rural emergency medical services - princeton university
TRANSCRIPT

Rural Emergency Medical Services
November 1989
OTA-H-445NTIS order #PB90-159047
Recommended Citation:
U.S. Congress, Office of Technology Assessment, Rural Emergency Medical Serv-ices—Special Report, OTA-H-445 (Washington, DC: U.S. Government Printing Office,November 1989).
Library of Congress Catalog Card Number 89-600774
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402-9325
(order form can be found in the back of this report)
Foreword
The problems of health care in rural areas have long occupied a special nichein policies designed to advance the Nation’s health. Programs for recruitment,training, and deployment of health care personnel, for constructing health carefacilities, and for financing health care, often have included special provisions forrural areas. These programs have often also included attempts to mitigate thenegative impacts on rural areas of policies primarily designed for and responsiveto the needs of urban areas. However, some rural areas continue to have high num-bers of hospital closures, ongoing problems in recruiting and retaining health per-sonnel, and difficulty in providing medical technologies commonly available inurban areas. Mounting concerns related to rural residents’ access to health careprompted the Senate Rural Health Caucus to request that OTA conduct an as-sessment of these and related issues. The first OTA paper prepared in connectionwith this assessment, Defining “Rural” Areas: Impacts on Health Care Policyand Research, was published in July 1989.
This Special Report, Rural Emergency Medical Services, is the second paperprepared in connection with that assessment. This report finds that many StateEMS systems are fragmented and lacking resources to remedy EMS problemsin rural areas. Many rural EMS programs lack specialized EMS providers, haveinadequate EMS transportation and communications equipment, and are not partof a planned regional EMS system. The report describes the availability and dis-tribution of emergency medical service (EMS) resources (e.g., personnel, trans-portation, facilities) and examines how limited Federal resources can be used toimprove rural EMS. In addition, the report discusses how Federal EMS resourcesmight be targeted to States’ rural areas.
This report is based, in part, on a May 1989 Rural EMS Workshop that wascosponsored by the Department of Transportation. Valuable guidance was providedby an advisory panel, chaired by Mr. James Bernstein of the North CarolinaDepartment of Human Resources. A number of other experts also provided in-formation and reviewed a draft of the report. The final responsibility for the con-tent of this report rests with OTA. Maria Hewitt was the primary author of thisstudy.

Advisory Panel—Rural Health Care
James Bernstein, Panel ChairDirector, Office of Health Resources DevelopmentNorth Carolina Department of Human Resources
Robert BerglandExecutive Vice President and General ManagerNational Rural Electric Cooperative
AssociationWashington, D.C.
James ColemanExecutive DirectorWest Alabama Health Services, Inc.
Sam CordesProfessor & HeadDepartment of Agricultural EconomicsUniversity of WyomingElizabeth DichterSenior Vice President for Corporate StrategiesLutheran Health SystemsDenver, Colorado -
Mary EllisDirectorIowa Department of
Kevin Fickenscher
Public Health
Assistant Dean and Executive DirectorMichigan State UniversityCenter for Medical StudiesKalamazoo, Michigan
Roland GardnerPresidentBeaufort-Jasper (South Carolina)
Comprehensive Health Center
Robert GrahamExecutive Vice PresidentAmerican Academy of Family PhysiciansKansas City, Missouri
Alice HershExecutive DirectorFoundation for Health Services ResearchWashington, D.C.David KindigDirectorPrograms in Health ManagementUniversity of Wisconsin-Madison
T. Carter Melton, Jr.PresidentRockingham Memorial HospitalHarrisonburg, Virginia
Jeffrey MerrillVice PresidentRobert Wood Johnson FoundationPrinceton, New JerseyMyrna PickardDeanSchool of NursingUniversity of Texas-Arlington
Carolyn RobertsPresidentCopley Health Systems, Inc.Morrisville, Vermont
Roger RosenblattProfessor & Vice ChairmanDepartment of Family MedicineUniversity of WashingtonPeter SybinskyDeputy Director for Planning, Legislation, and
OperationsHawaii Department of Health
Fred TinningPresidentKirksville College of Osteopathic MedicineKirksville, Missouri
Robert VraciuVice PresidentMarketing & PlanningHealthTrust, Inc.Nashville, Tennessee
Robert WalkerChairmanDepartment of Family and Community HealthMarshall University School of MedicineHuntington, West Virginia
NOTE: OTA appreciates and is grateful for the valuable assistance and thoughtful critiques provided by the advisorypanel members. The panel does not, however, necessarily approve, disapprove, or endorse this report. OTAassumes full responsibility for the report and the accuracy of its contents.
iv

OTA Project Staff—Rural Emergency Medical Services
Roger C. Herdman, Assistant Director, OTAHealth and Life Sciences Division
Clyde J. Behney, Health Program Manager
Elaine Power, Project Director, Rural Health Care (May 1989 to present)
Larry Miike, Project Director, Rural Health Care (August 1988 to June 1989)
Administrative Staff
Virginia H. Cwalina, Administrative Assistant
Carol A. Guntow, P.C. Specialist
Karen T. Davis, Secretary/Word Processor Specialist
Carolyn Martin, Secretary
Report Staff
Maria Hewitt, Study Director
Contractors
Jonathan Chin, University of MarylandHarvey Wolfe and Larry J. Shuman, University of Pittsburgh
Don G. Stamper, University of Missouri
Other Contributor
John L. Chew, Jr., Department of Transportation
Reviewers
OTA staff would like to express its appreciation to the following people for providing information and assistance.Susan BakerDirector, Injury Prevention CenterThe Johns Hopkins UniversitySchool of Hygiene and Public
HealthBaltimore, Maryland
Kathleen A. ClineEMS Medical DirectorPitt CountyGreenville, North Carolina
Jerry CoopeyOffice of Rural Health PolicyHealth Resources and Services
AdministrationRockville, Maryland
Jake CulpOffice of Rural Health PolicyHealth Resources and Services
AdministrationRockville, Maryland
Charles DetwilerPennsylvania Department of
HealthDivision of EMSHarrisburg, Pennsylvania
Gerald DoeksenDepartment of Agricultural
EconomicsOklahoma State UniversityStillwater, Oklahoma
Irene Fraser, PhDDivision of Health PolicyAmerican Hospital AssociationChicago, Illinois
George Garnett, M.D.Soldotna, Alaska
Michael GilbertsonDirectorNew York Department of Health,
EMS ProgramAlbany, New York
Victor GrimesSouth Carolina Department of
Health and EnvironmentalControl
Divison of EMSColumbia, South Carolina
Theodore W. HalpinScottsville, New York
Norman W. Hanson, Jr.Chief, EMS, Health Resources
DivisionMinnesota Department of HealthMinneapolis, Minnesota
Lawrence HughesDivision of Health PolicyAmerican Hospital AssociationChicago, Illinois
Ellen HumeNational EMS ClearinghouseThe Council of State GovernmentsLexington, Kentucky
Mark S. JohnsonCoordinator, Emergency Medical
ServicesAlaska Department of Health and
Social ServicesDivision of Public HealthJuneau, Alaska
Sandra W. JohnsonDirectorMaine Health Information CenterAugusta, Maine
Richard W. LooserExecutive DirectorWest Alabama Emergency
Medical Services, Inc.University, Alabama
Sue MaddenDirector of the Health Services
Information DivisionPublic Health FoundationWashington, D.C.
Carol MillerMountain ManagementOjo Sarco, New Mexico
Craig L. OlesenMedical Education DivisionAmerican Medical Resource
InstituteNorthbrook, Illinois
Janet ReichAdministrative DirectorRural Support Services Rose
Medical CenterEvergreen, Colorado
Thomas RickettsHealth Services Research CenterUniversity of North CarolinaChapel Hill, North Carolina
Dave SamuelsArizona EMS PhysiciansMeza, Arizona
John Spoor, MDDirector of Emergency ServicesMary Imogene HospitalCooperstown, New York
Scott SteinYork HospitalYork, Pennsylvania
E. Jerry SpykeSenior Public Health AdvisorCenter for Chronic DiseaseCenters for Disease ControlAtlanta, Georgia
Kathleen StageNational Association EMS
PhysiciansPittsburgh, Pennsylvania
Thorn SwanSedro Woolley, Washington
Gene WillardTexas Department of HealthAustin, Texas
Elizabeth WennarU.S. General Accounting OfficeWashington D.C.
Connie YeakleyOregon Health Division, EMS
SectionPortland, Oregon
NOTE: OTA appreciates and is grateful for the valuable assistance and thoughtful critiques provided by the reviewers. The reviewersdo not, however, necessarily approve, disapprove, or endorse this report. OTA assumes full responsibility for the reportand the accuracy of its contents.
vi

ContentsPage
CHAPTER 1. Summary and Policy Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .EMS IN A RURAL CONTEXT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Cardiac Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Trauma Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
OPTIONS FOR FEDERAL POLICY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Federal Initiatives in EMS Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Federal Guidelines or Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Federal EMS Technical Assistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Federally Sponsored EMS Research and Demonstration Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . .Federal Incentives for Planning and EMS Systems Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 2. Definition of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .EMERGENCY MEDICAL SERVICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Public Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prehospital Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Medical Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
RURAL AREAS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 3. The Demand for EMS Services in Rural Areas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .URBAN AND RURAL DIFFERENCES IN DEMAND FOR EMS SERVICES . . . . . . . . . . . . . . . . . .
Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 4. EMS in a Rural Context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .THE CHANGING RURAL HEALTH CARE ENVIRONMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .RURAL HEALTH CARE SYSTEMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Public Access to EMS Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prehospital Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Transportation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Medical Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Medical Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Regionalization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 5. Emergency Cardiac and Trauma Care in Rural Areas . . . . . . . . . . . . . . . . . . . . . . . . . . .CARDIAC CARE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .TRAUMA CARE... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Prevention Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prehospital Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hospital-Based Trauma Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Regionalization of Trauma Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHAPTER 6. Federal Policies Toward State Emergency Medical Services . . . . . . . . . . . . . . . . . . . . . .DEPARTMENT OF HEALTH AND HUMAN SERVICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .DEPARTMENT OF TRANSPORTATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Section 402 Funds for State Highway Safety Plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Section 403 Highway Safety Research and Demonstration Funds . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
DHHS AND DOT ALLOWABLE EMS EXPENDITURES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Appendix A. Rural EMS Workshop Participant\ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Appendix B. Designing an Appropriate EMS System in Rural Areas: Use of a
Computer Simulation Model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Appendix C. Trauma Service Designation Guidelines of the American College of Surgeons
and the American College of Emerging Physicians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Appendix D. Oregon Trauma Systems Summary and Hospital Resource Criteria . . . . . . . . . . . . . . . . . . . .Appendix E. Trauma Care/EMS Legislation Introduced During the 101st Congressional Session . . . . . .
11234567899
131313131414
17171718
252525252834373940
43434546464748
53535659606060
63
64
677989
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
vii

Contents-Continued
BoxesBox Page4-A. Rural EMS Communications: Problems and Potential Solutions as Presented at the
“National Rural EMS Needs Workshop, ” March 1989 . . . . . . . . . . . . . . . . ., . . . . . . . . . . . . . . . . . . . . 284-B. Prehospital Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304-C. EMS Prehospital Personnel: Problems and Potential Solutions as Presented at the
“National Rural EMS Needs Workshop, ” March 1989 .., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
FiguresFigure Page3-1. Death Rates From Unintentional Injury, Suicide, and Homicide by Place of Residence, 1977 -79.. 213-2. Motor Vehicle Related Death Rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223-3. Population Density . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223-4. Death Rates From Motor Vehicle Crashes by Place of Residence, 1977-79 . . . . . . . . . . . . . . . . . . . . . 234-1. A Nodal Concept of EMS for Rural Northeast Missour i . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364-2. Estimated U.S. Air Ambulance Distribution, 1988 .. ... ... ..,.,. ............ ... . 384-3. U.S. Helicopter Medevac Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 395-l. States Having All, None, or Some of Eight Essential Components of a Regional Trauma
System According to American College of Surgeons’ Criteria. 1987 . . . . . . . . . . . . . . . . . . . . . . . . . . . 495-2. StateTrauma Center Designation and Verification Practices, 1986-87 . . . . . . . . . . . . . . . . . . . . . . . . . . 506-1. State EMS Program Funding. 1988 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 536-~. State and Community Highway Safety Program Obligations (DOT Section 402)
Fiscal Year 1987—$111,539,200 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
TablesTable Page3-1. Prevalence of Injuries and Illness Among Patients Transported by Ambulance in Texas, 1988 . . . . 183-2. Prevalence of Injury and illness Among Calls for EMS Services in South Carolina, 1988 . . . . . . . . 193-3. Number of Episodes of Persons Injured and Number of Associated Restricted-Activity Days
and Bed Days by Whether in Moving Motor Vehicle, Whether at Work, Place of Accident,and Place of Residence: United States, 1987 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
3-4. Average Annual Number of Injuries Per 100 Persons Per Year, by Place of Residence andType of Injury: United States, 1980-81 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
3-5. Death and Disabling Injury Rates Among Workers by Industry, 1988 . . . . . . . . . . . . . . . . . . . . . . . . . . 223-6. Passenger Car Occupant Injury by Land Use and Speed Limit, 1986 . . . . . . . . . . . . . . . . . . . . . . . . . . . 243-7. Metropolitan (MSA) and Non-Metropolitan (Non-MSA) Motor Vehicle Fatality Rates-1986,
and Impact of 30 Percent Reduction in Non-MSA Deaths on Achieving the National 1990Objective for Injury Prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
4-1. State EMS Communications, 1986-87 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 274-~. Currency Certified Prehospital providers by State, 1986-87 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324-3. Ratios of Helicopters to Population by State, 1988, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 374-4. Percent of Community Hospitals With EMS-Related Services in Metropolitan and
Nonmetropolitan Hospitals by Bed Size, 1987 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 415-1 . Deaths Attributed to Cardiovascular Disease by MSA/non-MSA Residence, 1986 . . . . . . . . . . . . . . . 445-2. Percent oif Persons 18 Years of Age and Over Who Wore Seatbelts All or Most of the Time
When Riding in a Car by Sex, Age. and Residence: United States, 1985 . . . . . . . . . . . . . . . . . . . . . . . . 475-3. Percent occurrent Drinkers 18 Years and Over Who Had Driven a Car At Least Once in the
Past Year When They Thought They Might Have Had Too Much To Drink By Sex, Age, andResidence: United States, 1985 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
6-1 . State Expenditures for Emergency Medical Services, By Source of Funds, FY 1988 . . . . . . . . . . . . . 546-~. Distribution of preventive Health and Health Services Block Grant Expenditures of State
Health Agencies to Former Categorical Grant Areas, Fiscal Year 1988 . . . . . . . . . . . . . . . . . . . . . . . . . 576-3. Preventive Health and Health Services Block Grant Expenditures: Emergency Medical
Services, Fiscal Years 1982-1988 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 596-4. National Highway Traffic Safety Administration’s State and Community Highway Safety
Program (Section 402) Funding: Emergency Medical Services, Fiscal Years 1967-87 . . . . . . . . . . . . 596-5. National Highway Traffic Safety Administration’s Research and Demonstration Program
(Section 403) Funding: Emergency Medical Services, Fiscal Years 1981-88 . . . . . . . . . . . . . . . . . . . . 61
Vlll

Chapter 1
Summary and Policy Options
INTRODUCTION
The average U.S. resident will need ambu-lance service at least twice in his or her lifetimeand for some of these patients, delays inreceiving emergency care will contribute todeath or permanent injury. The one-quarter ofAmericans who live in rural areas, whichoccupy four-fifths the country’s land area, facespecial problems in receiving emergency care. Itis difficult to deliver emergency medical serv-ices (EMS) to widely dispersed populationsquickly and in small rural communities, theremay be less than one emergency call a day. Thisrelatively low volume of calls may mean that arural ambulance service cannot support itselffinancially and that rural EMS providers havedifficulty maintaining their specialized skills.The time it takes to reach emergency patientsmay always be longer in some rural areas thanin urban areas because of distances betweenservices and rural residents. Although problemsrelating to population dispersion are not easilyamenable to intervention, many of the problemsrural EMS providers are having in deliveringEMS care can be alleviated with additionalresources and system-wide planning.
Well-organized EMS systems are widelyrecognized as essential components of medicalcare. For rural residents for whom no localhospital is available, EMS may be particularlyimportant in helping residents to achieve physi-cal access to health care. Emergency medicalservices cannot replace basic primary careservices, but when medical emergencies occur,a well-organized EMS system can offer rapidmedical assistance and transportation to a facil-ity equipped to handle the emergency.
Emergency medical services include the person-nel, vehicles, equipment, and facilities used todeliver medical care to those with an un-predicted immediate need outside a hospital and
continued care once in an emergency facility(128).1 EMS systems are usually organized atthe State or regional level to provide coordinateddelivery in an appropriate geographic area (62).The primary goals of an EMS system are to:
●
●
●
provide immediate medical assistance atthe scene and while in transit;provide rapid transportation to a medicalfacility;have a coordinated, tiered level of hospitalcare so that the most seriously injured or illpatients are quickly triaged to specializedfacilities for their care, while the lessseverely injured or ill patients are cared forat less specialized facilities.
Comprehensive EMS systems have beenshown to save lives and reduce disabilities(76,128). Among the EMS system components
are required are:
quick public access,on-the-scene emergency care personnel,rapid transportation,physicians trained to provide EMS care andsupervise prehospital care,different levels of hospital care for treat-ment of patients with emergent conditionsranging from ‘‘urgent care’ to life-threatening trauma, andEMS surveillance systems to facilitatesystem evaluation.
A well-organized EMS system may enhancehealth care access, but evidence suggests thatnot all States have developed EMS systems thatextend to rural areas. What characterizes EMSsystems is their variability. Per capita expendi-tures for EMS in 1988 ranged from a low of 2cents in Ohio to nearly $14 in Hawaii (57). Asof 1986-87, only two States, Delaware andMaryland, had statewide access to EMS servicesthrough a 911 telephone number, while 21States had only partial 911 EMS access (105). A
lsome include rehabi]i[a~ive c~e in tie definition of an EMS systcm. WhIlc OTA recognizes [hc importance of th~ cormnuum of care required formany EMS patients, rehabilitative care is not specifically discussed in [his report.
- 1 -

2 ● Rural Emergency Medical Services
few States have directed the care of the seriouslyinjured to designated trauma centers, but othersdo not designate specialized facilities and lackregionalized systems of trauma care. SomeStates have developed model EMS systems thatintegrate urban and rural services, while othershave isolated, poorly organized rural EMSsystems with limited resources.
In the 1980s, EMS services have increasinglybecome a State responsibility. In 1988, over 80percent of State EMS funds derived from Stateor local sources. Federal funding of State EMSactivities is limited to support through thePreventive Health and Health Services BlockGrant program (administered by the Departmentof Health and Human Services (DHHS)) andthrough the Department of Transportation’s(DOT) National Highway Traffic Safety Ad-ministration (NHTSA). In 1988, $13 million ofDHHS’s block grant funds were spent by Stateson EMS, while DOT distributed nearly $5million for EMS through its State and Commu-nity Highway Safety Grant Program (section402 program) (24,57).
Federal EMS expenditures have declinedsharply in the last decade. Following passage ofthe 1973 EMS Systems Act, about $30 millionwere spent annually on EMS. In the early 1970s,EMS systems were found to be underequipped,poorly staffed, and fragmented. Many EMSservices were provided by funeral homes, andprehospital care providers often lacked basicmedical skills. The EMS Systems Act resourceswere targeted to rural areas because they weremore likely to be lacking resources than urbanareas.
Funding through the 1973 EMS Systems Actis credited with having provided incentives forregions to plan and upgrade EMS services.Many communities used EMS Act funds toimprove their communications systems, trainEMS prehospital providers, and regionalizecare. However, the goal of the EMS Act—to
blanket the country with high-quality EMSprograms—was not met before its demise in1981. In 1981, a number of categorical pro-grams, including EMS, were folded into a blockgrant program. With the advent of the blockgrant program, EMS spending declined and hasnot yet risen to spending levels of the late 1970s(128).
With new evidence that EMS systems arefragmented and lacking resources, several Fed-eral initiatives have been proposed to bolsterState EMS systems and target resources to ruralareas. How limited Federal resources can beused to improve rural EMS systems is thesubject of this report. The report describes theavailability and distribution of EMS resources(e.g., personnel, transportation, facilities) anddiscusses Federal EMS policies that affect theseresources, but does not specifically addressFederal EMS reimbursement policies. Thisreport is based, in part, on a May 1989 RuralEMS workshop (cosponsored by DOT andOTA) and on background papers prepared forthe workshop. (See app. A, list of workshopparticipants.)
EMS IN A RURAL CONTEXT
The past decade has witnessed major changesin the U.S. health care system, including bothhow health care is paid for (e.g., implementationof prospective hospital payment in the Medicareprogram) and how health care is delivered (e.g.,a shift to outpatient services). In some ruralareas2 a decline in the economy has accompa-nied these changes, making it difficult for manyrural health care systems that are small andlacking diversification to adjust to the newhealth care environment. Since 1981, nearly 550rural hospitals have closed (61 ). In communitieswith only a single hospital, hospital closure hasmeant that local access to hospital-based care islost and ready access to emergency care isdiminished.
z~l]e here we nmerous ways 10 deflnc mrd Mew, (his report defines rural axeas as those areas not desiwated as Metropolitan statistical ~e~(MSAS). Definitions of rural areas are reviewed in OTA’S staff paper, “Defining ‘Rural’ Areas: Impact on Health Care Policy and Research,” publishedin July 1989 (50).

Chapter 1-Summary and Policy Options . 3
Many rural areas have difficulty recruitingand retaining physicians, nurses, and otherhealth care personnel because of the heavydemands of rural practice (e.g., longer hours, nobackup) or because the area lacks a hospital orother resources that attract providers. In someareas, personnel shortages have been exacer-bated by diminished support from Federalprograms such as the National Health Servicecorps.
Access to well-trained personnel, essentialequipment, and facilities in rural communitiesthat lack a local hospital or physician maysometimes be achieved through cooperationwith neighboring communities that have medi-cal resources. If the availability of health careservices diminishes in rural areas, EMS provid-ers may have to assume new responsibilities.There may be an increased demand for none-mergency transportation to hospitals and forurgent primary care services (e.g., deliveringbabies). Rural EMS providers are having diffi-culty providing EMS services even withoutthese basic problems in the health care system.Some specific problems of rural EMS systemsare:
●
●
●
●
Many rural areas have sparse and dispersedpopulations that are far from care. Poorroads, or the absence of roads, can delayEMS transport.Public access to EMS is compromised byantiquated communications equipment. Uni-versal access to EMS by telephoning 911 isdesirable but lacking in many rural areas.Some rural residents must make long-distance telephone calls to obtain emer-gency assistance. Some rural areas do nothave telephone service.Radio “dead spots”3 and crowded radiofrequencies interfere with essential commu-nications between rural ambulance crewsand hospital-based physicians.There are shortages of prehospital careproviders, many of whom are volunteers.Available rural prehospital care providers
often have a less advanced level of trainingthan their urban counterparts. Training andcontinuing education opportunities are notavailable in many rural areas.Rural EMS providers have difficulty maintain-ing specialized skills because of a rela-tively low volume of EMS calls. There arefew innovative teaching strategies beingused to overcome this problem.There are few rural physicians trained toprovide medical supervision of local EMSoperations.Rural EMS providers often rely on oldambulances and ambulance equipment. Airmedical transportation to rapidly accessspecialized care is not readily available insome rural communities.Rural hospital emergency room physiciansand nurses often do not have advancedEMS training. Rural hospitals may nothave developed EMS protocols that desig-nate the roles and responsibility for EMSamong rural EMS providers. The role ofthe community or local hospital withinregionalized systems of special care, suchas trauma systems, has not been wellestablished.Rural areas often lack the resources neededto address EMS problems.
Information from three States (New York,Texas, and South Carolina) suggests that in bothrural and urban areas emergency medical serv-ices are more likely to be required for medicalconditions (e.g., heart disease and respiratorydistress) than for trauma. Two of the mostcommon types of EMS care, EMS cardiac andtrauma care, illustrate the special problems ofdelivering EMS services in rural areas.
Cardiac Care
Providing cardiac EMS care quickly is essen-tial but difficult in many rural areas. In the caseof cardiac arrest, cardiopulmonary resuscitation(CPR) must begin within 4 minutes and defini-tive care within 10 minutes of the arrest (1 16).Rural EMS systems are at a disadvantage in
Ssome ~r~ ~ea~ are ou~idc the range of available radio equipment.

4 ● Rural Emergency Medical Services
treating cardiovascular emergencies, becausethey often lack paramedic prehospital providers,who are much more successful than basic-levelemergency medical technicians (EMTs) in treat-ing cardiac arrest (52). However, some ruralcommunities have improved emergency cardiaccare by implementing ‘bystander’ education or“first responder” programs to improve thechances that CPR or first aid will be adminis-tered quickly and will continue until the ambu-lance arrives, and by training EMTs to useautomatic external defibrillators. Automatic exter-nal defibrillator are particularly well suited tothe needs of rural areas because they are easy touse, and because the skills needed to use them donot deteriorate even if the procedure is notperformed often (100).
Not all rural communities, however, have theresources or conditions that would permit effec-tive use of defibrillator by EMTs. If communi-ties are small, community members are nottrained in CPR techniques, and response timesare 10 minutes or more, a community shoulddirect its resources to improving these condi-tions before instituting an EMT defibrillationprogram (1 15). Defibrillator are relatively in-expensive, but training and system-wide super-vision of prehospital defibrillation programsmay not be. To improve rural EMS cardiac care,bystander and first responder training programscould be implemented; where feasible, EMSresponse times could be reduced; and physi-cians, nurses, and EMTs could be trained tosupervise and implement EMT-defibrillator pro-grams.
Trauma Care
Injuries4 occur with nearly equal frequency inurban and rural areas but tend to be more severein rural areas. Injury-related mortality is higherin rural areas, but basic information is lackingabout when, where, and why rural injury andinjury-related deaths occur.
Because time to definitive care is such acrucial factor in determining the trauma pa-
tient’s outcome, higher trauma-related mortalitymight be expected in rural areas due to delays indetection and response times. In some remoterural areas, delays are unavoidable, but responsetimes may be improved by increasing thenumber of available ambulances, improving airmedical services, or changing the placement ofground or air transport.
Reducing delays to care can also be accom-plished by shifting the onset of emergencytreatment from the hospital to the prehospitalperiod. Evidence suggests that a “scoop andrun’ approach is advisable in urban areas, butenhancing the trauma skills of rural EMTs toprovide more care during the prehospital phase(without prolonging the time to reach thehospital) might improve trauma outcomes inrural areas. Rural basic-level EMTs could betrained in intermediate skills and become certi-fied to provide more advanced trauma care (i.e.,become intermediate-level EMTs), although ifthey were so trained they might have troublemaintaining their skills and it is uncertainwhether trauma-related mortality and morbiditywould improve.
Severely injured rural patients should often beevaluated and stabilized expeditiously in thecommunity hospital, and then triaged to thenearest trauma center (21 ,54). According to theAmerican College of Surgeons, hospitals treat-ing trauma should, at a minimum, have emer-gency medicine physicians available in thehospital around the clock. However, 24-hourphysician coverage is often unavailable in ruralhospital emergency rooms, and available physi-cian and nursing staff may not have advancedtrauma care skills. Improving the training ofboth emergency room nurses and physicianswould improve rural trauma care, as wouldimplementation of trauma protocols that helpensure that a physician and other necessarypersonnel are available by the time a traumapatient arrives at the hospital.
Many States have attempted to regionalizetrauma care by designating or identifying hospi-
d~j~ and ~auma are synonymous teITns.

Chapter I-Summary and Policy Options ● 5
tals according to their level of trauma careservices. Most rural hospitals do not meet therequirements of even the lowest level of traumacare but nonetheless have an important role toplay in providing trauma care in rural areas.Developing specific trauma care guidelines forrural hospitals might prove helpful to ruralproviders and clarify the rural hospital’s rolewithin the trauma care system. A system thatintegrates all levels of hospital care within aState promotes regionalization and is likely toimprove rural trauma patient outcomes.
Research Needs
Before implementing programs to improverural trauma outcomes, it would be useful toknow more about the causes and consequencesof rural trauma, where along the continuum ofcare deaths are occurring (e.g., during theprehospital or hospital phase), and whetherthese deaths are potentially preventable. Imple-menting programs without such informationmay lead to inefficient use of limited resources(24). To begin to understand where, along thecontinuum of care, resources could be targetedto improve the outcome of rural trauma patients,population-based studies need to be conductedin rural areas. Ideally, hospital discharge datawould be examined so that the types of care andoutcomes of patients that both live and die couldbe evaluated.5 Because hospital discharge datamay not be readily available, studies of traumadeaths could be conducted to see what propor-tion of them are preventable. Studies of prevent-able mortality will shortly be conducted withsupport from the Department of Transportation(24).
Research is also needed to evaluate theeffectiveness of specific EMS interventionsnow commonly used. The evaluations must takeplace in both urban and rural areas, becausesome evidence suggests that some interventionsthat are inappropriate in urban areas may beeffective in rural areas. Initiation of fluidresuscitation for patients who have lost a lot of
blood, for example, is not indicated for patientsin urban areas that are within 20 minutes of atrauma hospital but may be appropriate in ruralenvironments where time-to-care may be longer.
The relative effectiveness of public educationand law enforcement in improving injury ratesin rural areas is another area worthy of investiga-tion. Some practices of rural residents probablycontribute to higher injury-related mortality.Only 25 percent of rural residents, for example,report using seat belts all or most of the timewhile driving, as compared to nearly 40 percentreported by urban residents. Public education,the enactment of State laws to require seat beltuse, and enforcement of existing laws couldcontribute to lower injury-related mortality andmorbidity.
The present impetus to improve EMS systemscenters on the adequacy of trauma care. Whiletrauma care is an important component of EMScare, the adequacy of nontrauma-related EMSservices needs to be examined as well. Thereappears to be an excess of deaths among traumavictims in rural areas, but it is not clear to whatextent these deaths are preventable throughmedical interventions. It may be that targetingresources to prevention may be more effective inreducing fatalities than improvements in traumacenters. EMS care is more likely to involvepatients with medical conditions such as cardiacarrest and strokes than trauma, and in the case ofsudden cardiac arrest, rural mortality mightdecline with EMS systems improvements suchas implementing EMT-Defibrillator programs.Whether patients suffering from cardiovascularemergencies might benefit from other system-wide changes, such as more regionalized care, isuncertain. A few States have verification anddesignation standards for cardiac care facilities,but most do not.
OPTIONS FOR FEDERAL POLICY
While some problems associated with deliv-ering EMS care in rural areas to widely dis-
5~e sen~ltivlty Index Rojmt, funded though DoT’s National Highway T’raffic Safety Adnlinis~ation, links statewide computerized crash rf3pOflS
with patient hospital records. This allows investigators to correlate factors such as EMS response time and seat-belt use to patient outcomes (53).
6 ● Rural Emergency Medical Services
persed populations may seem intractable, manyrural EMS problems can be resolved withadditional targeted resources and effective plan-ning and management. Among the most salientproblems confronting rural EMS systems are:
EMS personnel shortages;inadequate advanced training opportunitiesfor available EMS providers;a lack of medical supervision of local EMSoperations;antiquated equipment (e.g., communica-tions equipment);poor public access to EMS; andan absence of regionalized systems ofspecialized EMS care, such as traumasystems.
The Federal role in supporting State EMSprograms has waned in recent years, but evi-dence of serious impediments to quality EMScare in rural areas argues for an increasedFederal role. Providing EMS services is largelya State and local government responsibility;Federal resources have never been consistentlyavailable or sufficient to rely on for EMSoperations. Limited Federal resources might,however, successfully be used to:
●
●
●
●
●
It is
promote training of EMS providers,facilitate the development of national consen-sus guidelines or standards for prehospitalEMS providers and EMS facilities,provide technical assistance to States,support EMS-related research and demon-stration projects, andprovide incentives for States to implementplanning efforts.
in these areas that States continue to needFederal leadership ( 112).
Federal Initiatives in EMS Training
Option 1: Congress could fund theDepartment of Health and HumanServices (DHHS) to provide assistance inimproving the supply and level of skills ofrural prehospital and hospital-based EMSproviders. Increased Federal assistance
could include support of EMS training andcontinuing education programs, and Staterecruitment and placement programs.
Rural areas are suffering shortages of prehos-pital care providers and are dependent onvolunteer providers who tend to have lessadvanced training than their urban counterparts.Rural hospital-based nurses and physicians maynot have specialized training in EMS care, butnonetheless provide essential services to EMSpatients. Federal assistance to EMT, primarycare, and nursing training programs could im-prove the general availability of EMS providers.EMT programs that are accessible to ruralresidents could be targeted, because shortages ofrural volunteer EMTs are particularly acute. Asthe cost of EMT training and certification can bea deterrent for volunteers, States could beencouraged to subsidize training with Federalassistance. Providing assistance to State recruit-ment and placement programs could also im-prove the availability of EMS providers in ruralareas.
Federal resources could also be directed toEMS continuing education that is accessible toEMTs, nurses, and physicians already practic-ing in rural areas. Making continuing educationcourses in emergency medicine available torural providers could effectively improve therural hospital’s EMS medical response and thequality of the rural community’s EMS system.Increased support for EMS-related training andcontinuing education could be administrativelyhandled through. for example, the Health Re-sources and Services Administration’s Bureauof Health Professions. Many professional andnonprofit organizations are involved in EMS-related training, but there is no Federal agencythat monitors the availability or content of EMStraining.
Option 2: Congress could require DOT toreevaluate the standard curricula forprehospital EMS providers.
Although there are recognized shortages ofprehospital care providers, the specific set of

Chapter l--Summary and Policy Options ● 7
EMS skills required in rural and urban settingsis uncertain. A reexamination of prehospitalcare training and curriculum is justified becausethere is considerable controversy surroundingthe effectiveness of some standard prehospitalinterventions in both rural and urban settings.The standard curricula for prehospital providers,developed by DOT, could be reevaluated in lightof the unique characteristics of rural EMSproviders (i.e., most are volunteers) and thedemands of rural EMS practice. DOT (NHTSA)is sponsoring a development conference onEMS training in early 1990 where both traumaand nontrauma EMS training requirements willbe discussed. DOT could change the standardcurricula for first responders, and for basic,intermediate, and paramedic-level EMTs, butEMT-Defibrillator training would fall outside ofDOT’s authority. DOT’s conference on prehos-pital EMS provider responsibilities and trainingmight help clarify what should be included inEMT curricula and might help reduce theextreme differences in training that currentlyexist.
Federal Guidelines or Standards
Option 3: Federal legislation could facilitatethe development of national consensusguidelines or standards for prehospitalEMS providers.
There are about 36 recognized levels ofprehospital care providers across the Nation,and training requirements and levels of respon-sibility vary markedly by State. The AmericanSociety for Testing and Materials, a voluntarystandard development organization, has pub-lished standards for some EMS personnel, butthese have not been widely used. Federallegislation could ensure that national consensusguidelines or standards for prehospital EMS
providers be developed following the NationalDevelopment Conference on EMS training,sponsored by DOT, which is to be held in early1990.
Option 4: Federal legislation could facilitatethe development of national consensusguidelines or standards for specializedEMS facilities, such as trauma centers.Such guidelines or standards mightdelineate the role of small rural hospitals inEMS care.
Some proposed Federal EMS legislation tiesreceipt of EMS grants to adherence to a Stateplan that includes trauma facility designationaccording to national standards. Proponents ofnational trauma facility standards argue that fewStates have EMS systems that meet essentialcriteria, including facility standards, establishedby professional organizations (i.e., AmericanCollege of Surgeons, American College ofEmergency Physicians) and that such standardsare required to assure EMS quality.6 Opponentsof EMS initiatives tied to facility standardsargue that States have very diverse EMS needsand that imposing a national standard wouldprovide little flexibility.
Three-quarters of the States have developed,or are developing, some type of trauma facilityverification or designation program, but mostadapt standards (like those developed by theAmerican College of Surgeons) to meet State orregional needs. Developing national voluntaryguidelines or standards might be preferable tomandatory standards in light of States’ diverseneeds.7 A consensus development conference,such as those sponsored by the National Insti-tutes of Health, might provide a forum wherebynational consensus guidelines or standards couldbe developed with advisement from profes-
6Rwogn1zlng ~a( facl]lty stand~ds ml@t not be approprla[c]y applled in all areas, legislators have included prOvi SiOn~ wh~rcb a S[~lC ~~uld gc[a waiver of [he proposed trauma facllily standards after public notice and hcanngs.
7Ex1sting Fcdcra] rcwlatlon% re~ommcnd ~a[ Fcdcra] hc~lth and ~afc[} programs usc natlona] Vo}unlq con~n$us s(andwd~ ( 1 CFR Chapter ~
- 1978). The Office of Management and Budget Federal standards policy a~u) rccomrncnds the usc of national voluntag consensus slandards (CircularA-1 19 of November 1982).

8 ● Rural Emergency Medical Services
sional medical organizations and State and localofficials. 8
Some argue that the imposition of facility orsystem standards is premature in some areas andthat such standards will doom many areas’programs to failure. Any guidelines or standardsthat are developed could be phased in so thatresources could first be used to improve trainingand to upgrade communications and otherequipment. This would help to ensure that whenstandards were imposed, personnel and equipment-related criteria could be met. Some opposition tothe imposition of facility designation criteriaand triage protocols may be alleviated throughpublic and provider education.
Federal EMS Technical Assistance
Option 5: Congress could fund DOT andDHHS to augment technical assistance toState EMS offices.
The ability of States to provide technicalassistance to EMS providers needs to be im-proved, especially for those States with largeunderserved rural areas. Specific types of tech-nical assistance include:
development of communications systems;enhancement of management skills (e.g.,billing procedures, personnel practices);promotion of public education (e.g., raisepublic awareness of EMS system, injuryprevention);delivering air medical services in ruralareas;development of statewide or regional EMSsurveillance systems and reporting prac-tices; andimplementation and adherence to qualityassurance programs.
In many of these areas, Federal expertise isavailable to assist State EMS program directors.
EMS-related technical assistance to States iscurrently available through DOT’s NationalHighway Traffic Safety Administration. NHTSAassembles a team of technical advisors that mayinclude experts in such areas as rural EMSdelivery, data gathering systems, trauma sys-tems, and the development of legislative propos-als.9 The assessment team makes recommendationsto the States after comparing the status of EMSin the State to EMS system standards estab-lished by the assessment team (126). The scopeof technical assistance offered by DOT extendsbeyond highway safety issues and is offeredwhen requested by a State’s EMS office. DOTsupported the development of a computer simu-lation program for rural EMS system designthat, if adapted to the microcomputer, could bea useful adjunct to providing technical assis-tance.10
The Centers for Disease Control (CDC) alsohas a technical assistance program through itsDivision of Injury Epidemiology and Control.CDC can offer technical assistance in manyEMS-related areas such as injury surveillance,but there are areas of expertise that are lacking,such as EMS systems development. Less thanone-half of State health departments reporthaving injury reporting/surveillance systemsand when data sources are available, States donot always use them (47). As EMS planning andquality assurance are facilitated by such surveil-lance systems, this appears to be an area whereStates may benefit from technical assistance.
Several tools are available for EMS systemsto evaluate their performance. One methodinvolves comparing a system’s prehospital serv-ices for trauma patients to the experience ofother EMS systems. A database that includes theexperience of many providers can be used todevelop norms or a “yardstick” against whichthey can compare their patient survival experi-
8~e ~cncan socle~y for Tcs,llng and Materials (ASTM) has had scvcra] task groups addressing the devc]opmcnt of a nationa] consensus onguidelines for EMS facilities (ASTM Commitwc F30), bu[ representatives of professional organizations such as ACS and ACEP no longer participatebecause of concerns about the appropriateness and applicability of t,he ASTM process to the field of EMS (53,63).
9EMS advl~rs as~mblcd by DOT have provided assistance to eight States this year and plans are to extend assistance to eight more in calender Year1990 (24).
I~ls computer simulation model is described in app. B.

Chapter 1-Summary and Policy Options ● 9
ence (88). Such a database is central to the MajorTrauma Outcome Study. Here, data on traumapatients from over 100 hospitals are analyzed toestablish norms (e.g., mortality, complications)by cause of injury and injury severity (23).
Federally Sponsored EMS Research andDemonstration Programs
Option 6: Congress could fund DOT andDHHS to augment their EMS research anddemonstration programs and encouragethe investigation of EMS problems uniqueto rural areas and providers. The researchefforts of DOT’s NHTSA and DHHS’sNational Center for Health ServicesResearch and CDC could be coordinatedto address a broad range of outstandingresearch questions.
EMS research and development efforts cameto a virtual standstill following the demise of theEMS ACT in 1981. Under the EMS SystemsAct (section 1205), the National Center forHealth Services Research (NCHSR) was re-sponsible for EMS applied research. The resultsof the NCHSR research conducted in the midseventies has greatly influenced EMS practiceand has been useful to rural providers. NCHSR-supported research showed, for example, thatdefibrillator could be effectively used by pre-hospital providers on patients suffering out-of-hospital cardiac arrests.
CDC, through its Division of Injury Epidemiol-ogy and Control, has recently established fiveInjury Prevention Research Centers and hasfunded over thirty 3-year research and demon-stration projects.11 DOT has a small researchand development budget, but, these resourcesare used to investigate highway-related con-cerns. Additional funds could be used to expandand coordinate the research capabilities ofNCHSR, DOT, and CDC.
Although these efforts are noteworthy, thereare numerous outstanding EMS research ques-tions with direct relevance to rural areas that are
not being adequately addressed. These includesuch basic questions as, ‘‘is the demand forEMS different in rural as opposed to urbanareas?’ The results of such research could guidecurriculum revisions and the development ofany new prehospital provider standards orguidelines. Demonstration projects with anevaluation component could answer questionson the relative cost and effectiveness of innova-tive teaching strategies, such as home instruc-tion using videocassette recorders for EMTtraining or rural emergency room nurse andphysician continuing education. Such instruc-tion might help to solve some of the EMTshortages experienced in many rural areas andimprove the skill levels of existing rural pro-viders.
Federal Incentives for Planning andEMS Systems Development
Optimally, EMS systems have ongoing, dependa-ble State support. Several States have achievedself-sufficiency through innovative funding strate-gies (e.g., special funding through motor vehiclefees), but many State’s EMS programs areunderfunded and lack coordination. To promoteState EMS system development and planning,existing Federal EMS program support could beaugmented or new Federal EMS programsestablished.
Option 7: Congress could augment supportof existing Federal programs that addressEMS, namely the DHHS Preventive HealthBlock Grant Program and DOT’s Stateand Community Highway Safety GrantProgram. Consideration could be given toearmarking funds within these grantprograms for EMS.
The DHHS Preventive Health BlockGrant Program
States can use block grant money for a varietyof purposes, and investment in EMS cannot beassured without earmarking some portion of theDHHS block grant for EMS. Earmarking would
1 l~e gan~ were dls~lbuted ~ong five major clcments of inJ~ control: epidemiology, prevention, biomcchanics, acule care, and rehabilltahon
(27). Two of the funded projects relate to farm and rural injuries.

10 ● Rural Emergency Medical Services
be helpful in those States that have not givenhigh priority to EMS system development; butit would also mean that States with well-developed EMS systems would be required toexpend Federal block grant funds on EMS ratherthan on other State priorities.
Augmenting current Federal EMS-relatedprograms has the advantage of administrativeease and offers a flexible approach for Stateswith diverse needs. States could use the addi-tional block grant funds to invest in communica-tions equipment and improve training opportu-nities within the State. A disadvantage of usingthis approach is that it would be difficult toimpose any Federal EMS standards (e.g., desig-nation of facilities) or to tie funds to theimplementation of a State EMS plan, becauseunder the block grant program the State has thediscretion to use funds as it sees fit. Anotherdisadvantage of this approach is that it isdifficult to target Federal funds to States withidentified EMS problems or, within States, torural areas.
DOT’s State and Community Highway SafetyGrant Program
Augmenting DOT’s State and CommunityHighway Safety Grant Program could be a moreeffective way to promote EMS system develop-ment than augmenting the DHHS PreventiveHealth Block Grant Program. Unlike DHHS,DOT makes EMS money available to States toimplement a State Highway Safety Program thatincludes EMS. DOT has established EMSguidelines for States to follow in developingtheir highway safety program. With evidencethat the chances of being seriously injured ordying if involved in a motor-vehicle accident aretwo to three times higher in rural than urbanareas, there is a need to involve State highwaysafety programs and transportation experts inEMS systems development. DOT’s programcontains elements needed to promote EMSsystem development, but DOT’s focus is on
highway safety and trauma care. DOT’s EMSguidelines are, however, generalizable to mostemergency care (e.g., there are provisions forEMS training and emergency vehicle require-ments).
DOT’S grant program funds are now chan-neled to States through politically appointedState highway safety representatives. State DOThighway safety programs have been directed tocoordinate their activities with State EMSoffices, but there are still areas where there is alack of coordination.
If additional support were available, many ofthe technical assistance, research and develop-ment, and training issues could be adequatelyaddressed through interagency coordination andagreements. However, certain areas of expertiseare missing from the current Federal EMS-related agencies, specifically in the areas ofnontrauma-related EMS care and EMS systemsdevelopment.
Option 8: Congress could establish a newEMS categorical grant program withinDHHS.
Rather than augmenting current Federal EMSprograms, a categorical grant program could bereestablished within DHHS to specifically pro-mote EMS systems planning. The availability ofgrants to States could be tied to the developmentand implementation of a State EMS plan. Sucha program would reestablish a strong FederalEMS presence within DHHS, which could becoordinated with DOT’s EMS program. If sucha presence were established, many problemsrelated to coordination of current Federal effortsmight be solved or mitigated.12 If new Federalresources were directed to resolve some ruralEMS system problems, methods to allocateresources to those areas most in need could helpassure that limited resources are effectivelyused.
lz~ere WU an active Interagency CommitlCc on EMS from 1974 to 1981. Since then, a Federal Interagency Committee on Emergency MedicalServices (FICEMS) was chartered by tie Federal Emergency Management Agency (FEMA) but there is a need for improved interagency communication,particularly in the areas of training, communlcat]ons, and research and development (125).

Chapter 1--Summary and Policy Options ● 11
Targeting EMS Resources To Rural Areas
Option 9: To accommodate the diversity ofrural areas, any Federal EMS resourcesprovided to States could be tied toimplementation of a comprehensive Stateplan that addresses that State’s rural EMSsystem problems.
Different approaches could be used to targetFederal EMS resources to rural areas. Resourcescan go directly to rural areas, or they can beallocated to States based on a formula reflectingtheir rural population. Under the 1973 EMSSystems Act, grants could be made to any of 303EMS service areas, some of them rural areas.Sometimes, only certain areas within a Statewere funded under the competitive grant proc-ess. The grant program promoted regional EMSplanning but not necessarily statewide planning.If funds are to be directed to States and somefunds are to be used to solve rural EMSproblems, how to allocate those funds to ‘ruralareas is an important issue. An allocationformula might be based on the proportion of thepopulation that resides in nonmetropolitan areas,population density, square mileage of the State,or another indicator of rurality. Each has itsadvantages and disadvantages.
The basis used for allocation can have asubstantial influence on the distribution offunds. For example, over 80 percent of the Idahopopulation resided in nonmetropolitan areas in1980, but that population numbered less thanone million. Texas, on the other hand, had lessthan 20 percent of its population residing innonmetropolitan areas but had more than three
times the number (over 3 million) of nonmetro-politan residents. An allocation formula basedon the proportion of nonmetropolitan residentsmight leave States with very large nonmet-ropolitan populations at a disadvantage. In otherStates, rural EMS problems may be related tothe presence of large disadvantaged populations(e.g., those lacking in health insurance and withpoor health status). In these States, an allocationformula based on the composition, as well as therelative size of the nonmetropolitan population(e.g., percentage of the population that isuninsured) might be more appropriate. In some‘‘frontier’ 13 States, rural EMS problems can bedirectly related to large geographic EMS serviceareas that are sparsely populated. Here anallocation formula based on population densityor dispersion might be appropriate.
There may be some rural areas where directongoing subsidies are required to maintainservices. An EMS system is much like a publicutility offering electric or water service, in thatproviding services becomes disproportionatelymore costly as the number of consumers de-clines and becomes dispersed over wide areas.Ongoing subsidies in such situations are notnew; subsidies have been used to finance somerural electrification projects, and urban mailservices subsidize the more expensive ruralroutes. Some communities can form coopera-tives or linkages to broaden their service areaand conserve resources, but other communitiesare isolated and cannot. Helicopters and air-planes may be used to transport some isolatedpatients to a medical facility, but these cannotreplace an appropriate level of first response.
lg~e Iem “frontier” has &n used to describe areas with six or ICSS residents per square mile (50).

Chapter 2
Definition of Terms
EMERGENCY MEDICALSERVICES
Emergency medical services (EMS) include thepersonnel, vehicles, equipment, and facilities used todeliver medical care to those with an unpredictedimmediate need outside a hospital and continuedcare once in an emergency facility (127). ’ EMSsystems are generally organized at the State orregional level to provide coordinated delivery in anappropriate geographic area (62). Implementingcomprehensive EMS systems has been shown tosave lives and reduce disabilities (76,127). Theprimary goals of an EMS system are to:
1.
2.
3.
provide rapid transportation to a medicalfacility;provide immediate medical assistance at thescene and while in transit; andhave a coordinated, tiered level of hospital careso that the most seriously injured or ill patientsare quickly triaged to, and cared for at special-ized facilities, and the less severely injured orill patient cared for at less specialized facili-ties.
In reaching these goals, EMS systems extendbeyond the bounds of what is traditionally viewed asthe “medical system,” often overlapping with otherpublic safety systems such as local fire and policeservices. Rural EMS systems rely heavily on com-munity volunteers and may therefore serve as animportant interface between the public and the localhealth care system (85).
EMS systems include several components:
Public Access
Public access to an EMS system is optimallyachieved through a coordinated communicationssystem. Centralized communications centers may beaccessed directly by telephone or radio using a 911,800, or designated seven-digit number (sometimesreferred to as universal access). EMS systems canalso be accessed through fire and police depart-ments, hospitals, or telephone operators.
Prehospital Response
Public Safety Response
Prehospital response may begin shortly after anemergency victim is detected and before EMSprofessionals arrive. Bystanders trained in car-diopulmonary resuscitation (CPR) or first aid mayprovide assistance at the site or individuals trainedin basic emergency skills may be called to the site as“first responders” until the ambulance or otherEMS professionals arrive. Fire and police officialsor community members may be trained as firstresponders.
EMS Professional Response
After the EMS system has been called. a vehicleappropriately staffed and equipped is dispatched tothe scene. Depending on the nature of the emer-gency, extrication may be required, and medicalstabilization or treatment initiated. EMS personnelselect a facility to take the patient to (sometimesusing transport guidelines), and provide transporta-tion to that facility while continually monitoring andadministering care to the patient. Prehospital provid-ers are usually emergency medical technicians whoprovide basic life support care, which includes basicemergency care and CPR, and/or advanced lifesupport, which may include external defibrillationfor cardiac arrest patients and more invasive proce-dures such as starting intravenous lines. Prehospitalcare providers are ideally provided medical advicefrom physicians via vehicle-to-hospital communica-tions. In addition to providing such “on-line”medical control, physicians may also participate in‘‘off-line’ medical control through designing medi-cal protocols that guide prehospital providers’ care.Any in-transit communication of the patient’s condi-tion helps the receiving facility prepare for thearrival of the patient.
Transportation
Most EMS transportation is provided by ambu-lances. Helicopters are often used to transporttrauma patients to trauma centers, while airplanes orhelicopters are used to transfer stabilized patientsfrom one hospital to another. The duration of the
1 Some include ~ehabl]llatlvc ~mc ,n [he dcfinlllon of an EMS sys[em, Whl]e OTA re~ogni~cs [hc lrnp~flan~c of Lhc con~inuum Of CLMC rcqulrcd fOrmany EMS patients, rehabilitative care is not spcci fically d]scusscd in [his report.
–13–

14 ● Rural Emergency Medical Services
transportation phase is dependent on three factors:physical distance to be covered; mode of transporta-tion (land, air, water); and the type and condition ofthe roadway, airway, or water.
Medical Response
There are three levels of medical response:
. Primary medical response involves nonspe-cialty providers in facilities such as smallcommunity hospitals. Providers at these facili-ties can resuscitate and stabilize critically ill orinjured patients.
. Secondary medical response offers definitivetreatment by specialty providers (e.g., sur-geons, anesthesiologists). Secondary facilitiesgenerally have a physician available 24 hours aday and lab and x-ray services available within30 minutes.
. Tertiary medical response involves highly spe-cialized and technical services (e.g., burn care,spinal cord injury care). Generally, tertiaryfacilities such as trauma centers need highpatient volumes to operate efficiently.2
A number of professional organizations haveestablished guidelines to categorize hospitals by thelevel of emergency capabilities. The AmericanCollege of Surgeons, for example, has guidelines forthe designation of trauma centers (4). The AmericanCollege of Emergency Physicians has issued guide-lines that include prehospital care (3) (see ch. 5).
The major factor affecting the outcome of acritically injured or ill patient is time to definitivecare, therefore, efficient operation of an EMS systemby trained personnel is essential. Trauma patientoutcomes are best when patients are identified,transported, and cared for within a critical “goldenhour’ (127). For rural residents, this can be achievedwith initial resuscitation and stabilization providedby prehospital providers at the scene and duringtransport; more advanced stabilization at the ruralhospital; followed by rapid transfer to tertiary carefacilities (20,21 ,46,1 28). Optimal EMS care in ruralareas requires that the levels of medical responselocated in both rural and urban areas be wellcoordinated. EMS systems must also be coordinatedwith other public safety agencies such as fire, police,and disaster programs.
The responsibility of overseeing a State’s EMSsystem generally rests with a State EMS director.The State EMS director may, among other things, beresponsible for training and certifying EMS provid-ers, certifying ambulances and air-medical trans-portation services, and ensuring the coordination oflevels of EMS care provided within the State’shospitals. At the local level, EMS care may beorganized through the county, as a separate depart-ment of local government similar to those offeringpolice and fire protection. Alternatively, EMS serv-ices may be offered through an existing municipalagency. such as the fire department, where providersmay be cross-trained to assume both EMS andfire-fighting responsibilities. Hospital emergencydepartments, private ambulance services, or inde-pendent voluntary agencies may also operate andmanage a community’s EMS system (42,75). How-ever EMS services are organized, statewide orregional EMS patient surveillance systems, such astrauma registries, can be used by EMS planners toevaluate the EMS system. All EMS systems need notonly an administrative director, but a medicaldirector who prescribes, oversees, and is accounta-ble for medical care provided by the service orsystem (53). An EMS system may include a singlelocal service or it may encompass an entire State.
RURAL AREAS
Urban and rural areas are often defined using thedesignations of either the Office of Management andBudget (OMB) or the Bureau of the Census. Ruralareas are the remaining areas not captured in eitherOMB’s “metropolitan statistical area” (MSA) des-ignation or in Census’ urban or urbanized areadefinitions. Counties are the building blocks ofOMB’s MSAs and are easy to use, because county-based data are readily available. One or morecounties form an MSA on the basis of populationsize and density, plus the degree of area-wideeconomic integration as reflected in commutingpatterns. MSAs include a densely populated urbancore (called an urbanized area), with at least 50,000residents, that is part of a county or countiescomprised of at least 100,000 residents. The Census’
zTra~a centers and tra~a sys[cms arc one Cornponenl of EMS care and systems. Trauma ccntcrs offer definitive care for the critically injuredpatient. For patients with noninjury-rcla[ed medical conditions, the tertiary medical response may involve other specialized hospitals or centers.

Chapter 2--Definition of Terms ● 15
urban and urbanized area definitions rely on settle-ment size and density without following countyboundaries, making them more difficult to use.3
Both methods identify about a quarter of the U.S.population as rural or “nonmetropolitan.” but thesepopulations are not identical. For example, about 40percent of the Census-defined rural population livewithin MSAs, and 14 percent of the MSA populationlive in Census-defined rural areas.
This report will refer to nonmetropolitan areas asrural unless specified otherwise. It seems appropri-ate to use MSAs to describe ‘‘urban’ and ‘‘rural’access to, and organization of, EMS services,because EMS systems are generally organized alongthese lines. Specialized EMS services, such astrauma centers, for example, are generally locatedwithin the more densely populated urban areas ofMSAs and become less available as you move outinto the less populated non-MSAs. Nonmetropolitanhospitals are generally smaller than metropolitanhospitals and tend to have fewer specialized servicesavailable (6).
Unfortunately, statistics relevant to EMS are notpresented in a standardized fashion. Comparing
EMS-related data from one source to another,therefore, is almost impossible. The Department ofHealth and Human Services (DHHS), for example,publishes vital health statistics (e.g.. injury-relateddeaths) for metropolitan and nonmetropolitan coun-ties, 4 but the Department of Transportation (DOT)provides data in their Fatal Accident ReportingSystem and National Accident Sampling System(122) using their own definition of rural.5
In addition to using a standard definition of‘‘rural, ’ it is important to present data for ruralsubpopulations. Dichotomous measures of urbanity/rurality not only obscure important differencesbetween urban and rural areas but also wide varia-tions within rural areas. Consequently, there havebeen recommendations to implement a standardrural typology that would capture the elements ofrural diversity and improve use and comparison ofdata. Several rural “topologies” or classificationschemes have been developed for nonmetropolitanareas that may prove useful in presenting rural healthdata (50). It would be helpful to use such topologiesto present data on rural injury so that injuries uniqueto such environments as farms and mining areascould be identified.
3For de.alj~ ~nfomatlon on dcfinltlons of ~ra] ~cas, scc ‘‘&finlng ‘R~a] Areas: Impact on Hca]th CMC policy and Rcsc~ch, ” OTA Staff Paper,
July 1989 (available through GPO stock No. 052-003 -01156-5 or by calling the OTA Health Program at 202-228-6590).4DHHS subdlvl&S me~ow]l(an and nonmc~owll~an ~eas into urban and ‘ ‘not ~ban’ places, DHHs defines nonmcwopolitan urban places u areas
with populations of 10,000 or more.s~cordlng t. DOT, ~bm we= me ~eas Within bound~ie~ fixed by s~a[e or Ioca] officials that have a population of 5,000 Or ITIOK, ad We 1101
within another urban area, Rurat areas are those outside of the boundaries of ‘urban areas ( 122). Approximately one-quarter of the population of MSASmeet DOT’s definition of ‘rural and nearly one-third of non-MSAs meet DOT’s defirution of ‘urban.

Chapter 3
The Demand for EMS Services in Rural Areas
INTRODUCTION
Medical conditions that may require emergencymedical services (EMS) include medical emergen-cies, such as heart attacks, and critical injuries suchas those sustained in motor vehicle crashes andoccupational accidents. National data on what medi-cal conditions precipitate an EMS call are notavailable, but some State data suggest that EMS careis needed as frequently, if not more frequently. formedical conditions, such as heart attacks and respi-ratory distress, as for trauma (tables 3-1 and 3-2).This chapter describes urban and rural differences indemand for EMS services and in injury morbidityand mortality.
Each person is likely to need ambulance service atleast twice in his or her lifetime, but a population of10.000 residents generates only one true emergencycall a day (31). Small communities must be preparedfor relatively low volumes of calls that may not bewell distributed over the year. Severe trauma mayoccur infrequently, but a community may have todeal with multiple victims of an automobile crash atone time.
The demand for EMS services will increase in acontinuous fashion as the size of the servicepopulation increases, but the capacity of the EMSsystem to respond increases in discontinuous steps,especially in small communities. A small commu-nity with a two-ambulance system, for example,cannot meet a 20 percent increase in demand with a20 percent increase in capacity; acquiring a newambulance and staff would represent an increase incapacity of 50 percent ( 132).
Many nonmedical factors contribute to the de-mand for EMS services. Some individuals who needEMS services do not use them because they do notrealize that EMS services are required, lack serviceswithin their area. don’t know how to access thesystem, or may be unable to pay for the services.Conversely, some individuals use EMS services for
nonemergencies. This may occur if other healthservices are unavailable or less convenient. or if thepublic is uninformed of the purpose of EMS.
URBAN AND RURALDIFFERENCES IN DEMAND FOR
EMS SERVICES
There are marked urban/rural differences in EMSservice use in three States where statewide, compu-terized, ambulance-use data are available (Texas.South Carolina, New York).1 Ambulance-trans-ported patients in rural Texas are more likely to besuffering from a heart condition or stroke than urbanresidents and less likely to suffer from internalinjuries, injuries to the spine or brain, and lacerationsor penetrating trauma (table 3-1) (1 34). The higherdemand for EMS intervention for acute medicalconditions such as heart attacks or strokes is likelyexplained by the older age distribution of ruralresidents.2
Ambulance services are used more frequently bythe elderly in rural than urban areas. Over half (54percent) of ambulance-transported patients in ruralTexas were age 65 or older (29 percent were age 80or older) as compared to 29 percent in urban areas.There are similar findings in New York State whereover one-half (54 percent) of patients transported byambulance in rural counties were age 60 or older.compared to 42 percent for urban counties (42).3
South Carolina, in contrast. had less than one-quarter of patients age 65 or older among urban andrural ambulance transports in 1988.
Rural ambulance calls are more likely to be‘‘urgent, ’ or ‘‘critical in rural than urban areas ofTexas and South Carolina (44,134).4 In Texas, forexample, 44 percent of 1988 rural ambulance runswere categorized as ‘‘urgent’ and 7 percent ‘‘Cr-iti-Cal ‘ ‘ as compared to 31 percent, and 4 percent.respectively, for urban ambulance runs ( 134). Alarge percent of rural calls in both Texas and
IThcsc States ~crc identified by ~~lllng the Amcrlc:m Ambulance Associa[l{)n, and part icipan[s of the OTA/DOT Rural EMS Workshop. SLMCX ~1~1stiIIcwIdc, computcrwcd, ambulan& data that could bc anal) /cd b> mc[ropohuin and nonmc[ropolllan ,ama provided tic labulatlon~ Ibr OTA.
~Thu-teen pcrccnt of the ntxwnctropolitan popuIaIIoIl I\ cldcrl? { i,c,, agc 65 or older) while only 11 pcrccnt of hc mctropollmn populJIIon I\ cldcrl~( 1 13).
3Ambulancc u[llllatlon data were ava!lsblc for SC!LSC KXI urban and rural coun[]cs (42).~S1ml]~ Lnfoma[lon WaS not ava]lablc from NCW }’ork.
- 1 7 -

18 ● Rural Emergency Medical Services
Table 3-l-Prevalence of Injuries and Illness AmongPatients Transported by Ambulance
in Texas, 1988a
Percent of transports
Type of illness or injury Total Metro Non-metro
Illness:Heart complications . . . . . . . . . . . 12.6Strokes-CVA b . . . . . . . . . . . . . . . . 4.1Respiratory distress . . . . . . . . . . . 7.4Diabetic complications . . . . . . . . . 2.7Gastrointestinal illnesses . . . . . . . 5.1Convulsions or seizures . . . . . . . . 3.6Allergic reactions . . . . . . . . . . . . . . 0.5Fainting . . . . . . . . . . . . . . . . . . . . . 2.0Infectious diseases . . . . . . . . . . . . 1.0Emotional or mental distress . . . . 2.6Other illnesses . . . . . . . . . . . . . . . 12.1
InjuryLacerations or penetrating
trauma . . . . . . . . . . . . . . . . . . . . 9.4internal injuries . . . . . . . . . . . . . . . 2.7Injuries to spine or brain . . . . . . . . 4.5Multiple injuries . . . . . . . . . . . . . . . 0.5Fracture or dislocation . . . . . . . . . 10.9Scrapes, bruises, or cuts . . . . . . . 10.9Sprains or strains . . . . . . . . . . . . . 4.3Burns. . . . . . . . . . . . . . . . . . . . . . . 0.6Drowning, suffocation, or
choking . . . . . . . . . . . . . . . . . . . 0.3Other injuries . . . . . . . . . . . . . . . . . 2.5
Perinatal care:Obstetric or gynecological . . . . . . 1.9High-risk infants . . . . . . . . . . . . . . 0.2
Substance abuse:Drug overdose or poisoning . . . . . 1.6Acute alcohol intoxication . . . . . . 0.8No information available . . . . . . . . 17.2Total number of patients . . . . . . . 51,853
12.23.66.92.64.83.70.52.10.92.8
12.0
9.72.84.60.5
10.411.74.60.6
0.42.7
2.00.2
1.70.9
16.844.527
15.17.0
10.93.57.23.00.51.61.41.4
12.6
7.51.83.40.7
13.76.12.10.4
0.21.6
1.50.1
0.80.5
19.87.326
aThese data are based on ambulance run reports of a representativesample of Texas ambulanea serviees. There were an estimated onemillion ambulamx runs in Texas in 19SS. More than one oondition cm berefwted for each patient. Numbers m the table represent the pereent ofambulance transports for reported types of illness and injury.
~CVA. Cardlcnmacular accident.
80URCE: Texas Department of Health, Austin, TX, August 19S9.
South Carolina are for transportation. In SouthCarolina, for example, about 16 percent of ambu-lance calls in rural areas are for transportation tomedical exams, as compared to 10 percent in urbanareas (44)0
Injury is a major problem in rural areas, particu-larly injuries sustained in motor vehicle accidents.Injuries are more likely than other emergencyconditions to require specialized services such astrauma centers which are usually not immediatelyavailable in rural areas.
Injury
Injury is the leading cause of death among persons1 to 44 years old (1 19) and is the leading cause ofyears of potential life lost before the age of 65 ( 121 ).Injuries occur as, or less frequently in rural areasthan in urban areas (see table 3-3) and the types ofinjuries that occur in these areas are similar (table3-4).5 When injuries do occur, however, they appearto be more serious in rural areas; injured ruralresidents have more restricted-activity days and beddays than injured urban residents (table 3-3). This isespecially true for injuries occurring at home.
Death rates from unintentional injuries (bothmotor vehicle and nonmotor vehicle related) aretwice as high in remote rural areas than in the largestcities (figure 3-1 ) and death rates are inverselyrelated to population density (13). The chance ofdying in a rural area, if severely injured, are three tofour times higher than in urban areas (19,62). Someevidence suggests that aspects of the EMS systemmay contribute to the higher death rates. Forexample, younger and generally healthier adults diefrom less severe injuries in rural nontrauma centerhospitals than in urban trauma center hospitals (66).
Occupational Injuries
While national injury data do not reflect higherinjury rates in rural areas, certain rural subpopula-tions have more injuries because of the types ofoccupations they practice. Approximately 10 per-cent of employed rural residents 16 years of age andolder are employed in two of the most hazardousoccupations in America-farming and undergroundmining. Farming encompasses a wide range ofactivities that may pose health hazards, including theuse of farm machinery and tools and exposure tochemical fertilizers and pesticides. Mining hazardsinclude cave-ins, explosions, fires, and the inhala-tion of dust (78). Work-related deaths occur four tofive times more frequently among mining andagricultural workers than among workers as a whole,and disabling injuries occur two to three times moreoften (72) (see table 3-5).
Motor Vehicle Crashes
One-third of all injury-related deaths are attributa-ble to motor vehicles. Among those under age 35,motor vehicle crashes are the leading cause of death(12). There is wide geographic variation in motor
s~ese data we ]fiit~ tiWfw as they rely on self-reported injuries reported by phone interview (i.e., National Health Interview Smey).

Chapter 3---The Demand for EMS Services in Rural Areas ● 19
Table 3-2—Prevalence of Injury and Illness Among Calls for EMS Services inSouth Carolina, 1988 a (percent)
Metro Non-metro
Jan.- May- Aug.- Jan.- May- Aug. -Primary complaint April July Dec. April July Dec.
Total injury . . . . . . . . . . . . . . . . . .Fracture . . . . . . . . . . . . . . . . . . . . . . . .Spinal injury . . . . . . . . . . . . . . . . . . . .Laceration . . . . . . . . . . . . . . . . . . . . .Abrasion/contusion . . . . . . . . . . . . . . .Head injury . . . . . . . . . . . . . . . . . . . . . .Multitrauma/shock . . . . . . . . . . . . . . . .Hemorrhage . . . . . . . . . . . . . . . . . . . .Dislocation . . . . . . . . . . . . . . . . . . . . . .Puncture/stab . . . . . . . . . . . . . . . . . .Gunshot wound . . . . . . . . . . . . . . . .Burn . . . . . . . . . . . . . . . . . . . . . . . . .
Total cardiovascular . . . . . . . . . . . . . . . .Coronary problem . . . . . . . . . . . . . . .CVA/TIA/stroke . . . . . . . . . . . . . . . . .Cardiac arrest . . . . . . . . . . . . . . . . . . .Hypertension . . . . . . . . . . . . . . . . . .Congestive heart failure . . . . . . . . . . .
Other medical . . . . . . . . . . . . . . . . . .Vomiting . . . . . . . . . . . . . . . . . . . . . . .Gastro-intestinal problems . . . . . . . . .Genito-urinary problems . . . . . . . . . . .Hyperventilation . . . . . . . .Respiratory distress . . . . . . . . . . . . . . .Seizure . . . . . . . . . . . . . . . . . . . . . . . .Diabetic reaction . . . . . . . . . . . . . . . . .Insulin shock . . . . . . . . . . . . . . . . . . . .Fainting . . . . . . . . . . . . . . . . . . . . . .Unknown medical complaint . . . . . . . .Total medical . . . . . . . . . . . . . . . . . . .
Psychiatric/behavioral/drugs/alcohol:Psychiatric/behavioral . . . . . . . . . . . . .Overdose . . . . . . . . . . . . . . . . . . . . . . .Alcohol-like impairment. . . . . . . . . . . .
OB/GYN total . . . . . . . . . . . . . . . . . . . . . .Obstetric-prenatal . . . . . . . . . . . . . . .Obstetric-emergency . . . . . . . . . . . .
Transport for exam . . . . . . . . . . . . . . . . . .Nonemergency transport . . . . . . . . . . .No transport . . . . . . . . . . . . . . . . . . . . .
DOA-total: . . . . . . . . . . . . . . . . . . . . . . . . .DOA—no transport . . . . . . . . . . . . . .DOA—transport . . . . . . . . . . . . . . . . . .
Canceled call: . . . . . . . . . . . . . . . . . . . .False call . . . . . . . . . . . . . . . . . . . . . . . .Missing/wrong code . . . . . . . . . . . . . .
1533321010000
1492211
191211631012
33
221211
111
13321927
Total number of patients . ............9,958
2755542111110
1172110
161211431112
27
211211
111
13211626
12,524
2756433211110
1172110
161210531012
27
121211
101
13221625
12,888
1742321011000
1482211
171200632012
32
111211
162
113117
55,256
2665443111110
1272211
150100532012
27
111211
151
13211614
7,572
2755433211111
1172110
150100532012
26
111211
171
11311614
7,016
aThese data are based on a sample of 192 service providers’ ambulance run repOflS. one primary COmpklnt 1s reportedforeach call Numbersln the table represent thepercentof ambulance servlcecalls forpnmaryc omplamts. Cond!honsrepresenting less than 1 percent of calls were not Ilsted but are included m totals (e.g., drowning IS included In totalInjury).
KEY: CVA = Cardiovascular accident; DOA = dead on arrival; EMS = emergency medical services, OB/GYN =obstetrics-gynecology, TIA = transient ischemic attack
SOURCE’ South Carolina Department of Health and Environmental Control, Columbia, SC, September 1989
vehicle crash mortality (figure 3-2) and there is an evidence suggests that a disproportionate number ofinverse relationship between population density and motor vehicle-related deaths occur in rural areas inmortality (compare figure 3-2 map showing areas general (i.e., not just rural areas with low populationwith high motor vehicle crash-related mortality to density) (figure 3-4). More than half (56.9 percent)figure 3-3 map showing population density). Other of fatal traffic accidents occur in rural areas (as

Table 3-3-Number of Episodes of Persons Injured and Number of Associated Restricted-Activity Days and Bed Daysa
by Whether in Moving Motor Vehicle, Whether at Work, Place of Accident, and Place of Residence: United States, 1987
Number of restricted-activity days Number of bed daysNumber per 100 persons per year (per 100 persons per year) (per 100 persons per year)
MSAb MSA MSA
Central Not central Central Not central Central Not centralType of episode All city city Non-MSA All city city Non-MSA All city city Non-MSA
All episodes . . . . . . . . . 26.6 25.8 27.2 24.0 255.2 277.7 239.9 278.1 80.8 89.6 74.8 83.4Moving motor vehicle:
Total . . . . . . . . . . . . . 2.6 2.1 2.9 2.0 56.5 70.7 46.8 53.1 17.9 23.7 13.9 19.2Traffic only . . . . . . . . 2.1 1.6 2.5 1.8 49.3 62.3 40.5 43.8 15.9 20.5 12.8 15.4
Non-moving motorvehicle . . . . . . . . . 24.0 23.7 24.3 21.7 197.0 204.7 191.7 221.9 62.4 65.6 60.3 63.9
At work c . . . . . . . . . . . . 5.3 5.0 5.4 5.0 96.8 97.9 96.0 100.4 32.2 39.2 27.4 23.0Not at work . . . . . . . . . . 15.8 16.2 15.4 13.2 170.2 198.2 150.8 216.4 49.3 53.5 46.3 72.0Place of accident:
At home . . . . . . . . . . 89 9.1 8.7 8.4 56.4 55.9 56.7 85.0 16.7 11.6 20.2 29.6Street or highway . . 3.5 3.0 3.8 2.4 62.7 78.5 52.0 53.9 20.6 26.7 16.5 17.0Industrial place . . . . 3.2 2.8 3.4 2.9 52.7 57.8 49.2 53.0 17.5 23.1 13.7 9.3d
Other . . . . . . . . . . . . 6.8 7.1 6.6 6.0 58.5 59.5 57.9 61.1 15.4 16.8 14.5 18.3
%Arnates of activity restnct!on and bed days are based on the present effects of the mpmes no matter when they occurredbMSA = metropolitan statlsttcal area.CFor currently employed 18 years Of age and over onlYdFlgure does not meet standard of rehabhty or precmon.
SOURCE: U S Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Center for Health Statistics. Current Estimates from the National HealthInterview Survey: United States, 1987, Series 10, No. 186, DHHS Pub. No. (PHS) 66-1594, tables 51, 53, and 55, September 1988.

Chapter 3-The Demand for EMS Services in Rural Areas ● 21
Table 3-4-Average Annual Number of Injuriesa Per 100 Persons Per Year, by Place of Residence and Type of Injury:United States, 1980-81
MSAb
Central Not centralType of injury All city city Non-MSA
All injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33.2 32.4 34.2 32.6Skull fractures and intracranial injuries . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.2 1.0 0.8Fractures of lower limb . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.7 1.0 1.0Fractures of upper limb, neck, and trunk . . . . . . . . . . . . . . . . . . . . . . . 1.8 1.5 1.9 2.0Dislocations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.6 0.6 0.6 0.6Sprains and strains-total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.6 8.0 7.9 6.9Open wounds and lacerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.0 7.9 8.4 7.8Superficial injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.6 1.7 1.6 1.6Contusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.2 4.4 5.7 5.3Burns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.0 0.8 1.2Toxic effects-nonmedical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.8 0.9 0.8 0.8All other injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.6 4.5 4.6 4.7
a[njuries se~-reported inthet+ealth interview Survey.bMSA. metropo~tanstahsf@ area.
SOURCE: U.S. Departmentof Health and Human Services, Pubhc Health Service, Centers forDlsease Control National CenterforHealth Statwtics, Typesof hjuries and /impairments Due to hjuries.” Lhted States, Series 10, No. 159, DHHS Pub. No. (PHS) 87-1587, table 6, November 1986
Figure 3-l—Death Rates From Unintentional Injury,Suicide, and Homicide by Place of Residence, 1977-79
I Unintentional - motor vehicle
40
Suicide— — — — — — — — — — — — .
Homicide
30 —
20
\— . - - - ”
10 “
Largest Other Other Rural Ruralcitiesa large SMSAC non- remotee
citiesb remoted
aResiderlts d Cttles with 1 fIIilliOn or more Population.bResldents of cmes with population between 250,000 and 1 rnllllon.CReSlden& of Standard Metropolitan Statistical Area (SMSA) counties,
excluding residents of cities of 250,000 or more.~Resldents of nonmetropoiitan counhes that do not meet the definition of
“rural remote. ”eResldents of nonmetropotitan counties that are not adjacent to an SMSA
and have no settlement as large as 2,500 persons.
SOURCE: Susan P. Baker, Brian O’Neill, and Ronald S, Karpf, The /njuryfact Boo& (Lexington, MA: DC. HeaJth & Co., 1984). Reprintedwith Permwslon.
defined by DOT) ( 123) whereas only about one-thirdof the population resides there.
What accounts for the excess motor-vehicledeaths is unclear. Motor vehicle accidents do notseem to occur more frequently in rural areas. In1986, nearly one-fifth (18 percent) of people in-volved in motor vehicle accidents were in rural areas(as defined by DOT) at the time of the accident (table3-6). Given that approximately one-third of the U.S.population is rural (as defined by DOT), this level ofaccident occurrence may even be low.
Despite the fact that accidents seem to occur lessoften in rural areas, persons involved in ruralaccidents are three times more likely to sustainserious or untreatable injuries than those in urbanareas (table 3-6). Many more rural than urbanaccidents occur in areas with higher speed limits—nearly half (48.7 percent) of the accidents in ruralareas took place in areas with speed limits of 55MPH, compared to 8.7 percent in urban areas (seetable 3-6). People involved in accidents in higher-speed-limit rural areas are two to three times as likely tosustain serious or untreatable injuries than thoseinvolved in higher-speed-limit urban areas (2.4percent v. 0.9 percent) (see table 3-6).
Possible explanations for higher rates of motorvehicle-related injury and death in rural areasinclude (14):
. poorer road conditions and the absence ofsafety features such as guard rails;

22 ● Rural Emergency Medical Services
Table 3-5-Death and Disabling Injury Rates Among Workers by Industry, 1988
Deathsc Disabling injuriesd
Workers b Number Rate Number RateIndustrya (in 1,000s) (in 1,000s) (per 100,000s) (in 1,000s) (per 1 ,000)
All industries . . . . . . . . . . . . . . . . . . . . 114,300 10,600e 1,800 16Agriculture . . . . . . . . . . . . . . . . . . . . . . 3,100 1,500 48 f
140 45Mining, quarrying . . . . . . . . . . . . . . . . 800 200 25 30 38Construction . . . . . . . . . . . . . . . . . . . . 6,500 2,200 34 210 32Manufacturing . . . . . . . . . . . . . . . . . . . 19,500 1,100 6 350 18Transportation and public utilities . . . 5,800 1,400 24 140 24Trade . . . . . . . . . . . . . . . . . . . . . . . . . . 27,000 1,100 4 320 12Services . . . . . . . . . . . . . . . . . . . . . . . 34,600 1,500 4 330 10Government . . . . . . . . . . . . . . . . . . . . 17,000 1,600 9 280 16aA~~~Ulture ,ncludes forestry and fishing Mlnlng and quarrying Includes oil and gas extraction. Trade includes Wholesale and retail. serv~~s Includes finance,
insurance, and real estate.%Vorkersare all persons gainfully employed, mcludmg owners, managers, otherpald employees, the self employed, and unpaid family workers, but excludingprivate househo!d workers.
Cunlntentlonal ,njury death (lcD Underlying cau5e of death codes E.800.E949), Death from acc)dent IS a death which occurs wlthm 1 year of the accident.dDlsabllng ,njury ,5 an injury ~uslng death, permanent dlsabitlty, or any degree of temporary total disability beyond the day of the accident.e~out 3,900 of the deaths and 200,000 of the Injuries revolved motor vehicles.f~rlculture rate excludes deaths of ~er~ons under 14 years of age, Rates for other Industry divlslons do not require ttlls adjustment, Deaths of persons under14 are Included In the agriculture death total
SOURCE National Safety Council estimates (rounded) based on data from the National Center for Health Statistics, State wtai statistics departments, andState mdustrlal commmsions. Numbers of workers are based on Bureau of Labor Statlstlcs data and include persons aged 14 and over
Figure 3-2-Motor Vehicle Related Death Rates
SOURCE Baker et al., NEJM 316(22) page 1385
. a greater likelihood of travel at extremely highspeeds (65 MPH or greater);
● greater use of utility vehicles (jeep-like vehi-cles) and pickup trucks, which are associatedwith high death rates:
● lack of use of seat belts; and● greater distances between emergency facilities
and reduced access to major trauma centers.
Higher death rates in rural counties are notexplained by travel in rural areas by residents ofmore densely settled areas6 or by a large volume of
Figure 3-3-Population Density
SOURCE: Baker et al., NEJM 316(22) page 1385.
travel on major routes (14). In fact, none of theFederal interstate highways are distinguishable onthe map as connecting a string of counties with highdeath rates (see figure 3-2).
Reducing the motor vehicle fatality rate to nogreater than 18.0 per 100,000 population is one ofthe national 1990 objectives for injury preventionand control (119).7 This goal has been achieved inU.S. urban areas, where the motor vehicle accidentmortality rate was 17.3 in 1986 (see table 3-7). Incontrast, the rate for rural areas was 28.4. The U.S.
bMolor.vchic]c crash death rates Were a]s~ hlghcs[ in rural ~cas when calculated from National Cenler for Health sUUIStlCS data hal records tie
deceased county of residence instead of the place of accident occurrence.7The ~o~ for tie year 2000 is 17.0 per 100,000 ppulation ~24).

Chapter 3--The Demand for EMS Services in Rural Areas . 23
Figure 3-4--Death Rates From (Motor Vehicle Occupants) 1990 objective would be achieved if there was a 30Motor Vehicle Crashes by Place of Residence, 1977-79 percent reduction in the number of rural motor
30
20
10
0Largest Other Other Rural Ruralcities a large SMSAC non- remote e
citiesb remoted
aReS@ntS of cltles with 1 mllhon or more populationbResldents of cttles with population between 250,000 and 1 mllhon.cResldents of Standard Metropol i tan Statlstlcal Area (SMSA)
cauntles, excluding residents of c[tles of 250,000 or more.dResldents of nonmetrowlltan count~s that do not meet the definition of
“rural remote. ”eResldents of nonmetropolltan counttes t hat are not adjacent to an SMSA
and have no settlement as large as 2,500 persons.
SOURCE Susan P. Baker, Brian O’Nelll, and Ronald S. Karpf, The kyuryFact Book (Lexington, MA D C Health & Co., 1984) Reprintedwith Permlsslon
vehicle fatalities (table 3-7). While there is no clearexplanation for the dramatically higher mortalityrate in rural areas, preventive efforts in rural areasand improving rural EMS systems could prove to beeffective means of realizing the Nation’s objective.

24 ● Rural Emergency Medical Services
Table 3-&Passenger Car Occupant Injury by Land Use and Speed Limit, 1986
Vehicles OccupantsSerious to untreatable
All injuries (AIS > 1)a trauma (AIS > 3)a
Number Number Number Number(in 1,000s) Percent (in 1,000s) (in 1,000s) Percent (in 1,000s) Percent
Urban:25 MPH or less . . . . 1,342 19.6 2,000 349 17.4 8 0.430 to 40 MPH . . . . . 4,064 59.4 6,140 1,281 20.9 25 0.445 to 50 MPH . . . . . 839 12.3 1,245 323 25.9 8 0.655 MPH . . . . . . . . . 596 8.7 901 232 25.7 8 0.9
Total urban . . . . . . . 6,841 100.0 10,286 2,185 21.2 49 0.5
Rural:25 MPH or less . . . 161 11.5 252 40 15.9 1 0.430 to 40 MPH . . . . . 322 23.0 554 152 27.4 3 0.545 to 50 MPH . . . . . 234 16.7 362 109 30.1 7 1.955 MPH . . . . . . . . . . 681 48.7 1,137 349 30.7 27 2.4
Total rural . . . . . . . . 1,398 100.0 2,305 650 28.2 38 1.6
U.S. total . . . . . . . . . 8,239 12,591 2,835 22.5 87 0.7aAls (Abb~~vlated Injury scale) IS Use(j to rate the seventy of trauma, /+ score of 1 indicates minor trauma; 2 Indicates moderate traUma, 3 SerlOUS trauma,
4 severe trauma, 5 crltlcal trauma and 6 maximum trauma (currently untreatable). The scale was developed by the American Assoclatlon for AutomotweMed}clne.
SOURCE: U.S. Department of Transportation, National Highway Traf’hc Safety Admmistratlon, /Vationa/Acciderrt Samp/ing System, 1986, table 111-21.
Table 3-7--Metropolitan (MSA) and Non-Metropolitan (Non-MSA) Motor Vehicle Fatality Rates-1986,and Impact of 30 Percent Reduction in Non-MSA Deaths on Achieving the National 1990 Objective for
Injury Prevention (Motor Vehicle Fatality Rate of 18 per 100,000 population)
1986 1986 Motor vehicleUs . 1986 Motor vehicle accident death rates
population Motor vehicle accident death rates if 30% reduction in(in 1,000s) accident deaths (per 100,000) non-metro MVA deaths
U.S. total . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241,036 47,865 19.9 17.9Metropolitan . . . . . . . . . . . . . . . . . . . . . . . . . . 184,713 31,867 17.3 17.3Non-metropolitan . . . . . . . . . . . . . . . . . . . . 56,323 15,998 28.4 19.9
SOURCES. U.S. Department of Commerce, Bureau of the Census, StakMca/ Abstract of the (hkd States: 1988, 108 edmon (Washington, DC, U.S.Government Prmtmg OffCe, 1987); Department of Health and Human Services, Publlc Health Serwce, “Vital Stat@cs of the US : 1986,” vol. 2,Morta//ty, Pub No. 88-1114 (Washington, DC U S Government Prmtmg Office, 1988)

Chapter 4
EMS in a Rural Context
Several factors may adversely affect the deliveryof emergency medical services (EMS) in rural areas.This section first describes how the changing ruralhealth care environment affects the delivery ofemergency medical services. Second, problems inproviding rural emergency medical services aredescribed as are interventions that may help toovercome them.
THE CHANGING RURAL HEALTHCARE ENVIRONMENT
In some rural areas, a decline in the economy hasoccurred at the same time as major changes in theU.S. health care system. These changes include howhealth care is paid for (e.g., implementation ofprospective hospital payment in the Medicare pro-gram) and how health care is delivered (e.g., a shiftto outpatient services). Making adjustments to thenew national health care environment is difficult formany rural health care systems because they aresmall and lack diversification. Many rural hospitalsthat have not diversified and made other transitionalchanges are now financially vulnerable. Since 1981,nearly 550 rural hospitals have closed (61 ). In somecases, hospital closures do not adversely affectaccess to care and are appropriate (e.g., when a smallcommunity has more than one hospital and servicesare duplicated). However, in communities with onlya single hospital, hospital closure means that accessto hospital-based care is lost and ready access toemergency care is diminished. ’
Health care is inaccessible in some rural areasbecause of shortages of health care personnel. Sixpercent of rural counties (142 of 2,393 nonmetropo-litan counties) have no physicians (11 1 ) and approx-imately one-quarter of rural residents live in areasthat are federally designated health manpower short-age areas (HMSAS).2 Many rural areas have diffi-culty recruiting and retaining physicians, nurses, andother health care personnel because of the heavydemands of rural practice (e.g., longer hours, nobackup) or because there is no hospital or otherresources that attract providers (111). in some areas,personnel shortages have been exacerbated by di-
minished support from Federal programs such as theNational Health Service Corps (11 1). Furthermore.rural areas have been adversely affected by theincreased cost of medical liability insurance cover-age. especially for physicians providing obstetriccare (28).
RURAL HEALTH CARE SYSTEMSAccess to well-trained personnel, essential equip-
ment, and facilities in rural communities without alocal hospital or physician may sometimes beachieved through cooperation with neighboringcommunities with medical resources. As the availa-bility of health care services diminishes in ruralareas, EMS providers may be left assuming newresponsibilities. There may be an increased demandfor nonemergency transportation to hospitals anddemand for urgent primary care services (e.g..delivering babies). Anecdotal evidence suggests thatwhen a community hospital closes, the local EMSsystem has a higher number of calls that arenonemergent in nature ( 103) and there are delays inEMS response times (1 34). In these communities.the EMS system may need to reorient to providesome urgent care or to coordinate with localproviders to make such care available. Rural EMSproviders are having difficulty providing EMSservices even without these additional pressures.Problems in public access to EMS, prehospital care,and medical response are described in the nextsection, as are some potential solutions to theseproblems.
Public Access to EMS Systems
Sparse population, large, remote. or inaccessibleservice areas, poor weather and road conditions, andlimited access to communications may delay detec-tion and reporting of a need for emergency care. Anautomobile accident occurring along an infrequentlytraveled rural road may not be detected for hours.When such an accident is detected, access to theEMS system may be further delayed because phonesor other forms of communication are not available.Installation of emergency call boxes along major ruralhighways. and use of automobile cellular phones3
ZHMSAS Me ~omties, ~~s of ~outlc~, or Spcclfic racllltlcs \V1~ ~nc or fcW,cr ph~sl~lans per 3,()()() or 3,500 population (45 FR 75996).
sRe.lab]c ~ellul~ [clcphonc nc[works arc not Yc[ widely available ( 136)
QThc two States witi statewide 9 I 1 coverage arc Delaware and Maryland ( 105)
-25-

26 Rural Emergency Medical Services
and citizen band radios, could improve public accessin the case of motor vehicle crashes (64,82).
A coordinated communications system that in-cludes a widely recognized method to call for help.such as telephoning 911, facilitates a quick andappropriate EMS response. Trained dispatchers canelicit information about the event and can quicklymarshal needed resources. Appropriately traineddispatchers can also tell the caller what to do untiltrained EMS personnel arrive ( 129). When there ismore than one EMS number in a community.confusion over what number to call may result inresponse delays. As many as 85 emergency numberswere listed in the Greenville, North Carolina phonebook, covering 17 exchanges (52). Several EMSagencies in north-central Florida report that someresidents in their service areas have to use long-distance to call them by telephone (75).
Universal access to emergency care via 911 hasbeen mandated in 14 States, but statewide911 accessto EMS services is actually available in only twoStates (table 4-1) (105).4 Twenty-nine other Statesare at least half-covered by 911 access (table 4-1)(105). About two-thirds of States report having astatewide plan available for EMS communications(table 4-1),
Many rural areas lack central access and dispatchsystems and those with such systems often have oldequipment that needs to be replaced and upgraded(82). Furthermore, there is variability in the qualityof EMS dispatching that could be improved byagreeing on dispatch standards or protocols and byimplementing dispatcher training programs (82).Only six States report that they certify EMSdispatchers or telecommunicators (104).5
Access delays may also occur when the publicdoes not know how to contact the local EMS system.Public education can be effective in improvingEMS-related knowledge. Nebraska’s EMS publicinformation program, for example, appears to havebeen successful in educating the public on how toaccess the EMS system and how to provide some
basic emergency care. According to a statewidesurvey, as many as 83 percent of adults knew thetelephone number of the ambulance/rescue service.over half of the adults had taken first-aid courses, and37 percent had completed CPR training. In addition.virtually all of the secondary schools were teachingCPR (30). Many States, however, lack adequateEMS public education. A 1987 survey indicated thatfour State EMS organizations had no involvement inpublic education efforts.6 In the remaining 47jurisdictions that did have a public education effort,20 self-evaluated their public education programs asminimally effective, 23 considered their programsmoderately effective, and only 4 States rated theireducational programs as highly effective (106).7
EMS response time, the time elapsed from notifi-cation of an emergency to EMS arrival at the scene,tends to be longer in rural than urban areas. In thecase of motor vehicle fatalities, the average responsetime for rural areas (as defined by DOT) is almosttwice that of urban areas (1 1 v. 6 minutes) (123).s Inmany cases, the critical “golden hour’ is exceededbecause of delays in detection and EMS responsetime.
Response times can be reduced if an EMScommunication system is in place and emergencyvehicles can be dispatched from the field (e.g.,redirected when returning from another call). EMScommunications are hampered in many rural areasby radio “dead spots” that occur because of thelimited range of radio signals or because of geo-graphic barriers. Available radio frequencies allowcommunication between a central base station andan ambulance (or other receiver in the field) that are20 to 30 miles apart. To reach beyond these ranges,mechanisms to repeat or relay the signal must beused (129).
Thirty-one States reported that some rural areas oftheir State lacked EMS radio system coverage (82).Communications equipment such as VHF and UHFrelays, radio-telephone switching systems, micro-wave relay, and cellular telephones can overcome
4T~ Iwo s~tes with statewide 911 covcragc are Delaware and Maryland ( 105).
STwenty.foW states and tic Dis~i~l of col~bia repofled lha[ they did not ce~ify EMS dispatchers or kltxornmunkatms. [formation wasunavailable on dispatch certification from the rcmaining 20 States (104).
6The four s~te~ wl~ n. EMS organization Involvement in EMS public cducatlon were Arizona, Delaw~e, buisiana, and south Dakota.
TThe four States hat rat~ heir programs as highly effective were Indiana, Montana, New Mexico, and pemsylvania ~ 1 [M).8Rew~1ng of on-scene ~val times is incomp]e(e, ~ese data arc limited to the 37 States that reported fatal crash scene rc~ponsc times so Pcrcenl
of the time or more in 1987 (123).gIn tie futwe, mobile satellites may be used to improve rural EMS communications (~2).

Chapter 4--EMS in a Rural Context ● 27
Table 4-l-State EMS Communications, 1986-87
Statewide planavailable for EMS Legislation
Percent of populationwith access to EMS service
communications mandating Authority 7-digit MultipleState system 911 for 911 911 number numbers
Alabama . . . . . . . . . . . . . Yes No Local 60 40 0Alaska . . . . . . . . . . . . . . . . . . . . . . No No Local 85 10 5Arizona . . . . . . . . . . . . . . . . . . . . . Yes Yes State 90 NA NAArkansas . . . . . . . . . . . . . . . . . . . . Yes No Local 10 70 0
California. . . . . . . . . . . . . . . . . . . . Yes Yes Local 90 NA NAColorado . . . . . . . . . . . . . . . . . . . Yes No Local 80 0 20Connecticut . . . . . . . . . . . . . . . . . . NA Yes State 65 35 0Delaware. . . . . . . . . . . . . . . . . . . . Yes No Local 100 NA NADistrict of Columbia . . . . . . . . . . . No Yes State 10 NA NAFlorida . . . . . . . . . . . . . . . . . . . . . Yes No State 89 NA NA
Georgia . . . . . . . . . . . . . . . . . . . . Yes No Local 60 100 NAHawaii . . . . . . . . . . . . . . . . . . . . . . Yes No Regional 95 5 0Idaho . . . . . . . . . . . . . . . . . . . . . . . NA No Local 50 45 5Illinois . . . . . . . . . . . . . . . . . . . . NA No Local 50 45 5Indiana . . . . . . . . . . . . . . . . . . . . . NA No Local 40 45 5
lowa . . . . . . . . . . . . . . . . . . . . . . . . Yes No Local NA NA NAKansas . . . . . . . . . . . . . . . . . . . . . Yes No Local 70 30 0Kentucky . . . . . . . . . . . . . . . . . . . . NA Yes State 33 10 57Louisiana . . . . . . . . . . . . . . . . . . . NA No Local NA NA NAMaine . . . . . . . . . . . . . . . . . . . . . . NA No Regional 50 50 0
Maryland . . . . . . . . . . . . . . . . . . . . Yes Yes State 100 NA NAMassachusetts . . . . . . . . . . . . . . . Yes No Local 39 0 61Michigan . . . . . . . . . . . . . . . . . . . . NA Yes State 45 NA NAMinnesota . . . . . . . . . . . . . . . . . . . NA Yes Local 90 10 0Mississippi . . . . . . . . . . . . . . . . . . Yes No Local 50 50 0
Missouri . . . . . . . . . . . . . . . . . . . . Yes No Local 65 35 0Montana . . . . . . . . . . . . . . . . . . . . NA No State NA NA NANebraska . . . . . . . . . . . . . . . . . . . . Yes No State 90 0 10Nevada . . . . . . . . . . . . . . . . . . . . Yes No Regional 80 10 10New Hampshire . . . . . . . . . . . . . . Yes No Local 30 5 65
New Jersey . . . . . . . . . . . . . . . . . . Yes No Local a 27 0 73New Mexico . . . . . . . . . . . . . . . . . . Yes No Local 70 15 15New York . . . . . . . . . . . . . . . . . . . Yes No Local 65 10 25North Carolina.. . . . . . . . . . . . . . . Yes No Local 31 55 14North Dakota... . . . . . . . . . . . . . . NA No Local 32 68 0
Ohio . . . . . . . . . . . . . . . . . . . . . . . . NA Yes NA 30 70 0Oklahoma . . . . . . . . . . . . . . . . . . . Yes Yes Local 7 93 0Oregon . . . . . . . . . . . . . . . . . . . . . . Yes Yes State 90 5 5Pennsylvania . . . . . . . . . . . . . . . . . Yes No Local 45 40 15Rhode Island . . . . . . . . . . . . . . . . . Yes Yes State NA NA NA
South Carolina . . . . . . . . . . . . . . . Yes No Local 35 30 35South Dakota . . . . . . . . . . . . . . . . Yes No NA 60 25 15Tennessee . . . . . . . . . . . . . . . . . . . Yes No Local 50 30 20Texas . . . . . . . . . . . . . . . . . . . . . . . Yes Yes State 20 60 20Utah . . . . . . . . . . . . . . . . . . . . . . . . No No Local 80 10 10
Vermont . . . . . . . . . . . . . . . . . . . . Yes No Local 15 85 0Virginia . . . . . . . . . . . . . . . . . . . . . . NA No Local 79 16 5Washington . . . . . . . . . . . . . . . . . . Yes No Local 80 20 NAWest Virginia . . . . . . . . . . . . . . . . . Yes No Local 15 25 50Wisconsin . . . . . . . . . . . . . . . . . . . Yes No Local 41 30 29Wyoming . . . . . . . . . . . . . . . . . . . . NA No Local 90 4 6aLeglslatton pending,ABBREVIATIONS NA=lnformation not avaflable.
SOURCE: TheNationalEMSClearmghouse, “StateEMSOffce:Communlcafions Programs and DlsasterPreparedness:’ TheCouncflofStateGovernments,iron Works Pike, Lexington, KY,1988.

28 ● Rural Emergency Medical Services
these dead spots but are often too expensive for ruralcommunities (82). In addition to equipment costs,there are training and maintenance costs associatedwith the systems (82).
Radio frequency congestion is hampering EMScommunications in many areas. The congestionoccurs because many public safety services (e.g.,police, fire, local government, highway mainte-nance, and forestry conservation) share radio spec-tra. A special emergency radio service spectrumexists, but it is crowded with unrelated and nonemer-gency medical licensees. In 1987,40 States reportedhaving EMS radio communication interference prob-lems (105). The National Association of State andEmergency Medical Services Directors has recom-
mended that the Federal Communications Commis-sion (FCC) establish a new radio service dedicatedto EMS communications (71). Rural EMS commu-nications-related problems and potential solutionspresented at the March, 1989 “National Rural EMSNeeds Workshop” sponsored by the National RuralHealth Association, are summarized in box 4-A.
Prehospital Care
Prehospital care includes all care provided to anemergency patient prior to arriving at a hospital. Thecare may be provided by any of a number of differenttypes of providers, ranging from accident bystanderstrained in first aid or CPR to highly trainedemergency medical technicians (EMTs). Fire and
Box 4-A—Rural EMS Communications: Problems and Potential Solutions as Presented at the“National Rural EMS Needs Workshop,” March, 1989
Problems Solutions
● Public access to EMS services is hampered by . Develop central access/dispatch systems (e.g., 911).poor communications systems. . Install emergency call boxes along major rural highways.
. The public is uninformed about accessing the . Institute public education campaigns.EMS system.
. Many rural EMS communications systems are ● Improve and upgrade EMS radio communications systems.old and outdated.
. Rural areas have many radio ‘‘dead spots. . Expand coverage to wider areas through VHF and UHFrelays, microwave relay, radio-telephone switching sys-tems, and cellular telephones. Investigate use of mobilesatellites.
. EMS radio frequencies are congested in some . Federal Communications Commission (FCC) should desig-rural areas. nate additional exclusive VHF and UHF frequencies for
EMS.
. EMS communication are not always planned . Coordinate EMS services with local hospitals, FCC-and coordinated with other emergency services. designated frequency coordinators, disaster response,
public service agencies, and local, regional, and StateEMS planning agencies.
. EMS communications vary in quality by State . Develop consensus standards for EMS communicationsand area. equipment, radio frequencies, and dispatch centers. Estab-
lish standardized EMS communications protocols in eacharea or region under physician medical control anddirection.
. Provide technical assistance and training to upgradequality.
● Provide quality assurance programs for EMS communicationsoperations.
. What EMS communication systems are most . Conduct research on the cost-effectiveness of differentsuited to certain rural environments is unknown. types of EMS communications systems.
SOURCE: National Rural Health Association, “National Rural EMS Needs Workshop,” March, 1989, proceedings published in JEMS, June1989. Sponsored by the National Rural Health Association,

Chapter 4--EMS in a Rural Context ● 29
police department personnel may provide prehospi-tal care in addition to other services, such asextricating victims of motor vehicle crashes andcontrolling or preventing fires at the scene of anincident. Prehospital care may be provided at thescene of the emergency and while in transit to ahospital or trauma center. Among the factors thateffect the quality of prehospital care are:
the training of those administering care;the availability of transportation and of medicalequipment during transport;communications between prehospital providersand hospital-based providers; andthe existence of protocols for the type ofmedical assistance offered and the transfer ofpatients to an appropriate level of care.
Prehospital Care Providers
First Responders-When EMS response timesare long because of an area’s remoteness, roadconditions, or lack of EMS resources, communitymembers can be trained as ‘‘first responders” todeliver basic EMS care. First responders administerfirst aid, cardiopulmonary resuscitation (CPR) orother interventions until the ambulance (or aircraft)arrives at the scene. (See box 4-B---description ofprehospital care providers and their level of training)( 104). At least 42 States and the District of Columbiaofficially recognize first responders as providers ofemergency medical services (104).
Nationwide, over 100,000 first responders havebeen trained and certified (see table 4-2) (104), butStates have used different models to deliver thiscare. Some first responder programs rely on police,fire, or medical personnel within the community,while others rely on trained community volunteers.In some areas of rural Vermont, for example,‘‘off-dut y” rescue personnel (known as ‘‘jumpcrews’ can be summoned to an emergency viatwo-way portable radios from their home or otherremote location to provide basic and intermediatelife support until an ambulance arrives (51). Here,the first responders are highly trained and experi-enced. However, it may be difficult to find volun-teers that have time for both first response andambulance duties. In Idaho, quick response units(QRU) made up of trained volunteers have beenorganized throughout the State to offer basic life-support level service (7). First responders have been
used to provide advanced first aid and emergencycare in rural Georgian communities that lack both aresident physician and an ambulance service. Theirresponse times of 4 to 5 minutes compared favorablyto the average ambulance response time of 20minutes (69). Publications and courses are availablefor farm families and workers that provide emer-gency procedure instructions for bystanders of farmaccidents (67).
Emergency Medical Technicians—Ambulancecrews staffed by emergency medical technicians(EMTs) offer most prehospital care. In urban areasthe EMTs are usually paid, while in rural areasapproximately three-quarters of rural prehospitalEMS providers are volunteers (7). In some “fron-tier” States characterized by sparse populationsettlement (e.g., Idaho), about 90 percent of EMSprehospital personnel are volunteers (7). Withoutvolunteers, many rural communities would be una-ble to support an EMS system. Some rural countieshave no trained EMT providers. These communitiesrely on providers whose training is limited to first aid(45).
In general, rural EMS volunteer providers do nothave as high a level of training as urban providers.(See box 4-B for a description of the types ofprehospital care providers and their level of train-ing.) Most rural EMTs are “Basic EMTs” and canprovide noninvasive procedures such as first aid,maintaining an adequate airway, administering oxy-gen. and CPR. In some States, Basic EMTs arepermitted to perform more advanced skills such asmaintaining intravenous (IV) lines. An average of134 hours of training are required to become abasic-level EMT (104). A basic EMT may acquireadditional specialized training to treat patients withcardiac arrest due to ventricular fibrillation, withdefibrillator. (See ch. 5 for a more completediscussion of emergency cardiac care.)
Paramedics have the basic skills of an EMT butare also trained in Advanced Life Support (ALS).ALS-trained paramedics can start IV lines, givemedications, and intubate a patient whose upperairway is blocked (see box 4-B. responsibilities ofEMS personnel), Paramedic training usually in-volves about 750 hours (104). More than two-thirdsof States certify an intermediate level EMT (some-times called intermediate EMT or EMT-n).10 Their
l~~y.eight s~tes and (he District of Columbia reco~ize intermediate level EMTs ( IW).
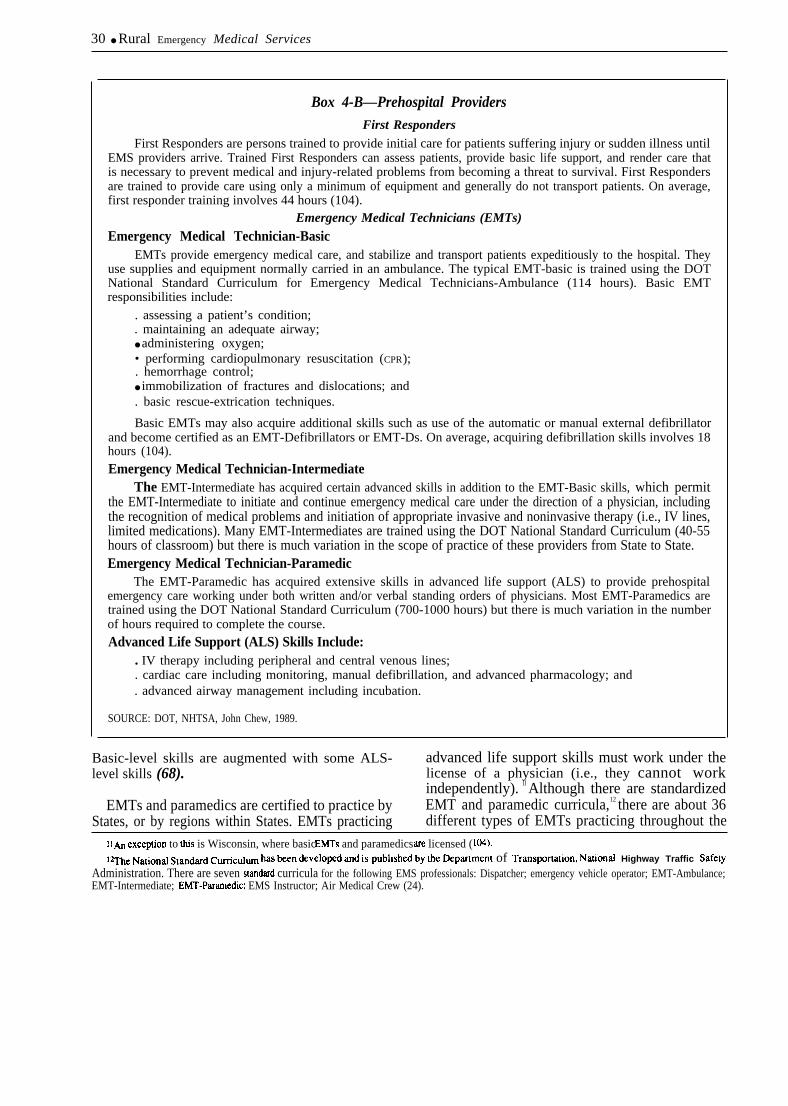
30 ● Rural Emergency Medical Services
Box 4-B—Prehospital ProvidersFirst Responders
First Responders are persons trained to provide initial care for patients suffering injury or sudden illness untilEMS providers arrive. Trained First Responders can assess patients, provide basic life support, and render care thatis necessary to prevent medical and injury-related problems from becoming a threat to survival. First Respondersare trained to provide care using only a minimum of equipment and generally do not transport patients. On average,first responder training involves 44 hours (104).
Emergency Medical Technicians (EMTs)
Emergency Medical Technician-BasicEMTs provide emergency medical care, and stabilize and transport patients expeditiously to the hospital. They
use supplies and equipment normally carried in an ambulance. The typical EMT-basic is trained using the DOTNational Standard Curriculum for Emergency Medical Technicians-Ambulance (114 hours). Basic EMTresponsibilities include:
. assessing a patient’s condition;
. maintaining an adequate airway;● administering oxygen;• performing cardiopulmonary resuscitation (CPR);. hemorrhage control;● immobilization of fractures and dislocations; and. basic rescue-extrication techniques.
Basic EMTs may also acquire additional skills such as use of the automatic or manual external defibrillatorand become certified as an EMT-Defibrillators or EMT-Ds. On average, acquiring defibrillation skills involves 18hours (104).Emergency Medical Technician-Intermediate
The EMT-Intermediate has acquired certain advanced skills in addition to the EMT-Basic skills, which permitthe EMT-Intermediate to initiate and continue emergency medical care under the direction of a physician, includingthe recognition of medical problems and initiation of appropriate invasive and noninvasive therapy (i.e., IV lines,limited medications). Many EMT-Intermediates are trained using the DOT National Standard Curriculum (40-55hours of classroom) but there is much variation in the scope of practice of these providers from State to State.Emergency Medical Technician-Paramedic
The EMT-Paramedic has acquired extensive skills in advanced life support (ALS) to provide prehospitalemergency care working under both written and/or verbal standing orders of physicians. Most EMT-Paramedics aretrained using the DOT National Standard Curriculum (700-1000 hours) but there is much variation in the numberof hours required to complete the course.Advanced Life Support (ALS) Skills Include:
. IV therapy including peripheral and central venous lines;
. cardiac care including monitoring, manual defibrillation, and advanced pharmacology; and
. advanced airway management including incubation.
SOURCE: DOT, NHTSA, John Chew, 1989.
Basic-level skills are augmented with some ALS- advanced life support skills must work under thelevel skills (68). license of a physician (i.e., they cannot work
independently). ll Although there are standardizedEMTs and paramedics are certified to practice by EMT and paramedic curricula,12 there are about 36
States, or by regions within States. EMTs practicing different types of EMTs practicing throughout the
11~ exception to MS is Wisconsin, where basic EMTs and paramedics ~ licensed ( IW).12~C Nation~ stand~d ~Cul~ has ~n &velo@ and is publlsh~ by me ~p~rnen[ of TrmSpo~liOn, Nationat Highway Traffic safety
Administration. There are seven standard curricula for the following EMS professionals: Dispatcher; emergency vehicle operator; EMT-Ambulance;EMT-Intermediate; EMT-Panrnedic; EMS Instructor; Air Medical Crew (24).

Chapter 4--EMS in u Rural Context ● 31
United States (97).13 If number of hours in trainingis an indicator of level of skills acquired in training.there are dramatic differences in skill levels. Thenumber of training hours required of basic EMTsranges from 104 in California to 315 in Hawaii.Paramedics are trained in 185 hours in Pennsylvaniaand 2,278 hours in Vermont (Vermont requires a6-month internship) (104). Despite the variation inhours of training required by States, most trainingprograms adhere to the National Standard Curriculaand meet or exceed established behavioral objec-tives (24).
Certification requirements for volunteer EMSproviders vary by State. Alabama, for example,exempts its EMS volunteers from certification (90).EMT certification requirements may even varywithin a State. In California the regulatory authorityfor EMTs rests with local government, so require-ments may vary by county. Some States will certifyEMTs who are certified by other States or registeredwith the National Registry of EMTs.14 EMTs needto be periodically recertified, usually every 2 to 3years (104).
In many rural areas the pool of potential EMSvolunteers is reported to be getting smaller aseconomic conditions have made it more difficult forrural residents to have the spare time required forvolunteer activities (1 12). It may be especially hardto get volunteers for daytime shifts (60). Theavailability of prehospital providers varies by State.Alabama has less than 1 EMT per 10,000 popula-tion, while South Dakota has nearly 5 per 10,000(see table 4-2) (104). Nationally, there is a shortageof trained paramedics, and ambulance services inrural areas often cannot afford to hire those that areavailable (39). The availability of paramedics alsovaries markedly by State; Mississippi has less thanone paramedic per 100,000 population while Floridahas nearly 5 paramedics per 100,000 residents (seetable 4-2) (104).
Potential disincentives to become trained as anEMT include the costs of initial training andrecertification, inaccessibility of training, concernsregarding liability, and fear of contracting conta-
gious diseases such as AIDS. The problem ofproviding volunteer EMT training in rural areas maybe alleviated with mobile EMT courses, correspon-dence courses. or courses adapted to VCRs for homeuse. Despite evidence of prehospital personnelshortages, few States provide financial assistance totrain prehospital providers. According to a 1986survey, only three States financially support theirfirst responder trainees, 12 States support EMTtrainees, and 5 States support paramedic trainees(104).15
The relatively small populations that characterizerural areas mean a low volume of emergency cases.In the face of low volumes, it is difficult for the ruralprehospital providers, especially those trained at theparamedic level, to maintain their skills. Rural EMSproviders could maintain and improve skills throughadditional inservice training, locating EMTs andparamedics in local emergency rooms,16 periodiccase critiques by medical advisers, and trainingEMTs in such intermediate skills as advancedairway management, IV therapy, and/or defibrilla-tion (i.e., upgrade the basic EMT to the Intermediate-level EMT).
An example of an innovative continuing educa-tion training program adapted to the needs of ruralproviders is the Idaho EMS Mobile Trauma TrainingUnit. Rural EMTs have an opportunity to maintainor upgrade skills through training programs thatemphasize application of practical skills. In 1984,the mobile unit made training available to 150 ruralcommunities throughout Idaho, providing traumaskills training for about 2,000 EMTs (10).
Idaho has also offered continuing educationprograms to EMS personnel throughout the State viaa‘‘telelecture’ program. Through teleconferencing,lectures by EMS experts have been ● ’attended”simultaneously by as many as 1.000 EMS personnelin 71 classrooms widely dispersed throughout theState (9). The system operates at relatively low costbut is dependent on a sophisticated statewidecommunication system, which includes mountain-top stations connected by microwave links toregional hospitals and to the Idaho Statewide EMS
l~Much of tie v~atlon in types of EMTs OCCLKS because S[atcs have adopted very different standards for inkmncdialc-level EMTs.14 Twenty five states and he ~s~c~ of Co]umbia use tic Nationa] Regis~ of Ems’ ex~inalion as tie basis of certification. An additional six States
accept National Registq examinations in Iicu of their State examinations. State policies dlctatc the ability to obtain cross-State certification. The NauonalRegistry of EMTs facilitates cross-State certification ( 110).
lsFo~y.Wven States responded to tic S~eY
l~egon has fip]ernenl~ a grant-funded, week-long urban ‘‘extcmship” program for rural EMTs (137).
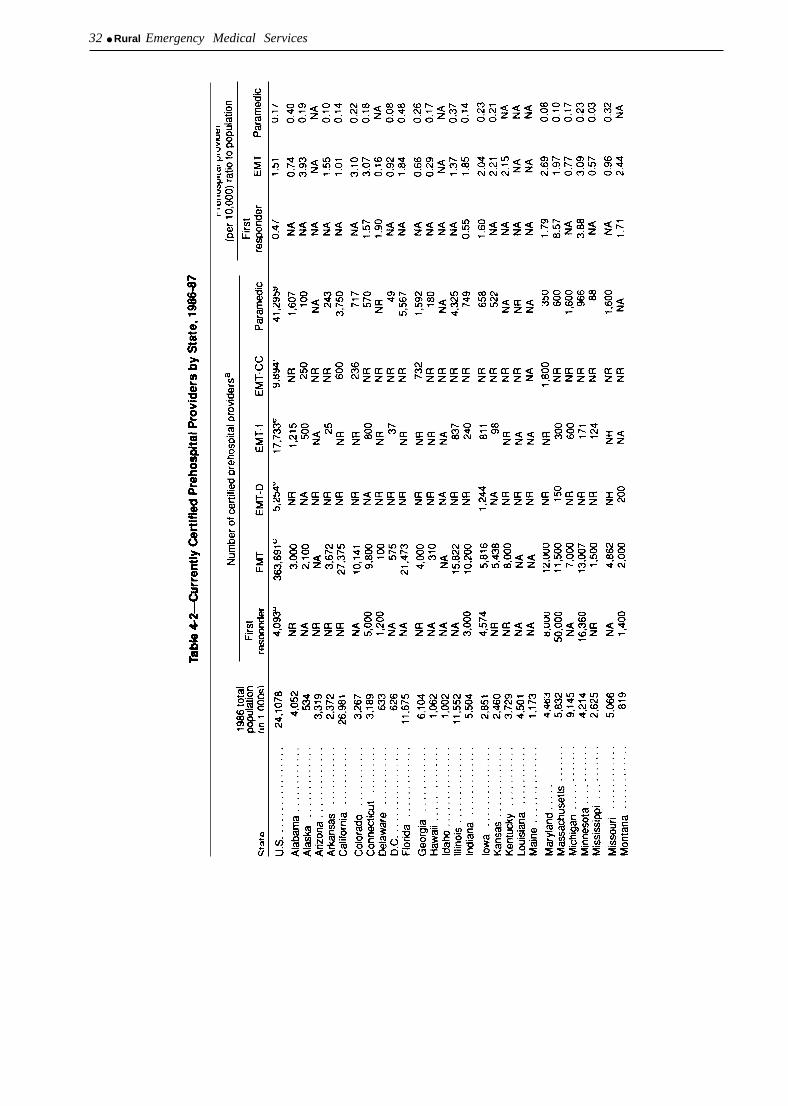
32 ● Rural Emergency Medical Services
-

Table 4-2-Currently Certified Prehospital Providers by State, 1986-87--Continued
Prehospital providerNumber of certified prehospital providers (per 10,000) ratio to population
1986 totalpopulation First First
State (in 1,000s) responder EMT EMT-D EMT-1 EMT-CC Paramedic responder EMT Paramedic
Nebraska . . . . . . . . . . .Nevada . . . . . . . . . . . . .New Hampshire . . . . . .New Jersey . . . . . . . . .New Mexico . . . . . . . . .
New York . . . . . . . . . . .North Carolina . . . . . . .North Dakota . . . . . . . .OhioOklahoma; . . . . . . . . . . . . . .
Oregon . . . . . . . . . . . . .Pennsylvania . . . . . . . .Rhode Island . . . . . . . .South Carolina . . . . . . .South Dakota . . . . . . .
Tennessee . . . . . . . . . .Texas . . . . . . . . . . . . . .Utah . . . . . . . . . . . . . . .Vermont . . . . . . . . . . . .Virginia . . . . . . . . . . . . .
Washington . . . . . . . . .West Virginia . . . . . . . .Wisconsin . . . . . . . . . . .Wyoming . . . . . . . . . . . .
1,598963
1,0277,6191,479
NANA1,200NA
500
7,500NA
18,0009,2002,600
NANA750
NRNA
NANA300
NA360
NANRNRNRNR
NANA
1401,112
240
1,385985
41NA225
6802,868
12853
61
6954,466
27628
NA
NANA1.17NA
0.34
NANA
0.44NANA
0.960.27NANANA
0.500.59NANANA
4.69NA
17.531.211.76
1.572.332.62NA
0.70
1.561.951.330.944.94
1.271.152.292.26NA
NANA0.140.150.16
17,7726,333
67910,7523,305
NANA
298NANA
27,94014,742
1,776NA2,310
NA114143
NR150
2,0261,424
29NA300
2,554256
NRNRNA
0.080.160.06NA
0.07
0.250.240.010.250.09
2,69811,888
9753,377
708
2,6003,243NANANA
4,20223,199
1,3003,1603,500
6,07819,2303,8181,225NA
8,8489,872
13,4002,100
350NR110
NRNR
1,300NR
520227
7
4001,704
490NRNA
4,80316,685
1,665541
5,787
4,4621,9184,785
507
2,4009,857NRNANA
NANR100
1,229NR
NA1,3161,718
383NA
NR765650650
NANRNRNANA
NR872
NRNR
0.140.270.170.05NA
1,261NA2,500
700
404NR250
60
665175525
30
0.28NA
0.521.38
1.985.152.804.14
0.150.090.110.06
Note NA =mdlcates Information not avalktieNR =prowder category not recognized/certifted by State.
aPrehosphal providers can hold more than one Certlficatlon In some States (e.g., certified as a paramedic an an EMT) and therefore the total number of prehospital providers by State cannot bedetermmed from this table.
bFlrst responder~lght states do not recognize first responders. An additional 25 States do, but dld not provide InformationCE~+II States recognize EMTs Seven States dtd not provide Information.dEM.~28 States do not recognize EMT-Ds. An additional 9 States do, but dld not prowde Information.eEMT-/-l I States do not recognwe EMTIs An additional 11 States do, but dld not prowde lnfOrmatlOnfE~T.C~3 States do not recc)gnlze EMT-CCS An additional 7 States do, but dld not prowde InformationgPararned/P2 States do not recognize pararnedcs An additional 9 States do, but dld not provide Information
SOURCE. National EMS Clearinghouse, “Tralnlng and Certiflcatlon of EMS Personnel,” January 1989.

34 ● Rural Emergency Medical Services
Communications Center (8). At the present time,few other States are using teleconferencing orcomputers for training.
Given the time and cost of training, it is importantto retain as many volunteer EMTs as possible. Thereis little information, however, about how longvolunteers remain in service. In West Virginia,where volunteer EMTs have to be recertified at leastevery 2 years, the average stay for an EMT is a littleover 2½ years (90), In Colorado. 15 percent ofEMTs do not become recertified. Surveys of volun-teer prehospital care providers suggest that amongthe most important factors that lead them to leaveEMS service are: economic conditions in rural areas;fear of personal risk; and costs associated withvolunteer work (62). Professionalization of volun-teer EMS services and management training mayresolve some other factors that lead volunteers todrop out, namely interpersonal conflicts, and thestress and burnout associated with EMS work (11 2).
Providing workers’ compensation for duty-related injuries and protection from liability mighthelp retain experienced rural EMS volunteer provid-ers. New York provides compensation coverage foralmost 400 volunteer squads. following passage ofthe Volunteer Ambulance Benefit Law (90).18 Vol-unteer fire fighters and EMTs would receive a taxcredit of $100 dollars under a Wisconsin bill thatwas recently introduced (Wisconsin, Assembly Bill2). On the Federal level, the Volunteer ProtectionAct (H.R. 91 1), currently under consideration byCongress, encourages States to grant certain volun-teers (such as those volunteering for nonprofit EMSdepartments) immunity from personal civil liability.Box 4-C summarized some of the problems relatedto maintaining qualified prehospital care providersin rural areas identified at the March 1989 NationalRural EMS Needs Workshop.
Transportation
EMS transport may be difficult in rural areasbecause of small, widely dispersed populations,geographic barriers, and inclement weather. Asdefinitive care is often located in distant cities, oneapproach to decreasing time to definitive care is to
improve the rural EMS transportation system. Ruraltransport may be improved through better organiza-tion of existing ground-based resources and by usingair medical transport services.
Ground Transportation
Nationally, there are over 12,000 ambulanceservices with nearly 35,000 ambulances (108). MostStates have developed regulations and standards forthe design of ambulance vehicles and equipmentused by EMS personnel, and for various EMSservices and personnel (108). Emergency vehiclesmay be classified as Basic Life Support (BLS),Advanced Life Support (ALS), or Mobile IntensiveCare Units (MICU), depending on their equipmentand staffing. The proportion of ambulance servicesstaffed by basic EMTs, intermediate EMTs, orparamedics varies by State. In North Dakota, forexample, only 3 of 130 ambulance services arestaffed by paramedics. In contrast, more than one-half of ambulance services in Florida, Missouri, andWest Virginia are staffed by paramedics ( 108).
Rural areas with no EMS prehospital system, orindependent but under-utilized systems, may con-sider linkage models to provide or improve services.Smaller population centers can be grouped into EMSservice areas and share resources. Recognizing thatcomplete ALS-level ambulance service coveragewas neither practical nor financially feasible in ruralnortheast Missouri, EMS planners developed a‘‘nodal’ ● concept of EMS. As shown in figure 4-1,BLS and ALS ambulance services are evenlydistributed throughout the region to promote accessto ALS care and to achieve an ambulance responsetime of 30 minutes or less. Most of the region iswithin 15 to 20 miles of EMS service, but ALSresponse times will likely exceed 30 minutes insome areas within the region (39).
Air Medical Transport
Rural areas that lack roads or are far fromhospitals are especially dependent on air medicaltransport services when medical emergencies occur.There are currently over 200 U.S. air medicalprograms that transport approximately 140,000 pa-
170nly MasWChWtts, Rh~e Is]and, SOu~ c~olina, and !VisConsin report using teleconferencing as part of the trtining process. Mwland and south
Carolina repot-l using computers for [raining (104).Igvo]unteer firefighters already had compensauon coverage.

Chapter 4--EMS in a Rural Context ● 35
Box 4-C—EMS Prehospital Personnel: Problems and Potential Solutions as Presented at the“National Rural EMS Needs Workshop,” March 1989
Problems Solutions
. There are shortages of volunteer EMS provid- . Outreach to high school groups, the elderly, ethnicers in rural areas. minorities and other groups traditionally not involved as
EMS volunteers.. Make EMS training more accessible to rural residents by
using alternative instructional modes such as videotapesand correspondence courses.
. Assure the availability of instructors in rural areas byrecruiting and training rural practitioners as trainers.Alleviate financial burdens of becoming an EMS volun-teer by providing tax credits, training scholarships, orliability insurance.
. The level of training of rural prehospital . Provide financial incentives for rural EMS providers toproviders is substantially below that of urban upgrade their skills in the form of training scholarships,providers. and tax breaks.
. Develop programs to allow rural prehospital providers tomaintain skills through such devices as accident simula-tion.
. The EMS standard training curricula does not . Conduct research to determine the knowledge required toalways reflect the needs of rural areas. carry out EMS field operations.
. Provide specialty courses suited to the needs of the ruralprovider (e.g., farm rescue).
. Rural EMS providers frequently lack guid- . Designate responsibility for medical control. Provideance from physicians. physicians charged with medical control responsibilities
appropriate training and orientation. Develop medicalcontrol consensus standards.
SOURCE: National Rural Health Association, “National Rural EMS Needs Workshop, ” March, 1989, Proceedings Published m JEMS, June1989. Sponsored by the National Rural Health Association.
tients a year, but evidence suggests that air medical are offered through the military (MAST)19 or areservices are unavailable in many rural areas.
Air medical programs use both fixed-wing aircraft(airplanes) and helicopters. Airplanes or helicoptersare used in interhospital transfers of critical patients,such as heart disease patients and newborns requir-ing intensive care. Helicopters are generally moresuitable than airplanes for transporting patients froman accident site to a hospital because of theirflexibility in landing at a scene and at a traumacenter. Geography and weather conditions such asheavy snow storms may, however, limit the use ofhelicopters. About 80 percent of helicopter transportservices are hospital-based, 10 to 15 percent areoffered through public agencies, and the remaining
privately run (29).
Helicopter service augments the ground ambu-lance program and should be used in instances wheretime, distance, medical personnel need, or sceneisolation warrant it (97). Air medical services areusually based at urban tertiary care hospitals. Theservice area extends about 150 miles beyond the airmedical base which generally includes rural areas. Itmay, however, take a helicopter as long as 90minutes to travel 150 miles. Fast airplanes areusually used for longer transports. Sparsely popu-lated States such as Alaska, Texas, Arizona, Mon-tana, and Wyoming rely primarily on airplanes fortheir EMS transports. In other areas, most EMS airtransport is provided by helicopters (97).
1’%4AST st~ds for ~]i~ Assistance [O safety and Traffic. Since 1969, 29 MAST programs have augmented some civilian EMS s~s(cms WI~military helicopters. MAST serves many ruraJ areas (91).

36 ● Rural Emergency Medical Services
Figure 4-1--A Nodal Concept of EMS for Rural Northeast Missouri
o Advanced Basic or Basic Life Support15 mile radius
o Advanced Life Support20 mile radius
SOURCE: East, S. and Tenbrink, T.D., 1989 (see ref. 39)
Many helicopter-transported patients are traumapatients, but only 15 to 25 percent of helicoptertransports emanate from the scene of an accident—most (75 to 85 percent) are interhospital transports(56). Many trauma cases are initially transported byground ambulance to a community hospital wherethe patient is resuscitated and stabilized before beingtransferred to tertiary care via helicopter.
The number of helicopter medical transport serv-ices has increased rapidly in the last 20 yearsfollowing successful experience with helicoptertransport during the Vietnam war. The availability ofair medical transport, however, varies widely byState (see table 4-3; and figures 4-2 and 4-3). Anestimated 20 percent of the population lack airmedical coverage, and the greatest voids are in ruralareas (97). Maine, Vermont, and New Hampshire
lack helicopter transport but have programs thatborder their States. Some evidence suggests thatproviders in rural areas delay requesting helicoptertransport when it is needed (41).
A few areas in the country may have too muchcoverage. Missouri, with 2.7 helicopters per millionpopulation has 3 times the national average (.9 permillion) and health planners have suggested thatthere be a freeze placed on acquiring new helicopters(65).
In some rural areas, there may be inadequateaccess to air medical transport services because thelow volume and high costs of providing the serviceare deemed “uneconomical” by privately run airmedical services. Sometimes service is inadequatebecause regionalization is lacking. Several programs

Chapter 4--EMS in u Rural Context ● 37
have, however, successfully extended service intorural areas using satellite placement of aircraft. TheMissouri Staff for Life program at the University ofMissouri, Columbia, for example, has located one ofits helicopters at a satellite location 62 miles southof the host facility at a rural level II trauma center.Satellite placement improves access to transport insouthern Missouri, where over half of the program’spatient volume is generated. Satellite placement wastried in northern Missouri but was not feasiblebecause of relatively low patient volume and a lackof local providers that could staff the helicopter.Northern Missouri is now served by a fast aircraftlocated in Columbia (97). The Flight for LifeProgram in Milwaukee, WI has also used a satellitehelicopter 50 miles south of the host facility toimprove response times in rural areas. Arizona andIllinois have achieved statewide access to air medi-cal services through a merger of public and privateair transport services. Here, aircraft are used for bothair medical and law enforcement purposes (97).
As helicopter services have proliferated, ques-tions have arisen regarding their costs. appropriateutilization, and safety. Helicopters cost from 1 to 2million dollars each and operating costs averageabout $650,000 per year (97).20 Surface ambulances,in contrast, cost about $75,000 and operating ex-penses average under $200,000 (97). The averagenumber of patient transports per aircraft is 300-500patients per year with optimal utilization at 500-700transports (97). With these costs and necessaryvolume, small rural communities cannot reasonablyacquire their own helicopters. However, in manyrural areas, helicopters are the only way to receiveneeded emergency medical care quickly. Some ruralareas have a sufficient volume of cases to be servedby private air medical companies. Where volume isinsufficient, States could help ensure that servicesare available to rural areas by encouraging State andprivate cooperative agreements, by promoting off-site placement of helicopters where feasible, utiliz-ing MAST resources where available, or throughsubsidies.
Medical Control
The quality of prehospital care may be compro-mised if ‘medical control’ is not provided. Medicalcontrol requires adequate communications systems
Table 4-3-Ratios of Helicoptersa to Populationby State, 1988
Rank 1987 Number of Rate/order State population helicopters million
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051
MontanaNorth DakotaArizonaOklahomaSouth DakotaMissouriColoradoTennesseeWyomingIdahoNevadaAlaskaNebraskaIowaAlabamaD.C.West VirginiaWashingtonLouisianaKentuckyNew MexicoArkansasUtahMississippiOhioMichiganNorth CarolinaTexasFloridaIllinoisMinnesotaVirginiaWisconsinPennsylvaniaSouth CarolinaCaliforniaGeorgiaKansasOregonIndianaMassachusettsConnecticutMarylandNew JerseyNew YorkVermontRhode IslandNew HampshireMaineHawaiiDelaware
Total:Averages:
809,000672,000
3,386,0003,272,000
709,0005,103,0003,296,0004,855,000
490,000998,000
1,007,000525,000
1,594,0002,834,0004,083,000
622,0001,897,0004,538,0004,461,0003,727,0001,500,0002,388,0001,680,0002,625,000
10,784,0009,200,0006,413,000
16,789,00012,023,00011,582,0004,246,0005,904,0004,807,000
11,936,0003,425,000
27,663,0006,222,0002,476,0002,724,0005,531,0005,855,0003,211,0004,535,0007,672,000
17,825,000548,000986,000
1,057,0001,187,0001,083,000
644,000243,399,000
53
1210
214
810
1221357137652323
1296
1410
934372
16311221112000000
2264,43
6.184.463.543.062.822.742.432.062.042.001.991.901.881.761.711.611.581.541.341.341.331.261.191.141.110.980.940.830.830.780.710.680.620.590.580.580.480.400.370.360.340.310.220.130.110.000.000.000.000.000.00—
0.93aNumber of hel~opters IS based on Assoclatlon of Alr Medical services
(AAMS), formerly the American Assoaatlon of Hosplt al Based EmergencyAlr Medical Serwces (ASHBEAMS). Some nonhosplt al based helicopters(e.g., public safety services) were excluded from these counts.
SOURCE Mlssourl Health Faclhtles Rewew Committee, “M!ssourl AlrAmbulance Report—1989,” January 1989.
zOA@lane ~an~po~ation se~lces generally opcra~e at 25 (o 40 per~en[ of tie cost of he]lcopter services kcauw most airplane SCNICt.3S N(? tlOt
dedicated solely to air medical transportation and opcratmg costs are lower (9’7).

38 ● Rural Emergency Medical Services
Figure 4-2-Estimated U.S. Air Ambulance Distribution, 1988a
Rate/million population
0.00
❑ 0.01-0.99
1.00-1.99
2.00-2.99
3.0+
Average of 4.3 Air Ambulance Units per State and an average of 0.93 per million population
%Jumber of helicopters is based on Association of Air Medical Services (AAMS), formerly the American Association of Hospital Based Emergency Air MedicalServices (ASHBEAMS). Some nonhospltal based hel~opters (e.g., public safety services) were excluded from these counts.
SOURCE: The Missouri Health Facxllhes Review Committee, “Mlssourl Alr Ambulance Report,” January 1989.
and commitment from the medical community. It issometimes difficult to get rural physicians to providemedical guidance in the form of practice guidelines(off-line medical control) and on-scene and transportmedical advice via radio (on-line medical control).Many emergency room medical directors in ruralhospitals are not EMS specialists and thereforecould benefit from training and orientation regarding
their medical control responsibilities (82).2] Con-sensus standards for medical control may be particu-larly useful in rural areas.
Prehospital providers may need advice regardingwhere to take an emergency patient. As the triagedecision is often critical to patient survival or death,the highest available level of medical expertiseshould be brought into the triage decision-making
21A tr~nlng COWW for phy~icians on [hc provision of mcdica] con~o] for EMS is under devc]oprnent by tie American cO]kgC Of EITW&31Cy
Physicians (ACEP) (63).

Chapter 4--EMS in a Rural Context ● 39
Figure 4-3--U.S. Helicopter Medevac Programs
Medevac sites+ 156 Hospital based
* 30 Public service
. 1 2 I n d e p e n d e n t
Two hundred and thirty-one helicopter ambulance services are run in 46 States and the District of Columbia by hospitals, the military andState and local police-and rescue services as of 1987. At least 19 additional programs are scheduled to start by early 1988.SOURCE: A. Schneider, Rescue at Risk, The Pittsburgh Press, 1987.
process. This responsibility is usually assumed bythe local emergency department physician (5). Someareas have designated trauma or critical care centersand explicit triage policies (see discussion in ch. 5).In other areas, policies dictate that patients be takento the nearest hospital. Critical trauma patients maybe transported to a trauma center after beingstabilized at a local hospital, but in some casesimmediate transport to the trauma center is required.It is especially important that medical control beavailable to prehospital care providers when triagepatterns are not explicit.
Fear of litigation may discourage some physiciansfrom providing medical control to the local EMSsystem. As of 1987, 18 States had enacted legislationthat protects physicians from civil liability when
they assume EMS medical control responsibilities(109).
Medical Response
Although many of the events precipitating theneed for EMS occur at the same rate in urban andrural areas, the level of hospital care required torespond to emergent events is not equally available.Because large numbers of people are concentrated inurban areas, the specialized services required to carefor the most acutely ill and injured patients can bemaintained. In rural areas, however, emergent eventsoccur infrequently, making it economically difficultto maintain a tertiary-level facility. Furthermore, itis difficult for rural EMS providers to maintainspecialized skills when they are infrequently used.When faced with emergencies that require services

40 ● Rural Emergency Medical Services
beyond those available in the local health caresystem, rural communities must have a system inplace to stabilize and transport patients. Integrationof levels of care or a referral systems approach toEMS are, however, nonexistent in many rural areas.
While access to specialized services, such as thoseavailable in a trauma center, is central to a good EMSsystem, local resources must be adequate to handlethe majority of EMS cases that do not require thesespecialized services. Most calls to an EMS systemcan be appropriately handled at a communityhospital. For example, about 90 to 95 percent oftrauma cases can be treated adequately at a commu-nity hospital (5), while only 5 to 10 percent of casesare critical and require more specialized services. Inthe evaluation of EMS systems, it is as important toexamine the availability of local hospital resourcesas it is to examine access to more distant specializedresources, such as trauma centers.
When a rural area has a community hospital, italmost always (98 percent) has an emergency roombut rarely has a trauma center (see table 4-4).22 Ingeneral, there are few specialized emergency physi-cians (i.e., Board-certified emergency physicians)and nurses in rural hospitals. Instead, physicians andnurses tend to be generalists who must provide carein all of the various hospital specialty areas. Theyprovide care in the emergency room if and when apatient presents there. These providers may not onlylack the specialized training required to appropri-ately manage emergency patients, but they often donot have the opportunity to frequently practicenecessary EMS skills and maintain proficiency(53,63). Making continuing education courses inemergency medicine available to physicians practic-ing in rural areas could effectively improve thecommunity hospital’s EMS medical response andimprove the quality of medical control of thecommunity’s EMS system.
EMS treatment delays may occur in rural hospi-tals because rural emergency departments are oftennot staffed by a physician 24 hours a day. In Idaho,for example, only 9 of the State’s 48 hospitals have24-hour physician coverage (108). Many rural hos-pitals have trouble paying for 24-hour emergency
room physician coverage and opt for rotating,on-call coverage (87).
Emergency room nurses are usually availableuntil the physician arrives, and outcomes of patientswith life-threatening emergencies may be improvedby upgrading and maintaining their skills (93). Asurvey of nurses providing emergency room care inrural areas cites understaffing of emergency depart-ments, underqualified nurses and physicians, a lackof continuing education programs, and the absenceof statewide emergency standards as among the mostserious problems facing rural emergency nurses(37). As of 1986-87, however, only Arizona, Illinois,and the District of Columbia had EMS offices thathad set minimum standards for nurse emergencydepartment practice. Furthermore, a 1986-87 Statesurvey showed that few State EMS offices wereconducting training programs for nurses (107).23
An innovative approach to continuing educationfor rural EMS providers is the use of computer-basedsimulation programs similar to those used to instructpilots. One such program includes a series of EMSpatient-management problems designed to helpphysicians, nurses, and critical care providers sharpentheir ability to make clinical decisions (43).
Regionalization
Many States have designated specialized facilitiesfor the treatment of trauma, burn, or other types ofemergency patients. Before designating facilities,States usually adopt standards for personnel andequipment that must be met before designation canoccur. Some States “verify* facilities that meet thestandard while others ‘‘designate’ facilities thatmeet the standards according to the State’s needs.Under the verification process, as many facilities asmeet the standard may be used for specializedservices. In contrast, under the designation process,facilities often compete to be designated (108).Facilities have been verified or designated for theirtrauma care, spinal injury care, poison centers,psychiatric services, burn centers, and cardiac care(108). Some States have triage criteria that specifywhen patients should bypass a nonspecialized hospi-tal for a specialized one (see ch. 5). The presence ofwritten agreements (sometimes called transfer agree-
22Whe~e. or ~ol ~ h~spi[~ has a tra~a ~cnler de~nds largc]y on the num~r of hospi(~ kds. Nearly one-lltird of rural hospitals with 20010300
beds have a trauma center.zJStates EMS offices ~a~ were offering nurw [r~nlng (or providing financia] assistance for training) include Alaska, Illinois, Maryland,
Massachusetts, Nevada, New Jersey, New Mexico, and Rhode Island ( 107).

Chapter 4-EMS in a Rural Context ● 41
Table 4-4--Percent of Community Hospitals With EMS-Related Servicesin Metropolitan and Nonmetropolitan Hospitals by Bed Size (under 300 beds), 1987°
Hospital location and bed size Emergency department Trauma center Blood bank
(number of hospitals) Percent Number Percent Number Percent Number
AMetropolitan:6-24 (22) . . . . . . . . . . . . . . . . . . . . 81.8 (18) — (o) 22.7 (5)25-49 (122) . . . . . . . . . . . . . . . . . . 83.6 (102) 3.3 (4) 52.5 (64)50-99 (363) . . . . . . . . . . . . . . . . . . 94.8 (344) 5.0 (18) 69.7 (253)100-199 (693) ., . . . . . . . . . . . . . . 96.7 (670) 16.2 (112) 77.8 (539)200-299 (571) . . . . . . . . . . . . . . . . 97.5 (557) 28.2 (161) 84.2 (481 )
Total (1 ,771) ., . . . . . . . . . . . . . . 95.5 (1 ,691) 16.7 (295) 75.8 (1 ,342)
Nonmetropolitan:6-24 (183) . . . . . . . . . . . . . . . . . . . 94.5 (173) 0.5 (1) 45.4 (83)25-49 (753) . . . . . . . . . . . . . . . . . . 97.9 (737) 2.9 (22) 49.8 (375)50-99 (831) . . . . . . . . . . . . . . . . . . 98.7 (820) 6.5 (54) 66.8 (555)100-199 (526) . . . . . . . . . . . . . . . . 97.7 (514) 16.0 75.5 (397)200-299 (132) . . . . . . . . . . . . . . . . 97.7 (1 29) 31.8 (42) 87.1 (11 5)
Total (2,425) . . . . . . . . . . . . . . . . 97.9 (2,373) 8.4 (203) 62.9 (1 ,525)
%ommunity hospitals are defmd as short-stay, non-Federal, nonspec!alty hospitals.
SOURCE: OTA analysis of data from The American Hospital Assoclatlon 1987 Annual Survey of Hospitals.
ments) between facilities providing different levelsof care can expedite a rapid patient transfer and maysave a rural hospital the cost of upgrading equipmentand resources.
Social and Political Constraints on Rural EMSDevelopment
Efforts to upgrade and regionalize rural EMSsystems are sometimes impeded by social andpolitical factors. Rural areas are frequently charac-terized by older, less affluent, and more traditionalresidents that may be less knowledgeable about theuse and efficacy of emergency medical services, andbe slower to accept new patterns of health caredelivery. Rural residents have been characterized(even by rural residents themselves) as “parochial,’“fiercely independent,” distrustful of urban initia-tives, and leery of control by State or FederalGovernments (135).
A rural community’s desire for local control andautonomy is oftentimes antithetical to the effort tocreate coordinated, regional EMS systems. In oneNew England State, the desire for local autonomywas intense; each community, regardless of size,wanted its own physician, its own ambulanceservice, and its own hospital (135). This pattern isneither cost-effective nor conducive to the mainte-nance of skills by the volunteer ambulance atten-dants. It has led to an excess of vehicles, anenormous EMS training burden because of the largenumber of volunteers required to staff the service, amultiplicity of dispatch centers, a suboptimal distri-
19-758 - 89 - 3 : QL 3
bution of vehicles, and a complicated coordinationtask (135). In the mid-1970’s, the region received alarge grant to establish a central communicationscenter with 911 access for all emergency services.Although the central communications center wasestablished, a 911 access system was not because ofopposition from 19 volunteer fire chiefs who wantedto retain dispatch rights. Consequently, a system ofcentral dispatch and 911 access remained elusivegoals for this area (135).
Efforts to regionalize services have sometimesfailed even when incentives such as free equipmentare offered in exchange for cooperation. In onePacific Northwest rural community, for example,local leaders decided not to request Federal fundingto purchase much-needed EMS communicationsequipment, because they wanted to avoid restric-tions attached to Federal funds for EMS even thoughthe town could not afford the equipment.
Some rural communities oppose governmentalregulation and intervention in the private sectoroperation of EMS services and there is oftenresistance to the passage of mandatory standards forEMS providers, vehicles, and facilities. Sometimes.resistance is simply due to the fact that localresources may be unavailable to upgrade the EMSsystem to meet new standards. Furthermore, nationalstandards may be viewed as inflexible and not suitedto the unique circumstances of rural areas. Withoutstandards, however, there is wide variation in thequality of services available in rural areas. Some

42 ● Rural Emergency Medical Services
local governments have agreed to subsidize a privateambulance service, but they often have not providedfor performance standards, ambulance regulations,contracts, or other needed mechanisms of publicaccountability for the tax dollars provided (135).
What may appear to outside EMS observers to bea major improvement in the quality of prehospitalcare may not be perceived as such by local residents.In one small community, for example, the localfuneral home (one of the last in the State still in theambulance business) decided to withdraw fromambulance service provision in the face of increas-ing financial losses and the possibility of the passageof State ambulance regulations. A pair of experi-enced paramedics from a nearby metropolitan areatook over the service and the town progressedrapidly from an inadequate, antiquated funeral homesystem to a well-equipped and well-staffed basic lifesupport system with advanced life support capabili-ties. The public, however, missed the low ratescharged by the funeral home (which had providedthe service largely for public relations reasons), wereunaware of the significant improvement in thequality of care, and did not understand why theparamedics spent so much time at the scene of theEMS incident (to stabilize the patient prior totransport). They much preferred the funeral homeservice.
One strategy that EMS leaders could use toameliorate some of the rural constraints on EMSsystem-building and regionalization is public educa-tion regarding the importance of EMS and how EMSsystems are organized. EMS leaders, for example,could make presentations at schools, city councilmeetings, senior citizen groups, civic clubs, andhealth fairs. They can also educate members of thelocal media concerning EMS issues, since the mediacan be an extremely effective means of raising theawareness of the public and elected officials.
The functions of State and regional EMS agenciesand councils could be supported as they can serve as
a valuable technical resource for rural providers,advising them concerning financial management,liability insurance, and third-party reimbursement;providing training equipment and courses; andseeking out public and private financial assistance.A decentralized structure of county and regionalcouncils may be effective in rural States marked byextreme local independence.
EMS leaders could attempt to capitalize on thecompetitiveness characteristic of rural towns andambulance service providers. For example, if EMSleaders can persuade the members of a key volunteersquad of the need for training, and modern equip-ment and vehicles, their example is likely to piquethe competitive spirit in neighboring squads, whomay then follow suit. The dedication of ruralvolunteers is impressive and can be a valuable assetin building and maintaining an EMS system.
While there are examples of communities thathave resisted EMS systems development, there arenumerous rural communities that have developedmodel EMS systems.
24 In the rural Texas panhandle,for example, an EMS system has been developed toprovide services in a 26 county, 26,000 square-milearea. The Panhandle Emergency Medical ServicesSystem (PEMSS) was originally federally funded,but it is now a nonprofit corporation sustainedthrough fees paid by 56 ambulance services locatedwithin the region.
25 Membership dues provide fortraining programs, vehicle and equipment pur-chases, quality assurance programs, ongoing com-munications networking, and system evaluation.26
Hospitals in the region are categorized according tolevel of care and there are comprehensive prehospi-tal medical and transport protocols. The region hasa single regional medical communications networkthat reaches throughout the Panhandles’ vast area(58).
24DHHS*S Offiw of’ RLWd Health Policy will complete some rurat EMS case studies by early 1990 (32).25~e pE+fSS mem~rs pay $0,17 ~r individ~l residing in tie member’s service area, FWS range from $45 to $36,000 per year (58),26pEMSS is ~on~oll~ by a ~~d of ~r~to~ hat governs tie organization with advisement from a regiona] advisory COMIIIlttfX (58).

Chapter S
Emergency Cardiac and Trauma Care in Rural Areas
Caring for victims of cardiac arrest and traumarepresent two of the most common demands of theemergency medical services (EMS) system. In thissection, the care of patients with these conditions isused to illustrate the special problems of deliveringEMS services in rural areas.
CARDIAC CARECardiovascular disease is the primary cause of
death in the United States, accounting for nearly halfof all deaths. More than half of cardiovasculardisease deaths are caused by coronary heart disease.and most of these deaths occur suddenly (suddencardiac arrest), usually outside of hospitals (52). ]
Requests for EMS services are more likely to berelated to complications of medical conditions suchas heart disease than for trauma. In rural Texas, forexample, about one in seven calls for EMS servicesare attributed to heart complications (see table 3-1).Coronary heart disease death rates are 25 percenthigher in rural areas but the fact that the ruralpopulation has proportionately more older residentsmay largely explain this difference (table 5-1 ).
At present, no more than 5 percent of suddencardiac arrest victims are successfully resuscitated,but the combination of a well-organized EMSsystem and the application of a relatively newtechnology—the automated external defibrillator—could raise the proportion of successful resuscita-tions 2 to as high as 30 percent (52). Factors thatmaximize a patients chances of recovering followingcardiac arrest relate to time to care and the skills ofthe prehospital provider. Providing cardiac EMScare quickly is essential but difficult in many ruralareas. In the case of cardiac arrest, cardio pulmonaryresuscitation (CPR) must begin within 4 minutes anddefinitive care within 10 minutes of a cardiac arrest(1 15). Rural EMS systems are at a disadvantage intreating cardiovascular emergencies because theyoften lack paramedics, who are much more success-ful than basic emergency medical technicians (EMT)in treating cases of prehospital cardiac arrest (52).Some evidence suggests that paramedics are aseffective as physicians in diagnosing and treating
acute cardiovascular emergencies (52). The skills ofthe basic EMT can, however, be upgraded so that heor she can use an external defibrillator to improve theoutcomes of patients suffering cardiac arrest.
Manual or automatic external defibrillators can beused to deliver electric countershocks to patients inventricular fibrillations.3 Manual defibrillator re-quire the operator to read an electrocardiogram andto determine if the heart rhythm warrants the use ofdefibrillation. Automatic or “smart” defibrillators.developed in the early 1980s, perform these func-tions and deliver a countershock when ventricularfibrillation is detected. The automatic defibrillatorallows persons with less medical experience andtraining to effectively treat critical dysrhythmia (79).
Paramedics and EMTs trained in advanced lifesupport (e.g., intermediate EMTs) can use externaldefibrillator. In addition, basic EMTs can receiveadditional training in the use of external defibrilla-tors and be certified as EMT-Ds (EMT-Defibrilla-tors). Basic-level EMTs can be trained to use manualdefibrillation in 16 to 20 hours and to use automaticdefibrillator in about 4 hours (1 00). In the future,first responders and other community members maybe trained in its use because automatic externaldefibrillator are so easy to use (52). Familymembers or fellow workers may defibrillate cardiacarrest victims at home or at work with a recentlydeveloped device that is stationed at home or workbut is connected to a hospital base station by phone.When a cardiac arrest occurs, the bystander canactivate the device to dial the hospital base stationautomatically, and after getting advice from aphysician (based on electrocardiogram readings). adefibrillating shock can be administered by phone(36).
Defibrillator, when used effectively by EMTs,can potentially save one out of five cardiac arrestvictims if used soon after a cardiac arrest (52). andsome studies have found lower cardiac arrest mortal-ity in communities where EMTs have been trainedto defibrillate ( 102). Not all communities. however,have the resources or the conditions that would
Icoronq hc~ dlxa.w is ~ausc~ bY ~hangcs In tic ~crlcs ]eadlng [~ ~C heafl (~oronq ~crlcs) tha( in[crfcrc with adcqua[c blood floW.
2A successful resuscitation is one that results m [he pahcnt surviving w hospl[al dlschargc (52).
3vcnt~1Cu]N fib~ll]a[lon, tie rhy~m most Of[cn ass~cla[cd wl~ ~~dia~ ~csl, is a Condllion in which the hem mus~les twitch in an uncoordinated
fashion, intcrfcnng with the pumping of blood ( 115).
- 4 3 -

.
Table 5-l—Deaths Attributed to Cardiovascular Disease by MSA/non-MSA Residence, 1986
Us. MSA Non-MSA
Crude a Crude Crudedeath rate death rate death rate
Cause of death Number (per 1 ,000) Number (per 1,000) Number (per 1 ,000)
All causes . . . . . . . . . . . . . . . . . . . . . 2,105,361 8.7 1,533,914 8.3 571,447 10.1Major cardiovascular diseasesb . 968,240 4.0 696,865 3.8 271,375 4.8
Diseases of the heartc . . . . . . 765,490 3.2 554,564 3.0 210,926 3.7Ischemic heart disease
(coronary heart disease)d . 520,729 2.2 377,888 2.0 142,841 2.5Other heart diseasee . . . . . . . . 215,315 0.9 153,527 10.8 61,788 1.1
aThe ~.u~ death ~a~e is ~alculat~ by dlv~lng the num~r of resident deaths by the area’s total population. It IS not adjusted to take an area’s age dlstrlbutlonmto aeeount.
biCD-390-448.clCD 390-398, 402, 404-429.dlcr) 410-414.elCD 415-429.
SOURCE: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Center for Health Statistics, VitalStatistics of the United States, 1986, vol. II—Mortality, Part B, table 8-9.
permit effective use of this technique by EMTs.Furthermore, a few States do not permit basic-levelEMTs trained as EMT-Ds to operate the defibrilla-tion equipment (74).
EMT-D programs are most cost-effective incommunities with more than a thousand people, orthose large enough to expect more than one out-of-hospital cardiac arrest each year. The costs ofinstituting an EMT-D program include training andequipment cost? and the salary of a medical director.In order to institute an EMT-D program, a medicaldirector must assure quality control through supervi-sion of trained EMTs.5 In some States, ‘‘standingorders’ from the medical director permit EMTs todefibrillate, while other States require direct radiocontact (telemetry) with the medical director.6 Defi-brillation, to be effective, must be instituted shortlyafter the onset of the heart attack. EMT-D programsare therefore most effective where cardiac arrests arewitnessed and when CPR is started by bystanders oremergency personnel within 4 minutes of thevictim’s collapse. In addition, EMT response timesmust be short-not more than 10 minutes-or thechances of survival are slim (1 15,130).
If communities are small, community membersare not trained in CPR, and response times are 10
minutes or more, a community should direct itsresources to improving these conditions beforeinstituting an EMT-D program (115,130). Becausemost cardiac arrests occur at home, in men over 60years old, some have recommended that CPRtraining be targeted to middle-aged women and thatphysicians encourage the families of cardiac patientsto learn CPR (52). Several communities havedeveloped dispatcher CPR programs where an EMSdispatcher offers CPR instruction to bystanders untilan EMS crew arrives at the scene (52).
Rural providers may have difficulty maintainingmanual defibrillation skills, as some estimatesindicate that a rural EMT-D in a small communitymay manage a cardiac arrest as seldom as once every8 years (100).7 To overcome this problem, practicalskills review should occur at least every 3 months(52). Automatic external defibrillator (AEDs) areparticularly well suited to the needs of rural areasbecause they are easier to use than manual defibrilla-tors and do not usually require recertification (100).Basic-level EMTs can quickly learn how to place thedefibrillator’s paddles and to start the automatedsystem. The AED will defibrillate only in thepresence of ventricular fibnllation.8
4Sm~] ~ulomaljc defibrlllators WC ~vai]ab]e for ~[wecn $5,~(~ [o $9,()()(), making ~cm affordable for many rural communities.
5Det~led, ~tep.by-~tep infomallon “n ~lannlng and implementing an EMT-D program Wa.S published in a Ihrec-part artic]c in MC Journal Of
Emergency Medical Services (33,34,35).6The llcen~e of tic mcdlca] director provldcs the authority for certified EMTs to dia~osc cardiac arrhythmias and IO usc a defibrillator.
7The respn~lblll(y, for rc]atlvc]y few Cwdlac ~est$ (approxlmaLe]y I per 1,~() popu]ali~n per yc~) may be shared by as man) aS 20 voiuntccrs in
a small community (100).8Ver1ficat10n tha[ ~ Pa[len( is ~ctua]]y in ~~dlac ~cs[ by determination of pu]sclcssness is cri[i~al and Yet difficull for (hc untrained. other conditions
such as seizures might confuse mcdlcally unskilled operators and potentially, a countcrshock could be lethal if administered inappropriately (52).

Chapter S--Emergency Cardiac and Trauma Care in Rural Areas . 45
Improving rural response time to cardiac arrestcalls can be achieved by stationing defibrillatorwith one or more on-call EMT-Ds instead of with theambulance. EMTs carrying defibrillator can pro-ceed directly to the patient while another EMT goesto the station house for the ambulance. Some ruralambulance services are notified by pager or tele-phone and then respond first to the ambulancegarage, then to the patient. Some services requireambulances to remain at the garage until at least twoor even three EMTs arrive, which delays response(loo).
Prehospital care providers may become moreinvolved in the treatment of patients with acutemyocardial infarction. Thrombolytic agents—drugsto restore blood flow to the heart-are now commonemergency room treatments for this type of heartattack. Some evidence suggests that if an adequatediagnosis is made, patients can safely be giventhrombolytic treatment in the field and transferredby ambulance (89). This may be a promisingintervention in some rural areas where time toemergency room care is long.
TRAUMA CAREInjury 9 occurs with about equal frequency in
urban and rural areas but tends to be more severe inrural areas (table 3-2). Motor vehicle accidents, forexample, occur with equal frequency (see table 3-5)but are more likely to occur at higher speeds in ruralareas and result in more serious injuries. Motorvehicle-related mortality is consequently 1.6 timeshigher in rural than urban areas (table 3-6). From 15to 30 percent of calls for EMS care in rural areas arerelated to injuries, but only about one-tenth of thesecalls would represent severe or critical injuries.When severe injuries do occur, they require immedi-ate medical attention and. sometimes, specializedtrauma care that may be far from rural areas. Anumber of factors may contribute to the severity ofinjury and higher injury-related mortality seen inrural areas (55):
● there may be long delays between the injuryand its discovery by a passerby;
● it may take a long time to get a patient from thescene of an accident to a hospital because ofdistances between the scene, the ambulanceservice, and the hospital;
●
●
●
●
●
prehospital care in many rural areas may beperformed by volunteers with basic EMT orfirst aid level training who are unable toprovide advanced airway management or vol-ume resuscitation;emergency departments in small rural hospitalsmay be staffed by primary care physicianswithout the knowledge or skills needed forcritical trauma management;there may be relatively few trauma cases at therural hospital, making it difficult for physiciansand nurses to maintain their skills;rural hospitals may not have 24-hour physicianand ancillary staff coverage (e.g., anesthesia,X-ray, and lab); andin situations involving multiple victims, delaysmay occur in the initial stabilization of thepatients because there are too few physicians ornurses available.
As many as 50 to 60 percent of critically injuredtrauma patients die before reaching the hospital (5)and another 20 percent die within the next 4 hours(66). Some estimate that 20 to 45 percent of thosewho reach the hospital alive but eventually die couldbe saved if regional systems of trauma care were inplace (16,19). Some argue that less than 10 percentof the United States has an effective trauma systemin place, but that with additional support, existingtechnology and expertise could be organized toprevent these avoidable deaths (16, 19). Basic infor-mation is lacking, however. on when, where, andwhy rural injury and injury-related deaths areoccurring. Before implementing programs to im-prove rural trauma outcomes, it would be useful toknow more about the causes and consequences ofrural trauma, where along the continuum of caredeaths are occurring (e.g., during the prehospital orhospital phase), and whether these deaths are poten-tially preventable. Implementing programs withoutsuch information may lead to inefficient use oflimited resources (24),
With available information, it is difficult to knowwhere to place limited resources. For example. if theexcess motor vehicle-related mortality in rural areasoccurs because of delays in discovering victims whohave had accidents on infrequently traveled ruralroads, improvements in the medical care system willprobably not prevent these deaths. Instead, improve-ments in road safety or communications (e.g.,
91nJuv and ~auma arc synonymous ~c~s.

46 ● Rural Emergency Medical Services
placing more call boxes along the sides of roads)may prove effective. Severity of injury in rural areasmay be higher because of a lack of adherence toeffective preventive practices. If, for example, ruralresidents are less likely to use seatbelts, are morelikely to exceed speed limits, and drive while drunk,public education campaigns and better enforcementof existing laws to support preventive practicesmight effectively reduce motor vehicle-related mor-bidity and mortality.
Because time to emergency care is such a crucialfactor in determining the trauma patient’s outcome,higher trauma-related mortality might be expectedin rural areas due to delays in detection and responsetimes. In some remote rural areas, delays areunavoidable, but response times can be improved insome areas by increasing the number of availableambulances, improving air medical services, orchanging the placement of ground or air transport.Reducing delays to emergency care can also beaccomplished by shifting the onset of emergencytreatment to the prehospital period. If rural EMTswere lacking the training to provide specific types ofcare that would benefit rural trauma patients, invest-ing in EMT training would clearly be warranted.Training the public in basic emergency care so thataccident bystanders are prepared to offer assistanceuntil an emergency vehicle arrives could also extendthe “golden hour* needed for trauma patients.
If there were evidence that prehospital care isadequate, but that deaths are occurring in ruralhospitals that are ill-equipped to provide traumacare, then resources could be directed to improvinghospital resources and the training of hospital-basednurses and physicians. It is possible that some ruraltrauma patients, needing the specialized services oftrauma centers, are not being transferred to thesefacilities quickly, or at all. If this were the case,improvements in regional systems—specifically,the institution of protocols guiding the transfer ofpatients from a rural hospital to trauma centers—could be considered. Unfortunately, there is notmuch quantitative evidence available to help poli-cymakers rationally allocate limited resources. Thissection reviews the available evidence and profes-sional opinion that lend support to specific interven-tions aimed at improving the outcomes of traumaoccurring in rural areas.
Prevention Education
There is evidence that public education is neededto improve rural residents’ preventive health behav-iors. Only 25 percent of rural residents report usingseatbelts all or most of the time as compared tonearly 40 percent reported by urban residents. Notusing seatbelts regularly appears to be a particularproblem among young adult males in the rural West.Here, only 16 percent report using seatbelts all ormost of the time, as compared to 30 percent amongtheir urban counterparts (table 5-2). Seatbelt usereduces front-seat, passenger vehicle, occupant fa-talities by about one-half (24).
The proportion of alcohol drinkers reporting thatthey had driven a car at least once in the past yearwhen they thought they might have had too much todrink is generally not that much higher in rural thanurban areas (18 percent v. 17 percent) but amongyoung adults, especially those in the Midwest,drinking and driving appears to be a serious problemin rural areas. Among rural, Midwestern, youngadult males who drink, over one-half report drivingafter having too much to drink (see table 5-3).
In addition to public education, States could beencouraged to adopt seatbelt laws and drunk drivinglaws and, where laws exist, actively enforce them.Thirty-four States have safety belt use laws and suchlaws reduce front-seat, passenger vehicle. occupantfatalities by about 7.5 percent (24).
Prehospital Care
There continues to be considerable controversysurrounding the appropriate level of prehospital carefor trauma patients. The majority of EMTs in ruralareas are trained to provide basic life support (BLS)prehospital care. Paramedics are trained in advancedlife support (ALS) which permits them to initiatetreatments including advanced airway management,administration of intravenous (IV) fluids, and decom-pression of tension pneumothorax. In the urbanenvironment, where level I or II trauma centers arewithin 20 minutes reach, it may be better to have thetrauma patient rapidly transported to the traumacenter than to take time to provide ALS in the field(15). Some studies in urban areas suggest that this“scoop and run” approach is preferable becausewhile providing prehospital ALS improves thechances that the trauma patient arrives at the hospitalalive, it doesn’t seem to improve the trauma patientsultimate outcome (80). There are few controlled
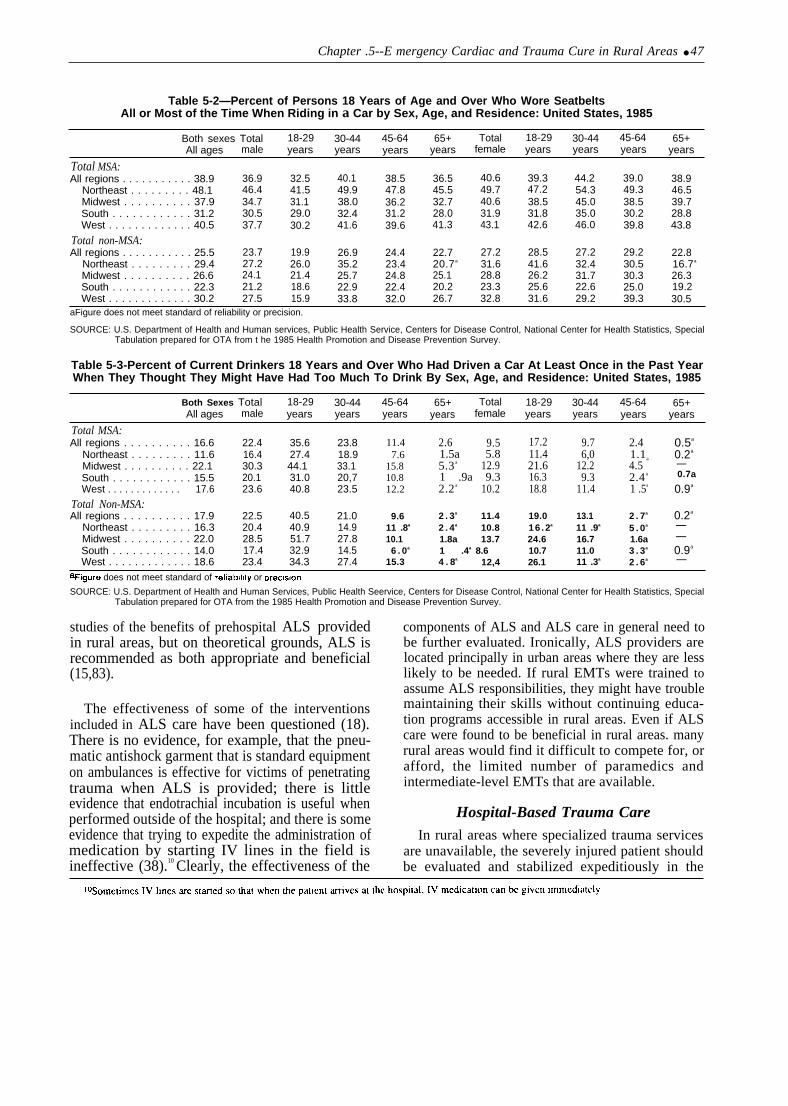
Chapter .5--E mergency Cardiac and Trauma Cure in Rural Areas ● 47
Table 5-2—Percent of Persons 18 Years of Age and Over Who Wore SeatbeltsAll or Most of the Time When Riding in a Car by Sex, Age, and Residence: United States, 1985
Both sexes Total 18-29 30-44 45-64 65+ Total 18-29 30-44 45-64 65+All ages male years years years years female years years years years
Total MSA:All regions . . . . . . . . . . . 38.9 36.9 32.5 40.1 38.5 36.5 40.6 39.3 44.2 39.0 38.9
Northeast . . . . . . . . . 48.1 46.4 41.5 49.9 47.8 45.5 49.7 47.2 54.3 49.3 46.5Midwest . . . . . . . . . . 37.9 34.7 31.1 38.0 36.2 32.7 40.6 38.5 45.0 38.5 39.7South . . . . . . . . . . . . 31.2 30.5 29.0 32.4 31.2 28.0 31.9 31.8 35.0 30.2 28.8West . . . . . . . . . . . . . 40.5 37.7 30.2 41.6 39.6 41.3 43.1 42.6 46.0 39.8 43.8
Total non-MSA:All regions . . . . . . . . . . . 25.5 23.7 19.9 26.9 24.4 22.7 27.2 28.5 27.2 29.2 22.8
Northeast . . . . . . . . . 29.4 27.2 26.0 35.2 23.4 20.7a 31.6 41.6 32.4 30.5 16.7a
Midwest . . . . . . . . . . 26.6 24.1 21.4 25.7 24.8 25.1 28.8 26.2 31.7 30.3 26.3South . . . . . . . . . . . . 22.3 21.2 18.6 22.9 22.4 20.2 23.3 25.6 22.6 25.0 19.2West . . . . . . . . . . . . . 30.2 27.5 15.9 33.8 32.0 26.7 32.8 31.6 29.2 39.3 30.5
aFigure does not meet standard of reliability or precision.
SOURCE: U.S. Department of Health and Human services, Public Health Service, Centers for Disease Control, National Center for Health Statistics, SpecialTabulation prepared for OTA from t he 1985 Health Promotion and Disease Prevention Survey.
Table 5-3-Percent of Current Drinkers 18 Years and Over Who Had Driven a Car At Least Once in the Past YearWhen They Thought They Might Have Had Too Much To Drink By Sex, Age, and Residence: United States, 1985
Both Sexes Total 18-29 30-44 45-64 65+ Total 18-29 30-44 45-64 65+All ages male years years years years female years years years years
Total MSA:All regions . . . . . . . . . . 16.6 22.4 35.6 23.8
Northeast . . . . . . . . . 11.6 16.4 27.4 18.9Midwest . . . . . . . . . . 22.1 30.3 44.1 33.1South . . . . . . . . . . . . 15.5 20.1 31.0 20,7West . . . . . . . . . . . . . 17.6 23.6 40.8 23.5
Total Non-MSA:All regions . . . . . . . . . . 17.9 22.5 40.5 21.0
Northeast . . . . . . . . . 16.3 20.4 40.9 14.9Midwest . . . . . . . . . . 22.0 28.5 51.7 27.8South . . . . . . . . . . . . 14.0 17.4 32.9 14.5West . . . . . . . . . . . . . 18.6 23.4 34.3 27.4
11.47.6
15.810.812.2
9.611 .8a
10.16 . 0a
15.3
2.6 9.5 17.2 9.7 2.41.5a 5.8 11.4 6,0 1.1a
5.3 a 12.9 21.6 12.2 4.51 .9a 9.3 16.3 9.3 2.4 a
2.2 a 10.2 18.8 11.4 1 .5a
2 . 3a 11.4 19.0 13.1 2 . 7a
2 . 4a 10.8 16 .2a 11 .9a 5 . 0a
1.8a 13.7 24.6 16.7 1.6a1 .4a 8.6 10.7 11.0 3 . 3a
4 . 8a 12,4 26.1 11 .3a 2 . 6a
0.5a
0.2a
—0.7a
0.9a
0.2a
——0.9a
—
+Igure does not meet standard of rellablhty or preclslon.
SOURCE: U.S. Department of Health and Human Services, Public Health Seervice, Centers for Disease Control, National Center for Health Statistics, SpecialTabulation prepared for OTA from the 1985 Health Promotion and Disease Prevention Survey.
studies of the benefits of prehospital ALS providedin rural areas, but on theoretical grounds, ALS isrecommended as both appropriate and beneficial(15,83).
The effectiveness of some of the interventionsincluded in ALS care have been questioned (18).There is no evidence, for example, that the pneu-matic antishock garment that is standard equipmenton ambulances is effective for victims of penetratingtrauma when ALS is provided; there is littleevidence that endotrachial incubation is useful whenperformed outside of the hospital; and there is someevidence that trying to expedite the administration ofmedication by starting IV lines in the field isineffective (38).10 Clearly, the effectiveness of the
components of ALS and ALS care in general need tobe further evaluated. Ironically, ALS providers arelocated principally in urban areas where they are lesslikely to be needed. If rural EMTs were trained toassume ALS responsibilities, they might have troublemaintaining their skills without continuing educa-tion programs accessible in rural areas. Even if ALScare were found to be beneficial in rural areas. manyrural areas would find it difficult to compete for, orafford, the limited number of paramedics andintermediate-level EMTs that are available.
Hospital-Based Trauma Care
In rural areas where specialized trauma servicesare unavailable, the severely injured patient shouldbe evaluated and stabilized expeditiously in the

48 ● Rural Emergency Medical Services
community hospital, and then triaged to the nearesttrauma center (21 ,54). The quality of trauma care inrural hospitals can be improved by promotingphysician and nurse education, instituting a traumaprotocol, promoting prompt resuscitation and stabi-lization of patients before transfer, and implement-ing a quality assurance program, such as a monthlycase review (131 ). Training opportunities tailoredfor rural physicians are available through the Ameri-can College of Surgeons (ACS). A 2-day AdvancedTrauma Life Support (ATLS) course was designedby ACS to meet the needs of rural physicians whomust occasionally stabilize and transfer traumavictims but who do not see major trauma oftenenough to develop expertise in this type of care (20).Since training began in January 1980, about 90,000physicians have been certified. ’ The AmericanCollege of Emergency Physicians offers a 2-dayBasic Trauma Life Support course for basic andadvanced EMTs, nurses, and paramedics, The Emer-gency Nurses Association sponsors the NursingCore Course, and the National Association of EMTssponsors a course in trauma life support for prehos-pital care providers.
When 24-hour physician coverage is unavailablein a rural hospital emergency room, a traumaprotocol can be implemented to help ensure that aphysician and necessary ancillary personnel will beavailable by the time a trauma patient arrives, andthat until the physician arrives, a well-trained nursecan assume immediate resuscitation and stabiliza-tion responsibilities. A rural hospital trauma proto-col may begin with communications between pre-hospital providers at the scene in regard to the natureof the patients injuries and condition. When notified,the nursing supervisor can call members of anestablished trauma team that includes physicians,nurses, a laboratory technician, an X-ray technician,an anesthetist, and possibly a social worker andmedical records clerk. While waiting for the patientto arrive, the nursing supervisor prepares the neededequipment and alerts the air medical service toprepare for a possible transport. Training ruralhospital providers to assume these responsibilitiesand implementing such a protocol avoids confusionand delays. Case reviews help to assure appropriate
rural hospital response and can include physiciansfrom a regional trauma center (55).
Regionalization of Trauma Care
According to guidelines of the American Collegeof Surgeons’ Committee on Trauma:
Each region must structure a trauma system in amanner that ensures the most prompt access toappropriate care and minimizes the risk of delay indiagnosis, delay in surgical intervention, and inade-quately focused care, which are responsible for mostof the preventable deaths from trauma (4).
The guidelines recognize that in rural areas, aninjured patient may be at substantial distances fromlevel I or level II trauma centers (see app. C for ACScriteria for level 1, II, and 111 hospitals) and suggestthat such patients should ideally be treated initiallyat the nearest available hospital facility. It isdesirable that,
. such a facility meet the requirements of a LevelIII trauma center or at least have emergency stafftrained in advanced trauma life support. Patientswith major injuries should then be secondarilytriaged to more distanced Level I or II traumacenters, should local resources prove inadequate forcontinued care (4). *2 An organized regional traumasystem that restricts specialized care to designatedfacilities has been shown to benefit patients withsevere injuries (22).
According to the ACS, ‘‘In the ideal prehospital caresystem there is preplanning, ensuring optimal use ofresources between communities and regions tominimize inefficiency and excessive cost’ (4).Accordingly, among the essential components of atrauma system are the legal authority and a formalprocess to designate trauma centers, use of ACSstandards in designating the trauma centers, use ofpatient volume or population data to ensure that thenumber of centers designated for an area arereasonable, presence of written triage criteria thatform the basis for bypassing nondesignated hospi-tals, use of monitoring systems, and statewidecoverage (133). A 1987 national survey of StateEMS programs indicated that only two States13 have
1 ITh~ ~ourw and ~cnlfic-tion we ~vailab]c (hrough the American Coilege of surgeons. There is no mforrna[ion avai]ablc on how many of the ccr[iticd
physicians arc rural practitioners or the type of physician certified (e.g., family practitioner, emergency physician).
IZRevised ACS standards mat include a Wction on “Optimal Care in the Ruml SCttlng’ are forthcoming.lsThe two States wi~ cornprehensiw trauma systems arc Maryland and Virginia.

trauma systems that include components deemedessential by the ACS Committee on Trauma (133).
At the time of the ACS survey, 2 States met allcriteria, 19 States and the District of Columbia haddesignated trauma centers, but lacked statewidecoverage and/or indicated that triage and qualityassurance programs were inadequate, leaving 29States that had not yet designated trauma centers(see figure 5-l). Somewhat different results werefound in a survey of State EMS directors. Accordingto this survey, also conducted in 1987, 14 Stateswere designating trauma centers and another 22were developing designation programs. An addi-
tional two States had verification programs withStandards. Only 13 States lacked either verificationor designition.14 and 3 of these States had developedstandards (see figure 5-2).
Guidelines for trauma care systems have beendeveloped by a number of professional organiza-tions and by the Joint Committee on the Accredita-tion of Healthcare Organizations (JCAHO). Both the1987 ACS guidelines and those published by theAmerican College of Emergency Physicians (ACEP)take into account some of the unique features of ruralhealth care. According to ACEP guidelines, some
Figure 5-l—States Having All, None, or Some of Eight Essential Components of a Regional Trauma SystemAccording to American College of Surgeons’ Criteria, 1987
n t s
All c o m p o n e n t s
. . . . . . . . . . .. . . . . . . . . .
SOURCE. J.G West et al , “Trauma Systems. Arrest Status—Future Challenges,” J A M A 259(24) 3597-1445, June 24, 1988
14 Dc.lwatloll involves ,dentlfylng a IImllcd number of hospi[als meeting s~Cified ~rl(crla 10 serve tie Lrauma ncedi of [hc SlalC. In COnlraSt,
vcriticalion involves certifying any number of hospitals that mcc[ specified critcrla ( 108).

50 ● Rural Emergency Medical Services
Figure 5-2-State Trauma Center Designation and Verification Practices, 1986-87
I
I
SOURCE: National EMS Clearinghouse, “Emergency Medical Services: Transportation Systems and Available Facilities,” 1988.
features of a trauma care system deemed “essen-tial’ in the urban environment are “desirable” inrural setting (see app. C).15 Universal access through911, for example, is essential in urban systems butdesirable in rural areas. Few States with hospitaltrauma verification or designation programs areusing the ACS or ACEP guidelines. Less thanone-third (9) of the 32 States that reported the typeof standards used in their programs reported usingthe ACS standards, according to the 1987 survey ofState EMS directors. Instead, most had adapted ACS
or ACEP guidelines to meet State or regional needs(108).
Some States have too many designated traumacenters. In Missouri, for example, there are 62designated trauma centers, or 1 per 80,000 residents.This exceeds the recommended ratio of 1 traumacenter per 350,000 residents (133).16 Evidencesuggests that some rural areas underutilize availableresources. In one region in the Southeast, forexample, relatively few life-threatening emergency
IsEleven components (i.e., medical direction, prevention, communication, training, triage, prehospital care, transportation, hospital care,rehabilitation, public education, and medical evaluation) of system management, prehospital care, hospital facilities and rchabditatlon services arcdescribed as essential or desirable in urban and rural settings, ACEP defines an urban systcm as one that encompasses at least one metropolitan area with250,000 persons. Rural systems are lacking any single population center (3).
l~e r~ommend~ ratio is bad on the average annu~ (ra~a rate of one case per 1,~ people and ACS’S recommenda~ion for a minimum of 350
patients per year at a level 11 trauma cam facili[y.

Chapter 5—Emergency Cardiac and Trauma Care in Rural Areas ● 51
cases were being transferred from rural hospitals toadjacent urban specialty hospitals (93).
Many rural hospitals cannot meet the require-ments of an ACS level III hospital, but nonethelesshave an important role to play in providing traumacare in rural areas. Specific trauma care guidelinesfor rural hospitals without level 111 resources mightprove helpful to rural providers. Oregon, for exam-ple, designates a fourth level of trauma care,specifically to meet the needs of rural hospitals, Alevel IV hospital requires an ACLS-trained nurse tobe in-hospital and immediately available, and anACLS and ATLS-trained physician to be on call andpromptly available (e.g., within the hospital, but notnecessarily in the emergency room). (See Oregonhospital criteria in app. D.) The Oregon system tiesthe resources of the urban level I and 11 hospitals to
the level 111 and IV hospitals to improve theirtrauma-related services. Level I and 11 hospitalsmust provide training for rural providers, providefeedback on patients referred to their hospitals by thelevel 111 and IV hospitals, and must provide peerreview of trauma cases as part of a regional qualityassurance program. Furthermore, Level I hospitalsmust provide telephone and onsite consultationswith physicians of the community and outlying areasas part of an outreach program (25). There wouldperhaps be less controversy surrounding triagecriteria if rural hospitals could establish their role inproviding care and formalize beneficial relation-ships with specialty hospitals. The availability ofrapid and aggressive treatment at the local levelbefore and during transport to definitive care willlikely improve rural trauma patient outcomes.

Chapter 6
Federal Policies Toward State Emergency Medical Services
States use many different sources to fund theiremergency medical services (EMS) activities andEMS resources vary dramatically by State. In 1988,over 80 percent of States EMS funds come fromState or local sources (57), Only 14 percent of StateEMS resources derive from Federal sources (figure6-l). This, however, varies markedly by State.Nebraska, for example, relies entirely on Federalsupport while Florida relies entirely on State funds.In 1988, per capita spending for EMS varied from alow of $0.02 per capita in Ohio to nearly $14 percapita in Hawaii (table 6-1) (57).
Federal support of State EMS programs derivesfrom two sources, the Department of Health andHuman Services (DHHS) and the Department ofTransportation (DOT).
DEPARTMENT OF HEALTH ANDHUMAN SERVICES
DHHS support of State EMS comes through thePreventive Health and Health Services Block Grant.EMS was among other categorical health programsthat were folded into the block grant in 1981following passage of the Omnibus Budget Reconcil-iation Act of 1981 (Public Law 97-35). The blockgrant program consolidated a wide range of activi-ties (42 U.S.C. 300w-3(a)(l)):
1, rodent control and fluoridation programs;2. hypertension control;3. health services for defined populations, com-
prehensive programs to deter smoking andalcohol use among children and adolescents,
Figure 6-l-State EMS Program Funding, 1988
State funds:
General State Revenuesand State special funds
(e. g., motor vehicleregistrat ion )
FederalBlo
I
l Funds
Other Federal funds(e. g., Federal Department of Transportation
%ther Federal, other State, or prwateSection 402)
SOURCE: The National EMS Clearinghouse, “The EMS Office, Its Structure and Functions,” The Council of State Governments, Iron Works Pike, Lexington,KY, 1988.
- 5 3 -

54 ● Rural Emergency Medical Services

Chapter 6---Federal Policies Toward State Emergency Medical Services ● 55

56 ● Rural Emergency Medical Services
4.5.
6.
7.
and other risk-reduction and health educationprograms;comprehensive public health services;demonstrating the establishment of homehealth agencies in areas where the services ofsuch agencies were not available;feasibility studies and planning for EMS sys-tems and the establishment, expansion, andimprovement of such systems; andservices to rape victims and for rape preven-tion.2
Under the block grant program, States can allo-cate funds to the seven service areas to suit theirneeds. In 1988, $13 million of block grant fundswere spent on EMS, representing about 15 percent ofall Preventive Health Block Grant funds availablethat year (table 6-2). Some States spend none of theirblock grant funds on EMS (e.g., Alabama, Ken-tucky), while others spend most of their block grantfunds on EMS (e.g., West Virginia, New Mexico)(57) (table 6-2). More than twice as much money,about $30 million per year, had been available forEMS through the Federal EMS categorical grantprogram established following passage of the Emer-gency Medical Services Systems Act of 1973(Public Law 93-154).
The 1973 EMS Systems Act program emphasizedthe development of regional systems to coordinateemergency medical services. Under the program,each of 303 defined EMS regions was eligible toreceive grants for up to 5 years, after which theywere to become self-sustaining (127). Rural areaswere targeted for assistance. At least 20 percent ofappropriations were made available to EMS systemsserving rural areas. Furthermore, special considera-tion was given to applicants from rural areas seekinggrants or contracts to support research in emergencymedical techniques, methods, devices, or delivery.
A State’s share of DHHS Preventive Health andHealth Services Block Grant funding was frozen atits share of categorical grants that the State receivedfor fiscal year 1981, the year legislation was enactedthat combined categorical programs-including EMS
services—into block grants. The block grant alloca-tions to States do not reflect population distribution3
because the categorical grant program had been acompetitive one. Table 6-3 summarizes PreventiveHealth and Health Services Block Grant funding andthe amount of these funds that States choose to spendon EMS since conversion from categorical to blockgrants in 1982, through fiscal year 1988. Since1983, 4 States have allocated between $12 millionand $17 million of block grant funds to EMSactivities (table 6-3).
The impact of the imposition of the block grantprogram on State’s EMS activities was evaluated ina 1986 General Accounting Office (GAO) report.GAO compared overall State EMS expenditures insix States5 for 1981 (the last year of the categoricalEMS Federal program), 1983 (the first year underthe block grant), and 1985 (127). By 1985, totalEMS funding had not returned to 1981 levels butEMS funding was increasing, primarily because ofincreased State funding of EMS activities. By 1985,States were assuming one-half of EMS costs ascompared to 27 percent in 1981 (127).
DEPARTMENT OFTRANSPORTATION
The DOT EMS program began with the HighwaySafety Act of 1966 (Public Law 89-564), which wasenacted following two national studies showingmajor deficiencies in EMS services (70,81). Underthe Act, DOT funds States to develop highwaysafety programs that include provisions for emer-gency services. DOT funding must be linked to itshighway responsibilities. DOT’s emphasis is there-fore on the prehospital stage and the initial stages ofhospital care for highway-injured patients, as well ason prevention and intervention activities that arehighway-related (53 FR 11255). The State andCommunity Highway Safety Grant Program isreferred to as the section 402 program. State fundingunder section 402 is apportioned among the Statesbased on a State’s population and public roadmileage. 6 In 1987, nearly $5 million were available
11984 legislation subsequently added grants for demonstration projects for the treatment of children for trauma or critical care (Publlc Law 98-555).zReplaced in 1986 by **victims of =x Offen=s and for PreventIon of sex offenses” (public Law 99-646 and Public Law 99-654).
sAn exception to ~is are block grants funds earmarked for the ‘‘sex offenses’ category, which are allocated according to population (53 FR 27766).‘41982 was a Uansition year from the categorical program to the block grant pmgrm.5The sjx States ~al GAO studicxj were California, Florida, Iowa, Massachusetts, Pennsylvania, and Texas.6Seventy.five ~.ent of funds UC allocated based on population and 25 percent are b~~~ on tie pub]ic road mileage. A portion of funds is ah
resewed for Indian tribes (23 U.S.C. 402(c)).

Chapter 6---Federal Policies Toward State Emergency Medical Services . 57
.
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
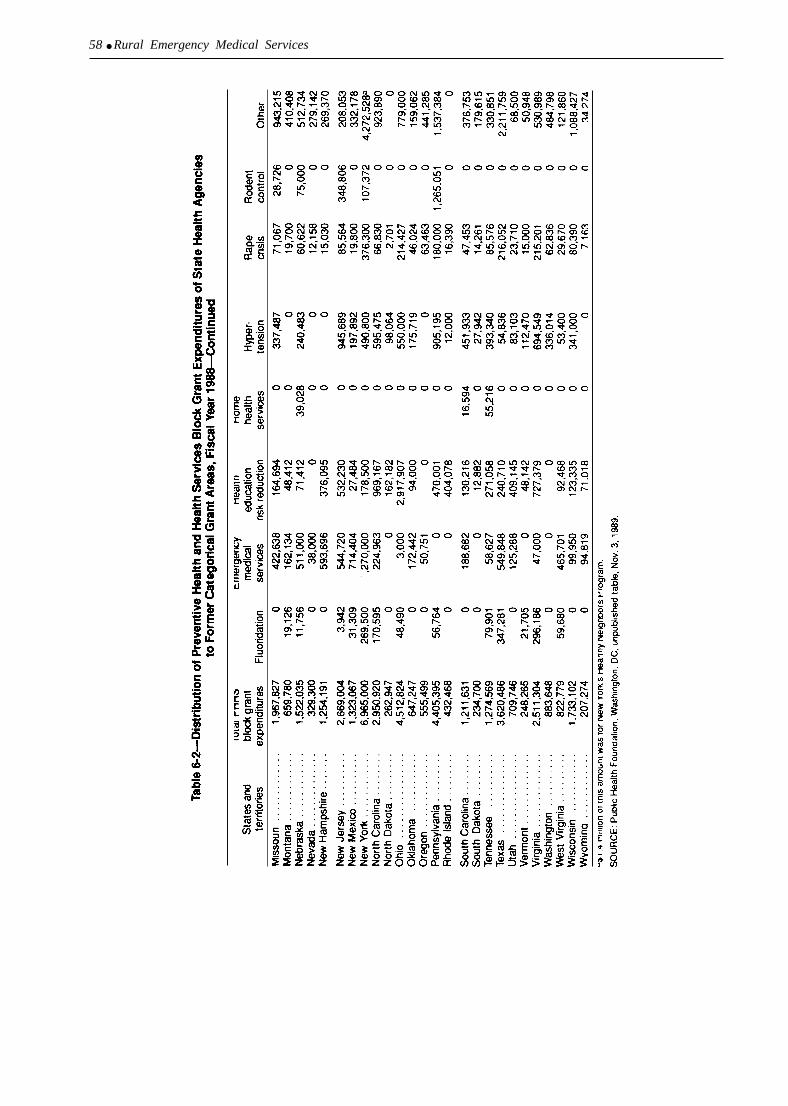
58 ● Rural Emergency Medical Services
-

Chapter 6---Federal Policies Toward State Emergency Medical Services ● 59
Table 6-3-Preventive Health and Health ServicesBlock Grant Expenditures: Emergency Medical
Services, Fiscal Years 1982-88
BlockFiscal year grant total
1982 . . . . . . $32,1 74,000a
1983 . . . . . . . 85,746,0001984 . . . . . . . 81,822,0001985 . . . . . . 86,564,0001986 . . . . . 88,701,0001987 . . . . . . . 84,129,0001988 . . . . . . . 87.966.000
EMSexpenditures
$ 4,776,00017,612,00015,132,00016,216,00016,407,00012,929,00013.175.000
Percentagespent on EMS
14.820.518.518.718.515.415.0
a Block grant totals are low in 1982 because this was a transitional year.
SOURCE: Public Health Foundation, 1220 L St , N W, Washington, DC20005, NOV. 3, 1989
to States through the 402 program (table 6-4). Thisrepresents about one-fifth of Federal EMS resourcesand about 3 percent of all EMS expenditures (i.e.,State and Federal) (figure 6-1 ).
DOT also has research, development, and demon-stration funds to support State or local agencies inthe areas of highway-safety personnel training andresearch, accident investigation procedures, andemergency service plans (referred to as the Section403 program). In 1988, DOT allocated just over700,000 through the section 403 research anddemonstration program.
Section 402 Funds for State HighwaySafety Plans
DOT has determined that the following sevenprograms have been the most effective in reducingaccidents, injuries, and fatalities, and DOT supportsinclusion of countermeasures in these areas intoState’s Highway Safety Programs (53 FR 11255):7
1. Alcohol and Other Drug Countermeasures.2. Police Traffic Services.3. Occupant Protection.4. Traffic Records.5. Emergency Medical Services.6. Motorcycle Safety.7. Roadway Safety.
DOT has guidelines for State Highway SafetyPrograms and to receive funds, a State must have itshighway safety program approved by DOT. Theguidelines related to EMS are as follows (23 CFR204.4):
Each State, in cooperation with its local politicalsubdivisions, should have a program to ensure that
Table 6-4-National Highway Traffic SafetyAdministration’s State and Community Highway
Safety Program (Section 402) Funding:Emergency Medical Services,
Fiscal Years 1967-87
NHTSA EMS PercentageFiscal year sec. 402 total sec. 402 total spent on EMS
1967-76 ... .$639,157,7001977 . . . . . . 125,700,1001978 . . . . . . 168,699,6001979 . . . . . . . 167,096,0001980 . . . . . . 190,243,0001981 . . . . . . 169,991,900
1982 . . . . . . . 92,582,3001983 . . . . . . . 91,845,2001984 . . . . . . . 95,077,8001985 . . . . . . 120,619,0001986 . . . . . . 116,827,5001987, . . . . . . 111,539.200
$89,074,30016,996,50022,686,90013,535,50018,771,90012,721,900
5,438,8004,964,8004,466,8005,332,6005,315,2004,708.900
13.913.513.4
8.19.97.5
5.95.44.74,44.64,2
SOURCE: Traffic Safety Program, National Highway Traffic Safety Admin-istration, U.S. Department of Transportation, “FY 1987 Sum-mary of State and Community Highway Safety Obligations(Section 402),” Nov. 13, 1987.
persons involved in highway accidents receiveprompt emergency medical care under the range ofemergency conditions encountered. The programshould provide, as a minimum. that:
1.
2.
3.
4.
5.
6.
7.
8.
There are training, licensing, and related re-quirements (as appropriate) for ambulance andrescue vehicle operators, attendants, drivers, anddispatchers.There are requirements for types and number ofemergency vehicles including supplies and equip-ment to be carried.There are requirements for the operation andcoordination of ambulances and other emergencycare systems.There are first aid training programs and refreshercourses for emergency service personnel, and thegeneral public is encouraged to take first aidcourses.There are criteria for the use of two-way communi-cations.There are procedures for summoning and dispatch-ing aid.There is an up-to-date, comprehensive plan foremergency medical services, including:a. Facilities and equipment.b. Definition of areas of responsibilities.c. Communications systems.This program should be periodically evaluatedby the State and the National Highway TrafficSafety Administration should be provided withan evaluation summary.
70~er ~ca$ may & funded, but only If thc S[alc can provldc a specific ra[lonalc and convincing informauon that this ls a special needs area
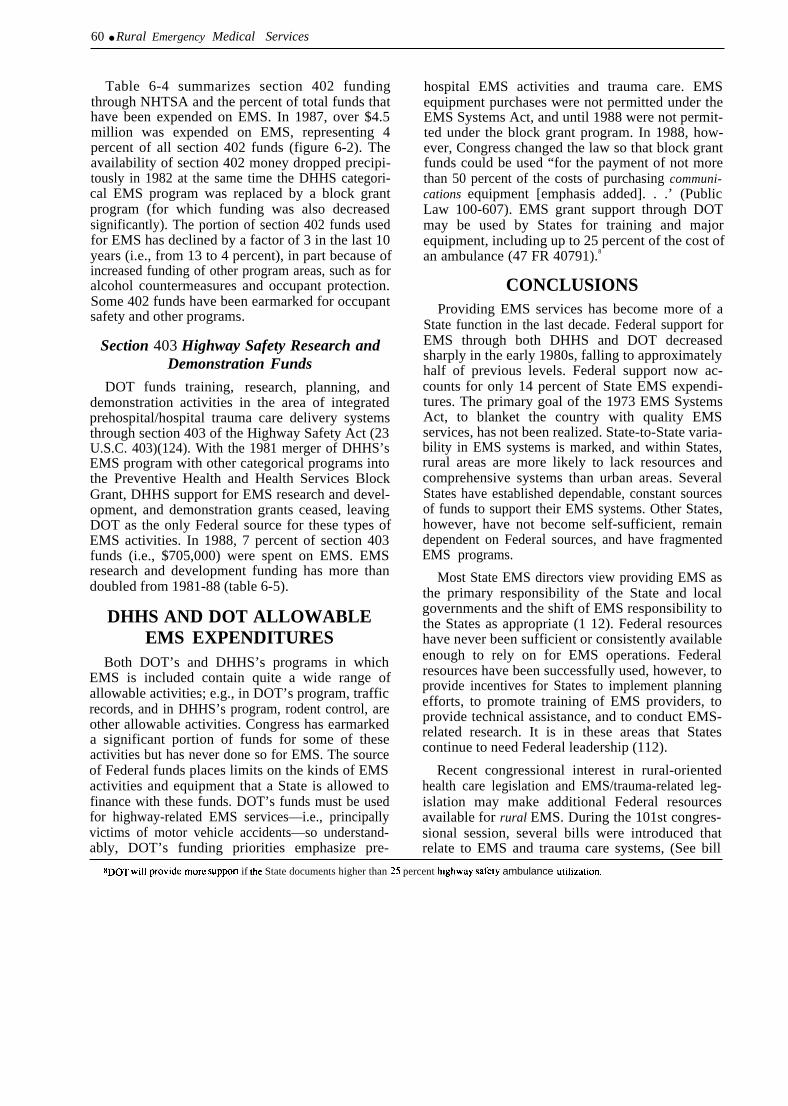
60 ● Rural Emergency Medical Services
Table 6-4 summarizes section 402 fundingthrough NHTSA and the percent of total funds thathave been expended on EMS. In 1987, over $4.5million was expended on EMS, representing 4percent of all section 402 funds (figure 6-2). Theavailability of section 402 money dropped precipi-tously in 1982 at the same time the DHHS categori-cal EMS program was replaced by a block grantprogram (for which funding was also decreasedsignificantly). The portion of section 402 funds usedfor EMS has declined by a factor of 3 in the last 10years (i.e., from 13 to 4 percent), in part because ofincreased funding of other program areas, such as foralcohol countermeasures and occupant protection.Some 402 funds have been earmarked for occupantsafety and other programs.
Section 403 Highway Safety Research andDemonstration Funds
DOT funds training, research, planning, anddemonstration activities in the area of integratedprehospital/hospital trauma care delivery systemsthrough section 403 of the Highway Safety Act (23U.S.C. 403)(124). With the 1981 merger of DHHS’sEMS program with other categorical programs intothe Preventive Health and Health Services BlockGrant, DHHS support for EMS research and devel-opment, and demonstration grants ceased, leavingDOT as the only Federal source for these types ofEMS activities. In 1988, 7 percent of section 403funds (i.e., $705,000) were spent on EMS. EMSresearch and development funding has more thandoubled from 1981-88 (table 6-5).
DHHS AND DOT ALLOWABLEEMS EXPENDITURES
Both DOT’s and DHHS’s programs in whichEMS is included contain quite a wide range ofallowable activities; e.g., in DOT’s program, trafficrecords, and in DHHS’s program, rodent control, areother allowable activities. Congress has earmarkeda significant portion of funds for some of theseactivities but has never done so for EMS. The sourceof Federal funds places limits on the kinds of EMSactivities and equipment that a State is allowed tofinance with these funds. DOT’s funds must be usedfor highway-related EMS services—i.e., principallyvictims of motor vehicle accidents—so understand-ably, DOT’s funding priorities emphasize pre-
hospital EMS activities and trauma care. EMSequipment purchases were not permitted under theEMS Systems Act, and until 1988 were not permit-ted under the block grant program. In 1988, how-ever, Congress changed the law so that block grantfunds could be used “for the payment of not morethan 50 percent of the costs of purchasing communi-cations equipment [emphasis added]. . .’ (PublicLaw 100-607). EMS grant support through DOTmay be used by States for training and majorequipment, including up to 25 percent of the cost ofan ambulance (47 FR 40791).8
CONCLUSIONSProviding EMS services has become more of a
State function in the last decade. Federal support forEMS through both DHHS and DOT decreasedsharply in the early 1980s, falling to approximatelyhalf of previous levels. Federal support now ac-counts for only 14 percent of State EMS expendi-tures. The primary goal of the 1973 EMS SystemsAct, to blanket the country with quality EMSservices, has not been realized. State-to-State varia-bility in EMS systems is marked, and within States,rural areas are more likely to lack resources andcomprehensive systems than urban areas. SeveralStates have established dependable, constant sourcesof funds to support their EMS systems. Other States,however, have not become self-sufficient, remaindependent on Federal sources, and have fragmentedEMS programs.
Most State EMS directors view providing EMS asthe primary responsibility of the State and localgovernments and the shift of EMS responsibility tothe States as appropriate (1 12). Federal resourceshave never been sufficient or consistently availableenough to rely on for EMS operations. Federalresources have been successfully used, however, toprovide incentives for States to implement planningefforts, to promote training of EMS providers, toprovide technical assistance, and to conduct EMS-related research. It is in these areas that Statescontinue to need Federal leadership (112).
Recent congressional interest in rural-orientedhealth care legislation and EMS/trauma-related leg-islation may make additional Federal resourcesavailable for rural EMS. During the 101st congres-sional session, several bills were introduced thatrelate to EMS and trauma care systems, (See bill
8DOT Wil] provide more SUppOrI if tie State documents higher than 25 percent highway safely ambulance utilization.
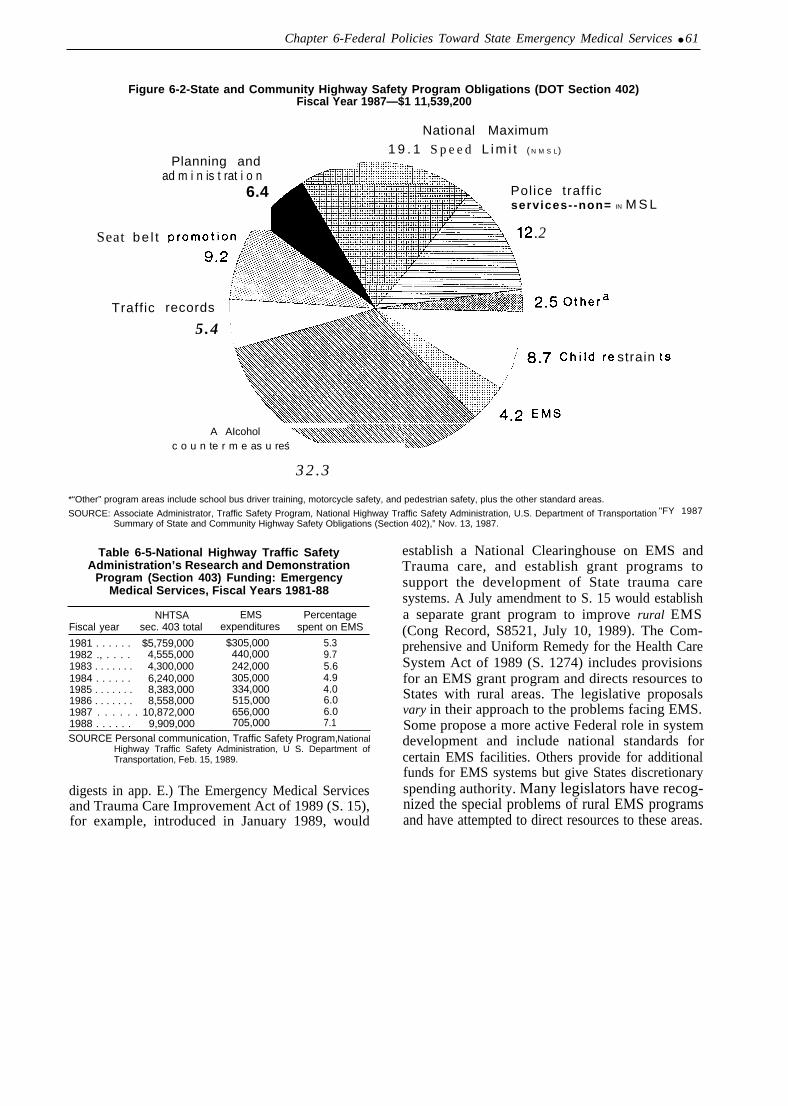
Chapter 6-Federal Policies Toward State Emergency Medical Services ● 61
Figure 6-2-State and Community Highway Safety Program Obligations (DOT Section 402)Fiscal Year 1987—$1 11,539,200
Seat be l t
Traff ic
National Maximum
Planning and1 9 . 1 S p e e d L i m i t ( N M S L)
ad m i n is t rat i o n6.4
records
5.4
Police traff icservices--non=
.2
32.3
/
A AIcoholc o u n te r m e as u res
IN M S L
strain
*“Other” program areas include school bus driver training, motorcycle safety, and pedestrian safety, plus the other standard areas.
SOURCE: Associate Administrator, Traffic Safety Program, National Highway Traffic Safety Administration, U.S. Department of TransportationSummary of State and Community Highway Safety Obligations (Section 402),” Nov. 13, 1987.
Table 6-5-National Highway Traffic SafetyAdministration’s Research and Demonstration
Program (Section 403) Funding: EmergencyMedical Services, Fiscal Years 1981-88
NHTSA EMS PercentageFiscal year sec. 403 total expenditures spent on EMS
1981 . . . . . . $5,759,000 $305,000 5.31982 ., . . . . 4,555,000 440,000 9.71983 . . . . . . . 4,300,000 242,000 5.61984 . . . . . . 6,240,000 305,000 4.91985 . . . . . . . 8,383,000 334,000 4.01986 . . . . . . . 8,558,000 515,000 6.01987 . . . . . . 10,872,000 656,000 6.01988 . . . . . . 9,909,000 705,000 7.1
SOURCE Personal communication, Traffic Safety Program, NationalHighway Traffic Safety Administration, U S. Department ofTransportation, Feb. 15, 1989.
digests in app. E.) The Emergency Medical Servicesand Trauma Care Improvement Act of 1989 (S. 15),for example, introduced in January 1989, would
"FY 1987
establish a National Clearinghouse on EMS andTrauma care, and establish grant programs tosupport the development of State trauma caresystems. A July amendment to S. 15 would establisha separate grant program to improve rural EMS(Cong Record, S8521, July 10, 1989). The Com-prehensive and Uniform Remedy for the Health CareSystem Act of 1989 (S. 1274) includes provisionsfor an EMS grant program and directs resources toStates with rural areas. The legislative proposalsvary in their approach to the problems facing EMS.Some propose a more active Federal role in systemdevelopment and include national standards forcertain EMS facilities. Others provide for additionalfunds for EMS systems but give States discretionaryspending authority. Many legislators have recog-nized the special problems of rural EMS programsand have attempted to direct resources to these areas.

Appendix A
Rural EMS Workshop Participants
Workshop held May 4 and 5, 1989. Cosponsored by: The Department of Transportation, National Highway TrafficSafety Administration and The Office of Technology Assessment
John C. AndersonCle Elum Family Medicine CenterCle Elum, Washington
Paul AndersonChiefBureau of Emergency Medical
ServicesBoise, Idaho
Stuart BrownDirectorDivision of Injury Epidemiology and
ControlCenter for Disease ControlAtlanta, Georgia
Jonathan ChinGraduate ProgramDepartment of Emergency Health
ServicesUniversity of MarylandBaltimore County, Maryland
Terry DimonNurse ManagerEmergency DepartmentMemorial Hospital of Laramie CountyCheyenne, Wyoming
Mary EllisDirectorIowa Department of Public HealthLucas State Office BuildingDes Moines, Iowa
John JohnsonDirectorEmergency Medical ServicesPorter Memorial HospitalValparaiso, Indiana
Ellen MacKenzieAssociate DirectorCenter for Health Services ResearchJohns Hopkins UniversityBaltimore, Maryland
Kim MaullProfessor & ChairDepartment of SurgeryUniversity of Tennessee Medical
CollegeKnoxville, Tennessee
Maureen McArdleTrauma CoordinatorEmergency Medical ServicesSan Diego, California
Susan McHenryDirectorDivision of Emergency ServicesVirginia Department of HealthRichmond, Virginia
William R. MetcalfDirectorEmergency Medical ServicesColorado Department of HealthDenver, Colorado
Stu ReynoldsNorthern Montana Surgical
AssociatesHavre, Montana
Don StamperManagerEmergency ServicesStaff for LifeUniversity of Missouri
Columbia, Missouri
Robert F. TredwellConsultantBrooksville, Maine
Carl Van CottCommunications DirectorOffice of Emergency Medical
ServicesState of North CarolinaRaleigh, North Carolina
Harvey WolfeChairmanIndustrial Engineering DepartmentSchool of EngineeringUniversity of PittsburghPittsburgh, Pennsylvania
Barak WolffBureau ChiefBureau of Primary Care/EMSSante Fe, New Mexico
Richard ZuschlagPresidentAcadian Ambulance Service, Inc.Lafayette, Louisiana
-63-

.
Appendix B
Designing an Appropriate EMS System in Rural Areas:Use of a Computer Simulation Model
A computer simulation model (called RURALSIM)has been designed to allow planners to examine how theirpresent emergency medical services (EMS) system func-tions and to determine the effects introducing changesinto their systems. 1 The model also allows planners to setgoals for long-term system improvements and to deter-mine if the goals can be met with available resources.RURALSIM was intended to help local decisionmakersallocate scarce EMS funds efficiently and to addressspecific questions such as:
●
●
●
●
Are an appropriate number of emergency responsevehicles in the area?Are they appropriately located within the region?Are the personnel on these vehicles trained at theappropriate level to serve the population in the area’?Are helicopters and fixed-wing aircraft required aspart of the system and where should they be located?
In this section, the computer simulation model isdescribed as are its attempted implementation in severalrural areas.2
The Computer Simulation ModelRURALSIM analyzes the effects of changes in the
EMS system in terms of a number of performancemeasures such as response time, level of response, andvehicle utilization. The model uses local EMS demandand response data to generate predicted occurrence andresponses at various times of day for a given area. Theplanner can hold the area’s demand for EMS servicesconstant and then alter the configuration of systemresources, The effects of introducing changes such asvehicle placement and relocation strategies, vehicledispatching policies and alternative forms of prehospitalcare can then be evaluated. EMS planners can useRURALSIM to evaluate the cost of alternative EMSconfigurations that achieve the desired goals, can modifythe system’s goals relative to cost constraints, andmaximize system effectiveness given a particular costbase.
RURALSIM can take into account several differentattributes of the region under study. These can be dividedinto five categories:
1. technological configurations of an EMS systemincluding access, communications, vehicle andresource deployment, field treatment, transporta-tion, and definitive treatment facilities;
2.
3.
4.
5.
different placement strategies for response andtransport vehicles including first responders, BasicLife Support and Advanced Life Support providers,and the availability of rescue land and air vehicles;characteristics of the region’s environment includ-ing populations and the affect of particular popula-tion attributes, geography, roads, and weatherconditions upon EMS demands, and responsecapabilities;policies and operating rules for the different EMSsystem components including dispatch policies;vehicle re-allocation, transport. and first responderpolicies; and hospital designation policies, whichaffect patient transport; andchanges in demand patterns caused by populationfluctuations and/or seasonal population shifts.
The model defines demand as a request for eitheremergency field treatment or routine transportation serv-ices. Within these two categories, demand is furthersubdivided according to type of case and severity level.Emergent case types may include: cardiac, trauma (non-motor vehicle related), and motor vehicle accident, andnon-trauma/non-cardiac. Special categories of incidents(e.g., basic manufacturing, mining, river) can also beincluded. For each type of emergent incident, three levelsof presenting severity are typically defined: life threaten-ing, severe, and minor/moderate. In addition to classi-fying demand by type and severity. RURALSIM alsoallows for variation in the demand rates by time of day andday of week.
RURALSIM must not only generate the emergencyincident according to type, severity, and time, but mustalso determine its location. In order to do this, a networkmodel is used to represent the region’s transportationsystem. The area’s primary roads, important secondaryroads, intersections, and population clusters are modeled.
Once an incident has been generated, the accesscomponent models the process which occurs between thetime of the incident and the time when initial contact ismade with the EMS system. The events which occur inthis period include incident detection, possible aidrendered by a citizen, and EMS system access utilizingpublic telephone, radio, call box, or direct contact. Giventhe complexity of the access problem and the unavailabil-ity of representative data, this process is modeled in termsof the probability that an incident is witnessed, the timefor discovery of unwitnessed incidents and the time to
I The de~elopm~[ of tie Cmputer slmu]a[lon model occur-red from 1979 to the mid- 1980s by researchers al the Unlvcrs]ty of Piusburgh, Health Operalwns ResearchGroup WIIJ supp~ from tie U.S. Dcpu[rnen[ of Transporta[wn (Shuman and Wolfe, 1989).
2fJour ~ra] sl[es wme used IO &velop R1.JRAL.SIM: 1 ) Amostoock. Penobsco[, Plscataqus, Waldo, Hancock, and Washington Courmes m Maine; 2) Camden, Mdler,and Morgan Coun[Ies (Lake of the Ozarks) m Mlssoun; 3) Craig, Delaware, Mayes, Muskogee, and Okmulgee Courmes m Oklahoma; and 4) Indiana Coun[y mPennsylvarua.
- 6 4 -

Appendix B--Designing an Appropriate EMS System in Rural Areas: Use of a Computer Simulation Model ● 65
contact the EMS system. These access probabilities andparameters must typically be estimated by EMS plannerssince little data are available. They may be varied indifferent simulation experiments in order to assess theireffects.
Three types of communication functions are consid-ered in RURALSIM: the initial request for assistance toactivate (access) the EMS system: communications be-tween the EMS dispatch center and the ambulance vehiclebase station; and communications between the EMSdispatch center and a responding vehicle away from thebase for the purpose of directing or redirecting the vehicleto or from an incident scene and for the purpose ofrelaying medical information and receiving medicalcommand. The system access is assumed to be viatelephone and is modeled as a time delay. Randomlygenerated time delays are also introduced depending onthe type of dispatch facility available (e.g., with or without911), and the means of communication with the basestations. Communications between the dispatch center (ormedical command) and a vehicle away from base are notexplicitly modeled (e.g., number of radio channels, etc. )but are assumed to be available for the purpose ofredirecting or calling off a vehicle.
The EMS system response function is concerned withambulance vehicle dispatch, prehospital treatment, andpatient transport. As input to the model, each ambulancevehicle must be specified according to its type (BLS,ALS, Rescue, or First Responder), base station, crewavailability, level of crew training, and shifts in service.
The heart of RURALSIM is its ‘ ‘dispatcher”’ module,A series of decision rules has been programmed intoRURALSIM to replicate the manner in which thesimulated region’s dispatchers would function. Thedispatcher must assign the different types of vehicles inaccord with the perceived severity of the incoming call. Ifprimary and secondary vehicles are not available,RURALSIM can search for the closest available vehicle,reassign a vehicle, or queue the patient until an appropri-ate vehicle becomes free.
Time spent at the scene is determined by the type andseverity of the incident, and the highest level of capabilityof the responding vehicles (BLS or ALS). Two variablesare involved in the field transportation function-thedecision to transport and the choice of destination.Patients may not be transported if their condition does notwarrant it, or if transportation is refused. Destination foremergency patients is typically a hospital within theregion or an adjoining area. Location, type and severity ofthe incident typically determine the receiving institution,Patients picked up at a hospital may be transported toanother hospital, an extended care facility, or the patientresidence.
The internal workings of the definitive care treatmentfacilities (hospitals) in the region are explicitly excludedfrom the model since little is to be gained by theirinclusion and their introduction would furthcr complicatethe model. Hospitals are modeled primarily as destina-tions for the transportation of patients.
RURALSIM collects relevant information on eachsimulated patient which describes the incident type andlocation. response times, and the resolution of the case.Output information on each patient includes: incidenttype, seventy level, location, time of incicient, timedispatch contacted, time each responding vehicle con-tacted, time each vehicle left its respective base orlocation, time each vehicle arrived at the scene, timepatient transported (or left scene), time patient arrived atreceiving facility, and time each vehicle was back inservice. From these profiles, response times, delay times.and total EMS service times can be determined for eachincident.
A number of measures of effectiveness are utilized tofacilitate the comparison of alternative configurations andpolicies. These include average BLS and ALS responsetimes, time first vehicle arrives at scene, percent ofpatients serviced (vehicle at scene) within 4 minutes ofcontacting the dispatcher, percent of patients serviced inmore than 10 minutes, the average time for eachcomponent of the incident (access, dispatch, response,field treatment, and transport), and vehicle utilization.Other measures such as the number of times a vehicle isunavailable for emergent requests and average patientwaits can be included.
A number of EMS options for improving an area’sEMS system can be evaluated by RURALSIM. Themodel allows planners to develop innovative strategies touse available resources to reduce the response time forcritically injured patients and thus improve the caredelivered at the scene.
Options to improve EMS access that can be consideredin the modeling exercise include using more efficientcommunications systems, improving response (by ena-bling care to be delivered to the scene with an acceptableresponse level), improving transportation, improvingskill maintenance of prehospital providers and improvingthe hospital or clinic response capability. In a rural areathe options must be chosen with respect to availableservices and individuals; the size and distribution ofpopulation clusters; and the social, cultural, economic,political, and geographic constraints and incentives char-acteristic of the specific community.
Three major groups of options are available to acommunity:
. those that facilitate the development of a new ruralEMS system;

—
66 ● Rural Emergency Medical Services
Ž those that provide linkages for small populationclusters and;
Ž those that offer solutions to specific problems in anexisting rural EMS system.
The first option group is, in reality, a process forbuilding an EMS system from scratch. The simulator canhelp develop a set of steps for building an effective EMSsystem in a rural area. The second option group pertainsto those communities that already have some form ofEMS, but do not appear to have the resources required toachieve a desired level of service, These options includean evaluation of various configurations of communitiescooperating with each other in order to provide a moreeffective system. Finally, there are options which aredirected at specific problems facing a functional EMSsystem (e. g., communication systems). For any specificEMS area, options from any or all three groups might beimportant to evaluate through simulation.
During field testing of the model in several rural areas,numerous shortcomings of the simulation model werenoted. These shortcomings included:
● it required data that was not available in rural areas;● it was so complex, it required reconfiguration before
it could be used in different rural environments;. results from simulations were not available in time
for local planners to use the information; and. a rational EMS system as specified by the model was
not implemented because there were limited plan-ning resources within the region and because ofvarious social and political constraints.
Example: Aroostoock County, Maine
The population of Aroostoock County, Maine wasapproximately 100,000 at the time of the field test. Thepopulation was scattered among 71 towns (most with apopulation under 1,000) most of which were spread overa 7,500-square-mile land area. At the time of the study, thecounty was served, somewhat sporadically. by 12 inde-pendent BLS ambulance providers. The development ofa countywide system and/or the introduction of ALScapabilities was being considered.
The impact of several EMS system changes wereevaluated including:
●
●
●
using an ALS non-transporting unit which operatedout of the region’s hospitals and from some of itsmore rural clinics;downgrading several very low volume BLS units toIRP status; other BLS units were redeployed toprovide both first response and transportation inconjunction with an ALS (non-transporting) unit;a transport vehicle unit was created to provideinterfacility transportation from the rural hospitals to
the State’s tertiary and secondary care facilities (atrip of up to 4 hours or more in some cases).
The results of this seemingly ideal and cost-effectivealternative were for the most part very promising:Average response times for a number of areas would bereduced by up to 2 minutes. However. even though thenumber of BLS vehicles deployed was reduced while anALS capability was introduced, the rural nature of the areawas not conducive to an acceptable ALS response timesthat remained relatively high (12.5 to 14.0 minutes).Further, the long-haul transfer vehicles were not utilizedwith the anticipated frequency, and hence, did not lead tosignificant system improvement.
While RURALSIM provided planners with a consider-able amount of information, much of its potential valuewas not realized, in part because there were delays due todata limitations and because RURALSIM needed to bereconfigured. Primary reasons for selecting Maine as thefirst test site were its computerized EMS data system, theonly such statewide system in existence at that time. andthe sophisticated staff. However, in a number of cases, thedata requirements of RURALSIM exceeded the capabili-ties of Maine’s system necessitating either manualcompilation or the development of alternative methods toestimate demand. Neither the local providers, nor thelocal communities were willing to accept a more efficientand effective EMS delivery system if it meant giving upa certain amount of local autonomy and independence.
The Future of RURALSIM:Microcomputer Adaptation
RURALSIM can’t be used directly by most rural EMSplanners because it requires a mainframe computer. Thecosts associated with modeling also limit its use. Themodel is so complex that a single simulation could costseveral hundred dollars. Since RURALSIM’s develop-ment, rapid advancements in personal computers haveoccurred and RURALSIM’s could be adapted to themicrocomputer. Adapting the computer model to amicrocomputer would allow rural areas with microcom-puters to conduct their own simulations and work with thesystem interactively.
A microcomputer version could be simplified and usedfor the training/education of rural EMS planners andadministrators. A number of different rural EMS scenar-ios could be developed which the ‘‘planner’ could use totest-out possible alternative EMS improvements. Themicrocomputer-based model could also serve as a techni-cal planning tool that could be incorporated into atechnical assistance program.

Appendix C
Trauma Service Designation Guidelines of theAmerican College of Surgeons and the
American College of Emerging Physicians
Hospital and Prehospital Resources forOptimal Care of the Injured Patient by the
Committee on Trauma of the AmericanCollege of Surgeons
This report was prepared by the Task Force of theCommittee on Trauma of the American College ofSurgeons (ACS). In June of 1986, the Board of regents ofthe American College of Surgeons approved this reportand authorized its publication as an official Collegedocument.
It is generally recognized that this document is a set ofguidelines representing current thinking for optimal careof the injured. Further revisions may be indicated assystems are developed to meet the complex demands ofseverely injured patients.
Levels of Care
The three levels of care suggested in this documentrepresent the best possible use of community resources.The organization of trauma services within the commu-nity or region must address the development of a goodprehospital system. The concept of taking the severelyinjured patient to the nearest hospital is no longeracceptable.
Levels I and II—Invariably, in planning for regionaltrauma needs, physicians, administrators, and healthplanners must address how many hospitals should bedesignated. Factors that must be considered includemaintenance of skills and experience, costs, populationdensity, and geography. The following guidelines areoffered to assist in this planning. General surgeons inLevel I centers might be considered to have adequateexperience in trauma surgery if they treat approximately50 severe and urgent injury cases per year. Based on the
number of surgeons in each institution, this will translateinto 600 to 1,000 patients treated in a Level I hospital, and350 to 600 patients treated in a Level II hospital. Sinceeach community must decide on the number of appropri-ate trauma facilities necessary to meet its commitment toexcellence in trauma care, it must consider the number ofsevere and urgent injuries to be handled as well as itsability to address its factors of geography and its abilityto concentrate its resources.
Level III—The Level II hospital generally servescommunities that do not have all the resources usuallyassociated with Level I or II institutions. However, as thefollowing tables show, a Level III hospital reflects amaximum commitment to trauma care (commensurate withresources. Planning for care of the injured in smallcommunities or suburban settings usually calls fortransfer agreements and protocols for the most severelyinjured. Designation of the Level III hospital may alsorequire innovate use of the region resources. Forexample, if there is no neurosurgeon in a large, sparselypopulated region it may require that a general surgeon beprepared to provide the emergency decompression ofmass lesions. Transfer to the most appropriate Level I orII hospital can then be arranged after the patient’s lifesaving operation has been carried out. Another exampleis the staffing of the Level III hospital. In many instancesit will be impractical to require a general surgeon to bein-house. With modern communication systems it seemsreasonable that the surgeon should be promptly availableand in a great majority of instance meet the patient in theemergency room on arrival. On-call personnel such aslaboratory, x-ray, and operating room nurses also can beactivated and respond promptly to the hospital when thefirst notification of a critically injured patient is received.The intent of this flexibility should be clear: to provide thebest possible care even in the most remove circumstances.
-67-
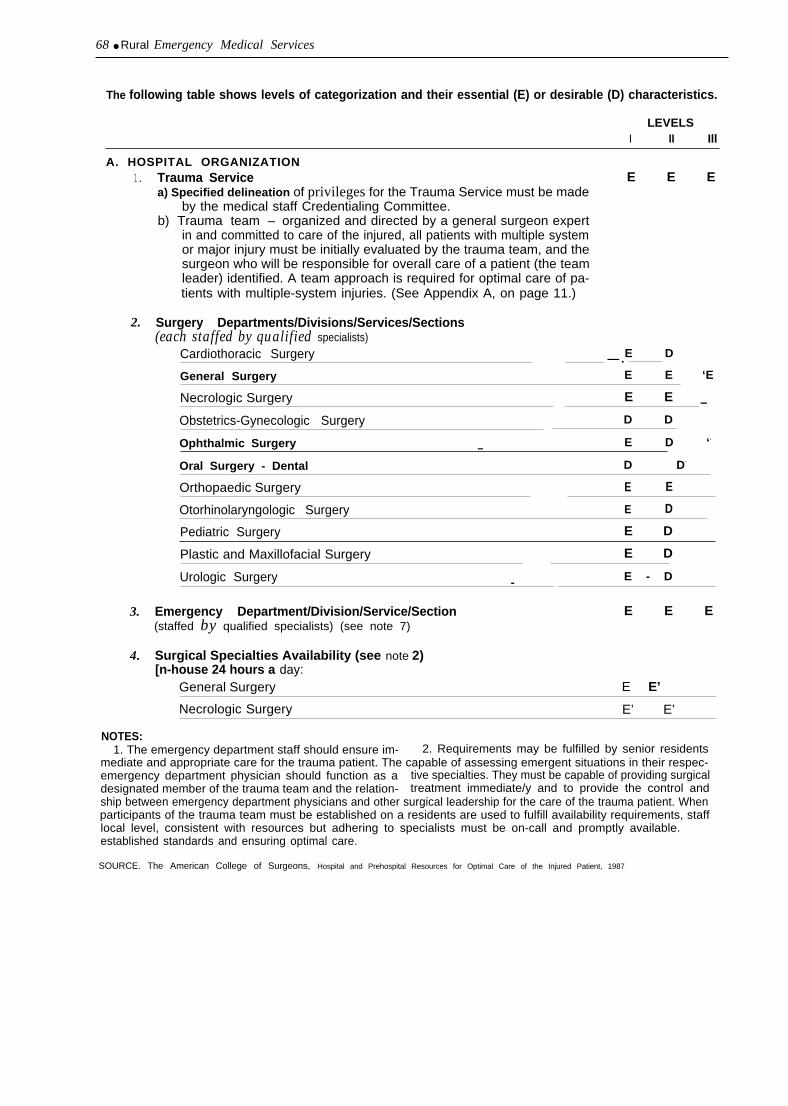
68 ● Rural Emergency Medical Services
The following table shows levels of categorization and their essential (E) or desirable (D) characteristics.
LEVELSI II Ill
A. HOSPITAL ORGANIZATION1.
2.
Trauma Service E E Ea) Specified delineation of privileges for the Trauma Service must be made
by the medical staff Credentialing Committee.b) Trauma team – organized and directed by a general surgeon expert
in and committed to care of the injured, all patients with multiple systemor major injury must be initially evaluated by the trauma team, and thesurgeon who will be responsible for overall care of a patient (the teamleader) identified. A team approach is required for optimal care of pa-tients with multiple-system injuries. (See Appendix A, on page 11.)
Surgery Departments/Divisions/Services/Sections(each staffed by qualified specialists)
Cardiothoracic Surgery E D— .General Surgery E E ‘E
3.
4.
Necrologic Surgery E E —Obstetrics-Gynecologic Surgery D D
Ophthalmic Surgery E D ‘-
—
Oral Surgery - Dental D D-
Orthopaedic Surgery
Otorhinolaryngologic Surgery
E
E
E
D
Pediatric Surgery E D
Plastic and Maxillofacial Surgery E D
Urologic Surgery E - D-
Emergency Department/Division/Service/Section E E E(staffed by qualified specialists) (see note 7)
Surgical Specialties Availability (see note 2)[n-house 24 hours a day:
General Surgery E E’
Necrologic Surgery E’ E’
NOTES:1. The emergency department staff should ensure im- 2. Requirements may be fulfilled by senior residents
mediate and appropriate care for the trauma patient. The capable of assessing emergent situations in their respec-emergency department physician should function as a tive specialties. They must be capable of providing surgicaldesignated member of the trauma team and the relation- treatment immediate/y and to provide the control andship between emergency department physicians and other surgical leadership for the care of the trauma patient. Whenparticipants of the trauma team must be established on a residents are used to fulfill availability requirements, stafflocal level, consistent with resources but adhering to specialists must be on-call and promptly available.established standards and ensuring optimal care.
SOURCE. The American College of Surgeons, Hospital and Prehospital Resources for Optimal Care of the Injured Patient, 1987

Appendix C—Trauma Service Designation Guidelines of ACS and ACEP ● 69
SURGICAL SPECIALTIES continuedLEVELS
I II Ill
On-call and promptly available from inside or outside hospital:Cardiac Surgery E D
General Surgery E
Necrologic Surgery D
Microsurgery Capabilities E D
Gynecologic Surgery E D
Hand Surgery E D
Ophthalmic Surgery E E D
Oral Surgery (dental) E D
Orthopedic Surgery E E D
Otorhinolaryngologic Surgery E E D
Pediatric Surgery E D
Plastic and Maxillofacial Surgery E E D
Thoracic Surgery E E D
Urologic Surgery E E D
5. Non-Surgical Specialties AvailabilityIn-hospital 24 hours a day:
Emergency Medicine E5 E’ E
Anesthesiology E’ E6,7 E’
On-call and promptly available from inside or outside hospital:Cardiology E E D
NOTES:3. The established trauma system should ideally ensure
that the trauma surgeon will be present in the emergencydepartment at the time of the patient’s arrival. When suffi-cient prior notification has not been possible, a designatedmember of the trauma team will immediately initiate theevaluation and resuscitation. Definitive surgical care mustbe instituted by the trauma surgeon in a timely manner thatis consistent with established standards.
4. An attending neurosurgeon must be promptly availableand dedicated to that hospital’s trauma service. The in-house requirement may be fulfilled by an in-houseneurosurgeon or surgeon (or physician in Level II facilities)who has special competence, as judged by the chief ofneurosurgery, in the care of patients with neural trauma,and who is capable of initiating measures directed towardstabilizing the patient and initiating diagnostic procedures.
5. In Level I and Level II institutions, requirements maybe fulfilled by senior level emergency medicine residents
capable of assessing emergency situations in trauma pa-tients and providing any indicated treatment. When resi-dents are used to fulfill availability requirements, the staffspecialist on call will be advised and be promptly available.
6. Requirements may be fulfilled by anesthesiologyresidents capable of assessing emergent situations intrauma patients and of providing any indicated treatment.When anesthesiology residents are used to fulfill availabilityrequirements, the staff anesthesiologist on call will be ad-vised and available promptly.
7. Requirements maybe fulfilled when local conditionsassure that the staff anesthesiologist will be in the hospitalat the time or shortly after the patient’s arrival in the hospitalDuring the interim period, prior to the arrival of the staffanesthesiologist, a certified nurse anesthetist (CRNA) ca-pable of assessing emergent situations in trauma patientsand of initiating and providing any indicated treatment willbe available.

70 ● Rural Emergency Medical Services
B.
Chest Medicine E D—Gastroenterology E D—Hematology E ‘E D——-———Infectious Diseases E D
Internal Medicine E “E E————— —— . .Nephrology E ‘E ‘D
Neuroradiology D
Pathology E E D
Pediatrics E E D
Psychiatry E D ‘-
Radiology E E D—
SPECIAL FACILITIES/RESOURCES/CAPABILITIES1. Emergency Department (ED)
a) Personnel1. Designated physician director E E E—2. Physician with special competence in care of the critically E E“ E
injured who is a designated member of the trauma teamand physically present in the ED 24 hours a day
3. RNs, LPNs, and nurses’ aides in adequate numbers E E ‘E—
b)
E E E
Equipment for resuscitation and to provide life support forthe critically or seriously injured shall include but not belimited to:1. Airway control and ventilation equipment including
Iaryngoscopes and endotracheal tubes of all sizes,bag-mask resuscitator, pocket masks, oxygen, andmechanical ventilator
2. Suction devices E ‘E E
3. Electrocardiograph-oscilloscope-defibrillator E E E
4. Apparatus to establish central venous pressure monitoring E E E
5. All standard intravenous fluids and administration devices, E E Eincluding intravenous catheters
6. Sterile surgical sets for procedures standard for ED, such E E Eas thoracostomy, cut-down, etc.
7. Gastric Iavage equipment E E E
8. Drugs and supplies necessary for emergency care E E E
9. X-ray capability, 24-hour coverage by in-house technician E E E
10. Two-way radio linked with vehicles of emergency transport E E Esystem
11. Skeletal traction device for cervical injuries E E E

Appendix C—Trauma Service Designation Guidelines of ACS and ACEP ● 71
LEVELSI II Ill
2.
3.
4.
5.
6.
Intensive Care Units (ICUs) for Trauma PatientsICUs may be separate specialty units.a) Designated medical director E E E—b) Physician on duty in ICU 24 hours a day or immediately E E D
available from in-hospital
c) Nurse-patient minimum ratio of 1:2 on each shift E E E
d) Immediate access to clinical laboratory services E E E
e) Equipment:1. Airway control and ventilation devices E E E
2. Oxygen source with concentration controls E E
3. Cardiac emergency cart E E E
4. Temporary transvenous pacemaker E E E—5. Electrocardiograph-oscilloscope-defibrillator E E E-
6. Cardiac output monitoring E E D
7. Electronic pressure monitoring E E D— . —8. Mechanical ventilator-respirators E E E
9. Patient weighing devices E E E—10. Pulmonary function measuring devices E E E——11. Temperature control devices E E E
12. Drugs, intravenous fluids, and supplies E E E
13. Intracranial pressure monitoring devices E E D
Postanesthetic Recovery Room (surgical intensive care unit is acceptable)a) Registered nurses and other essential personnel 24 hours E E E
a day
b) Appropriate monitoring and resuscitation equipment E E E
Acute Hemodialysis Capability (or transfer agreement) E D D
Organized Burn Care E E Ea) Physician-directed burn center staffed by nursing personnel
trained in burn care and equipped properly for care of theextensively burned patient,OR
b) Transfer agreement with nearby burn center or hospital with aburn unit — —.——
Acute Spinal Cord/Head Injury Management Capability E E Ea) In circumstances where a designated spinal cord injury rehabilitation
center exists in the region, early transfer should be considered;

72 ● Rural Emergency Medical Services
7.
8.
transfer agreements should be in effectb) In circumstances where a head injury center exists in the
region, transfer should be considered in selected patients;transfer agreements should be in effect
Radiological Special Capabilitiesa) Angiography of all types E E D
b) Sonography E D
c) Nuclear scanning E D
d) In-house computerized tomography with technician E E
Rehabilitation Medicine E E Ea) Physician-directed rehabilitation service staffed by nursing
personnel trained in rehabilitation care and equipped properlyfor care of the critically injured patient,OR
b) Transfer agreement when medically feasible to a nearbyrehabilitation service
C. OPERATING SUITE SPECIAL REQUIREMENTSEquipment-Instrumentation1.
2.
3.
4.
5.
6.
7.
8.
Operating room adequately staffed in-house and immediately available E E D24 hours-a day
Cardiopulmonary bypass capability E D
Operating microscope E D
Thermal control equipment:a) for patient E E E
b) for blood E E E
X-ray capability E E E—Endoscopes, all varieties E E E
Craniotome E E D
Monitoring equipment E E E
D. CLINICAL LABORATORY SERVICE (available 24 hours a day)1. Standard analyses of blood, urine, and other body fluids E E E
2. Blood typing and cross-matching E E E
E E E3. Coagulation studies
4. Comprehensive blood bank or access to a community central blood E E Ebank and adequate hospital storage facilities.
5. Blood gases and pH determinations E E E

Appendix C—Trauma Service Designation Guidelines of ACS and ACEP ● 73
ILEVELS
II Ill
6. Serum and urine osmolalitv E E D*y
7. Microbiology E E E—8. Drug and alcohol screening E E D“
“Toxicology screens need not be immediately available but are desirable. If not available, results should be includedin all quality assurance reviews.
E.
F.
G.
H.
1.
QUALITY ASSURANCE1.
2.
3.
4.
5.
6.
7.
Organized Quality Assurance Program E E E— —— . ——-..——.Special audit for all trauma deaths and other specified cases E E E(see Appendix G on page 42) ———— ————- ——— ————. —— —— — ——— ——Morbidity and mortality review E E E——— ————— -.Trauma conference, multidisciplinary (see note 8) E E -
—. ————-—— .—— — . — - — — —Medical nursing audit, utilization review, tissue review E E E—. ———Trauma registry review (see note 9) E E - ‘ - E
Review of prehospital and regional systems of trauma care E D D
OUTREACH PROGRAM E DTelephone and on-site consultations with physicians of the communityand outlying areas
PUBLIC EDUCATION EInjury prevention in the home and industry, and on the highways andathletic fields; standard first-aid; problems confronting public, medicalprofession, and hospitals regarding optimal care for the injured
TRAUMA RESEARCH PROGRAM E
TRAINING PROGRAM1. Formal programs in continuing education provided by hospital for:
a) Staff physicians E
E D
D D
E D
b) Nurses E E D
C) Allied health personnel E E ‘-D— ——. . ... —..——. — — d) Community physicians E E D. —. — —..—.— ——
NOTES:8. Regular and periodic multidisciplinary trauma confer- 9. Documentation of severity of injury (by trauma score,
ences that include all members of the trauma team should age, injury severity score) and outcome (survival, lengthbe he/d. This conference will be for the purpose of quality of stay, ICU length of stay) with monthly review of statistics.assurance through critiques of individual cases.

.
74 ● Rural Emergency Medical Services
Guidelines for Trauma Care Systems
[These guidelines were developed by the American College of Emergency American College ofPhysicians Trauma Committee and were opproved for publication by the Emergency PhysiciansBoard of Directors on September 18, 1986. These guidelines supersede the Dallas. Texasprevious position statement on trauma are (February 1982:11:105). Ameri-can College of Emergency Physicians: Guidelines for trauma care systems. Address for reprints: American College ofAnn Emerg Med April 1987:16:459-463.) Emergency Physicians. PO Box 619911,
Dallas. Texas 75261-9911
PREAMBLETrauma, defined as serious bodily injury, constitutes our most expensive
yet connectable national health problem.1 Trauma remains the leading causeof death for persons 1 to 37 years of age and the leading cause of disability forpersons of all ages. The overall cost of accidental injury currently exceeds$90 billion annually. 2 Although some areas have already organized and inte-grated the emergency medical services (EMS) system components and pro-viders that are essential to optimizing trauma care, others have failed to de-velop adequate trauma care systems or to acknowledge that such anapproach is necessary.
The American College of Emergency Physicians has long maintained acommitment to the comprehensive care of ill and injured persons, includingtreatment, education, and research. The ability to respond appropriately tothe needs of trauma victims requires the skills and efforts of the entirehealth care team. EMS systems should provide treatment for seriously in-jured patients in an organized and timely fashion. Trauma care is but oneaspect of EMS, however, and special provisions for trauma victims should notbe permitted to fragment the remainder of the emergency medical care sys-tem.
Trauma care represents a continuum that is best provided by an integratedsystem extending from prevention through rehabilitation and requiring closecooperation among specialists in each phase of care. A systems approach totrauma care acknowledges this continuum, improving quality and reducingmortality. Since 1976 the Committee on Trauma of the American College ofSurgeons has periodically published guidelines describing resources for trau-ma care.3 Because optimal treatment requires systems that encompass allaspects of care, however, the Trauma Committee of the American College ofEmergency Physicians has developed these guidelines, which complementthose of the American College of Surgeons by defining the components andproviders that are essential to urban and rural trauma care systems [Figure)
Emergency physicians should provide leadership in trauma care, not onlyby developing and managing systems, but also by directing prehospital care,providing emergency department resuscitation and stabilization, and facili-tating a smooth transition to inhospital care. The American College of Emer-gency Physicians recognizes that inhospital care for the seriously injured ISbest provided by facilities whose governing bodies, administrations, andmedical staffs are committed to excellence in trauma care, and that defini-tive, long-term treatment iS best provided by specialists who are specificallytraincd in trauma care.
The American College of Emergency Physicians encourages all medicalproviders to work together to afford optimal care to all injured persons in the most efficient manner possible. Such relationship between emergency phy-sicians at other members of the trauma care team must be established
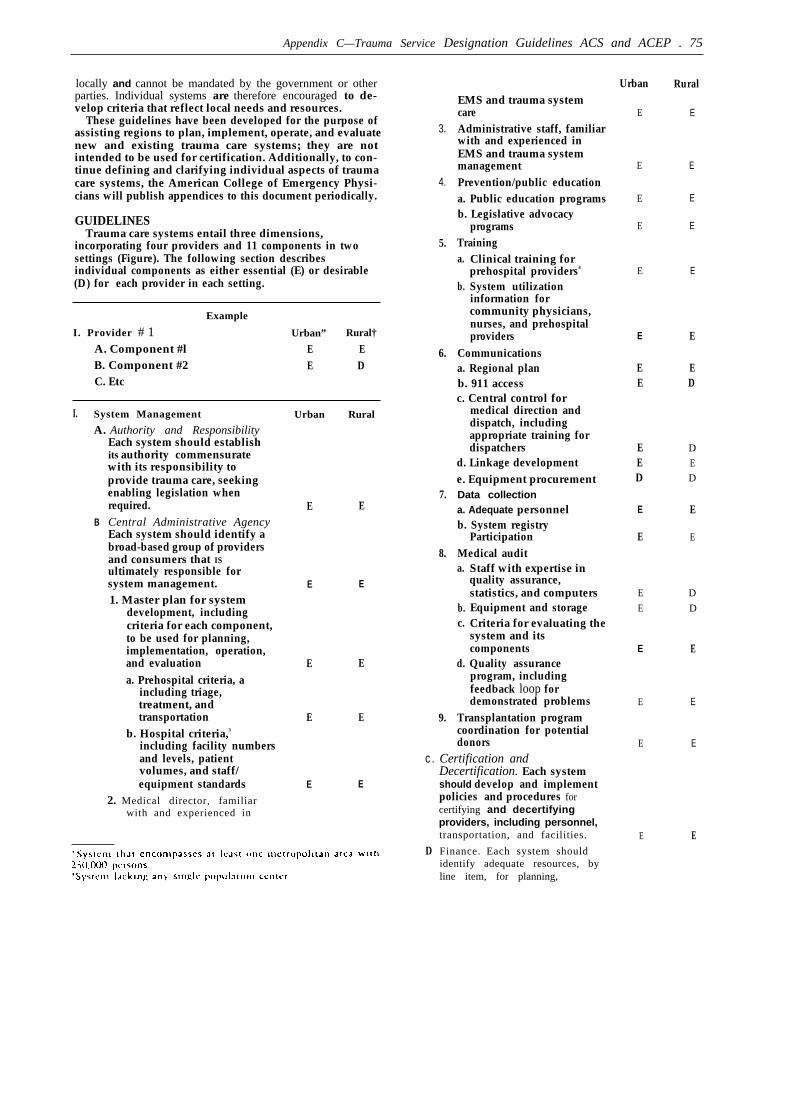
Appendix C—Trauma Service Designation Guidelines ACS and ACEP . 75
locally and cannot be mandated by the government or otherparties. Individual systems are therefore encouraged to de-velop criteria that reflect local needs and resources.
These guidelines have been developed for the purpose ofassisting regions to plan, implement, operate, and evaluatenew and existing trauma care systems; they are notintended to be used for certification. Additionally, to con-tinue defining and clarifying individual aspects of traumacare systems, the American College of Emergency Physi-cians will publish appendices to this document periodically.
GUIDELINESTrauma care systems entail three dimensions,
incorporating four providers and 11 components in twosettings (Figure). The following section describesindividual components as either essential (E) or desirable(D) for each provider in each setting.
Example
I. Provider # 1 Urban” Rural†
A. Component #l E EB. Component #2 E DC. Etc
I. System Management Urban Rural
A. Authority and Responsibility
Urban
E
E
E
E
E
Rural
E
E
E
E
E
EMS and trauma systemcareAdministrative staff, familiarwith and experienced inEMS and trauma systemmanagementPrevention/public educationa. Public education programsb. Legislative advocacy
programsTraining
3.
4.
5.
6.
a.
b.
Clinical training forprehospital providers4
System utilizationinformation forcommunity physicians,nurses, and prehospitalproviders
Communicationsa. Regional planb. 911 accessc. Central control for
medical direction anddispatch, includingappropriate training fordispatchers
d. Linkage developmente. Equipment procurementData collectiona. Adequate personnelb. System registry
ParticipationMedical audit
E E
EE
ED
Each system should establishits authority commensuratewith its responsibility toprovide trauma care, seekingenabling legislation whenrequired.Central Administrative Agency
EED
D
E
D
7.
8.
9.
E E E EB
Each system should identify abroad-based group of providersand consumers that ISultimately responsible forsystem management.1. Master plan for system
development, includingcriteria for each component,to be used for planning,implementation, operation,and evaluationa. Prehospital criteria, a
including triage,treatment, andtransportation
b. Hospital criteria,3
including facility numbersand levels, patientvolumes, and staff/equipment standards
2. Medical director, familiarwith and experienced in
E E
a.
b.c.
d.
Staff with expertise inquality assurance,statistics, and computersEquipment and storageCriteria for evaluating thesystem and itscomponentsQuality assurance
E EE
E
D
D
E EE E
E E
program, includingfeedback loop fordemonstrated problems
Transplantation programE
E
E
Ecoordination for potentialdonors
Certification andDecertification. Each systemshould develop and implementpolicies and procedures forcertifying and decertifyingproviders, including personnel,transportation, and facilities.
Finance. Each system shouldidentify adequate resources, byline item, for planning,
c.
D
E E
E E

r
Components
Medical Direction
Prevention
Communication
Training
Triage
Prehospital Care
Transportation
Hospital Care
Rehabilitation
Public Education
Medical Evaluation
Urban RuralImplementation, operation, andevaluation. E E
E. Emergency/DisasterPreparedness. Each systemshould develop a regionaldisaster plan that integratesEMS, trauma care, and disastermanagement system resources. E1. Regional plan for all
providers E2. Central control through
local emergencymanagement association D
E
E
DII. Prehospital Care
A. Management Agency Eachsystem should identify anagency that is ultimatelyresponsible for prehospital care.In some instances this functionmay be fulfilled by the centraladministrative agency. EI Administration
a. Medical director, familiar with and experienced inprehospital care E
b. Support staff, familiarwith and experienced inprehospital management E
2 Tra in ing
a Sufficient experiencedstaff E
E
FIGURE. Three dimensions of trauma care systems.
b. Curriculum 4 integratedwith system
3. Criteria
a. Protocols3 integrated withsystem
4. Certification anddecertificationa. Consistent with state and
local criteriab. Standardized clinical
examination5. Data collection integrated
with system6. Medical audit integrated
with systemB. Ambulance Standards. Each
system should establishstandards for land and airtransportation, subject tolegislative regulations.1. Personnel2. Equipment3
3. Process for ambulancecertification anddecertification
C Communication System. Each
D
E.
system should develop aprehospital communicationsystem that is fully integratedwith the remainder of the EMSand emergency/disasterpreparedness systems.1. Central control for medical
direction and dispatch2. Equipment
a. Minimize radio deadspace
b. Equip all vehicles andaircraft
Emergency/DisasterPreparedness Plan. Each systemshould develop a prehospitalemergency/disaster preparednessplan that IS fully integratedwith the remainder of the EMSsystem.Prevention/Public Education1. Injury prevention2 First aid and CPR
Ill Hospital FacilitiesA. Trauma Hospital.s Each system
should identify an appropriatenumber of trauma hospitals toprovide immediately availablesurgical care for seriouslyinjureed patients
Urban Rural
E E
E E
E
E
E
E
EEE
E
E
E
E
E
E
EE
E
E
E
E
EEE
E
E
D
D
D
E
EE

Appendix C—Trauma Service Designation Guidelines of ACS and ACEP ● 77
1. Standards3
a.b.c.d.
e.
f.
g.h.
i.
j.
Emergency department
Surgery departmentNursing careLaboratory/blood bank/x-rayComputerized axialtomographyTrauma nurse coordinatorTreatment protocolsIntegrated with EMSsystemDocumented institutionalcommitmentcurrent JCAHaccreditation
2. Communicationa. Integrated with EMS
systemb. Base station hospital
3. Helicopter landing capabilitya. On-siteb. Licensed by regulatory
authority4. Continuing medical
educationa. Physiciansb. Nursesc. Prehospital providers
5. Protocolsa. Prehospital bypass/
rerouting, coordinatedwith other traumahospitals through thecentral administrativeagency
b. Treatments3
c. Transfer,3 for all incomingpatients regardless oforigin
6. Prevention/public educationa. Community-based
programs7. Data collection
a. Adequate personnelb. Hospital registryc. System registry
participation8. Rehabilitation
a. (See Section IV)
9. Medical audita. Adequate personnel
b. Quality assurance
Urban
E
E
E
E
E
E
E
E
E
E
E
D
E
E
E
E
E
E
E
E
E
E
E
E
E
E
Rural
E
E
E
E
D
E
E
E
E
E
E
D
D
E
D
D
E
E
E
E
E
E
E
E
E
E
program, includingfeedback loop fordemonstrated problems
10. Emergency/disasterpreparedness plana. Internal planb. Integrated with remainder
of emergency/disasterpreparedness system
B. Specialty Cure Hospitals. Eachsystem should additionallyidentify specialty care hospitalsfor the small proportion ofpatients requiring suchtreatment. Access preferablyentails prehospital transport,but also includes interhospitaltransfer when medicallyappropriate. If adequate facilitiesdo not exist in the area, formaltransfer agreements should bedeveloped with nearbyresources.
1. standardsa. Pediatric trauma3
b. Bums3
c. Spinal cord traumasd. Hand trauma/limb
replantatione. Eye trauma
2. Current JCAH accreditation3. Communication
a. Integrated with EMSsystem
4. Helicopter landing capabilitya. On-siteb. Licensed by regulatory
authority5. Training
a. Physiciansb. Nursesc. Prehospital providers
6. Protocolsa.
h.c.
Prehospital bypass/rerouting, coordinatedwith other traumahospitals through thecentral administrativeagencyTreatment 3
Transfer, 3 for all incomingp a t i e n t s r e g a r d l e s s o forigin
7. Prevention/public education
a. Community-basedprograms
Urban Rural
E E
E E
E E
E
EEE
EEE
E
D
E
E
EE
E
E
E
E
E
DDD
DDE
E
D
E
D
D
D
E
E
E
E
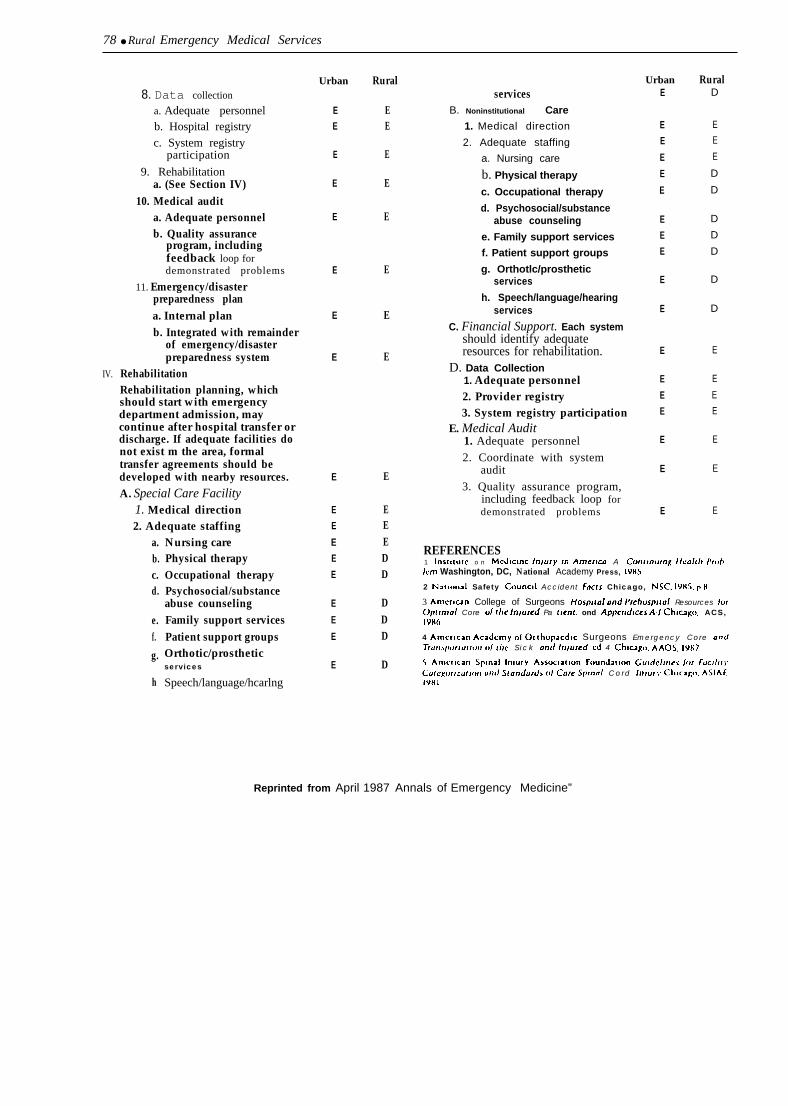
78 ● Rural Emergency Medical Services
IV.
8. Data collection
a. Adequate personnelb. Hospital registryc. System registry
participation
9. Rehabilitationa. (See Section IV)
10. Medical audita. Adequate personnelb. Quality assurance
program, includingfeedback loop fordemonstrated problems
11. Emergency/disasterpreparedness plana. Internal planb. Integrated with remainder
of emergency/disasterpreparedness system
RehabilitationRehabilitation planning, whichshould start with emergencydepartment admission, maycontinue after hospital transfer ordischarge. If adequate facilities donot exist m the area, formaltransfer agreements should bedeveloped with nearby resources.A. Special Care Facility
1. Medical direction2. Adequate staffing
a.b.c.d.
e.f.
g.
h
Nursing carePhysical therapyOccupational therapyPsychosocial/substanceabuse counselingFamily support servicesPatient support groupsOrthotic/prostheticservices
Speech/language/hcarlng
Urban
EE
E
E
E
E
E
E
E
E
E
E
E
E
E
E
E
E
Rural
EE
E
E
E
E
E
E
E
EEEDD
DDD
D
servicesB. Noninstitutional Care
1. Medical direction
2. Adequate staffing
a. Nursing care
b. Physical therapy
c. Occupational therapy
d. Psychosocial/substanceabuse counseling
e. Family support services
f. Patient support groups
g. Orthotlc/prostheticservices
h. Speech/language/hearingservices
C. Financial Support. Each systemshould identify adequateresources for rehabilitation.
D. Data Collection1. Adequate personnel2. Provider registry3. System registry participation
E. Medical Audit1. Adequate personnel
2. Coordinate with systemaudit
3. Quality assurance program,including feedback loop fordemonstrated problems
UrbanE
E
E
E
E
E
E
E
E
E
E
E
E
E
E
E
E
E
RuralD
E
E
E
D
D
D
D
D
D
D
E
E
E
E
E
E
E
REFERENCES1 Ins[itutc o n Mcdlcmc In\ury In Amertw A Crmtinutrrg Hcal(lt Proh/cm Washington, DC, National Academy Press, 19H5
2 Nattonal Safety Counctl Accident Fac(s Chicago, NSC, 19HS. p N
3 Amcmcan College of Surgeons HospItol and Prchosptrol Resources Io(@ulmo/ Core cd r/Je Irr\ured Pa fwn(. ond Appcrrdlces Al Chtciigo, ACS,Iwo
4 Amcrlcan Aca&my O( Orthopacdlc Surgeons Emergency Core orrdTrult\pw(uf~(Jf] (d f/Ic S i c k orrd Infurcd, cd 4 Chtcago, AAOS, 19S7
$ Am~.rlcan Splna] Inlury Assocla[lon Foundatmn L’uIdc/Incs /or FucI/If),Cule~or~zdf)(m und .’irorrdurdi ()/ Core !@nn/ Cord /n/ur\, Chicag(], ASIAF,19U I
Reprinted from April 1987 Annals of Emergency Medicine”
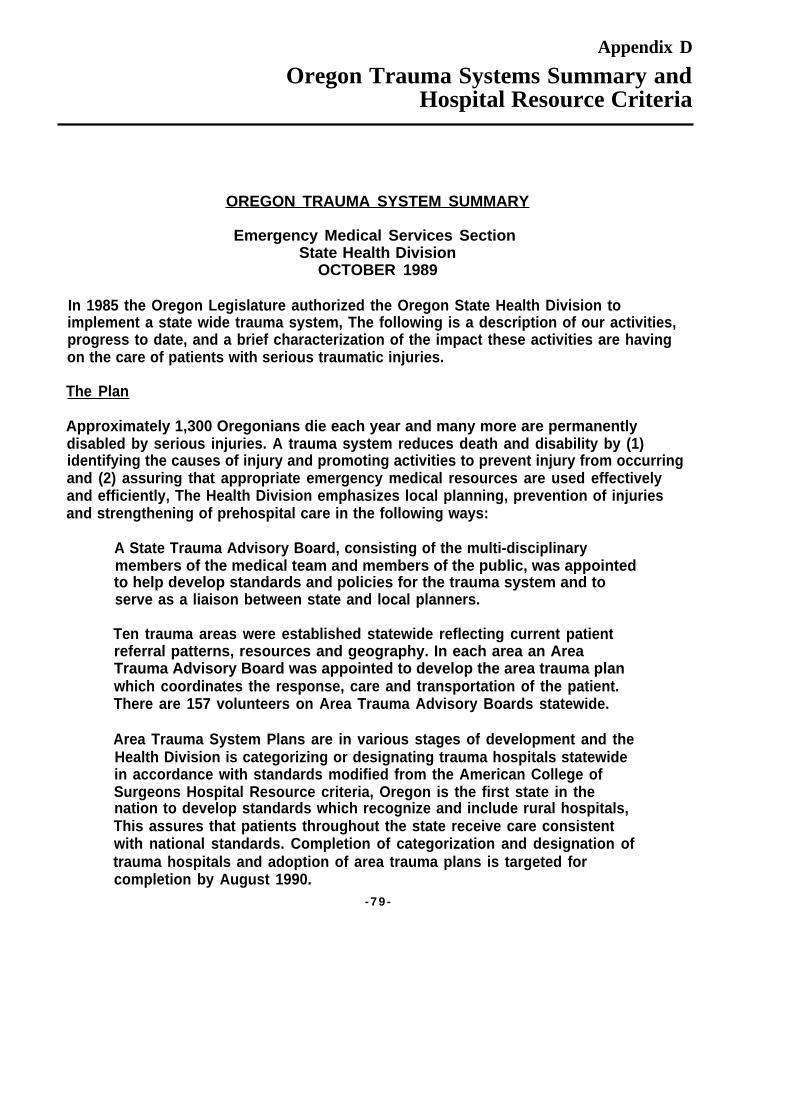
Appendix D
Oregon Trauma Systems Summary andHospital Resource Criteria
OREGON TRAUMA SYSTEM SUMMARY
Emergency Medical Services SectionState Health Division
OCTOBER 1989
In 1985 the Oregon Legislature authorized the Oregon State Health Division toimplement a state wide trauma system, The following is a description of our activities,progress to date, and a brief characterization of the impact these activities are havingon the care of patients with serious traumatic injuries.
The Plan
Approximately 1,300 Oregonians die each year and many more are permanentlydisabled by serious injuries. A trauma system reduces death and disability by (1)identifying the causes of injury and promoting activities to prevent injury from occurringand (2) assuring that appropriate emergency medical resources are used effectivelyand efficiently, The Health Division emphasizes local planning, prevention of injuriesand strengthening of prehospital care in the following ways:
A State Trauma Advisory Board, consisting of the multi-disciplinarymembers of the medical team and members of the public, was appointedto help develop standards and policies for the trauma system and toserve as a liaison between state and local planners.
Ten trauma areas were established statewide reflecting current patientreferral patterns, resources and geography. In each area an AreaTrauma Advisory Board was appointed to develop the area trauma planwhich coordinates the response, care and transportation of the patient.There are 157 volunteers on Area Trauma Advisory Boards statewide.
Area Trauma System Plans are in various stages of development and theHealth Division is categorizing or designating trauma hospitals statewidein accordance with standards modified from the American College ofSurgeons Hospital Resource criteria, Oregon is the first state in thenation to develop standards which recognize and include rural hospitals,This assures that patients throughout the state receive care consistentwith national standards. Completion of categorization and designation oftrauma hospitals and adoption of area trauma plans is targeted forcompletion by August 1990.
- 7 9 -

80 ● Rural Emergency Medical Services
A statewide information system or “injury registry” will gather data aboutcauses of injury, the emergency response and the patient outcome. Inaddition to evaluating the trauma system for quality assurance, this datawill provide information for prevention of injuries.
The Health Division is implementing an injury prevention program which will use theinjury data to develop and implement prevention strategies which focus on problemsspecific to Oregon. This program will provide technical assistance to help localprograms implement effective interventions.
The Health Division has conducted a major pediatric trauma project in aneffort to improve the emergency medical response specifically forseriously ill and injured children.
Progress to Date
The overriding concern both when this bill was passed and since, has been that thetrauma system must meet the diverse needs of Oregon. To address this concern theHealth Division held informational meetings in 21 cities to obtain input aboutemergency medical services problems and to encourage interest in local planning. Inresponse, 325 emergency providers applied to serve on our advisory board (mapattached).
During the past four years the 157 appointed members of the advisory boards havebeen helping to assure that statewide goals, standard and procedures for the traumasystem are appropriate. With the help of the state trauma advisory board, state staffnegotiated compromises among the various recommendations. The results of thisinput and discussion have been incorporated in the Trauma System Rules, filed inFebruary 1987, which establish the minimum standards for area plans covering theprehospital care interhospital transfer, and quality assurance, as well as theprocedures for hospital categorization and designation.
A Trauma System Resource Guide was developed which describes goals andguidelines of the trauma system and assists the area trauma advisory boards with theirtrauma system planning efforts, Another document, a request-for-proposal, assistshospitals in developing their trauma services and prepares them for verificationsurveys.
Current Activities
Each area trauma advisory board has been writing an area trauma system plan whichis due in three phases. The plan for Area 1 (the seven northwest counties of Oregon)has been completed and was implemented May 2, 1988. The state board is providingassistance and review to assure that area plans meet state standards. In the

Appendix D--Oregon Trauma Systems Summary and Hospital Resource Criteria . 81
meantime, the Health Division staff are organizing visits by teams of experts to allhospitals. This process of categorization and designation assures that patients aretreated in hospitals with a high commitment to trauma care regardless of hospital sizeand location.
Within Area #1 (see map attached) two level I trauma hospitals have been designatedin Portland, consistent with the recommendations set forth by the providers in the areatrauma system plan. In the surrounding counties, three level Ill & IV trauma hospitalswere designated, Since the trauma system was implemented in May 1988, the areaboard has been working with the Health Division to develop and implement a modelquality assurance program for the continual monitoring and evaluation of the traumasystem.
In Areas #7, #9, and #10 (most of Central and Eastern Oregon) the first part of thearea trauma system plans have been approved and are being implemented, Fifteenhospitals serving these areas were surveyed in November 1988 by teams of out-of-state trauma experts and were categorized as trauma hospitals.
The remaining trauma areas (Areas #2, #3, #4, #5, #6 and #8) are in various stagesof trauma system plan development.
The State Trauma Advisory Board is focusing on developing quality assuranceactivities, evaluating the rural hospital resource criteria, and continuing to assist AreaTrauma Advisory Boards with trauma plan development.
Impact on Patient Care
In some areas, the trauma planning process has provided a useful forum for amicableproblem solving. The emergency medical service providers are working out problemsand upgrading the quality of care through training and improved coordination. In otherareas, the trauma board is providing the forum for heated but fair resolution of long-standing controversies. The providers are compromising on their preferredapproaches to a trauma system. A few boards are struggling with what often seem tobe insurmountable problems and inadequate resources. Progress is slow in theseareas, In the area that has an implemented system hospitals are reporting excellentspin-off effects to non-trauma services as a result of developing their trauma service.Providers report that patients are receiving care that is more consistently in keepingwith the goals for rapid definitive care. In all areas of the state, the development of thetrauma system is being tackled by the appropriate people -- the providers who have toimplement it and the public who will be served by it. We expect to meet a 1990deadline for a system to improve care for all trauma patients.

82 ● Rural Emergency Medical Services
1
w
w
w
w
w
o

Appendix D-Oregon Trauma Systems Summary and Hospital Resource Criteria ● 83
o
0 0
0 00
0 0 0
J!
e
w wu
u 0

84 ● Rural Emergency Medical Services
w
w
w u
w0
0
00
v
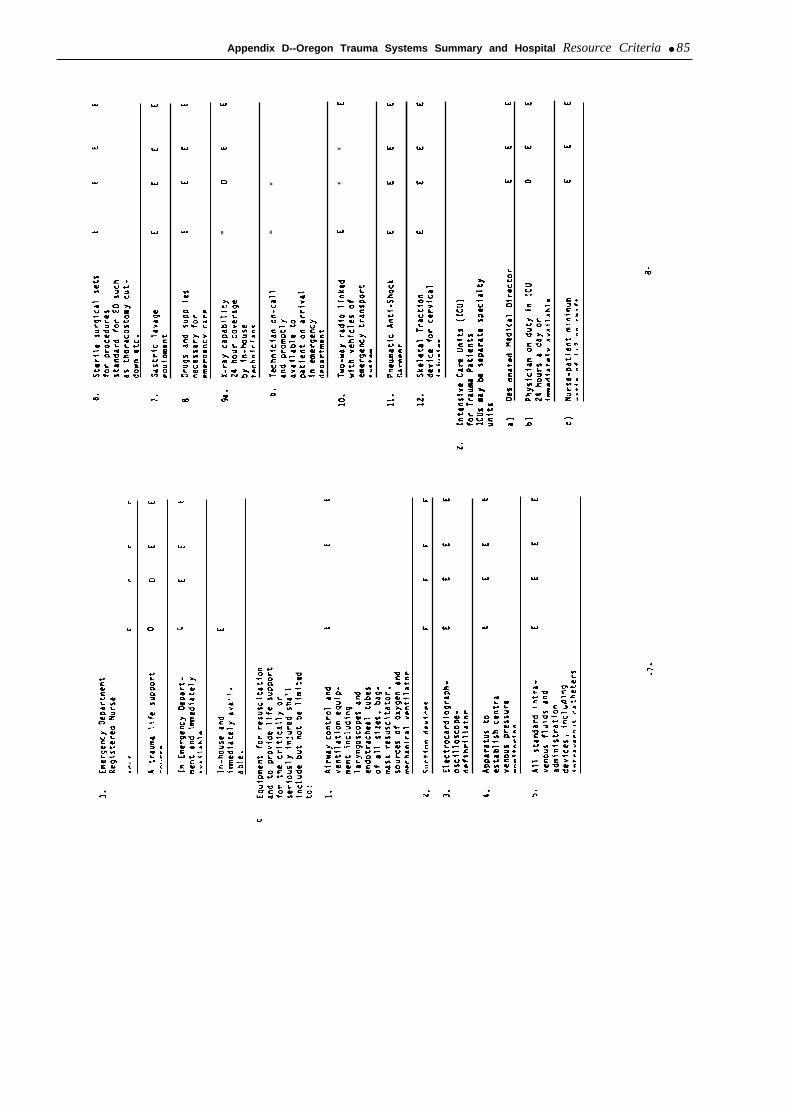
Appendix D--Oregon Trauma Systems Summary and Hospital Resource Criteria ● 85
w
wu
0 0
-
.
w
w

86 ● Rural Emergency Medical Services
w
a
.
D v
- 0
Appendix D-Oregon Trauma Systems Summary and Hospital Resource Criteria • 87
ww
w
w
w w
.
.0
.

88 ● Rural Emergency Medical Services
o
0

Appendix E
Trauma Care/EMS Legislation Introduced Duringthe 101st Congressional Session
S.15—Emergency Medical Services andTrauma Care Improvement Act of 1989
(C101) 01/25/89
Sen. Cranston (Cosp=23)Senate Labor and Human Resources
DIGEST AS INTRODUCED:
Emergency Medical Services and Trauma Care Im-provement Act of 1989—Amends the Public HealthService Act to create a new title on trauma care. Directsthe Secretary of Health and Human Services to provide forthe establishment and operation of a National Clearing-house on Emergency Medical Services and Trauma Care.Authorizes appropriations for FY 1990 through 1992 orfor the first three fiscal years for which funds areappropriated. Authorizes the Secretary to make grants andenter into cooperative agreements and contracts withrespect to emergency medical services and trauma caresystems to: ( 1 ) conduct and support research, training,evaluations, and demonstration projects; (2) providetechnical assistance to State and local agencies; and (3)establish guidelines for the development of uniform Statedata reporting systems.
Directs the Secretary to make an allotment for eachState for each fiscal year, mandating that at least 35percent, subject to adjustment, be used for planning,implementing, monitoring, and evaluating the operationof county, regional, or State trauma care systems. Setsforth requirements for such systems. Requires States touse at least 35 percent of the amount available to them fora fiscal year to reimburse designated trauma centers foruncompensated trauma care expenditures. Requires non-Federal matching contributions (in cash or in kind) in aspecified ratio for fiscal years after FY 1990. Requireseach State, for each fiscal year beginning with FY 1990,to submit the trauma care component of the Stateemergency medical services plan (State plan) to theSecretary. Sets forth requirements for the State plan.Requires that hospital emergency departments, withintheir capability, if an individual appears and requestsexamination and treatment: ( 1 ) examine for the existenceof an emergency medical condition or active labor and, ifsuch a condition or labor exists, treat the individual untilstable, subject to exception; and (2) transfer such individ-ual to other facilities only according to stated criteria.Requires States to adopt guidelines for the designation of
trauma centers, and for triage, transfer, and transportationpolicies, at least as stringent as the applicable guidelinesdeveloped by the American College of Surgeons and bythe American College of Emergency Physicians. Man-dates that States: (1) require each trauma center to provideinformation to the State central data reporting systemannually; (2) submit, to the Secretary at least annually. theinformation it receives from its data reporting andanalysis system; and (3) identify and submit to theSecretary a list of rural areas lacking certain emergencymedical services. Sets forth restrictions on the use of Stateallotments. Requires an annual report from each State tothe Secretary. Sets forth a formula for determination of theamount of allotments. Provides for: (1) repayment andoffset for failure to use funds as agreed: (2) criminalpenalties for certain false statements; (3) technical assis-tance and provision of supplies and services by theSecretary in lieu of grant funds; and (4) a report by theSecretary to the Congress.
Authorizes appropriations for FY 1990 through 1992.Directs the Secretary of Health and Human Services toconduct studies: (1) to determine the adequacy andappropriateness of the reimbursements provided to traumacenters under Title X1X (Medicaid) of the Social SecurityAct: and (2) of the long-term economic effects of trauma.Amends the Public Health Service Act to revise theapplication procedure for Preventive Health and HealthServices Block Grants to provide the State officerresponsible for the administration of the State highwaysafety program an opportunity to participate in thedevelopment of any plan relating to emergency medicalservices as such plan relates to high way safety. Allows theState official responsible for the provision of emergencymedical services the opportunity to participate in thedevelopment of the State highway safety program as suchprogram relates to emergency medical services.
Amends the Public Health Service Act and the Consol-idated Farm and Rural Development Act to allow certaingrant allotments to be used for the purchase of communi-cations equipment. Requires the Federal Communica-tions Commission to: ( 1 ) study the availability of radiofrequency channels for emergency medical servicescommunications: (2) establish a plan to ensure that theneeds of emergency medical services communications areprovided for in the allocations of frequencies for publicsafety; and (3) submit a report to Committees of theCongress containing such study and plan.
-89-

90 ● Rural Emergency Medical Services—
S. Amdt. No. 378—Amendment to S.15(C101) 07/20/89
Sen. Cranston (Acosp=9)Senate Labor and Human Resources
CONG REC S8521
AMENDMENT DIGEST:SENATE
To provide funding toservices in rural areas.
FROM HOUSE OR
support emergency medical
S.1274-Comprehensive and UniformRemedy for the Health Care System Act of
1989 (C1O1) 06/23/89Sen. HatchSenate Labor and Human Resources
DIGEST AS INTRODUCED:
Limited to provisions pertaining to EMS Comprehen-sive and Uniform Remedy for the Health Care System Actof 1989—Title V: Improving the Trauma Care System—Subtitle A: General Federal Emergency Medical ServicesPrograms-Amends the Public Health Service Act tocreate a new title on emergency medical services. Directsthe Secretary of Health and Human Services, by contract,to provide for the establishment and operation of aNational Clearinghouse on Emergency Medical Servicesand Trauma Care. Sets forth the duties of the Clearing-house. Allows the Clearinghouse to charge fees to defrayand, starting with FY 1991, to cover its costs of operating.Authorizes appropriations for FY 1990 through 1992 orfor the first through the third fiscal year after FY 1990 forwhich funds are appropriated under these provisions.
Directs the Secretary to promulgate regulations thatrequire States that receive grants under provisions addedby this Act relating to emergency medical services blockgrants to provide the Secretary with certain data andinformation concerning the use of the grants.
Authorizes the Secretary to make grants for researchand demonstration projects concerning ways to improvethe availability and quality of prehospital emergencymedical services in rural areas by: ( 1 ) developinginnovative uses of communications technologies; (2)making continuing education more accessible to emer-gency medical services personnel; (3) developing andrefining training curricula; (4) undertaking outcomestudies; and (5) developing innovative financing mecha-nisms. Authorizes appropriations for FY 1990 through1992.
Requires the Federal Communications Commission,within one year of enactment of this Act, to: (1) completea study of the availability of radio channels for emergency
medical services; (2) establish a plan to ensure that theneeds of such services shall be adequately provided for inthe allocation of frequencies; and (3) submit a reportcontaining the study and the plan to the appropriateCommittees of the Congress,
Subtitle B: Emergency Medical Services Block Grant—Amends the Public Health Service Act to authorizeappropriations for allotments to States for FY 1990through 1992. Directs the Secretary, for each such fiscalyear, to: (1) allot to each State an amount under a specifiedformula related to the population and land area of theState; and (2) make payments to each State. Prohibits theSecretary from making payments unless the State identi-fies any rural area for which there is no: ( 1 ) emergencymedical services access through a 911 telephone number;(2) basic life-support system; or (3) advanced life-supportsystem.
Sets forth application requirements.
Requires that amounts paid to a State under theallotments be used for: ( 1 ) accident prevention programs;(2) feasibility studies and planning activities for emer-gency medical services systems; (3) emergency medicalservices; (4) uncompensated trauma care as specified inthis Act; and (5) other activities as determined by theSecretary.
Allows a State that receives a grant under the allotmentto use not more than 25 percent of the grant to pay theexpenses of certain uncompensated trauma care that hasbeen provided.
Allows a State to use a limited amount to carry outemergency medical services activities under these provi-sions.
Removes provisions of the Public Health Service Actwhich allow States to use block grant allotment sums forfeasibility studies and planning for emergency medicalservices systems and the establishment, expansion, andimprovement of such systems.
H.R.911—Volunteer Protection Act of 1989(C101) 02107/89
Rep. Porter (Cosp=200)
DIGEST AS INTRODUCED:
Volunteer Protection Act of 1989—Prescribes circum-stances under which volunteers working for nonprofitorganizations or government entities shall be immunefrom personal financial liability for acts on behalf of theorganization or entity. Sets forth exceptions to andconditions on the granting of such immunity that a Statemay impose, Requires the Secretary of Health and HumanServices to increase by one percent the fiscal yearallotment which would otherwise be made to a State to

Appendix E—Trauma Care/EMS Legislation Introduced During the 101st Congressional Session ● 91
carry out the Social Services Block Grant Program underTitle XX of the Social Security Act if such State has,within two years, certified to the Secretary that it hasenacted a State law which provides such immunity.Provides for the continuation of such increase based on anannual recertification.
H.R.950—National Rural Health Care Act of1989 (C101) 02/09/89
Rep. Roybal (Cosp=30)
DIGEST AS INTRODUCED:
Limited to provisions pertaining to EMS—Amends thePublic Health Service Act to authorize the Secretary tomake grants to States which have submitted fiscal yearplans for comprehensive State rural health access plan-ning to assist States in such planning. Authorizesappropriations for such grant program through FY 1992.Requires each State to submit a comprehensive ruralemergency medical services plan to the Secretary for eachfiscal year, beginning with FY 1990. Authorizes appropri-ations through FY 1992 for payments to States, whichvary among States on the basis of the proportion of thenation’s rural population which reside in each State, tocover the costs of planning, implementing, and monitor-ing the operation of trauma care systems in rural areas.
Authorizes the Secretary to make grants to public andnonprofit entities for planning, constructing, equipping,supplying, and operating a rural health clinic and trainingthe personnel at such clinic. Authorizes the Secretary tomake grants to solo and small group medical practiceswhich provide primary health services to medicallyunderserved rural populations to assist such practices inpurchasing equipment and supplies and training person-nel. Sets forth grant conditions, including the requirementthat such clinics and practices accept as patients Medicareand Medicaid recipients residing in their service area, andprovide 24-hour-a-day emergency medical services.
Authorizes appropriations through FY 1992.
H.R.1587—Rural Emergency MedicalServices Improvement Act of 1989 (C101)
03/23/89Rep. Cooper (Cosp=51)House Energy and Commerce
DIGEST AS INTRODUCED:
Rural Emergency Medical Services Improvement Actof 1989—Amends the Public Health Service Act to createa new title on emergency medical services for rural areas.Directs the Secretary of Health and Human Services tomake an allotment for each State each fiscal year forimproving the availability and quality, in rural areas, of
emergency medical services and emergency medicalservices systems provided to victims of emergencies priorto the arrival of the victims at medical facilities. Requires,after FY 1990, non-Federal matching contributions in aspecified ratio.
Allows a State to expend payments received for: (1)recruitment, training, and retention of personnel; (2)purchase, upgrading, and maintenance of equipment; (3)planning, coordination, and support of local emergencymedical services and systems; and (4) public education.
Requires that the State plan for emergency servicesprovide for adequate services in rural areas. Sets forth aformula for determination of the amount of allotments.Authorizes appropriations for FY 1990 through 1992.Authorizes the Secretary to make grants for research intoand demonstration projects concerning ways to improvethe availability and quality of prehospital emergencymedical services in rural areas by using communicationstechnologies, making continuing education more accessi-ble, improving curricula, undertaking outcome studies,and developing innovative financing mechanisms.
Authorizes the Secretary to make grants for pilotprojects to develop community-based centers to coordi-nate and deliver comprehensive occupational health andsafety services to rural communities.
Authorizes appropriations for FY 1990 through 1992for improving rural prehospital emergency services andfor centers for rural occupational health and safetyservices.
H.R.1586—A Bill To Require a Study onMedicare Reimbursement for Ambulance
Services (C101) 03/23/89Rep. Cooper (Cosp=48)
DIGEST AS INTRODUCED:
Directs the Secretary of Health and Human Services toconduct a study into the adequacy and appropriateness ofMedicare (Title XVIII of the Social Security Act)payments for ambulance services and report the results ofsuch study to the Congress within one year of this Act’senactment.
H.R.1602—Trauma Care Systems Planningand Development Act of 1989 (C101) 03/23/89Rep. Bates (Cosp=37)House Energy and Commerce
DIGEST AS INTRODUCED:
Trauma Care Systems Planning and Development Actof 1989—Amends the Public Health Service Act to createa new title on trauma care.

92 ● Rural Emergency Medical Services
Authorizes the Secretary of Health and Human Serv-ices to make grants and enter into cooperative agreementsand contracts with respect to trauma care to: (1) conductand support research, training, evaluations, and demon-stration projects; (2) foster development of trauma caresystems; (3) collect and disseminate information; (4)provide technical assistance to State and local agencies;and (5) sponsor workshops and conferences.
Directs the Secretary to establish the Advisory Councilon Trauma Care Systems. Declares that, notwithstandingprovisions of the Federal Advisory Committee Act, theCouncil shall continue in existence until otherwiseprovided by law,
Directs the Secretary to make an allotment for eachState for each fiscal year for developing, implementing,and monitoring the modifications to the trauma-carecomponent of the State plan for the provision ofemergency medical services. Requires non-Federal match-ing contributions (in cash or in kind) in specified ratios forfiscal years after the first fiscal year of payments. Statesthat such component of the State plan will be modifiedwith regard to: ( 1 ) trauma care regions, centers, andsystems; (2) triage and transport of children; (3) accredita-tion and evaluation; (4) data reporting and analysissystems; (5) procedures for paramedical personnel toassess the severity of injuries; (6) transportation andtransfer policies; (7) public education; (8) coordinationand cooperation; and (9) other matters.
Requires States to adopt guidelines for the designationof trauma centers, and for triage, transfer, and transporta-tion policies, equivalent to the applicable guidelinesdeveloped by the American College of Surgeons and bythe American College of Emergency Physicians. Author-
izes the Secretary, after public notice and an opportunityfor comment, to waive the requirement of adoption ofsuch guidelines.
Mandates that States: (1) require each trauma center toprovide certain information to the State emergencymedical system annually; (2) submit to the Secretary, atleast annually, the information it receives from its datareporting and analysis system; and (3) identify and submitto the Secretary a list of rural areas lacking certainemergency medical services.
Sets forth restrictions on the use of State allotments.Requires an annual report from each State to theSecretary. Sets forth a formula for determination of theamount of allotments. Provides for: ( 1 ) repayment andoffset for failure to use funds as agreed; (2) criminalpenalties for certain false statements; (3) technical assis-tance and provision of supplies and services by theSecretary in lieu of grant funds; and (4) a report by theSecretary to the Congress.
Authorizes appropriations for FY 1990 through 1992.
Directs the Secretary of Health and Human Services toconduct studies to: (1) identify programs established byStates in order to reimburse trauma care centers and otherhealth care providers for the uncompensated provision ofhealth care; and (2) determine the adequacy and appropri-ateness of the reimbursements provided to trauma centersand ambulance service providers under Title XIX (Med-icaid) of the Social Security Act.
SOURCE: Congressional Research Service, Bill DigestFiles, SCORPIO, October 1989.

References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
American College of Emergency Physicians, ‘‘Pre-hospital Advanced Life Support Skills, Medica-tions, and Equipment, ’ Annals of EmergencyMedicine 17(10): 1109-111, October 1988.American College of Emergency Physicians, ‘Guide-lines for Emergency Medical Services Systems, ”Annals ofEmergency Medicine 17(7):742-745, July1988.American College of Emergency Physicians, ‘Guide-lines for Trauma Care Systems, ” Annals of Emer-gency Medicine 16(4):459-463, April 1987.American College of Surgeons, Committee onTrauma, Hospital and Prehospital Resources forOptimal Care of the Injured Patient and AppendicesA Through J, 1987.American College of Surgeons, Committee onTrauma, “Hospital Resources Documents: FieldCategorization of Trauma Patient (field triage), ”Bulletin American College of Surgeons 71( 10): 17-21, October 1986.American Hospital Association, OTA analysis ofdata from the American Hospital Association, 1987Annual Survey 1988-89.Anderson, P. B., “Rural ENIS, ” paper presented atthe Rural EMS Workshop-U. S. Congress, Officeof Technology Assessment, Washington, DC, May4-5, 1989.Anderson, P, B,, “The Idaho Statewide EMS Com-munications Center, ’ Emergency Medical Services10(4):7-13, July/August 1981.Anderson, P. B., Bjornson, D. R., and Wayne, M.,‘‘I”elelecture: Providing Effective Continuing Edu-cation, An Innovative Approach to Training inRural America, ” Journul of Emergency MedicalServices, March 1982.Anderson, P. B., Neuman, K. J., and Trimble, G. R.,“Trauma in the Country: A Statewide Approach toTrauma Skills Training for Rural EMTs, ’ Journalof Emergency Medical Services, March 1986, pp.61-63.Anderson, T. E., Rose, W. D., and bicht, M. J.,‘‘Physician-Staffed Helicopter Scene Response Froma Rural Trauma Center, Annals of EmergencyMedicine 16(1):58-61, January 1987.Baker, S. P., O’Neil], B., and Karpf, R. S., The InjuryFact Book (bxington, Massachusetts Toronto,1984).Baker, S. P., Whitfield, M. S., and O’Neill, B.,‘‘County Mapping of Injury Mortality, ’ Journal oj.Trauma 28(6):741-745, June 1988.Baker, S. P., Whitfield, M. S,, and O’Neill, B.,“Geographic Variations in Mortality From MotorVehicle Crashes, ” The New England Journal ofMedicine 316(22):1384-1387, May 28, 1987.
15.
16.
17,
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28,
Border, J., “Panel: Prehospital Trauma Care—Stabilize or Scoop and Run, ” Journal of Trauma23(8):703-71 1, 1983.Brodsky, H., and Hakkert, A. S., “Highway FatalAccidents and Accessibility of Emergency .NledicalServices,’ Social Science Medicine 17(1 1):731-740, 1983.Cadigan, R. T., and Bugarin, C. E., “Trauma Regis-tries: Bases for Comparison, ’ Presentation at theAnnual Meeting of the American Public HealthAssociation, New Orleans, LA, October 1988.Cales, R. H., ‘‘Advanced Life Support in PrehospitalTrauma Care: An Intervention in Search of anIndication?” Annals ofEmergeru?)h4edicine 17(6):65 1-653, June 1988.Cales, R. H., and Trunkey, D. D., “PreventableTrauma Deaths, Journal of the Americun MedicalAssociation 254(8):1059-63, 1985.Campbell, J. E., and McMahan, P., “Trauma Care:A Race Against Time, ” Alabama Medicine, Janu-ary 1985, pp. 10-39.Certo, T. F., Rogers, F. B., and Pilcher, D. B., “Re-view of Care of Fatally Injured Patients in a RuralState: 5-year FOI1OWUP,” The Journal of Trauma23(7):559-565, July 1983.Champion, H. R., “Trauma Care Systems: TheFederal Role, ” The Journal of Trauma 28(6):877-879, June 1988.Champion, H. R., Copes, S. C., Buyer, D., Flanagan,M. E., et al,, ‘‘Major Trauma in Geriatric Patients, ”American Journal of Public Health 79(9):1278-1282, September 1989.Chew, J. L., Emergency Medical Services ProgramSpecialist, National Highway Traffic Safety Ad-ministration, Department of Transportation, per-sonal communication, May, 1989.Commanday, C., ENIS Manager. Oregon Departm-ent of Human Resources, Health Division, per-sonal communication, September 1989.Committee on Trauma Research Commission onLife Sciences, National Research Council and theInstitute of Medicine, Injun’ in America: A L’{mtin-uing Public Health Problem (Washington, DC:National Academy Press, 1985).Committee to Review the Status and Progress of theInjury Control Program at the Centers for DiseaseControl, Injury Control: A Re~qie~v ifthc Status andProgress of the Injury Control Progrum at theCenters for Disease Control (Washington. DC:National Academy Press, 1988).Committee to Study Medical Professional Liabilityand the Delivery of Obstetrical Care, Division ofHealth Promotion and Disease Prevention, Instituteof Medicine, Medical Professional Liability and the
-93–

94 ● Rural Emergency Medical Services
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Delivery of Obstetrical Care (Washington, DC:National Academy Press, 1989).Coopers and Lybrond, “Air Ambulance Issues, ”proceedings of the Air Ambulance conferencesponsored by the Department of Transportation,National Highway Safety Administration, June23-24, 1988.Craren, E.J., Hoffman, K. D., and hopold, R.,‘‘Public Knowledge of EMS: Evaluating the Informa-tion/Public Education Component, ” Journal ofEMS, November 1986, pp. 36-38.Cross, C., “Southeast Ohio’s Answer to the Emer-gency in Emergency Medical Service,’ Appalachia,August-September 1973, pp. 1-11.Culp, J., Office of Rural Health Policy, HealthResources and Services Administration, Depart-ment of Health and Human Services, personalcommunication, Rockville, MD, October 1989.Cummins, R. O., Eisenberg, M. S., Graves, J. R., andDamon, S. K., “EMT-Defibrillation. Part 1: Is ItRight for You?” Journal of Emergency MedicalServices, January 1985, pp. 60-64.Cummins, R. O., Eisenberg, M. S., Graves, J. R., etal., “EMT-Defibrillation. Part 3: Achieving Medi-cal Control’ Journal of Emergency Medical Serv-ices, March 1985, pp. 48-53.Cummins, R. O., Graves, J. R., Eisenberg, M. S., etal., “EMT-Defibrillation. Part 2: ImplementingEMT- D,’ Journal of Emergency Medical Services,February 1985, pp. 44-47.Dalzell, G. W., Prouzina, S., Magee, H., et al.,“Assessment of a Device for Trans-TelephonicControl of Defibrillation,” The Lancet, 1(8587):695-6%, Mar. 26, 1988.Dimon, T., Chairperson, Emergency Nurses Associ-ation, Rural Special Interest Group, personal com-munication, May 1989.Donovan, P. J., Cline, D. M., Whitley, T. W., Foster,C., et al., “Prehospital Care by EMTs and EMT-Isin a Rural Setting: Prolongation of Scene Times byALS Procedures, ” Annals of Emergency Medicine,18:495-500, May 1989.East, S., and Tenbnnk, T. D., “A Nodal Concept ofEMS for Rural North Missouri, ’ Kirksville Collegeof Osteopathic Medicine, unpublished manuscript,August 1989.Ellis, E. G., “One Solution to the Rural MedicalProblem,’ Texas Hospitals 43(8):40-42, January1988.Garrison, H.G., Benson, N. H., and Whitley, T. W.,“Helicopter Use by Rural Emergency Departmentsto Transfer Trauma Victims: A Study of Time-to-Request Intervals, ” American Journal of Emerg-ency Medicine 7(4):384-6, July 1989.Gilbertson, M., Director of EMS, State of New YorkDepartment of Health, Albany, NY, personal com-
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
munication, August 1989.GoIdman, B., “Drama on Computer Screen Provesa Good Teacher, ” Canadian Medical AssociationJournal, 139:240-243, August 1988.Grimes, V., South Carolina Department of Healthand Environmental Control, Division of EMS,Columbia, SC, personal communication, August1989.Halpin, T. W., Emergency Medical Services Pro-gram, New York Department of Health, personalcommunication, Rochester, NY, October 1989.Hanson, N. W., Chief, Emergency Medical Services,Minnesota Department of Health, Minneapolis,MN, October 1989.Barrington, C., Gallagher, S. S., Burgess, L., et al.,injury Prevention Programs in State Health De-partments: A National Surve> (Boston, MA: Child-hood Injury Prevention Resource Center, March1988).Hartley, J. M., Landis, S. S., and Allison, E. J.,“Physicians’ Forum: Medical Direction and Ac-countability for EMS Advanced Life Support Carein Rural North Carolina, ” North Carolinu MedicalJournal 46(5):271-273, May 1985.Headricks, A., and Alberts, D., Center for HealthEconomics Research, “Closures of Rural HospitalsBetween 1980 and 1987, ” prepared for the Depart-ment of Health and Human Services, Health CareFinancing Administration, August 1989.Hewitt, M., “Defining “Rural” Areas: Impact onHealth Care Policy and Research,” U.S. Congress,Office of Technology Assessment, July 1989.Higgins, D., and Goss, J. R., “Jump Crews: AnApproach to Rural Emergency Medical Care, ’ TheEMT Journal 4(2):29-31, June 1980.Hunt, R. C., McCabe, J. B., Hamilton, G. C., et al.,“Influence of Emergency Medical Services Sys-tems and Prehospital Defibrillation on Survival ofSudden Cardiac Death Victims, American Journalof Emergency Medicine 7(1):68-82, January 1989.Johnson, J., Director, Emergency Medical Services,Porter Memorial Hospital, Valparaiso. Indiana,personal communication, October 1989.Krob, M. J., Cram, A. E., Vargish, T., et al., “RuralTrauma Care: A Study of Trauma Care in a RuralEmergency Medical Services Region, ” Annafs ofEmergency Medicine, 13:891-895, October 1984.Larson, D. M., and Mellstrom, M. S., “Managementof Multiple Trauma in a Rural Setting, ’ MinnesotaMedicine 70(1):43-5, January 1987.Macione, A. R., and Wilcox, D. E., “UtilizationPrediction of Helicopter Emergency Medical Serv-ices,” Annals of Emergency Medicine 16:391-399,April 1987.Madden S., Director, Health Services InformationDivision, Public Health Foundation, personal com-

58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
munication, N“ovember 1989.Marshall, S., and Croy, L., “How the West WasWon: A Systems Approach to EMS in the TexasPanhandle, ’ Journal of Emergeruy Medical Sen~-ices 14(6):50-53, June 1988.McGlown, K. J., “Flatiron: A MAST Service forRural Alabama. ” Journal qf Emergency MedicalServices 8(1 1):40-42, November 1983.McHenry, S., Director, Division of EmergencyServices, Virginia Department of Health,Richmond, Virginia, communication at the OTARural EMS Workshop, May 4-5, 1989, Washing-ton, DC.Merlis, M., “Rural Hospitals, ” Congressional Re-search Service (CRS) Report for Congress, CRS,Washington DC, May 2, 1989.Metcalf, W. R., “Emergency Medical Services, ”Presentation at A Workshop for State and LocalGovernment Officials on Rural Health Care, Spon-sored by the User Liaison Program, National Centerfor Health Services Research and Health CareTechnology Assessment, Public Health Service,U.S. Department of Health and Human Services,Boerne, TX, Nov. 30, 1988.Metcalf, W. R., Director, Emergency Medical Serv-ices, American College of Emergency Physicians,Dallas, TX, personal communication, October 1989.Miller, C., Mountain Management, Ojo Sarco, NewMexico, personal communication, October 1989.The Missouri Health Facilities Review Committee,Certificate of Need Program Staff, “Missouri AirAmbulance Report, ” The Missouri Certificate ofNeed Program, Jefferson City, MO, January 1989.Mueller, B. A., Rivara, F. P., and Bergman, A. B.,“Urban-rural Imcation and the Risk of Dying in aPedestrian-vehicle Collision,’ The Journal of Trauma28(1):91-94, January 1988.Murphy, D. J., Pollock, J., Smith G., et al., First onthe Scene, Northeast Regional Agricultural Engi-neering Service, Cooperative Extension, Ithaca,NY, January 1989.Murray, J., “Levels of Training for a Rural State, ”Emergency Medical Services 9(2):49-50, March-Aprd 1980.Myrick, J, A., Kay, B. J., Kishbaugh, D., et al.,“Acceptance of a Volunteer First-Responder Sys-tem in Rural Communities: A Field Experiment, ”Medical Care 21(4):389-399, April 1983.National Academy of Sciences, National ResearchCouncil, Accidental Death and Disability — TheNeglecled Disease of Modern Socie~’ (Washington,DC: National Academy Press, 1966).National Association of State Emergency MedicalServices Directors (NASEMSD), ‘Resolution: Emer-gency Medical Communications, ” adopted by theNASEMSD at Breckenridge, CO, Oct. 26, 1988.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
S2.
83.
84.
85.
86.
National Safety Council, “Work Accidents, 1987, ”National Safety Council 32-94:97-100, 1988.Newman, M. M., “Defibrillation Shakes the Niation:Results of the JEMS 1988 National Early Defibrilla-tion Study, ” Journal of Emergency Medical Sen-ices January 1989.Newman, M. M., Emergency Medical Services Con-sultant, personaJ communication, October 1989.North Central Florida Health Planning Council,Inc., Florida District III Health Plan, “EmergencyMedical Services, ” North Central Florida HealthPlanning Council, Inc., Gainesville, FL, 1988.Ornoto, J. P., Craren, E. J.. and Nelson, N. M.,“Impact of Improved Emergency Medical Servicesand Emergency Trauma Care on the Reduction inMortality from Trauma, ” The Journal oj” Trauma25(7):575-579, July 1985.Pierce, J. C., “Established Rural Health Systems, ”EMT Journal 5(1):40-41, February 1981.Ploss, J. E., “A History of the .Medical Care Programof the UMWA Welfare and Retirement Fund, ’unpublished Master of Science dissertation, Schoolof Hygiene and Public Health of the Johns HopkinsUniversity, 1981.Pens, P. T., “Advances in Pre-hospital Care: TheTechnology of Emergency Medical Services, ”Mental in.rtruments 22(3): 143-145, June 1988.Potter, D., Goldstein, G., Fung, S. C., and Selig, M.,“A Controlled Trail of Prehospital Advanced LifeSupport in Trauma, ” Annals of Emergency Medi-cine, 17:582-588, June 1988.President’s Commission on Highway Safety,Health, Medical Care and Transportation of (heinjured, 1965.Reeder, L., “Seeding Clouds of Change: TheDrought in Rural EMS, ” Journa/ of EmergencyMedical Services, 14(6)42-49, June 1988.Reins, H. D., Bartlett, R. L., and Chudy, N. E., “IsAdvanced Life Support Appropriate for Victims ofMotor Vehicle Accidents: The South CarolineHighway Trauma Project, ” Journal of Trauma28(5):563-570, 1988.Rosenberg, M. L., Graitcer, P. L.. and Waxweiler,R. J., “Introduction: Moving From the 1990 InjuryControl Objectives to State and bcal SurveillanceSystems’ in CDC Surveillance Summaries, Mor-bidity Mortality Weekly Revieti’, 37( SS- 1 ): 1-4, Feb-ruary 1988.Rosenblat~ R. A., and Amundson, B., “The Scopeof Service in Rural Hospitals: Recommendations ofthe WAMI Rural Hospital Projec~s, ’ OccasionalPaper #l, Rural Hospital Project, February 1988.Ruskin J. N., “Automatic External Defibrillatorand Sudden Cardiac Death, ” The New EnglandJournal of Medicine 319(1 1):713-715, Sept. 15,1988.
96 ● Rural Emergency Medical Services
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
Russell, G., ‘‘Providing Emergency Services in theSmall or Rural Hospital, ‘‘ Texas Hospitals 36(5):58-60, October 1980.Sacco, W. J., Jameson, J. W., Copes, W. S., et al.,“Partition: A Quantitative Method for EvaluatingPrehospital Services for Trauma Patients, ” Com-puters in Biology and Medicine 18(3):221-227,1988.Sanders, A. B., ‘‘Emergency Medicine, ’ Journal ofthe American h4edicul Association 261(19)2841-2843, May 19, 1989.Scalice, B. ‘‘More than a Numbers Game, ” Journalof Emergency Medical Services June 1988, pp.46-47.Scheib, B.T., “A Decade of Service: MAST-Military Assistance to Safety and Traftlc,’ Jourrudof Emergency Medical Services, November 1983,pp. 38-45.Schneider, A., Rescue at Risk (Pittsburgh, PA: ThePittsburgh Press, 1987).Spear, S. F., “Life-Threatening Emergencies: Pat-terns of Demand and Response of a RegionalEmergency Medical Services System, ” AmericanJournal of Preventive Medicine 2(3):163-8, May-June 1986.Spoor, J. E., ‘‘Rural Advanced EMT Training-PartIII,” Ernergerq Medical Service 10(1 ):52-55, January/February 1981.SpruilI, W.N. Jr., Director, Office of EmergencyMedical Services, Mississippi State Department ofHealth, Nationzd Survey of EMS Funding: Innova-tive Approaches, October 1984 (prepared on behalfof the National Association of State EMS Direc-tors).Stambler, H., Director, Office of Data Analysis andManagement, Bureau of Health Professions, HealthResources and Services Administration, U.S. De-partment of Health and Human Services, Rockville,MD, Sept. 8, 1989.Stamper, D., communication at the OTA Rural EMSWorkshop, May 4-5, 1989, Washington, DC.State EMS Office, ‘Communications Programs andDisaster Preparedness,’ Produced by the NationalEMS Clearinghouse and The Charles McC MathiasNational Study Center for Trauma and EMS, 1988.Steele, R., “Development of a Minimum Data Setfor Emergency Medical Services Patient RecordKeeping, ” prepared for Health Services Adminis-tration, July 1974.Stults, K. R., “EMT-Defibrillation in Rural Amer-ica, ’ Physician Assistunt, September 1986, pp.111-121.Stults, K. R., Brown, D. D., and Kerber, R. E., “Effi-cacy of an Automated External Defibrillator in theManagement of Out-of-Hospital Cardiac Arrest:Validation of the Diagnostic Algorithm and Initial
lo~.
103.
104.
105,
106.
107.
108.
109.
110.
111.
Clinical Experience in a Rural Environment, ”Circulation 73(4):701-709, April 1986.Stults, K. R., Brown, D. D., Schug, V. L., and Bean,J. A., ‘Prehospital Defibrillation Performed by Emer-gency Medical Technicians in Rural Communi-ties, ’ The New England Journul of Medicine310(4):219-223, January 1984.Swan, T., communication at the National RuralHealth Association, “National Rural EMS NeedsWorkshop,” San Diego meeting, March 1989.The National EMS Clearinghouse, “Training andCertification of EMS Personnel, ” The NationalEMS Clearinghouse, a service of The NationalAssociation of State Emergency Medical ServicesDirectors and The Council of State Governments,Iron Works Pike, bxington, KY, January 1989.The National EMS Clearinghouse and The CharlesMcC Mathias National Study Center for Traumaand EMS, “State EMS Office: CommunicationsPrograms and Disaster Preparedness, ” The Na-tional EMS Clearinghouse, a service of The Na-tional Association of State Emergency MedicalServices Directors and The Council of State Gov-ernments, Iron Works Pike, bxington KY, October1988.The National EMS Clearinghouse, “State EMSOffIce: Evaluation/Information Systems and PublicInformation/Education, The National EMS Clear-inghouse, a service of The National Association ofState Emergency Medical Services Directors andThe Council of State Governments, Iron WorksPike, kxington KY, October 1988.The National EMS Clearinghouse, “The EMSOffIce: Its Structure and Functions, ” The NationalEMS Clearinghouse, a service of The NationalAssociation of State Emergency Medical ServicesDirectors and The Council of State Governments,Iron Works Pike, bxington KY, January 1988.The National EMS Clearinghouse, “EmergencyMedical Services Transportation Systems and Avail-able Facilities, ” The National EMS Clearinghouse,a service of The National Association of StateEmergency Medical Services Directors and TheCouncil of State Governments, Iron Works Pike,hxington KY, January 1988.The National EMS Clearinghouse, “ProtectionFrom Liability for EMS Personnel, ” The NationalEMS Clearinghouse, a service of The NationalAssociation of State Emergency Medical ServicesDirectors and The Council of State Governments,Iron Works Pike, hxington, KY, August 1987.The National Registry of Emergency MedicalTechnicians, personal communication. August 1989.U.S. Congress, Office of Technology Assessment,“Rural Health Care, ’ in progress.
References ● 97
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
U.S. Congress, Office of Technology Assessment,Rural Emergency Medical Services Workshop,Washington, DC, May 4-5, 1989.U.S. Department of Commerce, Bureau of theCensus, 1980 Census of Population, Volume 1:Characteristics of the Population, December 1983.U.S. Department of Health and Human Services,National Center for Health Services Research andHealth Care Technology Assessment, “Can LayPersons Use AEDs to Save Heart Attack Victims?’NCHSR Research Activities, September 1989.U.S. Department of Health and Human Services,National Center for Health Services Research andHeaJth Care Technology Assessment, “CommunityPlanning for EMT Defibrillation, ” NCHSR Pro-gram Note, October 1985.U.S. Department of Health and Human Semices,National Center for Health Statistics, C,A. Schoen-born and M. Marano, 1988. Current estimates formthe National Health Interview Survey: L’nitedStates, 1987, Vital and Health Statistics. Series 10,No. 166, DHHS pub. No. (PHS) 88-1594, PublicHealth Sewice.U.S. Department of Health and Human Services,National Center for Health Statistics, J.G. Collins:Types of injuries and impairments due to injuries,United States. Vital and Health Statistics. Series 10,No. 159. DHHS Pub. No. (PHS) 87-1587, PublicHealth Service.U.S. Department of Health and Human Services,“Identification and Analysis of the Distribution ofPhysicians by Specialty Utilizing the Area ResourceFile (ARF) County-Specific Data Base,” preparedby Applied Management Sciences, Inc., Dec. 23,1988.U.S. Department of Health and Human Services,Public Health Service, Centers for Disease Control,“Perspectives in Disease Prevention and HealthPromotion: Progress Toward Achieving the Na-tional 1990 Objectives for Injury Prevention andControl,” MorbkiityMom.liiy Weekly Report 37(9):138-146, Mar. 11, 1988U.S. Department of HeaIth and Human Services,Public Health Semice, Centers for Disease Control,“CDC Surveillance Summaries,” Morbidity Mor-tality Week/y Report 37(N0. SS-1) February 1988.U.S. Department of Health and Human Services,Public Health Service, Centers for Disease Control,‘‘Premature Mortality due to Unintentional Injuries,United States, 1984, ” Morbidity Mortality WeeklyReport 36(49):814-815, Dec. 18, 1987.U.S. Department of Transportation, National Acci-dent Sampling System 1986, a report on traffic
123.
124.
125,
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
137.
crashes and injuries in the LTnited States, July 1988.U.S. Department of Transportation, National High-way Traffic Safety Administration, Fatal AccidentReporting System: 1987, December 1988.U.S. Department of Transportation, National High-way Traffic Safety Administration, ‘‘EmergencyMedical Servicesnrauma System Development,”undated paper, Washington, DC.U.S. Department of Transportation, National High-way Traffic Safety Administration, memo on coor-dinating committee, Washington, DC, 1984.U.S. Department of Transportation, National High-way Traffic Safety Administration, ‘‘EmergencyMedical Services Technical Assistance Program, ”undated paper, Washington, DC.U.S. General Accounting Office, States AssumeLeadership Role in Providing Emergenq MedicalServices, Publ. No. GAO/HRD-86-l 32 (Washing-ton, DC, September 1986).Urdaneta, L. F., Miller, B. K.. Ringenberg. B. J., etal., “Role of an Emergency Helicopter TransportService in Rural Trauma,” Arch. Surx. 122:992-996, September 1987.Van Cott, C., Communications Director, Office ofEmergency Medical Services, State of North Caro-lina, personal communication, October 1989.Vukov, L. F., White, R. D., Bachman, J. W., et al.,“New Perspectives on Rural EMT Defibrillation, ”Annals of Emergency Medicine 17:31 8-321, April1988.Wayne, R., “Rural Trauma Management, ” TheAmerican Journal of Surgery 157:463-467, May1989.Wears, R. L., “Predicting the Demand for Emer-gency Medical Services, ” Annals of EmergencyMedicine 18:705-707, June 1988.West, J. G., Williams, M. J., Trunkey, D. D., andWolferth, C. C., ‘‘Trauma Systems: Current Status—Future Challenge s,’ Journal of the American Medi-cal Association 259(24):3597- 1445, June 1988.Willard, G., Texas Department of Health, Austin,TX, personal communication, August 1989.Wolfe, H., and Shuman, L. J.. ‘‘RURALSIM: AModel for Rural EMS Systems Planning, ’ contractreport prepared for U.S. Congress, OTA, April1989.Yamamoto, L. G., “Cellular Telephone Communi-cation Between Hospitals and Ambulance s,’ Amer-ican Journal of Emergency Medicine 6(1 ):35-38,January 1988.Yeakley, C., Oregon Health Division, EMS Section,Portland, Oregon, personal communication, Octo-ber 1989,