rupture of the tracheobronchial tree
TRANSCRIPT

Thorax 1987;42:681-688
Rupture of the tracheobronchial tree
J C ROXBURGH
From the Department of Thoracic Surgery, Norfolk and Norwich Hospital, Norwich
ABSTRACT Eleven cases of tracheobronchial rupture are described. Nine were the result of externalnon-penetrating trauma and all but three had other serious injuries. The remaining two were causedby endobronchial intubation. Of the cases caused by external injury, respiratory tract injury was
confined to the cervical trachea in three. Two required tracheostomy and repair and the third wasmanaged conservatively; all made satisfactory recoveries. Intrathoracic rupture was recognised on
or soon after admission in three cases. One patient died of uncontrollable pulmonary haemorrhagebefore he could be operated on; immediate repair gave good long term results in the other two. Inthree cases rupture of the main bronchus was not recognised until complete obstruction developedthree, five, and 12 weeks after the accidents. The strictures were resected and the lung re-expanded.Robertshaw endobronchial tubes ruptured the left main bronchus in two patients undergoingoesophageal surgery. Uneventful recovery followed immediate repair. The difficulty of confirmingrupture of a major airway is discussed and the importance ofconserving the lung when the diagnosishas been missed is emphasised.
Rupture of the tracheobronchial tree, althoughdescribed well over 1.00 years ago,' is a modern haz-ard. It is in the main associated with blunt trauma ofthe chest and is often an injury of high speed acci-dents. As the number of people travelling at highspeed has increased so has the number of those sus-taining injuries to the chest. Most patients with tra-cheobronchial ruptures will be seen in the accidentand emergency departments of general hospitals andmanaged initially by general or orthopaedic surgeonsor by neurosurgeons, depending on the extent of theirassociated injuries. The diagnosis of tracheobronchialrupture is not easy but failure to diagnose it may leadto death or long term disability. Once diagnosed itcan be managed conservatively while a thoracic sur-gical opinion is sought. A good result can beexpected.
Case histories
ACUTE INJURIES1(a) Cervical1 A 6 year old girl fell off her bicycle, sustained ablow to her neck, and soon afterwards coughed up a
Address for reprint requests: Department of Surgery, MiddlesexHospital, London WIN 8AA.
Accepted 4 March 1987
little blood. Her voice was slightly altered. The onlyabnormality on physical examination was surgicalemphysema around the neck and anterior chest wall.Bronchoscopy showed a 15 cm tear in the posteriorwall of the trachea, 2 cm below the vocal cords. Atracheostomy was the only surgical intervention.Repeat bronchoscopy one week after that showed thetear was healing and she was extubated two weekslater. There have been no long term sequelae.2 An 18 year old motorcyclist was admitted uncon-scious to the accident and emergency departmentafter a road traffic accident in which he was "gar-rotted" by his haversack strap. There were extensiveabrasions and surgical emphysema over the front ofhis neck. He was dyspnoeic but not cyanosed. Thefindings at the initial clinical examination were other-wise unremarkable. A chest radiograph showed afracture of the right first rib and mediastinalemphysema. Bronchoscopy showed disruption of thetrachea anteriorly and towards the right side. A tem-porary tracheostomy at the level of the third ring wasthe only treatment needed. He made an uneventfulrecovery.3 A 30 year old man sustained multiple orthopaedicinjuries in a light aeroplane crash. He was foundunconscious but soon recovered consciousness. Hehad a compound fracture dislocation of his left ankleand a closed dislocation of his left hip. In additionthere was bruising around a superficial laceration onthe right side of his neck. His voice was hoarse. Exam-
681
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from
682ination of his chest showed nothing remarkable. Thedislocations were reduced under general anaesthesiawithout incident, and only at the end of the operationwas it noticed that his neck had become swollen bysurgical emphysema. Bronchoscopy then showed acircumferential tear of the left side of the trachea 1 cmbelow the vocal cords. A nasoendotracheal tube wasused as a splint for one week. Three and a half yearslater his voice is a little husky as a result of the directinjury to the larynx but there has been no other dis-ability.
1(b) Intrathoracic (blunt trauma)4 A 16 year old stable lad fell from his horse andwas kicked in the front of his chest. He rapidlybecame unrecognisable as a result of widespreadsurgical emphysema and on admission to hospital hewas dyspnoeic and cyanosed. There were fracturesof the 2nd-6th ribs on the right side with a largepneumothorax. After insertion of an intercostal tube500 ml of fresh blood were drained from the chest andthere was a brisk and persistent air leak. Bron-choscopy confirmed laceration of the trachea extend-ing into the right main bronchus. At thoracotomy alarge intrapulmonary haematoma associated with alaceration in the upper lobe was noted. There wasa 3 cm tear in the membranous trachea running fromabove the origin of the left main bronchus obliquelyacross to join a semicircular tear between the first andsecond rings of the right main bronchus. The leftmain bronchus was selectively intubated, the lacer-ation was repaired with interrupted sutures, and thesuture line was protected with azygos vein and pleura.The patient made a rapid recovery and apart fromminor problems with suture granulomas in the earlymonths there were no complications. Thirteen yearsafter the incident he remained well.5 A 20 year old rider of a light motorcycle ran intothe back of an unlit stationary lorry. On admission tothe accident unit she was conscious, not shocked, andin no respiratory distress. She had a depressed frontalfracture of the skull, a fracture of the 4th thoracicvertebra with immediate paralysis, and a large rightpneumothorax. There was no surgical emphysema. Achest drain was inserted and after this blood gas ten-sions were found to be normal. Her condition deterio-rated two hours later and a very brisk air leak devel-oped. A chest radiograph showed the right lung hadfailed to re-expand fully. Bronchoscopy confirmedthat the bronchus was ruptured. At thoracotomythere was complete transection of the lower divisionof the right main bronchus, the tear extending spirallyinto the upper lobe bronchus. An upper lobectomyand a sleeve anastomosis (with interrupted 3/0absorbable sutures) were performed. Apart from atension pneumothorax on the left side, which devel-
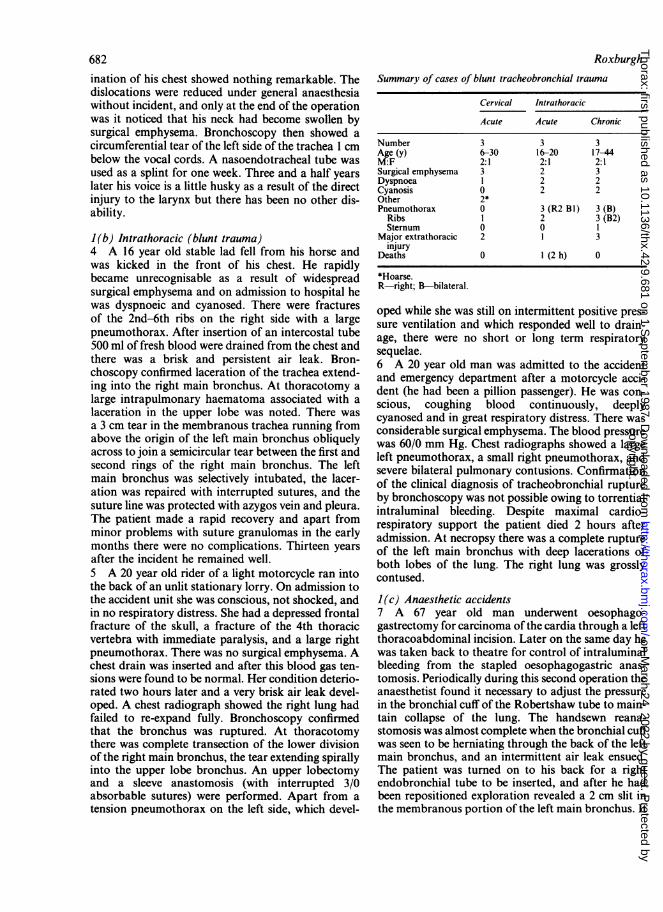
RoxburghSummary of cases of blunt tracheobronchial trauma
Cervical Intrathoracic
Acute Acute Chronic
Number 3 3 3Age (y) 6-30 16-20 17-44M:F 2:1 2:1 2:1Surgical emphysema 3 2 3Dyspnoea 1 2 2Cyanosis 0 2 2Other 2*Pneumothorax 0 3 (R2 B1) 3 (B)
Ribs 1 2 3 (B2)Sternum 0 0 1
Major extrathoracic 2 1 3injury
Deaths 0 1 (2 h) 0
*Hoarse.R-right; B-bilateral.
oped while she was still on intermittent positive pres-sure ventilation and which responded well to drain-age, there were no short or long term respiratorysequelae.6 A 20 year old man was admitted to the accidentand emergency department after a motorcycle acci-dent (he had been a pillion passenger). He was con-scious, coughing blood continuously, deeplycyanosed and in great respiratory distress. There wasconsiderable surgical emphysema. The blood pressurewas 60/0 mm Hg. Chest radiographs showed a largeleft pneumothorax, a small right pneumothorax, andsevere bilateral pulmonary contusions. Confirmationof the clinical diagnosis of tracheobronchial ruptureby bronchoscopy was not possible owing to torrentialintraluminal bleeding. Despite maximal cardio-respiratory support the patient died 2 hours afteradmission. At necropsy there was a complete ruptureof the left main bronchus with deep lacerations ofboth lobes of the lung. The right lung was grosslycontused.
I(c) Anaesthetic accidents7 A 67 year old man underwent oesophago-gastrectomy for carcinoma of the cardia through a leftthoracoabdominal incision. Later on the same day hewas taken back to theatre for control of intraluminalbleeding from the stapled oesophagogastric anas-tomosis. Periodically during this second operation theanaesthetist found it necessary to adjust the pressurein the bronchial cuff of the Robertshaw tube to main-tain collapse of the lung. The handsewn reana-stomosis was almost complete when the bronchial cuffwas seen to be herniating through the back of the leftmain bronchus, and an intermittent air leak ensued.The patient was turned on to his back for a rightendobronchial tube to be inserted, and after he hadbeen repositioned exploration revealed a 2 cm slit inthe membranous portion of the left main bronchus. It
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from
Rupture of the tracheobronchial tree
was repaired with interrupted sutures and coveredwith a pericardial flap. The patient made anuneventful recovery.8 A 78 year old woman with enormous achalasiawas undergoing oesophagectomy through a right tho-racotomy and had been intubated with a left Robert-shaw tube. While the upper oesophagus was beingmobilised surgical emphysema of the posterior medi-astinum was noted. When the overlying pleura wasincised an air leak developed, which becameprogressively larger. Exploration revealed that themembranous portion of the left main bronchus hadbeen perforated by the tip of the Robertshaw tube.The tube was withdrawn slightly and the defect easilyrepaired with three interrupted sutures. The operationwas completed without further incident and therewere no long term sequelae.
CHRONIC INJURIESPost-traumatic bronchial rupture9 A 44 year old male moped rider was a victim of aroad traffic accident and his left chest hit the kerb.When seen in the district general hospital he was dys-pnoeic but not cyanosed and there was gross surgicalemphysema over the anterior chest and neck. Therewas a large flail segment on the left side. A fracture ofthe base of the skull was diagnosed clinically. Chestradiographs confirmed multiple fractures of the leftribs and showed fractures of several right ribs. Bilat-eral pneumothoraces were present. Chest drains wereinserted and a tracheostomy was performed for pro-longed ventilation. Three weeks after the accident,with his lungs fully re-expanded and his rib fracturesstabilising, he was transferred from the intensive careunit to a general surgical ward, where he continued tomake slow progress. Two weeks later he complainedof vague discomfort in the chest wall and soon after-wards he became dyspnoeic and cyanosed. A chestradiograph showed complete collapse of the right lungwith mediastinal shift. He was referred for bron-choscopy, which showed the right main bronchus tobe stenosed just below its origin. The stricture wasresected and thick colourless mucus was sucked andexpressed from the collapsed lung. The right mainbronchus was reanastomosed with 3/0 non-absorbable sutures. The patient made an uneventfulrecovery, but later stuture granulomas necessitatedbronchoscopic removal of two of the non-absorbablesutures. A perfusion lung scan one year after injuryshowed good function on the side of the bronchialanastomosis but only moderate function on the left,where the chest wall had been more severely damaged.10 A 17 year old bicycle rider sustained severe crushinjuries to his head and chest. On arrival in the acci-dent and emergency department he was deeply uncon-scious and acutely hyperpnoeic. There was bruising
683
and gross surgical emphysema over the right chest andan obvious depressed fracture of the sternum. Therewas a large right sided pneumothorax and a smallerone on the left. Bilateral chest drains were inserted. Hewas admitted to a neurosurgical unit, whereexploratory burr holes were made and bronchoscopyand tracheostomy were carried out. Although bleed-ing made examination difficult, bronchoscopy wasreported as showing some oedema of both main bron-chi but no evidence of rupture. Two weeks later theright lung had not fully expanded despite intensivetreatment. He therefore had a repeat bronchoscopyand a stricture of the right main bronchus wasidentified. It was resected and an end to end anas-tomosis performed. Suture granulomas and a degreeof renewed stenosis necessitated several bron-choscopies and bronchial dilatations during the firsttwo years after operation but thereafter his respira-tory tract remained satisfactory.11 A 23 year old nurse had a road traffic accident inwhich she sustained very severe head injuries, frac-tures of the left clavicle, left 1st rib, right 1st and 2ndribs, bilateral pneumothoraces, and a fracture of theshaft of the right femur. At the hospital to which shewas admitted bilateral chest drains were inserted andwhen, 48 hours later, surgical enphysema hadincreased and she became hypoxic fibreoptic bron-schopy was performed. The right main bronchus wasreported to be oedematous but intact. She was trans-ferred to the nearest cardiothoracic centre for man-agement of her pulmonary complications; but herneurological condition was deteriorating, and withher respiratory function adequate she was moved tothe regional neurosurgical centre in yet another hospi-tal. After a brain scan she was kept under observationthere and made slow but steady progress. Three weekslater with her head injury improving and both lungsfully expanded she was fit enought to be transferred toan orthopaedic unit near her home for continuedmanagement of her fractured femur.
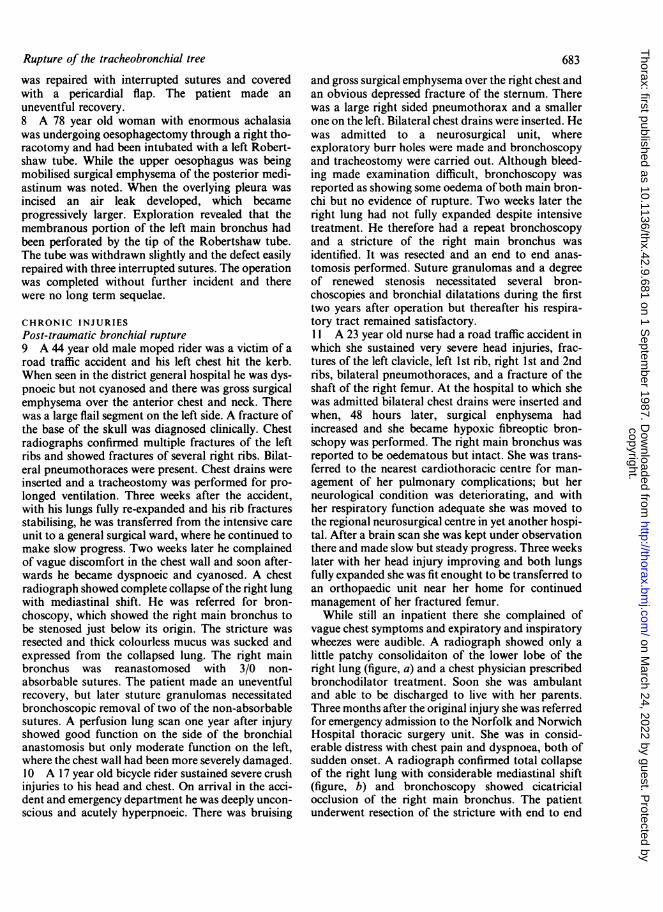
While still an inpatient there she complained ofvague chest symptoms and expiratory and inspiratorywheezes were audible. A radiograph showed only alittle patchy consolidaiton of the lower lobe of theright lung (figure, a) and a chest physician prescribedbronchodilator treatment. Soon she was ambulantand able to be discharged to live with her parents.Three months after the original injury she was referredfor emergency admission to the Norfolk and NorwichHospital thoracic surgery unit. She was in consid-erable distress with chest pain and dyspnoea, both ofsudden onset. A radiograph confirmed total collapseof the right lung with considerable mediastinal shift(figure, b) and bronchoscopy showed cicatricialocclusion of the right main bronchus. The patientunderwent resection of the stricture with end to end
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from

684anastomosis of the bronchus, a large amount of clearmucus being expressed from the collapsed lung.Recovery was uneventful and six months later respira-tory function tests, which included a flow-volumeloop, gave results within normal limits.
History
Rupture of the bronchus was first reported over 100years ago. Webb1 in 1848 reported the case of a manrun over by a cart who died from a ruptured liver. Atnecropsy the left main bronchus was found to be rup-tured. Winslow2 in 1871 recorded the first example ofsurvival from bronchial injury but the "patient" wasa wild canvasback duck. A rupture of the left mainbronchus had healed with development of a fibrouspouch. Nearly 60 years later the first human survivorwas reported by Kritzinski3 His patient was a womanwho had suffered severe right sided chest injuries atthe age of 10 years. When she died from pulmonarytuberculosis at the age of 31, necropsy showed that theright main bronchus had been completely occludedand there was no evidence of tuberculosis on that side.The disease that killed her was confined to the leftside.The first attempt at surgical repair was made in
1913 by Hotz,4 who operated on a 2 year old girl withan acute tracheobronchial rupture. The girl had beenrun over by a wine wagon and sustained severe chestinjuries. An emergency thoracotomy was performedas her condition deteriorated despite relief of her ten-sion pneumothorax. At operation a rupture of the leftmain bronchus was repaired. The child died on thefourth postoperative day from fulminant sepsis.Thereafter the surgical management of the problemscreated by bronchial rupture aimed at relieving thesymptoms of mediastinal shift or pulmonary sepsis.The mediastinal shift was treated by artificialpneumothorax5 or thoracoplasty6 or alternatively thelung was removed.6 Endoscopic dilatation or electro-cautery of the bronchial stenosis was also used.7Griffiths8 in 1948 was the first to report a successfullyresected post-traumatic bronchial stricture and threeyears later the first successful primary repair wasrecorded by Scannell.9
Roxburgh
Case 11: (a) six weeks and (b) 12 weeks after the originalinjury.
Incidence
In the 100 years following Webb's initial report 61cases were recorded and in the next 10 years (1948-58)a further 94,10 and by 1966 Chesterman"1 was able tocollect from the published reports over 200 cases. Inhis review he noted a male preponderance of 75%,and most patients were under 40 years of age. InBritain and the USA the vast majority of blunt chesttrauma arises from road traffic accidents, which mir-
rors the increase in the number of people engaging inhigh speed travel. Our experience suggests that tra-cheobronchial injury might be becoming more com-mon.The incidence of tracheobronchial rupture is
difficult to assess for two reasons. Firstly, manypatients die from more lethal and therefore more obvi-ous injuries before they reach hospital and, secondly,
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from

Rupture of the tracheobronchial tree
a proportion of patients present with its complicationslong after the accident. In a review12 of 1178 necrop-sies on trauma victims during the five years 1961-6there were 33 cases of tracheobronchial rupture.Twenty eight of these patients had died within twohours of the accident from other injuries. The injuryto the tracheobronchial tree was the cause of death inonly five of the 33 cases and only two of these hadreached hospital alive. Among 966 patients with chestinjuries reaching one hospital alive after road trafficaccidents, only seven cases of tracheobronchial rup-ture were found in 12 years, an incidence of 0-7%.'3A series of 353 patients with major chest injuries,treated in a referral centre over 10 years, was found toinclude eight (2-2%)."' The experience of 25 Britishthoracic surgeons led Bates'5 in 1977 to estimate thata thoracic surgeon in the United Kingdom would belikely to see no more than two cases, only one ofwhichwould be acute, in a working life of 30 years. The ninecases of tracheobronchial rupture in this seriesoccurred over a period of 15 years. The overall mor-tality rate in Burke's review of 167 bronchial ruptureswas 30%, with 52% of the deaths occurring within thefirst hour.'0 In most series about 80% of the injurieshave affected the region of the tracheobronchialjunction'6 17 and the above figures reflect the seri-ousness of intrathoracic rupture. Injuries to the cervi-cal trachea occur in 10-15% of cases'7 and are esti-mated to carry a 15% mortality from "hypoxia."' 8Life is more at risk in those with complete rupturethan in those with partial circumferential or longi-tudinal lacerations.
Mechanisms of traumatic injury
Schonberg'9 in 1912 was the first to propose a mech-anism of bronchial rupture. He postulated that in aclosed chest injury there is a reflex closure of the glot-tis and that this, along with the thoracic compression,causes a rapid rise in intraluminal pressure, which heargued would be highest in the larger airways. Thusrupture occurred once the pressure was too great forthe bronchial elasticity. The theory is supported byexperimental work on dogs,20 which showed afivefold increase in bronchial rupture when the chestwas compressed against a closed glottis. The experi-ments also indicated that the lateral force required tocause bronchial rupture is one third of that requiredin a vertical direction. Sudden anteroposterior com-pression of the chest increases its transverse diameterand as the lungs remain in contact with the chest walltraction on the relatively fixed carina is produced."The shearing force may well be too great for the elas-ticity of the bronchus and result in rupture.
All of these factors probably combine to cause theclassic bronchial ruptures, of which over 80% occur
685
within 2 5 cm of the carina. This is most likely whenthe chest wall is elastic and so compressible, whichmay in part explain the higher incidence in the young.Since these injuries are not usually associated withparenchymal or hilar vascular damage it has beenpostulated that extreme violence is not essential.2'This is supported by the findings of other work-ers,1' 18 who have shown that no more than half ofthese cases have associated injuries more severe thanrib fractures. By contrast, the many people sufferingextreme force to the chest, as evidenced by the inci-dence of other intrathoracic injuries, rarely sustaintracheobronchial injury, implying that the importantfactor is not the absolute force but the way in whichit is applied to the chest wall.The mechanism of cervical tracheal rupture is sim-
ple. The hyperextended neck causes the trachea to bestretched against the cervical spine. A direct blow tothe unprotected trachea then results in rupture, oftenwith no external evidence of trauma. Classically this issaid to occur when the car passenger hits the dash-board, the so called "padded dash syndrome."
Intubation inJury
Rupture of a major airway as a result of trachealintubation for anaesthesia is rare. Only five casesoccurred in over 2700 endobronchial intubations withCarlens tubes22; the two cases in this series occurredin a period of only two years. Single and double lumenred rubber and polyvinyl chloride (PVC) tubes haveall been implicated in tracheobronchial rupture.23 Aninexperienced operator, intubation stylets, and multi-ple attempts at intubation may all lead to ruptureregardless of the nature of the tube. The Robertshawtube, for example, curves in two planes and is madefrom stiff red rubber; the tip of the tube may thereforeproduce a laceration during placement or movementof the patient24 (case 8). Many red rubber tubes havehigh pressure cuffs, which when overinflated may leadto bronchial rupture25 (case 7); and if the cuff inflatesasymmetrically, as many of them do, it may also drivethe tip of the tube into the bronchial wall.2' Over-distension may occur when excessive volumes of airare injected in an attempt to obtain a good cuff seal orby diffusion of nitrous oxide into the balloon duringprolonged anaesthesia.2326 The newer, softer PVCtubes with low pressure concentric cuffs assume thehigh pressure characteristics of red rubber tubes ifmore than 3 ml of air is used to inflate the balloon.27Patients undergoing oesophageal surgery28 and thosewith chronic airways disease25 are said to be moresusceptible to this injury. Neonates as well as adultshave been affected, the premature infant being most atrisk.29 The use of suction catheters has led to tracheo-bronchial perforation, the resulting pneumothoraces
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from
686
requiring treatment by tube thoracostomy.30 In apostmortem study of 14 premature infants the seg-mental bronchi could be perforated with ease, while inthree term infants perforation did not occur.30
Diagnosis
As tracheobronchial rupture is a comparatively rarecondition, the diagnosis is easily missed. Except incases of injury to the cervical trachea in which therehas been a blow to the neck, the history is usuallynon-specific and clinical examination is seldom diag-nostic. A high index of suspicion is therefore neededin the treatment of all chest injuries. Dyspnoea hasbeen recorded in about 90% of cases,"1 31 -3 thedegree of respiratory distress varying with the rate andamount of air loss. Cyanosis and serious respiratoryembarrassment is present in 30% of cases. " 31 -37Surgical emphysema, including mediastinalemphysema, was found in only 65% ofpatients.'1 313. It may be slight (case 5) or massive(case 4). Haemoptysis is less frequent, occurring in20% of cases, 1 31 - 37 but it may be a major problem(case 6). About two thirds of patients will have apneumothorax, usually unilateral. Bilateral pneumo-thoraces occur in 5% of cases and are a major causeof hospital mortality" (case 6). Many authors'8 38consider a tension pneumothorax to be uncommonbut some quote an incidence as high as 25%."Two clinical types of bronchial rupture have been
described.39 Type I is obvious; the torn bronchusopens into the pleural cavity, a large pneumothoraxdevelops, there is a brisk and inexhaustable air leak ondrainage, the lung fails to expand, and indeed thepatient's condition may worsen quite dramatically.The diagnosis of tracheobronchial rupture is all butconfirmed. In type II the situation is quite different.There is little or no communication with the pleuralcavity and the pneumothorax if present is usuallysmall and responds to drainage, the pleural leak soonbecoming sealed with fibrin. Fractured ribs, especiallythe upper three, have been said to be relevant indiagnosis40 but their significance seems to have beenexaggerated. In 200 cases of bronchial rupture "chestwall fractures" were present in no more than onethird." This is explained by the elasticity of the chestwall in the comparatively young victims. Conversely,in 140 patients with first rib fractures, 15 of whichwere bilateral, there were only three examples of bron-chial rupture4' 42 and in 823 cases of multiple ribfractures there were only seven tracheobronchial rup-tures. ' Two radiological findings which may be ofhelp are deep cervical emphysema, seen in films of theupper mediastinum,43 and the rare "fallen lung sign,"in which the transected bronchus allows the lung tofall away from the mediastinum instead of towards it,
Roxburghas is the case in an ordinary pneumothorax.44Some points regarding injuries to the cervical tra-
chea merit special mention. With little or no localevidence of trauma symptoms may range from thoseso slight as to be disregarded to those of severe respi-ratory obstruction, with only the pretracheal fasciamaintaining the patency of the airway. This is illus-trated by a case of Bessor and Saegesser. 7 A womanwalked to hospital holding her head after a 60 mph(96 km/h) collision in the car she had been driving.There was no surgical emphysema and her chestradiograph was normal, but when her head was tiltedto take a Townes view of her cervical spine shesuffocated. At necropsy there was complete transec-tion of the cervical trachea.
Serious extrathoracic injuries may delay the recog-nition a tracheobronchial rupture for weeks ormonths, as in our cases 9, 10, and 11. They are foundin only half of all cases1' 18 and their presence doesnot help in assessing the likelihood tracheobronchialrupture. The early diagnosis of tracheal and bronchialrupture may be difficult. Only 53% of cervical and40% of bronchial ruptures were diagnosed within 48hours.'6 The essential investigation is bronchoscopy;but this is not always conclusive and cases 10 and 11illustrate that even an experienced bronchoscopistlooking for ruptures may be misled, particularly whenbleeding from further down obscures the view.Another bronchoscopy after the bleeding has ceasedis indicated if the slightest doubt remains.
Treatment and outcome
The initial treatment of tracheobronchial rupture con-sists of maintenance of the airway, reversal of shock,and relief of the pneumothorax. Ideally, definitive sur-gical repair follows immediately; but when the patientis unfit for emergency thoracotomy the passage of anendotracheal or endobronchial tube to ventilate thedistal tracheobronchial tree may stabilise a deterio-rating respiratory function. The repair may then beperformed later if the patient's condition improves. Insome patients with multiple injuries treatment ofmoresevere extrathoracic injuries may take precedence.
Small tears of the cervical trachea may be managedby tracheostomy alone or by splinting with anasotracheal tube. Complete transections of the tra-chea, however, should be managed by careful suture,care being taken to avoid damage to the recurrentlaryngeal nerves. A tracheostomy is sited below orthrough the anterior wall of the repaired airway, pro-tecting it from the peritracheal oedema that developsin the first few postoperative days. The tracheostomyis allowed to close when there is bronchoscopic evi-dence of healing, usually at 7-14 days. The manage-ment of the late sequelae of cervical rupture, such as
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from
Rupture of the tracheobronchial tree
subglottic stenosis, is best undertaken in a specialistcentre.
While small lacerations have been successfully man-aged conservatively,45 primary repair of bronchialrupture is the treatment of choice. There need be nocause for concern about the blood supply to the distalbronchus. It has been shown that the collateral supplyfrom the pulmonary arteries is more than adequate tosupply the distal bronchi,46 and end to end anas-tomosis after sleeve resection is a well established pro-cedure. Growth is also possible at the anastomosis, asshown by the successful repair of injuries in the youngchild.47 The edges are debrided, the mucosa is care-fully approximated, and the end to end anastomosis isfashioned, non-absorbable sutures being used. Thesuture line is protected by a pedicled pericardial,pleural, or intercostal muscle flap. Resection ofpulmonary tissue, as in case 5, may be required in themore extensive ruptures.
Late presentation of bronchial rupture with pul-monary collapse and stricture formation requirestreatment along much the same lines. Provided thatthere is no distal suppuration, reconstruction shouldbe attempted regardless of the time that has elapsedsince the original injury. Operations as long as 15years after the original injury have led to partial recov-ery of pulmonary function.48 Complete bronchialstenosis causing complete pulmonary atelectasis tendsto prevent suppuration49 (cases 9 and I 1). This clin-ical observation has been confirmed experimentally.50It is important to aspirate and express all of the thickcolourless mucus that has collected in the collapsedlung to assist re-expansion. In some cases irreversiblefibrosis will have occurred and conservation is notpossible. Three quarters of post-traumatic stricturesare managed by resection and reanastomosis alone. 17The remainder are treated by resection of the infectedor fibrosed lung, two thirds of these cases requiringpneumonectomy. 17The results of treatment of injuries to the cervical
trachea are good,5' as cases 1-3 show; but associatedlesions may cause long term morbidity. Injury of thelarynx and trauma to the recurrent laryngeal nervemay result in a permanently hoarse voice or whisperspeech.Good long term results may be expected in 90% of
patients with bronchial rupture treated by earlyrepair.18 In the early postoperative months, however,suture granulomas are not infrequent when non-absorbable sutures have been used. Suture granu-lomas may present with stridor or wheezing but thesputum is not always blood stained; anastomotic stric-tures may present with varying degrees of respiratoryembarrassment. Endoscopic suture removal with orwithout bronchial dilatation is all that is required inmany cases (cases 4, 9, and 10).
687
Full recovery of respiratory function may take upto one year52 and in many cases recovery is onlypartial. The left to right shunt that develops betweenthe pulmonary and bronchial arteries during theperiod of atelectasis may not be completely revers-ible."5 The concomitant parenchymal damage toeither lung or indeed the residual deformity of thethoracic cage may be contributory factors (case 9).The correct early diagnosis of tracheobronchial
rupture will lead to a reduction in the long term mor-bidity associated with this condition, and possiblyincreased survival. The responsibility for the earlydiagnosis and initial management lies in many caseswith general, orthopaedic, or neurological surgeons.These surgeons must therefore be aware of thisimportant, albeit uncommon, injury. The widespreaduse of fibreoptic bronchoscopy should enable regularexaminations of the suspect tracheobronchial tree toconfirm or refute the diagnosis. In cases whereeffective intrabronchial suction is required, however,rigid bronchoscopy remains the investigation ofchoice.
I wish to thank Mr W F Kerr, Mr C Parish, and MrB A Ross for allowing me to report their cases.
References
I Webb A. Pathalogica indica or the anatomy of indiandiseases. 2nd ed. Calcutta: Thacker, 1848:147.
2 Winslow WH. Rupture of bronchus of wild duck. Phila-delphia Medical Times 1871;1:225.
3 Krinitzki SI. Zur Kasuistik einer vollstandigenZerreibung des rechten Luftrohrenastes. VirchowsArch Pathol Anat 1928;266:815-9.
4 Vierheilig J. Die subkutane Bronchuszerreibung.Beitrage zur Klinischen Chirugie 1914;93:201-21.
5 Clerf LH. Rupture of main bronchus from externalinjury. Surgery 1940;7:276-9.
6 Kinsella TJ, Johnsrud LW. Traumatic rupture of thebronchus. J Thorac Surg 1947;16:571-83.
7 Loeffler L, Nager F. Uber traumatische Bronchostenoseund ihre Behandlung. Schweiz Med Wochenschr1941 ;71:293-7.
8 Griffith JL. Fracture of the bronchus. Thorax 1949;4:105-9.
9 Scannell JG. Rupture of the bronchus following closedinjury to the chest. Ann Surg 1951;133:127-30.
10 Burke JF. Early diagnosis of traumatic rupture of thebronchus. JAMA 1962;181:682-6.
11 Chesterman JT, Satsangi PN. Rupture of the trachea andbronchi by closed injury. Thorax 1966;21:21-7.
12 Bertelsen S, Howitz P. Injuries of the trachea and bron-chi. Thorax 1972;27:188-94.
13 Alyono D, Perry JF. Impact of speed limit I. Chestinjuries: review of 966 cases. J Thorac Cardiovasc Surg1982;83:519-22.
14 Dougall AM, Paul ME, Finley RJ, et al. Chest trauma-
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from
688current morbidity and mortality. J Trauma 1977;17:547-53.
15 Bates M. Rupture of the bronchus. In: Williams WG,Smith RE, eds. Trauma of the chest (the Coventryconference). Bristol: John Wright and Sons, 1977:142-50.
16 DorJ, Forster E, Le Brigand H. Rupture traumatiques desbronches et de la trachee thoracique. Vol 1. Paris: Doin,1964:232.
17 Beeson A, Seagesser F. A colour atlas ofchest trauma andassociated injuries. Vol 2. London: Wolfe Medical,1983:12.
18 Kirsh MM, Orringer MB, Behrendt DM, Sloan H.Management of tracheobronchial disruption second-ary to non penetrating trauma. Ann Thorac Surg1976;22:93-101.
19 Schonberg S. Bronchialrupturen bei thoraxkompression. Berl klin Wochenschr 1912;49:2218-21.
20 Lloyd JR, Heydinger DK, Klassen KP, Roetlig LC.Rupture of the main bronchi closed chest injury. ArchSurg 1958;77:597-605.
21 Black JBMcK, Lawson RAM. Rupture of the bronchusfollowing closed injury to the chest. J R Coll SurgEdinb 1970;15:21-6.
22 Guernelli N, Bragaglia RB, Briccoli A, Mastorilli M,Vecchi R. Tracheobronchial ruptures due to cuffedCarlens tubes. Ann Thorac Surg 1979;28:66-8.
23 Burton NA, Fall SM, Lyons T, Graeber GM. Rupture ofthe left main-stem bronchus with a polyvinylchloridedouble-lumen tube. Chest 1983;83:928-9.
24 Heisser M, Steinberg JJ, MacVaugh H, Klineberg PL.Bronchial rupture, a complication of use of theRobertshaw double-lumen tube. Anesthesiology1979;51:88.
25 Smith BAC, Hopkinson RB. Tracheal rupture duringanaesthesia. Anaesthesia 1984;39:894-8.
26 Forster JMG, Lau OJ, Alimo EB. Ruptured bronchusfollowing endobronchial intubation. Br J Anaesthiol1983;55:687-8.
27 Brodsky JB, Shulman MS, Mark JBD. Airway rupturewith a disposable double lumen tube [etter]. Anesthe-siology 1986;64:415.
28 Wagner DL, Gammage GW, Wong ML. Tracheal rup-ture following the insertion of a disposable double-lumen tube. Anesthesiology 1985;63:698-700.
29 McLeod BJ, Sumner E. Neonatal tracheal perforation.Anaesthesia 1986;41:67-70.
30 Anderson KD, Chandra R. Pneumothorax secondary toperforation of seqential bronchi by suction catheters. JPediatr Surg 1976;11:687-93.
31 Mazzei EA, Mulder DG. Closed chest injuries to thetrachea and bronchus. Arch Surg 1970;100:677-80.
32 Collins JP, Ketharanathan V, McConchie I. Rupture ofmajor bronchi resulting from closed chest injuries.Thorax 1973;28:371-5.
33 Grover FL, Ellestad C, Arom KV, Root D, Cruz AB,Trinkle JK. Diagnosis and management of majortracheobronchial injuries. Ann Thorac Surg
Roxburgh1979;28:384-91.
34 Deslauriers J, Beaulieu M, Archambault G, LaForge J,Bernier R. Diagnosis and long term follow up ofmajorbronchial disruptions due to nonpenetrating trauma.Ann Thorac Surg 1982;33:32-9.
35 Mills SA, Johnston FR, Hudspeth AS, Breyer RH,Myers RT, Cordell AR. Clinical spectrum of blunttracheobronchial disruption illustrated by seven cases.J Thorac Cardiovasc Surg 1982;84:49-58.
36 Amauchi W, Birolini D, Branco PD, Oliveira MRD.Injuries to the tracheobronchial tree in closed trauma.Thorax 1983;38:923-8.
37 Jones WS, Mavroudis C, Richardson D, Gray LA, HoweWR. Management of tracheobronchial disruption
-*resulting from blunt trauma. Surgery 1984;95:319-22.38 Wiot JF. Tracheobronchial trauma. Semin Roentgenol
1983;18:15-22.39 Davies D, Hopkins JS. Patterns in traumatic rupture of
the bronchus. Injury 1973;4:261-4.40 Crawford WO. Pulmonary injury in thoracic and non
thoracic injury. Radiology 1973;11:527-41.41 Albers JE, Rath RK, Glaser RS, Poddar PK. Severity of
intrathoracic injuries associated with first rib fractures.Ann Thorac Surg 1982;33:614-8.
42 Woodring JH, Fried AM, Hatfield DR, et al. Fracturesof the first and second ribs: predictive value for arterialand bronchial injury. AJR 1982;138:211-5.
43 Eijgelaar A, Van der Heide NH. A reliable early symp-tom of bronchial or tracheal rupture. Thorax 1970;25:116-25.
44 Oh KS, Fleischner FG, Wyman SM. Characteristic pul-monary finding in traumatic complete transection of amain-stem bronchus. Radiology 1969;92:371-2.
45 McMillan I. In discussion. Bates M. Rupture of the bron-chus. In: Williams WG, Smith RE, eds. Trauma of thechest (the Coventry conference). Bristol: John Wrightand Sons, 1977:151-2.
46 Ellis FH, Grindley JH, Edwardes JE. The bronchialarteries: 1-Experimental occlusion. Surgery 1951;30:810-26.
47 Rahbar A, Chang FC, Farha SJ. Rupture of the bron-chus: case report of successful resection and anas-tomosis in a 13 month infant. J Trauma 1978;18:140-1.
48 Samson PC. In discussion: Mahaffey DE, Creech 0,Boren HG, DeBakey ME. Traumatic rupture of theleft main bronchus successfully repaired eleven yearsafter injury. Thorac Surg 1956;32:331.
49 Paulson DL. Traumatic bronchial rupture with plasticrepair. J Thorac Surg 1957;22:636-45.
50 Tannenberg J, Pinner M. Atelectasis and bronchiectasis.J Thorac Surg 1942;11:571-616.
51 Wychulis AR, Neville WE. Tracheal and bronchialreconstructive procedures. Surg Gynecol Obstet1974;139:433-55.
52 Logeais Y, Florent D, Danrigal A, et al. Traumaticrupture of the right main bronchus in an eight yearold child successfully repaired eight years after injury.Ann Surg 1970;172:1039-47.
copyright. on M
arch 24, 2022 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.42.9.681 on 1 Septem
ber 1987. Dow
nloaded from