s3. · web viewpharynx - 3 division: nasopharynx, oropharynx, laryngeal pharynx – same...
TRANSCRIPT

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
Chapter 39 is on your own – it should be a review of A/P. It is the normal function of the GI tract. There will be questions on the exam that come from this chapter.
Note: Blue numbers correlate to your outline. The yellow numbers are accessory system/organs and are noted in the outline.
I. Main function of GI system is supplying nutrition. Accomplished through ingestion, digestion, absorption. Elimination is final step, excreting waste products of digestion.a. 30 feet long – 4 layers: mucosa, submucosa, muscle, serosa or fibrous tissue. The large
and small intestines have their own intrinsic nervous system.i. GI Nervous system is a ‘loop feedback’ – does not communicate w/spinal cord
or brain. It is call intrinsic or enteric system.ii. Pain receptors alter perceptions – leads to pain perception not necessarily
where problem is – this is called referred pain.
1
1
221
20
519
1
17
16
15
1
86
4
710,11,12
310
9 pyloricsphincter
2
6,7,8
5- GE junction
4
32
11

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
1. Eg: Appendicitis pain is usually manifest near the umbilicus yet the appendix is very near the pelvic bone.
b. GI system receives 30% of cardiac output, all contained in peritoneum (its own compartment).
i. Peritonitis is inflammation of this compartment – generally due to perforation of the intestine (either small or large) which then leaks fecal matter into an area that should be sterile. Can also result from perforation injuries, surgery….anything that introduces pathogens into the compartment.
II. Nausea and vomiting: Stomach is not really involved. The stomach, esophagus, andsphincters all relax, the forceful ejection producing emesis comes from the diaphragm. TRIGGERS?SEE PICTURE Happens w/tons of situations not related to GI(infection, MI, renal failure, drugs, smells, labor, Pain, Motion…..)
- Treatment: see table 42-1Many drugs – act on different sources.Zofran acts on Emetic center and has very few sideEffects.WARNING – Phenergen is vasocaustic–Not to be used _______________– IM or oral is best
HYDRATION: IV, clear liquids: avoid hot/cold (Broth/Gatorade high is Na+ can increase electrolyte problems).
- Potential complications: Alkalosis due to significant loss of acid – must be prolonged vomiting.
- Dehydration: happens rapidly in children and OA. Leads to electrolyte imbalances, decreased plasma and circulatory failure.
III. Upper GI: (Remember the numbers correlate to page one picture)
1- Tongue and paratid, sublingual, submandibular glands (yellow – 1)Functions: Tongue: mastication, deglutition (swallow), taste, speechGlands: Saliva production: 1 L per day, lubes food, prevents bacterial overgrowth.
AMYLASE (digestive enzyme in saliva) - begins breaking down the starches
2

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
Problems: Table 42-3 – ______________________________ – common in children but can occur in adults on antibiotics. Painful – inhibits eating, swallowing…. Looks like milk curds.
Gingivitis – due to negligent oral hygiene – lost teeth, foul odors, bleeding gums when brushing.Canker sores or Herpes – (viral) – steroids, mild antiseptic mouthwashes
2- Pharynx - 3 division: nasopharynx, oropharynx, laryngeal pharynx – same mucosal membrane as nasal cavity, mouth, auditory (Eustachian) tubes, and larynx. Function: secretion of mucus to aid swallowing.
3- Larynx - (common name is Adam’s apple) lies at beginning of trachea. Not considered part of digestive system – WHY do I mention it?Epiglottis: this acts like a lid or flap. When you swallow it closes off the larynx so you protect you airway.
4- Esophagus – lies behind the trachea Functions: Peristalsis – propulsion – moves food along…..Problem: _________________________
- Complications:o Esophagitis: o Esophageal stricture: – s/s dysphagia o Barretts( precancer): Acid alters DNA structures, risk increased by smoking/alcoholo Esophageal ulceration: o Esophageal Cancer:
5- G/E Junction, LES, S/C Junction – Gastro/esophageal junction, Lower esophageal sphincter,squamous/columnar Junction
Function:
- Problems: see GERDs
3
Not a disease but chronic symptoms of reflux-
MOST common upper GI problem in adults.
No single cause (refer to picture)
Manifestations: heartburn – abd pain (dyspepsia), pH of stomach content: ranges from 2-5 depending on food present or not.

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
6,7,8- Fundus, Body, Antrum (stomach)
9- Pyloric sphincter: Remember intrinsic nervous system? Presence of food triggers muscles of stomach to contract, mixing the food. Once it is a certain consistency call CHYME the pyloric sphincter opens and allows some to enter the duodenum.
Yellow #2 – Chief cells, Parietal cells, Goblet cells:
- Chief cells – release pepsinogen which digest proteins. Why could this be a problem? What is does our stomach consist of?
- Parietal cells – release hydrochloric acid (HCL), water and intrinsic factor. Why could this be a problem? What role does intrinsic factor play?
- Goblet cells – release mucus - our natural protection.- Brunners glands (in duodenum) release alkaline solution to neutralize acid
a. Hiatal Hernia: S/S same as GERDsTreated w/meds - if unsuccessful then they do a Nissen fundoplication (stomach wrap).
Incidence increases with age.b. Gastritis – Inflammation of the stomach lining. Causes:
- NSAIDS – also aspirin, steroids - Diet – alcohol (remember aspirin and alcohol
o Both absorbed in stomach.- Helicobacter pylori – fairly common – - Autoimmune - loss of parietal cells- Others:
o Radiationo Smokingo Nasogastric tubeso Psychologic stresso Physiologic stress; Burns, renal failure, sepsis, shock
4
Function: storage, mixing, and movement of food. Food moves into duodenum. LES and Pyloric sphincter keep contents within stomach. Remember pH of contents ranges from 2-5.
NOTE: only _______________, ________________, ___________________ absorbed in stomach

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
c. Ulcers- Anything that allows tissue and HCL to contact will cause ulcer. All the causes of gastritis
will promote ulcerations. See Patho Map – Lewis Fig 42-12- Gastric ulcers usually cause pain 1-2 hours after eating
“Pain is worse after I eat”- Duodenal ulcers usually cause pain 2-5 hours
“Pain feels better after I eat”- Complications:
o Hemorrhage – chronic GI bleedo Perforation – leads to peritonitis
d. Cancer – no single causative agent – think about cell changes that occur with any of the above mentioned issues. Cell changes can be triggers for cancer: so untreated H.pylori, gastritis…. can all result in cancer. Smoking and obesity both increase the risk.- S/S : weight loss, anorexia, indigestion, then pain.
e. UPPER GI BLEEDS: - Causes: WHY?
o Steroids, NSAIDS, aspirino Esophageal varices – patients with liver cirrhosis (discussed next week)o Esophogitiso Cancer – gastric or esophagealo Gastritiso Ulcers
- S/So Hematemesis – appears as bright red vomitus or coffee grounds
Bright red = Coffee grounds =
o Melena – __________________________________________________o Occult blood – small amounts of blood in vomitus, secretions, or stool – must have a
guaiac test.
f. FOODBORNE ILLNESS (Food Poisoning) – Focus on prevention- Nausea, vomiting, diarrhea, abd cramps – onset depends on causative agent (see
table 42-24)PLEASE notice the time differences – most don’t last long and are self- limiting. This is what many people have when they think they have 24 hour flu.
- Most dangerous = E. coli 0157:H7o Leads to hemorrhagic colitis and kidney failureo All people w/bloody diarrhea need a stool cultureo Will spread person to person – lives on surfaces for 72 hours
5

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
- Avoid antidiarrheal (Imodium) as it merely prolongs exposure to toxin – treat w/ restoring fluids/supportive care.
YELLOW CARDS – 4, 5, 6: (ACCESSORY ORGANS)
4- LIVER: functions as a filter
- Hepatic portal system: All blood from any digestive organ is filtered by the liver before returning to the heart.
- Hepatocytes: FUNCTIONING UNITSo Metabolizes: carbohydrates, proteins, fatso Detoxifies: inactivates drugs (first pass) – and harmful substanceso Produces bile (see gallbladder) – conjugates bilirubin– where does bilirubin come
from? Think RBCs. Jaundice (build up of bilirubin in serum) is evidence of either liver disease or
biliary diseaseo Stores glucose
- Kupffer cells: Macrophages (phagocytes) – attack bacteria and toxins
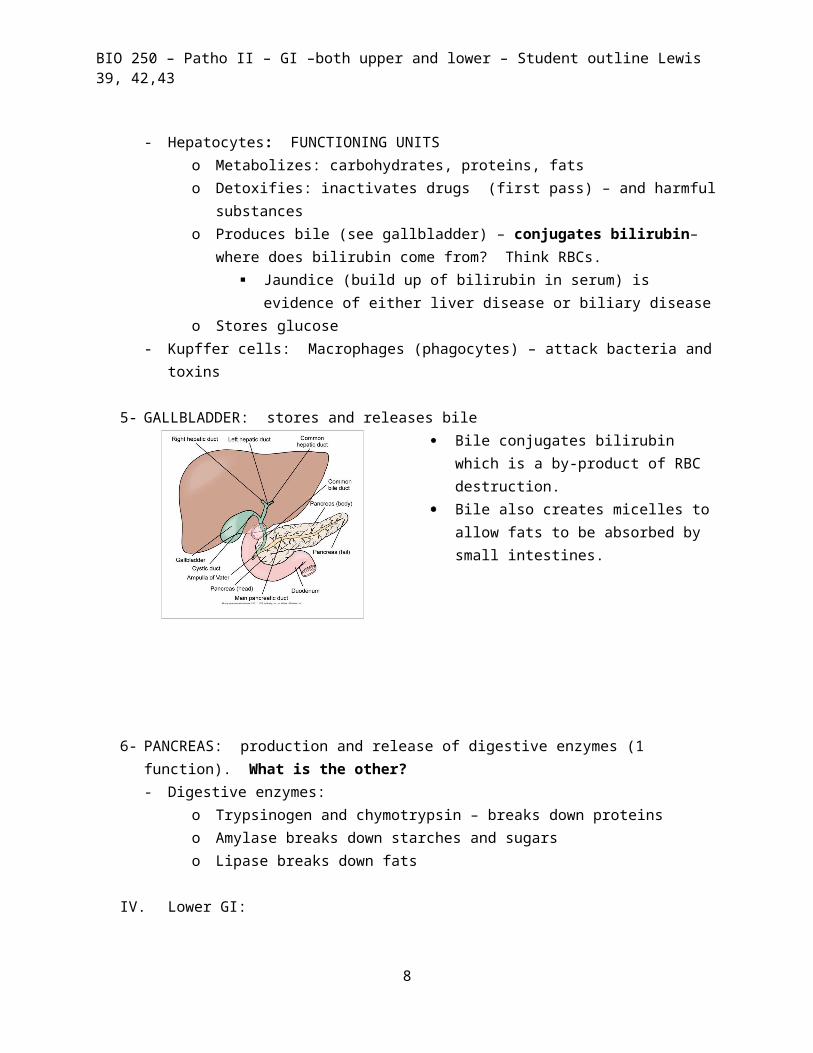
5- GALLBLADDER: stores and releases bile Bile conjugates bilirubin which is a by-
product of RBC destruction. Bile also creates micelles to allow fats to be
absorbed by small intestines.
6

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
6- PANCREAS: production and release of digestive enzymes (1 function). What is the other?- Digestive enzymes:
o Trypsinogen and chymotrypsin – breaks down proteinso Amylase breaks down starches and sugarso Lipase breaks down fats
IV. Lower GI:
BLUE 10, 11, 12- Duodenum, Jejunum, Ileum – (Brunners glands in the Duodenum produce neutralizing chemicals to eliminate the acid in chyme)
a. Function: digestion , absorptionb. Functioning unit: Villi/microvilli/Brush border
Production/release of Digestive Enzymes:
- Amylase - _____________________________________ digestion- Peptidases - ____________________________ digestion- Maltase and sucrose - ________________________digestion- Lactase - __________________________________________ digestion- Lipase - ________________________ digestion
c. Problems: 1. Duodenal ulcers (previously discussed)2. Decreased production of Enzymes Lactase deficiency is the most common – bloating, flatulence, cramping, diarrhea. Treatment is elimination of lactose (milk/milk products) from diet.
- MALABSORPTION S/S include: weight loss, diarrhea, steatorrhea
3. Celiac disease: autoimmune to gluten (found in wheat, barley, rye – and lots of processed foods). Only treatment is to modify diet. See table 43-33
4. Short Bowel – follows surgical resections (gastric bypass). Can lose 50% of small intestines without much change as long as terminal ileum and ileocecal valve remain intact. If these are removed you’ll see diarrhea, steatorrhea and malnutrition.
5. HERNIA – occurs when a portion of bowel protrudes through muscle wall.
- Inguinal – most common- Umbilical- Incisional
7
BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
S/S: mild pain, noticeable bulge DANGER: strangulation causing obstruction – Severe pain, vomiting, cramping, abd. distention
6. DIARRHEA- Why is diarrhea a problem? What could it lead to?Causes:-foodborne pathogens - fecal oral contaminations: E. coli, C. difficile, Norovirus- Antibiotics-large amounts of undigested carbs or fats (attract fluid)-decrease in digestive enzymes or biliary issues (lack of bile-fat remains in intestines).-Inflammatory bowel diseaseMost serious:- C. difficile – can progress to perforation, spores live up to __________________
on objects… can be transmitted from person to person/patient to patientNursing interventions to help prevent spread? Handwash, teach……
Treatment:- Self- limiting- Replace fluids/electrolytes- Culture for organisms, parasites, WBCs, blood…..- Antidiarrheal agents (use short time only) and NOT for infectious diarrhea
BLUE 13, 14 AND YELLOW 8 – Ileocecal valve, cecum, appendix
A. Function – connection from small intestine to large – surface changes (no more villi) B. Problems:
a. Acute abdominal pain:Causes:
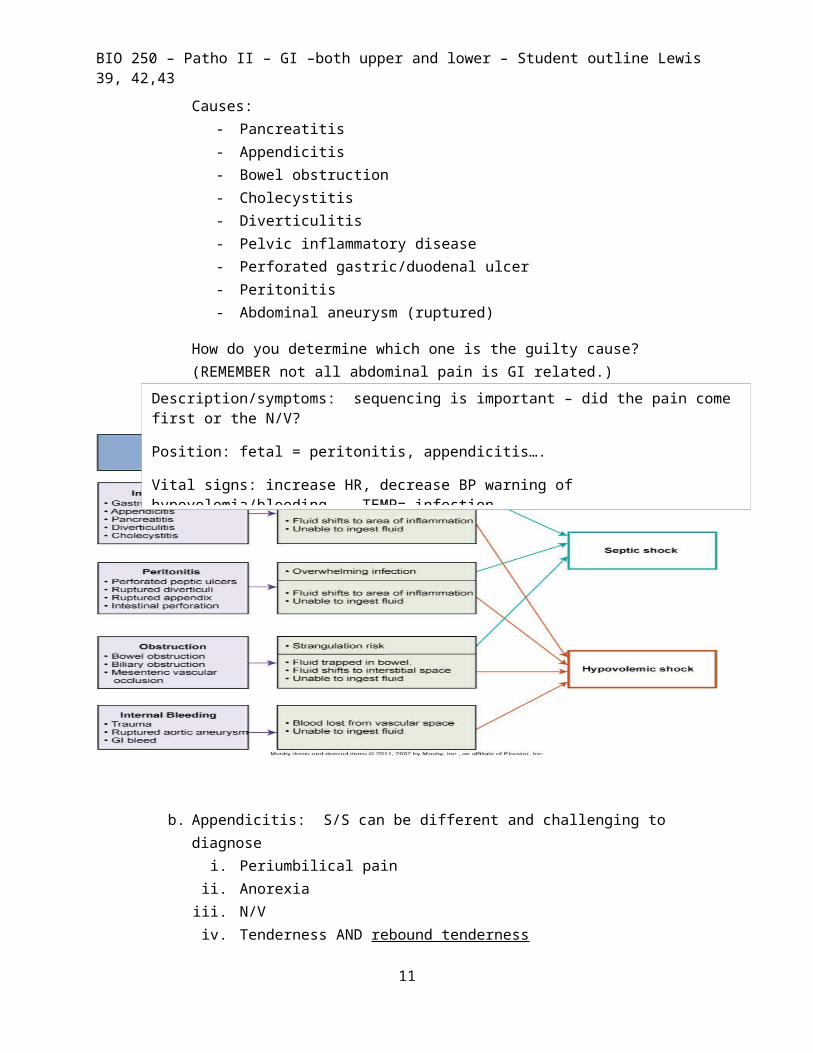
- Pancreatitis- Appendicitis- Bowel obstruction- Cholecystitis- Diverticulitis- Pelvic inflammatory disease- Perforated gastric/duodenal ulcer- Peritonitis- Abdominal aneurysm (ruptured)
How do you determine which one is the guilty cause? (REMEMBER not all abdominal pain is GI related.)
8
Description/symptoms: sequencing is important – did the pain come first or the N/V?
Position: fetal = peritonitis, appendicitis….
Vital signs: increase HR, decrease BP warning of hypovolemia/bleeding. TEMP= infection
palpation - rebound tenderness……

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
b. Appendicitis: S/S can be different and challenging to diagnosei. Periumbilical pain
ii. Anorexiaiii. N/Viv. Tenderness AND rebound tendernessv. Guarding
vi. Increased pain w/coughing, sneezing, deep breathingvii. Low grade fever
viii. Rovsing’s sign – ix. McBurney’s point –
C. Complication is PERITONITIS – a. Primary is due to blood borne pathogens entering peritoneal cavity.b. Secondary – most common – due to bowel perforation from any source.
i. S/S are same as appendicitis but escalate to severe pain, abdominal distention, fever, tachycardia, tachypnea.
ii. Treatment: NG suction, surgery, and lots, and lots of antibiotics - given IV
D. Paralytic ileus - a. Simply means peristalsis has stopped. Can be due to sedation, anesthesia, abd surgery
(most common cause).
9

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
BLUE 15, 16, 17, 18, 19 ASCENDING, HEPATIC FLEXURE, TRANSVERSE, SPLENIC FLEXURE, DESCENDINGA. Function:
a. Absorption of water and electrolytesB. Problems:
a. Inflammatory bowel disease (autoimmune) - comparison chart table 43-14i. Crohn’s disease - occurs ANYWHERE in the GI tract, has skip lesions (sections of
healthy tissue between inflamed tissue). Treated w/corticosteroids (Entocort and prednisone being the most common) and other drugs.
ii. Ulcerative Colitis – occurs only in the colon. Treatment is also corticosteroids and other drugs. Complete cure with colectomy.
iii. Fistulas can occur in eitheriv. Having either disease increases the risk of colon cancerv. S/S are bloody diarrhea/stools, weight loss, pain, fever, fatiguevi. First line of treatment with exacerbation is resting the bowel (complete NPO)
b. Intestinal obstruction: - can occur ANYWHERE along the tract
A- Adhesions, B - Strangulated inguinal hernia, C- Ileocecal intussusceptions, D - Intususception from polyps, E - Mesenteric occlusion – ischemic colitis, F - Neoplasm – cancer, G - Volvulus of sigmoid colon i. S/S depends on where the obstruction is:
o Small bowel: colicky intermittent pain, frequent vomiting can be PROJECTILE, some passage of stool, abd distention great – all in a short amount of time. IF DISTAL SM INTESTINE; VOMIT CAN SMELL LIKE FECAL MATTER AND BE BROWN
o Large bowel: mild cramping pain, absolute constipation, mild abd distention – takes time to come about.
ii. Treated w/NG tube, NPO, analgesics. They sometimes straighten themselves out – otherwise surgery is required.
10
BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
BLUE 20, 21, 22 Sigmoid Colon, rectum, anus
A. Function: defecationa. Facilitated by Valsalva maneuver: contraction of chest and abd muscles
i. Contraindicated in pts with head injury, eye surgery, cardiac problems (people have been found dead in the bathroom due to their heart stopping. If you have someone who is tachycardic you can get them to slow it down by using this maneuver.) hemorrhoids, abd surgery, portal hypertension (liver diseases).
B. Problems:a. Constipation –
i. S/S: hard, dry, difficult to pass stools, abd distention, bloating, increased flatulence.
ii. Due to: lack of dietary fiber, insufficient hydration, decreased physical activity, ignoring the urge. (use of Metamucil, citrcel, benefiber will help solve the problem – patients preconceived bias is that this is for OLD PEOPLE)
b. Diverticulosis/Diverticulitis - What’s the difference i. Due to increased pressures in the colonii. Most common in sigmoid but can be found anywhere along the coloniii. Risk is diverticulitis – inflammation from trapped fecal matter – can
lead to perforation.
c. Hemorrhoids- i. Caused by increased anal pressure: chronic constipation, pregnancy
(delivery), heavy lifting, prolonged sitting/standing, portal hypertension (liver disease).
ii. S/S: bleeding, pruritus, prolapse, pain
11

BIO 250 – Patho II – GI –both upper and lower – Student outline Lewis 39, 42,43
This picture is from Atlas of Pathophysiology published by Springhouse Corp. (2002). It shows diseases of the digestive system. I have included it as a visual aid.
12