s. amh in pcos research insights beyond a …. amh in pcos research insights beyond a diagnostic...
TRANSCRIPT

S. AMH in PCOS
Research Insights beyond a Diagnostic Marker
Dr. Anushree D. Patil, MD. DGO
Scientist - D
National Institute for Research in Reproductive Health
(Indian Council of Medical Research) (Dr. Anushree Patil, Dr. Shahina Begum, Dr. Beena Joshi)

Multidisciplinary PCOS Clinic at NIRRH
Gynaecologist Consultation Community Activities
Counseling on Nutrition and PCOS Yoga Session

Anti Mullerian Hormone
Anti-Müllerian hormone (AMH) is a
homodimeric glycoprotein linked by disulfide
bonds and a molecular weight of 140kDa.
The hormone belongs to the Transforming
Growth Factor-β (TGF-β) superfamily
The gene encoding AMH is located in the short
arm of chromosome 19
AMH plays an important role in male sex
differentiation as its production by the
embryonic testes induces the regression of
Mullerian ducts
AMH action is exerted through two receptors:
type I receptor (AMHRI) and type II receptor
(AMHRII) which are present on the AMH
target-organs (gonads and Mullerιan ducts)

Specific Actions of AMH in Human Ovary
AMH is produced by the granulosa cells of small growing follicles
In female neonates, AMH is virtually undetectable but increases gradually until pubertyand remains relatively stable thereafter and throughout the reproductive period
Inhibits initial follicle recruitment
Inhibits FSH-dependent growth and selection of pre antral and small antral follicles.
AMH remains highly expressed in cumulus cells of mature follicles.
AMH has inhibitory effect on FSH-induced CYP19a1 expression leading to reducedestradiol (E2) levels
Dewailly, D., et al., Hum Reprod Update, 2014

Two Cell Two Gonadotropin Theory

AMH: Clinical Utility
Interpretation AMH Range (ng/ml)
High Above 4.0
Normal 1.5 -4.0
Low Normal 1.0-1.5
Low 0.5-1.0
Diagnostic Marker
Ovarian Reserve
Follicular Fluid Levels
Correlate
with Pregnancy rate
Upcoming Diagnostic
Marker
For PCOS
Prognostic Marker
For predicting ovarian
response in COH
Tumor Marker
For Granulosa Cell
Tumors
Predictive Marker
For OHSS

AMH in PCOS AMH production in PCOS granulosa cells is increased by 75%*
AMH excess has an essential role in the process of follicular arrest
AMH may be used as a marker of ovarian follicle impairment inPCOS
Serum and follicular AMH levels are higher in PCOS**
Serum AMH values could be useful particularly in cases in which thetransvaginal ultrasound examination is not feasible***
Though values are higher in adolescents, not a predictor of PCOS
Age related decline has slower reduction rate of s. AMH
Levels lower in obese women with PCOS
*Pellat et al.; 2007. J Clin Endocrinol Metab 2007
**Fallat ME et al.; Fertil Steril 1997
***Pigny P et al.; J Clin Endocrinol Metab 2006

AMH in PCOS
AMH independently and positively correlated with LH,
testosterone, androstendione and free androgen index (FAI)
values and the number of small follicles*
Differences in AMH concentrations between four phenotypic
groups of PCOS reflected the severity of the syndrome
A correlation between AMH levels and HOMA-IR values has
not been confirmed in studies
Significant positive correlation between AMH levels and AGEs
in normal weight women with PCOS**
* Laven JS et al.; J Clin Endocrinol Metab 2004
**Diamanti-Kandarakis E et al.; Eur J Endocrinol 2009

Objective
To study the correlation of AMH among PCOS women with
Hormonal profile
Biochemical parameters
Anthropometric measurements
Body mass composition

Materials and Methods
Study design: Clinic based observational cross sectional study
Study sites: NIRRH Multidisciplinary PCOS Clinic
Study Population: Women diagnosed with PCOS using Rotterdam criteria
Selection Criteria
Inclusion criteria (2 out of 3)
Anovulation
Hyperandrogenism, clinical or biochemical
USG evidence of PCO
Exclusion criteria
Not willing for blood collection
On oral contraceptive pills
Study Duration: One Year

Investigations
• Hormonal
Hormonal Biochemical Ultrasound
FSH FBS USG pelvis for PCOS and endometrial
thickness
LH PGBS (post 75g) USG abdomen for Non Alcoholic Fatty
Liver (NAFL) and cholelithiasis
TSH, Free T4 Lipid profile
PRL LFT (only in NAFLD)
S. Testosterone Calcium
SHBG Hb CBC (routine)
17-OHP CRP
Insulin fasting
Insulin post
glucose
25(OH)D
AMH
Free Androgen Index & HOMAIR were calculated

64
9.926 4 4 6 6 6.53
0
10
20
30
40
50
60
70
6.3
27
11.6
55.2
0
10
20
30
40
50
60
< 19 19.1-23 23.1-24.9 Obese 25 and above
Per
cen
t
More than 0.8, 70%
less than 0.8,30%
More than 0.8 less than 0.8
Body Mass Index (n=100 PCOS Women) Waist Hip Ratio (n=100 PCOS women)
PCOS at NIRRH Infertility Clinic (n=383)
PCOS: NIRRH Data

Mean Age Hormonal and Biochemical parameters
(n=55)
Mean (±SD)
Age 26.33 years 5.088
LH 10.28 mIU /ml 6.28
FSH 06.63 mIU /ml 1.34
S. Testosterone 50.77 ng/dl 20.33
SHBG 33.63 nmol/ 18.02
FAI 06.59 04.45
HOMAIR 04.13 02.25
25(OH)D 12.77 ng/ml 07.96
AMH 07.96 ng/ml 04.70

Correlation between AMH and Age
Age Group n Mean AMH (±SD)
15-20 8 9.1 (5.4)
20-30 37 8.4 (4.8)
30-40 17 6.5 (4.8)
No significant difference was found
in mean AMH levels among age
groups
ANOVA, p= 0.35
0
2
4
6
8
10
12
14
16
18
20
10 15 20 25 30 35 40A
MH
val
ue
Age
Inverse relationship
between age and AMH
Correlation (r)= -0.14, p=0.27

Cut off Values of AMH for Diagnosis of PCOS
Author Year Cut off
level
pmol/ml
Sensitivity
(%)
Specificity
(%)
Iliodromiti 2016 33.6 82 79
Saikumar 2013 23.8 98 93
Casadei 2013 33 95 95
Dewailley 2011 35.7 92 97
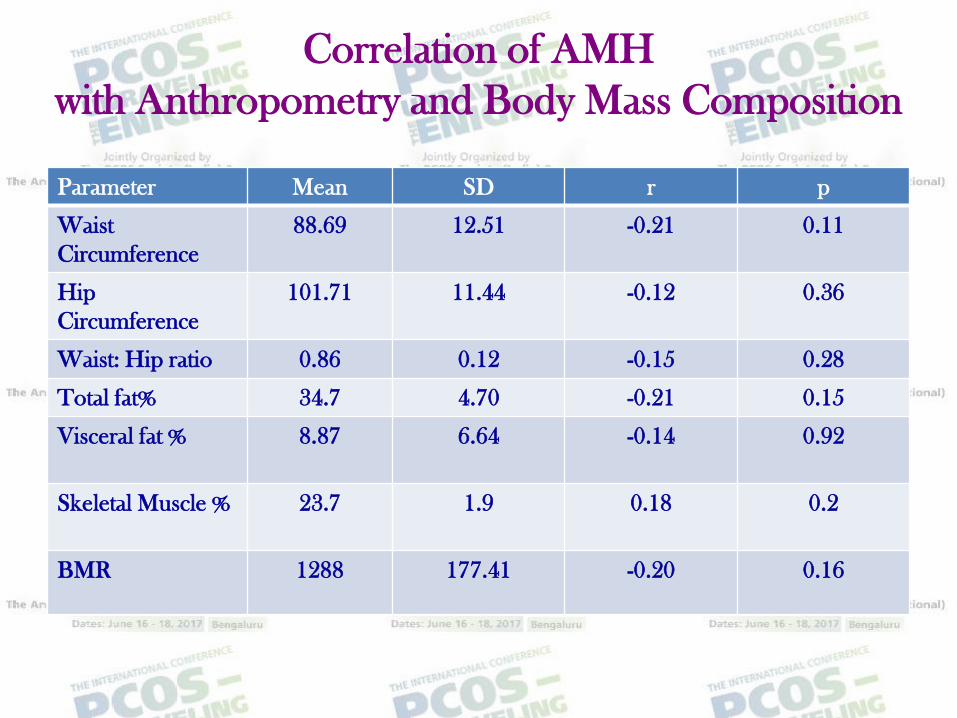
Correlation of AMH
with Anthropometry and Body Mass Composition
Parameter Mean SD r p
Waist
Circumference
88.69 12.51 -0.21 0.11
Hip
Circumference
101.71 11.44 -0.12 0.36
Waist: Hip ratio 0.86 0.12 -0.15 0.28
Total fat% 34.7 4.70 -0.21 0.15
Visceral fat % 8.87 6.64 -0.14 0.92
Skeletal Muscle % 23.7 1.9 0.18 0.2
BMR 1288 177.41 -0.20 0.16

Correlation between AMH and BMI
BMI Category n Mean AMH (SD)
<18 Underweight 1 6
18-23 Normal 13 9.9 (5.2)
23-25 Overweight 7 10.2 (5.3)
>25 Obese 34 7.2 (3.9)0
2
4
6
8
10
12
14
16
18
20
10 15 20 25 30 35 40 45
AM
H v
alu
e
BMI
r= -0.23, p=0.09
Difference was not statistically significant with BMI

Correlation of AMH
with Hormonal Biochemical Parameters
Variable r p value
LH 268 0.03*
FSH -0.14 0.24
s. Testosterone 0.28 0.02*
SHBG 0.8 0.52
FAI 0.147 0.293
HOMAIR -0.33 0.016*
25(OH)D 0.265 0.03*
Pearson Correlation applied

S. AMH and HOMAIR
Category
of Insulin
Resistance
HOMAIR n % Mean
AMH
ng/ml
SD
Normal
IR
<3 17 30.9 8.6 3.45
Moderate
IR
3-5 25 45.5 9.66 5.37
Severe IR >5 13 23.6 5.11 2.09

Limitations
Small sample size
Comparison with healthy controls required

Results
Inverse correlation with age
Positive correlation with LH and s. Testosterone
Negative correlation with HOMAIR
Conclusion
Beyond a diagnostic marker, AMH may have a
significant role in the hyperandrogenemia of PCOS

Clinical Implication: Monitoring Treatment Response
Contraceptives containing 35mg of ethynylestradiol and 2mg ofcyproterone acetate cause a significant suppression of gonadotropins andtestosterone levels, a reduction in the number of ovarian small follicles aswell as a significant reduction in AMH levels
Treatment of obese PCOS women with metformin resulted in thereduction of androgens and AMH levels, without any significant decreasein follicle number
On the other hand, gonadotropin-releasing hormone (GnRH) agonists donot seem to affect AMH concentrations
Panidis D et al, 2010 Gynecol Endocrinol 2010. Fleming R, Fertil Steril 2005
Piltonen Hum Reprod 2005

Novel Role of AMH in GnRH neuron excitability
AMH-dependent regulation of GnRH release could be involved in the pathophysiology of
fertility and could hold therapeutic potential for treating PCOS.
Irene Cimino, Nature Communications, Jan 2016

Future Directions
Standard cut off level for AMH level for
diagnosing PCOS needs to be established
Threshold for PCOS diagnosis may need to be
modified through the life span
Studies with large sample size for use of AMH
levels to diagnose PCOS in adolescents

Thank You!

• Finally, the• 2013 Endocrine Society guidelines• do not include a recommendation• for using AMH measurement as a• routine diagnostic tool for PCOS.3• Although AMH level and oligoanovulation• are correlated, • AMH• has not been proven to be an acceptable• indicator of ovulatory• dysfunction or hyper andro -• genism.23 Hence, • AMH level, if• used, should be combined with• other laboratory or clinical measures• of hyperandrogenism and/or• ovulatory dysfunction to maximize• its diagnostic sensitivity and specificity.• Furthermore, the role of• AMH is unclear in diagnosing subtypes• of PCOS,
