rural telemedicine for primary healthcare in …passino/telemedicine.pdf · rural telemedicine for...
TRANSCRIPT
IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004 0278-0079/04/$20.00©2004IEEE | 13
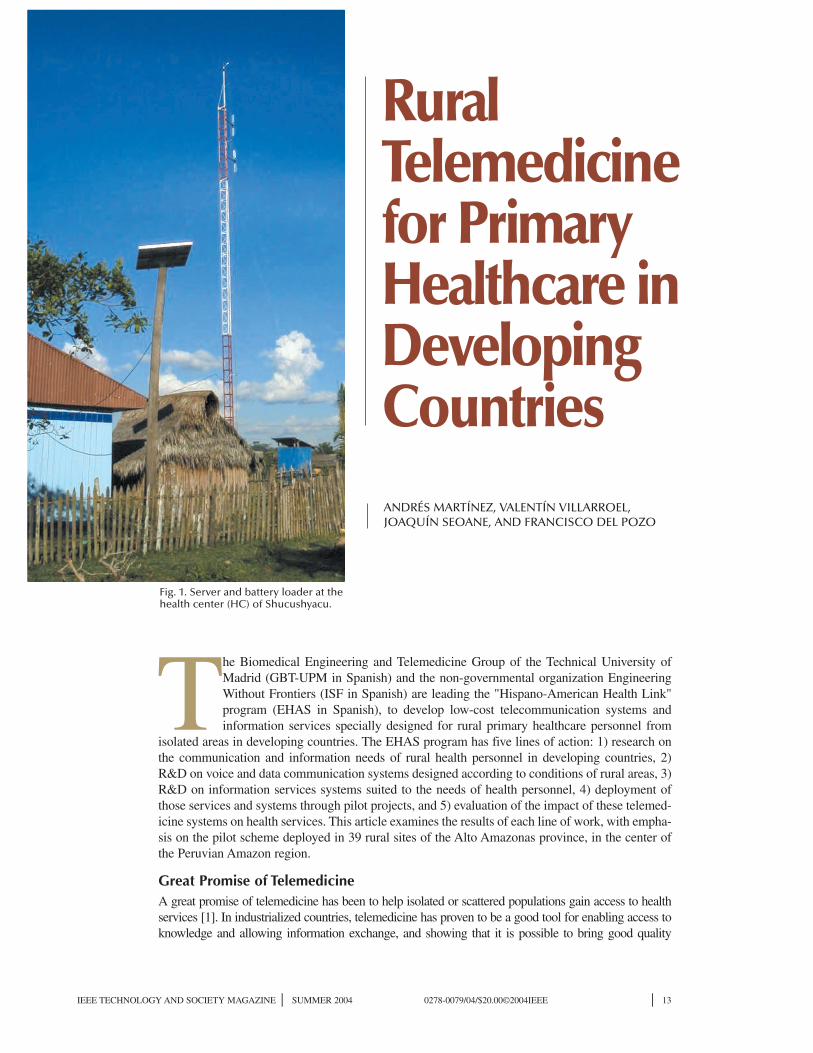
The Biomedical Engineering and Telemedicine Group of the Technical University ofMadrid (GBT-UPM in Spanish) and the non-governmental organization EngineeringWithout Frontiers (ISF in Spanish) are leading the "Hispano-American Health Link"program (EHAS in Spanish), to develop low-cost telecommunication systems andinformation services specially designed for rural primary healthcare personnel from
isolated areas in developing countries. The EHAS program has five lines of action: 1) research onthe communication and information needs of rural health personnel in developing countries, 2)R&D on voice and data communication systems designed according to conditions of rural areas, 3)R&D on information services systems suited to the needs of health personnel, 4) deployment ofthose services and systems through pilot projects, and 5) evaluation of the impact of these telemed-icine systems on health services. This article examines the results of each line of work, with empha-sis on the pilot scheme deployed in 39 rural sites of the Alto Amazonas province, in the center ofthe Peruvian Amazon region.
Great Promise of TelemedicineA great promise of telemedicine has been to help isolated or scattered populations gain access to healthservices [1]. In industrialized countries, telemedicine has proven to be a good tool for enabling access toknowledge and allowing information exchange, and showing that it is possible to bring good quality
Rural Telemedicine for Primary Healthcare in Developing CountriesANDRÉS MARTÍNEZ, VALENTÍN VILLARROEL,JOAQUÍN SEOANE, AND FRANCISCO DEL POZO
Fig. 1. Server and battery loader at thehealth center (HC) of Shucushyacu.

14 | IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004
healthcare to isolated communities [2].Telemedicine can also (and must)
be used to deliver healthcare to poorareas in countries with scarce infra-structure and to developing countries[3], [4]. But while information andcommunication technologies havetremendous potential for improvinghealthcare, we have to bear in mindthat in rural areas of many develop-
ing countries, telephone networksand computers are scarce (Fig. 2).This is especially true in the healthsector [5].
Another barrier to the imple-mentation of telemedicine in ruralareas of developing countries islimited access to electricity (Fig. 3)[6]. Yet another important factor isthe deficient transportation infra-
structure (Fig. 4) resulting in a lackof appropriate maintenance andcontrol systems, limited ability toafford expensive telecommunica-tion infrastructure, and poorlytrained health personnel. Due tothese restrictions, the rural popula-tions of developing countries(already a highly underservedgroup) are far from enjoying theadvantages of the so-called “GlobalInformation Society.” Informationand communication technologiesand services can improve the workconditions of isolated health staffonly if those technologies areselected, developed, adapted, andcarefully deployed to suit the popu-lation’s real needs in their real envi-ronment [7].
These facts highlight importantdifferences between developed anddeveloping countries that conditionany telemedicine project. More-over, there is a technology gapbetween urban and rural zoneswithin developing countries them-selves. While in the main towns ofdeveloping countries most moderncommunication networks are acces-sible (ISDN; xDSL; Frame Relay,etc.), there are many rural areaswithout even a basic telephone net-work. Therefore, while the telemed-icine experiences of urban areas,mostly interhospital projects, arevery similar anywhere, ruraltelemedicine projects seeking toimprove the efficiency of primarycare result in quite different imple-mentations, depending on whetherwe are dealing with rural areas ofindustrialized countries or isolatedrural areas of developing countries.The needs and priorities are com-pletely different [8]. Most impor-tantly, the lack of communicationinfrastructure and financial limita-tions condition enormously boththe appropriate technology and theservices required.
The Enlace Hispano Americanode Salud (EHAS) initiative is aviable proposal to deploy telemed-icine systems and services in ruralareas of developing countries.
Fig. 2. Number of telephones (fixed and cellular) per 100 inhabitants.
140phones (fixed & cellulars)/100 inhab.
120
100
80
60
40
200.5 4 1.3 3 6
99
133
84
101
86
0
Moz
ambi
que
Nic
arag
ua
Yem
en
Vie
tnam
Mor
occo
US
A
Nor
way
Gre
ece
Japa
n
Aus
tral
ia
Kw-h in 1998/inhab.
25000
20000
15000
10000
5000384 281 96 232 443
11832
24607
7322
3735
8717
0
Moz
ambi
que
Nic
arag
ua
Yem
en
Vie
tnam
Mor
occo
US
A
Nor
way
Gre
ece
Japa
n
Aus
tral
ia
Fig. 3. Electricity consumption per capita.

IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004 | 15
Rural Health Establishmentsin Developing CountriesMany developing countries orga-nize primary healthcare aroundtwo types of care centers. At themost basic level are Health Posts(HP), in other countries calledsurgeries. HPs are the way mostcitizens gain access to the health-care system. At the higher level areHealth Centers (HC), also referredto as either basic polyclinics orambulatory care centers, depend-ing on the country.
HPs and HCs are usually orga-nized into networks, with the HCthe reference point for several HPsthat depend clinically and adminis-tratively on the HC. This network isa "health micronet," the basic unit ofthe primary health system.
It is important to highlight thecommon characteristics of thesecenters throughout developingcountries. HPs are mainly locatedin small towns of no more than athousand inhabitants, have no tele-phone lines, and have a poor roadnetworks. HPs rarely have morethan one health worker (two inexceptional cases), normally aninfirmary technician or recentlygraduated physician with limitedtraining. HPs depend on HCs forsevere case referral, pharmaceuti-cal deliveries, epidemiologicalmanagement, and coordination ofthe general activities within themicronet. As a result of the wide-spread absence of communicationsystems, when health personnelneed to exchange information theyhave to travel on foot or by land orriver vehicles, taking hours or evendays to do so.
HCs are above HPs in thehealth system hierarchy. Thetowns where HCs are located usu-ally have access to the telephonenetwork. HCs are always headedby physicians, have equipment fordiagnostic tests, and sometimeshave hospitalization facilities. Asmentioned, the HC serves as thereference establishment for sever-al HPs.
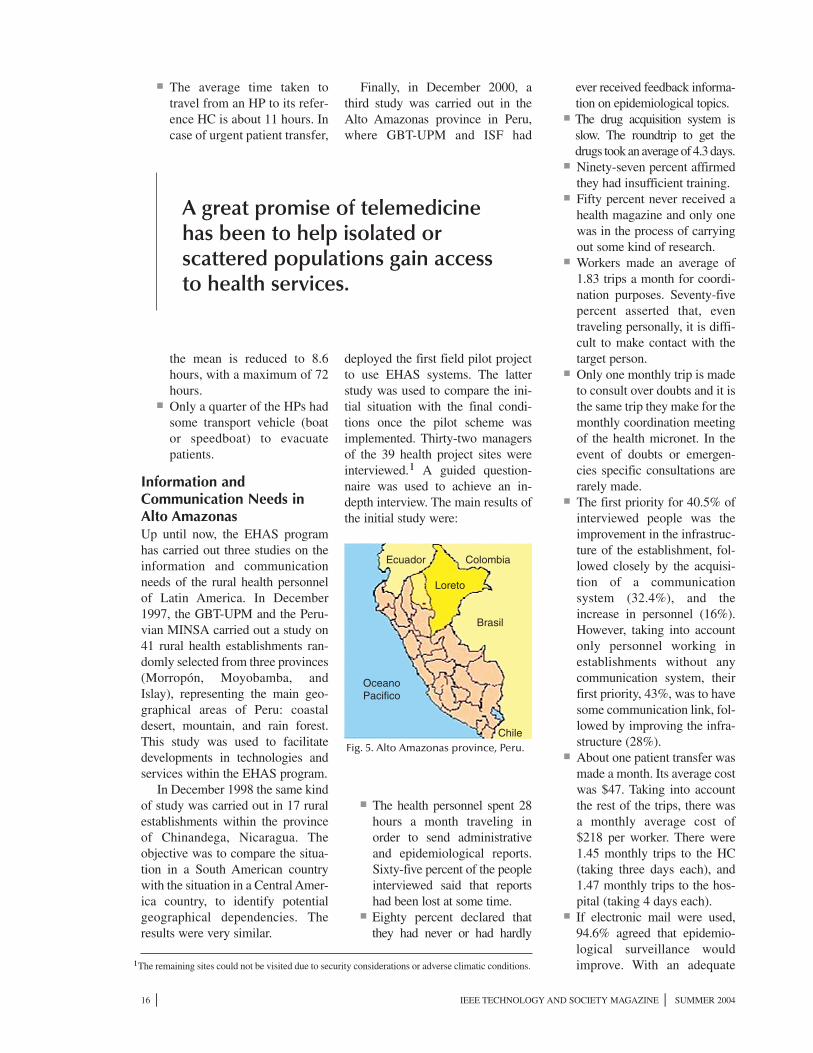
Primary Care System of theAlto Amazonas Province ofPeru We shall now explain in more detailthe situation of the primary healthestablishments of the Peruvian Min-istry of Health (MINSA) in theprovince of Alto Amazonas, Loretoregion, where the first deploymentexperience of EHAS technologiesand services is taking place. AltoAmazonas is a province with twicethe surface area of Belgium and 116200 inhabitants located in the Peru-vian rain forest (Fig. 5). Its capital isYurimaguas and the province isdivided into 11 districts.
According to the Peruvian Min-istry of Health (MINSA), Alto Ama-zonas province forms a unique
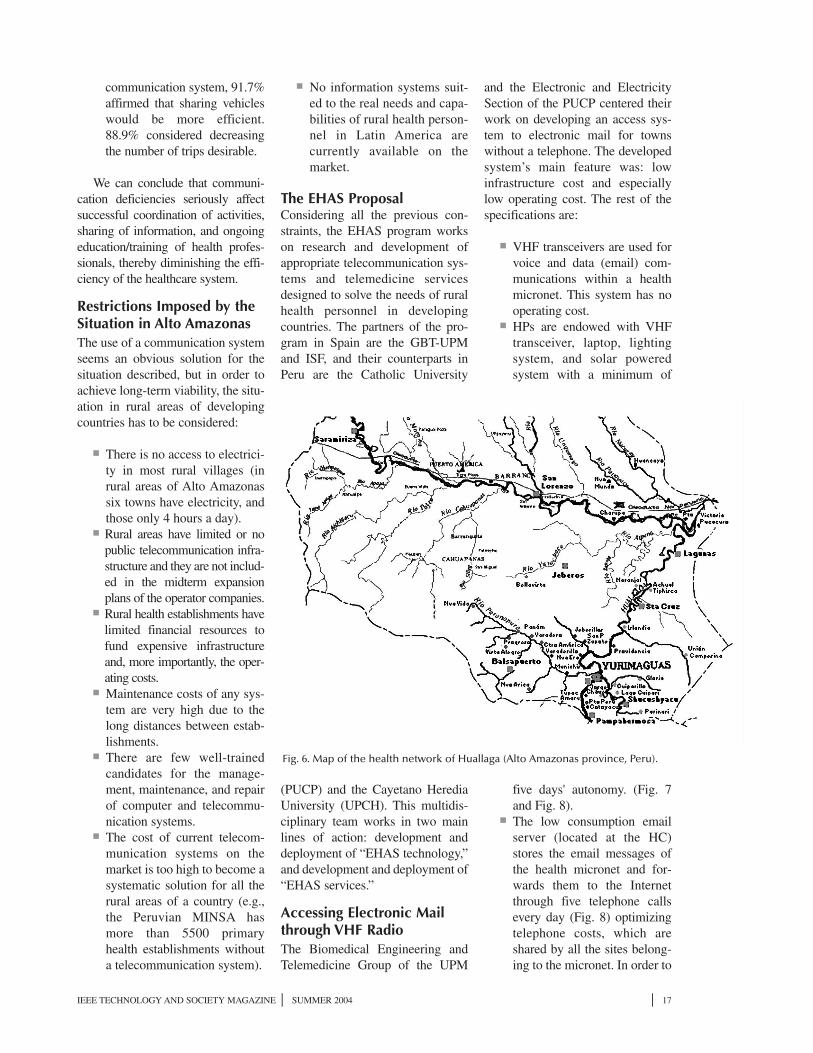
"health net" with 93 health estab-lishments: 1 provincial Hospital inYurimaguas, 11 HCs and 81 HPs.The pilot project of the EHAS pro-gram in Peru was carried out in thesouthern part of the province(referred to as "Huallaga health sub-net") (Fig. 6) and deployed telecom-munication systems in 40 establish-ments (the urban Hospital, 6 rural
HCs and 33 rural HPs). Alto Ama-zonas province has only one nonas-phalt road, which links the capitalwith the rest of the country. All oth-er surface transport within theprovince has to be carried out byriverboat. Only 8 out of the 93health establishments in theprovince are accessible by road.
On December 1, 2000, we foundthe following scenario in AltoAmazonas:
■ Only the Hospital and twoother HCs (one of them in thecapital) had a telephone. Sev-enty one percent of the estab-lishments did not have anycommunication system. Theremaining 29% had a HFradio or a public telephone in
the town. ■ Only one HP out of 32 had a
physician in charge. Infir-mary technicians headed therest. The average age ofphysicians heading HCs was32 years. They had 2 years'experience and only one yearworking in their currentestablishment.
Fig. 4. Paved roads per 100 000 inhabitants.
2000 Kms asphalted/100.000 inhab.
1800
1600
1200
1000
800
600
400
200 34 38 35 36 112
14191529
1021
676
1910
0
Moz
ambi
que
Nic
arag
ua
Yem
en
Vie
tnam
Mor
occo
US
A
Nor
way
Gre
ece
Japa
n
Aus
tral
ia
■ The average time taken totravel from an HP to its refer-ence HC is about 11 hours. Incase of urgent patient transfer,
the mean is reduced to 8.6hours, with a maximum of 72hours.
■ Only a quarter of the HPs hadsome transport vehicle (boator speedboat) to evacuatepatients.
Information andCommunication Needs inAlto AmazonasUp until now, the EHAS programhas carried out three studies on theinformation and communicationneeds of the rural health personnelof Latin America. In December1997, the GBT-UPM and the Peru-vian MINSA carried out a study on41 rural health establishments ran-domly selected from three provinces(Morropón, Moyobamba, andIslay), representing the main geo-graphical areas of Peru: coastaldesert, mountain, and rain forest.This study was used to facilitatedevelopments in technologies andservices within the EHAS program.
In December 1998 the same kindof study was carried out in 17 ruralestablishments within the provinceof Chinandega, Nicaragua. Theobjective was to compare the situa-tion in a South American countrywith the situation in a Central Amer-ica country, to identify potentialgeographical dependencies. Theresults were very similar.
Finally, in December 2000, athird study was carried out in theAlto Amazonas province in Peru,where GBT-UPM and ISF had
deployed the first field pilot projectto use EHAS systems. The latterstudy was used to compare the ini-tial situation with the final condi-tions once the pilot scheme wasimplemented. Thirty-two managersof the 39 health project sites wereinterviewed.1 A guided question-naire was used to achieve an in-depth interview. The main results ofthe initial study were:
■ The health personnel spent 28hours a month traveling inorder to send administrativeand epidemiological reports.Sixty-five percent of the peopleinterviewed said that reportshad been lost at some time.
■ Eighty percent declared thatthey had never or had hardly
ever received feedback informa-tion on epidemiological topics.
■ The drug acquisition system isslow. The roundtrip to get thedrugs took an average of 4.3 days.
■ Ninety-seven percent affirmedthey had insufficient training.
■ Fifty percent never received ahealth magazine and only onewas in the process of carryingout some kind of research.
■ Workers made an average of1.83 trips a month for coordi-nation purposes. Seventy-fivepercent asserted that, eventraveling personally, it is diffi-cult to make contact with thetarget person.
■ Only one monthly trip is madeto consult over doubts and it isthe same trip they make for themonthly coordination meetingof the health micronet. In theevent of doubts or emergen-cies specific consultations arerarely made.
■ The first priority for 40.5% ofinterviewed people was theimprovement in the infrastruc-ture of the establishment, fol-lowed closely by the acquisi-tion of a communicationsystem (32.4%), and theincrease in personnel (16%).However, taking into accountonly personnel working inestablishments without anycommunication system, theirfirst priority, 43%, was to havesome communication link, fol-lowed by improving the infra-structure (28%).
■ About one patient transfer wasmade a month. Its average costwas $47. Taking into accountthe rest of the trips, there wasa monthly average cost of$218 per worker. There were1.45 monthly trips to the HC(taking three days each), and1.47 monthly trips to the hos-pital (taking 4 days each).
■ If electronic mail were used,94.6% agreed that epidemio-logical surveillance wouldimprove. With an adequate
16 | IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004
OceanoPacifico
Loreto
Brasil
Chile
ColombiaEcuador
Fig. 5. Alto Amazonas province, Peru.
A great promise of telemedicinehas been to help isolated orscattered populations gain accessto health services.
1The remaining sites could not be visited due to security considerations or adverse climatic conditions.
IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004 | 17
communication system, 91.7%affirmed that sharing vehicleswould be more efficient.88.9% considered decreasingthe number of trips desirable.
We can conclude that communi-cation deficiencies seriously affectsuccessful coordination of activities,sharing of information, and ongoingeducation/training of health profes-sionals, thereby diminishing the effi-ciency of the healthcare system.
Restrictions Imposed by theSituation in Alto AmazonasThe use of a communication systemseems an obvious solution for thesituation described, but in order toachieve long-term viability, the situ-ation in rural areas of developingcountries has to be considered:
■ There is no access to electrici-ty in most rural villages (inrural areas of Alto Amazonassix towns have electricity, andthose only 4 hours a day).
■ Rural areas have limited or nopublic telecommunication infra-structure and they are not includ-ed in the midterm expansionplans of the operator companies.
■ Rural health establishments havelimited financial resources tofund expensive infrastructureand, more importantly, the oper-ating costs.
■ Maintenance costs of any sys-tem are very high due to thelong distances between estab-lishments.
■ There are few well-trainedcandidates for the manage-ment, maintenance, and repairof computer and telecommu-nication systems.
■ The cost of current telecom-munication systems on themarket is too high to become asystematic solution for all therural areas of a country (e.g.,the Peruvian MINSA hasmore than 5500 primaryhealth establishments withouta telecommunication system).
■ No information systems suit-ed to the real needs and capa-bilities of rural health person-nel in Latin America arecurrently available on themarket.
The EHAS ProposalConsidering all the previous con-straints, the EHAS program workson research and development ofappropriate telecommunication sys-tems and telemedicine servicesdesigned to solve the needs of ruralhealth personnel in developingcountries. The partners of the pro-gram in Spain are the GBT-UPMand ISF, and their counterparts inPeru are the Catholic University
(PUCP) and the Cayetano HerediaUniversity (UPCH). This multidis-ciplinary team works in two mainlines of action: development anddeployment of “EHAS technology,”and development and deployment of“EHAS services.”
Accessing Electronic Mailthrough VHF RadioThe Biomedical Engineering andTelemedicine Group of the UPM
and the Electronic and ElectricitySection of the PUCP centered theirwork on developing an access sys-tem to electronic mail for townswithout a telephone. The developedsystem’s main feature was: lowinfrastructure cost and especiallylow operating cost. The rest of thespecifications are:
■ VHF transceivers are used forvoice and data (email) com-munications within a healthmicronet. This system has nooperating cost.
■ HPs are endowed with VHFtransceiver, laptop, lightingsystem, and solar poweredsystem with a minimum of
five days' autonomy. (Fig. 7and Fig. 8).
■ The low consumption emailserver (located at the HC)stores the email messages ofthe health micronet and for-wards them to the Internetthrough five telephone callsevery day (Fig. 8) optimizingtelephone costs, which areshared by all the sites belong-ing to the micronet. In order to
Fig. 6. Map of the health network of Huallaga (Alto Amazonas province, Peru).

18 | IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004
simplify the network topology,the Peruvian government col-laborated with the project byinstalling 7 telephone lines.
■ Server main power is providedthrough a battery charger (Fig.1 and Fig. 9), taking advantageof the four hours of electricityin the capital district and opti-mizing the battery load.
■ A central server in Lima (per-manently connected to the
Internet) is the connectionbetween the EHAS networkand the Internet. When anemail comes from the Internet,the central server stores it tem-porally until the followingtelephone connection with theserver at the HC. To increasethe robustness of the wholesystem, a second server, locat-ed at the MINSA headquar-ters, is used.
To be able to use the traditionale-mail protocols (POP-3 andSMTP) and in order to use standardemail software clients, an open-source based application has beendesigned. This software is a localproxy of the server services, so thatthe email clients must be configuredas having local servers. The proxymultiplexes the connections, com-presses and encrypts them, and tun-nels them through the AX.25 con-nection.2 Using 9600 bps modemsand a standard 12.5 kHz channel, itis capable of transferring email mes-sages at an average rate of 17 Kbpsof real data.
The server at the HC is a robust,compact and low consumptionembedded computer with hard disk,telephone and radio modems, Ether-net, VHF transceiver, and controlcircuits. It has neither keyboard norscreen and works with a Linux basedoperating system (GNU/ Debian dis-tribution). Any number of local com-puters can be connected to it throughan Ethernet network, and otherremote ones by radio links.
This server has a system toorderly shut down services and thehard disk when an imminent powerfailure is detected, automaticallyrebooting all the system when ener-gy returns. Even so, to prevent pos-sible uncontrolled failures, a trans-actional files system has beeninstalled (ReiserFS).
In addition to the standard email
services (POP-3 and SMTP), a com-plementary program to that used inthe clients' is running in the server,demultiplexing, decrypting, anddecompressing the radio connec-tions. Email exchange with the out-side through the telephone line usesthe UUCP protocol, appropriate forintermittent connections. It uses theTCP transport through an InternetService Provider at the cost of alocal phone call.
The Linux kernel within theserver has been modified to allowDemand Assigned Multiple Access(DAMA) instead of CSMA, used bystandard AX.25. Thanks to that,each station does not need to see theothers, allowing smaller towers andless power, reducing the costs of thewhole system.
Special attention has been paid tomaintenance through local securitybackups for all hard disks and aremote maintenance system to accessall the computers by radio links.
Telemedicine Services forRural Health PersonnelThe Alexander Von Humbolt Insti-tute of Tropical Medicine from theUPCH works along with ISF in thedevelopment and deployment of ser-vices centered on the needs detected:distance training and remote accessto health information. Services thathave been structured in three cate-gories of “EHAS services”:
■ Distance training. Based onan education constructivistmodel,3 and taking intoaccount the principal trainingdeficiencies of health person-nel, we have developed twelveeight-credit courses, designedwith local MINSA managersresponsible of continuoustraining and centered on theprevalent diseases of ruralareas: childhood and maternalhealth, diarrhea, infectious dis-
Fig. 7. Infirmary technician using theVHF system for voice and data (email)communication.
Fig. 8. Solar modules and communica-tion tower in the HP of Lago Cuipari. 2AX.25 is a data communication protocol designed for semi-duplex radio communications.
3This model assumes that the education program will be successful only if it deals with con-tents that can be integrated in the daily work.

IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004 | 19
eases, nutrition, etc. Courses,sent through email, are devel-oped in HTML with JavaScriptto allow offline interactionwith the trainees. They alsohave a system for self-exami-nation and remote assessment.Other comple-mentary trainingunits are also provided, such as“the question of the day”: aclinically focused questionwhose answer is provided thefollowing day.
■ Electronic publications.“Sanicho” magazine is editedby UPCH to provide an infor-mal forum for the Alto Ama-zonas health personnel. Itincludes relevant news andevents to reduce the feeling ofisolation experienced by therural health professionals.
■ Access to experts and healthinformation. This kind of ser-vice allows a mediated accessto remote data bases and mag-azines related to health. TheEHAS program uses the ideaof “information access facili-tators.” Health personnel sendan email to EHAS requestinginformation, documents ormagazines. Facilitators lookfor material in local andremote databases, in maga-zines or from experts at theUPCH. Finally, they preparethe information to be sent backto rural personnel via email.
First EHAS Pilot Experiencein the FieldThe first pilot experience has takenplace in the health network of Hual-laga in Alto Amazonas, Peru. Thir-tynine EHAS telecommunicationsystems have been deployed. It con-sists of 7 email servers and 32 clientsystems. There is one server in theprovincial Hospital at Yurimaguasand six in the HCs of Shucushyacu,Lagunas, Santa Cruz, Pampaher-mosa, Jeberos, and Balsapuerto.Clients are distributed over these
seven health micronets as follows:eight depending on Yurimaguas,five on Shucushyacu, seven on Bal-sapuerto, five on Lagunas, four onSta. Cruz, two on Pampahermosaand one on Jeberos.
The provincial Hospital ofYurimaguas had a significant partic-ipation on the selection of the HCand HP involved as well as on thedesign of the hierarchical features ofthe communication network. To
encourage local appropriation, or afeeling of ownership, many institu-tions (province government, localauthorities and the recipients com-munities) were involved in the pro-ject through active contributions onsome deployment activities, such astransportation of experts, equip-ment, and materials, construction ofthe tower foundation, etc.
Users were trained on preventivemaintenance, operation of the com-munication system, and use of thecomputer (hardware and software).An adult training method was usedin the two 50-hour courses each userreceived. During the project twolocal technicians were trained innetwork maintenance and theprovince Hospital received supporton how to develop a maintenancesystem: procedures, equipmentreplacement, and economic provi-sions. Finally, managers of each
department at the province Hospitalreceived support on how to changetheir traditional procedures to newones in order to better benefit fromthe new communication system.
In order to make the technologyuseful for the organizations, wehave to adapt the organization to thetechnology, and also adapt the tech-nology to the organization. Theactions we took on the social level(local participation, users and tech-
nician training, maintenance proce-dures and organizational change)gave those results, better matchingthe technology and organization inboth directions: from technology toorganization, and from organizationto technology.
The network came into operationin September 2001 and two impactevaluations were programmed atmedium and long term (9 and 24months, respectively). These studiesare centered on measuring theimpact of EHAS systems (technolo-gy and services) on the health of thecommunity, as well as the healthpersonnel and health system. Theevaluation was made over four mainlines of inquiry [9]: the impact onthe health of patients, the impact onthe health attention process, the eco-nomic impact on the various partic-ipants, and the impact on the acces-sibility to a quality health service.
Fig. 9. Battery pack in the HC of Shucushyacu.

Impact of the Pilot Project(Medium Term)
Starting in May 2002, technical fea-sibility was evaluated by means of81 precisely defined indicators. Rel-evant information was compiled bydocumental review, direct observa-tion, focus groups and, most impor-tantly, questionnaire-driven inter-views of the 32 managers of the 39sites in the Alto Amazonas.
We present the main resultsgrouped into five categories: qualityof the system, improvement inurgent evacuation of patients,improvement in diagnosis and treat-ment capacity, improvement in epi-demiological surveillance, and cost-benefit study.
■ Quality of the system. Thesystem is highly used (100%frequently used the radio,71.4% the email, and 86.7%used the PC) and has a goodusability (radio system is easyto use for 100%, PC for 77%,and email for 93%). The voicesystem has a reliability of 97%and email 90%. The systemhas a good acceptabilityamong users and managers:100% think the system allowsbetter coordination, 93% thinkthe system allows them to bet-ter do their work and 80%
think the task load hasdecreased.
■ Improvement in emergencyevacuation of patients. Thefirst and main impact was pro-duced in this area. In 9 months,237 urgent evacuations werecarried out in the 39 establish-ments covered in the project. In100% of the evacuations thecommunication system wasused to communicate thepatients’ evacuation in order toprepare their reception, hithertoimpossible to achieve. In 64%of the cases the communicationsystem enabled the use of vehi-cles from other establishments,reducing the mean timeemployed for evacuation from8.61 hours to 5.17 hours (60%reduction). The use of the com-munication system has beencrucial in saving 60 patients'lives (25.3% of the cases).
■ Improvement in diagnosisand treatment capacity. Atpresent, 93.3% of the healthstaff covered by the projectconsider it fast and easy tomake consultations. Beforethe project, 93.8% of the peo-ple thought it was impossibleor very difficult. There havebeen 391 diagnosis-relatedquestions (10.06 per establish-ment) and 254 about treatment(6.52 per establishment).96.7% of those questions weresatisfactorily answered. In90% of the cases, questionswere asked while the patientwas in the establishment. Inmost of the cases, questionsare asked in real time over theradio, instead of using email.
The EHAS system has beenuseful for distance training; 5courses have been imparted(malaria, dengue, tuberculo-sis, breast breeding, and firstaid) and the participants eval-uated them with a score of16.95 / 20. 95.2% of inter-viewed people declared thatthe EHAS system was appro-
priate for training rural healthpersonnel.
■ Improvement in epidemio-logical surveillance. TheEHAS system has proved tobe effective in improvingthe epidemiological surveil-lance system in the Balsa-puerto health micronet (oneof the most isolated areas inAlto Amazonas), by reduc-ing by a quarter the numberof trips made to sendreports. Twice the numberof health establishments arenow reporting weekly, com-pared to before the EHASsystem. In 60% of the casesthe PC has been useful infilling in reports, allowing areduction in the monthlytime devoted to preparingreports from 20 hours to 13hours (35% reduction). Ma-laria detection time wasreduced by half.
■ Cost-benefit study. Theinfrastructure and set-upcosts per establishment cometo US$4195, and the estimat-ed cost of the telephone bill(seven telephone lines sharedby the 39 establishments)plus the system's mainte-nance and repair is US$704 /month for the entire commu-nication system. The totalcost of the system will berecovered by the savings gen-erated in 2.5 years (Fig. 10).In this forecast, we are onlyconsidering the savings ontravel (US$1718 monthly)and on patient evacuation(US$4230 monthly). Howev-er, if we also consider theindirect benefits, breakevenwill be reached in 13 months.The indirect benefits includethe increased productivity ofhealth staff due to reductionin travel and office tasks, andthe productivity increase ofpatients and relatives due tothe reduction in patient evac-uations.
20 | IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004
Fig. 10. Cost-benefit analysis usingonly the direct tangible benefits.
250
200costs
31
12 24 36 48 60months
directtangiblebenefits
150
100
xUS $1,000

Solving Efficacy andEfficiency Problems To the best of our knowledge, thisstudy is the first feasibility andimpact analysis of a rural telemedi-cine project for a developing coun-try that includes a large sample ofisolated communities (39 in thesame province) using radio-basedvoice and data (electronic mail)communication technologies.
This project has clearly demon-strated, supported by convincingstatistical evidence (to higher thana 95% degree of statistical signifi-cance in all cases), that the use oftechnologies appropriate to theavailable local resources (easy touse, robust, and with low operatingcosts) solves some of the importantefficacy and efficiency problems atthe rural primary healthcare level.It does so by improving the speedof resolution and diagnostic capac-ity of the health sites, by speedingup the patient evacuation system,by enhancing the efficiency of epi-demiological surveillance mecha-nisms, by facilitating pharmaceuti-cal deliveries, and by reducing thewidespread sense of isolation, bothprofessional and personal, felt bythe rural health personnel. The fea-sibility and sustainability of theVHF radio communication solu-tions provided to implement ruraltelemedicine systems in developingcountries has also been proved, thisbeing a conclusion that has notbeen demonstrated with othersatellite-based solutions. Theworking methodology used in theproject has also confirmed thehypothesis that only with participa-tive implementation programs,using solutions derived from theneeds and constraints of the targetcommunities, and not technology-driven, is it possible to achieve theglobal acceptance of all usersinvolved: administrators, healthprofessionals, and patients, as wellas the integration of a ruraltelemedicine system within thelocal health institutions.
Results obtained are intended to
demonstrate to the Health Ministriesof the region that the solution pro-posed, and its systems and services,is within the reach of most healthrural centers. There are more power-ful alternative technologies, but theydo not respond to the priorities of therural sector demands and, more crit-ically, they can never provide sus-tainable solutions, taking intoaccount the limitations of the devel-oping countries' health systems.
Companies, Public Administra-tions, and R+D centers have tounderstand that the massive implan-tation of telemedicine and telecom-
munications in isolated rural areasrequires a “two-way” approach. Inone way, the technology has to beadequate to the user context: localeconomic resources, human factorsand knowledge, cultural considera-tions, and energy considerations. Inthe other way, a natural interfacemust be provided between technol-ogy and the institutions: adequatetraining of the users and of mainte-nance personnel, and appropriatelevels of motivation and tools so theadministrative bodies may success-fully achieve the organizationalchanges required.
The EHAS experience demon-strates to health program fundingbodies that it is possible to improvethe efficiency of the isolated ruralsystems by means of systems andservices such as those we proposehere, based on low complexity andlow cost technology, as well asappropriate methodologies to sup-port the technological transfer.
Expansion of the EHASProgram Following the initial results of theimpact evaluation of Alto Ama-
zonas, the EHAS program is consid-ering five other pilot projects: twonew areas in Peru (Marañón networkin the Loreto region and Quispi-canchi-Acomayo health network inthe Cusco region); two more inColombia (the indigenous govern-ment of Guambía and the Munici-palities of Silvia, Jambaló, Alma-guer, Piamonte, Santa Rosa, and SanSebastián, all in the department ofCauca); and one more in Cuba, inthe province of Guantánamo.
One of the most importantresults of this program is the signif-icant North-South and South-South
collaboration in the telecommunica-tions and health sectors betweenuniversities, research centers, and anongovernmental organization withthe aim of developing solutions forrural health systems.
The new projects will test newtools created in EHAS laboratories,such as an electronic mail systemover HF radio, or a low orbit satel-lite mail gateway, both suited tozones with complicated orography,or a rural telemedicine system usingIEEE 802.11b for carrying media-rich data.
AcknowledgmentThe EHAS program has been possi-ble thanks to the financial support ofthe Spanish Agency for Internation-al Cooperation (AECI), the SpanishInterministerial Commission forScience and Technology (CICYT),the Latin American Program forScience and Technology for Devel-opment (CYTED), the SupervisoryOrganism for Private Investments inTelecommunication in Peru (OSIP-TEL), the InfoDev program, theCommittee for Solidarity andDevelopment of the UPM, the
IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004 | 21
There is almost no access toelectricity in most rural villages.

Council of Madrid, the SpanishAssociation of Engineers of theICAI and the Official Association ofIndustrial Engineers of Spain (COI-IM). The authors also want toacknowledge the work of the per-sonnel and volunteers of the NGOEngineering Without Frontiers, theworkers and managers of the Peru-vian Ministry of Health in Lima andAlto Amazonas, and the personnelof the Peruvian Ministry of Com-munications. A special mention forthe workers and managers of thePeruvian partners: UniversidadCatólica and Universidad CayetanoHeredia for their enormous effort.
Author InformationAndrés Martínez was with theGrupo de Bioingeniería y Telemed-icina, Universidad Politécnica deMadrid, Madrid, Spain, currentlyon leave at the Universidad Carlos
III de Madrid. Email: [email protected]. Valentín Villarroeland Francisco del Pozo are with theGrupo de Bioingeniería y Telemed-icina, Universidad Politécnica deMadrid, Madrid, Spain. Email:[email protected] and [email protected]. Joaquín Seoaneis with the Dpto de IngenieríaTelemática, Universidad Politécni-ca de Madrid, Madrid, Spain.Email: [email protected].
References[1] M.J. Field, Telemedicine, A Guide to Assess-ing Telecommunications in Health Care. Wash-ington, DC: National Academy Press, 1996.[2] J.C. Kyedar, Ed.,“Special Issue: Successstories in Telemedicine: Some empirical evi-dence,” Telemedicine J., vol. 9, no. 1, 2003. [3] R. Wootton, “The possible use of telemed-icine in developing countries,” J. Telemedicineand Telecare, vol. 3, pp. 23-26, 1997.[4] D. Wright D, “Telemedicine and developingcountries: A report of Study Group 2 of the ITUDevelopment Sector,” J. Telemedicine and Tele-
care, London, vol. 4, Suppl. 2, pp.1-85, 1997.[5] R.J. Rodrigues, C. Crawford, S. Koss, and M.McDonald, Telecommunitations in Health andHealthcare for Latin America and theCaribbean: Preliminary Report on an ExpertConsultation Meeting, PAHO: Health ServicesInformation System Program, Washington, DC,1998.[6] WHO (World Health Organization), [online] Telehealth and Telemedicine will hence-forth be part of the strategy for Health-for-All,press release, World Health Organization,1998, <http://www.who.org/inf-pr-1997/en/pr97-98.html>; accessed Feb. 27, 2002.[7] M. Sosa-Iudicissa, J. Levett, S. Mandil,and P.F. Beales, Eds., Health, InformationSociety and Developing Countries. Studies inHealth Technology and Informatics, vol. 23,European Commission DG XIII and WHO.Amsterdam, The Netherlands: IOSPress/Ohmsha, 1995.[8] N. Pakenham-Walsh, C. Priestley, R.Smith, “Meeting the information needs ofhealth workers in developing countries,”British Medical J., vol. 314, p. 90, 1997.[9] A. Martínez et al., Bases metodológicaspara evaluar la viabilidad y el impacto deproyectos de Telemedicina, OrganizaciónPanamericana de la Salud. Washington, DC:Oficina Regional de la Organización Mundialde la Salud, 2001.
22 | IEEE TECHNOLOGY AND SOCIETY MAGAZINE | SUMMER 2004
Call For Papers
Technology For Life:North Carolina Symposium
on Biotechnology and Bioinformatics
Research Triangle Park,North Carolina USA
October 13-15, 2004
http://ewh.ieee.org/cmte/tech4life
Technology for Life - NC Symposium on Biotechnology and Bioinformatics, sponsored by the Institute of Electrical and Electronics Engineers (IEEE),
North Carolina State University, and Duke University Medical Center, will be held October 13 to 15, 2004 in Research Triangle Park, NC, USA.
We seek original papers on bioinformatics, healthcare informatics, technology transfer in the biotechnology industry, and the impact of biotechnology on society.
For registration information and our Call For Papers, visit our website: http://ewh.ieee.org/cmte/tech4life.
We welcome you to North Carolina in Fall 2004.