s treptococcus pneumoniae antigen in urine: diagnostic usefulness and impact on outcome of...
TRANSCRIPT

ORIGINAL ARTICLE
Streptococcus pneumoniae antigen in urine: Diagnosticusefulness and impact on outcome of bacteraemic pneumococcal
pneumonia in a large series of adult patients
RAFAEL ZALACAIN,1 ALBERTO CAPELASTEGUI,2 LUIS ALBERTO RUIZ,1 AMAIA BILBAO,3
AINHOA GOMEZ,1 ANE URANGA2 AND PEDRO P. ESPAÑA2
1Department of Respiratory Medicine, Cruces University Hospital, Barakaldo, 2Department of Respiratory Medicine,Galdakao-Usansolo Hospital, Galdakao, 3Research Unit, Basurto University Hospital, Research Network on Health Services
for Chronic Diseases (REDISSEC), Bilbao, Bizkaia, Spain
ABSTRACT
Background and objective: Urinary pneumococcalantigen detection provides good results in the diagno-sis of pneumococcal pneumonia but has rarely beenused in bacteraemic pneumococcal pneumonia and itis not known whether it is associated with outcome inthis type of pneumonia. Our objectives were to assessthe usefulness of an immunochromatographic tech-nique for detecting the pneumococcal antigen in urinein a large prospective study of patients with bacte-raemic pneumococcal pneumonia and explore anypotential association with outcomes.Methods: This study, carried out over 8 years,included all adult immunocompetent patients admit-ted for bacteraemic pneumococcal pneumonia. Animmunochromatographic test for the Streptococcuspneumoniae antigen in urine was performed in thefirst 24 h. The sensitivity of test was assessed andpatients were divided into two groups according to testresults to explore differences on admission and duringthe course of the illness using logistic regressionmodels.Results: Of the 350 patients with bacteraemic pneu-mococcal pneumonia included, 261 (74.6%) were posi-tive for the antigen. Patient characteristics were verysimilar on admission and differences in severity (Pneu-monia Severity Index) were not statistically significant.In the adjusted analysis, antigen-positive patients hada higher risk of intensive care unit admission, treat-ment failure and adverse outcome.Conclusions: The sensitivity of the immunochro-matographic urinary antigen test was 74.6% and posi-tive results were associated with poorer clinicaloutcome. We therefore recommend systematic use ofthis test when pneumonia is diagnosed in the emer-gency department.
Key words: bacteraemic pneumococcal pneumonia,community-acquired pneumonia, outcome, sensitivity, urinarypneumococcal antigen.
Abbreviations: BPP, bacteraemic pneumococcal pneumonia;CAP, community-acquired pneumonia; CI, confidence interval;ICT, immunochromatography; ICU, intensive care unit; IMV, inva-sive mechanical ventilation; OR, odds ratio; PSI, PneumoniaSeverity Index; UPA, urinary pneumococcal antigen.
INTRODUCTION
It is well established that Streptococcus pneumoniae isthe aetiological agent most commonly associated withcommunity-acquired pneumonia (CAP). It can,however, be very difficult to make a definitive micro-biological diagnosis. The introduction of a techniquebased on the detection of the antigen in urine byimmunochromatography (ICT) has been effective inincreasing the microbiological diagnosis.1,2 Variousauthors have demonstrated that this test has goodsensitivity (70–80%) and excellent specificity (>90%).Unfortunately, these studies have included fewpatients (never over 100) of bacteraemic pneumo-coccal pneumonia (BPP), those considered as havingdefinitive diagnoses.3–9 This type of pneumonia ischaracterized by its severity; hence, it is important toidentify a method to rapidly obtain the aetiologicaldiagnosis and thence administer a specific antibiotictreatment10 while in the emergency department.
Correspondence: Rafael Zalacain, Department of RespiratoryMedicine, Hospital de Cruces, E-48903 Barakaldo, Bizkaia, Spain.Email: [email protected]
Received 4 October 2013; invited to revise 13 November 2013,7 February and 13 March 2014; revised 13 January, 17 Februaryand 7 April 2014; accepted 27 April 2014 (Associate Editor:Yuanlin Song).
Article first published online: 26 June 2014
SUMMARY AT A GLANCE
In bacteraemic pneumococcal pneumonia pa-tients, urinary pneumococcal antigen had goodsensitivity. In addition, we present a novel finding,that in these patients, despite a similar severity asassessed by the PSI, those positive for the antigenwere associated with poorer clinical outcome.
bs_bs_banner
© 2014 Asian Pacific Society of Respirology Respirology (2014) 19, 936–943doi: 10.1111/resp.12341

In the studies focusing on BPP, the sensitivity of theurinary pneumococcal antigen (UPA) has rangedbetween 40% and 100%, and there is a lack of consen-sus over which factors influence this rate.3–9 We con-sidered that it would be interesting to study a largeseries of consecutive patients with this type of pneu-monia to investigate the sensitivity of the techniqueand potentially associated factors, as well as theimplications of having a positive result on patientoutcome.
Our study had two objectives: to assess the useful-ness of the ICT technique for detecting the UPA in alarge prospective study of patients with BPP and toexplore whether the results of the test are associatedwith outcomes in this type of pneumonia.
METHODS
Patients and study design
The study was conducted between 2002 and 2010 intwo hospitals (Cruces Hospital and Galdakao-Usansolo Hospital) in the Basque Country (Spain).Routine UPA testing was carried out on all CAPpatients within 24 h.
We prospectively included all adult patients (≥18years of age) admitted for BPP. Patients were dividedinto two groups according to their UPA test results(positive or negative). Individuals with pneumoniawere excluded if they were known to be positive forhuman immunodeficiency virus or chronicallyimmunosuppressed, as were any who had had anepisode of pneumonia in the previous 3 months andthose with hospital-acquired pneumonia.
At the initial visit, a medical history was taken andtests were requested. Patients were treated empiri-cally, in accordance with the local guidelines, with abeta-lactam antibiotic with or without a macrolide orfluoroquinolone. They were monitored daily while inhospital, and when discharged, all the correspondingdata were recorded using a computer-assisted proto-col. The ethics committees of Cruces and Galdakaohospitals approved the study.
Study variables
Data were collected on patient clinical and demo-graphic characteristics, including the number of dayssince onset of the clinical symptoms, vaccinationstatus, previous antibiotic treatment, blood testresults and X-ray findings. To assess the severity of thepneumonia on admission, we used the PneumoniaSeverity Index (PSI).11
In terms of the microbiological variables, suscep-tibility testing of S.pneumoniae according to newbreak points was performed for penicillin, ceftria-xone, erythromycin and levofloxacin.12 We assessedthe various serotypes found, grouping them intothose associated with higher (3, 6A, 6B, 9N, 19F, 19Aand 23F) and lower (1, 7F, 8, 4 and 5) mortality.13
Treatment was characterized using the followingvariables: (i) appropriate antibiotics (empirical selec-tion in accordance with the recommendations of theSpanish Thoracic Society);14 (ii) and (iii) antibiotic
treatments within the first 4 or first 8 hours afterarrival at the emergency department, respectively;(iv) duration of antibiotic treatment; (v) duration ofintravenous antibiotic treatment; and (vi) type ofantibiotics.
The course of the illness and patient outcome weredescribed using the following variables: (i) admissionto the intensive care unit (ICU); (ii) use of invasivemechanical ventilation (IMV); (iii) septic shock; (iv)treatment failure; (v) in-hospital mortality; (vi)adverse outcome; (vii) 30-day mortality; and (viii)length of hospital stay.
Definitions
BPP was defined as the presence of new pulmonaryinfiltrate on chest X-ray together with acute signs andsymptoms suggestive of lower respiratory tract infec-tion in addition to one positive blood culture forS. pneumoniae taken within 24 h of presentation tothe hospital.
Septic shock was defined as a systolic blood pres-sure < 90 mm Hg and the need for a vasopressoragent for at least 4 h, after fluid therapy.15 Treatmentwas considered to have failed when there was clinicaldeterioration with haemodynamic instability duringhospitalization, appearance or worsening of respira-tory failure, a need for mechanical ventilation,progression of the pneumonia as indicated by radio-graphic findings or the appearance of a new infec-tious focus, or persistence or reappearance of fever, ifa change in treatment was required.16 Adverseoutcome of the illness was defined as in-hospitaldeath and/or the development of shock and/or needfor mechanical ventilation.17
Microbiological tests
Two blood cultures and a UPA test were performed foreach patient within 24 h of their arrival at hospital. Weused the BinaxNOW S. pneumoniae Antigen Card(Binax, Portland, ME, USA) for testing for the UPA.3,4
This test detects the C-polysaccharide present on thecell wall of all pneumococcal strains. Urine was con-centrated 25-fold by selective ultrafiltration (PM15000, Minicon Urifil-10 Concentrator; Millipore,Bedford, MA, USA).5,6 The results were consideredqualitatively, positive or negative.
Given that all the patients had a definitive aetiologi-cal diagnosis, we did not assess the specificity butrather only the sensitivity of the UPA test using thestandard formula.
Statistical analysis
For the descriptive analysis, frequencies and percent-ages, means and standard deviations or medians andinterquartile ranges were calculated, as appropriate.Patient characteristics, the variables related to treat-ment, course of the illness and outcome were com-pared in the two groups (positive or negative UPA testresults). Qualitative variables were compared withchi-square or Fisher exact tests, and quantitativevariables with Student’s t-tests or non-parametricWilcoxon tests.
Bacteraemic pneumococcal pneumonia 937
© 2014 Asian Pacific Society of Respirology Respirology (2014) 19, 936–943

Univariate logistic regression models were used forcomparing the variables related to course andoutcome in the two groups. Then, multivariate logis-tic regression models were built, adjusting for severity(PSI score), multilobar involvement and for othervariables known to have an impact on these resultsincluding previous antibiotic treatment, use of appro-priate antibiotics and administration of antibioticswithin 8 h.18–22 The results are reported as odds ratios(ORs) and 95% confidence intervals (CIs). The lengthsof hospital stay were compared using a generalizedlinear model and logarithmic transformation giventhe skewed distribution of the data. Finally, Kaplan–Meier survival curves were constructed for in-hospitaland 30-day mortality for each group of patients, andthese were compared using the log-rank test.
Differences were considered statistically significantif P < 0.05. All the statistical analysis was performedusing SAS for Windows version 9.2 (SAS Institute,Cary, NC, USA) and S-Plus 2000 (MathSoft Inc., Cam-bridge, MA, USA).
RESULTS
We included 350 patients; UPA test was positive in 261(74.6%). Patient characteristics, clinical data and testresults are summarized in Table 1.
There were no significant differences in patientcharacteristics or the number of days since onset ofthe illness. Among antigen-positive patients, therewere higher respiratory rates, lower arterial oxygenpressure and pH levels, and a higher rate of multilobarinvolvement, but the severity measured using the PSIwas similar in the two groups (P = 0.193). No differ-ences were found regarding other clinical, laboratoryor radiological parameters studied, or in the rates ofresistance to antibiotics.
Serotypes were identified in 288 (82.3%) and wefound between-group differences, serotypes 1 and 3being those most commonly associated with negativeand positive results respectively (P = 0.006 andP = 0.014). Overall, serotypes 3, 6A, 6B, 9N, 19F, 19Aand 23F were more common in antigen-positive(36.9% vs 18.5%, P = 0.005), and serotypes 1, 7F, 8, 4and 5 in antigen-negative (49.2% vs 29.4%; P = 0.003)patients.
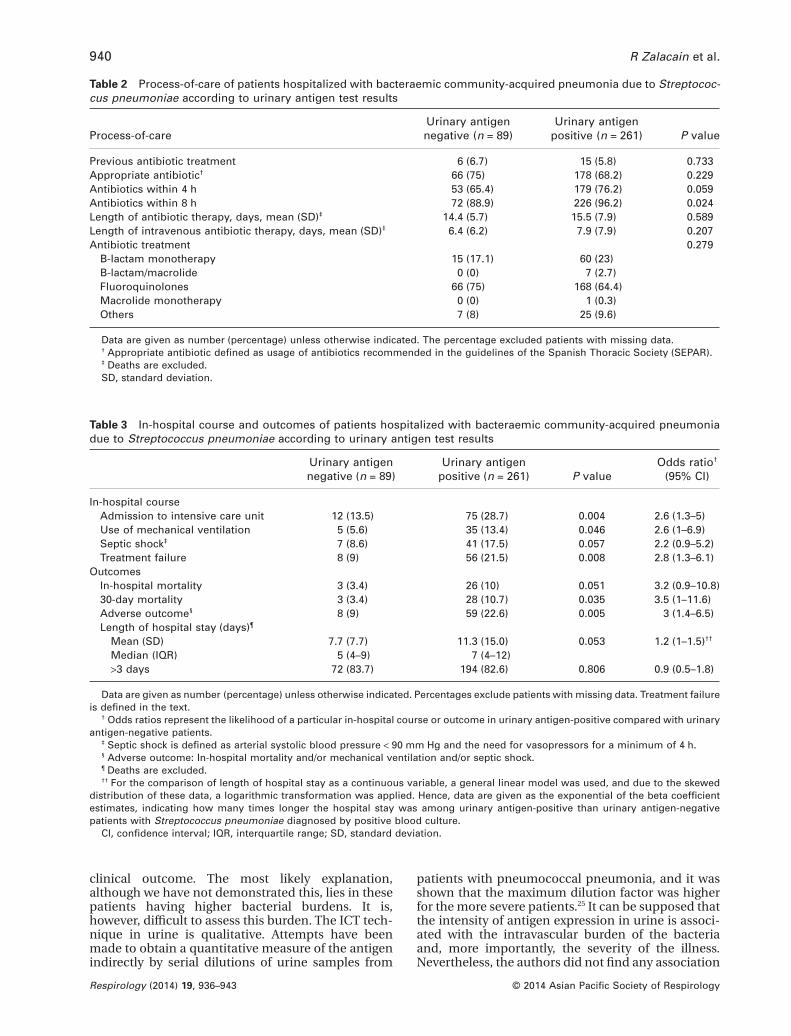
Treatments used are summarized in Table 2. Therewere no significant differences in the percentage ofpatients previously treated with antibiotics, or forwhom drugs were selected appropriately or givenwithin the first 4 h, though a higher percentage ofantigen-positive patients were started on antibioticswithin the first 8 h (P = 0.024). Most patients weretreated with fluoroquinolones and the type of antibi-otics (P = 0.279) and duration of the antibiotic treat-ments did not vary significantly.
In-hospital course and 30-day outcomes aredescribed in Table 3. Among antigen-positive pa-tients, there were higher rates of ICU admission, useof IMV, treatment failure, adverse outcome and30-day mortality. The mean length of hospital staywas similar in the two groups.
In the adjusted analysis controlling for the variableslisted in Table 4, antigen-positive patients had ahigher risk of ICU admission (OR, 2.6; 95% CI: 1.1–6;P = 0.025), treatment failure (OR, 3.2; 95% CI: 1.2–9.2;P = 0.023) and adverse outcome (OR, 3.3; 95% CI: 1.2–9.2; P = 0.023). The Kaplan–Meier survival curves forthe groups (Fig. 1) revealed differences in 30-day mor-tality (P = 0.036), but the differences in in-hospitalmortality were not significant (P = 0.062).
DISCUSSION
On the basis of our results, we can confirm that theUPA test has good sensitivity among individuals withBPP. In addition, we present a more novel finding,namely that in patients with this type of pneumoniaand with a similar severity as assessed by the PSI,those positive for the antigen tend to have a poorerclinical outcome.
To assess the sensitivity of a technique, it is essen-tial to focus on patients with a definitive diagnosissuch as those with BPP. Previously, various studiesbased on small samples of this type of patient haveobtained sensitivities ranging from 40% to 100%.3–9
Based on the largest sample of subjects reported todate, we found a sensitivity of 74.6%.
The reason why the UPA test is negative in somepatients remains unknown, though various factorshave been proposed, such as low levels of C-polysaccharide antigen and sequestration of theantigen by binding to serum antibodies in immunecomplexes, reducing urinary excretion of theantigen.23 Other possible factors include the numberof days from the onset of symptoms to diagnosis,6
previous antibiotic treatment4 and even severity.7 Inour sample, in which the test was performed withinthe first 24 h of arrival to the emergency departmentin all subjects, we found no associations with theselast three factors. A controversial issue with regards tothe sensitivity of this technique is the concentrationof urine, a procedure that allows the rate of diagnosesto be increased, although the results are variable.4,5 Inour hospitals, urine concentration is used routinely; itis easy to perform and causes only a relatively smalldelay in diagnosis.
For the first time, we report evidence that positiveUPA test results in BPP are associated with an adverseclinical outcome in hospital. We have conducted aprospective study with a large number of patients,collecting a wide range of data and adjusting the sta-tistical analysis for factors known to have an impacton the progression of this type of pneumonia.18–22 Pre-viously, just one study had found an associationbetween positive UPA test results and BPP,24 but noassociation with an adverse outcome had beenreported. Our two groups had a similar severity asassessed by the PSI. Further, the serotypes associatedwith greater mortality13 were more common amongthe antigen-positive group, and those associated witha lower mortality more common in antigen-negativeindividuals.
The question that arises is why, in patients withsimilar severity, those positive for UPA have a poorer
R Zalacain et al.938
© 2014 Asian Pacific Society of RespirologyRespirology (2014) 19, 936–943
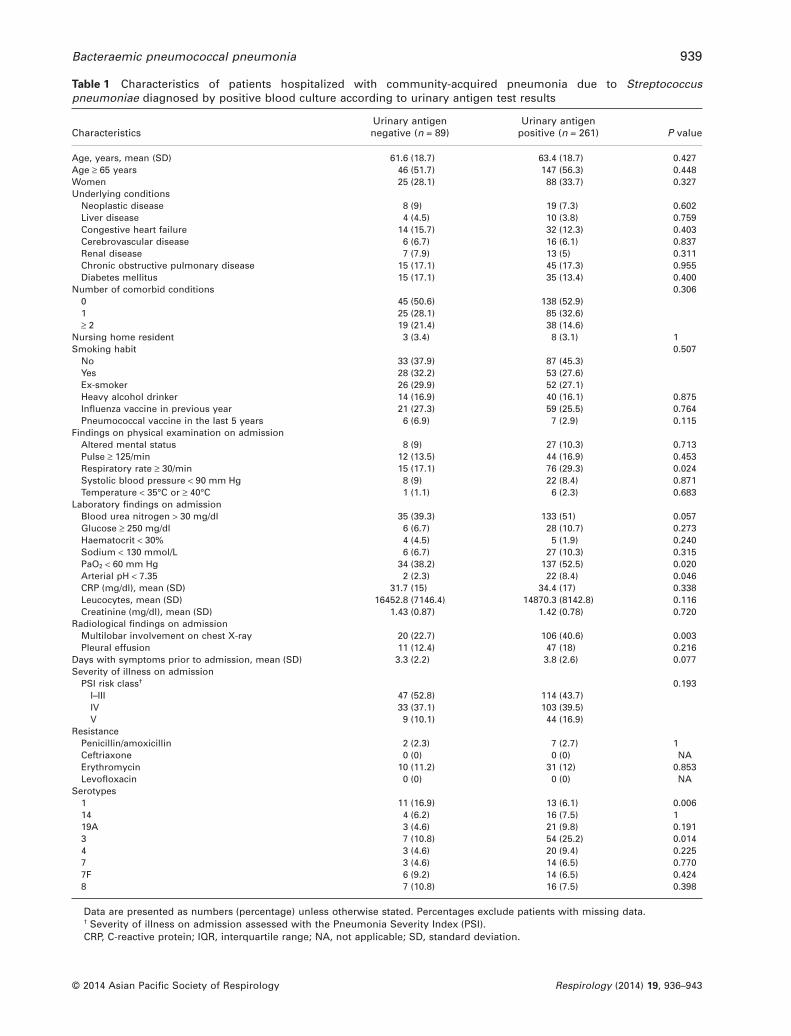
Table 1 Characteristics of patients hospitalized with community-acquired pneumonia due to Streptococcuspneumoniae diagnosed by positive blood culture according to urinary antigen test results
CharacteristicsUrinary antigennegative (n = 89)
Urinary antigenpositive (n = 261) P value
Age, years, mean (SD) 61.6 (18.7) 63.4 (18.7) 0.427Age ≥ 65 years 46 (51.7) 147 (56.3) 0.448Women 25 (28.1) 88 (33.7) 0.327Underlying conditions
Neoplastic disease 8 (9) 19 (7.3) 0.602Liver disease 4 (4.5) 10 (3.8) 0.759Congestive heart failure 14 (15.7) 32 (12.3) 0.403Cerebrovascular disease 6 (6.7) 16 (6.1) 0.837Renal disease 7 (7.9) 13 (5) 0.311Chronic obstructive pulmonary disease 15 (17.1) 45 (17.3) 0.955Diabetes mellitus 15 (17.1) 35 (13.4) 0.400
Number of comorbid conditions 0.3060 45 (50.6) 138 (52.9)1 25 (28.1) 85 (32.6)≥ 2 19 (21.4) 38 (14.6)
Nursing home resident 3 (3.4) 8 (3.1) 1Smoking habit 0.507
No 33 (37.9) 87 (45.3)Yes 28 (32.2) 53 (27.6)Ex-smoker 26 (29.9) 52 (27.1)Heavy alcohol drinker 14 (16.9) 40 (16.1) 0.875Influenza vaccine in previous year 21 (27.3) 59 (25.5) 0.764Pneumococcal vaccine in the last 5 years 6 (6.9) 7 (2.9) 0.115
Findings on physical examination on admissionAltered mental status 8 (9) 27 (10.3) 0.713Pulse ≥ 125/min 12 (13.5) 44 (16.9) 0.453Respiratory rate ≥ 30/min 15 (17.1) 76 (29.3) 0.024Systolic blood pressure < 90 mm Hg 8 (9) 22 (8.4) 0.871Temperature < 35°C or ≥ 40°C 1 (1.1) 6 (2.3) 0.683
Laboratory findings on admissionBlood urea nitrogen > 30 mg/dl 35 (39.3) 133 (51) 0.057Glucose ≥ 250 mg/dl 6 (6.7) 28 (10.7) 0.273Haematocrit < 30% 4 (4.5) 5 (1.9) 0.240Sodium < 130 mmol/L 6 (6.7) 27 (10.3) 0.315PaO2 < 60 mm Hg 34 (38.2) 137 (52.5) 0.020Arterial pH < 7.35 2 (2.3) 22 (8.4) 0.046CRP (mg/dl), mean (SD) 31.7 (15) 34.4 (17) 0.338Leucocytes, mean (SD) 16452.8 (7146.4) 14870.3 (8142.8) 0.116Creatinine (mg/dl), mean (SD) 1.43 (0.87) 1.42 (0.78) 0.720
Radiological findings on admissionMultilobar involvement on chest X-ray 20 (22.7) 106 (40.6) 0.003Pleural effusion 11 (12.4) 47 (18) 0.216
Days with symptoms prior to admission, mean (SD) 3.3 (2.2) 3.8 (2.6) 0.077Severity of illness on admission
PSI risk class† 0.193I–III 47 (52.8) 114 (43.7)IV 33 (37.1) 103 (39.5)V 9 (10.1) 44 (16.9)
ResistancePenicillin/amoxicillin 2 (2.3) 7 (2.7) 1Ceftriaxone 0 (0) 0 (0) NAErythromycin 10 (11.2) 31 (12) 0.853Levofloxacin 0 (0) 0 (0) NA
Serotypes1 11 (16.9) 13 (6.1) 0.00614 4 (6.2) 16 (7.5) 119A 3 (4.6) 21 (9.8) 0.1913 7 (10.8) 54 (25.2) 0.0144 3 (4.6) 20 (9.4) 0.2257 3 (4.6) 14 (6.5) 0.7707F 6 (9.2) 14 (6.5) 0.4248 7 (10.8) 16 (7.5) 0.398
Data are presented as numbers (percentage) unless otherwise stated. Percentages exclude patients with missing data.† Severity of illness on admission assessed with the Pneumonia Severity Index (PSI).CRP, C-reactive protein; IQR, interquartile range; NA, not applicable; SD, standard deviation.
Bacteraemic pneumococcal pneumonia 939
© 2014 Asian Pacific Society of Respirology Respirology (2014) 19, 936–943
clinical outcome. The most likely explanation,although we have not demonstrated this, lies in thesepatients having higher bacterial burdens. It is,however, difficult to assess this burden. The ICT tech-nique in urine is qualitative. Attempts have beenmade to obtain a quantitative measure of the antigenindirectly by serial dilutions of urine samples from
patients with pneumococcal pneumonia, and it wasshown that the maximum dilution factor was higherfor the more severe patients.25 It can be supposed thatthe intensity of antigen expression in urine is associ-ated with the intravascular burden of the bacteriaand, more importantly, the severity of the illness.Nevertheless, the authors did not find any association
Table 2 Process-of-care of patients hospitalized with bacteraemic community-acquired pneumonia due to Streptococ-cus pneumoniae according to urinary antigen test results
Process-of-careUrinary antigennegative (n = 89)
Urinary antigenpositive (n = 261) P value
Previous antibiotic treatment 6 (6.7) 15 (5.8) 0.733Appropriate antibiotic† 66 (75) 178 (68.2) 0.229Antibiotics within 4 h 53 (65.4) 179 (76.2) 0.059Antibiotics within 8 h 72 (88.9) 226 (96.2) 0.024Length of antibiotic therapy, days, mean (SD)‡ 14.4 (5.7) 15.5 (7.9) 0.589Length of intravenous antibiotic therapy, days, mean (SD)‡ 6.4 (6.2) 7.9 (7.9) 0.207Antibiotic treatment 0.279
B-lactam monotherapy 15 (17.1) 60 (23)B-lactam/macrolide 0 (0) 7 (2.7)Fluoroquinolones 66 (75) 168 (64.4)Macrolide monotherapy 0 (0) 1 (0.3)Others 7 (8) 25 (9.6)
Data are given as number (percentage) unless otherwise indicated. The percentage excluded patients with missing data.† Appropriate antibiotic defined as usage of antibiotics recommended in the guidelines of the Spanish Thoracic Society (SEPAR).‡ Deaths are excluded.SD, standard deviation.
Table 3 In-hospital course and outcomes of patients hospitalized with bacteraemic community-acquired pneumoniadue to Streptococcus pneumoniae according to urinary antigen test results
Urinary antigennegative (n = 89)
Urinary antigenpositive (n = 261) P value
Odds ratio†
(95% CI)
In-hospital courseAdmission to intensive care unit 12 (13.5) 75 (28.7) 0.004 2.6 (1.3–5)Use of mechanical ventilation 5 (5.6) 35 (13.4) 0.046 2.6 (1–6.9)Septic shock‡ 7 (8.6) 41 (17.5) 0.057 2.2 (0.9–5.2)Treatment failure 8 (9) 56 (21.5) 0.008 2.8 (1.3–6.1)
OutcomesIn-hospital mortality 3 (3.4) 26 (10) 0.051 3.2 (0.9–10.8)30-day mortality 3 (3.4) 28 (10.7) 0.035 3.5 (1–11.6)Adverse outcome§ 8 (9) 59 (22.6) 0.005 3 (1.4–6.5)Length of hospital stay (days)¶
Mean (SD) 7.7 (7.7) 11.3 (15.0) 0.053 1.2 (1–1.5)††
Median (IQR) 5 (4–9) 7 (4–12)>3 days 72 (83.7) 194 (82.6) 0.806 0.9 (0.5–1.8)
Data are given as number (percentage) unless otherwise indicated. Percentages exclude patients with missing data. Treatment failureis defined in the text.
† Odds ratios represent the likelihood of a particular in-hospital course or outcome in urinary antigen-positive compared with urinaryantigen-negative patients.
‡ Septic shock is defined as arterial systolic blood pressure < 90 mm Hg and the need for vasopressors for a minimum of 4 h.§ Adverse outcome: In-hospital mortality and/or mechanical ventilation and/or septic shock.¶ Deaths are excluded.†† For the comparison of length of hospital stay as a continuous variable, a general linear model was used, and due to the skewed
distribution of these data, a logarithmic transformation was applied. Hence, data are given as the exponential of the beta coefficientestimates, indicating how many times longer the hospital stay was among urinary antigen-positive than urinary antigen-negativepatients with Streptococcus pneumoniae diagnosed by positive blood culture.
CI, confidence interval; IQR, interquartile range; SD, standard deviation.
R Zalacain et al.940
© 2014 Asian Pacific Society of RespirologyRespirology (2014) 19, 936–943

with the course of the illness.25 For blood, the bestapproach to determining bacterial burden seems tobe a polymerase chain reaction-based technique fordetecting genes of S. pneumoniae.26 Rello et al., usingthe autolysin gene in 93 cases of pneumococcal pneu-monia, found an association between high bacterialburden and higher mortality, a greater risk of septicshock and need for mechanical ventilation.27 Itseems therefore plausible that a higher bacterialburden would be associated with greater urinaryexcretion of the antigen and a higher rate of positivetest results.
Secondly, it could also be supposed that antigen-positive patients would correspond to those in whichthere was a stronger inflammatory response that hasbeen associated with greater severity.28 In our study,the only indicator of inflammation considered wasC-reactive protein and the levels were similar regard-less of antigen test results.
Thirdly, impairment of renal function could influ-ence the results. A study of patients with BPP foundthat those with impaired renal function were morelikely to be antigen positive; however, as in mostcases, the cause was reversible, above all dehydration,thus the high rate of positive results could be due tothe urine being more concentrated.29 No differenceswere found regarding these renal parameters betweenour two groups.
Lastly, we should consider the presence of certainserotypes. We observed that the serotypes that havebeen associated with higher mortality were morecommonly found in the antigen-positive patients,while those associated with lower mortality weremore prevalent among patients with negativeresults.13,20 Although what the ICT technique detects isthe C polysaccharide, which is present in all theserotypes, it could be that some have lower levels ofthis polysaccharide and hence it is not detected inurine.
Table 4 Comparison between in-hospital course andoutcomes of patients hospitalized with community-acquired pneumonia due to Streptococcus pneumoniaediagnosed by positive blood culture according to urinaryantigen results: Adjusted analysis
Odds ratio(95% CI)† P value
In-hospital courseAdmission to intensive care unit 2.6 (1.1–6) 0.025Use of mechanical ventilation 3.8 (0.8–17) 0.085Septic shock‡ 1.9 (0.7–5.5) 0.223Treatment failure 3.2 (1.2–9.2) 0.023
OutcomesIn-hospital mortality 2.2 (0.6–8.6) 0.24830-day mortality 2.6 (0.7–9.8) 0.159Adverse outcome§ 3.3 (1.2−9.2) 0.023Length of hospital stay (days)¶
Continuous†† 1 (0.9–1.3) 0.652>3 days 0.7 (0.3–1.4) 0.285
† Odds ratios represent the likelihood of a particular in-hospitalcourse or outcome in urinary antigen-positive compared withurinary antigen-negative patients, adjusted for PSI, multilobarinvolvement on chest X ray, use of appropriate antibiotics, anti-biotic administration prior to hospital admission and antibioticswithin 8 h, except for mortality because there was no casewithout antibiotic within 8 h who died.
‡ Septic shock defined as arterial systolic blood pres-sure < 90 mm Hg and need for vasopressors ≥ 4 h.
§ Adverse outcome: In-hospital mortality and/or mechanicalventilation and/or septic shock.
¶ Deaths are excluded.†† For the comparison of length of hospital stay as a continu-
ous variable, a general linear model was used, and due to theskewed distribution of these data, a logarithmic transformationwas applied. Hence, data are given as the exponential of the betacoefficient estimates, indicating how many times longer the hos-pital stay was among urinary antigen-positive than urinaryantigen-negative patients with Streptococcus pneumoniae diag-nosed by positive blood culture.
CI, confidence interval.
Figure 1 Kaplan–Meier survival curves for in-hospital and 30-day mortality for urinary antigen positive and negative patients. Thelog-rank test detected statistically significant differences between the two curves for 30-mortality (P = 0.036), but not for in-hospitalmortality (P = 0.062). , urinary antigen negative; , urinary antigen positive.
Bacteraemic pneumococcal pneumonia 941
© 2014 Asian Pacific Society of Respirology Respirology (2014) 19, 936–943

The study has some limitations. Our results exclu-sively show the patients with BPP. The role of UPA asan adverse outcome marker in non-bacteraemicpatients should be explored in future studies. As bac-terial burden was not assessed, we are not ableexplore its relationship with test results or its poten-tial usefulness as a marker of severity.27 There werefew negative UPA with poor evolution which condi-tioned the statistical analysis. Further, in the multi-variate analysis, we would like to have considered useof antibiotic therapy including a macrolide,30 but werenot able to since only seven patients (2%) were giventhis treatment. It would have also been interesting toadjust for serotypes,13,20 but this was not possiblegiven the high dispersion of the data.
We conclude that the ICT technique has a sensitiv-ity of nearly 75% in cases of BPP, and is not clearlyaffected by any of the factors considered, although therole of serotypes should be explored in furtherstudies. In addition, positive UPA test patients tendedto have a poorer outcome of the illness. Given this,and consistent with recent recommendations,1,31 weadvocate the routine use of this technique in emer-gency departments, to guide the decision to start spe-cific antibiotic treatments.
REFERENCES
1 Bartlett JG. Diagnostic tests for agents of community-acquiredpneumonia. Clin. Infect. Dis. 2011; 52(Suppl. 4): S296–304.
2 Blaschke AJ. Interpreting assays for the detection of Streptococ-cus pneumoniae. Clin. Infect. Dis. 2011; 52(Suppl. 4): S331–7.
3 Domínguez J, Gali N, Blanco S, Pedroso P, Prat C, Matas L, AusinaV. Detection of Streptococcus pneumoniae antigen by a rapidimmunochromatographic assay in urine samples. Chest 2001;119: 243–9.
4 Murdoch DR, Laing RTR, Mills GD, Karalus NC, Town GI, MirrettS, Reller LB. Evaluation of a rapid immunochromatographic testfor detection of Streptococcus pneumoniae antigen in urinesamples from adults with community-acquired pneumonia. J.Clin. Microbiol. 2001; 39: 3495–8.
5 Marcos MA, Jiménez de Anta MT, de la Bellacasa JP, González J,Martínez E, García E, Mensa J, de Roux A, Torres A. Rapid urinaryantigen test for diagnosis of pneumococcal community-acquired pneumonia in adults. Eur. Respir. J. 2003; 21: 209–14.
6 Gutiérrez F, Masía M, Rodríguez JC, Ayelo A, Soldán B, Cebrián L,Mirete C, Royo G, Hidalgo AM. Evaluation of theimmunochromatographic Binax NOW assay for detection ofStreptococcus pneumoniae urinary antigen in a prospective studyof community-acquired pneumonia in Spain. Clin. Infect. Dis.2003; 36: 286–92.
7 Rosón B, Fernández-Sabé N, Carratalá J, Verdaguer R, Dorca J,Manresa F, Gudiol F. Contribution of a urinary antigen assay(Binax NOW) to the early diagnosis of pneumococcal pneumo-nia. Clin. Infect. Dis. 2004; 38: 222–6.
8 Smith MD, Sheppard CL, Hogan A, Creek M, Morris R, DanceDAB, Cartwright K. Diagnosis of Streptococcus pneumoniaeinfections in adults with bacteremia and community-acquiredpneumonia: clinical comparison of pneumococcal PCR andurinary antigen detection. J. Clin. Microbiol. 2009; 47: 1046–9.
9 Sordé R, Falcó V, Lowak M, Domingo E, Ferrer A, Burgos J, PuigM, Cabral E, Len O, Pahissa A. Current and potential usefulnessof pneumococcal urinary antigen detection in hospitalizedpatients with community-acquired pneumonia to guide antimi-crobial therapy. Arch. Intern. Med. 2011; 171: 166–72.
10 Rueda AM, Serpa JA, Matioobi M, Mushtaq M, Musher DM. Thespectrum of invasive pneumococcal disease at an adult tertiarycare hospital in the early 21st century. Medicine (Baltimore)2010; 89: 331–6.
11 Fine MJ, Auble TE, Yealy DM, Hanusa DH, Weissfeld LA, SingerDE, Coley CM, Marrie TJ, Kapoor WN. A prediction rule to iden-tify low-risk patients with community-acquired pneumonia. N.Engl. J. Med. 1997; 336: 243–50.
12 Clinical and Laboratory Standards Institute. Performance Stand-ards for Antimicrobial Susceptibility Testing: Eighteenth Informa-tional Supplement. M100-S18. CLSI, Wayne, PA, 2008.
13 Weinberge DM, Harboe ZB, Sanders EAM, Ndiritu M, KlugmanKP, Ruckinger S, Dagan R, Adeqbola R, Cutts F, Johnson HL et al.Risk of death from pneumococcal pneumonia is a stableserotype-associated property: a meta-analysis. Clin. Infect. Dis.2010; 51: 692–9.
14 Ménendez R, Torres A, Aspa J, Capelastegui A, Prat C,Rodríguez de Castro F. Community-acquired pneumonia.New guidelines of the Spanish Society of Chest Diseases andThoracic Surgery (SEPAR). Arch. Bronconeumol. 2010; 46:543–58.
15 Levy MM, Fink M, Marshall JC, Abraham E, Angus D, Cook D,Cohen J, Opal SM, Vincent JL, Ramsay G. SCCM/ESICM/ATS/SISinternational sepsis definitions conference. Crit. Care Med. 2003;31: 1250–6.
16 Menéndez R, Torres A, Zalacain R, Aspa J, Martín Villasclaras JJ,Borderías L, Benítez Moya JM, Ruiz-Manzano J,Rodríguez de Castro F, Blanquer J et al. Risk factors of treatmentfailure in community-acquired pneumonia: implications fordisease outcome. Thorax 2004; 59: 960–5.
17 España PP, Capelastegui A, Gorordo I, Esteban C, Oribe M,Ortega M, Bilbao A, Quintana JM. Development and validation ofa clinical prediction rule for severe community-acquired pneu-monia. Am. J. Respir. Crit. Care Med. 2006; 174: 1249–56.
18 Garnacho-Montero J, García-Cabrera E, Diaz-Martin A,Lepe-Jimenez JA, Iraurgui-Arcarazo P, Jiménez-Alvárez R,Revuelto-Rey J, Aznar-Martín J. Determinants of outcome inpatients with bacteraemic pneumococcal pneumonia: impor-tance of early adequate treatment. Scand. J. Infect. Dis. 2010; 42:185–92.
19 Luján M, Gallego M, Fontanals D, Mariscal D, Rello J. Prospectiveobservational study of bacteremic pneumococcal pneumonia:effect of discordant therapy on mortality. Crit. Care Med. 2004;32: 625–31.
20 García-Vidal C, Ardanuy C, Tubau F, Viasus D, Dorca J, Liñares J,Gudiol F, Carratalá J. Pneumococcal pneumonia presenting withseptic shock: host- and pathogen-related factors and outcomes.Thorax 2010; 65: 77–81.
21 Yu VL, Chiou CCC, Feldman C, Ortqvist A, Rello J, Morris AJ,Baddour LM, Luna CM, Snydman DR, Ip M et al. An interna-tional prospective study of pneumococcal bacteremia: correla-tion with in vitro resistance, antibiotics administered andclinical outcome. Clin. Infect. Dis. 2003; 37: 230–7.
22 Cilloniz C, Torres A. Understanding mortality in bacteremicpneumococcal pneumonia. J. Bras. Pneumol. 2012; 38: 419–21.
23 Boulware DR, Daley CL, Merrifield C, Hopewell PC, Janoff EN.Rapid diagnosis of pneumococcal pneumonia among HIV-infected adults with urine antigen detection. J. Infect. 2007; 55:300–9.
24 Perelló R, Miró O, Marcos MA, Almela M, Bragulat E, Sánchez M,Agustí C, Miró JM, Moreno A. Predicting bacteremic pneumoniain HIV-1-infected patients consulting the ED. Am. J. Emerg. Med.2010; 28: 454–9.
25 Tateda K, Kusano E, Matsumoto T, Kimura K, Uchida K, NakataK, Yamaguchi K. Semi-quantitative analysis of Streptococcuspneumoniae urinary antigen: kinetics of antigen titers and sever-ity of disease. Scand. J. Infect. Dis. 2006; 38: 166–71.
26 Peters RPH, de Boer RF, Schuurman T, Gierveld S, Kooistra-SmidM, van Agtmel MA, Vandenbroucke-Grauls CMJE, Persoons MCJ,Savelkoul PHM. Streptococcus pneumoniae DNA load in blood as
R Zalacain et al.942
© 2014 Asian Pacific Society of RespirologyRespirology (2014) 19, 936–943

a marker of infection in patients with community-acquiredpneumonia. J. Clin. Microbiol. 2009; 47: 3308–12.
27 Rello J, Lisboa T, Lujan M, Gallego M, Kee C, Kay I, López D,Waterer GW. Severity of pneumococcal pneumonia associatedwith genomic bacterial pneumonia. Chest 2009; 136: 832–40.
28 Ramírez P, Ferrer M, Martí V, Reyes S, Martínez R, Menéndez R,Ewig S, Torres A. Inflammatory biomarkers and prediction forintensive care unit admission in severe community-acquiredpneumonia. Crit. Care Med. 2011; 39: 2211–17.
29 Selickman J, Paxos M, File TM, Seltzern R, Bonilla H. Perfor-mance measure of urinary antigen in patients with Streptococcus
pneumoniae bacteremia. Diagn. Microbiol. Infect. Dis. 2010; 67:129–33.
30 Martínez JA, Horcajada JP, Almela M, Marco F, Soriano A, GarcíaE, Marco MA, Torres A, Mensa J. Addition of a macrolide to abeta-lactam-based empirical antibiotic regimen is associatedwith lower mortality for patients with bacteremic pneumococcalpneumonia. Clin. Infect. Dis. 2003; 36: 289–95.
31 Yu VL. A clinical solution to antimicrobial resistance incommunity-acquired pneumonia. Narrowing the spectrum ofantimicrobial therapy. Arch. Intern. Med. 2011; 171: 172–3.
Bacteraemic pneumococcal pneumonia 943
© 2014 Asian Pacific Society of Respirology Respirology (2014) 19, 936–943