of Creative Commons Attribution 3.0 License
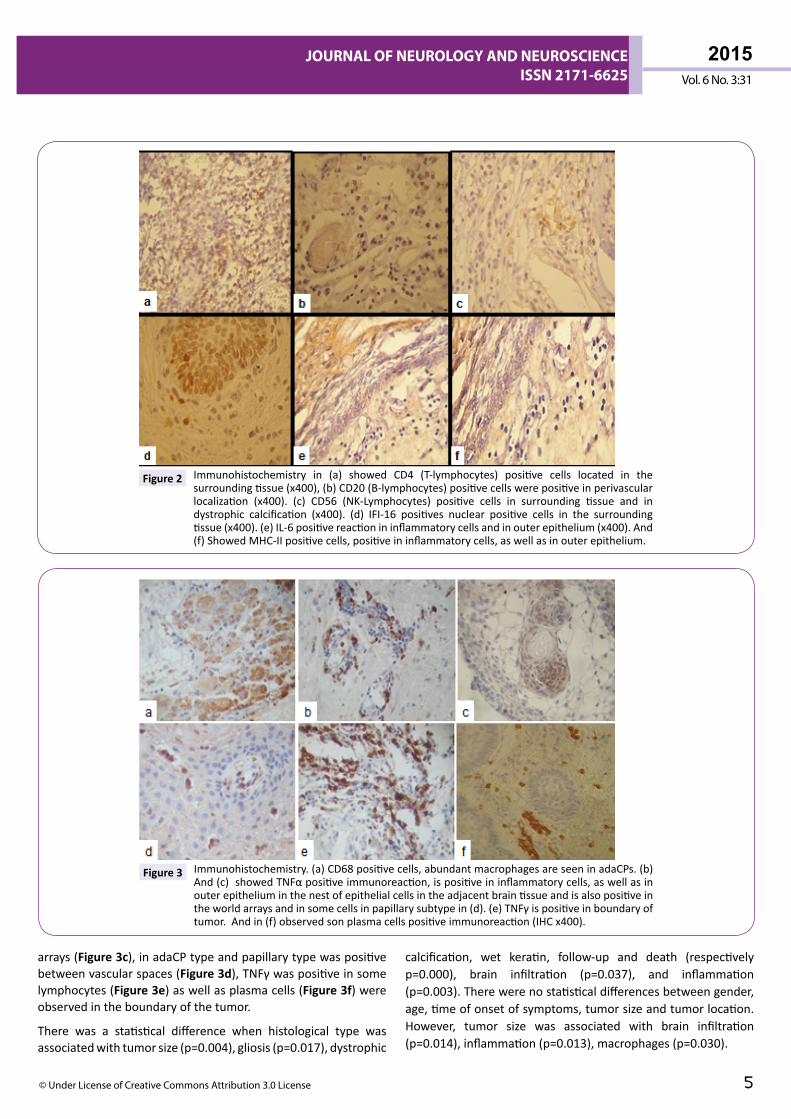
arrays(Figure 3c),inadaCPtypeandpapillarytypewaspositivebetweenvascularspaces(Figure 3d),TNFγwaspositiveinsomelymphocytes(Figure 3e)aswellasplasmacells(Figure 3f)wereobservedintheboundaryofthetumor.
There was a statistical difference when histological type wasassociatedwithtumorsize(p=0.004),gliosis(p=0.017),dystrophic
calcification, wet keratin, follow-up and death (respectivelyp=0.000), brain infiltration (p=0.037), and inflammation(p=0.003).Therewerenostatisticaldifferencesbetweengender,age,timeofonsetofsymptoms,tumorsizeandtumorlocation.However, tumor size was associated with brain infiltration(p=0.014),inflammation(p=0.013),macrophages(p=0.030).
Figure 2 Immunohistochemistry in (a) showed CD4 (T-lymphocytes) positive cells located in thesurroundingtissue(x400),(b)CD20(B-lymphocytes)positivecellswerepositiveinperivascularlocalization (x400). (c) CD56 (NK-Lymphocytes) positive cells in surrounding tissue and indystrophic calcification (x400). (d) IFI-16 positives nuclear positive cells in the surroundingtissue(x400).(e)IL-6positivereactionininflammatorycellsandinouterepithelium(x400).And(f)ShowedMHC-IIpositivecells,positiveininflammatorycells,aswellasinouterepithelium.
Figure 3 Immunohistochemistry.(a)CD68positivecells,abundantmacrophagesareseeninadaCPs.(b)And(c)showedTNFαpositiveimmunoreaction,ispositiveininflammatorycells,aswellasinouterepitheliuminthenestofepithelialcellsintheadjacentbraintissueandisalsopositiveintheworldarraysandinsomecellsinpapillarysubtypein(d).(e)TNFγispositiveinboundaryoftumor.Andin(f)observedsonplasmacellspositiveimmunoreaction(IHCx400).
6
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
This article is available in: www.jneuro.com
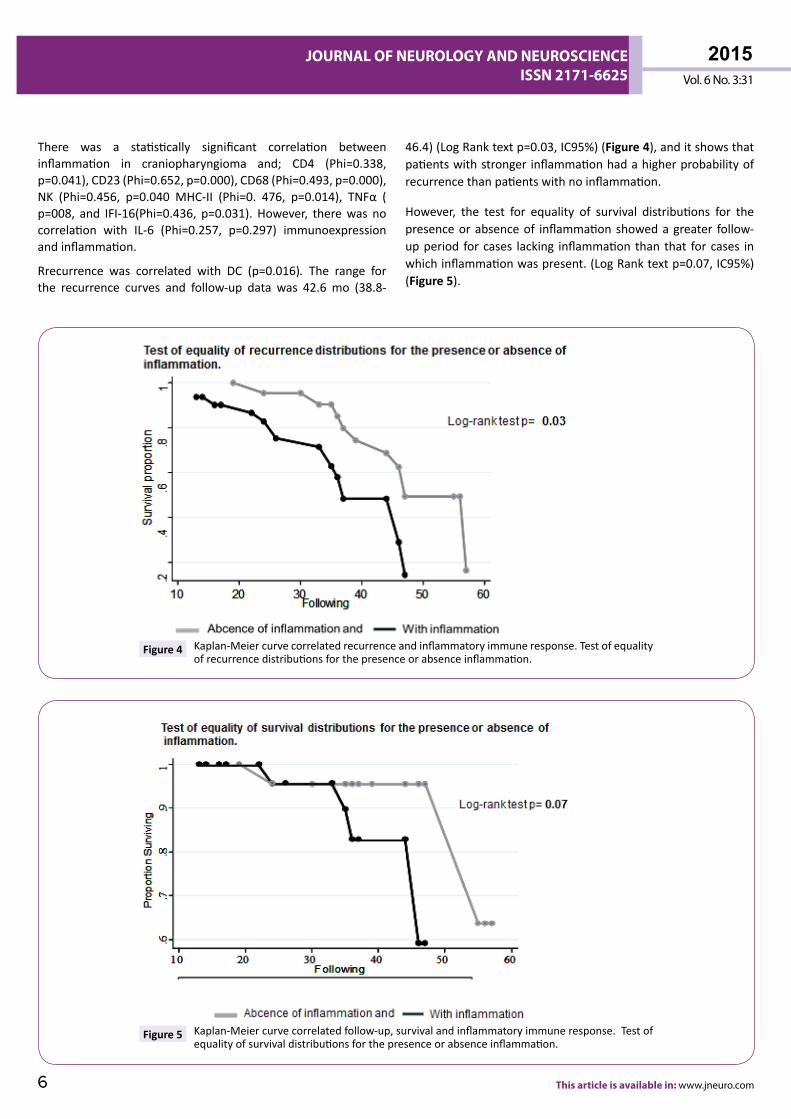
There was a statistically significant correlation betweeninflammation in craniopharyngioma and; CD4 (Phi=0.338,p=0.041),CD23(Phi=0.652,p=0.000),CD68(Phi=0.493,p=0.000),NK (Phi=0.456, p=0.040 MHC-II (Phi=0. 476, p=0.014), TNFα (p=008, and IFI-16(Phi=0.436, p=0.031). However, therewas nocorrelation with IL-6 (Phi=0.257, p=0.297) immunoexpressionandinflammation.
Rrecurrence was correlated with DC (p=0.016). The range forthe recurrence curves and follow-up data was 42.6 mo (38.8-
46.4)(LogRanktextp=0.03,IC95%)(Figure 4),anditshowsthatpatientswithstrongerinflammationhadahigherprobabilityofrecurrencethanpatientswithnoinflammation.
However, the test for equality of survival distributions for thepresenceorabsenceof inflammationshowedagreater follow-upperiod forcases lacking inflammationthan that forcases inwhichinflammationwaspresent.(LogRanktextp=0.07,IC95%)(Figure 5).
Figure 4 Kaplan-Meiercurvecorrelatedrecurrenceandinflammatoryimmuneresponse.Testofequalityofrecurrencedistributionsforthepresenceorabsenceinflammation.
Figure 5 Kaplan-Meiercurvecorrelatedfollow-up,survivalandinflammatoryimmuneresponse.Testofequalityofsurvivaldistributionsforthepresenceorabsenceinflammation.

7
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
© Under License of Creative Commons Attribution 3.0 License
DiscussionThetotalremovalofcraniopharyngiomascanbedifficultbecauseof their tendency to adhere to surrounding vital structures.Frequently,adjacentbraintissueisinfiltratedbyleukocytesandcytokine(s) produced by tumor cellsmay play a pivotal role intissuereaction[3,7,10].Twosubtypescouldbedistinguished:anadamantinomatous(Ada)formthatismorecommoninchildren,and a papillary (Pa) form that is observed almost exclusivelyin adults [1]. The tumour is usually part cystic and part solid.Besides thesehistologicaldifferences, these twovariantsdifferin somemolecular features that have been recently identifiedand couldhave important therapeutic implications [3,5]. It hasbeen demonstrated that inflammation and macrophages canbe present within the tumor and in the surrounding tissue,but to our knowledge this is the first clinico-pathologic andimmunohistochemical report considering inflammation asbiologicalbehaviour[8].
BleedingandescapeofkeratinousmaterialfromtheCPscanresultinyellowfociofxanthogranulomatousinflammation.Microscopicexamination of these yellow foci of xanthogranulomatousinflammation reveals foamy macrophages and giantmultinucleatedcellssurroundingcholesterolclefts[8].Onlyafewstudies have addressed themolecular classification of the cystfluid so far and themechanismsof actionof intracysticagentsarenotclearlyunderstoodyet[8,9].MorerecentstudiessuggestthatthecysticelementofCPscouldbealsotheresultofanactiveproductionofthefluidbytheepithelialcellsoftumor[2,3].Thepatternofembryologicalformationofthehypothalamic-pituitaryaxis plays a major role in its propensity for developing cysticepithelial lesions. Subsequent inflammatory, metaplastic, andneoplasticprocessesmaypromotefurtherprogressionalongthepathologicalcontinuum,rangingfrombenignepithelialcyststoaggressiveneoplasticcysticCPs [1-3].Thenumerouspathologyreportsoncraniopharyngiomadescribetheclassicalfeaturesofsquamousepitheliumandkeratin.Relatively littleattentionhasbeenpaidtoitsstromaandthesurroundingtissueandimmuneresponse [7,8]. The tumor stroma have reactive changes andcommonly showed cyst formation and calcification [9]. Muchrecentresearchaimstocharacterizethecystfluidtounderstandthemechanism of formation and to refine treatments able toreduce cyst volume and inhibit the formation of new cysts.Indeed, the formation mechanism of cystic fluid has alwaysbeen debated: it could be the result of blood-brain barrierimpairment[2],butsurelyanactivesecretoryprocesstakespartinitsformation[3,4],orisduetoepithelialcellssecretion[6,7],ruptureofthosestructures[8,9],oilmachineryfluidcomponentsofthecyststructuresorissecondarytoanimmuneresponsethatproduceandspontaneousinvolution[11].Spontaneousruptureofcraniopharyngiomacystscanbedividedintothreesubtypes:cyst rupture associated with chemical meningitis; cyst rupturewithimprovementinsymptomsrelatedtothecraniopharyngiomaandnotassociatedwithchemicalmeningitis;andasymptomaticrupture[6,7].Signsofasepticmeningitis, includingneutrophilicpleocytosis, thepresenceof cholesterol crystals,macrophages,
granulomasformationandinflammatoryresponse.Inflammationis likely toproducegreatertumoradherencetoand infiltrationof adjacent brain tissue [3]. The inflammatory cytokines hasbeen examined at various inflammatory levels of AdaCps [12].IL-1alpha, IL-6 and TNF-alpha has been reported significantlyhigher in the cyst fluid than in cerebrospinal fluid (CSF) [12],Mori et al. [13], observed that IL-6 plays an important role intheinflammatoryreactionthatoccursintheinterfacebetweenthecraniopharyngiomaand thebrainparenchyma.α-defensins1-3 and other proteins and peptides have been involved ininflammation, mineralization processes and lipid transport[10].ApolipoproteinA-I,A-II,C-IandJ,haemoglobinfragments,ubiquitin,α-2-HS-glycoproteinorfetuinA,α-1-antichymotrypsin,vitamin D binding protein, and α-1-acid glycoprotein werealso have been characterized in the oil machinery fluid [10].Thymosinsβ4andβ10peptideshasbeenalso identified intheintracysticfluidAdaCPs[14].Thepresenceofβ-thymosinsintheintracysticfluidofthetumourconfirmedthesecretionoftheseproteinsintheextracellularenvironment[14].Duetoactivityandantiapoptoticandanti-inflammatorypropertiescouldbestrictlyinvolvedinbothtumourprogressionandcystdevelopmentandgrowth [14]. Galectin-3, p53, and the macrophage movementinhibiting factor (MIF) are known to play crucial roles in theseprocesses [15].Thecentralnervoussystem(CNS) isconsideredasan"immunologicallyprivileged"site[16].However,thisnotionhas been slowly overturned by the realization that the neuro-immunologic interface is, in fact, dynamic andnot absolvedofimmunity's ability to recognizedanger.Numerous studies haveinvestigated the immune system of brain tumour patients,mainlyinthecontextofmalignantglioma.Braintumourpatientssufferfromextensive immunosuppressiondueto lymphopenia,decreased lymphocyte proliferation, and diminished cytotoxicactivity, reduced MHC class I expression on monocytes andpredominanceofanti-inflammatoryT-helper2-type(Th2)cytokineproduction [16]. Derivatives of the monocyte/macrophagelineage appear to enter and take up residence in variousstructuresoftheCNSaspartofnormalontogenyandphysiology[16].Leukocytemigrationintoandthroughtissuesisfundamentalto normal physiology, immunopathology and host defence.Leukocyte entry into the CNS is restricted, in part, because oftheblood-brainbarrier(BBB)[16].Immunocompetentcells,suchasT-lymphocytesofbothCD4andCD8positive.Currently, thisimmunesystem-tumorinteractionisrepresentedbytheconceptofcancerimmunoediting,whichemphasizesthatimmunitymaysubserveeitherclassicalcancerimmunosurveillancefunctionsorpromotetheeventualoutgrowthofimmunoevasivecancercells[16].Moreover,cancerpatientsmountbothcellularandhumoraladaptive,aswellasinnate,immuneresponsestothetumorstheyharbour. In concert with adaptive immune recognition, recentprovocative data suggest that the innate immune system alsodiscriminatesbetweentumorcellsandnormalcells. Eiseleetal.[17], showed that human glioma cells expressMICA/B aswellasULBP1-3 and that the expression of these ligands in gliomamaybeinfluencedbyTGF-β.Moreover,Wuetal.[18]Providedevidencethattumor-initiatingcellswithingliomas−alsoreferred

8
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
This article is available in: www.jneuro.com
to as glioma stem cells and characterized by their CD133 cellsurface marker expression−express NKG2D and NKp30/44/46ligands.OurresultsshowaperivascularinfiltrateofCD20+cells,andthefollowingstatisticaldifferenceswhenassociatingitwithtumorsize(p=0.004),histologicaltype(p=0.013),braininfiltrationandmodeofinflammatorycellinfiltration(p=0.000respectively).CD4 positive immunoreaction was expressed in peritumoralareaandwasassociatedwithtumorsize(p=0.028),histologicaltype(p=0.000),braininfiltrationandmodeofinflammatorycellinfiltration(p=0.000respectively).TheinflammationlabelledbyCD45has been identified commonly in the craniopharyngiomatissues involving the third ventricular floor [8]. Liu et al. [19]suggestedthatthedifference inthe inflammationbetweenthetwotypesofcraniopharyngiomamayaffecttheprognosisofthepatients,andthatACFshowedmarkedlyhigherCD45andICAM-1expressionsthanPCF.
Stevens et al. [20] characterized the immune infiltrates ingliomas,carcinomametastases,CPandmeningiomas.InfiltratesingliomasconsistalmostexclusivelyofT-cellsofthesuppressor/cytotoxic typewhereas infiltrates in carcinomametastasesandCPscontainconsiderablenumbersofCD4+TcellsandB-cells.
TIL display, antigen-specific activated (TIL) must be able tomovetorelevanttumorsitesinthebrain.GiventheanatomicalcomplexityoftheCNS,ithasbeenproposedthattherearethreemethodsbywhichimmunecellsmayaccesstheCNS:frombloodtotheCSFviathechoroidplexus,frombloodtothesubarachnoidspace,andfrombloodtoparenchyma[20].However,theblood-brainbarrier(BBB)anditsintegrityinthesettingofgliomabeforeaddressinghowlymphocytesmaytrafficfromthebloodtotumorsitesintheCNSparenchyma[21].
Tcellshomingtothebrainfirstslowdownbyslowlytetheringtocapillaryendotheliumina"rolling"stepmediatedbyinteractionsbetween endothelial cell E- or P-selectins and P-selectinglycoprotein ligand-1 (PSGL-1) [21]. Subsequently, lymphocyteintegrin molecules become "activated" when chemokines,likely present on the vascular endothelium, engage cognateG protein-coupled chemokine receptors on lymphocytes.Enhanced adhesion is likely mediated through interactionsbetweenintegrin:ligandpairsα4,β1/7,VCAM-1andLFA:ICAM-1expressedonlymphocytesandendothelium,respectively[21].LymphocytesultimatelytransmigratetotheCNSparenchymainthe"diapedesis"step,whichmayoccurviatrans-orpara-cellularendothelialtransport[21].
Natural killer (NK) cells are large granular lymphocytes of theinnate immune system. These cells are able to directly lyseinfectedortransformedcellswithoutspecificimmunization[16],theyalsoaretheleastabundantimmunecellpopulationwithinthebraintumourmicroenvironment.NKcellscanalsorecognisetheFcpartofantibodiesvialowaffinityFcγRIIIA(CD16)receptorandperformantibodydependentcellularcytotoxicity(ADCC)ofantibody-coated cellsMoreover, they secrete various cytokinesandchemokines,suchasinterferongamma(IFN-γ)[21,22].
Hypoxia inducible factor-1 alpha (HIF-1α), which is one of the
hypoxiainduciblefactor-1subunits[19],andplaysanimportantrole in tumor cells adaptation tohypoxicmicroenvironmentbyregulatingitsdownstreamgenes, includingvascularendothelialgrowthfactor(VEGF)andcarbonicanhydrase9(CA9).Proescholdtetal. [23]ReportedHIF-1αexpressionwas largelyabsent inCPcysts. In addition, HIF-1α expression promotes tumor growth,angiogenesisandprogression.However,adaptingtothehypoxicconditions, HIF-1α and VEGF mRNA are largely expressed inrecurrent CP [23]. Therefore, preventing the tumor cells fromadapting to thehypoxic conditionsmaybeaneffectiveway toobviatetherelapseofcraniopharyngioma.Variousstudieshaveshownthattheformationofnewbloodvessels,theangiogenesis,plays a significant role in tumor progression [24]. Possibly thecellular adaptation to hypoxia is a key factor of angiogenesisunder hypoxic microenvironment within craniopharyngioma[19,23,24].
In Craniopharyngiomas, the role of the immune response iseven more complex. An alternative explanation could be theinvolvement of the innate immune response which wouldaccountforsomespecificfeaturesofthecysticfluidsuchasitsinflammatorypropertiesresponsibleforthechemicalmeningitissustainedbycraniopharyngiomafluidspillintothesubarachnoidspace [7,8]. The vasospasm inducedby the contactof the cystfluidtoarteriesevidenceof localsynthesisof IgGandelevatedlactate levels in cyst fluid, which do not correlate with serumlactatelevels,andfinally,thestrongaffinityofnaturalkiller(NK)cellstocraniopharyngioma[13].
Macrophage-inhibiting factor is another molecule probablyinvolvedintheontogenesisofcraniopharyngioma.Macrophagemigration inhibitory factor (MIF) roles as a pleiotropic protein,participating in inflammatory and immune responses [25].MIFwas originally discovered as a lymphokine involved in delayedhypersensitivity and various macrophage functions, includingphagocytosis, spreading, and oncogenesis activity. It wasdemonstrated that anti-MIF antibodies effectively suppresstumor growth and tumor-associated angiogenesis, suggestingthat MIF is involved not only in inflammatory and immuneresponsesbutalsointumorcellgrowth[26].TheMIFexpressionlevel seems to correlate with the risk of recurrence in CP, asit was significantly lower in rapidly recurring CPs than in theslowly recurring or nonrecurring lesions [25,27]. Analogous toMIF,galectin-3levelsofexpressionhasbeenstudiedandhadasignificantlylowerexpressioninrapidlyrecurrentCPs.Inviewoftheantiapoptoticroleofgalectin-3,itslowlevelofexpressioninrecurringCPsseemstoberelatedmoretoitsroleinphagocytosis.In this context the low levels of galectin-3 could correlate theontogenesis of craniopharyngioma with defects in the normalbiological elimination of embryonal tissue remnants. Tumor-associated macrophages (TAMs) are called as “corrupted” byneoplasmscellsandsubsequentlyfacilitate,ratherthan inhibit,tumormetastasis,whichreside inthetumormass,playcentralroles in this intra tumoral interchange. A prevalent hypothesissuggests that macrophages are corrupted by cancer cells andsubsequentlycontributetotumorprogressioninsteadoftumorinhibition[27].Thismechanismcomprisesaparacrinesignalling

9
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
© Under License of Creative Commons Attribution 3.0 License
loop between tumor cells and TAMs that involves variouschemokinesandcytokines[28].Thesefactorssecretedbycancercellscontributetodown-regulationofbothexpressionofmajorhistocompatibility complex class II and macrophage ability topresentantigen.Pukropetal.[29]suggestedthatTAMsinfluencethe tumor microenvironment by modulating Wnt signaling.They showed that TAMs secreteWnt-5a,which inducesMMP-7 expression in cancer cells and facilitates successful invasion.Previously,itwasshownthatmacrophage-derivedWntmoleculespromote vascular remodelling and that tumor cells are highlymobileandintravasatearoundperivascularTAMclusters.Takentogether, we guesswork that invasive TAMs link angiogenesisand tumor invasion and which Wnt-signaling plays a role inmediatingtheiractivity[28,29].Certainly,amolecularguaranteeofadaCP istheactivatedWntsignalingpathwaymaintainedbynuclearβ-cateninaccumulationinasubsetofthesetumorcells,supplementedbyapeculiargrowthpattern inaspecific tumorstem cell (TSC) population in human CPs, which represents atumorstemcellnicheandaddstotumorrecurrence[29].
The presence of these antimicrobial peptides could suggest apossible involvement of the innate immune response in theformationandmaintenanceoftheCPsassociatedcystorsimplybeexpressionofan inflammatory response takingplacewithinthe CPs cyst. Detection of α-defensins 1–3 excludes that cystfluidformationcanderivefromdisruptionofblood–brainbarrierand suggests the involvement of innate immune response inpathology of CPs cyst formation. The reduction of α-defensinscouldderivebothfromdirectantitumoraleffectofinterferon-αonsquamousepithelialcellsofcraniopharyngiomacystandfromits immuno-modulatory effects on the recruitment of cells ofinnateimmunesystems[30].
The reduction of α- defensins, could derive from the directantitumoral effect on the squamous epithelial cells of the CPscyst, which reduces their secretory activity, from its immuno-modulatory effects on the recruitment of cells of the innateimmune systems, from its anti-angiogenetic activity or acombinationoftheabovementionedmechanisms[16].
Interferons are glycoproteins pertaining to the cytokine family
and are related to cell growth factor beta and tumor necrosisfactor,whichareresponsibleforthecontrolofcelldifferentiationandproliferation[30].INF-αbelongstoafamilyofproteinswithantiproliferative and immunomodulatory functions but it isusedas antitumoral agent.A recent studyon theuseof INF-αagainstCPssuggestsapossibleroleoftheFas-inducedapoptosis.Pro-apoptotic and anti-angiogenetic activities, rather than therecentlydescribedeffectsonimmunecells[31].Theantitumoralactivityofinterferonsisduetotheiranti-proliferation,cytotoxicandmaturational effects,with the simultaneousmodulation inpatientimmuneresponse.
TAMstosecreteproteaseswithinthetumormicroenvironment,suchasurokinaseplasminogenactivator[32],cathepsinsBandDandmatrixmetallopeptidases2and9.ItisbelievedthattheseTAM-derived enzymes digest the tumor basement membrane,facilitatingtumorcellescape[33,34].
ConclusionThere was a statistically significant correlation betweeninflammation in craniopharyngioma and; CD4, CD23, CD68,NK, TNFα, TNFγ, MHC-II, and IFI-16, fascin and plasma cellsimmunoexpression. However, there was no correlationbetweenIL-6immunoexpressionandinflammation.Tumorsize,histologicaltype,modeof inflammationandinflammatorycellsare important inbiologicalbehaviours forthefollow-upofCPs.InflammationinCPwascorrelatedwithabadprognosisandwesuggested that tumor-associated macrophages (TAMs) play animportantroleincraniopharyngioma,furtherstudiesareneeded.AdaCP could express high levels of secretedmitogenic signals,includingmembers of several families, as well as chemokines,cytokineswithpro-inflammatoryaction,andtheircorrespondingreceptors, suggesting an important autocrine/paracrine role ofthesecellsinthepathogenesisofadaCPs.
Conflict of InterestThe authors declare no conflict of interests in terms ofemploymentorleadershipposition,stockownership,honoraria,researchfunding,experttestimonyorotherremuneration.
10
ARCHIVOS DE MEDICINAISSN 1698-9465
2015Vol. 6 No. 3:31
JOURNAL OF NEUROLOGY AND NEUROSCIENCEISSN 2171-6625
This article is available in: www.jneuro.com
References 1 Louis DN, Ohgaki H, Wiestler OD, CaveneeWK, Burger PC, et al.
(2009) The 2007 WHO Classification of Tumours of the CentralNervousSystem.ActaNeuropathol(Berl)114:97-109.
2 Hirano A, Ghatek NR, Zimmerman HM (1973) Fenestrated bloodvesselsincraniopharyngioma.ActaNeuropathol26:171-17710.
3 PetitoCK,DeGirolamoU,EarleKM(1967)Craniopharyngiomas.Aclinicalandpathologicalreview.Cancer37:1944-1952.
4 ArefyevaIA,SemenovaJB,ZubairaevMS,KondrashevaEA,MoshkinAV (2002) Analysis of fluid in craniopharyngiomarelated cysts inchildren:proteins,lactateandpH.ActaNeurochir144:551-554.
5 KaravitakiN,BrufaniC,WarnerJT,AdamsCB,RichardsP,etal.(2005)Craniopharyngiomas in children and adults: Systematic analysis of121caseswithlong-termfollow-up.ClinEndocrinol(Oxf)62:397-409.
6 Szeifert GT, Julow J, Szabolcs M, Slowik F, Balint K, et al. (1991)Secretory component of cystic craniopharyngiomas: a mucino-histochemicalandelectron-microscopicstudy.SurgNeurol36:286-293.
7 Szeifert GT, Julow J, Szabolcs M, Slowik F, Balint K, et al. (1991)Secretory component of cystic craniopharyngiomas: a mucino-histochemicalandelectron-microscopicstudy.SurgNeurol36:286-293.
8 Kumar A, Kasliwal MK, Suri A, Sharma BS (2010) Spontaneousasymptomaticruptureofcysticcraniopharyngioma inachild:casereportandreviewoftheliterature.ChildNeurol25:1555-1558.
9 KasaiH,HiranoA,LlenaJF,KawamotoK(1997)Ahistopathologicalstudyofcraniopharyngiomawithspecialreferencetoitsstromaandsurroundingtissue.BrainTumorPathol14:41-45.
10 Martelli C, IavaroneF,Vincenzoni F,RossettiDV,D'Angelo L, et al.(2014) Proteomic characterization of pediatric craniopharyngiomaintracystic fluid by LC-MS top-down/bottom-up integratedapproaches.Electrophoresis35:2172-2183.
11 KinoshitaY,TominagaA1,UsuiS,KurisuK(2014)Acraniopharyngiomawith spontaneous involution of a gadolinium-enhanced region onmagneticresonanceimaging.SurgNeurolInt5:128.
12 Zhou J, Qi ST, Chen LG, Huang CR, You J, et al. (2013) Expressionpatternofinflammatorycytokinesatvariousinflammatorylevelsofadamantinomatouscraniopharyngioma.ZhonghuaYiXueZaZhi93:2499-2501.
13 MoriS,YamaguchiK,MoritaH,MohriN(1985)DistributionofHNK-1+cellsinmalignantlymphomas.ActaPatholJpn35:339-350,
14 Desiderio C, Martelli C, Rossetti DV, Di Rocco C, D'Angelo L, etal. (2013) Identification of thymosins β4 and β 10 in paediatriccraniopharyngiomacysticfluid.ChildsNervSyst29:951-960.
15 LefrancF,ChevalierC,VinchonSBM,DhellemmesP,SchüringMP,etal.(2003)Characterizationofthelevelsofexpressionofretinoicacidreceptors, galectin-3, macrophagemigration inhibiting factor, andp53in51adamantinomatouscraniopharyngiomas.JofNeurosurgery98:145-153.
16 ParneyI(2012)Basicconceptsingliomaimmunology.In:YamanakaR,editor.Glioma.NewYork:Springer42-52.
17 EiseleG,WischhusenJ,MittelbronnM,MeyermannR,WaldhauerI,etal.(2006)TGF-betaandmetalloproteinasesdifferentiallysuppressNKG2D ligand surface expression onmalignant glioma cells. Brain129:2416-2425.
18 WuA,WiesnerS,XiaoJ,EricsonK,ChenW,etal.(2007)ExpressionofMHCIandNKligandsonhumanCD133(+)gliomacells:Possibletargetsofimmunotherapy.JNeurooncol83:121-131.
19 Liu H, Liu Z, Li J, Li Q, You C, et al. (2014) Relative quantitativeexpression of hypoxia-inducible factor 1α messenger ribonucleicacidinrecurrentcraniopharyngiomas.NeurolIndia62:53-56.
20 Stevens A, Kloter I, RoggendorfW (1988) Inflammatory infiltratesandnaturalkillercellpresenceinhumanbraintumors.Cancer61:738-743
21 RansohoffRM,KivisäkkP,KiddG (2003)Threeormore routes forleukocyte migration into the central nervous system. Nat RevImmunol3:569-581.
22 EngelhardtB,RansohoffRM(2005)TheinsandoutsofT-lymphocytetraffickingtotheCNS:Anatomicalsitesandmolecularmechanisms.TrendsImmunol26:485-495.
23 ProescholdtM,MerrillM,StoerrEM,LohmeierA,DietmaierW,etal.(2011)ExpressionofcarbonicanhydraseIXincraniopharyngiomas.JNeurosurg115:796-801.
24 Vidal S, Kovacs K, Lloyd RV, Meyer FB, Scheithauer BW (2002)Angiogenesisinpatientswithcraniopharyngiomas:Correlationwithtreatmentandoutcome.Cancer94:738-745.
25 NishihiraJ(2000)MacrophageMigrationInhibitoryFactor(MIF):ItsEssential Role in the Immune System and Cell Growth. Journal ofInterferon&CytokineResearch20:751-762.
26 Pettorini BL, Inzitari R, Massimi L, Tamburrini G, Caldarelli M,et al. (2010) The role of inflammation in the genesis of the cysticcomponentofcraniopharyngiomas.ChildsNervSyst26:1779-1784.
27 PollardJW(2004)Tumour-educatedmacrophagespromotetumourprogressionandmetastasis.NatRevCancer4:71-78
28 Oljavo LS, Whittaker CA, Condeelis JS, Pollard JW (2010) Geneexpression analysis of macrophages that facilitate tumor invasionsupports a role for Wnt-signaling in mediating their activity inprimarymammarytumors.JImmunol184:702-712.
29 PukropT,KlemmF,HagemannTh,GradlD,SchulzM,etal. (2006)Wnt 5a signaling is critical for macrophage-induced invasion ofbreastcancercelllines.PNAS103:5454-5459
30 AmaguchiK,MoritaH,MohriN(1988)DistributionofHNK-1+cellsinmalignantlymphomas.ActaPatholJpn35:339-350,
31 Hölsken A, Gebhardt M, Buchfelder M, Fahlbusch R, BlümckeI, et al. (2011) EGFR signaling regulates tumor cell migration incraniopharyngiomas.ClinCancerRes17:4367-4377.
32 TagliaferriP,CaragliaM,BudillonA(2005)Newpharmacokineticandpharmacodynamicstoolsforinterferon-alpha(IFN-alpha)treatmentofhumancancer.CancerImmunolImmunother54:1-10
33 VasiljevaO,PapazoglouA,KrügerA,BrodoefelH,KorovinM,etal.(2006) Tumor cell-derived and macrophage-derived cathepsin Bpromotes progression and lung metastasis of mammary cancer.CancerRes66:5242-5250.
34 Hagemann T, Robinson SC, Schulz M, Trümper L, Balkwill FR, etal. (2004) Enhanced invasiveness of breast cancer cell lines uponco-cultivation with macrophages is due to TNF-α dependent up-regulation of matrix metalloproteases. Carcinogenesis 25: 1543-1549.