saem 1989 annual meeting program
DESCRIPTION
ÂTRANSCRIPT

SAEM
Society forAcademicMedicine
Emergency
1989 Annual MeetingProgram
May 22-25, 1989San Diego, California

Call for AbstractsSociety for Academic Emergency Medicine
1990 Annual MeetingMay 2l-24, Minneapolis, Minnesota
The 20th Annual Meeting of the Society for Academic E,mergency Medicine will be held May 2l-24, lgg}at the Hyatt Hotel in Minneapolis, Minnesota.
Program Chairman, Paul Auerbach, MD, is now accepting abstracts fbr review fbr oral and poster presenta-tion at the 1990 Annual Meeting. Because of the large number of abstract submissions, the Annual MeetingProgram Committee has developed a two-page abstract form to be used fbr all abstract submissions. A copyof the abstract form is published in this program. Abstract fbrms will be mailed to the SAEM membership,will be published in the December issue of Annals of'Ernergcnc'y Medicine, and will be senr upon requesrto the SAEM office. Abstracts not submitted on the official abstract fbrm will be returned to the author forresubmission.
The deadline for the submission of abstracts for the 1990 Annual Meeting is January 19, 1990.All abstracts must be submitted on the official abstract form and must be postmarked no later thanJanuary 19.
Mail eight copies of the abstract form to:SAEM Annual Meeting Abstracts900 West OttawaLansing, Michigan 48915
Call (517) 485-5484 if you have any questions or would like to request an abstract fbrm.
Abstracts submitted or the resultant manuscripts must not appear in a ref'creedjournal prior to publicationof the meeting abstracts in the April 1990 issue of Annals of'Emargent'y Metlit ' ine, and must not have beenpresented previously at a national meeting.
Annals ofEmergency Medicine is the official journal of the Society for Academic Emergency Medicine. SAEMstrongly recommends that authors submit their manuscripts to Annals. Annals will notify authors of a deci-sion regarding publication within 90 days of receipt.
Cash awards will be given for the best abstracts in the following categories: Clinical Oral (Human Subjects),Basic Science Oral, Methodology Oral, Resident Oral, Scientiflc Poster, Methodology Poster, Resident Poster,and Oral or Poster Presentation in Pediatric Acute Care and Trauma. An award will be given by Annalsof Emergency Medicine for the Best Resident Paper published in Annals. All awarcl winners will be announcedat the 2lst Annual Meeting which will be held in Washington, DC in May 1991.
All abstracts must be submitted on an official abstract form. Please read the Callfor Abstracts carefullv for details and instructions.
PLEASE POST

INTRODUCTION
I would like to take this opportunity to welcome you to the inaugural Scientific Meeting of the Societyfor Academic Emergency Medicine (SAEM). The program content reflects the goals and o-bjectives of thisnew Society which include but are not limited to: 1) sponsoring forums for the presentation of scientificinvestigations, 2) promoting the academic maturation and education of its membeis, and 3) facilitating in-teraction and dialogue between its members and other organizations to further research and patient dare.
It bodes well that the Society's first meeting will be the largest truly scientific assembly ever convenedof individuals involved in academic emergency medicine. The Program Committee reviewed 473 abstractsand accepted 216. Both of these figures are records when compared to past University Association for Emer-gency Medicine meetings. Residents and fellows were the primary investigators in 87 of the studies to bepresented. Registration and attendance at the meeting will also be a new high. Attendees will have the optionof attending several tracks dealing with a specific research area or focus. the Society will highlight its first"state-of-the-art" presentation, "AIDS Research," on wednesday, May 24th.
The various committees and subcommittees of the Society will meet during the four days of the AnnualMeeting. These meetings are open to the membership and those interested in becoming more involved incommittee goals and tasks are encouraged to attend.
Ample time has been scheduled to allow registrants to attend the exhibits. The Sheraton on Harbor Islandand the city of San Diego offer a wide variety of attractions to occupy your spare time. I encourage youto take advantage of the Southern California climate.
James T. Niemann, MDPresident
INDEX
Banque t and A i r c ra f t Ca r r i e r Tou r . . . . . . . , 1
Ge neral Informatiorr
K e n n e d y L e c t u r e . . . . . . . . . . 4
State-Of-The-Art: AIDS Research
In te rna t i ona l Sess ion . . . . . . . 6
Academic Excel lence and Academic Leadership Awards. . . . . . . . j
Schedule of Events 8-13Posters .14-16
Abstracts. 17-40 & 45-68E x h i b i t o r s L i s t i n g . . . . . . . . . 4 1
Hotel Meeting Room Floor Plans . . . . .42-43
V a d e M e c u m . . . . 6 9 - 7 i
Annual Business Meet ing Agenda . . . . .72-73
constitution of the Society for Academic Emergency Medicine . . . . 77-78
Bylaws of the Society for Academic Emergency Medic ine . . . . . . . .79-81
1990 Abstract Form . . . .82-83
Membership Application
1990 Call for Abstracts
2-3
. .inside back cover

1989 ANNUAL AWARDS BANQUET
As always, the Annual Awards Banquet promises to be a fine ending to an outstanding educational ex-perience! All active, associate, and international members are entitled to one free ticket tolhe Banquet, butadvance registration is a must. In order for accurate meal counts, all banquet tickets must be requestedby May 19 in order to insure a ticket. Only a limited number of banquet tickets will be available at the Registra-tion Desk in San Diego and if you have not pre-registered you may not be able to obtain a ticket.
Tickets for resident members, presenters and others are available at $40 each. Purchased tickets must alsobe reserved by May 19 and additional tickets may not be available at the Registration Desk.
- Thls year's Banquet will begin with the annual loading of the buses with a departure of 6:00 pm fromthe Sheraton Hotel. The site of this year's Banquet is thi San Diego Wild Animal park which is located30 miles north of San Diego and the anticipated bus ride is approiimately 40 minutes.
The Wild Animal Park is a sprawling 1,800 acre sanctuary which enables animals to roam freely in set-tings similar to their native homelands. The Wild Animal Park has gained world-wide recognition for itsconservation efforts and offers you the opportunity to experience its uniqueness.
Upon arrival to the Witd Animal Park, registrants will journey through animal habitats of Africa via theWgasas Bush Line Monorail. This 50 minute tour will inciude guid"r de"scribing many of the 2,400 animalsliving together. It will be a special treat to view behaviors oianimals living in entire herds and flocks.
A cocktail reception and dinner will follow the tour. The dinner will be held in the Mombasa pavilionand will include a delicious two-entree buffet. And of course, the annual Imago Obscura and James MacKenzieAwards will be presented!
Buses will leave the Wild Animal Park at approximately l0:fi) pm and arrival at the Sheraton Hotel shouldn'tbe later than I l :00 pm.
The Annual Awards Banquet is a tradition you won't want to miss! If you haven't signed up for your ticket,call the SAEM office immediately at (517) 495-54g4.
AIRCRAFT CARRIER TOURThanks to the {.1.S. Navy, the SAEM Annual Meeting registrants have a rare opportunity to tour the U..S..S.
Independence, one of the 14 aircraft carriers in the U.S. fl"ei. These tours will be available only on Wednesday,May 24 and rhursday, May 25 and can accommodate only 75 persons each day.
The tours will take a total of about two hours; from l:00 to 3:00 pm. The tour will begin with boardingbuses for a departure time of l:00 pm. A scenic ride to the North Islind Naval Station locited on CoronadSFlTd via the magnificent Coronado Bay Bridge will take approximately 30 minutes. A one-hour tour willfollow and will include a tour of the bridge, flight deck, medical department, hangar deck and ward room.Buses will depart at approximately 2:30 for a 3:00 pm arrival bac-k at the Shera-ton on Harbor Island.
- Since only 75 persons per day will be accommodated each day, registrants must sign-up on a first come,first served basis. Sign-up sheets will be available at the SAEM Registition Desk startiig on Sunday evening,May 21.
- This is a rare opportunity for our membership to tour a most impressive ship and SAEM is grateful tothe U.S. Navy for its assistance and permission. Dr. Klingelberge., of the U.S. Naval Hospital in'San Diegohas been the coordinator of this event.
EMRA RECEPTION
EMRA - Emergency Medicine will host a Reception on Tuesday, May
23 from 6:30-7:30 pm. The highlight of the reception will be the presen-
tation of the 1989 Jean Hollister Award for Excellence in EMS and
Prehospital Care and the 1989 EMRA Academic Excellence Award.
Hors d'oeurves will be served and a cash bar will be available. All
interested EMRA members and others are invited to attend. The Recep-
tion is sponsoredby Emergency Medicine.
EXHIBITS
Exhibits will be available for viewing on May 22 from l:00-5:00 pm
and on May 23 from 8:00-l l:00 am and l:00-4:00 pm and on May
24 from 8:00-11:00 am. The exhibits will be located in the Exhibit
Hall and a list of exhibitors is included in this program. All coffee
breaks during exhibit hours will be held in the Exhibit Hall' Registra-
tion will also be located in the Exhibit Hall. Please take an opportunity
to view the exhibits durine the scheduled coffee breaks.
TECHNOLOGY FORUM
An informal Technology Forum will be held on Tuesday, May 23 from
8:00-11:00 am in the San Carlos Room. This wil l include a discussion
of the Technology Advisory Board.
EMRA RESIDENT RESEARCH FORUM
The annual EMRA Resident Research Forum will be held on Tues-
day, May 23 fromT:30-9:00 pm and will focus on Manuscript Prepara-
tion. Dr. Ronald Krome, Editor Emeritus of the Annals of Emergency
Medicine, will begin the forum with a discussion on how to prepare
a manuscript for publication. Dr. Krome was the editor of Annals for
15 years and brings a wealth of knowledge and experience to this topic.
The Forum will continue with a panel discussion by the editors of the
Emergency Medicine journals who will describe the general focus of
their respective journals and any aspects of manuscript preparation
which are of special interest to them. This will be followed by an open
question and answer period. All Annual Meeting registrants are in-
vited to attend this session.
RESEARCH DIRECTORS' LUNCHEON
The Second Annual Research Directors' Luncheon will be held Tues-
day, May 23 from 1l:30 am to l:00 pm in the Harbor Terrace Room
of the Sheraton on Harbor Island. This year's roundtable discussionwill focus on the topic, "Research Directors: Qualifications and Ex-
pectations." Dr. Gary Krause will begin the discussion with a report
from a survey on the status of research directors. Research directors
and all others interested in conducting research in Emergency Medicine
are welcome to attend. However, space is limited and advance registra-
tion is required. Tickets are $25 and a few tickets may be available
at the Registration Desk on May 22.
FELLOWS DINNER AND PROGRAM
The Annual Fellows Dinner and Program will be held Monday, May
22 from 7:30 pm to 9:30 pm in the Fairbanks Ballroom of the Sheraton
Grand Hotel. The topic of this year's Fellows Dinner and Program
will be, "Fellowship Training Curricula. " Dr. Peter van Ligten, Dr'
Richard Dart, Dr. Eric Davis, and Dr. Gerard Martin will discuss their
experiences and recommendations and this will be followed by a ques-
GENERAL INFORMATION
SundayMondayTuesdayWednesday
Thursday
tion and answer period. Space is limited and advance registration ls
required. Tickets are $25 and a few tickets may be available at the
Registration Desk on May 22.
OPENING COCKTAIL RECEPTION
SAEM is hosting an opening cocktail reception on Monday, May 22from 6:00 pm until 7:30 pm in the Bel Aire Ballroom of the SheratonGrand Hotel. All Annual Meeting registrants are invited to attend andcelebrate the new organization and toast to its future. Hors d'oeurveswill be served and a cash bar will be available.
PROCEEDINGSProceedings of the Annual Meeting will not be prepared as a separate
publication. However, selected presentations, scientific papers and per.
tinent discussion will be printed in the Annals of Emergency Medicine,
the journal of the American College of Emergency Physicians and
Society for Academic Emergency Medicine. In addition, the
from the 1989 Annual Meeting have been published in the April
issue of Annals of Emergency Medicine.
I99O CALL FOR ABSTRACTS
1990 Annual Meeting will be held May 2l-24 in Minneapolis'
Call for Abstracts is published in this program. Because there
changes in this year's abstract submission process, please read the
for Abstracts carefully and post it in your institution. The deadline
submission of abstracts for the 1990 Annual Meeting is January
I 990.
SAEM MEMBERSHIP
A membership application is included in this program and
copies are available upon request to the SAEM office at 900 West
tawa, Lansing, Michigan 48915 or cal l (517) 485-5484. I f you are
a member, please consider joining SAEM. If you are already a
give this application to a colleague. SAEM needs your support for
growth and development of academic Emergency Medicine.
SAEM BOARD OF DIRECTORS MEETING
The SAEM Board of Directors will convene a meetins on TrMay 23 from from 7:00-10:00 pm in the Chenin Room. Thiswill be chaired by Arthur B. Sanders, MD, who begins his termthe SAEM president at the Annual Business Meeting on May 23.interested members and others are invited to attend this, andmeetinss of the Board of Directors.
REGISTRATION AND INFORMATION
All registrants must check in at the SAEM Registration Desk to
up name badges which are required for admission into the
Meeting sessions. The Registration Desk will be open during the
listed below:
7:00-9:00 pm7:00 am-5:00 pm7:00 am-5:00 pm
7:00-l 1:00 aml:00-5:00 pm
7:00 am-5:00 pm
Exhibit HallExhibit HallExhibit HallExhibir HallFoyer, GrandFoyer, Grand
JAMES MACKENZIE AWARDThe James R. Mackenzie Award, named after one of UA/EM'sfbunders and first presidents of the society, was established to recognizethe importance of the honest, vigorous, and thoughtful discussion ofresearch papers at a scientific meeting. The Mackenzie Awardrecognizes that person who through discussion of one or more presen-tations at the meeting contributed to the scientific and intellectual qualityof the meeting in a signif icant and meaningful way. Al l investigatorsunderstand that, in order to have their work recognized, they must pres-ent it to their peers. The purposes of such presentations are: todisseminate new information, to educate others, to stimulate questionswhich wil l clari fy the hypothese, methods, results and conclusions ofthe work presented, and to receive constructive cri t icism which wil lgenerate new ideas and improve future work. The Mackenzie Awardis the embodiment of the bel ief that these things are important. Theaward is presented to encourage members to vigorously participate inthe proceedings of the meeting, because it is to promote these interac-t ions that the meeting is held. The Mackenzie Award has begun to beperceived in an increasingly inappropriate way. This trend could beturned around and the award placed back in its proper and rightfulperspective as emblematic of signif icant contr ibution to the annualnrcetlng.
POSTERS
Posters wil l bc set-up each morning f iom 9:00-12:00 noon and mustbc disnrantled each al iern<xrn by -5:00 pm. The schedule is as fbl lows:
Poster Session I 2:45-5: l-5 pm E,xhibit Hal l (Sheraton, on Har-bor Island)
Postcr Session II l :00-3:30 pnr LzrJol la, Monterey, Carmel, DelMar Rooms (Grand Hotel)
Poster Session II I l :30-4:00 pm (Same as Poster Session II)
ANNUAL BUSINESS MEETING
The Associatkrn wil l hold i ts Annual Business Meeting from l:00-2:30pm on Tuesday. May 23 in the Burgundy Ballroom. Al l members ofthe associat ion are urged to attend, however, only act ive members areel igible to vote.
SPEAKERS'READY ROOMA speakers' ready room will be available firr those who wish to checktheir slides in advance of their presentation. Keys to the ready room willbe available at the Registration Desk.
May 22 Roorn 5l l , Sheraton on Harbor IslandMay 23 - Towers II, Sheraton on Harbor IslandMay 24 - Towers Lounge, Sheraton on Harbor IslandMay 2-5 - Room I 14, Sheraton Grand
MESSAGE BOARD
A message board will be rnaintained at the Registration Desk. Phonemessages can be left at the SAEM Registration Desk by calling theSheraton on Harbor Island at (619) 692-2269 on May 22-24 and atthe Sheraton Grand on May 25 at (619) 692-2783 and requesting theSAEM Registrat ion Desk.
CONTINUING EDUCATION
The University of California, San Diego, accredited by the Accredita-tion Council for Continuing Medical Education, certifies that this pro-gram meets the criteria for Category I toward the Physicians Recogni-tion Award of the American Medical Association. The Annual Meetinghas also applied for Category I credit from the American College ofEmergency Physicians. A verification of CME credits will be sent toeach registrant immediately following the Annual Meeting.
ADDITIONAL MEETINGS
Monday, May 22
EMRA Board of Director Meeting8:00 am-12:00 noon - Room 414
Annals Editorial Board Meeting9:00 am-3:00 pm - Rooms 4l l -415
SAEM Research Committee Meetinel :00-3:00 pm - Room 418
SAEM Undergraduate Curriculum CommitteeMeeting
5:00-6:00 pm - Room 418
Tuesday, May 23
SAEM Technology Advisory Board Meeting8:00- l l :00 am - San Car los Room
SAEM Education Committee Meeting9 :30 - l l : 00 am - Room 515
SAEM Board of Directors Meetins7:00-10:00 pm - Chenin Ror im
Wednesday, }Iay 24
AJEM Editorial Board Meeringl2:3o- l :30 pm - Room 511
SAEM EMS Educators Committee Meetins3 :30 -5 :00 pm - Room 418
Residency Directors Meeting7:30-9:30 pm - White Wines Rooms
Thursday, May 25
Academic Chairs Meeting9 :30 - l l : 30 am - Room 518
PLACEMENT SERVICEA bulletin board will be maintained near the Registration Desk for per-sons wishing to post posit ions and physicians avai lable l ist ings.
EDUCATIONAL COLLABORATION OF MILITARYAND CIVILIAN TRAINING PROGRAMSA special session wil l be held on Tuesday, May 23 from 5:15 to 6:30pm and will focus on collaboration of military and civilian trainingprograms. Dr. William Dalsey will moderate this session and willdiscuss, "Research Consort iums." Dr. Wil l iam Bickel l wi l l discuss,"Research Ventures and Funding," Dr. Matthew Rice wil l discuss,"MAST Helicopter Programs and EMS," and Dr. Glenn Hamiltonand Dr. Raymond Ten Eyck will discuss, "Combined Residency Pro-grams. ' '
Additional panelists from all three military services who are activelyinvolved in a wide-range of activities will also be present to discussthe possibilities and help guide participants through the bureaucracyto avoid some of the pitfalls which can occur in dealing with themilitary. These additional panelists will include Dr. Gary Lammert,Residency Director at the San Diego Naval Hospital; Dr. MonteMellon, the Department of Transportation Consultant in EmergencyMedicine; Dr. John Howell, Assistant Chief of Emergency Medicineat Wilford Hall Medical Center; Dr. Alan Morgan, Residency Direc-tor, Darnall Army Medical Center; Dr. John Prescott, Chairman,Department of Emergency Medicine, Fort Bragg; Dr. Tim Coleridge,Emergency Medicine Consultant to the Army Surgeon General; andDr. Mitzi Johnson, Chief of EMS, Wright Patterson Air Force Base.

KENNEDY LECTT]RE
D. KaY Clawson, MDChairman, Executive Council, AAMC
Executive Vice ChancellorUniversity of Kansas School of Medicine
"The Education of the Emergency Physician"
Doctor Clawson is a graduate of Harvard Medical School and
entered academic medicine after completing his orthopaedic
training at Stanford University. He became one of the youngest
department chairmen in the country when he founded the ortho-
paedic department at the University of Washington' His
academic accomplishments are impressive. He has authored
seventy-five papers, five books, and numerous other publi-
cations.
Doctor Clawson has focused his career on improving the
quality of medical education. "My driving force," he said
recently, "is to get enthusiasm back into medical education"'
At the University of Washington, he took an innovative,
problem-solving approach to teaching, presenting students with
patients and having them determine how their diseases had
developed. He was twice awarded the Outstanding Teacher
Award there. He was Dean of the University of Kentucky
Medical School until he took his present position as the Exec-
utive Vice Chancellor of the University of Kansas Medical
Center. He founded the Emergency Medicine residency at the
University of Kentucky and is now starting an Emergency
Medicine program at the University of Kansas'
In recognition of his commitment to medical education,
has been elected to many leadership roles in the
of American Medical Colleges. He served as the Chairman
the Council of Deans in 1986 and is presently the Chai
of the Executive Council of the AAMC.
Doctor Clawson was chosen as Kennedy lecturer this
because he has actively and effectively worked to establish
separate identity of Emergency Medicine in organized
medicine. His acceptance and appreciation of the
ability and potential of Emergency Medicine has done
to establish its credentials in the upper echelons of
medical education in the United States. As Chairman of
Executive Committee of the AAMC, his support for
Medicine continues. The AAMC now has a separate
for Emergency Medicine faculty, and Emergency Medicino
its own listing in the AAMC statistics and publications'
The Society for Academic Emergency Medicine
the support that Doctor Clawson continues to give to
Emergency Medicine. The Society is honored this year to
Doctor D. Kay Clawson presenting the 1989 Kennedy
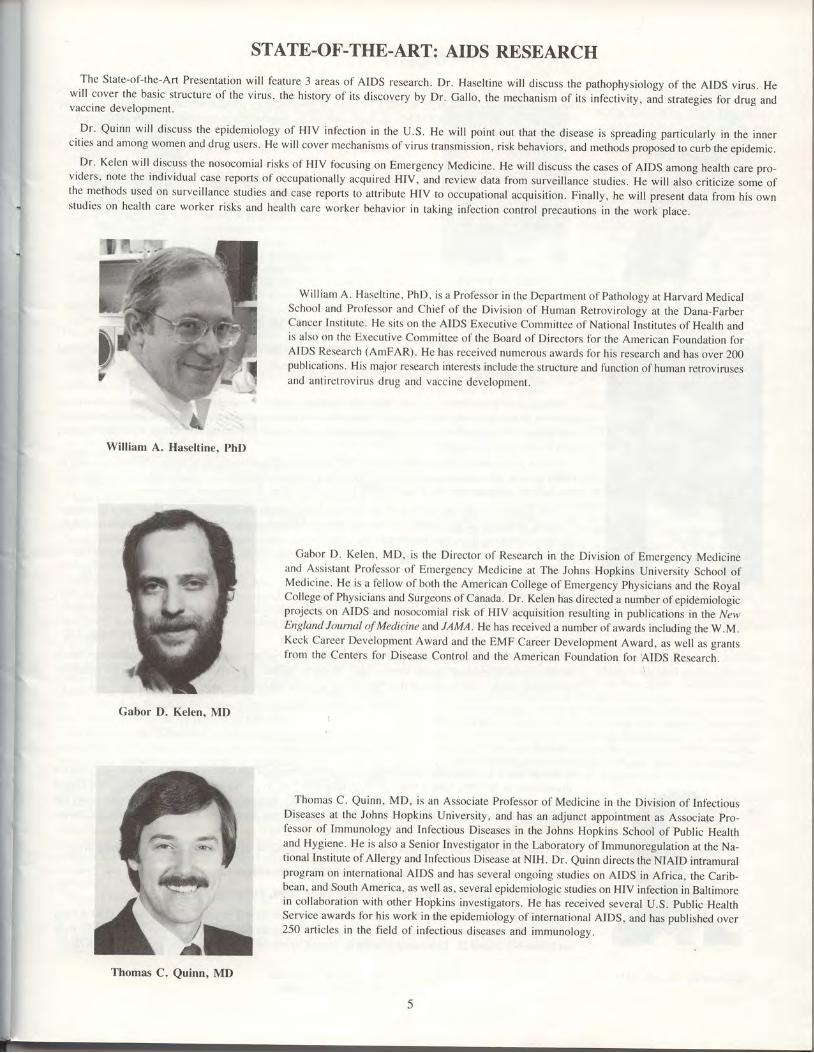
STATE-OF-THE-ART: AIDS RESEARCHThe State-of-the-Art Presentation will feature 3 areas of AIDS research. Dr. Haseltine will discuss the pathophysiology of the AIDS virus. He
will cover the basic structure of the virus, the history of its discovery by Dr. Gallo, the mechanism of its infectivity, and strategies fbr drug andvaccine development.
Dr' Quinn will discuss the epidemiology of HIV infection in the U.S. He will point out that the disease is spreading particularly in the innercities and among women and drug users. He will cover mechanisms of virus transmission, risk behaviors, and methods proposed to curb the epidemic.
Dr' Kelen will discuss the nosocomial risks of HIV focusing on Emergency Medicine. He will discuss the cases of AIDS among health care pro-viders, note the individual case reports of occupationally acquired HIV, and review data from surveillance studies. He will also criticize some ofthe methods used on surveillance studies and case reports to attribute HIV to occupational acquisition. Finally, he will present data from his ownstudies on health care worker risks and health care worker behavior in taking infection control precautions in the work place.
William A. Haseltine, PhD, is a Professor in the Department of Pathology at Harvard MedicalSchool and Professor and Chief of the Division of Human Retrovirology at the Dana-FarberCancer Institute. He sits on the AIDS Executive Committee of National Institutes of Health andis also on the Executive Committee of the Board of Directors for the American Foundation forAIDS Research (AmFAR). He has received numerous awards for his research and has over 200publications. His major research interests include the structure and function of human retrovirusesand antiretrovirus drug and vaccine development.
William A. Haseltine, PhD
Gabor D. Kelen, MD, is the Director of Research in the Division of Emergency Medicineand Assistant Professor of Emergency Medicine at The Johns Hopkins University School ofMedicine. He is a fellow of both the American College of Emergency Physicians and the RoyalCollege of Physicians and Surgeons of Canada. Dr. Kelen has directed a number of epidemiologicprojects on AIDS and nosocomial risk of HIV acquisition resulting in publications in the NewEngland Journal of Medicine and JAMA. He has received a number of awards including the W.M.Keck Career Development Award and the EMF Career Development Award, as well as grantsfrom the Centers for Disease Control and the American Foundation for AIDS Research.
Gabor D. Kelen, MD
Thomas C. Quinn, MD, is an Associate Professor of Medicine in the Division of InfectiousDiseases at the Johns Hopkins University, and has an adjunct appointment as Associate pro-fessor of Immunology and Infectious Diseases in the Johns Hopkins School of public Healthand Hygiene. He is also a Senior Investigator in the Laboratory of Immunoregulation at the Na-tional Institute of Allergy and Infectious Disease at NIH. Dr. Quinn directs the NIAID intramuralprogram on international AIDS and has several ongoing studies on AIDS in Africa, the Carib-bean, and South America, as well as, several epidemiologic studies on HIV infection in Baltimorein collaboration with other Hopkins investigators. He has received several U.S. Public HealthService awards for his work in the epidemiology of international AIDS, and has published over250 articles in the field of infectious diseases and immunology.
Thomas C. Quinn, MD

Herman H. Delooz. MD. PhD
David J. Steedman, MD
n = 1 2
Time (minutes) 0
INTERNATIONAL SESSION
Dr. Delooz is the Director of the Emergency Department and Emergency Medical Services at the University
Hospital Sint-Rafaell Gasthuisberg, as well as Professor of Anesthesiology and Critical Care Medicine at the Catholic
University in Leuven, Belgium SAEM is pleased to address the membership on the topic of, "Academic Emergen-
cy Medicine in Europe."
1988 Best Paper of the Emergency Medicine Research Society
Effect of a mechanical chest compression and ventilation device on arterial and central vehous blood
gas values during cardiac arrest in man, David J. Steedman, BSC, MB, ChB, FRCS, Robert Perchick,
MD, and Colin E. Robertson, MB, ChB, FRCP, FRCS
During cardioplumonary arrest the difference between arterial and central venous carbon dioxide levels
provides an indication of pulmonary blood flow. However the sequential determination of arterial and central
venous gas values in patients undergoing cardiopulmonary resuscitation in the emergency department has not
previously been investigated.
Twelve pre-hospital cardiac arrest patients had simultaneous measurements of central venous and
blood gases at lO-minute intervals during CPR with a mechanical chest compression and ventilation device.
All patients received only basic life support prior to arrival in the emergency department.
There was a predominant acidosis on the basis of both arterial and central venous blood gas
Both the mean arterial and central venous pCO2 levels fell during the course of the resuscitation as did
difference between these two measurements.
a H + ( m m o l / l )
sy I {+ (mmol / l )
paC02(kPa)
pcvC02(kPa)
63.6+6.996 .3+9 .14 .7 +0 .8t l . 2 + 1 . 6
n : 7l 0
63 .8 t 15 .486.4+8.24 . 8 + 1 . 210 .6 +0 .8
n : 520
69.2+13.4103.5 + 12.94 . 3 + 1 . 38 . 9 + 1 . 4
305 ? 5 +
78.5 t9.i
7 .8 t 1 .8
The profound difference between arterial and central venous pCO2 values reflects the poor pulmonary
flow produced by external cardiac compression. However the decrease in this difference during the
tion effort suggests the improved flow which can be achieved using a mechanical device.
Dr. Nowak will address the membership on current activities of the International Committee including
presentation to the 1988 Annual Meeting of the Emergency Medicine Research Society (EMRS) in the
Kingdom, the combined SAEM and EMRS meeting in 1990, the newly developed Best Resident/Fellow
Presentation International Award, and the 6th World Congress on Emergency and Disaster Medicine.
tant dates are found below:
6th World Congress on Emergency and Disaster Medicine - September 10-15' 1989' Hong Kong
EMRS Annual Meeting - November 24-25, 1989, York, United Kingdom
SAEM-EMRS Combined Meeting - October 18-20' 1990, Edinburgh' Scotland
The first recipient of the Best Resident/Fellow Oral Presentation will be selected at the 1989 SAEM
Meeting. The recipient will receive an expense paid trip to attend the 1989 EMRS Annual Meeting in
Richard M. Nowak, MD
on November 24 and25. This award is being sponsored by the Emergency Medicine Residents'Associ
r
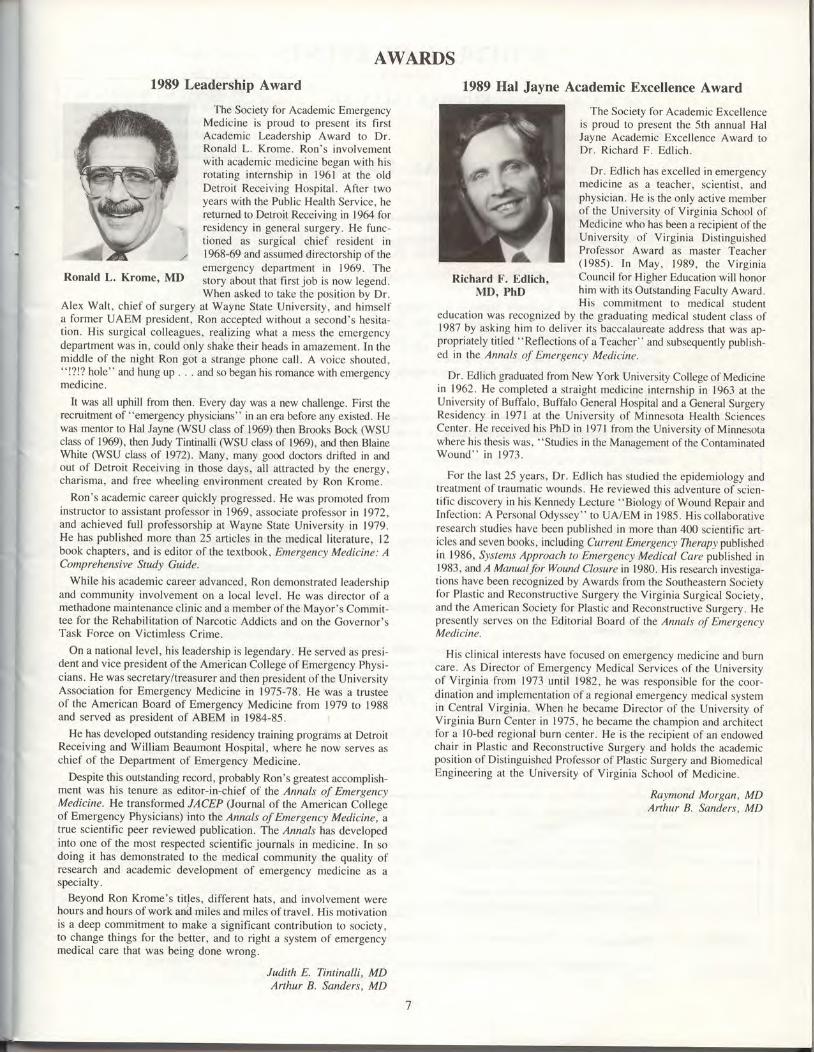
AWARDS1989 Leadership Award
Ronald L. Krome, MD
The Society fbr Academic EmergencyMedicine is proud to present its flrstAcademic Leadership Award to Dr.Ronald L. Krome. Ron's involvementwith academic medicine began with hisrotat ing internship in 196l at the oldDetroit Receiving Hospital. After twoyears with the Public Health Service, hereturned to Detroit Receiving in 1964 forresidency in general surgery. He func-tioned as surgical chief resident in1968-69 and assumed directorship of theemergency department in 1969. Thestory about that first job is now legend.When asked to take the position by Dr.
Alex Walt, chief of surgery at Wayne State University, and himselfa fbrmer UAEM president, Ron accepted without a second's hesita-t ion. His surgical col leagues, re4l izing what a mess the emergencydepartment was in, could only shake their heads in amazement. In themiddle of the night Ron got a strange phone cal l . A voice shouted," !'l!? hole" and hung up . . . and so began his romance with emergencymedicine.
It was all uphill from then. Every day was a new challenge. First therecruitment of "emergency physicians" in an era before any existed. Hewas mentor to Hal Jayne (WSU class of 1969) then Brooks Bock (WSUclass of 1969), then Judy Tintinalli flMSU class of 1969), and then BlaineWhite @SU class of 1972). Many, many go<lc doctors drifted in andout of Detroit Receiving in those days, all attracted by the energy,charisma, and fiee wheeling environment created by Ron Krome.
Ron's academic career quickly progressed. He was promoted frominstructor to assistant professor in 1969, associate prof'essor in 1972,and achieved full professorship at Wayne State University in 1979.He has published more than 25 art icles in the medical l i terature, l2book chapters, and is editor of the textbook , Emergency Medicine: AComprehensive Study Guide.
While his academic career advanced, Ron demonstrated leadershipand community involvement on a local level. He was director ol 'amethadone maintenance clinic and a member of the Mayor's Commit-tee for the Rehabilitation of Narcotic Addicts and on the Governor'sTask Force on Vict imless Crime.
On a national level, his leadership is legendary. He served as presi-dent and vice president of the American College of Emergency Physi-cians. He was secretary/treasurer and then president ofthe UniversityAssociation for Emergency Medicine in 197-5-78. He was a rrusteeof the American Board of Emergency Medicine from 1979 to 1988and served as president of ABEM in 1984-85.
He has developed outstanding residency training programs at DetroitReceiving and William Beaumont Hospital, where he now serves aschief of the Department of Emergency Medicine.
Despite this outstanding record, probably Ron's greatest accomplish-ment was his tenure as editor-in-chief of the Annals oJ' EmergencyMedicine. He transformed JACEP (Journal of the American Collegeof Emergency Physicians) into the Annals of Emergency Medicine, atrue scientific peer reviewed publication. The Annals has developedinto one of the most respected scientific journals in medicine. In sodoing it has demonstrated to the medical community the quality ofresearch and academic development of emergency medicine as aspecialty.
Beyond Ron Krome's titles, different hats, and involvement werehours and hours of work and miles and miles of travel. His motivationis a deep commitment to make a significant contribution to society,to change things for the better, and to right a system of emergencymedical care that was being done wrong.
Judith E. Tintinalli. MDArthur B. Sanders, MD
Richard F. Edlich.MD, PhD
Academic Excellence Award
The Society fbr Academic Excellenceis proud to present the 5th annual HalJayne Academic Excellence Award toDr. Richard F. Edl ich.
Dr. Edl ich has excel led in emergencymedicine as a teacher, scientist, andphysician. He is the only active memberof the University of Virginia School ofMedicine who has been a recipient of theUniversity of Virginia Dist inguishedProfessor Award as master Teacher(1985) . In May, 1989, the V i rg in iaCouncil for Higher Education will honorhim with its Outstanding Faculty Award.His commitment to medical student
education was recognized by the graduating medical student class of1987 by asking him to del iver i ts baccalaureate address that was ap-propriately titled "Ret1ections ofa Teacher" and subsequently publish-ed in the Annals ol Emergen<'v Medicine.
Dr. Edlich graduated fiom New York University Collegc of Medicinein 1962. He completed a straight medicine internship in 1963 at theUniversity of Buffalo, Buffalo General Hospital and a General SurgeryResidency in l97 l at the University of Minnes<xa Health SciencesCenter. He rcccived his PhD in l97l fiom the University of Minnesntawherc his thesis was, "Studies in the Management of the ContaminatedWound" in 1973.
For the last 25 years, Dr. Edl ich has studied the epidemiology andtreatment ol traumatic wounds. He reviewed this adventure of scien,t i l ic discovery in his Kennedy Lecture "Biology of Wound Repair andInl 'ect ion: A Personal Odyssey" to UA/EM in 198-5. His col laborativeresearch studics have been published in mure than 400 scienti f ic art-icles and seven books, including Currcnt Emergercv Therupy publishedin 1986, Sy^rlarn^r Approach to EmergenL'y Medical Carc published in1983, and,4 ManualJbrWound Ckssure in 1980. His research investiga-tions have been recognized by Awards fiom the Southeastern Societyl irr Plast ic and Reconstructive Surgery the Virginia Surgical Society,and the Arnerican Society tbr Plastic and Reconstructive Surgery. Hepresently serves on the Edikrrial Board of the Annal.s oJ'EmergencyMedicine.
His clinical interests have fbcused on emergency medicine and burncare. As Director of Emergency Medical Services of the Universityof Virginia from 1973 unti l 1982, he was responsible for the coor-dination and implementation of a regional emergency medical systemin Central Virginia. When he became Director of the University ofVirginia Burn Center in 1975, he became the champion and architectftrr a lO-bed regional burn center. He is the recipient of an endowedchair in Plastic and Reconstructive Surgery and holds the academicposition ol'Distinguished Prof'essor of Plastic Surgery and BiomedicalEngineering at the University of Virginia School of Medicine.
Raymond Morgan, MDArthur B. Sanders, MD
1989 Hal Jayne

SCHEDULE OF EVENTS
SUNDAY, MAY 21
7:00-9:00 pm Registration, Exhibit Hall
7:00 am-5:00 pm
8:15-8:30 am
8:30-8:50 am
8:50-9:10 am
9:10-10:00 am
MONDAY, M.AY 22
Registration, Exhibit Hall
Opening Remarks, Jerris R, Hedges, MD, Program Chairman, ChabLis Ballroom
The Academic Department of Emergency Medicine: What Can it Do?, Chablis Ballroom
Glenn C. Hamilton, MD, Professor and Chairman, Department of Emergency Medicine, Wright State University
How To Obtain Academic Department Status, Chablis BallroomAlexander Trott, MD, University of Cincinnati
Panef Discussion on Academic Status in Emergency Medicine, Chablis BallroomE. Jackson Allison, Jr., MD, MPH, East Carolina UniversityGlenn C. Hamilton, MD, Ilright State UniversityPaul Mehne, MD, Associate Dean for Student Affairs, East Carolina UniversityAlexander Trott, MD, University of CincinnatiDavid llagner, MD, Medical College of Pennsylvania
Coffee Break, Ballroom Foyerl0 :00-10:15 am
l l : 0 0 - 1 1 : 1 5 a m Coffee Break, Ballroom Foyer
l2 :00-1:00 pm
l:00-1:45 pm
l:45-2:00 pm
2:00-2:45 pm
2:45-3:00 pm
3:45-4:00 pm
4:00-5:00 pm
Lunch Break
Manpower Projections: AAMC, SAEM, and ACEP Perspectives, Chablis BallroomModerator: Arthur B. Sanders, MD, PresidentElect, Society for Academic Emergency Medicine
Jacek Franaszek, MD, President, American College of Emergency PhysiciansGlenn C. Hamilton, MD, Administative Board, Council of Academic Societies, AAMC
Coffee Break - Exhibits Open, fuhibit Hall
Indigent Health Care: The Carrot or the Stick? Chablis BallroomMichael J. Bresler, MD, Stanford University
Coffee Break - Exhibits Open, Exhibit Hall
Coffee Break, Exhibit Hall
Faculty Development, Institutional Responsibilities, and Strategies, Chablis Ballroom
Frank T. Stritter, PhD
All meetings will be held in theSheraton Hotel on Harbor Islandunless otherwise indicated. TheSheraton Grand Hotel is ndxt doorto the Sheraton on Harbor Island.
10: l5-11:00 am Track A: Developing Positive Resident Attitudes,Chablis BallroomMichael E. Gallery, PhD, Associate Executive Direc-tor, ACEP
l0: l5-11:00 am Track B: The Impaired Physician,Burgundy BallroomStephen Scheiber, MD, Executive Secretary,American Board of Psychiatry and Neurology
I l:15-12:00 noon Track A: Clinical Teaching Skills'Chablis BallroomFrank T. Stritter, PhD, Professor, SchooLs ofMedicine and Education, University of NorthCarolina at Chapel Hill
I l:15-12:00 noon Track B: Teaching the Non-Emergency MedicineRotator, Burgundy BallroomMargaret M. Barron, MD, Chnirman of EmergencyMedicine, Providence Hospital, Washington, DC
3:00-3:45 pm Track A: 24 Hour Coverage: Ways of Dealing withthe Issue, Chablis BallroomModerator: Louis Binder, MD, Texas Tech University
E. Jackson Allison, MD, East Carolina UniversityGlenn Hamilton, MD, Wright State UniversityDaniel Spaite, MD, University of ArizonaRobert Prosser, MD, University of KansasWilliam Robinson, MD, Truman Medical Center
Track B: The Role of EMS in the Academic Setting'Burgundy BallroomModerator: Ron lnw, MD, University of Chicago
Kathleen Cline, MD, East Carolina UniversityPaul Pepe, MD, Baylor Collge of Medicine

5:00-5:30 pm
7:00 am-5:00 pm Registration, Exhibit Hart 'TUESDAY' MAY 23
8:00-12:00 noon Poster Session I Set-Up, Exhibit Hall
8:00-8:15 am Announcements, Jerrts R, Hedges, MD, Chablis Ballroom
6:00-7:30 pm
7:30-9:30 pm
Awards Presentations, Chablis Ballroom
1989 Hal Jayne Award for Academic ExcellenceRichard F. Edlich, MD, PhDThe Hal Jayne Academic Excellence Award is sponsored by Spectrum Emergency Care, Inc.
1989 Academic Leadership AwardRonald L. Krome, MD
1988 Best Oral Basic Science"Amanba Phalloides Poisoning: Mechanism of Cimetidine Protection, " Sandra M. Schneider, MD, University of PittsburghThis award is sponsored by Emergency Medicine
1988 Best Oral Clinical Science"The Inability of Prehospital Trauma Prediction Rules to Classify Trauma Patients Accurately," William G. Baxt, MD,University of Califurnia, San DiegoThis award is sponsored by MICROMEDEX, Inc.
1988 Best Oral Methodology"Attending Coverage in Academic Emergency Medicine: A National Survey," Phittip L. Hennemnn, MD, Harbor-IICLAThis award is sponsored by SAEM
1988 Best Scientific Poster*Defining Normal Capillary Refill: Variation with Age, Sex, and Temperature," David L. Schriger, MD, UCLAThis award is sponsored by Emergency Medicine and Ambulatory Care News
1988 Best Methodology Poster"A Computer-Assisted Learning Tool Designed to lmprove Clinical Problem solving Skills," Frank J. papa, DO, TexasCollege of Osteopathic MedicineThis award is sponsored by SAEM
1988 Best Pediatric Acute Care and Trauma"Endotracheal Intubation of Pediatric Patients by Paramedics," Peter Aijian, MD, Valley Medical CenterThis award is sponsored by Pediatric Trauma and Acute Care
1988 Best Resident Poster"Reliability of Clinical Presentation for Predicting Significant Viper Envenomation," Katherine M. Hurlbut, MD, Ilniver-sity of ArizonaThis award is sponsored by Pergamon Press
1988 Annals Best Resident Paper"The Evaluation of Suspected Renal Colic: Ultrasound Scan vs. Excretory Urography," Douglas Sinclair, MD, VictoriaGeneral Hospital, Halifax, Nova ScotiaThis award is sponsored by Annals of Emergency Medicine
Opening Reception, Bel Aire Ballroom (Grand Hotel)
Emergency Medicine Fellows Dinner and Program, Fairbanks Ballroom (Grand Hotel)"Fellowship Training Curricula"Peter van Ligten, MD, Ohio State LlniversityRichard Dart, MD, University of ArizonaEric Davis, MD, Medical College of Pennsylvania, Allegheny CampusGerard Martin, MD, Henry Ford Hospital
8:15-9:30 am Plenary Session, Chablis BallroomModerator: John McCabe, MD, State University of New york
132. Emergency Department Diagnosis of Ectopic Pregnancy, Thomas G. Stovall, MD, (Jniversity of Tennessee133. Mortality and Morbidity Following the 1988 Earthquake in Soviet Armenia, Gabor D. Kelen, MD, Johns Hopkins
University
134. Analysis of the Emergency Department Management of Suspected Bacterial Meningitis, David A. Talan, MD, IlCLtl135. Ciprofloxacin in the Treatment of Acute Infectious Diarrhea, Martha Neighbor, MD, University of Califurnia, San
Francisco
136' Evaluation of Women With Possible Appendicitis Using Technetium-99M Leukocyte Scan, Terri A. Halt, MD,Harbor-UCI-4
9:30-10:00 am Coffee Break - Exhibits Open, Exhibit Hall

10:00- Track A: Administration, Chablis Ballroomll:30 am Moderator: Inuis Binder, MD, Texas Tech Universin
10:00- Track B: Respiratory, Burgundy Ballroom11:30 am Moderator: Jerome Hoflman, MD
143. Hypoxic Hazards of Paper Bag Rebreathing inHyperventilating Patients, Michael Callaham, MD,University of Califurnia, San Francisco
144. Inhaled Sodium Bicarbonate Therapy for Chlorine In-halation Injuries, Carey D. Chisholm, MD, JointMilitary Medical Command, San Antonio
145. Response of Bronchial Smooth Muscle to MgCl2 inYitro, William H. Spivey, MD, Medical College ofPennsylvania
146. Prospective Comparison of Inhaled Atropine andMetaproterenol in the Therapy of Refractory StatusAsthmaticus, Gary P. Young, MD, Ponland VeteransAdministration Medical Center
147. Adjunctive Use of Ipratropium Bromide in theEmergency Management of Acute Asthma, Steven M.Tiernan, MD, Darnall Army Community Hospital
148. The Utility of Extended Emergency Department Treat-ment of Asthma: An Analysis of Improvement in PeakExpiratory Flow Rate as a Function of Time, DanielG. Murphy, MD, Cook County Hospital
137. A Mathematical Model of Psychosomatic Symptomsin the Practice of Emergency Medicine, Raywin R.Huang, MD, Michigan State University
138. Refusing Care to Patients Who Present to an Emergen-cy Department, Robert W. Derlet, MD, University ofCalifurnia, Davis
139. Emergency Department Diversion of Non-Urgent Pa-tients to an Off-Site Walk-In Facility, Keith T.Sivertson, MD, Johns Hopkins University
140. Early Unexpected Deaths Following Admission Fromthe Emergency Department, Joseph G. Mueller, MD,Christ Hospital
14l. Use of Autopsy Results in the Emergency Depart-ment's Quality Assurance Plan, Mary C. Burke, MD,U niv e rs ity of Mas sachus ett s
142. DRGs the "Negative" Trauma Work-Up, CatherineM. Dougherry, RN, UMDNJ - Roben Wood JohnsonMedical School
I I :30 am- I :00 pm
l:00-2:30 pm
2:30-2:45 pm
2:45-5:15 pm
5 :15 -6 :30 pm
6:30-8:00 pm
7:00-10:00 pm
6:30-7:30 pm
7:30-9:30 pm
Research Directorst Luncheon, Harbor Tercace"Research Directors: Qualifications and Expectations"David Cline, MD, East Carolina UniversityGary Krause, MD, Wayne State University
SAEM Annual Business Meeting, Burgundy BallroomSee agenda, slate of nominees and proposed Constitution and Bylaws amendments in this program.
Coffee Break - Exhibits Open, Exhibit Hall
Poster Session l, Exhibit Hall
Governmental Affairs Committee Session, Chablis Ballroom"Academic Emergency Medicine's Interface with Federal Agencies and Research"Moderator: J. Douglas llhite, MD, Georgetown University
William kthr, Executive Secretary, Health Services Research Study Section, National Centerfor HealthServices ResearchJohn Spiegel, Deputy Director, Health Standards and Quality Bureau, Health Care Financing AdministationRichard Cummins, MD, University of WashingtonMickey Eisenberg, MD, University of WashingtonBonita Singal, MD, University of Cincinnati
This panel will explore current programs where federal funding agencies have developed projects with emergencyto investigate selected topics of research. Academic emergency physicians active in these programs will present theirand representatives of federal agencies will discuss their mission, program development, and attempt to project possiblel iaisons.
"Educational Collaboration of Military and Civilian Training Programs", Burgundy BallroomModerator: William C. Dalsey, MD, Iackland Air Force Base
William Bickell, MD, University of OklahomaGlenn Hamihon, MD, Wright State UniversityMatthew Rice, MD, Madigan Army Medical CenterRaymond Ten Eyck, MD, Unifurmed Services University of the Health Sciences
SAEM Board of Directors Meeting, Chenin Room
EMRA - Emergency Medicine Reception, Harbor TerraceDuring this reception EMRA will present the Jean Hollister Award and the EMRA Academic Excellence Award. Allregistrants are invited to attend.
EMRA-SAEM Resident Research Forum. Chablis Ballroom"Manuscript Preparation in Emergency Medicine"Ronald L. Krome, MD, Editor Emeritus, Annals of Emergency Medicine
John McCabe, MD, Editor, ResuscitationPeter Rosen, MD, Editor, Journal of Emergency MedicineJoseph Waeckerle, MD, Editor, Annals of Emergency MedicineJ. Douglns White, MD, Editor, American Journal of Emergency Medicine
l 0

WEDNESDAY, M.AY 247:00-12:00 noon Registration, Exhibit Hall
8:00-12:00 noon Poster Sessions II Set-Up, LaJolla, Monterey, Carmel and Del Mar (Grand Hotel)8:00-8:15 am Announcements, Jerris R. Hedges, MD, Chablis Ballroom
8:15- Track A: Cerebral Resuscitation, Chablis Ballroom9:45 pm Moderator: Gerard Manin, MD, Henry Ford Hospital
149. Evaluation of Brain Edema Using euantitativeMagnetic Resonance Imaging, James E. Olson, phD,Wright State University
150. Effect of High-Dose Norepinephrine VersusEpinephrine on Cerebral and Mycardial Blood FlowDuring CPR, James 14. Hoekstra, MD, Ohio StateUniversity
l5l. Cerebrovascular Occlusion: When Do HemorrhaeicInfarcts Develop? Gabrielle de Counen-Myers, Mb,University of Cincinnati
152. Cerebral Multifocal Hypoperfusion After Cardiac Ar-rest in Dogs, Mitigated by Hypertension andHemodilution, Fritz Sterz, MD, University ofPittsburgh
153. Cerebral Ischemia and Reperfusion: Failure of Hyper-baric Oxygen Therapy to Promote Increased Survivalor Neurologic Protection, Jeffrey p. Smith, MD,Geo r ge lVashington U niv e r s ity
154. A Dose Response Study of an Experimental IronChelator for Inhibition of DNA Damage by OxygenRadicals, Debra M. Feldmnn, MD, Wayne StateUniversity
8:15- Track B: Cardiac Arrest/EMS, Burgundy Ballroom9'.45 am Moderator: David Wilcox, MD, IJniversity of Massachusetts
155 . The Relative Contributions of Early Defibillation andACLS Interventions to Resuscitation and SurvivalFrom Prehospital Cardiac Arrest, Judith R. Graves,EMT-P, RN, University of Washington
156. EMT-D Survivors: The Contribution of Defibrillation,Daniel Fark, MD, Medical College of Wisconsin
157. Prehospital Transcutaneous Cardiac pacing - phaseil, William C. Dalsey, MD, Wilfurd Hall MedicalCenter, Lackland Air Force Base
158. Survival Prognosis for the Elderly Following Out-Of-Hospital Cardiac Arrest, MarniJ. Bonnin, MD, BaylorCollege of Medicine
159. Prehospital Prophylactic Lidocaine Does NotFavorably Affect the Outcome of Patients With ChestPain, Kathleen M. Hargarten, MD, Medical Colleseof Wisconsin
9:45-10:15 am
10:15-12:00 noon
12:00-1:00 pm
l:00-3:30 pm
3:30-4:00 pm
Coffee Break - Exhibits Open, Exhibit Hall
State-of-the-Art Presentation: AIDS Research, Chabtis BailroomModerator: Michael Callaham, MD, Ilniversity of Catifurnia, San Francisco"Pathophysiology of HIV Infection," William Haseltine, PhD, Chief, Division of Human Retrovirology, Dana
Farber Cancer Institute, Harvard Medical School"Epidemiology of HIV Infection, " Thomas C. Quinn, MD, Senior Investigator, Narional Institute of Atlergy andInfectious Diseases, National Institutes of Health and Associate Professor of Medicine, Johns Hopkins I)niv:ersity'Risk of Nosocomial Infection with HIV," Gabor D. Kelen, MD, Director of Research and Asiistant professirof Emergency Medicine, Johns Hopkins IJniversity
Lunch Break
Poster Session Il, ln Jolla, Del Mar, Carmel and Monterey (Grand Hotel)
Coffee Break, Foyer (Grand Hotel)
4:00- Track A: Pediatrics. Chablis Ballroom5:30 pm Moderator: Dee Hodge, MD, University of Southern
Califurnia
160. Comparison of Topical Anesthetic Agents in theRepair of Facial and Scalp Lacerations in Children,David A. Ross, MD, University of Cincinnati
161. TAC vs Cocaine Alone, Lind.a Crabbe, MD. St. Fran-cis Hospital
4:00- Track B: Infectious Disease, Burgundy Ballroom5:30 pm Moderator: Robert McNamara, MD, Medical College of
Pennsylvania
166. Cat Bite Wounds: Risk Factors forlnfection, DanielJ. Dire, MD, Darnall Army Community Hospital
167. The Use of Oral Acyclovir in the Treatment ofHerpetic Whitlow, Eric A. Davis, MD, Medical Col-lege of Pennsylvania, Allegheny Campus
162. Safety Practices and Living Conditions of l-ow Income 168. Screening for Syphilis in the Emergency Department:Urban Children, Lisa J. Santer, MD, Case Western RPR's in Patienti wittr Suspected s"*uully iransmirReserve University ted Diseases, Amy Ernst, UO, St. Franiis Hospital
163' Undiagnosed Abuse in Children Under Three With 169. HTLV-I Infection in a Inner-City Emergency Depart-Femoral Fracture, Heidi J. Dalton, MD, Wayne State ment Population: The Next Retrovirus Epidemic?Univ'ersity Gabor D. Kelen, MD, Johns Hopkins Uniiersity
164. Outpatient Management of Febrile Infants 28 to 90 170. Multicenter HIV and Hepatitis B SeroprevalenceDays of Age With Intramuscular Ceftriaxone, Marc Sndy, Barbara Wayson, Mb, oregon Heaih SciencesN. Baskin, MD, Children's Hospital, Boston (Jniversity
165 ' Outcome in Highly Febrile Nonbacteremic Children, 171 . Hepatitis B Infection and Human ImmunodeficiencyJoan Burg, MD, Children's Hospital, Boston Virus Infection in Emergency Department patients,
Keith T. Sivertson, MD, Johns Hopkins UniversitvSee next page for Track C
l l

4:00-5:30 pm Track C: Cardiac Resuscitation, Palomar BallroomModerator: Gary Krause, MD, Wayne State University
lT2.TheEffects of Fructose-1,6-Diphosphate on Myocardial Necrosis During Coronary Artery Occlusion, Timothy G. Janz, MD,
Wright State University
l73.High Energy Phosphate Metabolism During Ventricular Fibrillation, Robert Neumar, Ohio State Universiry
174 Factors lnfluencing Neurologic Recovery After Cardiac Arrest, Norman Abramson, MD, Universiry of Pittsburgh
lT5.Improved Resuscitation and Limited Myocardial Infarct Size Following Cardiopulmonary Bypass (CPB) Reperfusion, Mark
Angelos, MD, Wright State University
176. Comparison of Epinephrine and Dopamine in Cardiopulmonary Resuscitation, Karl H. Lindner, MD, University of Ulm, West
Germnny
177. Monitoring End-Tidal Carbon Dioxide as a Prognostic Index During Cardiopulmonary Resuscitation in Humans, Arthur B.
Sanders, MD, University of Arizona
5:30-7:00 pm International Affairs Committee Session, P alomar Ball room' 'Academic Emergency Medicine in Europe,' ' Herman Dektoz, MD, I)niversity Hospital of St. Rafaell Gasthuisberg, Leuven'
Belgium"Report on the Emergency Medicine Research Society and the 1990 SAEM-EMRS Combined Meeting in Edinburgh, Scotland,'l
Richard M. Nowak, MD, Chairman, International Committeepresentation of 1988 EMRS Best paper: "Effect of a Mechanical Chest Compression and Ventrilation,Device on Arterial
and Central Venous Blood Gas Valuesburing Cardiac Arrest," David J. Steedman, MD, Royal Infrmary of Edinburgh, Scotland
Emergency Medicine Residency Directors Meeting, Wite Wines Rooms: Riesling, Gamay, Colombard, and Chenin"Dual Residency Training Programs""lmpact of New York Regulations on Emergency Medicine Training: Staffing, Recruitment, Salaries""Advancing Medical Student Awareness of Emergency Medicine: Recruitment of Top Students""Locked Out of Emergency Medicine: The Problem of the Flexible Resident Who Doesn't Match""Using New Technologies for Efficiency and Education: Computer, Videotape, EMail, FAX, Etc."
Also, ieports from other organizations and discussion of organization of residency directors'
7:30-9:30 pm
THURSDAY, MAY 25
7:00 am-5:00 pm Registration, Bel Aire Ballroom Foyer (Grand Hotel)
8:00 am-12:00 noonPoster Session III Set-Up, Del Mar, La Jolla, Monterey, and Carmel (Grand Hotel)
Announcements, Jerris R. Hed.ges, MD, Bel Aire Ballroom (Grand Hotel)
Kennedy Lecture, Bel Aire Ballroom (Grand Hotel)"The Eduiation of the Emergency Physician," D. Kay Clawson, MD, Chairman, Executive Council, Association oJ
Medic1l Colleges and Executive Vice Chancellor, (Jniversity of Kansas School of Medicine
Coffee Break. Bel Aire Ballroom Foyer
8:00-8: l5 am
8:15-9:00 am
9:00-9: l5 am
9: l5 - Track A: Trauma-EMS, Be l A i re Ba l l room10:45 am Moderator: RonaM Low, MD, University of Chicago
178. A Prospective Study of Helmet Usage on MotorcycleTrauma, Patrick J. Kelly, MD, University of lllinois
179. Comparison of Different Definitions of CriticalTrauma Patients, Michael Smith, MD' Highbnd
General Hospital
180. Prehospital Advanced Trauma Life Support forPenetrating Cardiac Wounds, Ben Honigman, MD,University of Colorado
l8l . Impact of Interhospital Air Transport on Mortality in
a Rural Trauma System, Robert C. Campbell' MD'
Memorial Medical Center, Inc.
l82.The Impact of a Regionalized Trauma System onTrauma Care in San Diego County' David A. Guss,MD, Ilniversity of Califurnia, San Diego
Track B: Clinical, Fairbanks Ballroom (Grand Hotel)
Moderator: Phil Henneman, MD, Hcrbor-UCL4
183. Comparison of Cimetidine and Diphenhydramine inthe Treatment of Acute Urticaria, Ronald Moscati,MD, Darnall Army Community Hospital
184. Cimetidine in the Treatment of Acute Allergic Reac-
tions, Jeffrey W. Runge, MD, Charlotte MemorialHospital
185. Early Detection of Acute Myocardial Infarction: Im-
munochemical Determination of CPK-MB VersusStandard Electrophoresis, W. Brian Gbler' MD,Vanderbilt University
186. Use of Indomethacin Suppositories in the Treatmentof Ureteral Colic, Scott Melanson, MD, GeisingerMedical Center
1 87 . Indomethacion for Relief of Acute Renal, Colic, AllanB. Wolfson, MD, University of Pittsburgh
188. Stabilization of Unstable Pelvic Ring Fractures With
Military Anti-Shock Trousers: A Radiographic Assess-ment, Carlos C. Huerta, MD, Mt. Sinai MedicalCenter of Cleveland
t2

10:45- l l :00 am Coffee Break, Bel Aire Ballroom Foyer
I l:00- Track A: Shock-Neurologic Trauma, Bel Aire Ballroom12:30 pm Moderator: Steven Dronen, MD, University of Cincinrnti
189. Neutrophil Medicated Microvascular lnjury, DonnaL. Carden, MD, lnusiana State University
190. The Detrimental Effects of Intravenous CrystalloidFollowing Aortomy in the Swine, William H. Bickell,MD, lztterman Army Institute of Research
19l.An Evaluation of the Diagnostic Capabilities ofMagnetic Resonance Imaging with a Comparison toComputerized Tomography in Acute Spinal Columnlnjury, M. Andrew Levitt, DO, Thomns JeffersonUniversity
l92.Effect of Hypertonic vs Normotonic Resuscitation onIntracranial Pressure After Combined Head Iniurv andHemorrhagic Shock, Charlene B. Irvin, MD,"Uiiver-sity of Cincinnati
193. Effect of Chemical Interventions on Cerebral EdemaFormation Following Head Trauma in Rats, MichelleH. Biros, MD, Hennepin County Medical Center
194. Oral Intubation in the Multiply Injured patient: TheRisk of Exacerbating Spinal Cord Damage, KennethJ. Rhee, MD, University of Califurnia, Davis
ll:00- Track B: CPR, Fairbanks Ballroom12:30 pm Moderator: Richard Cummins, MD, [Jniversity of
Washington
195. Evaluation of Direct Mechanical Ventr icularAssistance Following Fifteen Minutes of VentricularFibrillation, Mark P. Anstadr, MD, Ohio StateUniversity
196. Coronary Perfusion pressures Durine CpR are Hisherin Patients with Eventual Return of Spontun.ou.
"Cir-
culation, Timothy J. Appleton, Henry Ford Hospitall9l.High Dose Epinephrine and Coronary perfusion
Pressure During Cardiac Arrest in Humans, NormanA. Paradis, MD, Henry Ford Hospital
198. Extreme Systemic and Cerebral Oxygen ExtractionDuring Human CPR, Mark G. Goetting, MD, HenryFord Hospital
199. Cerebral Lactate Uptake During prolonged GlobalIschemia in Humans, Emanuel p. Rivers, MD, HenryFord Hospital
200. Lidoflazine Administration to Survivors of Cardiac Ar_rest, Nomnn Abramson, MD, L/niversity of pittsburgh
ll:00-12:30 pm Track C: Toxicology, Fairbanks BallroomModerator: Edward Krenzelok, MD, pinsburgh poison Center201. Glucagon: Prehospital Therapy for Hypoglycemia, Rade B. Vukmir, MD, IJniversity of pittsburgh202. Accurate_Prediction of Tricyclic Antidepressant Overdose Complications Using ED presentation: A prospective Study,
Garritt E. Foulke, MD, IJniversity of Califurnia, Daws203. Hyperventilation in Tricyclic Antidepressant Toxicity, Heeten Desai, MD, University of Arizona204.The Effect of Alpha-l Acid Glycoprotein on Nortriptyline Toxicity in Swine, David C. Seaberg, MD, University of piusburgh205. The Evaluation of Cocaine Induced Chest Pain, Glenn Tokarski, MD, Henry Ford Hospital206.Severe Oral Phenytoin Intoxication: Lack of Cardiovascular Morbidity, Collette D. Wyte, Detroit Receiving Hospital
l2 :30- l :30 pm
l:30-4:00 pm
4:00-4:15 pm
Lunch Break
Poster Session IlI, Oet Mar, La Jolla, Monterey, and Carmel (Grand Hotel)Coffee Break, Bel Aire Ballroom Foyer
l 3
4:15- Track A: Trauma. Bel Aire Ballroom5:30 pm Moderator: John Marx, MD, University oJ'Colorado
207. Decreased Inflammatory Reaction (Enhanced BurnWound Healing) in Non-ionic Surfactant Treated Rats,Paul W. Paustian, Jr., MD, Eisenhowqr Army MedicalCenter
208. Effect of Povidone-Iodine and Saline Soakins onQuantitative Bacterial Wound Tissue Counts in ,{cuteTraumatic Contaminated Wounds, Mark Fourre, MD.Valley Medical Center
209. Tetanus Immunization Status and ImmunolosicResponse to a Booster in an Emergency DepartmJntGeriatric Population, Annie Gareau, MD, Universityof Toronto
210. Utility of Contrast Duodenography in the Detectionof Proximal Small Bowel Injury Following BluntTrauma, Joanne M. Edney, MD, Denver beneralHospital
2ll.Computed Tomography (CT) in the Evaluation ofBlunt Abdominal Trauma, William C. pevec, (Jniver-sity of Pittsburgh
4:15- Track B: Environmental-Toxicology , Fairbanks5:30 pm Ballroom
Moderator: Richard Dart, MD, University of Arizona212..4 Comparative Rewarming Trial of Gastric vs.
Peritoneal Lavage in a Hypothermic Model, M. An_drew lzvitt, DO, Thomas Jffirson llniversity
213. Protocols for the Use of a portable HyperbaricChamber for the Treatment of High AltitudeDisorders, Robert L. Taber, MD, St. Luke's Hospital
214. A Novel Strategy for Therapy ofAcute Iron poison-ing, John R. Mahoney, Jr., phD, Universi\ ofMinnesota
215. Combined Therapy with Cimetidine, penicillin, andAscorbic Acid for Alpha Amanitin Toxicity in Mice,Sandra M. Schneider, MD, University of pittsburgh
2l6.Contribution of Sorbitol Combined with ActivatedCharcoal in Prevention of Salicylate Absorption, RayE. Keller, MD, Geisinger Medical Center
6:00-11:00 pm SAEM Annual Banquet

POSTER PRESENTATIONSPoster Session I - Tuesday, May 23
"Frequent Fliers": A Protocol fbr the Management of FrequentVisitors to a Community Hospital Emergency Department, pliiB. Fontanarosa, MD, Northeastern Ohio [Jniversitrcs
X-Ray Ordering: Agreement Between the Triage Nurse andPhysician in a Pediatr ic Emergency Department. Z elurul Ropp,MD, Children's Hospital of Eastern Ontario
Emergency Department Medical Record euality - Measurcclby fmplicit and Explicit Methods in an Academic Settinc., AmoldR. So.sbw, MD, Univer.sity of'Massachusetts
A Dictated and Transcribed Medical Record Can be Cost Ei'-l'ective, Hurlan A. Stueven, MD, Medit'al College of'Wi.sconsin
Emcrgency Department Patients with PID: Do They UnderstandTheir Diagnosis' ! El i t ,ubeth A. Cunpbell , RN, Unit,ersity r lPenn.rylvaniu
AIDS Education in the Emergency Department, Duvid Mugid,BS, Univertitt, tl Pcnnsylvaniu
Erlcrgcncy Physicians Responses to Famil ies Fol lowing patientDcath.'[crri Schmidt, MD, Oregon Hrulth St'ience.t Univcrsitt,
Teaching E,thics in Emergency Medicine, Zbigniaw Snxlulski ,MI), Butterwtrth Ho.spitul
Problern-Based ACLS Instruction: A Modcl Approach lorUndcrgraduate Entergency Medical Education, Robcrr F.Polglust, Mcrcer Universit v-
Analyzing Clinical Case Distr ibutions to Improvc an ErlergcneyClerkship, kthcrt A. Dcktren?.o, BS, Albany Mcdicul Colle.qc
An Evaluation of 'Pediatr ic Emergency Medicine Education: AreThe Nceds ol Enrergcncy Medicinc and lts Residcnts Being Mer'/Ri<'hurd M. Cuntor, MD, State IJnivcrsit,- of New ktrk
Paranredic Physical Assessment and Intervention in Children.Nuncy A. Schonleld, MD, Chiltlren's Hospitu! rl ltt"- Angelas
The lrnpact of 'a Didactic Session on the Success of Fel ine En-d<rtrachcal f ntubation by Paranredics, 'fhomas
E. Tarrulrup, MD,Stutc Uniy,ersit1, tsl New ktrk
The Ell 'cct ol ' an Explici t Airway protocol on Fl ight NurseBchavior and Perfirrmance, Kenncth J. Rhee, MD, UniversitvoJ Calilorniu, Duvis
Developnrent ol'a Computer Modcl to Predict EMS Systerr per-t irrnrance After Changes in Numbcr, l ,ocation and Area ofResponsibi l i ty of EMS Units, El izabeth Criss, RN, UniversityoJ Arizonu
Sequential Cl inical Trials in Emergency Medicine, Roger. l .Lewis, MD, PhD, Harbor-UCI-4
Effects of Acute Ethanol Ingestion on Orthostat ic Vital Signs,Christian Tomasz.ew.ski , MD, East Carolina Universtlt
Evaluation of the Tilt Test in an Adult Emergency DepartmentPopulation, Bernard Lopez, MD, Thomas Jefferson University
Probability of Appendicitis Befbre and After Observation, ktuisG. GraJf, MD, New Britain General Hospital
Threatened Abortion: A Prospective Study of Predictors of Out-come in an Emergency Department Population, Jean Abbott,MD, University of Colorado
Predictors of Electrolyte Abnormalities in Elderly patients,Bctnita M. Singal, MD, University of Cincinnati
Symptom Severity in Acute Myocardial Infarction and its Ef-fect on Patient Delay and Use of 9l | , Mary T. Ho, MD, (Jniver-sity of Washington
27 .
Frequency Analysis of the Electrocardiogram in Humans DuringVentricular Fibrillation, Roger D4wonczyk, pE, Ohio StateUniversity
The Diagnostic Impact of Prehospital l2-Lead Electrocar-diography, ktm P. AuJilerheide, MD, Medical College oJWisc'onsin
A Computer Based Time-Insensitive Predictive Instrument forPredicting Myocardial Infarction in the Emergency Depanment,Charles B. Cairns, MD, Harbor-IJCLA
Comparison of Creatine Kinase and CKMB in Emergency Depart-ment Patients Admitted to Rule Out Myocardial Infarction, GaryP. Young, MD, Portlarul Veterans Administration Medical Center
Squamous Cells as Predictors of Contaminated Urine Culture.F-rank G. Waltcr, MD, Valley Medical Center
28. Stab Wounds of the Chest: Uti l i ry of the Expiratory ChestRadiograph Alone, Sric A. Heine, MD, Medicat Collexe ofPennsylvunitt
Detection of Sofi Tissue Foreign Bodies by plain Radiography,Xcrography, Conrputerized Axial Tomography and Ultrasono-graphy, Georgc L. Ellis, MD, University rl'Pittshurgh
Portable Ultrasound in Patients with Suspected Cholecvstitis: Per-lirrmancc ancl Interpretation by Emergency Department Physi-cians. Lcon Gussow, MD, Cutk County Hospitul
Passive Hemagglutination Inhibition Test filr Diagnosis of BrownRecluse Spider Bite E,nvenomation, Steven M. Burrctt, MD,Universitv ol Oklafutma
32. Standard Formulation of Nitroglycerin Ointment and Hot packsl irr Venous Dilat ion in Pediatr ic Intravenous Access. Mark C.Clark, MD, Univcrsitv of Pennsvlvania
Ketanrine Sedation Protocol fbr Emergency Pediatric Pmcedures,N. Eric Johnson, MD, MPH, ktmu Lirula Univer,sitv
34. Inrpact ol ' the HIV Epidernic: Emergency Department ResourceUti l izat ion by Patients with Known Human ImmunodeficiencyVirus (HIV-l) Int'ection, Gary Johnson, MD, Johns HopkinsUniversitv
35. Emergency Department Compliance with a Standard for theManagement ol' Patients with Uncomplicated Recurrent Convul-sions, lzrrrl' J. BaralJ', MD, UCLA
Adherence to Universal Precautions by Health Care providers per-firrming Emergency Interventions in an Inner-City EmergencyDepaftnrent, Thomns DiGiovanna, MD, Johns Hopkins lJniversity
Prevention of Disease Transmission by Using Mouthto-MaskVentilations During CPR, PatrickJ. Connor, MD, NorthwestemUniversity
Incidence of Reported and Confirmed Risk of Exposure to Com-municable Disease in an Urban EMS System, Peul E. Pepe, MD,Baybr College of Medicine
The Persistent Problem of Tetanus, Lisa Grininger, MD,Harbor-UCI-4
40. A Prospective Study Examining the Need for Coverage for VibrioOrganisms in Salt Water Contaminated Wounds, Jonathan S.Olshaker, MD, Naval Hospital, San Diego
41 . Management of Pyelonephritis in an Oberservation lJnit, GeorgeL. H. I&trd, MD, Universiry of Mississippi
12. Observation Unit Treatment of Pyelonephritis, ft. Scott Israel,MD, Capt., USAF, Wilford Hall USAF Medical Center
L . )
24
25.
26.4 .
29
t0
I I
l L .
l 3
1 5 .
I 0 .
6 .
1 9 .
3 1 .
.) -)
t 4
36
31
38
39
1 6 .
l 7
1 8 .
20.
21 .
22
t 4

43
44
- ? 'o " iPoster Session II - Wednesday, l'.4lay 24 i ,a
C ) J
Poison Control Centers Are Cost Effective, Robert L. Galli,MD, UCLA
A New Drug Screening System "Multi-HPLC" by High per-formance Liquid Chromatography Using Multi-Wavelength UVDetector, Shinichiro Suzaki, MD, Nippon Medical School,Tokyo, Japan
Multiple Dose Charcoal Therapy for Salicylate Poisoning, MiltonTenenbein, MD, University of Manitoba
In Vitro Absorption Properties of Activated Charcoal withSelected Inorganic Compounds, Rosalind D. Mitchell, MD,University of Southern California
Role of Activated Charcoal and Sodium Polystyrene Sulfonate(Kayexalate) in Gastric Decontamination for Lithium Intoxica-tion: An Animal Model, James G. Linakis, MD, Chitdren'sHospital, Boston
Rate of Absorption of Iron From Chewable Tablets, Jumes P.Winter, MD, Hennepin County Medical Center
Clonidine Poisoning in Young Children, Jomes F. Wilelt, II,MD, Children's Hospital oJ' Philadelphia
Dimethyl-PGE2 Prolongs Survival From Alpha Amanit in,Edward A. Michelson, MD, University ofPittsburgh
Empiric Use of Naloxone in Patients with Altered Mental Status:A Reappraisal , Jerome R. Hofiman, MD, UCLA
Endotracheal Naloxone in Rabbits: No Adverse Effects on BlotxlGases and Lung Tissues, Stephen C. Rector, MD, We* VirginiaUniversity
Pharmocologic Interventions in Acute Cocaine Toxicity, MarcSmith. MD. Harbor-UCL4
Agents Which Protect Against Cocaine-lnduced Death andSeizures in Animals, Robert W. Derlet, MD, University d'California, Davis
Life-Threatening Events After Theophylline Intoxication - AProspective Analysis of 144 Cases, Michael Shanrun, MD,MPH, Children's Hospital, Bostctn
56. Init ial ECG Findings in 187 Cases of Cycl ic AntidepressanrOverdose, Frank W. ktvoie, MD, University ti'ktuisville
China White Epidemic: An Eastern United States EmergencyDepartment Experience, Marcus L. Martin, MD, Medical Col-lege of Pennsylvania, Allegheny Campus
The Effect of Electric Shock Therapy on Local Tissue Reac-tion to Poisonous Snake Venom Injection in Rabbits, Cassan-dra Stroud, MD, Orbndo Regional Medical Center
Acute Iron Poisonings in Children: Evaluation of the predic-tive Value of Clinical and Laboratory Parameters - lVithdrawn
Polymyxin B for Experimental Shock From Meningococcal En-dotoxin, Greg Baldwin, MD, Children's Hospital, Boston
Bacteremia in Children with Otitis Media, Sara A. Schutz.man,MD, Children's Hospital, Boston
An Evaluation of the Emergency Department Treatment of StatusEpilepticus in Children, Steven A. Phillips, MD, StanfordUniversity
Staples Versus Sutures for Wound Closure in the PediatricPopulation, Susan M. Dunmire, MD, University of Pittsburgh
Six Years Experience in the ED Resuscitation and ICU Treat-ment of Drowning: Patient Characteristics Predictive of Out-come and Evaluation of Conservative Management, Janekwelle, MD, Children's Hospital of Philadelphia
Comparison of Serum Phenobarbital Levels After Single Ver-sus Multiple Attempts at Intraosseous Infusion, Michael Choo,MD, St. Vincent Medical Center
Comparison of Intravenous and Intraosseous Administration ofEpinephrine in a Cardiac Arrest Model, Steven G. Crespo, MD,Medical College of Pennsylvania
Comparison of Intravenous Intraosseous, and Intramuscular Ad-ministration of Succinylcholine in Sheep, Steven Pace, MD,Madigan Army Medical Center
Comparison of Intraosseous Versus Intravenous Loading of Pheny-toin in Pigs and Effect on Bone Marrow, Paul J. Vinsel, DO,Cpt. MC, Darnall Army Community Hospital
Criticaf lrssons from Prehospital Pediatric Cardiac Arrest, RobenF. Itrvery, BA, MICP, New Jersey Trauma Center
Caretaker Neglect and Injury Prevention Instruction fbr PreschoolChild Injuries: 475 Consecutive Cases, David M. Cline, MD, EastCarolina University
Variables Predicting the Need for Major Procedures DuringPediatric Critical Care Transport, Karin A. McCloskey, MD, Har-vard Medical School
Pediatr ic Risk of Mortal i ty (PRISM) Score: A Poor Predicror inTriage of Patients fbr Pediatric Transport (PT), Richard A. Orr,MD, University of Pittsburgh
The Association Between Scene Time, Prehospital Procedures,and Injury Severity Parameters Among Severely Injured Patients,David Tse, MD, University oJ'Arizona
The Elfect of Alcohol Consumption on the Outcome of Motor-cycle Accident Victims, Janet Williams, MD, Meelical Collesertf Pennsylvania, Allegheny Campu.s
Comparison of Complication and Mortality Rate Between DirectTrauma Admissions and Transfer Trauma Admissions to a RuralTrauma Center, Dale A. Albright, DO, Geisinger Medicul Center
Etfect of the 65 MPH Speed Limit Change on Mortal i ty andTrauma Severity in Mokrr Vehicle Accidents, David P. Milz.rutn,MD, Eastern Virginia Graduate School of Medicine
Control l ing For Severity of Injuries in Emergency MedicineResearch: Iss vs. Triss, C. Gene Cayten, MD, MPH, New YorkMedical College
E,volution of Trauma Care, A County Experience, Gerardo A.Gomez, MD, University rl'Miami
The Failure of Trauma Systems in Southern California to AffectDeath Rates From Mokrr Vehicle Accidents, Joseph Morales, MD,University oJ Southern Califurnia
EMS Field Triage Based on Tiered Categorization of HospitalEmergency Department and Acute In-Patient Bed Availability,Barthoktmew J. Tortella, MD, Universitv tf Medicine & Den-tistry of New Jersey
Factors Influencing the Operational Saf'ety of Aeromedical Heli-copters, Ronald B. lnw, MD, University of Chicago
Ef'fectiveness of Cervical Spine Stabilization Devices Measuredby Accelerometry, Ahimsa P. Sumchai, MD, Palo Alto VeteransAdministration
Transient Neurologic Deficits Without Cervical Spine Fractureor Dislocation Following Blunt Trauma, Phil B. Fontanarosa,MD, Maryland Institute for Emergency Medical Services System
The Impact of a Cervical Spine Radiographic Protocol on CostAnd Prophylactic Spinal Immobilization , Robert J. Schwartz, MD,MPH, HartJord Hospital
Indications for Head CT Scanning in Trauma Patients, John C.Fitzpatrick, MD, UMDNJ-Roben Wood Johnson Medical School
Concomittant Femur Fracture and Head Injury: A Reliable In-dicator of Visceral Torso lnjury , Constantinn Pippis , BS, UMDNJ-Robert lltood Johnsr.tn Medical School
The Value ofAlkaline Phosphatase in Peritoneal Lavage, StephenM. Megison, MD, University of Texas Southwestern MedicalCenter at Dallas
66
67
68
69.
70 .
7 t .
72 .
73 .
t + .
75 .
'76.
17 .
78 .
79.
80.
45.
46
47.
4 8 .
49
50
52
53
54
55
5 1 .
8 l
82.
84
85
86
57 .
58
59.
60
6 1 .
62.
o J .
64
l 5
65. 87

i
l
88.
Poster Session III - Thursday, May 25Clinical Comparison of Resuscitation and Survival Rates for1980 and 1985 ACLS Protocols in Out-of-Hospital VentricularFibrillation Cardiac Arrests, Ford C. Erickson, MD, HennepinCounty Medical Center
Defibrillation by Intermediate EMTs: The Illinois Prolect,Kathryn L. Mueller, MD, University of Colorado
Transtelephonic Defibrillation, Jay S. Feldstein, DO, MedicalCenter of Delaware
Dangers of Defibrillation: Injuries to Emergency Personnel Dur-ing Patient Resuscitation, Waruen Gibbs, MD, University ofWashington
Morphology of Myocardial Necroses After 15 or l7 Min VFCardiac Arrest and Cardiopulmonary Bypass in Dogs, AnnRadovsky, PhD, DVM, University of Pittsburgh
The Effect of Bolus Injection on Circulation Time During CPR,Charles L. Emerman, MD, Cleveland Metropolitan GeneralHospital
Effects of Arterial and Venous Volume Infusion on CoronaryPerfusion Pressure During Canine CPR, Nina T. Gentile , MD,Henry Ford Hospital
The Effectiveness of Bystander CPR in an Animal Model, JamesHoekstra, MD, Ohio State University
Left Ventricular Volume and Aortic Flow Relationships Dur-ing High-Impulse Cardiopulmonary Resuscitation: ImplicationsRegarding Mechanism of Blood Flow , James E. Manning, MD,Harbor-UCl,A
Failure of Fructose-1, 6-Diphosphate to Promote Increased Sur-vival or Neurological Protection Following Resuscitation fromExperimental Cardiac Arrest, Robett E. Rosenthal, MD, Georgell'ashington Univers ity
No Improved Outcome After Prolonged Cardiac Arrest andTreatment With Excitatory Neurotransmitter Receptor BlockerMK-801 in Dogs, Fritz Sterz, MD, University of Pittsburgh
Influence of Epinephrine and Norepinephrine on ArteriovenouspH and Carbon Dioxide Gradients During CPR, Karl H. Lind-ner, MD, University of Ulm, West Germany
100. Effects of Epinephrine and Norepinephrine on Cerebral OxygenDef ivery and Consumption During CPR, Karl H. Linder, MD,University of Ulm, West Germany
l0l. Transcranial Doppler Determination of Cerebral Perfusion inPatients Undergoing Cardiopulmonary Resuscitation: Metho-dofogy and Preliminary Findings, Lawrence M. lzwis, MD, St.Lrtuis University
102. The Prognostic Value of the Glasgow Coma S,oale Measured24 Hours After Inpatient Single Cardiopulmonary Arrest andResescitation, Bruce M. Thompson, MD, Henry Ford Hospital
103. Inadequate Airway Management Compromising EMT-I Auto-matic Defibrillator Use, Graham Billingham, MD, UCLA
104. Adequate Ventilation Using a Mask and Bag While Maintain-ing Cervical Neutrality, Wendy Delaney, MD, State Universityof New York - Will be presented on May 23rd
105. Asthmatic Cardiac Arrest: An Indication for Empiric BilateralTube Thoracostomies, Elaine B. Josephson, MD, Henry FordHospital
106. Pre-Hospital Use of Inhaled Bronchodilators in Reversible Air-way Disease, Irene Machel, MD, Moristown Memoial Hospital
107. Prehospital Administration of Inhaled Metaproterenol, DavidR. Eitel, MD, York Hospital
108. Comparison of Two Delivery Methods of Albuterol in TheEmergency Department Management of Acute Asthma, FrancoisR. LtFleche, MD, Eastem Virginia Gradunte School of Medicine
Utility of the Peak Expiratory Flow Rate in the Differentiationof Acute Dyspnea: Pulmonary Edema Versus Obstructive/Bronchospastic Disease, David Cionni, MD, Medical College ofPennsylvania
Innovations in Aminophylline Monitoring and Therapy, Dr.Russell J. Kino, Australasian College of Emergency Medicine
Impact of Portable Pulse Oximetry on Arterial Blood Gas Analysisin an Urban Emergency Department, Cynthia A. Cofer, MD,University of Tennessee
Aspiration During Manual Low Frequency JetYentilation, DonaldM. Yealy, MD, University of Pittsburgh
Emergency Intubation in the Uncooperative Trauma Patient,Joseph J. Kuchinski, Jr, DO, Philadelphia College of OsteopathicMedicine
The Value of End-Tidal C02 Measurement in the Detection ofEsophageal Intubation During Cardiac Arrest, Assaad J. Sayah,MD, William Beaumont Hospital
Core Temperature Measurement in Hypovolemic Resuscitation,Robin W. Nicholson, MD, University of Arizona
Exsanguination Cardiac Arrest in Dogs: Pathophysiology ofDying, Samuel A. Tisherman, University of Pittsburgh
Exsanguination Versus Ventricular Fibrillation Cardiac Arrest inDogs: Comparison of Neurologic Outcome Preliminary Data,Samuel A. Tisherman, University of Pittsburgh
Norepinephrine in Hemorrhagic Shock, Peter F. Van Ligten, W,Ohio State University
Isosolute Comparison of Intraosseous (IO) NaCl/6% DextranT0(HSD) to lO 0.9% (NS) in a Hemorrhagic Shock Model,.IoftnA. Marx, MD, Denver General Hospital
Rapid Correction of Severe Hyponatremia Results inBrain Protein Oxidation, and Altered Blood Chemistries,S. Mickel, MD, National Institute of Neurological DisordersStroke
Cardiovascular and Neurohumoral Responses Following Burnjury, Ralph L. Crum, MD, University of Califurnia, San
The Significance of Neutrophilia in Afebrile Elderly Patients,ward A. Michelson, MD, University of Pittsburgh
Oral Labetalol vs Oral Nifedipine in HypertensiveAlison J. McDonald, MD, University of Pittsburgh
Cardiovascular Side Effects of Emersencv Intravenous
Supraventricular Tachyarrhythmias and Rate-Related Hsion: Cardiovascular Effects and Efficacy of IntraVerapamil, Bruce E. Haynes, MD, Harbor-UCl,A
Efficacy of Pseudoephedrine in the Prevention of MiddleSqueeze, Michael Brown, MD, Butterworth Hospital
A Safety Assessment of High-Dose Narcotic AnalgesiaEmergency Department Procedures, William G. Barsan,U niv e rs ity of C inc innat i
128. Intranasal ButorDhanol for the Treatment of Moderate toMuscufoskeletal Pain, James Scott, MD, GeorgeUniversity
129. Exposure of Emergency Medicine Personnel to Ionizingtion During Cervical Spine Radiography, Craig M. Singer,UCLA
89.
90.
9 l
92.
93.
94.
95
96
97.
98
99.
130. A Radiographic Evaluation of Variousmobilization, James Scott, MD, George
Methods of AnkleWashington
l3l. Radial Artery Catheterization of Critically Ill PatientsEmergency Department, Gregory F. Bachhuber, MD,County Medical Center
t 6

Abstracts of the 1gth Annual Meeting of thesociety for Academic Emergency Medicine.Study done primarily by a resident.Edttor's note: The following 276 trbstracts wil l be ltresentecl at the Annual Meeting of the SocietyMedicine in S-an Diego, May 22-25. Presenters' nirrn", are printcrl in italics; *Lti| pr"rriti, t,specified by the authors.
Poster Presentations Radiograph ordering: Triage nurse versus physician
No.2 1 2'16
1 71 81 2241 2
Al l radiographsAnkleKneeFingerWristChestAbdomen
Sensi l iv i ty.7385.88.67.67.21. 1 7
f or Ac ad entic Em er gencynot indicated, none was
PPV Kappa.74 .65' 91 87.78 .83100 . 79.80 .72.50 .?8.50 .24
1 'Frequent Fliers'- A Protocol for the Management ofFrequent Visitors to a Community Hospital EmergencyDepartmentA Schuckman, PB FontanarosalDepartment of EmergencyMedicine, Northeastern Ohio Universit ies College of Meditine,Akron City Hospital, Akron
Most emcrgency dcpartmcnts havc p:r t icr . r ts who prcscnt f rc_clucnt ly , account for a substant ia l nr-rmbci of rcpcat v is i is , and of tcnhavr t ' i thcr rn inor cor lp la ints ur major dernani ls . Encountcrs wi t l . rsuch " r eg ,u l i r r s " r n i r y b t ' d i l f i cu l t , l r us t r a l i l r g , anJ t i r r r e - consL r r l i ngtor thc cmL.rscncy physic ian. Wc prcscnt a mcthod for man:rgcmcntof paticnts with frcclucnt ED visits, or ,,frcclucr-rt flicrs.,, Tl-rc stcpsfor . implerncnt ing thc program incluclc pat i "nt ic lcnt i f rcat ion, cs,tablisl-rrncnt of a con{iclcntial filc, cnsunng thc diagnosis, :lrrangc_mcnt of fo l low-up and cont inr_r i ty of carc, pcr iodic ' i i lc rcv icw andupdatc, and staf f cducat ion. Thc major i ty o i pat icnts havc a historyof onc or morc of thc fo l lowrng: chronic pain syndrume, bordcr l incpersonalrty, psychiatric disordcr, chronic rncdical problcms, drr-rg_secking bchavior , drug zrbr-rsc, or a lcohol ism. pat icnis wi th f rcq LrcntED vis i ts for acute rncdical problcms, such as s ic l< lc cr l l t l isctrse,chronic obstruct ivc pulmonary c l iscasc, or posi t ivc HIV ant ibot ly ,are also includcd. Thc namcs of a l l f rcc lucnt f l icrs arc kcpt on'acomputcr izccl l is t that is upclatccl cvcry two months. Each j rat icnthas a confidcntial filc, _availablc only tir tl-rc crrcrgcr-rcy physician,that contains copics of thc rccorc ls f rom prcvioui .ED'v is i is a longwith a transcribcd sumrnary of ED diigr-roscs, trcat,.,-,",-,1, ",..,Jaf tcrcarc p lar-rs. Inforrnat ion conccrning mccl icai , socia l , psycho-logical , ancl lcgal intcrvcnt ion is a lso includcd. Thc f i lcs arc r i ra in-ta incd by onc. intcrcstod physic ian who, whcn avai lablc in t l rc ED,cvaluatcs ancl t rcats thosc pat icnts. Thc physic ian also rcvicwsprcvious hospi ta l rccords, corurnunicatcs wi th the pat icr- r ts , prcvi_ous and currcnt physic ians, formulatcs pat icnt carc p lans, i i lcnt i_f ics a cont inui ty of carc physic ian, coir fcrs wi th fami l ics, ar-rd,whcrc indicatcd, involvcs lcgal author i t ics {such as thc narcot icsburcar-r.or child protcctivc scrviccs). Erncrgcncy physrcr:rns, r.r urscs,counscl lors, and socia l workcrs must bc knowlcdgcablc of thcsystcm and prcsent a r - rn i f ied and consistcr-r t appi t rach to thepaticnt. We havc usccl thc frccluent flier prograrn ovir thc past fouryears, clccreasing the numbcr of paticnti with n-rorc thar-r i0 visitsper ycar f rorn 30 pat icnts in l9B4 to two in 19g7.
-2. Radiograph Ordering: Agreement Between the TriageNurse and Physician in a pediatric EmergencyDepartmentL Ropp, R Blouin, C Dulberg, M LilChildren's Hospital of EasternOntario, and Department of Epidemiology, Universrty of Ottawa,Ottawa, Ontario,
Techniqucs to rcduce paticnt waiting time arc of impurtance inbusy emcrgency departmcnts. Wc hypothcsizccl that thc triagcnurse in a busy pediatric ED could accuratcly ordcr radiographi,thus rcducing patient waiting timc. AII patients registering'aithcED of thc Children's Hospital of Eastcm Ontario in a onc-wcckperiod were entered into the study. A study form was attachccl toeach chart at rcgistration. It was rcmovcd and cornplctecl by thctriage nurse prior to the physician seeing the chart. Thc triagc nursedoc.umented whethcr thcy would send ihe patient for a radlographif allowcd-to. If a radiograph would have bccn ordcred, do.r-c.,ir-tion was donc as to the function deficit, swelling, deformity, andspecific.radiograph desired. The radiographs thit wcre aciuallyordercd by the physicians wcre subseqt cnily obtaincd. Data wercanalyzed for agrecment beyond chanci {kappa), sensitivity, speci-.f ic i ty , and posi t ive (PPV) and negat ive pr id ict ive values. 'Racl io-graphs o_rdered by the emergency physician were uscd as the goldstandard.
Tr iage nurses showct l good agrccmcnt wi th physic ians in thco r t l e r i t r g o f ( x t I c l l l i t y I i l ( l i r )A r i t l l l s .
3_Emergency Department Medical Record euality -Measured by lmplicit and Explicit Methods in anAcademic SettingAB SoslowlDepartment of Emergency Medicjne, WorcesterMemorial Hospital, Worcester, Massachusetts
Controvcrsy st i l l cx ists i r - r thc f ie ld of 11r-ra l i ty of care asse ssr .ncnras to thc correlat ion bctweurr thc adct lu, tcy ( ) f t l te rncdical rccordancl pat icnt outcol lcs. Str- r thcs drs,rgrec as to thr t lual i ty 0f carcrcndcrccl , ba.sct l on rctrospcct ivc chart aut l i t , c lcpcndi i tg orr 'whcthe rimp l i c i t ( sub j cc t i v c ) o r cxp l i c i t { ob j cc t i v c ) c r i i c r i a a r c uscc l . Th i sstu( ly was cont luctccl at thc cncl of an acaclcrnic ycar (March to f uncl91313) at a t ra jor , ,130-bcd r- r rban tcachir- rg af f i l ia tc of thc Univcrs i tyof Massachusct ts Mcdicai School whosc LcveI U cnrcrgcncy dcpart_rurcr . r t , s taf fcc l by 24-hor-rr at tcncl ing physic ians, hor, rscstai f lc i rcr-gcncy nrccl ic inc ancl intcrnal n-redic inc) , anr l nursc prr tc l r loncrs/cvaluatcs rr rurc rhan 30,(XX) pat icnts an' r , ra l ly . Thc stL idy. , , , . , . ,1. , r r . r ' ithc congrucncy bctwccn an cxpl icr t ancl : rn i r .npl ic i t crr t . r ia ep-pnrach v is- 'a-v is two cont l lon ancl l totcnt ia l ly scr iotrs pat tent col l -p la ints - chcst pain ancl abckrnr in i l pain. ED rccorc ls 'of ranclonr lysclcctccl pat icnts {13 to 89 ycars o l i l ) who prcscntccl wi th coni_p l i t i n t s o f chcs t pa in ( 142 ) ; r n r l r r h tL , r r r 1 , . , . r ' l r r r i n { 159 ) anc l wc rcsubscclr - rcr t ly cLschargccl c ' ' rpr iscd thc str t ly p.pr- i la t i . . . l \cc.r r lswcrc gradcd by di f fcrcnt nonblr t rc lcc l dcpartntcnfal i r t tcnding phy_sic ians, as part of our dcpartrncntal eA progranr, r , rnawarc , l f thcstucly t lcs ig 'or intcnt / as t . thc 1. , rcsct ' rcc i , . , thc n-rcdical rcc.rc ls. fspe c i f ic l - r is tor ic i r l and cxaminat ior e lcnrcnts {objcct ivc) , anci l larylaboratory/racl iographic usc, and ovcral l adcquacy of thc historyanr. l cxaminat ior-r (sr- rb jcct ivc) . Physic ians did dot sc l f graclc. A 10,1,s l rbsct of t i rc stucly samplc dcrn. .st ratccl an intcr .bscrver Dosr.vcc.rrc lat i . r . r . f 0. t i4. A po.s i t ivc c.r rc lat ion (r = 0.13 l , abr i t rnr i r i r r l prr in;r = 0;78, chcst pain l , indcpcnclcnt of thc provic lcr ur c i thcr c l in icaicondi t ion, cxrstccl bctwecn thc cxpl ic i t scorc ancl thc sub;cct ivcscore. . Thcrc wcrc s igni f icar"r t c l i f fcrcnccs bctwccr-r ancl arrongattcndir - rg physic ians, nursc pract i t ioncrs, and al l houscstaf f lcvcl ias to thci r n ' rcc l ical rccord 'qual i ty ,"
br-r t ovcral l , at tcncl ing physi-c ians scorc_d l - r ighcr than l - rouscstaf f and nurse pract i t ioncis 'whcncomparcd by thc expl ic i t approach. Thcrc wcrc fcwer but st i l ls igni f icant d i f fcrcnccs in thci r grading whcn asscsscd by thc sr-rb iec_trvc approach.
4 A Dictated and Transcribed Medical Becord Can BeCost EffectiveHA Stueven, D Tonsfeldt, E Cisek, K Hargarten, p Aufderheide/Milwaukee County Medical Complex, Medical College of Wisconsin,Milwaukee
A dictatcd and transcribcd emcrgency dcpartment record pro-vides an rmprovcd rncdicai/ legal/bi l l ing doiurncnt with a morep.rofessional appearance. A major concern has been raiscd regardingthe cost of that transcribcd rncdical record. Our ED Lad anexpcriencc with a computcnzed and dictatcd nredrcal rccord for atwo-y_car pcriod. The Dictaphonc" data bank and transcriptronrstswerc located rn the ED. The rccord was transcribcd onto an IBM "-AT computer using Mult iMatc- softwarc with f ixcd hcacl inss. The
t 7

Imean dictat ion t rme was 2.4 x 1.3 minutes wi th a record length of214 + BB.6 words. Transcr ipt ion was in i t ia l ly provided 16 hours perday, seven days per week. Our average ED record could becompleted every eight minutes, with a well-trained transcription-ist producing seven records per hour. In an optimal system theaverage cost per record wi l l be approximately $1.25. To evaluatethe effectiveness of the system for reimbursement purposes/ oneyear of billing data was reviewed for distribution of level of servicebcforc and af tcr inst i tut ion of the dictat ion system and mul t ip l icdtimes current charges {or both periods. The avcrage increase inphysic ian charges as a rcsul t of d ictat ing was $17.30 per record.Thc transcrrption cost was easily offset by the increasc in docu-rncnted level of scrvice. We believe such a system can be costcf fcct ive.
5 Emergency Department Patients With PID: Do TheyUnderstand Their Diagnosis?B Abbuhl, S Stemhagen, E Campbell /Emergency ServicesDepartment, Hospital of the University of Pennsylvania,Philadelohia
Pelvic inf lammatory dlsease (PID) is a frcquent problem incmcrgency departments and outpatient cl inics, with at least oncmil l ion women a year bcing treated for PID in the United Statcs.Thc projected annual cost of PID and i ts sccluelae wil l total $3.5bi l l ion by 1 990. For many PID paticnts, thc ED is thcir f i rst contactwith medical care. Control of this cpidemic recluires that EDpationts understand their diagnosis and comply with medicalrccommcndations and fol low-up. A prospcctive telephone surveyof womcn discharged from thc ED with PID was initiated todetcrminc levcl of understanding of the diagnosis and its potentialconscclucncos and thc self-reported compliance rates with mcdica-tion and follow-up. Of thc 90 patients contacted, we found that2L)% did not know that PID was an infection of the femalereproductivc organs and less than half knew at least two of the fourrnajor cornplications of PID. There were no apparent predictors ofundcrstanding, including levcl of schooling, prior episodes of PID,or using the ED as a primary sourcc of medical care. Patients'undcrstanding of thcir diagnosis was signif icantly associated withknowing the cornplications of PID but not associated with eithershort-tcrm compliance or satisfact ion with care. We also assessedpaticnts' understanding of a Pap smear and found that 47% couldnot dcscribe thc test or its function. Even more alarming, 46lo ofour paticnts thought they had a Pap test at their recent ED visit,whcn, in fact, they had not. This study points to a significant lackof understanding in ED PID patients regarding their diagnosis, itspotcntial complications, and use of the Pap smear. Possible inter-vcntions appropriate for EDs are discussed.
.6 AIDS Education in the Emergency DepartmentD Magid, A Behrman, A Stemhagen, S Jacobson/Department ofCl in ical Epidemiology, Emergency Department, and EmergencyServices Deparlment, Hospital of the University of Pennsylvania,Phi ladelphia
Preventing the further spread of AIDS depends on educating thepublic to reduce the risk of infection. This study describes AIDScducation in a unique setting and represents one of the few AIDSeducation programs that have been validated by controlled testing.To test the hypothesis that effective community AIDS educationcan be based in an ED setting, we designed and evaluated twoeducational interventions in an urban, high-volume ED waitingroom. Eight hundred subjects (patients and visitors) completed apreintervention knowledge, attitude/ and behavior survey. Thesubjects then were assigned to one of three groups: an active groupexposed to a videotape, written material, and a preceptor for reviewand questions; a passive group exposed to a videotape and writtenmaterial only; and a control group without access to our educationprogram. Long-term knowledge gains and reported risk reductionbehavior were evaluated by follow-up testing within a five-weekperiod. Complete follow-up was achieved for 78% of subjects. Thecost-benefit of each educational program was evaluated. Signifi-cant knowledge gains were found between each of the two inter-vention groups when compared with the controis {P <. .01). Theactive group demonstrated greater knowledge gains than the pas-
sive group {P < .05). Significant reductions in reported high-risk be-havior were found in both intervention groups compared withcontrols (P < .01). This study demonstrates that an ED-based AIDSeducational program can have a significant impact on improvingknowledge and on reducing reported AIDS risk behaviors in a high-risk population.
7 Emergency Physician Responses to FamiliesFollowing Patient DeathT Schnidt, SW Tolle/Departments of Emergency Medicine andMedicine, Oregon Health Sciences University, Port land
Stress for physicians in response to a patient death in the emer-gency department is assumed to be great, but there are no studresaddressing this phenomenon. Studies of the family's response to anED death suggest that survivors are left with unanswered questionsand unmet needs. We developed a questionnaire to evaluate physi-cian responses at the time of patient death and their subsequentinteraction with survivors. Questionnaires were sent to 138 Ore-gon emergency physicians and completed by 83% {115). Compari-sons were made with a previous study of primary care physiciansin the state using matching questionnaire items. The mean numberof dcaths encountered by emergency physicians was l7 (SD 1 15)per year. At one hospital this number was verified by an independ-cnt audit of the number of ED deaths. Emergency physicians weremuch more likely than primary care physicians (71% vs 29%) toask survivors to come to the hospital so they could be notified inperson {chi-square; P < .0001 ) and reported spending a mean of 15.5minutes {SD t 10.8) with survivors. Notifying these survivors isconsidered emotionally difficult by most (70%) emergency physicians surveyed. Outreach by all providers was relatively infre-quent. Five percent of emergency physicians and 7"/o of primarycarc providers routinely sent sympathy cards. Only 3% of emer-gency physicians routinely made a follow-up call versus l9% ofprimary care physicians, and 7"/o routinely called with autopsyresults versus 77% oI primary care physicians (chi-square; P <.00011. We conclude that survivors and physicians would benefitfrom ED bereavement programs that help emergency physiciansprovide outreach to families after a patient death because 94% ofphysicians reported a need for education in this area but less thanhalf reported obtaining that training. Instituting these programsmight raise emergency physician job satisfaction and potentiallydecrease liability by increasing the physician-family bond withsurvivors.
.8 Teaching Ethics in Emergency MedicineZ Srodulski, J Jones, J Dougherty/Department oJ EmergencyMedicine, Butterworth Hospital, Michigan State University Collegeof Human Medicine, Grand Rapids; Department of EmergencyMedicine, Akron General Medical Center, Akron, Ohio
There has been a sharp increase in recent years in the variety andcomplexity of ethical problems in the practice of emergencymedicine. To determine the extent of formaiized training ioremergency medicine residents in this area, we surveyed aII USresidency program directors. The data received from the replying 69of 73 residencies in operation for more than one year are summa-rized. Although 6B program directors believed that medical ethicsshould be part of an emergency medicine residency curriculum,only 42 {61%) had any specific teaching dedicated to this subiect.The mean number of hours per year spent teaching ethical issueswas six (range, one to 20|. This time is generally subdividedbetween didactic lectures (33%|, group discussion (25%), bedsideteaching l24o/o), assigned reading llI%1, and case presentationsl7%1. Of the 27 139'/"irprograms surveyed without medical ethicsincorporated into their existing curriculum, l4 anticipated addingthis subject to their program in the near future. Specific ethicalissues that were considered important for inclusion into the cur-riculum were informed consent, confidentiality, resuscitation de'cisions, duty to treat, rights of minors, patient transfers, and organdonation. Frequent suggestions by program directors included theneed for more formal teaching in medical ethics, use of problem-based learning activities/ organized reading lists, and medicolegalseminars. The data generated by this study reinforce the need forimproved training in medical ethics among endorsed emergencymedicine residency programs. Innovative teaching methods aresuggested.
9 Problem-Based ACLS Instruction: A ModelApproachfor Undergraduate Emergency Medical EducationRF Polglase, DC Parish, RL Buckley, RW Smith, TA Joiner/Departments of Internal Medicine and Family Practice, MercerUniversity School of Medicine and the Medical Center of CentralGeorgia, Macon
The optimal {ormat for teaching advanced cardiac iife support{ACLS) to medical students and others with little emergencymedicine experience has not been studied extensively. We reportan ACLS course taught to sophomore medical students using a
l 8

problem-based learning model. Thc lecture format was replace d bva ser ies of c l in ical problcms emphasiz ing var ious port ions of theACLS coursc. Students met weekly wi th an ACLS instructor whoserved as a tutor to d iscuss the problem. A set of learning object ivcswas compiled for the entirc coursc and givcn to students to guidctheir s tudies. Enhanced pract lce t ime t [at inc ludcd teachins sta-t rons and ski l ls laborator ies was of fered. When tcsrcd, . t r ' ,d.nt ,from the problem-based program performecl bcttcr than seniormcdical students from a tradrtional ACLS course that we tausht inthc same timc framc. We concludc that thc rrroblem-based forn-ratis an cf fect ive forn-rat for teachrng ACLS tr i thosc who havc hadl i t r l c p r i o r expc r i ence i n emt . r gcncy me r l i c i ne anJ /o r r e s r r sc i t a r i opat tempts.
ment in pediatr ic t ra in ing included incrcased pcdiatr ic e lect ivcs(19% ), increase d use of chi ldrcn's hospi ta ls l9%), and incrcascd uscof pecLatr ic facul ty {9 ' l . ) . One hundred s ixtyninc recent graduatesconpletcd the survey; 57o/o werc board cert i f icd. Thcy le l t mostuncomfortable wi th newborn resuscrtat ion, Vp shunt problcms,and.hema-tologic or cardiac cmergcncies. problen' rat ic proccduraiski l ls inc ludcd cr icothyrotomy, internal jugular and iubclavianvcin acccss, and suprapubic b laddcr aspirat ion. Animal laborato_r ics wcrc thc prcferred method for s l<r l l , icu. l , ,p, - , ,cnt in vent i lat iontechniques, cnclotracheal rntubat iun, and vcni ,us access. pcdiatr icadvanccd l i fc sr-rpport cer t i f icat ion was uncornmon l l2%1. Fcwgraduatcs {21%) wcrc interestcd in pcdiatr ic t :mcrgcncy mcdic incfc l lowships. Pract icc locat ion was rarc ly inf lucnccd by conf idcnccin. thc managcmcnt of pccl iat r ic cmcrgcncics. Residcncy graduatcsbcl icvc that thcy would bcncf i t f rom incrcascd usc of animallaboratorrcs dur ing rcsic lency t ra in ing. The volumc of pediatnc pa-t icnts and proccdurcs sccn in residcncy corrc latcs wel l wi th thai inactual pract icc. Pcdiatr ic at lvanccd l i fc support c()urscs may pro-v ic lc a uscful mcchanism for n ' rcct ing residcncy t ra in ing ncccl i .
12 Paramedic Physical Assessment and Intervention inChi ldrenNA Schonfeld, K Park, R Lev, AJ Haftel/Department of EmergencyMedicine, Children's Hospital of Los Angeles
This stucly cvaluatccl paramccl ic physical asscssmcnt of c l i i l -c l rcn i r - r thc f ic ld and thc impact of IV l inc inscr t ion on st : rb i l rzat iont imc. A. rct rospcct ivc rcv icw of paramcr l ic and crncrgcncy dcpart_mcnt churts of chi ldrcn t ransportcd by paramcci ics ovcr an l lJ-month pcr iod was pcrforutccl , Four l rundrccl n incty- i ivc pat icnts{agcs I ntonth to l t l ycars) wcrc t ransportcd, 194 for ntcdicalindicat ions and 301 for t rauut t r . Thc rr rosi col ln lon nccl ical com-plarnts wcrc scizurcs ancl rcspiratory d ist rcss. Thc r .ncan r .nobi l iza-t ion t intc intcrval ( t i r - r - rc of a larm to t i lnc at p i t t ic l t t 's s ic lc) was (r .5rninLl tcs, mcar-r stabi l izat ion intcrval {SI) was 12.5 rr r inutes, andr l ]can t ransport t i l rc to thc ED was f i .8 l l l inutcs. Onc hr . rndrcclscvcntccn pat icnts had an IV l i r . rc at tcmptct l , wi th 101 succcssfulinscr t ior-rs ( f l6 '2,) . IV l r r . rcs wcrc at tcr .nptccl ancl sncccssful r .norcof tcn in chi lc l rcn ntorc than l2 months old {1, < .01 ) . Whcn an IV l rncwas at tcmptccl , thc Si i r - rcrcasccl s igni f icant ly to 15.5 nt inr . r tcs {1) <.0001). Thcrc was r- ro s igni f icant c l i f fcrencc bctwccn thc ol l tcol tcof pat icnts of s i r r i lar acui ty who did or d id not havc an IV l incinscrtct l . Four parar.nccl ic f ic ld physical z lsscssmcnt paralrctcrswcrc corrparcd wi th thosc donc by thc rccciv ing ED physic ian:lcvcl of consciousrrcss {LOC), pupi l lary rcact ion, rcspirat( ) ry prr-tcrn, ancl sk in f indings. TI-rc pararrccl ics ancl cmcrgcncy physic ians,: lsscssmcnts agrccd in morc than 50,2, of pat icnts. Thc nr . r r rbcr ofpat icnts for whom di f fcrcnccs occurrcd, l ly p2lranctcr , wcrc LOC(106), pupi l lary rcact ion {13), rcspiratory pat tcrn {30), and skinf indings {72). Whcn a di f fercncc occurrcd, t i - rc r rararrcdic unclcrcs-t in-ratcd thc scvcr i ty of the pat ient s conr l i t i t i r r as fo l lows: LOC( i3 ' l " ) , pupi l lary rcact ion (307,) , rcspiratory pat tcrn {( r0%,) , and skinf indings (53%). Undcrcst imat ion of thc scvcr i ty of thc pat icnt ,sconcl i t ion may rcsul t in wi thholding basic intcrvcnt ions, such asassistcd vcnt i lat ion. Cl in ical asscssmcnt of thc pccl iat r ic pat icntm_ust bc crnphasizcd in paramcdic educat ion to cnsLlrc appropnatcl i fc-saving intcrvcnt ion. Paramcdics arc gcncral ly succci i fu i wi thIV l inc i r - rsert ion in chi ldrcn morc than I ycar o ld, but usr-ra l ly at thccxpensc of longcr f ic ld stabi l izat ion intervals.
13 The lmpact of a Didactic Session on the Success ofFel ine Endotracheal Intubation by ParamedicsTE Terndrup, RA Cherry, CM Madden, RM Cantor, JB McCabe/Departments of Crit ical Care and Emergency Medicine, andPediatr ics, and Paramedic Education, SUNY Health SciencesCenter, Syracuse
While cl inical reports of cndotracheal intubation (ETI) of adultpatients by paramcdrcs dcmonstratc more than 907. succcss rates,reports of prchospital pcdratr ic intubation suggest suboptrmalsuccess rates. Thc small , anesthetizcd cat may be uscd to evaluatcinfant ETI performance. Wc hypothcsized that a bricf drdacticscssion would improve ETI success by paramedrcs. Thirty-ninecertified paramedics with standard training rn adult ETi wererandomized to control or experimcntal groups. Thc expcrimentalgroup (201 reccived a 40-minute lccture emphasizing in{ant arrwayanatomy/ equipment, ETI technique, and monitoring for complica-t ions. Six small (mean weight, 3.2 kg), young (mean age, 5.9months) cats werc uniformly anesthetized with kctamine andaccpromazine. Equiprnent was selectcd from standard ETI matcri-als. Supervisory physicians (fivc) were blinded to group dcsignation
First time pass rates, ACLS testing stationsby student group
Problem-Based (%)( n = 1 1 )
Mega code 90.9Mean writtentest grade 86.8Course passrate 100
Seniors (%) Residents (%)(n=1 8) (n=37)
50 .0 91 .9
83 .3
6 1 . 1
94.6
95.0
10 Analyzing Clinical Case Distributions to lmprove anEmergency Medicine ClerkshipRA Delorenzo, D Mayer, EC Geehr/ Department of EmergencyMedicine, Albany Medical College, Albany, New york
Rccommendations for a corc curriculum for unclcrgracluatcemcrgency medic ine cducat ion have bccn publ ishcd t ry ACEp;rnr lothcrs. I t is expected that a combinat ion of bcdsidc tcachin, : anddidact ic sessions wr11 covcr a l l aspects of thc curr icul lmr, hut rh ishas not been dcmonstratcd. This study clcscribcs a mcthod of usir-rgthc distribution o{ clinical cascs to shapc thc rnix of clir-rical anJdidact ic learning in an emcrgcncy mct l ic inc c lcrkship. Al l scniorstudents part ic ipatc in a four-wcck c lnergcncy rncdic inc rotat ion.A bricf log describing each clinical oncolrntcr is rnaintainccl by thcstLldents. Data frorn one year w(]rc sortcd int0 32 catcgorics aciaptcdfrom thc ACEP guidclines and tabulatcd to dctcrrninc thc distribu-tion of cascs seen by each studcnt. A critcrion of u0,2, of stuclcntscncountering at least ono case in each catcgory was choscn tocnsure a rcasonablc lcvcl of cxposllrc to a particular casc r_rr tr.roic.Onc hundrcd twcnry- three stu j .nts wcrc cxp,rrcd to an avcrrr [c of63 .7 ! ) 7 .5 (SD l pa t i en t s . Scvcn ca t cgo r i c s r nc t t hc c r r t e r i on i 2 t es rs igni f icant at 0.05), inc luding musculoskclcta l i r - r jur ics ( t j .0 t 5.0pat ients pcr studcnt) and abdominal pain (4.( r + 2.U1. Twcntv- f ivcca t cgo r i c s f a i l cd r hc c r i t e r i on , i nc l ud ing u r i nn r y t r c c t i n f cc t i ons(2.6 r 2.O) and head t rauma (1.7 t 1.5) . Rcsul ts indicatc thatexposure to certain categories of patients, with approprratc moni-toring, can bc reasonably cnsurcd rn our clinical sctting. C)thcrcategories occur with insufficient {rectuency ancl dcmand incrcasctldidactic coverage. The didactic portii)n of the curriculum can bcadjusted so that categorics ndt mccting thc criterior-r will bccmphasized whi le those mect ing thc cnter ion wi l l bc dcempha-sized. A method has been descr ibed that ident i f ics gaps in thcclinical exposure of students and permits appropriatc idcntifica-tion of didactic sessions to crcate a clcrkship cxpericncc morcconsistent with recommcnded guidelines.
11 An Evaluation of Pediatric Emergency MedicineEducation: Are the Needs of Emergency Medicine andIts Residents Being Met?RM Cantor, TE Terndrup, M Madden, JB McCabe/Department ofCrit ical Care and Emergency Medicine, SUNY Health SciencesCenter, Syracuse
To ascertain current training of emergency mcdicine rcsidentsin pediatric emergency care, we surveyed al1 emergency mcdicineresidency programs and recent emergency medrcine graduates fortheir imprcssions of the quality of pediatric emergency training re-ceived. Forty-eight (68%) pro€irams returned survcys. They esti-mated 8.4 pediatric encounters per day pcr resident as comparedwith 28.6 adult patient encounters (P < .0001 ). Twenty-four perccntrequ i r ed pcd ia t r i c consu l r a t i on p r i o r r o l a r i cn r d i scha rge . Thcmost common pediatric electives offered were pcdiatric emctgencydepartment, pediatric ward, and NICU. pediatric curriculum foi-lowed core content in 54T" ol programs. Animal laboratories wereused in 75% of programs to teach pediatric skills. Most programdirectors believed that the graduates were competent in the man-agement of pediatric emergencies. Suggestions offered for improve-
t 9

and evaluated equipment select ion, ETI t ime, tubeplacement, and
complicatrons. i*.nty paramedics were assigned to the experi-
-"niri gto"p and 19 io-the control group. Three were excluded
from the'conirol group a{ter randomization. Control subjects were
significantly oldei and had significantiy less estimated ETI experi-
encc (8.4 i 9.5 ETIs versus 34 + (r2) . However, there were no
significant differcnces in the percentage of successfully intubated
ci ts, 57% and 67"1 . l t , r r t ro l and exper imental groups, respec-
t ivc iy. Equipment st : i . ! . ' r , was iudged to be more appropr iate in
s igni i lcant ly more at tempted intubat ions for the exper imental
group, 96% versus U2.5% (P < .051. However, there was no apparent
inc."asc in the success rates when the appropriate laryngoscope, ET
tube, and sty let werc used. Compl icat ions occurred in 50% of at-
tcmptcd intubat ions. Fi f teen percent of successful ETI exceeded 30
." . , -d. of intubat ion t ime. TLe corrc lat ion between thc number of
successful ly intubated cats and years as a paramedic ( r = '24), years
as an EMT (r = .24), and thc number of prcvious ETI ( r = '31)was
poor. Al though a didact ic session improvcs equipment select ion, i t
ii,1 not signiiicantly improvo ETI succcss Educational strategies
mrrst b" icvcloped' to improvc ETI sk i l ls of prehospi ta l providcrs
whcn dcal ing wi th infants.
14 The Effect of an Explici t Airway Protocol on Fl ight
Nurse Behavior and PerlormanceKJ Rhee, RJ O'Malley/Divisron ot Emergency Medicine and Clinical
Toxicology, Department of Internal Medicine, and NursingAdminist i i t ion, University of Cali fornia' Davis, Medical Center,
SacramentoFlight nurscs who arc unaccompanicd by.physicians are otten
called'irn to make important management dccisions under great
tirnc prcssures. This itudy cxamined the cffects of an explicit
dccisiirn tree on thc airway management of patients transportediri,- ttt. sccnc of accident rlr illnesi by comparing the year preccd-
ing thc inst i tut ion of this protocol {year I ) to the year after lyear 2l '
Thc protocol was a.t "xplicit decision tree using Glasgow Coma
Scalo {GCS) on arr ival of the f l ight crcw as.thc'primary cri terion to
dccidc whcn airway mancuvcri (oral trachcal/nasotrachcal/cr ico-thyruturt yl wcre rcquircd. fhc fiight nurses had been trained and
ccitified in all airway mancuvcrs two ycars bcforc implementation
ui th. ptutu.ul, and no special training other than instruct ion in the
dctai ls of the iccision t ice was givcn at the t ime o{ the protocol 's
implcmcntation.
ol previous EMS system models such as the standard set coverage
-od.l , tott t ional 'base location model, and queuing model are
remedied. Predictions of response times citywide, in speci{ic ge.o-
nrrohi. areas, and for each individual paramedic-rescue unit can be
e;til;J fostulating changes in the number of units, location of
units, oi changes in serviie area responsibility {eg, contemplatedareas of annexition). The model's ability to predict response time
Derformance was compared with actual paramedic-rescue times
i\4odel predictions were within 2% of real systemperformance as
determined {rom computerized dispatchrng records'
Paramedic Response Times - 8 Minutes
SystemEMS Uni t 1EMS Uni t 2EMS Uni t 3
SimulationPrediction (%)
9 192.39 1 . 390.2
TrueData (%)
9292.893.292.2
Patients with airway maneuver/Total
Successf ul Patients/AttemPtedpailenIS
Average GCS (atlemPtedairway) 3.4 (sD, 1.03) 4.6 (sD, 2.88)t
.Year 1 and 2 significantly dif{erent using chi-square (P< 05) -tYear 1 and 2 significantly different using Studenl's t test (P < 05)
An cxplicit airway managemcnt protocol influcnccd the behavior
and pcrformance of {light nurses.
15 Development of a Computer Model to Predict EMS
Svstem Perlormance After Changes in Number,
Location, and Area of Responsibi l i ty of EMS Units
TD Vatenzuela, EA Criss, DW Spaite, HW Meislin, J Goldberg/
SeoiJn of Emergency Medicine, Arizona Health Scie-nces Center;
O"p"rtt.nt of lridustiial and Systems Engineering, College ol
Engineering, University of Arizona, Tucsoniinc" tf,.ir inception as experiments in the prehospitai care of
cardiac arrest, emergency medical services (EMS) systems have
broadened their scope to cope with a wide variety of illnesses and
i"r". . prr i" ienancc of ,n LmS system, capable of providing phy-
;;;;-i";"i medical interventions promptly, requires a significant
inu.r,-.rr, of community ,esorr.cis. To iacilitate EMS planning'
we developed a computer model of the EMS system-in a community
ot-+OO,OOb populaf ion covering-144 square miles The model
l".n*otrr"t ,raffic engineering data (average speeds on different
;oii-ffi;t;;;..red tiauel tiries between points.in the citvJ' and
EfvfS tj'.t"- performance data (call volume, call locations' re-
*ont.ii-"t, on-scene times, transport times) from the paramedic-
;ffi;;;;;. oiir,. -.rto'pohtan fire department The model
,".1""t, i". at e effects of oui-of-service time and dispatch of units
ito- lolrtlont other than their normal base' Inherent limrtations
In summary, we have developed an EMS system computer model
iharallowsplanners to accurately predict the effect of a variety of
il;;r.n .n^t*.s on response times in an urban paramedic-rescue
.16 Sequential Clinical Trials in Emergency MedicineRJ Lewis, HA Bessen/Department of Emergency Medicine' Los
Angeles CountyiHarbor-UCLA Medical Center, Torrancetlinical trials in emergency medicine often concem the efficacy
of critical interventions" in reducing morbidity and mortality'
Usua1ly, a fixed number of patients are evaluated before the data are
in^lrlr"A. Unfortunately, more patielts may be enrolled than are
necessary to obtain a result, and therefore some may be unnecessar-
iiv *p"t'.a to a less ef{icacious treatment ln a sequential trial, the
iit^ u" tr^n^lyzed aher eachpatient, and the trial is halted as soon
,r ""ri-"", efftcacy or laclithereo{ is demonstrated' Thus, the
,,rr-be, of patients required is reduced and depe-nds on the out-
.o-.r ottt.iu"<l duringthe trial. The purpose of this study was to
a.rno"taita" the advaritages of sequeniial trials over a fixed design'
W. tl"u" ana\yzed by computer iimulation a trial of trepatitis-B
ur".in" (ru rnll I Me'd r98U 303:833-841) a1-d i-trial of the MAST
s.r,rt in tiarrm, (Ann Emerg'Med 1987iI5:653-658)' In the simula-
iionr, prti.ntt are assigned to control and test groups, their out'
.ornJ.'trnaottlly deter"mined according-to the frequency of out-
.o-", ob.".u"din the actual studies, and the simulated sequential
.rJv-it-."",inued untii the results become statistically signifi
"rri]rft""*"ds of possible realizations of each trial are simulated,
""a-tn"t att" distribution of required patient numbers is deter-
-in.O- ftt. risk of type I and type II error is s€t at 0'05' In the first
study, *e found thai a sequential trial suf{iciently- sensitive to
;;;;;; , ;"".ne-induced reduction in hepatitis B of 50% would
have required a median of 150 patients in order to demonstrate
;ffi;";t;;l;;; the observed ua"iit'. efficacv of 9.2oh rhe actual
i,"ay "i.ii 1,083 patients. The MAST studv used 201 patients' A
more sensrtlve sequential study, designed.to detect a 50% reduc'
i-lo"-i"--ott"tity,'wou1d have terminated with a median of 102
o",i."a. and also demonstrated lack of efficacy' We conclude that
i.""""ii"t trials usually require fewer patients than {ixed trials to
reach statistically valid conclusions.
.17 Eftects of Acute Ethanol Ingestion on Orthostatic
V i ta lS ignsCA Tomiszewski DM Cline, TW Whitley/Department of
et"rg.n.y Medicine, East Carol ina University, Greenvi l le, North
Carol inaThere are no accepted criteria for orthostatic tilt testing tn in'
toxicated subiects. W-e per{ormed a prospective, randomized, cro-ss-
"".. .*Jy *iih l6 healihv sub jectJwho.received ethanol ( I i g/kgl
". *r,.iipt".eboJ added'to nonalcoholic beer' orthostatic vital
.tg"t, .tt i"ot concentration, and- volume status were checked
ho'"riy fo..ight hours. Peak ethanol concentration was 1 16 5 t 14'5
iini !t one"hour. Analysis of variance {ANOVA) for repeated
;;;r;;.;;;t;aled a significant difference in orthostatic pulse
;h;;#i;t either group 6r time. Bonferroni's t procedure revealed
the dIf{erence between the ethanol 122'l t l3'4 beats) and controi
It-i.i xl .SA.^tsJ groups to be signif icant {P < '005) at two hours after
ingestion. By cuirent clinical iriteria, eight of the ethanol group
r"'Uj..tt "td ^on. in the placebo group were orthostatic at this
ii-!. e, second ANOVA foi repeated measures showed significant
di{ferences in volume status for either group or time' Bonferroni's
20
Year 1
33t344 (5,6%l
22t33 (66.70/.\
Year 2
107t474 (22.6%Y
96t107 (89.7%r

t procedure revcaled a s igni f icant f lu id def ic i t {a95 mL) at f ive, s ix,and seven hours af ter ingest ion versus nonc in the placebo group.ANOVAs for repcated measures did not reveal statistical diffeiences in or thostat ic b lood pressure changes for c i ther group or t imc.Our resul ts show that acute ethanol intoxicat ion causcs an car lvorthostat ic pulse change, which resolvcs spontancously as ethanolconcentrat ion decreases despi tc a delaycd diurcsis.
- 18 Evaluation of the Tilt Test in an Adult EmergencyDepartment PopulationMA Levitt, M Lieberman, B Lopez, M Sutton/Thomas JeffersonUniversity Hospital, Philadelphia. pennsylvania
Pat ients prcsent ing to an urban cmcrgcncy dcpartmcr"r t wi thcornplaints suggestive of dchydration and/or bloocl loss wcrc cn_tered into a study to evaluatc thc " t i l t tcst , ' in an aclu l t EDpopulat ion. As part of thc i r cvaluat ion, changcs in hcart ratc andblood pressure frorn lying to standing wcrc obiaincd in a star-rdarcl-izcd fashion. Body dehydrat ion perccnt was calc l l la tcd for cachpat iont wi th prcviously pr_rbl ishcd calculat ions using nreasurcdserum osmolal i ty and body weight . intcrnal or cxtcrnal Lr lccdinxwas recorded i f prescnt . Mcan dchydrat ion pcrccntagc for th issamplc populat ion (202)was 3 .721:2. t ) . TI- r is samplc was .subdiv idcdinto those pat ients wi th a d iagnosis of b lood loss lgr , rup I ) and thoscpatients with. a diagnosis of dchydration (group 2). Mcan clchyclra_t ion perccnt for group 1 (36) was 2.73 t2.38 ancl group 2 ( l ( r ( r j was3 94 ! 2.97 lP = .0226). Multiple ANOVA tcsting rcvcalccl syncopclP = .037) and lack of axi l lary sweat (p = .02(r) to bc s igni f icani lycorrelatcd wi th dchydrat ion pcrcentagc. Syrnpton-rat ic respuuse t i )the t i l t test was nonsigni f icant (p: .93). A forward stcpwisc l incarrcgression modcl was constructod for thc cont inuoirs var iablcs{agc, changc in hcart ratc [HRl, changc in systol ic prcssurc lSBp],and changc in d iastdic prcssLrrc [Dp]) mcasurcd against dcl iydr , i -tion pcrcentage. In thc wholc san-rplc ar-rd in group 2, thc r.nodclsfound changc in HR (P = .0165) anci agc (1, = .0 '047) ' to dcnronstratca t rue associat ion wi th dchydrat ion porccnt :1gc. Nonc of thcscvariablcs wcrc significant in thc group I r.nodcl. Thc authursconcludc that rn orthostatic mczrsllrcmcnt or-rly HR ar-rcl :rgc havc atruc associat ion wi th levcl of dchyclrat ion. Howcvcr, thc arnour.r t ofvar iat ion in t ichvdrnt ion pcrcentoge e xpla inet l bv HR;rrr t l i lge ts n()rc l i n i ca l l y t r s c fu l . Thcsc mcasu rcmc l . l t s dc l l . l ( ) ns t r t t e n ( ) : l s \ o ( , u l t l onwith b lood loss. I t appoars that thcrc is too rruch indiv idualvarration in a paticnt's orthostatic rcsponsc tO clcl-rydratior-r anclb lood loss to c lctcrminc dcgrcc or prcscncc of dchydrat ion or bkroclrOSS.
19 Probabi l i ty of Appendic i t is Before and Af terObservationLG Graff, MJ Radford, C Werne/New Britain General Hospital, NewBri ta in, Connect icut ; Univers i ty of Connect icut Heal th Center,Farmington
The cffect of observatiorl on the probability of appcndicitis wzrscxamincd rctrospcct ivc ly in 252 cclnscclr t ivc pai i ;nts wi th ab_dominal pain who underwcnt short- tcrrn obscrvat ion (10 4 t l .Zhours) pr ior to thc decis ion to opcrate. Alvarado's scor ing systc l rwas used.to- assign a probability of appcndicitis to cach. pzrticr-rtbeforc and after observation. Mean scoic of paticnts with appcncli-c i t rs , increased fo l lowing obscrvat ion f rom 6.U + 0.6 to Z.U 1-0.q (p< .0 1 ), corresponding to a changc in probability of appcndicitis froin35% to 55%. Mean score of pat icnts wi thout ippenci ic i t is dc_c reased f rom3 .8 +0 .3 t o 1 .6 t .O2 (p< .01 ) , c c r r r espc ,nd ing toa changcin probabi l i ty f rom t i% to 3%. Fol lowrng obscrvat ion, thc dl f fcr-encc betwcen mcan scores of pat ients wi t l - r and wrthout apnendicr_trs increascd f rom 2.6 + 0.6 to 6.2 t .O5 {1, < .01). Twi-Lry_twocontingcncy table analysis showed that observation imnrovcdmean accuracy f rom 65Y" to 85% lp < .01), mcan probabi l i ty of d i_agnos.is (positive predictive valuel fron 70y" to 80o/o lp < .0 1 ), mcanspeci f ic i ty f rom 657" to 86% (P < .01] , and mean sensi t iv i ty f rom7O"h to B0% (NS). By incorporat ing change in scorc fo l iowingobservation as a function of prcobseivation score, sensrtrvity fur-ther increased f rom 80% to 93% lp < .01 ) , and pat ients wrth appen_dicitis could be separated from those without. In this group ofpatients with an initial intermediate probability of having appen-dicitis, observation improved the ability to distinguish pnii."t.with and without appendicrtrs.
20 Threatened Abortion: A Prospective Study ofPredictors ol Outcome in an Emergency DepartmentPopulation
J Abbott, M Zaccardi, SR Lowenstein/Department of Surgery,Div is ion of Emergency Medic ine and Trauma, Emergency Medic ineCl in ical Research Center, Univers i ty of Colorado Heal th SciencesCenter, Denver
Al t l iough, thrcatened abort ion is a common problerr i in thccmcrgcncy departmcnt, no prospcct ivc studics in an ED sct t inghavc becn reported. Wc cxamincd prospect ivc ly the prescnratron,c l in ical coursc, and outcomc of 75 consccut ivc threatcncd abort ionpat icnts in our urban teaching hospi ta l . Al l pat icnts were in thcf i rs t hal f of prcgnancy and had vaginal b lccding, a c losccl ccruix, anda posrt ivc prcgnancy tcst . Whi lc a 50,2, ratc of fc ta l loss is of tcnquotccl for thrcatcncd abortron patrcnts, a lmost thrcc qu:rr tcrs172"1,) of our pat icnts l - rac1 fcta l dcmisc; only 2g.1, had a goodol l tcomc (prcgnancy v iablc at 20 wceks). Two fcta l dcmiscs wcrccctoprc. C)bstctr ic h istory, racc, matcrn:11 agc, hcrnatocnt , v i ta ls igns, prcscnce and c lurat ion of cranps, I . ) rcscncc of c lots or abclorni_nal tcndcrncss on cxaminat ion, ancl durat ion of b lccding wcrc nothclpfu l in prccl ic t i r " rg oLl tcolnc. Thc t in. re s incc last rncnstrualpcr iod was hclpfu l : avcragc t inrc was 90 + l l days for good ol l tcontcpat icnts vcrsus (r4 + 3 days for pat ients wi th fcta l loss {1, = .00t i ) .Also, pat icnts wi t l . r act ivc b lccding wcrc morc l ikc ly to suf fcr fe t : r lIoss {RR = 2.3, P = .03). Thc prcsencc of fcr : r l hcart act iv i tv bvul t r : rsouncl was a strong prcdictor of goocl outcor. r - rc { / , . .001). Alsr i ,a quant i tat ivc huuan chor io l r ic gonadotropin {HCG) lcvcl < ( r ,500m lU /nL ( / r < . 001 ) and t hc abscncc o f a gcs t : t t i ona l sac by u l t r a -sor-rncl (P < .001 I wcrc strong prcdictors of bad outcomc. For t . rat icntswi th an HCG > (r ,500 mlU/ni l ar . rd no fcta l hcart act iv i tv . thuchancc of a good uutcor. r . tc was only onc tn f ivc. Al l pat icnts wi th anHCC . 6 ,500 r r r lU / rnL h i r t l t r . r : r l t l t n r i se .
.21 Predictors of Electro lyte Abnormal i t ies in Elder ly
Patientsplrtl Singal, JRtledges, PA Succop/Depatrtments of EmergencyMedic ine and Environmental Heal th, Div isron of Biostat is t ics,Div is ion of Emergency Medic ine, Oregon f , {eal th SciencesUnivers i ty , Port land
Thc scrur l c lcctro lytc pancl is or . tc of thc r t rost comrr. ronlv ner_forr lcd laburatory tcsts in the crncrgcncy r lc ,partn.rcnt . Th. pur1i , ,s .of th is study is to val ic latc I prcvior-rs ly pLrbl ishcd decis ion ru lL fororc lcr ing stat scr l lm c lcctr , r ly tcs {Lowc et t l , l . rH7) : rncl to cvaluatco thc r p r cd i c t o r s o f a c l i n i ca l l y s i gn i f i can t c l ec t r o l y t c abno rma l i t y(CSEA) in our study populat ior . r {cmcrgcncy patrcnts >.5.5 ycars o ld j .A rcscarchcr stat ionccl in thc ED intcrv icwcr l the t rcat ing fhysic iarrin : r tota l of l , lJ l0 pat icrr t cr . rcountcrs. Extcnsivc fo l l i rw- i rn wasconcluctccl to r lc tcn.r . r i r . rc whcthcr thc scrum clcctnr lv tc n,r , rc l , , . -dcrccl in thc ED rcsul tcc l rn i r CSEA anci i f t l . rosc pat icr . r ts who t l i t l nothavc thc tcst ordcrcd on thc int lux v is i t har l d \ i rhstr lL lcnt physic iancncountcr (<14 days) in whic l - r a CSEA was founcl . Scvcrr h i rndrcdninty-scvcrr pat icnts l - rad c lcctro lytcs <l r t lcrccl on thc indcx v is i t .Onc I rundrct l twcnty- four showcd a CSEA { f rcc lucncy = I S.(r ,2, ) . Thcscnsi t iv . i ty_and-spcci f ic i ty of Lowc's cr i tcr ia for prcdict ing CSEAswcrc calculatccl -scnsi t iv i ty , .94 1t15,r , CI =. tJt t - .97); spcci f ic i ty , 09I t )5" / , ' CI = .07 - .11 ) . Of thc 1,013 pat icnts who did not havc a scnrnrc lcctro lytc pancl on thc inc lcx v is i t , s ix wcrc found to havc a CSEAat a s l rbscqucnt physic ian c l tcolut tcr . Lowc,s cr i tcr ia nrcdictcd al lof thcsc. Tl" rc rc lat ionship bctwcen thc f re ctucncy of C.SEA end thcr e J s o r r t h e t c s t w i . l : , r r t l e r . d w e r c l r r i t l v z e t l L i s i n A t h , . e h i : . 1 t r ; r r r . t e s t .Logist ic rcgrcssion analysis w:rs pcr fornted to dctcnninc whichcl in ical fcaturcs wcrc indcpcndcnt ly and s igr-r i f icant ly prcdict ivc ofCSEA. Thc r tost colr l t lor t rcason givcn for ct rdcr ing c lcctnr ly tcs isto scrccn for an unexpcctccl abr-ronnality. Tlrc frcclucncy of
'CSte
for th is group was .11 cornparcd wl th . j0 i f thc p l iys ic ian ordcrcdthc tcst to conf i rm a suspcctcd abnormal i ty ana .Oj i i thc tcst wasorclcrcd by thc nursc to cxpcdi te pat ic l l t c i l rc . These t l i f fcrcnccs arcsigni f icant (1, < .001). L.r part icular , c tncrgcl tcy physic ians who donot suspect CSEA is prcscnt and cmcrgcncy nurscs who draw bloodpr ior to physic ian cvaluat ion rnay f tncl that Lowc's cr i tcrra l t rprovcdecis ion rnaking. Tl - rcy should also bc awarc that c ldcr lv pnir"nt ,wi th a h istory of renal d iscasc, a lcohol isn-r , and i rnpairct l a i r i l i ,y t , ,comntunicate may be at incrcased r isk for CSEA.
22 Symptom Severity in Acute Myocardial lnfarct ion andits Effect on Patient Delay and Use of 91 1MT Ho, MS Eisenberg, S Schaeffer, S Damon, p Litwjn, MpLarson/Center for Evaluatron of Emergency Medical Services, KingCounty Department of Health, Emergency Medical ServicesDivision; Department of Medicine, University of Washington, Seatt le
Wc studicd whcther symptom scverity is predict ive of acutemyocardial infarct ion {AMI) and how it af{ecis patient delay in
21

seeking care or use o{ the 911 number. For 15 months beginning
October 1986, 5,206 patients were admitted to King County,
Washington, hospitals for possible AML Patient records were re-
viewed for patrent delay, mode of transport, and discharge diagno-
sis. For patients with a discharge diagnosis of AMI, the admission
ECC wai reviewed. A reprcsentat ive subset of pat ients {2,388' 4!%1.
was interviewed by phone to assess symptom severity on a sca-le ot
I ( lowest) to 10. Symptoms rated as I to 4 were considered mi ld, 5
to 7 moderate, and 8 to 10 scvere. There was no significant
correlation betwecn severity and discharge diagnosis o{ AMI -
mild,26"ki moderate, 23ok; severe,277".Thete was also no corre-
lation between severity and whether the discharge diagnosis was
cardiac rc latcd (AMI, angina, acute pulmonary edema) - mi ld,
55%; moderatc, 53%; severe, 55%. Of pat icnts wi th AMI (552), ST
clevat ion was present in 55% with mi ld, 53% with moderate, and
67"1' with t.u".c symptoms. Scvcrity significantly influenced
nat icnt delav and use oI9l l :57"1, of pat ients wi th mi ld symptoms
ic layed moic than two hrrurs, only 32% used 911;51% with
rrlud".ute symptoms delayed more than two hours, 427" used 9ll;
46'% with severc symptoms delayed morc than two hours, 4t37o
uscd 911. In pat icnts wi th chest pain, ef for ts to shorten dclay in
scekins carc and to j .ncrcase use of 9 1 I should strcss that symptom
scver i ty is unimportant .
23 Frequency Analysis ol the Electrocardiogram inHuman Beings During Ventricular FibrillationCG Brown, R Neumar, R DzwonczyklDivision of EmergencyMedicine and Department of Anesthesiology, The Ohio StateUniversity, Columbus
Rcccnt rcports havc suggested that the init ial treatmcnt of ven-tr icular f ibr i l lat ion (VF) may be dependent on downtime, thcduration of t ime betwccn thc onsct of cardiac arrcst and thcinitiation of advanccd cardiac lifc support. Howcver, thcrc cxrsts n<rrcl iable method of cst imating downtimc in the prehospital sett ing.Wc havc prcviously charactcrizcd thc dynamics of thc ECG in thefrcclucncy domain during VF in a swine rnodel and havc shown thatrncdian ficqucncy of thc VF ECG can bc used to accurately rlcasurcdowntimc during VF. Thc purposc of this study was to charactcrizethc dynar-nic characteristics of the VF ECG in human beings- Theanalcig ECG signal was rccordcd from sevcn pcrsons who developedVF during ambulatory cardiac monitoring The analog -VF ECGsignal was digitizcd ̂ t 128 Hz, and cach four seconds of data wcretransformcd into thc frcqucncy domain using a fast Fouricr trans-fonn. Thc rncdian frcqucncy thcn was dctcrmined and plottedvcrsus downtime f or al l paticnts. The duration of VF for these sevcnpaticnts rangcd from I .53 to 1U.27 minutes At the onset of VF thcnu"rag" -cdia.t frccluency was 4.40 x L2l Hz. The median fre-urlcniv dccrcascd to 3.38 t l .0B Hz at 3.20 minutes and thenincrcascd to a pcak of 4.14 tO.6I Hz at 5.87 minutes. The medianfrcouencv then decreased over time. Thc average coefficient ofvariation for all seven subiects was 24.737". It appcars that thcmcdian frcquency of the human VF ECG signal displays a dynamicanrl rcpcatallc pattcrn with rcspect to time. It is possible to modclthesc iata to cstimatc downtime during VF and thus guide initialtherapy.
24 The Diagnostic lmpact of Prehospital 12'LeadElectrocardiographyTP Aufderheide. GE Hendley, RK Thakur, FA Laitinen, JR Mateer'HA Stueven, DW Olson, KM Hargarten, KC Preuss, RG Hoffman/Medical College oJ Wisconsin, Milwaukee County Medical Complex.
During a ien-month period, i53 blinded prehospital l2-leadECGs of diagnostic quality were obtained by paramedics on 157adult patients presenting with chest pain. Final hospital diagnoseswere classified into thiee groups: group l, acute myocardialinfarction (AMI, 24); group 2, suspected angina (62); group 3,noncardiac chest pain (67). Paramedic and base physician clinicaldiagnoses, and prehospital and emcrgency department ECGs weresimilarly classlfied and compared. ECGs were independently,blindly, and retrospectively read by two cardiologists. For patientswith AMI, prehospital ECG alone had significantly higher specific-ity and potiti'tte predictive value than did the paramedic or basephys ic ian c l in ica l d iagnos is . For pa t ien ts w i th suspec ted-ang ina ,iombining the paramedic clinical diagnosis and the prehospitalECG signiTicantiy improved sensit ivi ty i90 i vs 62.3, P <.O01) andincreased negative predict ive value (88.5 vs 70.I, P <.02). There wasa high conc-ordanCe between blinded prehospital and ED ECCdiagnosis
1�99.3% Ior Ali.1rl, 92.8% for anginaJ. Futhermore, ten
prtLntt wirose prehospital ECGs demonstrated ischemia and who
had the final diagnosis of angina or AMI were mistriaged by
paramedics and/or received no advanced life support therapy.
Drehospital ECGs increase diagnostrc sensitivity and specificity,
approach congruity with ED diagnoses, and may improve accuracy
in triage of chest pain patients.
Specificity + Predictive -PredictiveValue Value
70.57" 133.3% L 93.5'l.- i
u rI
69.0'l. I 32.5"/" 87.O"/"
J r | '99.2o/a 92.87.
' 92.1"/"
Group l Sensitivi ly
Paramedicclinicaldiagnosis 75.0%
Base physicianc l in ica ld iagnos is 59 .1%
PrehospilalECG 54.2o/o- P = N S . t P < . 0 0 1
.25 A Computer-Based Time-lnsensitive PredictiveInstrument lor Predicting Myocardial Inlarction in theEmergency DepartmentCB Cairns, JT Nremann, PL Henneman, lG Mena, MM Laks/TheUCLA School of Medicine, Departments of Emergency Medicine'Nuclear Medicine, and Medicine, Division of Cardiology, Harbor-UCLA Medical Center, Torrance
The purpose of this study was to assess the diagnostic value ofa computcr-based, time-insensitive predictive instrument (TIPI) indetecting acute myocardial infarction {AMI) in patients whoseinitial ECG was not diagnostic for AMI. A TIPI probability score forAMI was calculated using four clinical variables {age, sex, presenceor absence of chest/left arm pain, and whether chest pain was theprimary presenting symptom) and computer interpretatron .ofnonspecific ST segment-T wave abnormalities using specificallydesigncd ECG computer language. Forty-nine patients with chestpain'suggestive of AMI and nonspecific ST-T wave changes wereenrollcd, had thallium-201 and technetium-99m cardiac scanspcrformed and ECCs recorded in the emergency department, and,iollowine admission had serial CK-MB determinations made andserial Eiis obtained. A TIPI probability score was computed usingthe initial ED ECG. An increase in CK-MB fraction {> 5%) wasnoted in four of 50 patients. Twenty-four 149'hlhad an abnormalwall motion study, and l3 of these had an abnormal thallium scan(scan sensitivity ior AMI, 757o; specificity,4O"/oi positive predic-iive value, 10%; negative predictive value, 95%). Of those patientswith CK-MB elevation, a TIPI AMI probability score of > 37ok hada sensitivity of I00% and a specificity oI 79"/o for AMI (positivepredictive valte, 667oi negative predictive value, 100%). W-. .91-clude that this computer:based predictive instrument is highlysensitive in detecting AMI, more accurate than early radionuclidescanning in detecting AMI, easily accessed in the ED, and ofpotential value in triage.
26 Comparison of Creatine Kinase and CKMB inEmergency Department Patients Admitted to Rule OutMyocardial InfarctionGP Young, T Green/Portland Veterans Administration MedicalCenter and Oregon Health Sciences University, Portland
We retrospeitively analyzed total creatine kinase (CK) andCKMB levels drawn in the emergency department on 222 consecu-tive patients admitted to rule out myocardial infarction to comparetheii relative accuracy. For all o{ the patients, the mean CK was 149x7g U lL (normal range, to 2321 andthe mean CKMB was i3 t 9 U/L {normal range, to 23). For the a3 (19%l MI patients, the mean CKwas 371 t lStU lL and the mean CKMB was 26 + 13 U/L. For theI79 l8l%) nonMl patients, the mean CK was-95 !66UlL and themean CKMBwas l0+ 8 U/L. In theED, lTof theMlpatients (40%)had an elevated CK and 15 ,34%) had an elevated CKMB (true-positives, P > .05, chi-square). Of the nonMl p-atients, nine (57o-) hadan elevated CK and eight {4.5%) had an elevated CKMB {false-positives, P > .05, chi-square). For the CK values in the ED, theipecificiiy was 94"/o, the sensitivity was -39o/o, the positive predic-tive value was 65%, and the negative predictive vaiue was 85o/o.Forthe CKMB values in the ED, the specificity was967o, the sensitiv-ity was 35%, the positive predictive value was 657o, and thenegative predictive-value wis 86%. These results indicate thatthJre is nb significant difference between the CK and the CKMBwhen used in the ED diagnosis of MI.
.27 Squamous Cells as Predictors of ContaminatedUrine CulturesFG Walter, RK Knopp/University of California, San Francisco,School of Medicine; Fresno-Central San Joaquin Valley Medical
22

E_ducat ion Program; Department of Emergency Medic ine, Val leyMedical Center, Fresno, Cal i fornia
Squamous ccl ls arc commonly bcl ieved to indicate a contami-na t cd u r rnc samp le . Howcv r r , no pub l i shed ev i dcncc ux i s t \ r osupport th is_assumpt ion. Therefore, 105 women wi th symptomssuggest ivc of ur inary t ract rnfect ion were studied prospcct ively inol l r .emergcncy dcpartment. Each pat ient had two ur ine samples, amidstream clean-catch (MSCC) in i t ia l ly , then a catheterrzcd{CATH). Both samplcs wtrc analyzrd for squarnous ccl ls andcul tured. Contaminat ion was def incd as less than 10,000 colonies/mL or a ur ine sample that grcw thrcc or morc specics of commensalbacter ia. Of the 105 pat ients, 22 lZO"/ ,1 had contaminated MSCCurine sampies. Although CATH urrne containccl from O to (r0squamous ccl ls / low power f ic ld (LpF, ic , l00x), no CATH sanrplcgrew contaminants. For MSCC samples, the posi t ive prccl ic t ivcvalue {PPV) of squamous ccl ls for coniamrnat ion is sumnar izccl asfol lows, wi th 90% conf idcnce intcrvals: 0 squamous ccl ls /LRf, 0%PPV {0% to I00%); L to l0 sc luamous cel ls /LpF, 20, / . ppv l l l .5, t ,t -o 28.5"k) ; i0 to 30 squamous cel ls /LpF, I9% ppv l7.77" to 3) , .0.1) ;3.0 to 60 squamous cells/LPF, 3U% PPV lr).3"1, t<t 65.67o)i and morcthan 60 squamous ccl ls /LPF, 50%, PpV (O%, to 100%,). Wc concluclcthat sc luamous ccl ls in CATH ur inc samplcs arc not prccl ic t ivc ofcontaminatcd CATH ur ine, and that t l - rc c l in ic ian should not r . rcc-cssarily discard a urine samplc as contamin:ltcd bccar-rsc sciLr:lmousccus arc prescnt .
28 Stab Wounds of the Chest: Uti l i ty ol the ExpiratoryChest Radiograph AloneRM McNamara, EA HeinelDepartment of Emergency Medicine, TheMedical College of Pennsylvania, Philadelphia
I t is general ly rccommcndcd that radiographic cxarninat ion furpotent ia l pncutnothorax includcs both inspiratory ( ICR) ancl cxpi-ratory_ (ECR) chest radiographs. This stut ly rct rospoctrvcly cxam-incd the uscfulness of thc ECR alonc in t l0 pat icnt i sustain ing stabwounds of the chest dur ing a two-ycar pcr iocl . A board-cci i i f icdcmcrgency physic ian indcpcndcnt ly intcrprctcd only thc ECR inthcse pat icnts. This rcading was thcn con-rparcd to a radio logist 'sintcrprctat ion of both v icws and, i f pcr formcd, a latcral v icw. Dis-crcpancics werc rcv iewcd and anothcr radio logist 's opin i0n soughtif nccessary to rcsolvc a diffcrcnce. Finclings wcrc clas,sificd in thiccgroups: pneumothorax, cf fusion/ inf i l t ratc/atc lcctasis, ancl Othcrs igni f icant f inc i ings. A tota l of 219 scts of both ICR ancl ECR wcrcavai iablc for revicw, and 121 had an includcd latcral v icw. Tl - rcrcwcre B7 (40%)pncurnothoraccs wi th onc fa lsc-posi t ivc {Fp) and twofalse-negativc {FN) intorprctations by thc cmcrgcncy physrciar-r.Both false-negative rcadings wcrc a minimal apical pncJmothuraxthat was dcmonstrable on the ECR. Thcrc wcrc 9g 1.44, ,1,) instanccsof e i thcr ef fusion, inf i l t ratc, or atc lcctasis wi th onc fa lsc-posi t ivcand four falsc-ncgativc intcrprctations by thc cn"rcrgcncy physi-cian. Two of the false-negative rcadings wcrc evicicnt on rorcvicwof thc.ECR, ancl the other two werc small cffusions scen only on thelatcral view. Three of the ten other significant findings {hilar rnass,rib fracture, dcnsity) were initially rnrsscd by thc crncrgcncyphysician but were obvious on a rcrcview of thc ECR. Scoaratcanalysis of the 56 scts of radiographs that wcrc thc initial crncr-gcncy department studies revealcd ten ( l t i%) pncumothoraccs,sevcneffusior-r/infiltrate/atelectasis, andthreeothcrfindinss. Thcrcwerc no falsc-positive or false-ncgativc rcadings by thc cmcrgencyphysician in this group. A propcrly intcrpreted ECR appcars'io bcsufficient in the cvaluation of patients with stab wounds to thcchest .
29 Detection of Soft Tissue Foreign Bodies by plainRadiography, Xerography, Computerized AxialTomography, and UltrasonographyGL El l is , M Ginsburg, L Flom/Western Pennsylvania Hospi ta l ;Univers i ty of Pi t tsburgh, Af l i l ia ted Residency in EmergencyMedic ine, Pi t tsburgh, Pennsylvania
_ The ourpose oi this study was to detcrmine the reliability ofplain.radiography, xerography, computerized axial tomography,and ultrasonography in the detection of soft tissue foreien bodiis ofvarious materials. Fragments of glass and wood measuring 5 mmlong by 2 mm wide were placed between two pieces of meat withthe preparation submerged under water to prcvent air entrapmcntat.the inter{ace. The preparation was thin examined by plarnradiography, positive and negative xerography, cornputerized axraltomography, and ultrasonography. The glass foreign bodies werereliably detected by all of the modalitics tested. The wooden andplastic foreign bodies were poorly visualized by plain radiography.
Xcrography and cornputerized axial tomography achicved slightcnhanccment but d id not rc l iably d i f {ercnt iatc the foreign bod' icsfrorn intr ins ic var iat ions of radiodcnsi ty prescnt tn the sof t t issucrnocle l . On thc other hand, u l t rasonugraphy rc l iably dctectcd thcforc ign bodres composcd of p last ic and wood. Wc concludcd thatul t rasonogra_phy is thc method of choicc in dctect ing forc ign bodiescomposccl of materral that is not s igni f icant ly radiodensc.
30 Portable Ultrasound in Patients With SuspectedCholecystit is: Performance and Interpretatioi byEmergency PhysiciansL Gussow, R Himmelman, R Zalenski/Deparlment of EmergencyMedicine and Division of Trauma, Department of Surgery, CookCounty Hospital, Chicago, l l l inois
Alt l - rough scvcral studics havc shown thc uscfulncss of u l t ra_sonography pcrforrnccl by racl io logists in thc cmcrgcncy dcpart-mcnt/ nonc havc cxaminccl thc accuracy achicvablc by cn-rcrgcncyphysic ians wi thout pr ior forr .n:r l u l t rasound t ra in ing. fh is . i tudywas undcrtakcn to cvaluatc cmcrgcncy physic ian usc of u l t ra-sonography to c lctcrminc thc prcscrrcc or abscncc of gal ls toncs.Thrcc cmcrgcncy physic ians wcrc givcr . r approxir -natc ly c ight hoursof t ra inrng in_gal lb laddcr v isr-ra l izat ion and diagnosis. by 'an ul t ra-souncl tcc l . rnologist on thc ScanMatc I I , portablc u l t rasound scan_nc r lDamon Co rp ) . Pa t t cn t s c r r t r r u t l i r r t o t l r c s t udy wc rc a l l adm i t -tcd to thc hospi ta l through thc ED wi th suspcctcd cholccyst i t rs orch.olc l i thtasis. No pi l t ic l t t hacl rcccivcd a prcvious sonogram orothcr c lcf in i t ivc tcst fur gal ls toncs. Nonc had gal ls toncs v is ib lc onr t hd r r r r r i n ; r l r : r t l r og r t r ph . Thu i nvcs r i g : r t o r s r r r nne t l t h ( . f i l t i r . n r i n ( ) nuor two posi t ions (supinc, lc f t la tcral dccubi t t rs) , took polaroid,p icturcs_ of thc rnost rcprcsct l tat ivc v ie ws, r rnt l inrrncdiatc ly intcr-prctcd t l rc sc:ut i ls l . rosi t ivc for gal ls toncs, ncgat ive, or inc lctcrr l i_natc. This b l indcd intcrprctat ion was comparcd to thc gold stan_darcl of forrnal u l t rasor-rography pcrformccl in thc radio logy dcpart-l .ncnt or f i r - rc i ings at sr l rgcry. Forty- four pt t ic l ' l ts wcrc cntcrccl . Thclrrc:ln :lgc was 39; 6[l'2, wcrc wollclt. Thc prcvalcncc ratc ofgal ls toncs was 57'2, 125 of aa) Twe nty- tw() ica,rs , "crc rcad asl . rosi t ivc by t l - rc cr .ncrgcr. rcy |hysic iarr ; ; r l l l .ut onc agrccd wi th t l - rcgolc l s tandarcl (posi t rvc prccl ic t ivc valuc = 95,2,1. Thir tccn scanswcrc rcacl as ncgat ivc; a l l br , r t onc agrcccl wi th thc gold stanclarc l(ncgir t ivc prccl ic t ivc valL lc =92, ' l ) . Ninc scans (20,2,)wcre rcad as in-dctcn.ninatc; of thcsc, thrcc wcrc posi t ivc ant l s ix wcrc ncgat ivo bythc gold stanclarc l . Wc concludc that cmcrgcncy physic ian 1re r f r r l l -ancc of u l t rasouncl scanning is fcasib lc ar-rd acct i ra ic and can aid inc i iagnosis ancl pat icnt d isposi t ion. This warrants fur thcr study.
31 Passive Hemagglutination Inhibit ion Test forDiagnosis of Brown Recluse Spider Bite EnvenomationSM Barrett, M Romine-Jenkins, JP Campbell/Oklahoma MedicalCenter, University of Oklahoma Health Sciences Center, OklahomaCity
Brown rcclusc (Fiddlcback) spic lcr b i tc (BRSB) cnvcnonrat ion isa cornlnon causc of nccrot ic sk in lcs iot- rs in thc Midwcst . Howcvcr,ot l - rcr ct io logics of sk in nccrosis cx ist . Prcscnt ly , thc c l iagnosis o iBRSB cnvcnornat ion is madc c l inrcal ly . Wc rcport a passivc hcmag-glut inat ion inhib i t ion (PHAI) tcst to d iagnose l lRSI l in huminbcings. Thc PHAI assay has bccn usccl succcssful ly to idcnt i fvvcnom frorn BRSB lcs ions in guinca pigs, but thc tcsr h;rs ntr t yr : tbccn uscd for d iagnost ic purposcs in human tr ia ls. To dcvclop ihctcst , brown rcclusc spidcrs wcrc capt l l rcd and disscctcd. Spidcrvcl - lom was poolcd and conccntratcd. Rabbi ts wcrc in icctcd wi thvcnom to inducc ant ibody format ion. Final ly , human rcd bloodccl ls wcrc coated wrth spidcr ve nom using a microt i ter p late. ThcPHAI tcst thcn was standardized against contro ls to achicvc <tpt i -mal concentrat ions of venom, rabbi t ant ibody, and sensi t iZedhuman rcd ccl ls . I f spider vcnorn is prescnt in rnatcr ia l f rom anccrot ic lcs ion, th is venom wi l l b ind wi th rabbi t antrbody so thathcmagglutination does not occur. If venon-r is not prescnt, rabbitant ibody is f rec to b ind wi th venom, coat ing red cel l membranes sothat hernagglut inat ion occurs. Thercfore, hcmagglut inat ion inhi-b i t ion is d iagnost ic of BRSB cnvenomat ion. Thc stascs of the pHAItest wi l l bc d isplayed along wi th posi t ive and negat ivc resul ts andcontrol samples. Furthermorc, using venom from other spiderspecies capablc of inducing necrot ic sk in lcs ions, we wi l l d isplaythe.specificity of the PHAI test for ve nom from thc brown reciusesploer.
.32 Standard Formulation of Nitroglycerin Ointment andHot Packs for Venous Dilation in Pediatric IntravenousAccess
MC Clark, K Shaw, D Schaible, N Mackey/Department .olEmergency Medicine, Children's Hospital oI Phi ladelphia, University
of Pennsylvania School oi Medicine, Phi ladelphia.We siudied the e{{ectiveness of 2% nitroglycerin ointment
(NTGI or hot packs in di lat ing cutaneous. veins to faci l i tate IV
access in 149 nonacute patrents with stable vital signs from I
-onth to 17 years o{ age. Patients were randomly assigned to
,."r,-".r , groups of NTC (44), hot packs (51), -or control {54J'Oi",-"", #as ,ppli.d for three minutes {rom l-mL syringes based
,- th. prti..tt't "g" "t follows: 0 to (r months, 0 QQ mL; 6 months
to 3 years,0.09 mi;3 to l3 ycars, 0. I(r mL; and older than 13,0 25
-i. bo-i".t.iaily'available hot packs were applied along with the
ointment but only activated in the hot pack group Placebo oint-
ment and inactivatcd hot packs were applied in the control Sroup'Vcin diameter was measured by using prccision calipers' Thcre
wcre no cliffcrences among thc groups in patient weight, age, sex,
or prctreatment mcan vein size Nonc ol the treatments alterco
vital signs, nor were side effects noted during 30 minutes <lf
observaiion. NTG application rcsultcd in significant vcin dilation
"u-prt", l tu placcbo ( l = .03210.3U mm SD; P = '041as did hot pack
application ( i = O.:+ t o.+A mm SD; P = .03). Overal l IV succcss rate
i is75%, and no dif ferences in success rate werc detected among
thc sroups. We dcmonstratcd a safe dose for a standard formulation,rt NiC'",r, prcviously studied in thc pediatr ic populat ion that
dilatcs cutancous veins. Hot packs, also heretoforc unstudied, werc
..irritv as cffcctivc as NTG in vein dilation Further study to
;"';1";1. ,h" abilitv of thcse tcchniques to improve the succcss of
tV ,. ."t t in infants and chi ldren wilh smal1 veins is warrantcd'
'33 Ketamine Sedation Protocol for Emergency PediatricProceduresSM Green, NE Johnson, R Nakamura/Department of EmergencyMedicine, Loma Linda Universrty Medical Center, Loma Linda'
CaliJornia- -- wc rcviewed the kctaminc litcrature and studicd thc efiicacy of
a low-dosc scdativc protocol in childrcn undergoing cmergoncyproccdurcs. One hundred cight paticnts ages l4 months to 13 years
i:"."lu.J in,tr*uscular racemii kctamine 4 mg/kg with 0 01 mg/
k{ atropinc. Onsct of dissociat ive sedation within f ive minutes
i,!.rit.'Jit il3'X, of patients; adccluate analgesia, immobility, and
r"Jrii,it wcrc achicvcd in 97"1,. No adjunctive rcstraint or local
ancrthctic was uscd in 86% . Mcan time from in jection to dischargc
,"". 82 rrrir't,.,t.s irangc, 30 to 175). Patients werc monitored by pulse
,t-l-.,.y and bedside nursing, without IV or- intubation' Therc
wcrc no'cl inical complicationi, although one 1fl-month-old expe-
ricncccl cmesis with transient cyanotic laryngospasm' Emesis
occurrcd in (r%. No nightmarcs wcrc notcd ln thls age group'
Parcntal ancl physician satis{action werc high immediately and on
{ollow-un intcrvicw. As with all scdative agents, use should be
lirnitcd io pcrsonnel capablc and cquipped to manage alrway
.nt.i*"n.i". such as laiyngospasm. Contraindications are dis-
.urt"?. W. concur with 25 yeais of studics documenting.efficacyand safcty of ketamine sedation for outpatient proccdures ln
sclectcd pcdiatr ic Patients.
.34 lmpact of the HIV Epidemic: Emergency DepartmentResource Utilization by Patients With Known Humanlmmunodeficiency Virus (HlV-1) InfectionGD Kelen, G Johnson, T DiGiovanna, K Loring, KT Sivertson/Diuit ion oi Emergency Medicine and Johns Hopkins University
School oi Medicine, Balt imore, MarylandInner-city emergency departments are increa.singly being used
by paiients with HIV I infeciion. We undertook this study to assess
thc reasons {or emergency visits to an inner-city ED by patients
;i[L;;;" HIV infiction. Retrospective chart review of a four-
month Derlod in 1988 revealed thaf 164 patients with known HIV
i"i..tio'" accounted for 256 ll .4%l ED visits Only 27 of the visits
*.r.]ot..r.nns clearly unrelated to HIV infection, and 130 visits
l5l%) became admissions. The most common complalnts we.re'i.",intE;Il,
tever \25"/"l, malaise (I8 % ), and chest pain (I47' ) The
rno.? "o--'n" diagnosei wete Pneumocystis pneumonia (13%)'
"""-i."ri."t neuiological disorder ( l3%), other pneumonia {7%)'rep.is (f,y' l, and volum-e deplction ((r% )r 9j t\t It^:itt
from patients
*t" f-tra a 'iegular
.orrt". oi care, 70"/o ll27 of-Ilz) occurred during
times when tir.re.or....s were unavailable Oddsratio (OR) analy-
sis of the payor status of the 256 visits revealed that HIV patients
were 2.4 iim.t -o.e likely to have inadequate or no lnsurance
.ot"p-.d with the general emergency. population (95% CI=1 84-
3.33, P. .01). Patients without a regular source of care (50) were
more likely to hAve inadequate or no insurance in compari,son^withthose who were regularly followed (OR = 2'I, 95"/o CI = I'0-4'9, P =
.5J. Visits with third-party coverage ( 187) were more than 3'2 times
"r' lik"ty to result in idmissions than visits with inadequate
.o"..r*. 1'95% CI: 1.66-6.I; P < .01). Because admissions are based
onlv o"n severity of illness and not payor status, HIV pattents
*i,ito"a insurance likely use the ED as their primary source of care'
We conclude that this dD is sought when other sources of care are
""^u^iirlf., but HlV-infected patients are les.s able to pay for
serviccs than others. Adequately subsidized and alternate sources
of care are essential to ichieve appropriate use of emergency
services by these complex patients.
35 Emergency Department Complianc€ With a Standardfor the Minaglmeirt of Patients With UncomplicatedRecurrent ConvulsionsLJ Baraff, DL Schriger, S Starkman/The Emergency Medicine
Center, UCLA Medical Center, Los AngelesWe conducted a retrospective study to determine if the treat-
ment of uncomplicated iecurrettt convulsions in a university
.-.tg*.v depariment met a minimum standard defined by the
fr""iiv ^tia ii compliance related to the resident's-specialty or
o"ri*i'"a"r," year oi training. The standard described items to be
i".l"a"a in the medical reiord and the appropriate diagnostic
evaluation. A chart score was defined by the presence of ten
.s""i*i,ta eight desirable hrstory and physical items; a perfect
r."i" *rt ioo. only anticonvulsant and ethanol levels were deemed
anoror,tiate for all patients when drawn; a head computed tomogra-
o'fi'u tirn was deemed appropriate if the patient's neurologic-status
i.i"ii-.,.a or failed to'retlrn to baseline in one hour' All other
;;;;t; evaluated individuallv bv the authors' One hundred
.unr".rrtiu. ED patients l8 years or older-who presented with a
,""rlrr"n, convuliion and weie not hospitalized were the subiects
of this study. Patients ranged in age from 18 to 88 years (mean,32
t I .2 ISEM]|. ED t irne rattged fro- 26 to 58I minutes {mean, 209 '
f f l . nnci l la.y service chirges {ASCsl ranged from $0 to $1,779
f -.arr", $ii6t. only 26.1dof these charges were {or tests deemed
,pptopti"t.. There was a significant relationship between the ED
i'i?e ind ASCs (Spearman c6rrelation = 0.4459i P < '0001)' Medical
rccord scorcs ranged from 8 to 79 (mean, 59 t 1 4)'.ASCs f or patients
secn by emergenJy medicine residents were less than for those seen
[v -"6i"i"" iesidents ($82 vs $227; P = .003)' A-SCs- were higher!9rp'Cy t-Z versus PGY 3-5 residents i$238 vs $185, P = 16) We
conclude that physician documentation did not meet the detlned
standard, exceisive use of ancillary s-ervices resulted in unneces-
;;; ;;tit and long ED times, and there was. a difference in the
o.t'fot-rt". of res'ident physicians by specialty with emergencyphysicians ordering fewer ancillary services'
'36 Adherence to Universal Precautions by Health CareProviders Performing Emergency lnterventions in anlnner-City EmergencY DePartmentGD Keten,'T DiGioianni, D Kalainov, L Bisson, E Junkins, A Stein'C Scott, ti Sivertson/Division of Emergency Medicine and Johns
Hopkins University School of Medicine, Balt imore, Maryland-'to det.rmineif health care workers (HCws) adhere to "univer-
sal precautions" we prospectively observed 129 HCWs performing
1,274 intetventlons on i51 coniecutive patients requiring.rapid
intcrventions in an inner-city emergency department located in an
iIv-ende-ic area. Institution-widi and department- specific in-
structional sessions on universal precautions were held for HCWs
itt.or-,ghor'tt the year prior to the initiation of the study'-Interven'
;i;;;;;;; classified as maiot 142.5%) or minor ls7 '4%l depending
nt i}r" pot."tial for exposure as dictated by the universal precau-
tions guidelines. Among the interventions observed, residents
;.tf";;i 473, consuitants 192, attendings 103, nursing staff 97'
iri"-.ai". 7 6, radiograph technicians ! f ,^.a,nd housekeeping,32'
ict ive bleeding *", p.. t . t t t rn 112 174'I%), with 38 , '25'1.%l oI
ifr.." ff..ai"g"ptofrls.ly. Overall adherence was adequate during
16.5% otmai&interventions and 64.8% of minor interventions.(P< .05]. During minor interventions, adherence wes the same for
tr""-, pi.t.tit ations 162.97o1 and nontrauma presentationsl6T 0%)
f p r .OSi. However, in the prese.nct .of pl9f9:: bleeding, adherence
during minor interventiona declined to 19 '77" ir'ttatmatic presen-
i"tio"'t (p < .05) and 07o in nontrauma presentations (P < '05)'
During maior procedures, adherence was 34'0% with traumatic
pt.t.""t"tioi-tt and 0'B% with nontraumatic presentations (P < 05J'
ihe overall adherence rate for HCWs was residents, 58%; attend-
i"gr,lS "/;r.o"sultants, 43 %; nursing staff, 44"k ; paramedics, 8%;
24

radiograph technic ians, l4Y"; and housckccping, g l%. When prc-caut ions were inadequate, surgical masks were used least (22.4%1,fo l lowed by eye protect ion (45.0%), gowns (49.6 ' lo) , and gloves
173.7%1. A quest ionnarre administered immediately af tcr thc studyper iod revcaled that the most common reasons given lor notadhcring to universal prccautions were lack of timc to put onprotect ivc mater ia ls 147%) and inter ference in ski l l fu l pcr formanccof proccdures (33% ). Wc conclude that HCWs in th is se t t inH are nottaking adcquate precaut ions dur ing carc of cr i t ical ly i l l pat icnts andthat other st ratcgies for implemcnt ing univcrsal prccaLl t lons nccdto bc dcvcloped.
*37 Prevention of Disease Transmission by Using Mouth-to-Mask Ventilations During CPRRK Cydulka, PJ Connor, TF Myerstseclion of Emergency Medicine,Northwestern Memorial Hospital, Northwestern University MedicalSchool; Loyola University Medical School, Chicago, l l l inois
The possib i l i ty of d iseasc t ransmission has causccl conccrnamong Iaypcrsons and rnedical personncl whilc pcrforn-ring mouth-to-nouth vcnt i lat ions dur ing CPR. Rcccnt ly , prcfcrcncc has bccncxprcssed for thc usc of protect tve barr icr prccaut ions dur i r - rg CPR.We asscsscd f lows obtainablc whi lc usins r-nask or faccshic ldbarr icrs. We also asscsscd thc adccluacy of barr icr Fr() tcur i ( rnsprovidcd by the use of thcsc dcviccs. Dupl icatc r .ncasurerncnts offorced v i ta l capaci ty {FVC) and onc-sccond forcccl cxpiratory vol-umc {FEV) were obtaincd on two indiv iduals whi lc r - rs ing l7diffcrcnt resuscitation dcviccs. Subsccluent to flow tcstir-rg, alltnasks wcrc stcr i l ized, appl icc l to tho tostors ' faccs: ts d i rcctcd by thcmanufacturcrs' instruction, and cr.rlturccl {or oral flora. Eight of thcdcvices were faccshic lds (Microshic ld ' , Rcsprronics", Resusfacc ' ,Rcsusaid- , Samari tan' , Hygicnic- , Mcdicarc- , Portcx ' ) , c ight wcrcmasks (Dynamed ' , Globc ' , LSP 447 ' , Rcs-Q-Onc", MTM-ER '
,Rightway- ' , MTM-ELV' , Lacdcr l ' )and or-rc of thc c lcv iccs c l id notmcct cr i tcr ia for c i thcr {accshic ld or mask lHudson') . FVC and FEVacl-r icved using c i thcr faccshield or rnask t lev iees wcrc s imi lar{ faccshic ld FVC, 90.5 ' l . prcdictcc l ; SD 10.3 v; mask FVC, 90.3 '2,p r cd i c t ed ; SD 7 .1 ;1 ) > .051 ; ( f accsh i c l d FEV , t 31 .3 ' 2 , p r cd i c t cd ; S t )21.2 v; mask FEV,789% prcdrctcd; SD 15.2, 1) > .05). Al though nosignificant differcnccs arnong FVC valucs wcrc notccl bctwccnmanufacturcrs, a s igni f icant ly lowcr FEV was obtainccl whi lc usingthe Portex ' faccshic ld. No mask dcviccs cr-r l turccl nosi t ivc for oral{ lora, whi lc s ix faccshic ld dcviccs cul turet l p<rs i t ive: for oral f lora (1 '<.0071. Onlv thc Microshic ld ' ancl Portcx ' faccshic ld dcviccs c l ic lnot dcvclop a positivc cultLrrc. In conclusion, wc achicvccl adcquatcf low volumcs wi th a l l mask ancl faccshic lc l dcviccs. Howcvcr, wcrccomrnend using c i thcr a mask dcvicc or the Microshic ld ' faccsl- r -icld for barricr typc protcction whcn pcrforming mouth-to-r-r.routl-rvcnt i lat ion.
38 Incidence of Reported and Confirmed Risk ofExposure to Communicable Disease in an Urban EMSSystemPE Pepe, MJ Bonnin, GD Gray/Departments of Medic ine andSurgery, Baylor Col lege of Medic ine; Ci ty of Houston EmergencyMedical Services, Houston, Texas
It is gcncrally agreed that EMS pcrsonnel arc frcquer-rtly cxposcdto commLrr-r icable d isease (CD) dur ing thc course of thci r dut ics. Wcprospectively studicd a1l possible exposurcs rcportcd within zr largeurban frrc dcpartment-based EMS organizatron durir-rg a l2-monthperiod. Using criteria cstablished by the statc hcalth dcpartmcnt,wc invcstigated all reported CD cxposurcs and then delincatcdthosc that const i tuted a possib lc s ignrf icant r isk for exposurc, suchas a contaminated needlest ick, b lood-splat tcr on nonintact sk in, oraerosolized secretion into the eyes, moLlth, or nosc. Thc rcsultsdemonstrated that cmployees reported 703 possiblc pcrsonnclexposures to CD during the 12 months studicd. Of these 703reported exposurcs, only 99 l l4%) were determincd to havc had anactual potential for significant cxposure to CD. These 99 cascsinvolved 24 exposurcs to patients with AIDS or scrologicallypositive for HIV and to 15 patients with hcpatitis B. Of thc 2(rreported needlesticks, only 20 were determined to be from possiblycontaminated nccdies, but two did involve confirmed HIV-positivcpaticnts and two involved confirrncd hcpatitis B patients. Thcother 16 nccdlesticks involved patients of unknown scrologrcalstatus. In relation to the high number of annual rcsponscs madc byEMS personncl, the reported nurnber of CD exposLrres appears to bevery low. Furtherrnore, the great majority of claimed cxposurcs donot actually involve significant risk. On the other hand, despiteextensrve education and precautionary measlues takcn to prevent
such cxposures, there st i l l ex ists an extrcmcly smal l but f in i te r iskof accidental exposure to lc thal CDs in thc del ivery of prehospi ta lmecl ical carc.
'39 The Persistent Problem of TetanusL Grininger, F Bongard, S Klein/Harbor-UCLA Medical Center,Torrance. California
A2o-ycar (1966 1986) rct rospcct ive analysis was conductcd ofal l cases of tc tanus t rcatcd at Harbor-UCLA Mcdical Ccntcr toidcnt i fy the contemporary c l inrcal prof i lc and pi t fa l ls in recognt-t ion ancl to review thc managcrncnt of cstabl ishcd infe ct ion. Eightcascs wcrc idcnt i f icd, and f ive we re avar lablc for rcv icw, inc ludingthrcc mcn and two womcn {agc rangc, 2 l to 7t t ycars) . No pat icnthad any f r l r rn of systcmic i r lmnrrosupprrssion or rcccivcd propcrpr ior immunizat ion. Al l pat icnts prcscntccl wi th jaw pain, t r isrr - rus,and dyspl-ragia. Two l " rad a history of t r iv ia l uppcr cxtrcmity lace ra-t ions, two had rcccived nccdlcst ick in jur ics, and onc pat icnr wasadrni t tcc l wi th a gangrcnous foot . Thc t i rnc intcrval bctwccn in juryant l onsct of symptorrrs was c ight days to onc month. Thc diagnosisof tc tanus was madc on c l in ical grounds in a l l cascs, and O tcLaniwas cul turcd f rorn thc wouncl of onc pat icr . l t . Onc of f ivc pat icntsunclcrwcnt wound dcbr idclncnt . Al l Dat icnts dcrnonstratcd mr.rsc lcspaslrs that var icc l in scvcr i ty ; two Fir t l rnts reLlu i rcd barbi turatcsancl onc rcr ln i rcd ncurornuscul ; r r par: r lys is t0 achicvc adcquatcvcnt i lat ion. Thrcc c lcmonstratccl cardiovascular instabi l i ty . Four off ivc surv ivccl , and al l had major in-hospi ta l compl icat ions. Wcconcluclc that tc tanLls rcmains a lc thal infcct ious c l iscasc notcn-t ra l ly cumpl icat ing a spcctmrr of c l in ical problcnrs; [ r revent ionwith apprcpr iatc i r ln. r r . rn izat ion is manclatory, ancl a h igh inclcx ofsuspicron is rcquircd tu rccognizc arrc l tn i t iatc ncccssary thcrapy.
40 A Prospective Study Examining the Need forCoverage lor Vibrio Organisms in Saltwater-Contaminated WoundsJS Olshaker, JF Brown, D Tek/Department of Emergency Medicine,Naval Hospital, San Diego, California
Expcr icr . rcc gained in our inst i tut iot . r has suggcstct l that dcspi tcpropcr i r r igat i r )n/ many sal twatcr-contar .n inatct l wouncls that gctno ant ib iot ic covcragc c lcvclo l . r infcct ions. Thc sclcct iot . r of ct .npir iccovcr: lgc f r l r sal twatcr-contar . r . r inatccl wounds has bcen conrrovcr-s ia l bccausc of uniquc r .n icroorgirn isr . r . rs in t l rc r rar ine e l tv i ro l tn l r : nt .Rcccnt l i tcrat l r rc l - ras spcci f ic i r l ly c l iscussccl thc spcctntr .n of d iscasccruscd by Vi l t r lo organis lns. Wc cxanr inccl in i r p l rspcct ivu, r r r r r -cl<lnrzccl stuciy tl-rc frcclucr-rcy ar-rtl clinical e ffccts of Vllrrio organ-isr-r ' rs i r . r sal twatcr-contanr inatct l wounds. Tl ' r i r ty p i t t je nts wurrcntcrccl i r - r t l - rc stucly ovcr: l onc-yci l r pcr iod. Af tcr inr t i : r l cvalu:r t ior . rin thc cucrgcncy dcpartrncnt pat icnts who l - rad a socia l sccur i tynur.nbcr cr-rdrng i r - r : ln cvcn nurnbcr wcrc p l l t on : l scvcn rhy courscof Vcloccf " 250 rng four t i rncs dai ly . Those whosc socia l sccurr tynumbcr cndccl rn an oclc l numbcr wcrc p l l t on a scvcn-day coursc ofVcloccf "250 mg four t imcs dai ly in adcl i t ion to a scvcn-d:ry courseo f Scp t ra DS" . Vc locc f ' was i n i t r a l l y choscn becausc o f i t s b roadcovcragc of most of t l - rc mul t i tudc of org:rn isnrs cx1-rcctcd in mar inc-contaminatccl wouncls. Scptra ' was pickcd as thc scconcl ant ib iot icspcci f ical ly to g ivc at ld i t ional covcragc lor Vibr io. Wouncl cul turcswcrc donc on al l pat icnts bcforc ar-r t ib iot ic t rcatrrcnt w:rs bcgurr .Al l pat icnts wcrc sccn in fo l low-up in our wound c l rn ic in two andscvcn days. Scvcntccn pat icnts rcccivcd only Vcloccf ' . T l - r i r tccr . rp: l t icnts rcccivcd both Vckrccf ' ancl Scptra ' . No pat icnt in c i thcrgroup c lcvclopcd any s ign of c l in ical infcct ion. Onc of 30 cul turcs(3.3 '2,)grcw oLt t Vibr io a lg inolyt ic t ts . Thc samc cul turc a lso grcwottt Acntntonos hyclrr4thilia. Sixtccn culturcs {53'lo) grcw outStaphylococt :us l rurc l ls . No othcr organisrns grcw out in cul turc.Wc c<rnclude that although Villrio organisms do cxlst rn ourmar inc cnvironmcnt i thcy arc rarc ly c l in ical ly s igni f icant . Addi-t ronal coveragc spcci f ical ly for Vibr io is unncccssary, adding extracxpcnsc ancl r is l< of rnedicat ion s idc cf fccts. ln v i t ro data suggcstthat d ic loxaci l l in is a chcapcr, rcasonable al tcrnat ivc to Veloccf- orothcr ccphalospor ins in thc cmpir ic t rcatmcnt of sal twatcr-con-taminatcd wounds.
-41 Management of Pyelonephrit is in an Observation UnitGLH Ward, RC Jorden, HW Serverance/Division of EmergencyMedicine, University of Mississippi Medical Center, Jackson
This study was undcrtakcn to dctcrmine i f pat icnts wi th thecl in ical d iagnosis of pyelonephr i t is could be managed as outpa-t icnts af ter receiv ing thci r in i t ia l t reatnent in thc cmergencydepartmcnt obscrvat ion uni ts. Diagnost ic cr i tcr ia inc luded f lanktcndcrness, pyur ia (> a WBC/hpf ) , and bacter i r - rna greatcr than 1+.
ZJ

!1i
Exclusion criteria consisted of septrc shock (BP < 90 mm Hg), ageIess than I4, male gender, pregnancy, d iabetes mel l i tus, immuno-compromise, and debi l i tat ion f rom chronic i l lness. A11 pat ientswere admitted to the ED observation unit where they received twodoses of t r imethopr im/sul famethoxazole {TMP/SMX) IV at a I2-hour dosing interval. At the end of this period patients werc eitherdischarged on a ten-day course of oral TMP/SMX double strengthor were admit ted for addi t ional IV ant ib iot ic therapy. Al l d is-chargcd pat lents were advised to return for a fo l low-up v is i t rn twoweeks. One pat ient required admission to the hospi ta l , whi le 59pa t ren t s we rc d i scha rgcd f r om thc obse rva t i on un i t . I n c i gh t o f r he59 pat ients ur inc cul tures were er ther lost or not performed; theseeight paticnts were excluded from further analysis. An additionalnine pat ients had negat ive ur ine cul tures and were el iminated f romfurther study. The remaining 42 pat ients had posi t ive cul tures. Onepatient whose culturc grew Proteus mfuabilis had recurrent infec-t ions and requrred admission for removal of a stag-horn calculus.Another pat ient had pers istent cul ture-negatrve pyur ia that re-solved af ter an addi t ional ten-day course of oral TMP/SMX. Thercn-rainder of the paticnts, including thre e with Escherichia coli in-fcct ions resistant to TMP/SMX, did we1l . Based on these data wcconclude that pyelonephr i t is cannot a lways be diagnosed sole ly oncl in ical grounds; and that pat icnts wi th pyelonephr i t rs, despi tesigni f icant fcvcr or nausca and vomit ing, can bc t rcatcd as outpa-t icnts af ter a br ief per iod of observat ion and ant ib iot ics.
.42 Observation Unit Treatment of PyelonephritisHS Israel, JA Marx, SR Lowenstein/Departments of EmergencyMedic ine, Wi l ford Hal l USAF Medical Center, San Antonio, Texas;Denver Af f i l ia ted Residency in Emergency Medic ine, Univers i ty ofColorado Heal th Sciences Center, Denver
Pat icnts wi th pyeloncphr i t is arc usual ly admit ted to thc hospi-ta l for t rcatment. To test the hypothcsis that outpat ient therapy iscf f icacious, wc rctrospect ively rcv iewed the records of 147 pat icntsadmit tcd to thc obscrvat ion uni t of an urban cmcrgcncy dcpart-rne nt wi th a d iagnosis of pye lonephr i t is . A1l pat ients were womcn,with a mcan agc ol 27 + 9 ycars. Most had frcquency, urgcncy/dysur ia, fcver, nausca, f lank pain, fevcr , pyur ia, and leukocytosis.Thcy wcrc t rcatcd wi th IV ant ib iot ics, hydrat ion, analgesics, andant icmct ics. Therc wcre no t rcatmcnt compl icat ions. Eighty pcr-ccnt of thc ur inc cul turcs grcw morc than 100,000 colonies of asinglc isolatc, which provcd t<tbe Escher ichi t t col i in 85% of cases.Af tcr a mcan obscrvat ion uni t coursc <t f 7.4 t 2.9 hours thc oat ientwas admit tcd to the hospi ta l i f c l in ical ly unimproved or wasdischarged on oral ant ib iot ics. Twenty- four pat ients requiredadmission at the cnd of their obscrvat ion uni t course {19) orreturned af ter d ischarge and rcquircd admission ( f iveJ. Intractablepain and vomit ing wcre thc most common reasons for outpat icntt reatmcnt fa i lurc. No histor ical data, physical examinat ion f ind-ings, or laboratory var iable on in i t ia l presentat ion to the ED wcrcpredictive of the outcornc of obscrvation unit therapy. The obser-vat ion uni t is an cf{ect ivc a l ternat ivc to hospi ta l izat ion for thein i t ia l t reatmcnt of most cascs of pyclonephr i t is .
43 Poison Control Centers Are Cost EffectiveJJ Guterman, G Koehler, RL Galli, BE Haynes, MJ Bayer/UCLASchool of Medicine, Olive View Medical Center, Department ofEmergency Medicine, Sylmar, Cali fornia; Los Angeles RegionalPoison Control Center, Los Angeles; Emergency Medical ServicesAuthority, Sacramento, Cali fornia
The California Emergency Medical Services Authority coordi-nates the regional poison control centers iRPCCs). From DecemberI to 7, 1988, each center surveyed callers with regard to what theiractions would have been had an RPCC not been available. Eiehthundred frfteen ouestionnaires were tabulated. Twentv-two oir-cent of respondents wouid have gone to an emergency departmentor private physician. Eight percent would have called 911. Fifty-nine percent would have called an ED or private physician. Eighty-five percent of poison exposure calls from the public are managedby RPCCs at home without further health care {acility expendi-tures. For the six centers reporting data, RPCC annual humanexposure call volume from the public is estimated to be 138,315calls. This est imate is from an eight-month study period in 1987.Cost est imates derived by the EMS Authority include $153.00 foran ED visit, $30.00 for an office visit, and $370.00 for a 9I 1 call. Thetotal estimated annualized cost of care for these Datients had anRPCC not been available rs $8,246,464 to $12,341,t65. The annualoperating budget for the six RPCCs is $4,150,000. The results ofthis survey suggest savings o{ at least $4,100,000 per year in
avoidable health care costs.44 A New Drug Screening System, "Multi-HPLC," byHigh-Performance Liquid Chromatography Using Multi-wavelength UV DetectorS Suzaki, Y Yamamoto, T Otsuka, M Hayashida, M Nihira, TWatanabe/Departments of Emergency and Critical Care Medicine,and Legal Medicine, Nippon Medical School, Tokyo, Japan
Rapid, accurate analysis of poisoning is rather difficult, espe-cially in cases of multiple drug ingestion. We present a newlydeveloped drug screening system. Multi-HPLC, using a micropro-ccssor-controllcd, simultaneous, multiwavelength HPLC detec-tor. The Multi-HPLC system consrsts of reversed phase HPLC witha |ASCO Fine Pak SIL C18 column, a 32-photodiode array ofMULTI-320 multiwavelength (195 to 350 nm) UV detector, and adata processor. The data processing program, DP-L320, analyzesnot only by retention time, but also by the spectrum search andpeak deconvolution method, enabling separation of the superim-posed multicomponent peaks. With the retention time predictionprogram, thc scparation and identification procedure is nearlyautomatic. As a standard drug library, the 47 toxic drugs mostfrecluently encountered in fapan are registered in the system. Ap-proximately 945% of the drug poisoning cases should be covered.In the quantitative analysis, each drug can be analyzed at rtsoptimum wavelength. The sensrtivity (the lowest level of analysis)reaches 10 ng. Possible applications of this system were demon-strated using gastric compounds, sera, and urine specimens ofpolydrug poison victims. The Multi-HPLC system is consideredclinically practical and beneficial.
45 Multiple-Dose Charcoal Therapy for SalicylatePoisoningM Tenenbein, LA Kirshenbaum, DS Sitar/Departments oJ Pediatricsand Pharmacology, University of Manitoba; Manitoba PoisonControl Centre, Winnipeg, Manitoba, Canada
Activated charcoal is administered routinely to overdose pa-tients to prevent drug absorption. The administration of multipledoses of charcoal enhances the excretion of already absorbedphenobarbital and theophylline. This study assesses this interven-tion for acetylsalicylic acid. Twenty healthy adults participated inthis randomized, controlled, two-limbed crossover study. On twooccasions at least one week apart, each volunteer ingested asolution of 2,880 mg of acetylsalicylic acid in 250 mL of 4 to 5 Cwater after an eight-hour fast. Fasting was continued for another l2hours. At four, six, eight, and ten hours after ingestion in theexperimental 1imb, each volunteer ingested 25 g activated charcoalin 125 mL water. Serial blood samples were collected l4 times overthe first 48 hours, as was all voided urine. Serum salicylic acidconcentrations were measured by high-performance liquid chro-matography from which pharmacokinetic variables were derived.Urine salicylate excretion was quantitated by Trinder's method.Student's I test was used for statistical analyses. The area under theserum concentration versus time curve from the beginning of theintervention to the end of the study period showed a decrease inbioavailability oI 9./o. Urinary salicylate excretion was decreasedby 1 8 % . Although statistically significant, they both were quanti.tatively modest and therefore of questionable therapeutic import.Thus we were unable to demonstrate clinically important en-hanced salicylate excretion due to multiple-dose charcoal therapy,
* 46 ln Vitro Adsorption Properties of Activated CharcoalWith Selected Inorganic CompoundsRD Mitchell, CB Walberg, RC Gupta/Department of EmergencyMedicine, University of Southern Cali fornia, Los Angeles CountyMedical Center
Activated charcoal is a weli-known and often-used adsorbent inthe treatment of acute poisonings. Many references recommendthe use of activated charcoal with a number of inorganic com-pounds by listing them in toxin tables. A literature review of theadsorption properties of arsenic, iodine, mercuric chloride, silver,boric acid, and bromide to activated charcoal revealed misapplica-tion of research findings and conflicting recommendations. Labo-ratory evidence that the inorganic compounds described adsorb toactivated charcoal in a significant manner is insufficient or lackingin many instances. The in vitro adsorption properties of arsenic,iodine, mercuric chloride, silver, boric acid, and bromide weredetermined with the followine conclusions: toxin adsorbed relatesdirectly to the dosage and specific preparation of activated charcoal;arsenic, boric acid, and potassium bromide do not significantlyadsorb to activated charcoal, and mercuric chloride. silver, and
I
I
. 26

iodine adsorb to activated charcoal. The in vitro findines forarsenic, bromide, and s i lver have not becn reportcd in the i i tcra-turc. There is documcnted in v i t ro analysis of iodine, mercur icchlorrdc, and boric acid with results sunilar to those reDorted in ourstudy. In vitro studies may vary significantly frorn in vivo findings,thereforc, in vivo rcsearch should be uscd to guide clinical prac-t iccs. .Whcn th is is no1 possib le duc to thc impract ical i ty o i thctoxin bcing studied, current in vitrc.t work should euide oui recommcn t l a t i ons {o r a r . t i va t t d cha rcoa l t r s c .
'47 Activated Charcoal and Sodium polystyreneSulfonate (Kayexalate'D) in Gastr ic Decontamination forLithium lntoxication: An Animal ModelJG Linakis, PG Lacouture, MS Eisenberg, TJ Maher, WJ Lewander,JL Driscol l , AD Woolf/Division of Emergency Medicine, TheChildren's Hospital; Massachusetts Poison Control System;Massachusetts College of Pharmacy, Boston; Department ofPediatr ics, Rhode lsland Hospital; The Rhode lsland poisonCenter, Providence
To dctermine whcthcr sodiurn polystyrcne sulfonatc is cffcc-t ive in clccreasing thc absorption of l i thiurn and to tcst thc :rssump-t ion that l i thium is poorly adsorbecl by activatcd charcoal, I 2lJ rni icwcrc a.dminrstcrcd an orogastr ic dosc of l i thrum chloridc {250 mg/kg) fol lowed imrncdiately by orogastr ic sodium polystyrcnc sulfon-ate ( 10 g/kg SPS group), act ivatcd charcoal (u.6lJ g/kg, AC group), orw.a1er i_n an cquivalcnt volumc (control group). Sr_rbgroups of cachof thc three groups wcrc sacrificcd at onc, two, four, irncl cight hor_rrsaftcr trcatlncnt ancl scrum analyzccl for l i thiurn concuntrat ion.
Time Atter=Lithium Administration (hr)1 2 4 8
2 .69 1 .75 1 .36 1 .26
2 .51 1 .74 1 .83
Case rcports of c lonid ine ingest ions suggcst that such pat tentsusual ly need intensive carc. We rcviewcd 4/ consecutrvc cascs.Mean age o{ pat ients was 2/ + l6 months {rangc, 9 to 134 months).The avcrage t ime f rom ingest ion to symptoms was 52 minutcs wi th75 % of pat ients d isplaying symptorns wi th in onc h, )ur of insest ion.Dclayed progrcssion of symptoms did not occur, and dur i t ion ofsymptoms was 9.5 + 5.5 hours. Averagc length of stay was 33 + I Ihours. Dcpresscd sensor ium occurrcd in 94"k of pat icnts. andbradycardia, l-rypotcr"rsion, or hypcrtcnsir)n was secn rn 79"1, ofpat lcnts. Ovcr onc th i rd of patrcnts had apnea or deprcssed rcspira-t ions. Thcrapy includcd support ive carc {endotrachcal intubat ionin_13% ), gastr ic .emptying { ipe cac 3t i %, ) , naloxonc (40%; dosc rangc,.00U to .22 mg/kg), atropinc (15, /" ) , and dopaminc {2,2,) . Naloxr inec:ruscd t ransicn-t improvcmcnt in l3 of l9 pat icnts. Thrcc pat icntswho rcspondcd later rcqurrcd i r - r tubatron, and in thrcc othcrs,naloxunc w:rs associatcd wi th hypcrtcnsion. Clonidrnc can causcr.najor ncurologic and cardropulmonary cf fccts. Ipccac is cuntra in_dicat_cd c luc to rapid onsct { r f le thargy. Naloxone is a poor ant ic lotcfor ckrnic l inc ancl may inducc hypcrtcnsiorr . Fcw pai icnts rcquirevent l latory or prcssor s l lpport .
50 Dimethyl-PGE, Prolongs Survival From AlphaAmani t inEA Michelson, SM Schneider/Montefiore Hospital, University ofPittsburgh
Alpl ' ra an-ranrt in (A) is thc toxin bcl icvct l rcsponsiblc for dci r t l , rsf rorn ingcst iOrr of thc toxre ntusl t rOt, r .D Art t , tn i to p l ta lkt i t las. l , l ( t -D imc thy l -P ( )E2 {PGE) i s a p ros tag land in w i t h known hcpa t i c cv ,toprotcct ivc cf fccts agalnst scvcral tox i r . rs. T l rc protcetrve nrceha-n i s r . n i s L l ncc r t a i n . Wc t nvcs t rga ted t hc c f f ce t , , f i r ( ;E on t ox i c i t y o fA in our r .nousc ntodcl . Swiss fcrnalc r l icc wcrc d iv ided into f rvcgroLrps : lnd t rcatccl wi th A 0.(r3 mg/ l<g intrapcr i toncal ly . Group Ircccrvccl no fur thcr thcrapy whi lc gror . rps 2 t l - r rough .5 rcce ivcd pGE1.50 gg/ l<g intrapcr i toncal ly af tcr dclays of onc ancl onc hal f , two,thrcc, and f ivc hours f rorn A in jcct ion. A s ixt l " r group rcccivc i l onlyPCE. Anir- r - ra ls wcrc g ivcn f rcc acccss to foocl and watcr and fo l lowci ldai ly for surv ival to onc wcck. Survival c lata wcrc ana]yzccl bvKaplan-Mcicr ancl l l rcs low tcsts. Thcrc wcrc no dcaths rn ih" fCicontro l group, ancl l l i o f 20 1 '90"1,) t lcaths in thc A contrc l group.Orr ly . thc micc in groupr 5 ( f ivc-hour dclay r- rnt i l in jcct ion) cxpci i -cnccc l an i nc r casc i n su r v i va l ( 1 , < .01 ) . pGE fa i l cd t o i nc i cascsurvival whcn givcn wi th in thrcc hours of A; howcvcr, i t wascf fcct ivc i r f tcr a c lc lay of f ivc hours. p( lE prcsr . rmably l - ras a shorthal f - l i fc ant l is no longcr cf fcct ivc two to thrce hours af tcr aclnr in i -st rat io l t . Our data suggest A toxic i ty is dclaycd duc to c i thcrdclaycd abs<tryr t ion or t imc ncccssary for toxtc convcrsron. Wcconclut lc that a s inglc c losc of l , l ( r -d imcthyl-pGE, prolongs s l r r -v ival af tcr cxposurc to a lpha arn:rn i t rn in our rnr)Lrse ln i ldc l , but onlvi f g ivcn fo lkrwing a dclay of f ivc hor-rrs.
51 Empiric Use of Naloxone in Patients With AlteredMental Status: A ReappraisatJR Hoffman, JS Luo, D Schriger/Emergency Medicine Center,UCLA Medical Center, Los Angeles, California
This study was pcrformccl to tcst thc hypothcsrs that thcn]ajor i ty of Opiatc ovcrdose pat icnts wi th a l tcrcd-rncntal s tatL ls canbc idcnt i f icd by c l in ical s igns and symptoms, and that cr-nplr lc Lrscof naloxonc in a l l pat icnts wi th a l tcred mcntal status is thcreforcunncccssaryi as wcl l as cxtrcmcly cost ly . We rcvicwcd rccort ls of230 pat icnts who rcccivccl nal( )xunc f ( ) r . lcLt tu a l tcrcd mcntal status.Only 25 pat ic l t ts (3.4 ' l . )had a complctc responsc to th is agcnt ; l9176%lhad a { inal hospi ta l d iagnosrs of opiatc ovcrdosc. Of thcsc 19pat icnts, 1 i l (95%) had rcspiratory ratcs lcss than or et lual to l2; I 7{90'2,) had constr ic tcd pupi ls ; and 15 179, '1,) had a known hisr , r ry r , fc l rug abuse. Thcse numbers wcrc vast ly d i f fercnt {p < .01 for a l lcompansons) for thc great major i ty of pat icnts who nerthcr re-sponded to naloxonc nor had an ul t i r -nate diagnosrs of opiateoverdosc. Six "complete rcsponders ' provcd not to have opiateovcrdose; thci r assumcd response was f rcquent ly due to spontanc-ous in-rprovcrncnt during a postictal period. partial or questionablcresponsc to naloxone also confuscd the diagnosis in 32 pat ients,nonc of whom proved to have opiate ovcrdose, and onfu ten ofwhom had any c l in ical indicators or possib le opiate usc. Select iveusc of_naloxone rn pat icnts in th is ser ics onihc basrs of easi lydcf ined c l in ical character is t ics would have ident i f ied v i r tual ly a i lresponders with opiatc overdosc and decrcased use of thc drug by897_o. Econornrc savings associated wi th widespread adoptron ofsuch a pol icy would be enormous wi th no appaient c l in ical detr i -
Control (L i th ium mEq/L)Activated charcoal (Lithium
mEq/L)Sodium polystyrene sulfonate
( l i th ium, mEq/L) 1.63 1.04P (Sodium polystyrene Sutfonate
versus contro l ) <.01 < .01P (Sodium polystyrene sulfonate
versus activated charcoal) < .01
1 . 0 6
0.57 0.76
< . 01 < . 01
< . 0 1 < . 0 1 < . 0 5
Stat is t ical analysrs rcvcalcd no ovcral l d i f fcrcr-rcc bctwccn thc ACgroup and thc control groups, howcvcr, thc SpS gror"rp dilfcrccl fronrboth thc contro l ancl thc AC groups at cach t i rnc intcrval , wi thl i th iurn conccntr^t ions s igni f icant ly lowcr in thc SpS group. Thcscresul ts dcmonstratc that socl iurn polystyrcnc sul fonatc cf fcct ivc lyrcduccs thc systcmic absorption of lithium in an rn vivrr n-roclcl, anilthat l i th ium is not cf fcct ivc ly bound by act ivatcd charcoal .
'48 Rate of Absorpt ion of l ron From Chewable Tablets
CS Hornfeldt , JP Winter , LJ Ling/Hennepin Regional poisonCenter, Department of Emergency Medrcine, Hennepin CountyMedical Center, Minneapol is , Minnesota
The treatmcnt of iron poisonings ( 1 1,t34(r, Z 1 %, chcwablc f urr"r-r,l987l is bascd on serurn i ron lcvcls. Thc l i tcraturc of fcrs manytimes for drawing levels, from two to six hours, baset.l rrn adulttablets such as ferrous sul fate. The i ron f rom such tablcts is s lowlyand erratically absorbed. Becausc the ability to clraw a singlc rronlevcl would rnean savings in laboratory tests and cfirergcncy nrrlc/wc hypothesized that i ron f rom chewablc v i tamins is rcadi lvabsorbed and an optimal drawing time for a single scrum iron lcvelcan bc determincd. Hcal thy, fasted adul ts chcwcd and ingcstcd 10and 5 mg/kg of iron in a chewablc vitamin form in t-ri s"narat.studics. Iron lcvels wcre drawn serially over cight to l2 hours. At10 and 5 mg/kg, the averagc peak was 321.2 and24B.4 yrg,ldL, withmean t ime to pcak at270.0 minutes (4.5 hours) and 252.0 minutos{4.2 hours) . Student 's t test for paired data showcd mean t lmes topeak to not be s igni f icant ly d i f ferent {p > . l ) . Mean in i t ia l tota l i ron-binding capaci t ies were 334.2 and 332.4. I ron absorbcd af ter chcw-able vitamin ingcstion reached maxirnum lcvels four to fivc hoursafter ingestion, and a three-hour level was within 9O7" and L)4,% ofpeak, rcspect ively. Al1 subjects had modcrate symptoms. A s ingleserum iron lcvel a{tcr four hours gives a strong indication ofwhether toxicity lnay occur when moderatc amounts of iron havebeen ingestcd.
-49 Clonidine Poisoning in Young GhildrenJF Wiley /l C Wiley, S Torrey, F Henretig/Departments ofPediatrics, Children's Hospital of Philadelphia and St Christopher,sHospital for Children, Philadelphia, Pennsylvania
21

'lli
t
l iI i 'l
52 Endotracheal Naloxone in Rabbits: No AdverseEffects on Blood Gases and Lung TissueSC Rector, RW Geiss, K Beamer, P LeggiEmergency Service, and
Departments of Surgery and Pathology, West Virginia School of
Medic ine, MorgantownWe compaied endotracheal naloxone with normal saline solu-
tion to study the effects on arterial blood gases an-d lung tissue in
16 rabbits. -ihe pulmonary effects of endotracheal naloxone have
not been studied previously. Eight rabbits received naloxone through
an endotracheal tubc, and eight contro ls received normal sal ine '
Blon,l gas.s were sampled {or 30 minutes. Four subiect rabbits and
four controls were killed after two days; the remaining rabbits were
i<i l led af ter s ix weeks. Microscopic analysis of lung t issue was donc
by a pathologist blinded to the identity of thespecimens There was
no significa;t diffcrence in blood gasvalues between the naloxone
anil iontrol groups. By microscopy, therc was no observed pattern
of var iance' in iu lmonary pathology between the subjcct and
control groups. This cxperiment rcvcaled no adverse effects on
rabbl t b lood gases ancl lung t issuc af ter one dose of endotracheal
,rri,,"nt-t" as compared with saline Further study is needcd bcfore
cndotrachcal naloxone can be considered safe for human usc'
*53 Pharmacologic Interventions in Acute CocaineToxicityM Smith, D Garner, J NiemanniDepartments of EmergencyMedicine and Cardiology, Harbor-UOLA Medical Center, Torrance,California
Cocainc toxicity is an incrcasing cause oi mortauty among
.ro"r!"n.y <lcpartment patients. Several experimental models of
"o.r-" t<ixiciiy in whlih subjccts were pretrcated with pharma-
cologic agcnts have appeared in the literature; however, no one has
J.r;;t.i; motlcl in *hi.h th" subiects had cocaine administeredi-r"i-" pt"t"t-rcologic intcrvention. We sought to develop this
-ud.l. hrtt werc catheterized chronically in the iugular vein and
."i,iri,l "t,"ty, had a rcctal tempcraturc probc placc4, and had their
intra-artcr iai prcssurcs and waveforms recorded Thc LD50 of IV
..r."in. was dctermined to bc l4 mg/kg, which was confirmed in a
control group of ton rats with a 50% mortality. Aftcr cxpcrimen-
tally cnsuring thcir nonlcthality, labetalol, dt'azepam, chlorpro-
marrnc, clantiolcnc, propranolol, and nitrendipine were admini-
ri.t"J i--"aiatcly aftcr the LD50 dosc of cocainc' Mortality
ir.."rt.a in the labetalol and propranolol groups (P < '05, chi-
scluarc with Yatcs corrcction factor) and was statistically un-
cha.,ged with thc other agents. No universal antidote for cocaine
;;."" was clctccted. Thcrapy should be dirccted toward treat-
mcnt of symptoms.
54 Agents That Protect Against Cocaine'lnduced Death
and Seizures in AnimalsRW Derlet, TE Albertson/Divisions of Emergency Medicine and
Cl in ical Toxicology, Univers i ty of Cal i iorn ia, Davis, School of
Medic ine, SacramentoA number of agents were studied to determinc their effective-
ness rn protcctlng rats against seizute or death induced by cocaine'
In this model, control ritt wete given 70 mg/kg cocaine intraperi-
i."""ffv. Conirol animals developed seizures 94^%" oI the time, and
82% died in mean t imes of 6.4 t 0.4 and l0 '0 + 0 7 minutes,
i"rpe.tiuely. Animals were given test agents. intraperitoneally 30
minutes piio. to injection oi cocaine' In this model, significant
;lii.;;;;ti".i botit cocaitte-induced seizure and death was af-
forded'by'pretreatment with diazepam, pen-tobarbital, - and the
Ce,sA "p, i i . . b locker SKF 10033A {p ' .Oi) .Only ]ook oI animals
receiving diazepam at the highest dose {2 0 tg/fg) .tested died'
iiri"p.iia.l a.t'd prop.anolol tended to minimally decrease the
a.^, t l .^ , . , but th is d id not reach stat is t icals lgni l icance (P > '05) '
eif'tot"titnia., phenytoin, valproic acid, and labetalol had no effect
r";;il.i;g;h; d."th t"t., th" calcium channel blockers verapamil'
nifedipine, and diltiazem enhanced toxicity' Agents that enhance
the efiect'of the central neurotransmitter gamma-aminobutyric
,"ia "pp.r.,o have the greatest e{{icacy in protecting against the
to"i. ei{..ts of cocaine,-while other classic anticonvulsants, cat-
..t'tttr-in. blockers, and calcium channel blockers failed to pro-
tect .
55 Life-Threatening Events After Theophyllinelntoxication: A Prolpective Analysis of 144 CasesM Shannon, fH LovejoylThe Children's Hospital, Harvard Medical
School, The Massachusetts Poison Control System, BostonTo further characterize the appearance of Iife-threateningevents
lLTEsl such as seizures and severe cardiac arrhythmias, following
ih.*irvllln. intoxication (serum theophylline > 30 pg/mL), we fol-
Iowed i+4 cases o{ theophyl l ine porsoning referred to our poison
""rr*. ou.t a two-and-one -hall'y€ar period. Fifty-two patients had
acute theophylline intoxication; 64 had-chronic.theophylline in-
toxicationiand 28 had acute-on-chronic theophylline intoxication'
Mean age of patients was 32 years (range, 3 days to-84 years|; me11
oeak th"eophvi l ine level was 59.4 pg/ml irange, 30 to 211 pC/mU'
i...r.irt.h featr,res included " me"n potassium level of 3'4 mEq/L
lrange, 2.2 to 5.8 mEq/L), mean glucose of 173 mg/dl ltange, 92 to'iii'istarl, and tre-ori in 45 (31%J. Thirtv-nine patients {27%)
had, i tE (seizures, 13; arrhythmias, 27)- Nine patients died' Dis-
tinct features were iound when acute and chronic theophylline in-
toxication patients were separated.
A steowise logistic regression equation confirmed these correla-
t ions with age, peak theophyl l ine level, and LTEs., excludrng potas-
sium and drug Loingestion as significattl sevariibles' On the basis
of these dataiwe citnclude thai peak theophylline.level predicts
LTEs in patients with acute but not chronic theophylline intoxica-
trun.re"p..di.ts LTEs in patients with chronic but not acute theo-pt 'rvi t in. intoxication, hemodialysis-perfusion is indicated in pa-
i i . i . r t t rvi th acutc theophyl l ine intoxication and theophyl l ine. lev-
"ir- t ioo ptciml, and Lemodialysis-perfusion is indicated for
nati .n ts *hoj iave chronic theophyi l ineintoxication and theophyl-
i inc Ievels of more than 45 pgiml with age more than 60 years'
56lnit ial ECG Findings in 187 Cases of Cycl ic
Antidepressant OverdoseFW Laioie, GG Gansert, RE WeissiDepartment of EmergencyMedicine, School of Medicine' University of Louisvi l le, Louisvi l le '
KentuckyECG changes associated with cyclic antidepressant {TCA) over'
dore h*. been the subject of many reports in the medical litera-
irrr.. u.rt, tr,e, QRS duration, QT inteival, and most recently/ the
i.i-t""t +o -t qns (T40) axis have been reported to be valuable
i;;i;;;;. of TCi overdose. To evaluate the discriminant andpiedictiue abiiities of these and other ECG- parameters in TCA
iu.iaot., we retrospectively reviewed the charts,of all overdose
Datients ad-i t ted to intensive care units of our faci l i ty during a 30-
month period. Of 401 patients reviewed, 358 had initial emergencyJ"o"r,*.n, toxicologic screening, ECGs, and records available for
analysis, and were iniluded in the study. The study population was
aiuid.a into t*o groups based on the presence or absence of TCA
"r i""t"f"gi. ...?.ttt. The TCA+ group comprised 52 2% and the
i-e- gro"i+2.8% of the study population Mean^age was 33 I li
t;. 1; wave axis, PR intervai, initial 40^ms QRS axis, and tota^l
bnS a*is were nof statistically different QRS duration, QTc, T40
ixis, and heart rate were all found to be independently significandy
different between the two groups by t test (P < '001) Using
..-rno"fy quoted discriminating values i> J99 ryt for QRS dura-
ii"". > f OOl-in for heart tate, ald 130" to 270' for T40 axis), we
calculated the sensitivities, specificities, andp.ositive and negativepi.ai"i*. "^t"es (Tabte). Eacir parameter collld be used to correctly
iirr.itv only 607. to 62oh of Cases, with all-four in combination
.o....ily classi{ying only 66/" We conclude,- despite recent re'
Dorts, that ECG parameters, although helpful i f present, cannot be
iJ.i on to include or exclude the diagnosis of TCA overdose'
Peak TheoPhYlline LevelLTE NO LTE P
Acute 117.6 60.7 < 0001Chronic 48.1 48 6 NS
Parameter Sensitivity(%) Specificity("/d PPV
Heart rate 68 59 0 64
QRS duration 44 83 0 74
T40 axis 29 83 0 65
OTc
Age (Years)LTE No Lte P1 8.1 20j NS63.3 31.0 <.0001
NPV Pearson's R
0.63 0.08950.42 0.335'�10.53 0.2315
- 0.2292
57 China White Epidemic: An Eastern United StatesEmergency Department ExPerienceUt Uirtin, J-Hecker, RF Clark, JH Frye, DV Jehle, EJ Lucid/
Medical College of Pennsylvania' Al legheny Campgs, Department
of Emergency Medicine and Emergency Medicine Residency
Proqraml Al legheny General Hospital, Pit tsburgh, Pennsylvania-i:tri"" whlte (i-methyl fentanyl) (3MF), an extremely potent
ry";ili; ;;i;g;. of fentanvl, was implicated in a series ol
28

narcotic deaths in the western United States in the period l9B4 to1985. We report the first outbreak of narcotic overdoies in the Eastinvolving 3MI, which occurred in Allegheny County, pennsylva-nia, in 1988. Emergency physicians became suspicious of 3MF usefol lowing an unusual increase in narcotic ou.rdos., presenring tothe ED coupledwith screens negative for opiates, despite dramlticresponses to naloxone. Speci{ic testing was positive for indicatorsof fentanyl derivatives in some cases. We reviewed g5.246 patientvisits to our ED over the 24-month period |anuary l9g7 ro 0...-_ber l98B for epidemiologic study. patients were included if thevmet the criteria of a suspected unintentional narcotic overdose, buiexcluded if not given naloxone. A cluster was defined as a oeriodwith a statistically significant increase in overdoses above theexpected number for an interval of equal length. Although therewere no_significant clinical differences in case presentation ovcrthe study period, there was a statistically significant, I2-foldincrease in overdoses during the September to November 19ggcluster imean, 13 per month ue.s.rs 1.05 per month, p <.001Wilcoxon rank sum test). A dramatic increase in unintentionaldrug overdose deaths occurred in the county during this cluster.Investigations found 3MF present in street dr.rgr ard parapherna_lia. A total o{ I8 fentanyl-positive unintentio-nal drug overdosedeaths, predominantly male (89% ) and black 156./"), age iange 19 to44 yearc.(mean, 34.9), were reported by the county coroner {13clunng cluster). Narcotic overdoses and unintentional drus over_dose deaths declined sharply with confiscation of the clandestine3MF lab. We conclude that it is important for emergency physi-cians to recognize early that overdoses responsive to n;loxonc withinconsistent routine toxicologic screens may be due to a fentanylanalogue.
.58 Effect of Electric Shock Therapy on Local TissueReaction to Poisonous Snake Venom Injection inRabbits9.S!g!d,t!_4*ol, T Wagner, JL Fatk/Department ot EmergencyMedicine, Orlando Regional Medical Cenier, Orlando, Flori-da;Djvision of Emergency Medicine, Department of Surgery, Universityof Florida College of Medicine, Gainesvi l le
This-study evaluated the ef{ect of locally applied electric cur_rent on local tissye damage resulting from snake venom injection.Female New Zealand White rabbits were anesthetized with 100 meintraperitoneal pentobarbital. proximal hind legs were shaved,cleansed,.and injected subcuraneously with I mg]kg fresh venomharvested from Eastern Diamondback rattles'nalies lCrotalusadamant.eous). Animals were randomly assigned to be shockedigroup A) or sham-shocked (group B). Four tw6-second dischargeseach delivering 1,800 V, 8.18 amps direct current were admilni-stered.directly- through the injectibn site at ten-second intervals,ten mrnutes atter venom iniection. Lesions were measured at 12.24, and 48 hours after injection by applying calipers across the edgesof the short_and long axis o{ the-bulioui lesions by an obse.verblinded to the randomization scheme. Area o{ the lesions wascalculated and indexed for body weight. Lesion sizes between thegroups were compared using the unpaired two-tailed t test. Threeanimals died within 24 hours. Data ate reported as mean + SM.
Group :Short Axis (cm) Long Axis (cm) Area Index (cnf/kg)A B P A B P A B P
Time (hr)12 2 .4 !02 . 2 .9 !0 .4 .29 3 .110.3 4 .o l . } .4 .11 2 .8 10 .7 4 .0 i1 .1 .3 .1 .3124 2 .510.4 3 .310.3 .13 3 .5 t0 .5 3 .9 t0 .4 .56 3 .3 t0 .8 5 .311.1 .16 .1648 4.6i0.4 4.610.7 .99 7.2:tO.7 6.6t0.8 .57 1 1 .grt .5 1 i .512.4.88 .88
In this rabbit modei we were unable to confirm Drevious anecdotaireports of the efficacy of electric shock therapy in amelioratinglocal tissue destruction resulting from snake envenomation. Fur-ther study of this treatment using technical variations is warrantedbefore discarding it as useiess.
59 Acute lron Poisoning in Children: Evaluation of thePredictive Value of Clinical and Laboratory parametersNA Schonfeld, AJ Haftel/Childrens Hospitpkqf Los Angeles, LosAngeles. Cali fornia "*t; .M Wm
Ingestion of iron-co464rffiW@llri^tions is the fifth mostcommon toxic ingpsXqfuftfthffdien. The clinical severity is usu_ally correlated tffi ffi&ilnum semm iron level attained withinthe t lrst srx hoursbfrer ingestion. Minimal toxicity is found withiron levels below 300 pg/dl. Many hospitals, however, do not
provide iron levels on an emergency basis. One hundred hospitalswi th.24-hour emergency serv ices were surveyed, and only '50%cou_ld provide an iron level in less than six hours. This studyevaluated whether certain clinical and laboratory parameters couldbe used to predict serum iron level and, therefori, the severity ofacute iron ingestion in children. The records of childrcn whopresented to the Childrens Hospital of Los Angeles emergency de-partment from 1978 to 1985 for acute iron ingestion were rcviewed.One hundred four children were seen in the ED for acute ironingestion during that period;94 were included in the study. The agerange was I I months to 6.5 years, with a mean of 30 months. pealserum iron levels ranged from 38 to 923 p.gldL, with a mean o1272pg/dl . F ive laboratory or c l in ical parameters s igni f icant ly (p < .01)correlated with serum iron levels of 300 gg/di or greater: agc onpresentation of less than 2years; vomiting; WBC count in excess of13,000 mL; anion gap greater than l ( r mEq/L; or the presence ofradiopaque densities on abdominal flat plate radiograpliy. Of thescfive risk factors, no child in thc study with zero risk-factors had alevel of 300 prg/L or more. Conversely, all children with two or morcof these r isk factors had levels in excess of 300 pg/L. Thc c l in icaland laboratory parameters of age at prescntation; presence of vom-itjng, WBC count, anion gap, and KUB appearance can be used toident i fy chi ldrcn at r isk for toxic serum levels of i ron.
'60 Polymyxin B for Experimental Shock FromMeningococcal EndotoxinG Baldwin, G Caputo, G Alpert, J Parsonett, G Siber, M Baskin, GFleisher/The Children's Hospital, Harvard Medical School, Boston,Massachusetts
One third of chi ldren with meningococcemia devclop shock anddie. Polymyxin B has been reportcd to ameliorate endotoxic shockdue to Escherichitt coli by binding endotoxin. We performed doseti trat ion curves with mcningococcal cndotoxin and studiecl thccffect on mcningococcal cndotoxin-induced shock in a rabbitmodel. Femoral arterial and vcnous l incs were placed, and rabbitsrc-ceivcd IV sal ine, cndotoxin (10 Ug/kg), or polymyxin B (5 mg/kg)30 minutes prior to endotoxin. pulsc, rcspirat ion, mean aricr lJlpressurc,_artcrial blood gases, and levcls of cndotoxin and tumornecrosis factor were monitorcd. Rabbits receiving cndotoxin (six ofsix with seven of seven without polymyxin B) but not sal ine {zcroof f ive) developed shock as indicated by tachycardia, bradypnea,hypotension, rnetabolic acidosis, and death by 24 hours.
Time After Endotoxin (min)0 120
Pulse RespirationsSaline 212 228Endotoxin(mg/kg) 224 260Bindingendotoxinwrth
MAP Pulse Respirations91 212. 160.
92 305 108
MAP1 03-
8 1
polymyxin B 221 267 92 308 g4 89
The group receiv ingpolymyxin B did not d i f fer (p > .05)f rom the onetreated wi th b inding endotoxin (Table, .p < .05). Endotoxin andtumor necrosis factor levels were undetectable in controls andpeaked at I to 20 ng for endotoxin and 1,100 to l , ( r00 U for tumornecrosis factor {0.1 mL} in the endotoxin- t reatcd groups. We did notshow protection by polymyxin B in meningoiocial cndotoxinshock.
'61 Bacteremia in Children With Otit is MediaSA Schutzman, S Petrycki, GR Fleisherffhe Children's Hosoital.Harvard Medical School, Boston, Massachusetts
Occult bacteremia occurs in 3 % to 5 % of young febrile childrenwith no apparent source of infection and carries a risk of suDDura_tive complications. Although otitis media is a frequent o.currince,the incidence of associated bacteremia has not been well studied.To quantitate the incidence of bacteremia in otitis media, chartswere reviewed from consecutive patrents seen Novembe r l9g7 toMarch 1988 in The Children,s Hospital emergency department,ages 3 to 36 rnonths, who had temperatures of 39 C or more and whowere diagnosed with isolated clinical otitis media. Seven hundredforty-eight patients were identified. Blood cultures were obtainedfrom 421patients 156%1, and, all were treated with oral antibiotics.The mean temperature of children who had blood cultures was 39.gC versus 39.6 C in those who did not (p< .00I ). Mean ages of thosewith and without blood cultures were l4.l and Il-.6 months.respectively {P< .001). Fourteen of 421 patients (3.3%} who had
29

rlli
blood cultures were bacteremic. These included ten with S pneu-moniaet one with H influenzae, two with N meningitidis, and onewith Salmonella. An increased incidence of bacteremia occurred athigher temperatures, s ix oI 276 12.2%) wi th a temperature of 39.0to 39.9 C were bacteremic versus eight of 145 ! ,5.5%) of chi ldrenwith temperature above 40 C (P : .07). However, 43o/" oI thebacteremic pat ients had a temperature less than 40 C. We concludethat young febr i le chi ldren wi th ot i t is media had a 3.3% incidenceof bacteremia, a comparable rate to those previously reported withno focus; and failure to obtain a blood culture on all children ages3 to 3(r months with temperatures of 39 C or more and otitis mcdrawi l l re sul t in an inabi l i ty to detect a large number of pat ients wi thDacteremla.
.62 An Evaluation of the Emergency DepartmentTreatment of Status Epilepticus in ChildrenSA Phi l l ips, RJ Shanahan/Department of Neurology, StanfordUnivers i ty Medical Center, Stanford, Cal i fornia; Department ofPediatr ic Neurology, Chi ldren's Hospi ta l , Oakland, Cal i fornia
We reviewcd emergency department records of 161 episodes ofstatus cpi lcpt icus in chi ldren f rom i983 to 1987. In i t ia l t reatmentwas administered in an ED at a community hospi ta l {CH) in 43%of cpisodes, a community medical ccnter (CMC) in 207", and acounty hospi ta l (CoH) in [ i%, and 29Y" wcre t reated at Chi ldren'sHospi ta l . Sixty- two pcrccnt were boys and 3U% were gi r ls (agerange, I month to 17 years; averaget 3.1 years) . Wc compared thetrcatmcnt rcceived in refcrcncc to three Daramctcrs - - ant iconvul-sant dosage iAD), t iming of administrat ion (TA), and ant iconvul-s ivc scqucnce (AS) - - wi th reccnt ly publ ished protocols for thc t reat-mcnt of status epi lcpt icus in chi ldren. Thc avcrage seizure durat ion{ASD) and thc f rcqucncy of intubat ion (FI} werc also reviewed inrcfcrcncc to the abovc Darameters.
CH CMC CHO CoHn = 70 (6hl n = 32(ok, n= 46(o/d n = 12lohl
AD' 38 (54) 18 (56) 46 (100) 7 (59)AD<' 30 (43) 1 1 (35) 0 4(33)A D > i 2 ( 3 ) 3 ( 9 ) 0 1 ( 8 )TA' 25(36) 14 \44) 44 (96) 3 (25)TA' 45 (64) 1 8 (56) 2 (4) 9 (75)AS ' 42 (60) 19 (59) 43 (93) 8 (67)AS3 28 (40) 13 (41) 3 (7 ) 4 (33)
FI ASDe4 (min)6 1 1 0 573 16350 9853f 9776' 1395 6 1 0 1 ,83 146.
( 4 , P < . 0 5 )lRecommended, ' �Delayed, 3Not recommended
Wc conclude that by fo l lowing publ ishcd protocols {or thc t rcat-mcnt of status cpilcpticus in childrcn thc average scizure durationand thc incidence of intubatron appears to be decreased. This is lessl ikely to occur rn an ED in a CH, a CMC, or a CoH. Undertreatment,c i ther in thc administrat ion of less than thc rccommended ant icon-vulsant dosagc and/or delayed timing of administration, increasesthe frequcncy of intubation and scizure duration.
-63 Staples Versus Sutures for Wound Closure in thePediatric PopulationSM Dunmire, DM Yealy, R Karasic, S Fuchs, RD Stewartiuniversityof Pi t tsburgh Af l i l ia ted Residency in Emergency Medic ine; Centerfor Emergency Medic ine of Western Pennsylvania, Pi t tsburgh
Wound repair with staples has been found to be a raprd andcffcctivc alternative rn suturing in adults, but has not been studicdin the pediatric population. This technique offers the potentialadvantage of a faster wound closure for the child, resulting in a lessemotionally trying experience for the patient/ parents, and physi-cian. We desrgned a prospective, randomized trial to comparesuturcs with staples in the pediatric patlent, specifically examiningclosure trmes and cosmetic results. Thirty-eight children rangingin age frorn 1B months to i6 years with iacerations of the scalp,trunk, and extremities were included. Wound closure by trainedhousestaff was preceded by a standardized irrrgation and anesthesiaprotocol. Sutures and staples were removed seven days after clo-sure. Photographs of the wound taken eight to l2 months afterrepair were revrewed separately by three plastic surgeons blinded tothe method of closure. Cosmesis was rated on a scale of 0 to 3,which scored width and discoloratlon of scar. orominence of sutureor staple holes, and hair loss. Data were analyied using a two-tailedWilcoxon rank sum and Student's t test. with the aloha eror set at0.05. The mean t ime of sk in c losure wi th staoles *r i 0.97 minutescompared wi th 20.9 minutes for suture. .pr i r 11, = .000001). Themean cosmetic score o{ 2.3 for both suture and staole closures wasnot significant. No significant differences were found between thegroups when reviewing age, race, length, and location of laceration.
In conclusion, scalp and extremity wound closure by stapling wasfound to be significantly faster and cosmetically equal to suturingin the pediatric population.
.64 Six Years Experience in Emergency DepartmentResuscitation and ICU Treatment of Drowning: PatientCharacteristics Predictive of Outcome and Evaluation ofConservative ManagementJ Lavelle, KN Shaw/Department of Emergency Medicine, Children'sHospital of Phi ladelphia; University of Pennsylvania School ofMedicine, Phi ladelphia
Drowning is a major cause of accidental death in children, butcontroversy exists regarding its treatment and the patient charac-terrstics that prcdict outcome. Most centers advocate some form ofcerebral resuscitatrve therapy iuse of steriods, barbiturate coma,and aggressive treatment of raised intracranial pressure). At ourinstitution a more conservative approach rs practiced, limited tothc support of vital systems. Review of all ICU admissions fromfanuary 1982 to December 1988 identified 54 patients with signifi-cant submersion injury. Forty-four patient records were avaiiablefor rctrospective analysis. Data were gathered regarding the cir-cumstances of submersion and rescue, condition on arrival in theemergency dcpartment, and hospital treatment and outcome. ICUtreatment consisted of modest fluid restriction { 75 % maintenance}and normalization of blood pressure and arterial blood gases.Prchospital variables, apnea and asystole, were associated withpoor outcome as were ED characteristics, nonreative pupils, asystole,pH less than 7.1, and Glascow Coma Scale of 5 or less (P < .01).However, in patients with these poor predictors, l0% to 24% stilthad intact survrval suggesting that resuscitative efforts in the EDmust not be withheld from any comatose patient. On arrival at theICU, a Glasgow Coma Scale o{ less than 5 was associated withdeath or vegetative state. Improvement in the neurologic examina-tion from the ED to the ICU was an indicator of sood outcome.Characterist ics not useful in prognostication wer? age under 3years, submersion time of five minutes or less, time to resuscita-tion of ten minutes or more, and cyanosis at the scene. Comparisonof outcome in patients who received conservative management tooutcome with those who received aggressive cerebral resuscitationlConn, Canad Anaesth Soc l, l98ol, did not demonstrate a benefitfrom thc more complicated therapy. The findings of the presentstudy cmphasize the role of prevention, prehospital care, and EDmanagement in the care of submersion victims. Additionaily,conscrvativc managemenr appears as effect ivc as aggressive resus-citat ion.
-65 Comparison of Serum Phenobarbital Levels AfterSingle Versus Multiple Attempts at IntraosseouslnfusionK Brickman, P Rega, M Choo, M Guinness/Emergency MedicineResidency, St Vincent Medical Center, and The Toledo Hospital,Toledo, Ohio
For nontraumatized bone, in which a single intraosseous at.tempt was used for drug infusion, serum drug levels have provencomparable to those drugs administered intravenously. However,in the clinical situation, inexperienced personnel may performmultiple intraosseous attempts. This potentially could allowsignificant extravasation form multiple intramedullary entrancesites. Our study was designed to compare serum drug levels arisingfrom traumatized bone {multiple intraosseous attempts) with thosearrsing from nontraumatized bone (single intraosseous attempt).We administered phenobarbital to 24 dogs randomly divided intotraumatized (13) and nontraumatized ( l l lgroups. In the trauma-tized group, we created three intramedullary insertion sites in alinear fashion and infused only through the central site. In thenontraumatized group, only a single infusion site was created.Phenobarbital then was infused into the intramedullary space, andcentral venous phenobarbital samples were collected at one-,three-, six-, and ten-minute intervals. The single-attempt, non-traumatized/group attained signficantly higher serum phenobarbital levels at each interval compared with the multiple-attempt,traumatized group iP < .0001). Therefore, it is critical to achievesingle-attempt intraosseous needle placement for intraosseousinfusion to be an effective mode of therapy.
'66 Comparison of Intravenous and lntraosseousAdministration of Epinephrine in a Cardiac Arrest ModelSG Crespo, WH Spivey, M Scholfstall/Department of EmergencyMedicine, Division of Research, The Medical College of
30

Pennsylvania, Phi ladelphiaThis study compared serum catccholamine levels and blood
pressure response to int raosseous and intravenous ( IV) epinephr inein a cardiac arrest model . F i f teen swine (10 to 15 kgl wereanesthet ized wi th ketamine intramuscular ly and alpha-chioraloseIV and ventilated with room air. Thc right femoral artery, carotidartery, and external jugular vein wcrc cannulated for blood sam-pl ing and blood pressure measurement. Cardiac arrest was inducedwith 50 to 60 Hz current delivcred to thc right vcntriclc by venouspacemaker. Blood pressure and lead II ECG were monitorcdcontinuously. Blood sarnplcs for epincphrinc were drawn bcforearrest and every two rninutes thereafter; at fivc minutcs, cardraccompressions were in i t iatcd wi th a mechanical rcsusci tator andthe animal was vcnt i latcd wi th 100% oxygen. Frvc animalsreceived no furthcr therapy and servcd as contiols; fivc receivccl IVepinephr ine 0.0I mg/kg at tcn and 20 minutrs af t t ' r arrcst , and f ivcreceived intraosscous cpinephr ine 0.01 mg/kg. Blood samples wcreassaycd for epincphr inc using a Bcckman high-prcssuie l iquidchromatograph.Epinephr ine and mean arter ia l p." . rur . (MApIarcl is ted for contro l , IV, and intraosscolrs infusion at bascl inc and ats ix, 12,22, and 30 minutcs zr f tcr arrest .
Thcre has been much recent literaturc supportlng the rcsur-gence of use of the intraosseous route of access in Dcdiatr ics.Intraosseous l ines providc a t imcly noncol lapsib le rout . to thecrrculat ion in rnedical or t raumat ic emcrgenci t ls whcn IV access isunobtainablc. Therc has bccn no contro l led study compar ing IVand intraosscous loading of phenytoin. A 15 mg/kg dose ofp- l - renytoin was administered over l5 minutes to p ig i 'us ing ei therthe IV (s ix) or t ib ia l int raosscous route (s ix) . fcmbral ar tery b loodsarnples were drawn cvery f ive minutes for 35 minutes af tcrin i t iat ion of thc infusion to dctermrnc phenytoin lcvels. There wasno stat is t rcal d i f fercnce between thc two groups using analysis ofvar iancc rcpeatcd measures (P =. i06). I t has bccn suggested thatalkal ine substanccs or thosc wi th h igh osmolar i ty rnayi iamagc themarrow' howevcr, mrcroscopic examinat ion of thc corte i andmarrow at thc int raosseous s i te rn the sc pigs was nonnal f ive wceksaf ter rnfusion. Wc concludc that the rntraosseous rourc ls ancf fect ivc a l tcrnatrvc to IV loading of phenytoin wi thout pernanentdar-nagc ttl thc marrow.
69 Crit ical Lessons From Prehospital pediatric CardiacArrestRF Lavery, BJ Tortella, CC Griff in/New Jersey Trauma Center,University Emergency Medical Services, New Jersev MedicalSchool; University of Medicine and Dentistry of NewJersey,NewarkThis report examined pediatric (<18 years old) cardiac arrest oatients over atwo-year per iod. History, mechantsm of in lury. on-scene t imes, ano proceoureattempts and successes were obtained from mobile intensive care unitambulance run sheets. Forty-seven patients were reviewed, representing 3%of all pediatric advanced life support responses, and were divided into medical(61%) and surgical (39%) cases. Mean on-scene t ime for a l l arrests was 13.0mlnutes. Medical arrest mean on-scene t ime was 15.2 minutes, which wassigni f icant ly longer than that for t raumat ic arrests, 9.9 minutes (p < .05). Meanon-scene t rme for unsuccessful lV l ine placement was 10.4 minutes, whichwas s igni f icant ly shorter than that for successful cases, 15.0 minutes (p<.05). Further data analysis revealed the fo l lowing:
Epinephr ineMAP
Epinephr ineMAP
Route ofAdministration
InlraosseousIntramuscular
Controls
Basef ine 6 12. 6 1 . 4 7 6 ! 4 3 3 8 1 1 81 ' 1 6 r ' 1 5 4 2 ! 1 4 3 1 ! 1 7
22 303 6 1 1 4 3 8 1 2 11 8 1 5 1 2 + 3
Intraosseous Epinephrine at 10 and 20 MinE p i n e p h r i n e 1 . 5 1 1 9 5 1 1 0 0 2 9 1 ! j Z 4 Z g 7 ! 9 6 9 6 1 4 0M A P 1 2 0 r 3 8 5 3 1 1 1 4 1 r 2 4 3 4 + 2 1 2 5 r 1 4
An ANOVA dcmonstratcd a s igni f icant incrcasc in cpincphr i t - rclevcls at 12 and 22 minl l tcs for thc IV and intraosscr)Lls groupscompared with controls. Thcrc was no diffcrcncc bctwccn thc iVand intraosscous groups. Thcsc data suggcst cprncphr inc is t rans-portcd to thc central circulation as cffectivcly as front thc boncduring cardiac arrcst.
67 Comparison of Intravenous, Intraosseous, andIntramuscular Administration of Succinylcholine inSheepGP Moore, SA Pace, W Busby/Emergency Medicine Residency,Fort Hood, Texas; Emergency Medicine Residency, Madigan ArmyMedical Center, Tacoma, Washington
The intraosscous route of vascular access has bccn ponularizcclrccent ly for resusci tat ion in chi ldrcn. Succinylchol in" has [ r . "n an-ecdotally_ rcported for airway maltagcrncltt rntraosscously. Thisdrug coulcl bc used for control of thc airway in pcdiatrii burr-rs,status epi lept icus, head in jury, or combat ivc pat icnts. No scr icsquantifying thecfficacy of thc intraosscous rouic has bccn rcportcdfor succinylcholine. To accornplish this goa1, six sheep scrvrng astheir own contro ls were ancsthet izcd wi th halothanc and intu-bated. Succinylchol inc (1 mg/kg) was givcn, and t l . rc t imc torcspiratory arlest as wc11 as thc loss of the ,'train-of-four" stimula-tion of the anterior tibial ncrve was notcd. Each shccp was studicdsuccessively using the IV, intraosseous, and intramuscular routcsof administration with a minirnum of seven days scparating trials.Results werc as follows:
lV Epinephr ine at 10 and 20 Min1 . 1 r 1 . 8 5 1 t 1 8 2 3 5 1 1 1 8 2 9 2 t 2 1 7 3 8 ! 2 3' 1 1 6 r 1 2 4 2 ! 1 3 6 5 1 1 7 5 6 r B 2 4 + 1 2
Average Time to Average Time to LossRespiratoryArrest of"Train-of-Four"(sec) (sec)30.8 t 7.3 93.3 t 34.057 .5 r 10 .3 100 .8 !24 .2
230.0 : t 106.0 291 .0 t 109.0
Endotracheal On-scene lV Line On-sceneIntubation time (min) t ime (min)
ETI No ETI tV No tVAttempl Success Attempt Attempt Atlempl Success Attempt AttemDI88"" 86" . 1 ' � . / 5 .0 58 . . 30 . . 11 .7 9 .596% 820/" 13.2 3.0 93% 78% 13.4 6 5
Age< l y r
> l y r
All groups_were statistically significantly diffferent using thc I testfor thc di { ference o{ means {P < .0015). Wc concludc that thc in-traosscous route of administration of succinylcholinc in this scriesof shcep is comparable to the IV roure and is superior to the intra-muscular route.
.68 Comparison of Intraosseous Versus IntravenousLoading of Phenytoin in Pigs and Effect on Bone MarrowPJ Vinsel, GP Moore, KC O'Hair/Department of EmergencyMedicine, Darnall Army Community Hospital, Fort Hood, Texas
This is thc f i rs t rcport of on-sccl tc t imcs ancl succcss ratcs forpcdiatr ic cardiac arrcst pat icnts. Thc data show that paramcdicsspcncl s igni f icant ly longcrat thc scenc wi th rncdical than wi th t rau-mat ic arrosts/ yct c l r not c lc lay on thc sccnc whcn r . rnablc tocstabl is l - r an IV l inc or intubatc. Whcn cxamining thosc pat icntslcss t ] ran I ycar o ld, paramcdics havc a tcnclcncy to 'sc iop anclt ransport" and furgo intubat ion and forgo intr - rbat ion and IV l incp lace t t t , t t t . T l t e r ea : r , ns f o r t h i 5 a r t p r csc ' n t l y und l : r i n v r . s t i l i l i ( ) l t ,but t l - rcsc data c lo s l rpport cxpansion of thc pcdiatr i . rcg,-r . , .nts u iparamccl ics ' curr iculum to providc grcatcr c l in ical conf idcncc andtcchnical sccur i ty . Thcsc data also ra isc thc c lucst ion as to whcthcrth is "scoop and t ransport" tcndcncy may bc promptcd by paramcdicdiscornfor t wi th pcdiatr ic IV and ai rway managcmcnt.
70 Caretaker Neglect and In jury Prevent ion Instruct ionfor Preschool Chi ld In jur ies:475 Consect ive CasesDM Cl ine, T Grant , J King, C Snow, E Katz, A Stewart , E Carrol ,TW Whit ley/Departments of Emergency Medic ine, HomeEconomics, Psychiatry, and Pediatr ics, East Carol ina Univers i tv ,Greenvi l le , North Carol ina
Prcschool in jury rcduct ion through instruct ion has bccn docu-mentcd, but not in thc cmergcncy dcpartmcnt. A pancl f rom thecmergcncy rnedic ine, chi ld dcvcloprnent, psychiatry, and pediat-ncs dcpartmcnts rct rospcct ively rcv icwcd 475 consecut ivc in jur icsin 366 chi ldren, agcs I to ( r0 rnonths. Group conscnsus was reachcdconccrning pcrccived caretakcr neglcct leading to in jury, chi ldabuse, prcvcntablc in jur ies, and documentcd instruct ion. Carc-taker neglect was perccived in 40% of in jur ies: poor supervis ion,18.3%,; poor chi ldproof ing, 7.2o/o; more than 24 hours delay, 2.3%;and multiple typcs, 12.7'k. No significant di{fercnces werc founclin neglect f requencies for chi ldren wi th one (282), two (( r1) , threel2 l l , or four ( two) emcrgency vrs i ts dur ing thc 30-month studyper iod. ,Chi 'sc luare rcvcaled that burns and poisonrngs had s igni f i -cant ly h igher ncglect f requencres, whi le in jur ies f rom {al ls , la iera-t ions, and sprains had s ignf icant ly lower neglect f requencies. Basedon the chart, thc panel recornmended Social Servicc investicationfor 43 children: physical abuse, five, all rcported; repeated nJglect,
3 l

1|i
i iiirl
38, 16 reported; 14 unreported; and rn eight cases the chart refutedsuch need. Thirty-eight percent of injuries were potentially pre-ventable through childproofing 120%) or supervision (18%), butinjury prevention instruction was documented in only 77o. Exam-ining all documentation, the potential for injury prevention is notbeing addressed by emergency staff for this patient population.
71 Variables Predict ing the Need for Major ProceduresDuring Pediatric Critical Care TransportKA McOloskey, W King/The Chi ldren's Hospi ta l , Harvard MedicalSchool , Boston, Massachusetts; The Chi ldren's Hospi ta l ofAlabama
Few standards exist for determination of when to use a oediatrrccr i t ical care t ransport team to t ransfer an acutely i l l chi ld f rom anonpediatric hospital to a tertiary care center. This cross-sectionalstudy evaluated c l in ical cr i ter ia to a id in that determinat ion. Threehundred sixty-nine pediatric transports were evaluated by multiplelogistic regression analysis on six variables: age, vital signs, recentseizure act iv i ty / current endotracheal intubat ion, current respira-tory distress, and respiratory diagnosis. The outcome variable wasthc nced for major procedures (chest tube intubat ion, int raosseousinfusion, umbi l ical catheter p lacement) dur ing t ransport . Maiorprocedures were performed dur ing 33 of the 3(r9 t ransports (8.9%).Pat ients wi th currcnt intubat ion had 2. I t imes thc odds of requir inga major procedure as compared wi th a nonintubated pat ient lP : .07 ,a lpha =.10). Pat ients less than 1 yearof agewithunstablevi ta l s ignshad (r .4 t imes thc odds of requir ing a major procedure comparedwith pat ients in that age group wi th stable v i ta l s igns (P = .004). Inpat ients o lder than or age 1, v i ta l s ign stabi l i ty was not a s igni f icantfactor (P = .41 ) . I f in tubat ion, age, and v i ta l s ign status werc used asabove to dctcrminc the use of the t ransDort team, 113 of thc 369transports (30% I would have used thc tcam. Thc t rue -posi t ive rate,that is , cascs in which the procedural expert ise of thc tcam/MD wasnecded, would have been 18.6%. The fa lse-negat ive rate, that is ,cascs in which thc tcam/MD was not uscd but proccdural expcrtiscwas nccdcd was 4.9"/" .
72 Pediatric Risk of Mortality (PRISM) Score: A PoorPredictor in Triage of Patients for Pediatric TransportRA Orr, T Venkataraman, CA Singleton/Department ofAnesthesiology/Crit ical Care Medicine and Pediatr ics, Children'sHospital of Pit tsburgh, University of Pit tsburgh, Pit tsburgh,Pennsylvania
Risk of mortality indiccs validated for intcnsive care {ICU) havebcen uscd to evaluate triage of patients requiring pediatric trans-port. Pcdiatric transport patlents admrtted to ICU may require ahigher lcvel of care, that rs, major interventions during transport.The validity of the PRISM score, a risk of mortality index, inidentifying pediatric transport patients who require admission toICU has not becn demonstrated. We studied all patients requrringpediatric transport to our hospital bctwcen October and Dccember19U7 to test whcther PRISM can identi fy patients who need ICU.PRISM was scorcd at initial phone contact and on arrival of thetransport team at the referring hospital. Pediatric transport out-come was defincd as admission location in our hospital (ICU versusnonICU). Phone contact PRISM and eight-hour therapeutic inver-vcntion score (TISS) of patients admitted to each locatron werecompared. One hundred fifty-six patrents were studied; 77 went toICU and 79 to nonICU areas. Sixty-nine of 77 ICU patients had apredicted risk of mortality oI 5%" or less. Of these 69 patients, 4216t %1 were intubated, 14 l2\%lneeded inotropes, 13 (I9%) neededdrugs for active seizures, and cight ( 1 2% ) needed more than 20 rl.Llkg fluids for hypotension. The sensitivity of a phone contact PRISMscorc greatcr than 1 in correctly classifying patients going to an ICUarea was only 64%, decreasing to 137" for phone contact PRISMscores greater than 10. InIact,25 of 84 i30%)patients with a phonecontact PRISM of 0 required ICU. Overa11, 145 of 156 patients hada low predicted r isk of mortal i ty (< 5%) based on phone contactPRISM and age. ICU patients had higher TISS scores 120.6 r 14.5versus 3.9 + 3.7, ICU versus nonICU, P < .001). TISS for patientswith a predicted risk of mortality 5% or less was also significantlyhigher for ICU patients (19.8 t 14.8 versus 3.8 + 3.6 ICU, versusnonlCU, P < .001). Ninety-three percent of patients transported toour hospital had a predicted risk of mortality of 5 % or less, and 48"/oof patrents with a predicted risk of mortality of 5% or less requiredICU. ICU patients did require a higher level of care based on TISS.The sensivity of the phone contact PRISM score in identifyingpatients requiring ICU was poor. A particular phone contact PRISM
score did not reliably identify patients requiring major interven-tions during pediatric transport who were subsequently admittedto ICU. Risk of mortality indices should not be used for triage o{pediatric transport.
.73 The Associat ion Between Scene Time, PrehospitalProcedures, and Iniury Severity Parameters AmongSeverely Injured PatientsD Tse, DW Spaite, TD Valenzuela, EA Criss, HW Meisl in, MMahoney/Section of Emergency Medicine, College of Medicine,University of Arizona; Tucson Fire Department, Tucson, Arizona
To evaluate the relationship between injury severity and timespent at the scene by paramedics, we studied 98 consecutivepatients with Injury Severity Scores (ISS) greater than 15 brought toa Level I trauma center by EMS personnei from a medium-sizedmetropolitan fire department. Complete hospital records wereavailable for each patient, and autopsy reports were obtained for allfatalities. There were 66 men and 32 women wrth a mean age of 34.4years. Thirty-two patients died 132.6%1. Blunt and penetratingtrauma accounted for 68.4o/" and 3I.6To of cases, respectively.Mean scene t irne (ST) was 8.14 min (SD, 3.481. ST versus injuryscvcrity parameters revealed the following:
Trauma ScoreVariable 0-12 13-16Patients 46 51(mean) 7.65 8.73I tes t (P) < .07Procedures 2.26 1.29Itest P <.0005
GCS ISS Fatality3-1213-15 21-7516-20 Yes No60 37 71 27 32 667.80 8.89 7.85 8.93 7.97 8.23<.08 <.08 >.25
2.00 1 .35 1 .87 1 .37 2 .25 1 .49P < .005 P<.01 P< .0005
PCAYes No1 6 8 17.36 8.38> . 1 02.38 1 ,63P < .005
'lvlean number of prehospital procedures; GCS, Glasgow Coma Scale.
Two frndings were noted. More prehospital procedures were per-formed on the more severely injured cases; and there was a trendtoward shorter scene times for more severely injured patients withseveral categories approaching statistical significance. A compari-son of concurrent cases of nontraumatic, adult PCA ( 145 patients)revealed a significantly longer mean scene time (16.06 min) thanthe severely injured group (P <.0001). We conclude that propertraining and emphasis can lead to shorter scene times for victimsof trauma in a metropolitan EMS system. In addition, the mostseverely injured victims may spend less time at the scene despitethe fact that more procedures are performed on these patients,
*74 Ellect of Alcohol Consumption on the Outcome ofMotorcycle Accident VictimsJ Wil l iams, F Harchelroad, D Jehle/Al legheny General Hospital,Department of Emergency Medicine, Pit tsburgh, Pennsylvania
The effect of acute alcohol consumDtion on the outcome of mo-torcycle accident victims admitted to ;ur trauma center was retro-spectively reviewed from 1983 through 1987. Alcohol consump-tion was present in 65% of 182 patients who formed our studygroup; 68% of these had blood alcohol levels (BALsf above 100 mg/dL. There was no significant difference in age between thosevictims of alcohol-related and nonalcohol-related accidents. Al-though the mean length of hospitalization did not differ significantly between the two groups (15.9 versus 18.3 days, P + .054), themean Injury Severity Score was significantly higher in those pa.tients who had consumed alcohol (20.9 versus 17.6, P =.025). Theseverity of head injury did not significantly differ between the twogroups, but those victims with BAL above 0 had a greater incidenceof head injury than those with BAL of 0 (69.5% versus 495%, P =.49), and there was no significant difference in mortality betweenthose victims with BAL above 0 and those with BAL of 0 (6.8%versus 10.37o, P = .28}. Those patients with BAL above 0 hadsignificantly fewer extremity, pelvic, and rib fractures than thosewith BAL of O 163.9% versus 73.6%, P = .O49). We conclude thatthere rs no difference in mortality between the two groups and thatthe higher Injury Severity Scores in ethanol-related victims may beexplained by the greater incidence of head injury in that group.
-75 Comparison of Complication and Mortality RateBetween Direct Trauma Admissions and TransferTrauma Admissions to a Rural Trauma CenterDA Albright, M Indeck/Geisinger Medical Center, Danville,Pennsylvania
A retrospective review of 1,701 consecutive trauma patients ad-mitted from October 1986 through |uly 1988 was done to deter-mine if a difference existed in morbidity and mortality betweenthose patients admitted directly from the scene versus thosetransferred to a rural trauma center. We excluded 331 cases that
32

were admit ted to thc or thopcdics dcpartment due to minor in jur iesfrom falls and stab wounds, that is, sirnple fractures and laceratedte.ndons. Twenty-s ix cases were cxcluded due to incompletc charts.This left (r03 direct trauma admissions and 240 transfeiadmissionsftom nontrauma centers. The patients wcre matched by age anclin jury Sevcr i ty Score ( ISS). Al l pat ients ' charts wcre revicwecl forrenal , .pulmonary, hepat ic, sept ia, cardiovascular , and hematologiccompl icat ions. Comp[cat ion rates for agc and ISS as indepcndentvarrablcs wcrc evaluated for both groups {p = 0) . Dircct admissionshad an overal l compl icatron rate o l 27.53"1, ( 1 (16 of 603) and t ransferadmissrons had an overal l compl icat ion ratc o l29.73ok lZ2O of 7 a} l .There was no stat is t ical d i f fcrencc bctween thc ace and ISS matchcdgroups {P = .35). When age and ISS matchcd, chrect adrnissronspcci{ ic compl icat ion ratc was compared wi th t ransfcr acln iss ionspeci{ ic comphcat ion rates, only , rne was srar is t rcal ly s igni f icar-r t ;pulmonary (P = .03551, renal (P = .20091, sopt ic (1) = . lar t6 j ; othcr (P= . ,5619), hcpat ic lP = .5746), cardiovascular lp = .68971, and hcma-tologic (1 i = .9308). Direct admissions had a (r .4% n-ror ta l i rv ratc. andtransfcr pat icnts had a 6.1 1 % mortal i ty ratc {1) = .9) . eoih agc andISS are independcnt factors influcncing cor-nplication ratc ir.r ruralt raurna pat ients. Wc wcre unablc to show a di f fcrcncc i r - r ovcral lcompl icat ion or rnorta l i ty ratcs in 1,344 pat tcnts bctwccn di rcctt rauma admissions and t ransfcr t raLul la ld i r issrrrns wlrcn uratchcdby agc ar-rd ISS. Thcrc was, howcvcr, a significant cliffcrcncc in tl-rcpulmonary compl icat ion ratc betwccn thc two groups.
'76 Effect of the 65 mph Speed Limit Changes onMortality and Trauma Severity in Motor VehicleAccidentsDP Milzman, R LeFleche, J Vargas/Department of EmergencyMedicine, Eastern Virginia Graduate School of Medicine, Norfolk,Virginia. F i f tccn ycars of succcssful rcduct iorrs i r - r h ighway fata l i t ie s nraybc changing s incc thc controvcrs ia l Surfacc TransDortatron ant lUr-r i forrn Rclocat ion Assistancc Act of Apr i l lg t iZ |SRURAA) r l -lowccl st r r tcs to rzr isc thc spccd l imi t L ip to ( r5 mph Ort mralintcrstatos. In a rct rospcct ivc study, wc asscssccl t l rc i r rpact of th islcgis lat ion on thc inc idcncc of r - r - rotor vchic lc fata l i t i is ant l rnycornpounding factors that may havc prchospi ta l and/() r e lnurgeneydcpartmcnt t rcatmcnt impl icat ions. Al l fata l i t ics f ronr Jt i ly t i rScptcrnbcr l9 l l l l , on thc 9t3% of Virg in ia 's 253 mi lcs of iuralintcrstatc h ighways wi th thc new (r5 rnph l imi t wcrc cor lparcr lwi th thc samc pcr iod in l9 l .J7 wi th 55 mph spcct l l i r .n i ts . Motorvchic lc fata l i t ics incrc:rsct l 23. .5 '2, on ru i i r l rnterstatcs in lg l l lJ .Fatal i t ics rncrcascd only 4.5 % or-r a l l othcr Virg in ia roacls, rncl r - rd i r rga 14.O%, incrcasc on urban intcrstatcs thzr t rnaint : l inccl thc .55 ntnhspccd l imi t . I t was not possib lc to conlparc in i t ia l t raurna re, ,n i rgof t_hc{atal i t ics by stat is t ical mcthocls bcc:rusc many of thc rccorc l ilackccl standardized assessrnent cr i tcr ia. Crash scvcrr tv. howcvcr.was subjcct ivc ly incrcascd ar-rc l rcf lcctccl by a 135,2, increi rsr infatalitics_among thosc wcaring seat belts in l9iil.t cor-nparccl witl-rI 9U 7. Calculated valucs show a 3 lii7n incrcasc in tl-rc in-rp:ict forcc fora 3,000-1b vchic lc t ravcl ing 65 mph ovcr onc going 5! mph. Thcscdata suggcst that therc is an incrcascd fat i r l i ty-ratc z issociatccld i rect ly wi th spced l i rn i t incrcasc to ( r5 utph. Al thougl-r a longcrstudy pcr iod is needcd to cstabl ish a largcr databasc, thcsc prc l imi-nary results reflcct on possiblc changcs needcd ir-r rural cmcrgcncymedical serv ices to dcal wi th an incrcascd scvcr i ty of rnotr r r vrh ic lcaccidcnts. The necd to recvaluatc the rncreasc in spret l l imi t shouldalso bc undertaken i f futurc rcports cont inuc to show incrcascdfatal i ty ratcs.
77 Control l ing for Severity of Injuries in EmergencyMedicine Research: ISS Versus TRISSJG Murphy, CG Cayten, WM Stahl/lnstitute for Trauma &Emergency Care, New York Medical College, Valhal la, Our Lady ofMercy Medical Center, Lincoln Medical & Mental Health Center.Bronx, New York
Thc Injury Severity Scorc (ISS) and age can be used retrospec,tively to control for trauma severity. Howcvc;, the TRISS mcthodrequires in addition that thc Revised Trauma Scorc (RTS), usingvalues of blood pressure/ Glasgow Coma Scalc, and rcspiratory rate,be taken in the emergency department. Rclat ionships-betwccn ISSand age, and TRISS with survival and hospital length of stay {LOS)tor survivors were comparcd by cause of in jury: penctrating (pNTR),motor vehrclc accident (MVA), low fal l {LI), or othcr blunt {OB).Data were col lectcd over six months ior 1,367 consecl l t ivc adultpatients who died or stayed in four traurna and four nontralllnacentcrs for 48 hours or morc.
Mean Dearhs LT#:' to,t
. "noCause N Age (%l TRTSS' Agef TRTSS- Age,.PNTR 268 29.8 30 (11.2) 0.7811 0.28f i 0.06n o 21i lMVA 389 39.5 23 (5.9) 0.54f i 0.21n 0.08n 0.1811LF 450 75.6 28 (6.2) 0.00 0.03n 0 0311 0.1211oB 260 40.3 13 (5.0) 0.56f t 0.18n 0.16i l 0.30rr'Correlation (12) between TRISS and survival/LOS.rRegression (r2) between ISS and age, and survival/LOS.t tP r < 0 .01 .For survtval , thc cxplanatory powe r of TRISS was twicc that of ISSancl agc in a l l catcgor ies; nci ther adcquatc ly expla incd surv ivalamong thosc wi t l - r LF. ISS and agc wcrc bct ter prcdictors of LOSamong surv ivors. l {c lat ionslr ips var ied by causc of rn jury. Rc-scarchcrs should cor-rs idcr thc ISS whcn LOS is studied but TRISS
which rcclu i rcs RTS data col lcct ion i r - r thc ED - to contro l forscvcr i ty rn stucl ics of surv ival .
78 Evolut ion of Trauma Care, A County Exper ienceGA Gomez, K Vernberg, DJ Kreis, PM Byers, J Yaf fa, K Buechter,J Davis, L Mar l in, J Eckes, E Fine, R ZeppalDepartment o l Surgery,Univers i ty of Miami School of Medic ine
A county r ru l t iccntcr t ra l l l r : r systc l -n (MTS) including oncLcvcl I and s ix Lcvcl I I t raurna ccnters was cstabl ishcd in l9 l . t5.Af tcr l ( r months, f ivc Levcl I I ccntcrs droppcd out lerv iug;r rwu-ccnter t raLlnta systcn-r (TTS); prcscnt ly thc Lcvcl I t raunta ccntur rsthc only vcr i f icc l ce ntcr in thc county (OTS). Approximatc ly .35,2,of a l l r la jor t rauma pat ic l l ts wcrc t r : lnsportccl to thc Lcvcl I ccntcrt l r . r r rng th_c MTS phasc, 70'2, dur ing TTS phasc, and applrx in-ratc ly90'2, in the OTS phasc. Tl ' r rs prc l i r r inary str - rc ly cvaluatcd patrcr-r toLl tcortc as mcasurcd by r- ronCNS prcve ntablc c lcaths c l r . r r ing four-nronth pcr iocls f ronr MTS ( l9t t5 to l g l i ( r ) and TTS (19f i ( r to 1987) andto contp: t re thc rcsul ts wi th a s iutr lar stucly conductcd in I9 l t2 wi thno t raLluta systcnt (NTS). A tota l of l3. l nonCNS dcaths wcrcrcvicwcr l , ( r , l f ront thc f i rs t phasc {MTS) ar . rd Z0 f ror l thc scconr lphasc {TTS) l i r th gnrr-rps wcrc corrparablc wi th rcspcct to;rgc, scx,tnechunisr . r . r of in jury, ancl In jury Scvcr i ty Scorcs. Autopsirs we reyrcrkrrnrct l on al l pat icnts. Using thc proccss of gnup revlcw, s lxdcaths (9.5 '2,) werc j t rdgccl to bc prcventable dr . r r ing ihc MTS andf i ve { 7 . I ' 2 , ) c l u r i ng t hc TTS . P rchosp i t a l dchy o r n i i s r , , " r ' " gcn rcn tr tccour-r tcc l for thrcc of thc I I prcvcntablc dcaths, rn ist l iagnosis,t l - r rcc; hospi t i r l misr lanagcmcnt, two, dclay or surgcry/ two, and tnonc thc_indicatcr l surgical pnlcct l l r rc was not pcr for t lcd. Contpar i -son of the data rcvcals:
NonCNS Deaths
4.1982 \12 months) (NTS) 246B. 1985-86 (4 months) (MTS) 63C. 1986-87 (4 months) (TTS) 70
n52
v.2 1 . 1
6 9 .55 7 . 1
This str . rc ly sLUlgcsts a s igrr i f icant i t . r - rprovcrre nt in carc of majort raunta v ict ints wi th a t raLlnta systc l r (B ancl C) r rs contparccl wi thno t r a ru l a sys t c r r (A l { 1 , < .0051 . A l t hough no t s t : t t i s t i ca l l y s i gn i f i ,cant , i r krwcr pcrccntagc of prcvcntablc c lcat l - rs was obscrvcd di r r insTTS (7 . l ' 2 , ) as comparcd w r th MTS (9 .5 ,2 , ) .
79 The Failure of Trauma Systems in Southern Californiato Affect Death Rates From Motor Vehicle AccidentsJ Morales, D Rasumoff, A lscovich/Los Angeles County-Universityof Southern California Medical Center, Los Anqeles; Si FrancisHospi ta l , Santa Barbara. Cal i fornia
On thc prcmisc that carc of majur t raum:l v ic t ims would bci r .nprovcd by t ransport ing thcm to specia l izccl ccntcrs staf fcd bysurgcons,_C)rangc County in 19i i0 and Los Angcles County in 19t t3inst i tutcd t rauma systcms. Analysis of motor vchic lc n-ror ta l i tystat is t ics ovcr thc past ten yczrrs showed thc fo l lowing: thc dccl incin motor vchic lc accrdcnt {MVA) morta l i ty in Orar-rgc Countyfo l lowirrg inst i tut ion of a t rauma systcn thcre was, ' in fact , adupl icat ion of a statcwi t lc t rcnd occurr ing at thc samc t imc; t rcndsin rnotor vchic le morta l i ty pcr 100,000 populat ion rn the t raumasystc ln count ics as comparcd wi th thc rest Of Cal i fornia are s imi lar ;n ' rotor vchic le morta l r ty per I00,000 populat ion has worsencd inLos Angclcs County s incc the inst i tut io l r of i ts t raur la systeln in1983, as i t has in Orange County and statcwidc dur ing ihc samcpcr iod; and thc l ikel ihood of an MVA being fata l is appioximatelythe same in 1987 as i t was in lgZu both in the count ic i wi th t rn. , - "systcrns and in thc rest of the statc. Wc conclude that thc establ ish_ment of organized traurna systems with trauma centcrs staffed bvsllrgcons has had no significant effect on mortality fro- rnotc,,vehic le accidents in thc count ics in Southcrn Cal i fornia that have
Preventable Oeaths
33

adopted such systems. Basic studies, which so rar have not beendone/ are needed to define the factors that influence t.ru_,T^otilily and to evaluate their relative importance.p.O__etvJ!.rjeH Triage Based on riereOtiiegorization ofnospttat Emergency Department and Acute In_patientBed AvailabitityRF Lavery, BJ Tortella, CC Griff in/University of Medicine and!:ll:lrt,:l Ngw Jers^9y: UniversityHospitai New Jersey MedicalDcnoo.t, New Jersey State Trauma Center. Newark
Urban emergency departments have borne thc brunt of an in-crcascd demand for cmcrgcncy medical carc prompted hy the in_creasing patient load, cl,osure of hospital beds, and p.*p..11*payment system short fa l ls wi th indigent , ,pat ient
au_pi"g ; fnl9[33, our state-supported,.tertiary .ri., .,rbnr-, i.r.}rl"l'flolpi,niwas recciv ing a. d isproport ionatc amount ls7.B% [ lB,0i6t t "Ti i i "cmcrgcncy medica_l systcrn (EMS) paticnt rransports l3I,l92). It.1- :
l l l ! . ,1 nat ionaJly that othcr hoip i ta ls hat l a i tcrnpicd ro t lcal
w l r n r n l s cns l s by l im i t t ng sc r v i ccs , t u rn i ng away cc r t a i n t ypcs o fpa t r cn r s , o r s imp l y c l os i ng t hc i r EDs . Thc EMS sys rem cons r t l c rudrncse resnonscs L rnacccn tab l c and i ns t cad cs tab l i shcd a D i vc r t /Bypass/Rotat ion
_systcm to morc appropr iatc ly a l r" i f , "* ' i i4 tpat icnts.among thc s ix hospi ta ls in ihe scrv icc area based on theavai labi l i ty of ED and acute in_pat ient convcnt ional ""a ,p. . i " f tybcds.. D.ivert signified that a hospital hJ;;;;;;; rn-patient bedsavailablc in certain categories, .*, -.ai.rffruigicai/pediatricsBypass s igni f icd that an ED had no avai lablc U"ar, - i igrratcrs of thcacutc ln-pat ient status. A Rotat ion is inst i tutcd when al l t orpi tn i ,
1l".l ln,D]_y,"lr.,,rr Bypass and.mcans thar EMS rranporrs rtt pri i"ni,ro alt nosnltals, rcgardlcss 0f their Divcrt/Bypass stat lrs, baicd on aprcsct rotat ion l ist. Divcrt status alk;wcd a'hospital to continuc t irrcccive paticnts for which i t h.ad heds,. cg, mcdical/surgi." i , *fr i i"av.iding paticnts who rcquircd ,yp., ui rr.a, it ri *ir" dii ;;, ici;.Thc Bypass status recoinir",l ihc fr.t tf,ri-rii, havc finitc re_sourccs that can bc temporari ly saturatcd, ."grid1.., r i f the acutcin-housc bcd status. This systcm rcsultcj iniJniversity Hospitalrccciving rrnl y 2 7,k, 1110,7.12lt r f EMS paticn ts in I 9Ut{ {.19,750). Usinr.:radr r ) c ( )nsu l ta t ron w i th thc mcd ica l co tnmand phys ic ian whcrq lappropriatc, transports can thus be directed to h<xpitals that havcrcsourccs avai lablc to bcst carc for thc spccif ic n".a, uf t f ," prt i . 'nt.
Urban EMS systcms shoulcl considc, i" l t i iui ing,*f"r , t i* iJ lr t"_gorization systcm to cnsurc optimal carc of t t . eUS paticnt.
81 Factors Influencing the Operational Safety ofAeromedical HelicopternA
!y, I,tt! Ounn, G Tagney,.tJ BtumeniUniversity of Chicago,
I hc saicty of acromcdical transport has bccn the sub-ject ofablrndant rccent d iscussion and ncws coverage by the lny 'p icr . .
l1:utgur invcst igators at tcrnpt ing to understand th i , ph.nn_.nun
navc dcvcropcd their knowledge basc f rom studies of icc idents andcxpcrt conse nsus. Wc are th_e f i rs t to usc epidernio logic methods to: ,Y*y, f : : l , . l lperat ional safcty of aeromet l ical i r rn.po. . Wc stud_rcd zo5/.l.JU. ilrghts.rcported by programs listed in thc IgBg Direc_tory ol A1r Medical Services. The overall ratc of accidents (defincdas pcrsonal injury or ma jor property_danlage) and incidents irigriii_cant property damagcJ wcre 34 accidents per million ttiglr,, ,;d -lnc loents per mr l l ron f l iehts. Less act ive hel icopterprograms ( f ly ing
ly i t :hr l , i jo f l ig ,hts per yearJ
.were more l ikely to exper iencemrsnaps: luU accrdcnts per mi l l ion; IZ6 incidents per mi l l ioncompared with busier helicopter programs, 22 accidents p* _ii_lion {? < .005), 65 incidents pe, mittio"" 1F ='.Oif ). ,i-tr".,a was also
: : j :d- l " i h, . l icopters, f lown by thc s ix largest iMS h. l i . ; ; i ; ;
venoo rs t o have a r e l a t r vc l y l ow acc iden t r a te , 17 pe r m i l l i on ,
::Tlli.^d 11,h..:lrli"* small.vendors, s3 pel rnilion, ,h;;;ilrn rs was no t s ta t rs_ t rca l l y s ign i f i canr a t the a lpha leve l o f .d5 .:: l lC1l, l l :
cumptctety capable of f l ights under instrument f l ightsrutcs {al l heticopte-rs and al l p, i lots legal ly_ IFR capable and , progirrnl: l r- . I t . l l i , , ing
IFR f l isht lhad no arcrdents durins r z,SSe f l isht i .bccause or the re ta t i ve ly smal l number o l IFR_capab le I l igh tsJh is:llrl.l.t,
improvedsa{ety margin is not sratistically significant atrnc alpna ot .U5 tevel. programs in which the pilots were iFR currentDur. sillr rrmrted by 1aw or practice to VFR flight had the sameaccrdent and tncidenr rates as programs that did not require IFRcurrency training of their pilots.
82 Effectiveness of Cervical Spine Stabilization DevicesMeasured by AccelerometryEE Sabelman, AP Sumchai, JM-lVartino/Rehabilitation, Research &Development Center, palo Alto Veterans nOministrition, palo Alto,uailTornta
Accelerometry is the measurement of acceleration and vibrationin th.e en.vironment and/or the human body,s responre to i t . f neappilcatton ot accelerometry to the measurement of cervical spinedisplacement is described. There exist -irir,-"r. ,..elerometersthat measure accelerations in three ,*.. "o-ro"ty used in bailis_tics.testing, aeronautics research, motor vehicle .oitlrio.r, ,na gritilp:l:
The .degree of stabilization ot " ,"Ui..tb spine can becarculated- rry lntegrarion of the relative three-dimensional accel_erations of the head and thorax. Accelerometry was apphed to theevaluation of several new stabilization devices iirctuaing the fACndevicc, the Milier backboard, the oi"i. Ul.f.U"r.ilrria , .r.lon7epoxy composite backboard. In addition, two rigid i..ur.rl "oli"ir,thc Philadelphra and Stifneck, were evaluated.-fr.lJrrr"-..,,. *.r.made using miniaturc (0.5 inch cube), 5G r.. . l"r l-"t . .s mountedon a nead bancl and strapped to the chest. The difference betweenrnc accelerauons detectcd by these sensors is proport ional to theratc of change of displacement across the sub;icil-neck. Sensorsy:lc_c9ll9ctcd_by cablcs,to an amplificr package t."ai"g in; rnIBM PC/AT,with analog/digirar converter ind N6tebook software.:l:t^",:t^qlt !f
tle tlne were synchronized with the computerpror ot accelcratron in thrce axes to identify events in the recoidingsequence. Mcasurements were begun with the subject supine anjl:.:1 ti l::k in neutral position."The art,l"."rJJi ^"aii^tyuiwerc acceleratrons gcnerated during device instaliation, 1og rollmaneuvers, and active and passive neck movement. Acceieraiionswcre intcgrated for velocity and displacement. pattern matchint oiaccclcrat ions gcneratcd_ by thc insial lat ion ,na ,ppj i .r . ion ot thevanous dcvlces rdcnti f ied comlnon high_risk events includingclosure o{ fastcncrs during installationjahuft "o-rrrr., of back-brrard cdgcs with f loor,_ and sl ipping "t ' , t L i , l f r i"*. torro,h.n: l l -11:
, .ru.: not becn adequately t ightcned. The basic premise onwnlch accclcrornetry is applied as a research tool is that the humannead and thorax are coupled by the neck. The accelerometric evalu_atlon ot ccrvical immobilization devices has identified eventscapablc of inducing potentially injurious ..rui."1 .pin. motion.
83 Transient Neurologic Deficits Without CervicalspineFracture or Distocatioin Fot towin g ai, ni ii"r r"M Blanda, CM Dunham, pB Fontanaroia, H Baython, J Blanda/Maryland Institute for Emergency Medicai Servi6es bystems,Baltimore; Department of Emergency lVeAicine,-Norttreastern OhioUniversities. Coltege of Medicind, Akion City Hospitai, nXron
Ccrvical spine injury is a prirnary cori.rn in the evaluation ofpaticnts sustaining blunt trauma. White a substantial ,rumber oipatients will have cervical spine fracture or dislocation, either withor without accompanyingrreurologic deficit;, tti"r. i. "'ruUgroup Lipatients without cervical fracture or dislocation who ilanliesitransient neurologic signs and symptoms referabie to the cervicalsprnal cord. l he purpose of this study was to identify this subsetofpatients with transient cervical neuropathy {"tto*i"! li"ritir"..,1?,:l:.r.:l:'i:e t}e presenting ctinical f.r;;;.r;;"o anatyze theraorog,rapnrc trnclrngs, and to evaluate the association with under.lyrng cervlcal sprne abnormalities. The medical records of 7g5patients with blunt cervical spine trauma treated over a three_yeaiperiod were retro.spectively_reviewed. f*."ty prtia"ts with tran-sient neuroiogic de{icits of the cervical spinal ioid without fractureor dislocation were identified. Fi{ty peicent hrj oth., associatedi:t-'.yii::,
but no patient had maior organ involrrement. Fourpatientsnad a htstory of previous spinc in jur ies. Symptoms included weak_ness 170%1, paresthesias l t ingl ing) (507"), numbness (40%), and9::1..r::d
feeling (I5%). Cervtdipine t.jira"ir*, *"s presenr rn/u70. Neurologrc examination revealed motor weakniss in allpatients: 40%, ypper extremity onlyi 35y",all four extremities; and2O%o, unilateral. Fifty perceni had absent reflexes-and 60%'hadscnsory deficirs in the involved extremit ies. Bladder function, analsph-incter tone, and perianal sensation *.r. "oilff..t.a i,i ,"yfll-i:", {n3tvs1s of^radio.logic studies revealea ""a"rfyi"f .eiuicitaonormatrtres rn 6OTo that included degenerative joinf disease,3llf1:::l:11.,
Lgamentous instability, t Er"irt.J at.'", and Klippei:.]1.^o,.l"1Tt?.
Twenty five percent of patients were initiallyrreared wtth Cardner_Wells tongs and steroids, while the remain-1ng patlents were treated with a rigid cervical collar and steroids.All,patients had cornplete resolut"ion of ,y-pio-. and deficitswrtnin r 4 days, wrth deficits in 75 % resolving in less than {ive days,No patient required surgery The data ,,rgglrt thrr euen though:jlTi:l!
neurologic deficits not associa6-d with cervical spiierracrure or drslocatron are an uncommon sequelae of blunt cervicallTlTal
their presence may indicate signi{icant underiying cervical
34
spine abnormalities, and consultatio"n with a spinai s.irgeon is

warranteo.
84 The lmpact of a Cervical Spine Radiographic protocolon Cost and Prophylactic Spinal lmmobilizdtionSGA Gabram, RJ Schwartz, LM Jacobs/Hartford Hosoital.Unrversity of Connecticut School of Medicine, Hartford
A prospect ive cohort study was conducted to determine theimpact of a protocol for the radrographic cvaluation of thc cervicalspine of b lunt- in jured pat icnts. A1l admit ted blunt t rauma uat ientswi th suspectcd in jury to the ccrv ical spinc were cntered into thcstudy. Data on_pat ients were col lectcd two months pr ior {25) andtwo months af ter protocol (68J. Thc protocol e l iminatcd rout incobl ique v icws and instr tutcd ear l ier computcd tomography (CT)scanning of thc odontoid i f open-mouth Watcr 's v iews'werc 'unob_tainable. Data elcments inc luded agc, mcchanism of in jury, In juryScver i ty Score { lSS), Glasgow Coma Scale (GCS), number,r f dnys , i fspinal col lar immobi l izat ion, d iagnoses rc lated to cerv ical spincin jur ies, radiograph-relatcd charges, and rnr t ia l physical cxamina_t ion-resul ts. The two grol rps wcrc not stat is t ical ly d i f ferent in agc,GCS, ISS, and numbcr intubatcd. Thrcc pat icnts in thc prcprotoi i r igroup had conf i rmcd (CT scan) spinal in jur ics; there wcrc nonc inthe af tcr protocol group. Thc rangc of days pat icnts wcrc immobi-hzed was one to I I (mean, 1. t37) for the pr ior group and onc to four{mean, 1.2) for thc af ter group {p = .003). For thosl pat ients whoscin i t ia l physical and radiographic examinatrons wcrc suggcst ivc ofan in jury, thc numbcr of days for cerv ical col lar imrnobi l izat iondccreascd f rom 5.2 days in the pr ior groul"r to l . t i days in thc af tcrgroup (P = .01). Intubatcd pat icnts dccrcascd f rorn 4.1 days to 1.6
lays (P = .009). Cervical spinc-rc latcd radiograph chargcs c lccrcascd
trom $8,782 {mean, $1 17) to $6,679 (mcan, $9t3) lp = .07()1. Thc uscof a prcdetermined- protocol for cvzr luat ing thc ccrv ical spinc inblunt trauma can dccrcasc thc numbcr of clays of ccrvic:rl spincirnmobilization and dccrease radiograph-rclatcd chargcs.
'85 Indicat ions For Head CT Scanning in Trauma pat ients,1p litzpatrick, SZ Trooskin, L Flancbaum/Department of Surgery,UMDNJ-Robert Wood Johnson Medical School , New Brunswick,New Jersev
Thc prccise indicat ions for hcacl computccl tomography (CT)scans rn thc cvaluat ion of t rauma pat icnts havc noi l tccn wcl ldcf ined. Mastcrs et a l dcscr ibcd an aisessrncnt systcm for c loscd-hcad injurics dividing paticnts into thrcc cat"guri", (low, rnodcr-atc, and high indcx of suspicron for intracranial injury) basccl onsymptoms. The.purposc of this rctrospcctivc study was to idcntifythosc critcria obtaincd prospcctivcly on history and physical cx,aminat ion that would most scnsi t ivc ly idcnt i fy which pat icntswould bcnefit from having a hcad CT scan. Wc rcvicwccl thc chartsof 166 pat ients f i t t ing thc cr i tcr ia of Mastcrs ct a l for inc lusion intoa.moderate indcx of suspic ion for c loscd-hcacl in jury (MIS) and whoalso had hcad CT scans. Data wcrc col lcctccl rc lat ive ro nar iuntdcrnographics {age, scx, race, mode of in j r " r ry) , prcscntat ion {vtra lsigns, Iniury Sevcrity Scorc IISS], Glasgow Corna Scalc), diagnosticworkup and resul ts. The l2 factors that p laccd pat ients in thc MISgroup (1(16 CT scans,38 posi t ivc) wcrc t iansicni loss of conscious-ness (LOC), drug or a lcohol uso, progrcssivc headachc, unrc l iablchistory.of injury, age lcss than 2, posi-traur-natic scizurc, arnncsia,multiplc !r1!ma, scrious facial injury, suspectcd basilar fracturc,possib le chi ld abuse, and possrble pcnetrat ing or dcpresscd f racturc.lhe factors s igni f icant ly associated wi th posrt ive scans on chi_square analysis were LOC, senous facial injury, suspectcd basilarfracture, and possible penctrating or dcpresscd skull fracturc. Stcp-wise regression analysis identified the lattcr threc variablcs as in_dependent predictors of injury, while LOC was depcndent on thepresence o{ one of the other three factors for statistiCal sisni{icancc.The three independent variables identified 33 of thc 31 posirivcscans in the MIS group. The other five positivc scans were analyzedfor similarities and were all {ound to shlre a total ISS of I Z or ereater(net ISS of I 3 or greater not including transient LOC in one piiient ).Of other demographic variables and vital signs collectcd on admls-s ion, only CPR was s igni f rcant ly associated wi th posi t ive CT scanslP: .0002). The data suggcsr that CT scans are indicatcd whencver
3 patient- w.ith MIS presents with a serious facial injury, possible
basilar skull fracture, possible penetrating/depressed .kr.ll f."c-ture, has had CPR, or has sustained trauma with as ISS of 13 orgreater, excluding the neurologtc component. Also, it may bepossrble to avoid scanning of patients with transient LOC andmoderate extracranial trauma {ISS 12 or less) as there were noinjuries associated with these criteria alone.
86 Concomitant Femur Fracture and Head Injury: AReliable Indicator of Visceral Torso InjuryC Pippis, D Unkle, SE Ross, KF O'Mailey/Divlsion of Trauma andEmergency Medical Services, UMDNJ-Robert Wood JohnsonMedical School at Camden, Cooper Hospi ta l /Univers i ty MedicalCenter, Camden, New Jersev
Al though major tn jury to the hcad and extrrml t ics is usua. l lvdiscovcred_dur ing in i t ia l asscssment in thc f ie ld, in jur ies to thcchcst or abdomen arc much morc di f f icul t to rccoqnizc at that t lm(] .Indicators o{ the prcsencc of s igni f icant , but rn i i ia l ly occul t , in ju_r ics to the chcst or abdomcn arc thus highly useful in thc devclop_mcnt of t r ragc systcms. To invcst igatc thc val id i ty of concomitanthcad in jury and femoral f racturc as an indicator of thc r isk ofv isceral in jury, a 3 l -month revicw of a l l pat ients adrni t ted to aLcvcl I t rauma ccntcr af tcr sr-rsta in ing hlunt in jury (1,922) wasundcrtaken. Thcrc werc 4t i l pat ients wi th s igni f icai r t thoracic orabdon'r inal in jur ics (AIS > 2) for an ovcral l inc idcncc of 25, /u. In thcsubgrcup of pat icnts who had suf fcrcd both a s igni f icant hcad in jury(AIS > 2) and a fcmur f racture (103), thc inc idencc of thoracic orabdorninal in jury was 43.7% 145 of 103). This rcrrrcsentcd a stat is_t ical ly s igni f icant incrcasur l incr t lencu {1 ' . .O0i using chi-sc luarcar-ra lysrs) whcn comparcd wi th pat icnts wi th head in lury unaccom-panicd by fcmoral f racturc (210 of 945, ZZ, l , \ , fcrnoral f ractureunaccon-rpanicd by hcad in jury (13 <i 68, 19"1,) , or thc cnt i repoptr lat ion. Thc prcscncc o{ a hcad in jury or f rmoral f racturc a loncwas not associatcd wi th an incrcascd r isk of v isccral in jury. Weconcludc that pat icnts wi th hcad rn jury in cornbinat ion wi thfcr .noral f racturc arc at s igni f icant r isk for th()r i rc ic or abdorninalin jury. This f inding should bc considcrcd for incornorat i ( )n intot r i : r g r gu i t i e J i ncs .
.87 The Value of Alkaline Phosphatase in peritonealLavageSM Megison, JA Weigelt/The University of Texas SouthwesternMedical Center at Dallas
. Thc accuracy of pcr i toncal l : rvagc for t r : lL lm:1 is l imi tcc l by i tsrc l : r t ivc lack of scnsi t iv i ty for hol low v iscus in jury. pcr i toncallavagc pcrforrncd in thc c log indicatcs that a lkal inc r rhosphatasc{AP) in lavagc f lu id is an car ly indicator of intcst inal inrr . r rv. ' l f thr :scrcsul ts wcrc conf i rmcd in human pat icnts, Ap dctcr in inat ionwou ld imp rovc l avagc scns i t i v r t y f , r i ho l l ow v i scus i n j u r i c s . Apwas t .ncasurccl i r - r r l l Inyn*. samplcs scnt for laboratury assay dur inga onc-ycar pcr iocl . Two hr"rndrcd nincty- two lav:rgcs wcrc pcr_fon.ncd; 25 wcrc posi t ivc by laburatory cr i tcr ia and (16 wcrc grois lyposi t ivc. Thcrc wcrc l3 intcst inal in jur ics; n inc wcrc grosslyposi t ivc ancl four wcrc d iagnoscd by laboratory rcsul ts. T i r rcc <i ft hcsc f ou rpa t i cn t s w i t h i n t cs t i na l i n j u r i es had c l cva t cd l avagc Ap .Al l . thrcc ( lavagcd f rurr 30 minutcs to two hours af tcr rn jury) a lsohacl c lcvatcd WBCs or b i lc in thc lavagc f lu id. Thc rcmainingintcst inal in lury was c l iagnoscd by lavagc bi lc but l - rad no c lcvat ionof AP { lavagcd l5 minutcs af tcr in jury) . Two pat icnts wi th e lcvatcdAP in othcrwisc ncgat ivc lavagcs wcrc obscrvcd for at lcast f ivcclays. Nci t l - rcr dcrnonstratcd any cvidcncc of int ra-abdominal in-jury. AP in pcr i toncal lavagc is no bct tcr than t radi t ional dctermi_nants o l intcst inal in jury. In fact , in no pat icnt was Ap hclpfu l indiagnosing a hol low v iscus in jury and i ts use would havc prornptcdtwo unn_cccssary ccl iotomics. Thcse data c io not support ihc u i . , , flavagc alkal inc phosphatasc to idcr-r t i fy hol low v is ius in lur ics.
-88 Clinical Comparison of Hesuscitation and SurvivalRates for 1980 and 1985 ACLS Protocols in Out-of-Hospital Ventricular Fibri l lation Cardiac ArrestsFC Erickson, BD Mahoney, KA Griff ith/Department of EmergencyMedicine, Hennepin County Medical Center, Minneapolis,Minnesota
The I 9U5 rcvis ion of thc Standarcls and Guidcl ines for AdvancedCardiac Li fe Support (ACLS) for ventr icular f ibr i l la t ion lVFl cardiacarrests is bascd primarily on theorctical laboratory data and previ_ous c l in ical exper iencc. Therc were no contro l led c l in ical ourcomestudies completcd pr ior to i ts adopt ion and promulgat ion. Whi leintu i t ivc ly and empir ical ly bel icved to be bet ter , t t remains c l in i_cal ly unproven. We analyzed al l consccut ivc out-of-hospi ta l VFcardiac arrests transported by the Hcnnepin Ambulance Service toHenncpin County Mcdical Ccnter during a one-year period beforeand onc year after our EMS system adopted the l9B5 ACLS revi-sions. Patients were cxcluded if their arrest was traumatic, hypoth_ermic/ toxjc/ suicide, elcctrocution, drowning, or they were underI (r ycars of age. One hundred thrrty-nine fiatients were entered into
35

this retrospective chart study, (r5 ln the first group managed
according io the l9B0 protocol and, 74 in the second managed
according to the l9B5 tcui t io. t . There werc no stat is t ical ly s igni f i -
cant dif{irences (P < .05) in age, sex, or time to initiation of ACLS
treatment betwecn the groups. The f i rs t group had a resusci tat ion
ratc of 33.8%, dischargeiate-of 18.5o1, , and discharged funct ional ly
thc samc rate of 13.8%. Thc second group had rates of 41 97",
18.9 ' / " , and 14.97n, respcct ively. Whi le therc appcars to be a t rend
tu*rtd high"t rcsuscitition rates with thc new VF protocol, thelc
arc no staiistically significant differcnces in any of the rates found'
Wc conclude that the new VF protocol is nei ther rcmarkably bct ter
nor worsc than the old protocol . Also, using beta analysrs, grven
only an [3'lo improvemcnt in resuscitation ratcs and virtually idcn-
t ical d ischarge rates, i t would requirc a massivc study to dcmo.n-
strate a stat i ; t ical ly s igni{ icant d i l fcrencc in outcomcs bctween the
two protocols.
89 Defibri l lation By Intermediate EMTs: The ll l inoisProiectKL Muelter, S Anneken/Department of Surgery' Division ofEmergency Medicine and Trauma, Emergency Medicine ClinicalReseirch Center, University of Colorado Health Sciences Center,Denver; Christ Hospital, Oaklawn, l l l inois
A study was undcrtakcn in I l l inois to ver i fy reports of succcssful
cncrgcncy mcdic inc technic ian-def ibr i l la t ion (EMT D) programs
in Iowa and Seatt le. Intcrmcdiate EMTs wcre t ra ined to idcnt i fy
vcntr icular f ibr i l la t ion (VF) and opcrate a moni tor-dcf ibr i l la tor '
Monthly tcst ing conf i rmed thc abi l i ty of a l l EMT-ls to def ibr i l la tc
a manncquin wi th in 90 scconds of d iscovcr ing VF. Six suburban
and rurai hospi ta ls wcre involved in thc study. Resusci tat ion
ol l tcomcs wcrc cornpared betwccn phasc I (bcforc EMT dcf ibr i l la-
t ion t ra in ing, ( r5) and phasc 2 (af tcr t ra in ing, 73). Pat icnts in-phascs
I and 2 wci l s i rn i lar- in agc, scx, cardiac history, causc of dcath,
c l is t r ibut ion of cascs among thc hospi ta ls, and ai rway uscd dur ing
transDort . T imcs f rom cal l to EMT arr ival on sccnc wcrc also
sirn i l i r (phasc 1, 5.9 min + 0.49; phasc 2, 5 '7 r0.39l . Inphasc2,77 " / "
of cascs had VF whcn f i rs t rnoni torod at thc sccnc, in phasc I only
28'/,, hatlVF whcn first monitorcd at thc hospital. This diffcrcncc
was cxpcctcd: in phase 2 thc avcragc t imc bctwccn on-sccnc arr ival
ancl rhythrn dctcrminat ion at thc hospi ta l was 2l .4 t 0 97 rn inutcs '
In nhaic 2 morc arrcsts wcrc wi tncsicd (6t3 '2, vs 5 i '2, , 1)= '03) and
nr<irc pat icnts rcccivcd bystandcr CPR ]3(r '2, us 2O"l ' , 1)= 04)- Dc-
spi tc t tv tT-D t ra in ing and grcatcr numbcrs o{ wi tncsscd and by-
s iandcr-assisted pat i ints in phasc 2, thcrc was no di f fcrcncc bc-
twccn thc gtu. ,pt in long-tcrm surv ivors ( thrcc of65 in-phasc I vs
two of 73 in phase 2) . Ai ihough arr ival t imc, numbcr of wi tncsscd
arrcsts, and bvstander CPR wcrc wi th in acccptcd l imi ts of an EMT-
D program, thcrc was ntl incrcasc in long-tcrm survivors Trarning
fl{fs'tu dcfibrillatc docs not guarantcc highcr ratcs of survival'
90 Transtelephonic DelibrillationJS Fetdstein, J Henry, B Simmons, L Ni towski , R O'Connor/Medical
Center of DelawareThc purposc of th is study was to asscss thc safcty and ef f icacy
of a dcvicc allowing for tianstclcphonic dcfibrillation Fiftecn
naticnts wcrc tlcfibriilatcd using thls device. The initial rhythrn
*u, . , ,urr . vcntr icular f ibr i l la t ion (VF) in tcn pat ients, f ine VF in
for.rr, and ventricular tachycardia in onc. -The transtclephonic
svstcm consists of a patient unit containing ciectrodes, a mlcropro-
."rrur, , DC defibdllator, and a microphone. The base station
consists of a control panel and ECG display' Opening the paticnt
unit and connccting it to a standard telephone iack initiates a
pr"p.ugrr--"d dia"ltng sequcnce that automatically dials and
, . t iut t t the base stat ion wherc a physic ian can communicatc,
monitor, and, if necessary, defibrillate from a remote location'
Fiftecn patients who prescnted to our cmergency department in
car,liac ,rre.t were placed on patient units that activated our base
stat ion in , , . .not . io. r t ion wi th in our ED. In a l l cases voice and
ECG transmission werc established without difficulty Twcnty
asvnchronous defibrillation shocks ranging {rom 200 to 360 J were
deiivcred transtelephonically as well. We believe that this system
i. n r"t. and ef{icaiious metLod for treating VF and has unlimited
prchospi ta l uses.
91 Dangers of Defibri l lation: lniuries to EmergencyPersonnel During Patient ResuscitationW Gibbs, M Eisenberg, S K DamoniCenter for Evaluation ofEmergency Medical Services, King Courty Health Department'fmerlency Medical Services Division; Department of Medicine,
University of Washington, Seatt leOthei than one individual case report and a number of inciden-
tal accounts, there have been no studres of the nature or risk topersons providing defibrillatory shocks. In this study, we report the
severity and nrtrrie of injuries to prehospital emergency personnelin King County, Washington. In addition, we describe the types ofinjuriei o".r.,rtit-tg to defibriliator operators voluntarily reported tothc Food and Drug Administration. In King County, prehospitalcmergcncy pcrsonnel reported eight accidental shocks One indi-viduai was admittcd tulh. hospital for three days and requiredlldocainc for premature vcntricular contractions Most injurieswere the resuft of accidentai contact with the patient rather thanequipment failurc, although the most serious case was due tocquipmcnt failure. There were l3 injuries reported to the FDA over. ihi."-rnd-one-ha1f-year pcriod. Most injuries involved a mildshock or burn. Threc patiants were admittcd to the hospital forobservation. Two caseJinvolved machine failure. The rate of iniuryfor oaramcdics was one pcr 1,700 defibrillatory shocks and for"-"rg"r-t"y medical technician-defibrillator-personnel was one per
1,000 de{i6rillatory shocks. Thesc rates probably overestimate thereal risk. Emphasii on safety and incorporatron of safcty proceduresinto resuscitition protocols can make the ratc of injury even lower'
92 Morphology of Myocardial Necroses Alter 15 or 17
Minutei of Ventricular Fibrillation Cardiac Arresl andCardiopulmonary BYPass in DogsA Badoisky, P Safar, FSterz, Y Leonov/lnternational ResuscitationResearch Oenter and Department of Anesthesiology, University 0fPittsburgh
In st-udics of normothermic ventricular fibrillation (VF) cardiacarrcst (no flow) of tcn to 20 minutes, dogs with previously healthyhcarts dcveloped multifocal myocardial necroses. Cardiac outputaftcr arrcst is transiently reduced, but recovers. After VF of 30minutcs, hcartbeat recovcrcd only transiently. In this study,-mor'phology and pathogeneses o{ the necroses were explorea r!ttt!t-ilu. airlr wcrc subiected to VF by external AC shock (50 to 100 VJ,no f low of l5 minutes {ten) or i7 - inut"s (25), reperfusion withcardiopulmonary bypass, external defibrillation with DC 200 to
400 f, intcrmittcnt positivc prcssure ventilation to 24 hours,intcnsive carc to 96 h<jurs, and perfusion fixation sacrifice' Grossly,thc hcarts showed necroses/ piimariiy involving the subepicardiallaycr of thc right ventriculai free wall, of which a mean of l0%(maximum, SfjZ)ot the surface area was necrotic/ versus only l7oof thc lcft vcntricle. There was no correlation between myocardialand brain histologic damage scores. Myocardial necroses were
most promrnent ;long the pulmonary artery-outflow tract andbcncaih the middle ofihe coionary groove of the right ventricuiarwa11. Light mrcroscopy showed necrotic.myofibers with homoge-nous hy'pcreosinophilia. The post-VF {no flow) myocardial necrosesmay 1-,c tauscd by'a cornbinaiion of electric iniury and reperfusioniniurv. CPR trauma and coronary obstruction were ruled out'
93 The Effect of Bolus Injection on Circulation TimeDuring CPRCL Eierman, A Pinchak, J Hagen, D Hancock/Departments ofEmergency Medicine and Anesthesiology, Cleveland MetropolitanGeneial Hbspital, Case Western Reserve University, Cleveland,Oh io
Sevcral previous studies have demonstrated that peripheral ve-nous iniection during CPR leads to prolonged circulation times andio* p.rt drug levelsl Current ACi-S guidelines recommend that a
bolus of fiush solution be injected following peripheral iniection of
medication; however, there is limited evidence that this technique
ir l" tr., effective. The purpose of this study was to investigate the
e{{ect of a bolus iniection-on dye circulation times during CPR'
Eight n-rongrcl dogs weighing between lB.and 28 kg were instru'
minted wiih B-in. "atheiers placed in each of the carotid arteries
and a Swan-Ganz catheter pissed into the pulmonaryartery' The
animals were cradled in a dorsal support and a modified Thumper@was positioned over the lower ventral thorax' Measurements ol
end-iidal CO., central venous, and arterial blood pressures were
made througliout the study. Cardiac arrest was- induced by 60-HzLlectrical stinulus applied to a right ventricular wire' Repeatedrniections o{ indocyanine green dye, 2.5 mg in 2 mL of diluent were
made either with (method 1) or without (method 2J a 20 mL salineilush in a random order. Eight injections were made in each dog
with half of the iniections foliowed by a sahne flush' Dye was
withdrawn from the left carotid artery by a motorized syringe
through the densitometer cell o{ a dye dilution conputer' Dye cir-
36

Group123
cuiation time was measured as the time to first appearance of thedye at the densitometer cell. There was no difference in svstolic.diastolic, or coronary perfusion. There was no difference in ETCO.following injection with or without saline flush. The dye circulalt ion t ime wi th sal ine f lush was SL7 f 20.8 seconds, whi le thecirculation time without saline flush was 86.9 + 43.6 seconds lp <.001). The peak dye concentration following injection with saiineflush was 3.8 t l. t mg/L while the peak dye ioncentratron withoutsal ine f lush was 2.8 t 0.9 mg/L (P < .001). We conclude that a 20 mLsaline flush can enhance circulation times and peak dye levelsfollowing peripheral iniection during CpR. Further work remainsto be done to establ ish the opt imal volume of f lush to be used incl in ical s i tuat ions.
*94 Effects of Arterial and Venous Volume Infusion onCoronary Perfusion Pressure During Canine CpRNT Gentile, GB Martin, J Moeggenberg, TJ Appleton, NA paradis,RM Nowak/Department of Emergency Medicine, Henry FordHospital, Detroit , Michigan
Intra-arterial {IA) infusion has been rcported to be rnore cffectivethan IV in{usion in treating cardiac arreit due ro exsangulnarlon.Computer modeling suggests that IA rnfusion, but not IV, mayimprove coronary perfusion pressure {CPP} during CpR. The pur-pose of this study was to deterrnine if IA or IV volume infuiionduring CPR could augment the effect of epinephrine on Cpp.Fifteen mongrel dogs with mean werght 26.3 t 4.4 kg were anesthe-tized and mechanically ventilated. Right atrial iRA) and aortic {Ao)catheters were placed. Additional Ao and central venous catheterswere placed for fluid infusion. Ventricular ftbrillation was inducedand Thumper@ CPR begun five minutes later (T = 5). At T = I0 alldogs received 0.045 mg/kg epinephrine IV. Group t received IVepinephrine only. Group 2 also received an IV bolus of 500 mLsaline over three minutes through the central venous cathetcr.Group 3 received the same volume IA. Resuscitation was at-tempted at T=18 with standard protocol.
adminstrat ion between the B-CPR and no B-CpR groups {p > .09).No successful resuscitations were noted in either group foilowinginitial defibrillation or following epinephrine therapy. The resultiof th is p i lot s tudy fa i led to demonstrate the ef fect iv iness of B-CpReven if started eariy after cardiac arrest. This study suggests that B-CPR may only be effective in maintaining critical perfusion to theheart and brain for a relativeiy short duration.
-96 Left Ventricular Volume and Aortic FlowRelationships During High-lmputse CPR: lmplicationsRegarding Mechanism of Blood FlowJE Manning, PCD Pelikan, JT Niemann/UCLA School of Medicine,the Departments of Emergency Medicine and Medicine,(Cardiology), Harbor-UCLA Medical Center, Torrance, Cali fornia:The Saint John's Heart Inst i tute, Santa Monica, Cali fornia
The purpose of this study was to assess thc mechanism for bloodflow during manual conventional CPR iCCpR) {chest compressionrate, 80 to 100/min) and high-impuse CPR (HICPR) (comprcssionrate, I20 to 150/min). Mil lar catheters were posit ioned in thc as-cending aorta {Ao) and left ventr iclc {LV) of cight minipigs. Ao andLV pressurcs, LV dp/dt, Ao f low-velocity (AoFl, and changes in LVvolume {LW) (conductance methodl were rccorded after cardiacarrcst and during HICPR and CCPR performed in a randorn man-ner. CCPR and HICPR were performcd twicc in each animal.HICPR signif icantly increased {P < .0001)peak Ao prcssure (67 + 6mm Hg vs 46 ! 41, LV pressure ( 70 t 3 vs 47 t 5i1, and LV dp I dt l7c)t)+ 1 26 mm Hg/sec vs 255 t 471. A decreasc in LW occurred Uu 1 22ms after the onset of AoF during CCPR, at 6I + 7 rns during HICpRlP = NS), and at -3 * 5 ms prearrest. During CCPR, 24 + 5% of totalAoF occurred before onset of LW decrease,34 +.5% of total AoFoccurred bcforc a volume change durrng HICPR (p = NS) and 4 t I %prcarrest. In seven of 1(r HICPR studies, LW increased (r + 3 mLduring early CPR systole and AoF. In 30 of 32 studies, LWdecrcascd during late systolc and in 16 (ninc CCpR, scven HICPR),thc lowe st LVV was notcd to occur t i9 + I 7 ms af tcr f orward f krw hadccased. We conclude that CCPR and HICPR share common mecha-nisms for forward f low; the lack of a consistent relat ionshinbctwccn LV volumc changes and f low suggests that changcs in LVvolume (dimension) during CPR arc not due to vcntr icular com-pression; and f low prcceding LV volume changcs supports intratho-racic pressurc fluctuations as a driving forcc for antegrade bloodi low.
97 Failure of Fructose-1 ,6-Diphosphate to PromoteIncreased Survival or Neurological Protection FollowingResuscitation From Experimental Cardiac ArrestRE Bosenthal, SM Sharpe, GH Marshall Jr, JP Smith, RF Shesser/Department of Emergency Medicine, The George WashingtonUniversity Medical Center, Washington, DC
Cerebral viability is strictly dependent on the production anduse of ATP. Under aerobic condirtions, more than B0% of ATpformation is due to oxidative phosphorylat ion. Oxidativephosphoryiation ceases rapidly during ischemia and may remarninhibited following restoration of normal blood flow. Durins thcseperiods the neuron must rely on glycolysis for production oJ Rfp.Although initially increased during ischemia, glycolysis soon slowsas a result of acidosis-induced inhibition of intermediatc enzymes.Exogenously adminrstered fructose- 1,6-diphosphate (FDp) has bccnshown to increase glycolytic production of ATp through stimula-tion of both phosphofructokinase as well as pyruvate kinase.Following experimental hypoxia, FDP has been shown to prolongtime to respiratory arrest as well as to increase immediate salvagefrom hypoxic cardiac arrest. This study was designed to determineth_e utility of FDP for promoting survival and neurologrc recoveryfollowing experimental cardiac arrest and resuscitation. Male Wistarrats {weighing 380 to 445 g), anesthetized with an Ip injection ofketamine (36 mgf and xylazine {0.5 mg), were subjected to con-trolled ventilation with room air followine midline tracheotomv.Intracardiac inject ion of 0.4 mL cold I ozo XCI fol lowed by m"nurlthoracic compression was used to induce six minutes of cardiacarrest. ROSC was accomplished using IACCPR (70 per minute)synchronous with ventilation with room air. Fifty-four survivorsalternately received either FDP i200 mg/kg Ip) or similar volume ofsaline immediately on resuscitation. Animal survival was recordeddaily with neurologic deficit scores {NDS)being measured in thoseanimals surviving ten days. There was no difference in survivalbetween groups with l4 of 27 152.k) in each group surviving the fullten days. NDS of survivors for FDP (8.61 14.5) or control {5.8 t 12.2)rats were also not significantly different {two sample t test, p = .571.
CPR (Ao-HA diastolic gradient, mm Hg)
T=10 Max R i se T=13 T=15 T=1812.4!4.2 33.014.4 26.415.0 25.2r5.1 20.215.520.4!4.3 43.2!8.2 30.213.8 31.214,9 29.6!6.711 .8t2.4 34.0!4.2 23.413.8 18.013.6 14.0x3.2
cantly affect outcome, includcantly aflect outcome, including ischemia time prior to B-CPR,drrration of B-CPR, and paramedic response time. The p.rrpose olresponse time. The purpose of
half minutes after epinephrine administration. Ap {mm Hg), MBF
this study was to determine the effectiv-eness of B-CpR inan animalmodel of cardiac arrest and resuscitation. Ten swine were instru-mented for aortic pressure {AP}, myocardial (MBF), and cerebralblood flow iCBF) measurements using tracer microspheres. Ven-tricular fibrillation (VFlwas then induced. After two minutes of VFthe animals were assigned to receive either B-CPR for eight min-utes ifive) or remain in VF without CPR for an additional eishtminutes (five). Following this, both groups received 100% oxygena-tion and three defibrillations initially. If defibrillation was unsuc-cessful, CPR was continued and epinephrine 0.02 mg/kg wasadministered. Defibrillation was attempted again threJand one
The maximum rise in CPP was at T = I 1.6 I 1.3. Althoueh Cppincreased significantly in all groups (P < .005), there was nodifference between groups in the extent of increase (p > .051. Thisstudy failed to demonstrate an advantase to the addition of IA or IVfluid loading to therapeutic epinephrine dosing in dogs.
95 The Effectiveness of Bystander CPR in an AnimalModelJ Hoekstra, K Rinnert, P Van Ligten, R Neumar, HA Werman, CGBrown/Division of Emergency Medicine, The Ohio State University,Columbus
Several clinical studies have attempted to discern the effective-ness of bystander CPR {B-CPR}. The results of these studies areconflicting but suggest that B-CPR is effective if initiated early andif advanced cardiac life support {ACLS) is instituted within l2minutes after the onset of cardiac arrest. One problem in comparingthese studies is the inability to control for variables that slsnifi-
onds and five and one half minutes after beginning B-CPR, and one
natr mlnutes atter eplnephrrne ad.mlnrstration. AP {mm Hg), MBJ{ml/min/100 g) and CBF {ml/min/100 g) were measured 30 seconds and five and one half minutes after beginning B-CPR, and onrminute a{ter epinephrine administration. There were no sisnifi-cant di{ferences in diastolic AP, MBF, and CBF durine the initialand later stage of B-CPR {P > .14}. There was no dif ference in thechange in diastolic AP, MBF, and CBF following epinephrine
37
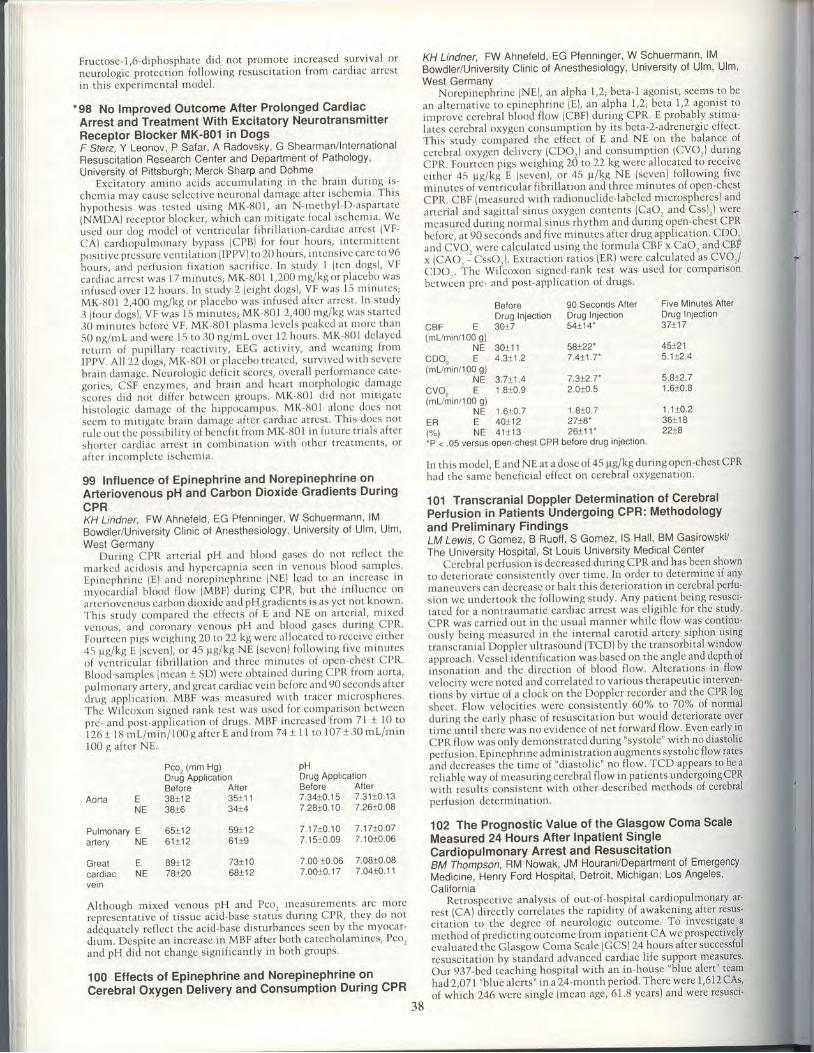
Fructose-1,6-dlphosphate did not promote increased survival or
neurologic proiection following resuscitation from cardiac arrest
in th is exper imental mode1.
'98 No lmproved Outcome After Prolonged CardiacArrest and Treatment With Excitatory NeurotransmitterReceptor Blocker MK-801 in DogsF Steiz, Y Leonov, P Safar, A Radovsky, G Shearman/lnternationalResuscitation Research Center and Department of Pathology,University of Pittsburgh; Merck Sharp and Dohme
Exci tatory amino acids accumulat ing in the brain dur ing- is-
chemia may cause sclect ive neuronal damage af ter- ischemia' This
hypothesis was tcsted using MK-801, an N-methyl-D-aspartate
{NMDA) receptor b locker, which can mit igatc focal ischcmia We
used our dog-model of vcntr icular f ibr i l la t ion-cardiac arrest (VF-
CAI cardiopulmonary bypass (CPB) for four hours, intcrmittcntposi t ive preisure vent i lat ion ( IPPV) to 20 hours, intensivc carc to 96
i-to.,.t, ,.td perfusion fixation sacrificc. In study I (ten dogs), VF
cardiac arrc i t was I 7 minutes; MK-f{O1 I ,200 mg/kg, or p lactbo was
infused over 12 hours. In study 2 {e ight dogs), VF was 15 minutcs;
MK-801 2,400 mg/kg or p lacebo was infuscd af tcr arrest ln study
3 ( four dogs), VF was- 15 minutcs; MK U01 2,400 mg/kg was star tcd
30 minutes beforc VF. MK-UO1 plasma levcls pcaked at morc than
50 ng/rr l ancl wcre 15 to 30 ng/ml over l2 hours MK 801 delaycd
," t . , in nf pupi l lary rcact iv i ty , EEG act iv i ty , and wcanrng f rom
IPPV. A1l ZZ , iugt , MK-U01 or p laccbo t rcated, surv ived wi th scvcre
brain damagc. Ncurologic deficit scores, overall performance catc-
gor ies, CSF cnzymcs, and brain and heart morphologic damagc
scorcs did not d i f fer bctwccn groups. MK-t l0 l d id not mi t igate
histo logic darnage of the hippocampus. MK-t iO1 alonc docs not
sccm t ; mi t igate brain damage af ter cardiac arrcst . This does not
ru lc out the pi rss ib i l i ty of benef i t f rom MK-801 in futurc t r ia ls af ter
shortcr cardiac arrcst in combinat ion wi th other t rcatmcnts/ or
af tcr incornplete ischemia.
99 Influence of Epinephrine and Norepinephrine onArteriovenous pH and Carbon Dioxide Gradients DuringCPRKH Lindner, FW Ahneleld, EG Pfenninger, W Schuermann, lMBowdler/University Clinic of Anesthesiology, University of Ulm, Ulm'West Germany
During CPR artcrial pH and blood gascs do not rcflcct thcrnarked ai idosis and hyp-rcapnia sccn in vcnous blood samplcs '
Epincphr inc (EJ and noicpincphr inc (NE) lc 'ad to an incrcase in
myocar<t ia l b iood f low (Mnr) dur ing CPR, but the inf luence on
artcriovcnous carbon dioxide and pH gradients is as yct not known'
This study compared the cf fects-of E and NE on ar ter ia l , mixed
venous, ancl coronary venous pH and blood ga-scs during CPR'
Folrr tccn pigs wcighing 20 to22 kg wcrc al locatcd to reccivc c i ther
45 pg/kg L (sevcn), or 45 pg/ l<g NE (sevcn) fo l lowing f ive minutes
of vent i icular f ibr i l la t ion and three tn inutcs of open-chest CPR'
Blood samples (mean + SD) were obtained dur ingCPR from aorta,
pulmonary artcry, and great cardiac vein be{orc and 90 scconds after
i rug appl icat ion. MBF was mcasured wi th t racer tn icro-sphercs '
rhc'wlicoxon signed rank test was uscd for comparison between
prc- and post-appl icat ion of drugs. MBF increased f rom 71 + 10 to
i z 6 t t g m t - / m i n / t o O g a f t e r E a n d f r o m 7 4 + 1 l t o 1 0 7 t 3 0 m l / m i n
100 g af ter NE.
KH Lindner, FW Ahnefeld, EG Pfenninger, W Schuermann, lMBowdler/Unrversity Cl inic of Anesthesiology, University of Ulm, Ulm,West Germany
Norepinephrine (NE), an alpha l,2l beta-l agonist, seems to bean alternative to epinephrine (E), an alpha l,2ibeta 1,2 agonrst toimprovc cerebral blood flow (CBF) duringCPR. E probably stimu-latis cerebral oxygen consumption by its beta-2-adrenergic effect'This study compired the effect of E and NE on the balance ofcerebral oxygen delivery {CDO,) and consumption (CVO,) durinsCPR. Fourteen pigs weighing 26 to 22 kg were allocated to receivecither 45 pC/ki E {sevenl, or 45 pr/kg NE (seven) fol lowing-f iveminutes oi v'inlricular fibrillation and three minutes of open-chestCPR. CBF (measured with radronuclide-labelcd microspheres) andarterial and sagittal sinus oxygen contents (CaO, and Css)r) 19rymeasured during normal sinus rhythm and during open-chest CPRbeforc, at 90 seconds and five minutes after drug appliration C?O,and CVO. werc calculated using the formula CBF x CaOr and CBFx {CAO. - ' CssO. ). Extraction rat ios (ER) were calculated as CVO'/CDO . ihc Wilcoxon signed-rank test was used for comparisonbetwCen prc- and post-application of drugs.
Before 90 Seconds After Five Mlnutes AfterDrug Injection Drug Injection Drug Inlection30x7 54x14- 37x17U E T E
(mL/min/100 g)NE 3011 1
cDo, E 4.3!1 ,2(mL/min/100 g)
NE 3.711 .4cvo, E 1.810.9(ml/min/100 g)
NE 1 .610 .7E 40!12N E 4 1 1 1 3
58x22- 45!217.4t1 .7. 5 j t2.4
7.3t2.7- 5.8t2.72.010.5 1.610.8
ER(%)
1 .810 .7z t t o
26t11'�
11 t0 .23611 I22t8
Although mixed venous pH and Pco, measutements are more
reoreseitative o{ tissue r"ld-brte statG during CPR, they do not
adequately reflect the acid-base disturbances seen by the myocar-
dium. Despite an increase in MBF after both catecholamines, Pco,
and pH did not change significantly in both groups.
100 Effects of Epinephrine and Norepinephrine onCerebralOxygeri Delivery and Consumption During CPR
-P < .05 versus open-chest CPR before drug injection.
In this n.rodcl, E and NE at a dose of 45 prgikg during open-chest CPRhad thc same beneficial effect on cerebral oxygenation.
101 Transcranial Doppler Determination of CerebralPerfusion in Patients Undergoing CPR: Methodologyand Preliminary FindingsLM Lewis, C Gomez, B Ruo{{, S Gomez, lS Hall, BM Gasirowski/The University Hospital, St Louis University Medical-Center
Cerebral perlusion is decreased during CPR andfras been shownto dcteriorate consrstently over time. In order to determine i{ anymaneuvers can decrease or halt this deterioratron in cerebral perfu-
sion we undertook thc fol lowing study. Any patient being resusci 'tated for a nontraumatic cardiac arrest was eligible for the study'CPR was carried out in the usual manner while flow was continu'ously being measured in the internal carotid artery siphon usingtranscranra"l Doppler ultrasound (TCD)by the transo-rbital windowapproach. Vessejldentification was based on the angle and depth of
inionation and the direction of blood flow. Alterations in flow
velocity wcre noted and correlated to various th€rapeutic intewen-tions by virtue of a clock on the DoppleJ recorder and the CPR log
she.t. Flow velocrties were consisienily 6O% to 70% of normalduring the early phase of resuscitation but would deteriorate overtime until there was no evidence of net forward flow' Even early in
CPR flo* *tt nnlv demonstrated during "systole" with no diastolicperfusron. Epinephrine administration augments systolic flow ratesand decreases the time of "diastolic" no flow. TCD appears to be a
reliable way of rneasuring cerebral flow in patients yndergoing CPRwith resulis consistent with other described methods of cerebralperfusion determination.
102 The Prognostic Value of the Glasgow Coma ScaleMeasured 24 Hours After lnpatient SingleCardiopulmonary Arrest and ResuscitationBM Tho"mpson, RM Nowak, JM HouraniiDepartment of EmergencyMedicine, Henry Ford Hospital, Detroit , Michigan; Los Angeles,Cali fornia
Retrospective analysis of out-of-hospital cardiopulmonary ar'rest (CA) iirectly correlates the rapidity of awakening after resus-citation to the degree o{ neurologic outcome. To investrgate a
method of predictiig outcome from inpatient CA we-prospectivelyevaluated the Glasg5w Coma Scale (GCS) 24 hours a{ter successfulresuscitation by stindard advanced cardiac life support measures'Our 937-bed teaching hospital with an in-house "blue alert" team
had2,O7I "blue alertsl' in a14-month period. There were 1,612 CAs,
of which 246werc single {mean age,6I.8 yearsJ andwere resusci'
BeforeAorta E 38112
NE 3816
Pulmonary E 65112artery NE 6111 2
Great E 89i12cardiac NE 78!20vei n
Pco, (mm Hg)Drug Application
pHDrug ApplicationBefore After7 .34 t0 .1 5 7 .3110 .1 37.2810.10 7.2610.08
7 .17 r0 .10 7 .17L0 .077.1510.09 7.1010.06
7.00 10.06 7.0810.087 .00+.0.17 7 .04!0 .11
After3511 134!4
5911 26119
7311 06811 2
38

tated wi th c losed-chcst CPR and current ACLS euidel ines. Thcrewerc 106 142.7%) who died pr ior ro scor ing, leaving l40 pat ientscompris ing th is report . Sixty-one
1�43.6%) had a GCS of 9 or lcss and
al l but one died dur ing hospi ta l izat ion ( th is pat icnt had a preex-ist ing intracerebral b leed and depressed GCS pr ior to arrest) . Theremaining 79 (56.a%) had a GCS of t0 or more and 48 (( r0.8%,) weredrscharged, of whom 45
, �93.8%) went homc. Thus, in our study
GCS measurcd at 24 hours af ter rcsusci tat ion in thcse par ie l t ts wasan accluate prcdictor of o l r tcome. Pat icnts wi thout prccxlsr tngintracranial pathology with a GCS of 9 or less at 24 hour; uniformlydied, whi le approximately one-hal f wrth a score of l0 or morcsurvived to bc drscharged. I f conf i rmcd by other studics, thcscguidcl ines may bc used to g ivc rcal is t ic cxpectatrons to thc fan"r i lyor to a i locate medical resoLrrccs in thcse t imcs of economic ac-countabi l i ty .
103 lnadequate Airway Management CompromisingEMT-I Automat ic Def ibr i l la tor UseFD Pratt, J Potter, G Billingham, JT Niemann/UCLA Schoot ofMedic ine, Department of Emergency Medic ine, Harbor-UOLAMedical Center, Torrance, Cal i fornia; Fi re Department, County ofLos Angeles; Emergency Department, Daniel Freeman Hospi ia l
Pr ior work dcscr ib ing automat ic/scmiautomat ic dcf ibr i l la tor(ASD) use by EMT-I personncl ernphasizcd thc r- rccd fur laypcrsonCPR and ear ly acccss to advanced rcscuers. Howcver, thc t ' f fcct r r fairway managcmcnt by EMT-Is bcforc ancl :rftcr ASD usc or.rsurv ival has not becn addrcsscd. An ASD program using EMT-Ifirefighters was initiated by the Los Ar.rgelci Cirunty Firc'bcpart-mcnt in |une 1988. Thc 15 ASDs wcrc usccl on 90 nat icnts bvfanuary 1989. Protocol data forms wcrc complctcd t ry the EMT-Iusing thc ASD, and cassct tc- tapcd data of ECG rhythn"rs and on-sccnc voicc rccordings wcrc analyzcd. Dur ing l2 (13,2,) o{ ourdef ibr i l la tor uscs, tho pat tcntrs vcnt i l : r t ion and oxygcnat i t )n werucompromiscd by vorni t ing and subscclucnt aspirat ion pr ior toEMTI arr ival . A1l of thc pat ionts wi th a i rway compromisc cxpircc l .Six (50%)of thcsc pat icnts wcrc in vcntr ic l r lar f ibr i l la t ion, wi th apr<l lcctccl surv ival of l5% to 19'2, . Inaclcquatc : r i rway l r : rnagcmcntby EMT-I personncl r.rsing dcmancl valvc/mask dcviccs couicl havcdiminishcd thc cxpcctcd rcsusci tat ion ratc f rom vcntr icular f ibr i l -la t ion. Bascd on our car ly cxpcr icncc, wc rccornl l rcncl that morccmphasis bc placcd on ai rway managcrncnt whcn in i t iat ing ASDprograms. Also, advanccd ai rway adjuncts (csophagcal ocbturatorai rway, cndotrachcal tubc) should bc considercd for incorporat ionrnto thc EMT-l scopc of pract icc to cnhancc surv ival af tcr ASD usc.
-104 Adequate Ventilation Using a Mask and Bag WhileMaintaining Cervical NeutralityW Delaney, RE Kaiser JriDepartment of Anesthesiology, SUNy atBuffalo School of Medicine and Biomedical Sciences
We asscssecl thc abi l i ty to adccl , ratc ly vcnt i latc pat icnts in thcneutral posi t ion wi th a bag-mask wi thout ccrvrcal Jxtcnsion as isrecommended to f ic ld pcrsonnel for suspcctcd cerv ical spi r - rc-in jured pat ients. We prospect ivc ly studicd 100 consccr"r t iv i pa-ticnts admittecl for clectivc surgery uncler gcncral ancsthcsra. Thcstudy included analysis of agc, scx, wcigl-rt, hcight, prcscncc ofteeth, and ASA status. Fi f teen pat icnts wcrc cxcludcd duc todeviat ion f rom the protocol . Af tcr induct ion of ancsthcsia, wccould adecluately vcntilatc (r4 paticnts in thc ncutral posrtion{group 1) . The other 2I pat icnts requircd ai rway manipulat ion -- jawthrust, oral pharyngeal airway, or cervical extension to adecluatclyventilate (group 2). Group 2 patients wcrc olclcr, sicker, zrnd ap-peared to be hcavier and morc often edcntulous. Four Datj.cnts(4.7%) rcclu i red ccrv ical cxtension to vent i latc. Undcr idc j l condi-t ions, 95% of pat ients could be vent i latcd maintain ing ccrv icalneutra l i ty combined wi th the use of the jaw thrust or or i l pharyn-geal a i rway. We concludc that at least 5% of pat ients in whomcervical ncutrality is maintained arc at risk for inadequatc ventlla-tion and subsequent cerebral hypoxia.
Bi lateral Tube ThoracostomiesEB Josephson, MG Goetting/Departments of Emergency Medicineand Pediatr ics, Henry Ford Hospi ta l , Detro i t , Michigan
Asthma can induce high intrathoracic prcssure and alvcolar d is-tent ion/ p lacing the pat ient at r isk for barotrauma. pncumothorax(PT) can prccip i tatc cardiac arrest (CA) dur ing scvcrc asthmaattacks. In addi t ion, assistcd vcnt i lat ion dur ing CA may alsctproducc PT. This study conparcd the f rcquency of pT in asthmat icCA (ACA) and nonasthmat ic medical CA (NACA)and assesscd thcrc l iabi l i ty of c l in ical s igns to dctcct PT dur ing ACA. Wc cxanrncdthc medical records and radiographs, and intcrv iewcd thc t rcat ingp.hysic ian_s of e ight consccut ive pat ients wi th ACA. Wc comparcJthcrn wrth 50 consccut ive adul t s tudy pat ients in NACA. pT wasdiagnoscd i f prescnt radiografhical ly o i d iscovercd at tubc thora-costomy. Mcdian agcs wcre 14 years ( range, 12 to 52) in ACA and67 years ( range, 33 to 92) in NACA. Al though age di f fercd bctweengror-rps, body wcight and therapy wcrc comparablc. pT was morcfrccluent in ACA (s ix of c ight vs s ix of 50; 1 ' . .01). Only r ight-s idedPT uccurrcd in NACA (s i te of subclavian cathctcr izat ion), whcrcasthrcc of s ix l lT in ACA could not bc at t r ib l l tcd to nccdlc puncture.Asthrnat ic PT was not dctectcd c l in ical ly whi lc four of s ix wcrccLagnoscd in thc NACA group. Wc concludc that pT in ACA occursfrcc luent ly , of tcn is unrc latcd to l inc p laccmcnt. and is c l i f f icul t toc lctcct c l inrcal ly . Thcrcfore, e rnpir ic h l latcral chL'sr tubc placcmcntshould bc an cssent ia l part of rcsusci tat ion cf for ts dur ing ACA.
.106 Prehospital Use of lnhaled Bronchodilators inReversible Airway DiseaseI Machel, S Nevins/Department ol Emergency Medicine, Residencyin Emergency Medicine, Morristown Memorial Hospital, Morrrstown,New Jersey
Sincc thc aclvcnt of mobi lc intcnsivc care uni ts, prchosprta lt rc: l tntcnt of b l rnchospast ic lung t l iscasc has bccn pussib lc; how-cvcr, i t has bccn l int i tcd to agcnts having c i t l - rcr a h igh lcvcl of s idcc{fccts or low cf f icacy. Ncbul izcd bcta-agonists arc rccognizcd asthc mainstay of t rcatmcnt of acutc rcvcrs ib lc a i rway drscJsc in thchospi ta l sct t ing. Our purposc was to invcst igatc thc Lr t i l i ty andcor.npl icat ior-rs of thrs thcrapy in thc f ie ld, as wcl l as thc accuracy ofdiagr-rosis of bronchospasm in a prchospi ta l carc systcm wi th i rutstancl i r - rg ordcrs. Pararncdics wcrc instructccl by rcspiratory thcra-l . r is ts ancl physic ians in thc adn-r in ist rat ion of isocthar inc andrnctaprotcrcnol wi t l - r a hand,hcld ncbul izcr , and wc prospcct ivc lystudiccl 94 pat icnts in which t l - r is thcrapy was givcn. Onc patrcntwas unablc to comply wi th thc t rcatncnt , onc dcvclopcd s. ,pravcn-tr icular tacl - rycardia, onc dcvckrpccl scvcrc hypcrtcnsi , ,n, an. l t l r r . .wcrc j r . rc lgcd to havc bccn t rcatccl inappropr iatc ly. Al l othcr pat icntswcrc corrcct ly c l iagnoscd as having an c lcmcnt of rcvcrs ib lc a i rwaycl iscasc ancl wcrc t rc: l tcd appropr iatc ly. Forty-scvcn pat icnts had af i r - ra l d iagnosis of uncompl icatcd bronchospasm. Thc othcrs hacl af inal c l iagr-rosis of bronchos|asrn as wcl l is at l t l i t i r rnal d iagnoscsrncluding congcst ivc hcart fa i lurc, pncumonia, l -ncrast i r r i i lungci iscasc, pncurnoth<lrax, and gastro intcst lnal b lccding. Ovcral i ,70 'Z ' of pat icnts showcd i rnprovcmcnt, 27,X, showcd no changc, ar-rd2(2, worscncd. Wc concludc that ncbul izccl bcta-agonist thcrapy inthc prc l - rospi ta l carc sct t i r . rg is fcasib lc and that in carcfu l ly sc lcctcdpat icnts i t is both safc ar-rd cf fcct ivc.
107 Prehospital Administrat ion of lnhaledMetaproterenolDR Eitel, SA Meador, R Drawbaugh, D Hess, NK Sabulsky/Department ol Emergency Medicine, York Hospital, Yon<,Pennsylvania; Division of Emergency Medicine, The PennsylvaniaState University, The Mil ton S Hershey Medical Center, Hershey;School of Respiratory Therapy, York Hospital, York College ofPennsylvania, York
This study evaluatccl the prchospital use of inhaled mctap-rotcrcnol. Advanced l i fc support providers from seven medtc unitswcrc traincd using a standarizcd training curr iculum to idcnti fypatrents l ikely to bcnefi t from prehospital administratron of in-haled rnctaproterenol. Candrdatcs for treatment wcrc those with ahistory and symptoms suggestivc of acute obstructivc lung discase,those unlikcly to bc rn congestivc heart failure, and those with noother contraindicatron for this therapy. Trcatmcnts were admini-stered by direct ion of medical command. Unit doses of metaD-roterenol were uscd in a small volume ncbulizer powerrd by 8 i /min 0,. Each treatment was evaluated by objective (peak f low,respiralory rate, heart rate) and subjective (dyspnea, wheczing, airentry/ tremor) criteria. Data after admissron were used to assessfield diagnostic accuracy. We prospectively included 122 patients
No.Ase (y0WeightY. ldealASA% with teeth-Student's ttest at 0.02tChi-square at 0.02.
Group 16436.5373.27+7.471 .57892
Group 22 150.6-80.98+23.562.00f72
105 Asthmatic Cardiac Arrest: An Indication for Empiric
39
rn the study {71 men, ages 63 + 19 years) . Overal l , pcak f lows
rncrcascd (102 t 50 L/rn in bcforc t reatmcnt, 139 t l {4 L/rn in af ter
t reatment, P < .00 1 ) , respiratory rates dccrcased l34 ! 7 bcforc, 29+ 7 af ter , l ' < .0011; and heart rates did not changc (1 15 1 20 bcfore,l14 t 20 af tcr , P = .51). In 62'% c: f pat icnts, the increasc in f lowcxcccded l5%. Wheezing improved in 59"1 ' of the pat ients, wors-
cned in 4 '%, and did not change in thc others. Air cntry inrprovcdin 59' lo of pat icnts. Mi ld t rcrnor occurrcd in 87, of pat icnts,
mocleratc t rcmor occurrcd in l "k, and no t remor occurrcd rn theothcrs. Signi f icant c lysrhythmias did not occur. Advanccd l i fesupport providcrs corrcct ly idcnt i f icd pat icnts for th is thcrapy, andno tcchnical problcn-rs wcrc cncountcrcd in thc f ie ld wi th th is
t rcatmcnt approach. Wc concludc that aclvanccd l r fc support pr , '
v idcrs can bc taught to idcnt i fy pat icnts l ikc ly to bcncf i t f ron ' r
inhalcd metaprotcrcnol , that inhalcd mctaprotcrcnol can bc ad-ministcrcd in thc f ie ld, and that mctaprotcrcn(t l is both safc ancl
cf fcct ivc whcn uscd in thc prchospi ta l sct t ing.
- 108 Comparison of Two Delivery Methods of Albuterol inEmergency Department Management of Acute AsthmaFR LaFleche, DP Milzman, CB Philput, MJ Bono, J Vargas/EasternVirginia Graduate School of Medicine, Emergency MedicineResidency Program, Eastern Virginia Medical School, Norfolk
In aclltc ashtrna, {1, sytnpathomitnctics l-ravc long l.rccn adr-r-rini-stcrccl by hand-hcld ncbul izcrs in ct -ncrgcncy dcpartr -ucnts. Ncwcr
studics havc c lcrnunstratcd the casc and c l l icacy of using mctcrccl -
t f t rsc inhalcrs wi th sp:rccr at t : rchtncnts in thc ambulatory carc t rcat-
r - r . rcr . r t of c l ' r ronic obstruct ivc pulmonary discasc ancl asthma. This
si r - rg lc-bl ind, prospcct ivc study comparcd thc cf f icacy of a lbutcrolaclministcrcd by hand-hcld ncbr ' r l izcr vcrsus a tnctcrcd-c losc- in-halcr wi th an InspirEasc" at tachlnct t t . Forty-ninc adul t pat icnts
wi th acl l tc asthrna prcscnt ing to thc ED wcrc randomly assignccl to
tur-rc of two grol lps. Trcatmcnt consrstccl of c i t l - rcr 2.5 mg albutcrolin.J r rL normal sal inc by hand-hcld ncbul izcr (group l )or s ix puf fs
of a lbr . r tcro l (0.( r mg) g ivcn at o l lc- ln inLl tc intcrv:r ls by mctcrccl -c loscinhalcr wi th thc L-rspirEasc" at tacht lcnt (group 2) rcpcatccl cvcry 30
lu l inLl tcs thrcc t imcs. Thc groups wcrc wcl l rnatc l - rcc l f t t r : rgc, scx,pr ior r -ncdicat ion, and scvcr i ty of at tack as dctcrmined by a physi-
c lan scvcnty : lsscsslncnr scorc ancl in i t ia l pcak cxpiratory f low ratc
iPEFR). Thcrc was no stat is t ical c l i f fcrcncc in PEFR improvcl 'ncntbctwccn thc two groups. Group I (25) had protrcat lncnt PEFRs of
166.5 ! 63.2 and post- t rcatmcnt PEFRs of 2U0.5 + 139.(r vcrsr-rs 159'6+ 5(r .5 and 2115.0 t 8u.0 for group 2 (24). Thcrc was also no c l t f fercncc
in the f rcc lucncy of adrnin ist rat ion of aminophyl l tnc, stcroids,at lmission, or advcrsc s idc cf{ccts. Wc concluclc that a lbutcrol
ach.nin istcrcd wi th a rnctcrcd-dosc inhalcr wi th thc InspirEasc'at tachmcnt is as cf fcct ivc as hand-hcld ncbul izcrs for thc t rcatmcntof acutc astht .na in thc ED and of fcrs thc advantage c l f lowcr cost and
casc of adrnin ist rat ion.
109 Util i ty of Peak Expiratory Flow Rate in theDifferentiation of Acute Dyspnea: Pulmonary EdemaVersus Obstructive/Bronchospastic DiseaseRM McNamara, D CionnilMedical College of Pennsylvania,Phi ladelphia
I t occ:rs ional ly rnay bc di f f icul t in the prehospi ta l or cmorgcncydcpartmcnt set t ing to d ist inguish thc ct io logy of an acutc episodc
of rcspiratory d ist ress. This study prospcct ivc ly examined thc 'use-fu lncis of thc absolutc pcak expiratory f low ratc (PEFR) in thc c l i f -fcrcnt iat ion of acutc, moderatc- to-sevcrc dyspnca due to conges-
t ivo hcart fa i lurc {CHF) wi th pulmonary cdcma from that sccon-
dary to obstruct ive/bronchospast ic lung diseasc (OBLD). Adul t EDpat icnts, agc 30 or o lder, wcrc inc ludcd i f a PEFR was dctermincdpnor to pharrnacologic intcrvent ion and a data shcct was com-plctcd rcgarding their ED cvaluat ions. Only cprsodcs of dyspnea
ihoueht duc to CHF or OBLD alonc at the t ime of hospi ta l d ischargc
wcrc subiectcd to anaiysis. Stat is t ical analysis uscd Fishcr 's exact
test or an unpaired t test when appropriatc. A total of 36 cprsodes(OBLD, LZj CHF, l4) o{ acute, moderate- to-sevcre dyspnea in 35
Dat ients met the entry cr i ter ia. Therc was no stat is t ical ly s igni f i -
iant diffcrcnce betwcen the two groups rn agc, sex, race, and the
prcsenting respiratory rate, hcart rate, mean artcrial blood pressurc,
or thc presencc of diaphoresrs. Thc majority of the OBLD group ( l9
oI 22,86%) prcsented with wheezing; howcver, a 1ar5;e pcrce-ntagc
of thc CHF group { ten of 14,71%l a lso prescnted wi th somc degrec
of whcezing. The OBLD group was more likely to report taking
bronchodi l i tors (91% vs 3(r%, 1 ' � < .001)and less l ikely on a loop
diuret ic and/or d igoxin {14% vs 57%, P < .01). The mcan absolute
PEFR I SD for thc OBLD group was I 10 1 49 L/min versus 225 x97
L/min for the CHF group iP < .0001). By combinrng the medicat ionhistory wi th the PEFR i t was possib le to correct ly c lassl fy a l l
cpisodes. PEFR appcars to be a useful tool in d i f ferent iat ing acute
dyspnca sccondary to thesc cnt l t ies.
*110 Innovat ions in Aminophyl l ine Moni tor ing andTherapyBJ Kino, R Day, G Pearce, G Fulde/Australasian College ofEmergency Medicine, St Vincent's Hospital, Sydney, Australia
Wc hypothcsized that an indiv idual ized computer-bascd proto-
col can improvc accuracy in achicving targetcd therapeut ic p lasma
theophyl l inc lcvcls and l i rn i t tox ic i ty , as comparcd wi th standardcInical pract icc. Wc prospcct ivc ly comparcd theophyl l ine conccn-
trations acl'ricvcd in two sccluct-ttial groups of crnergency depart-mcnt pat icnts rcquir ing IV aminophyl l ine for acute bronchospasm.Cor-r t r i r l pat icnts {4(r) rcccivcd aminophyl l inc thcrapy accordrng to
widcly uscd clinical guidclir-res, while tl-re amount of aminophyl-l inc g ivcr-r to cxpcr imcntal group pat icnts (43) was indiv idual ized
accurding to a computcr ized modcl . Thc computcr uscd easi lydc{ incd pat icnt charactcr is t ics and includcd basel ine thcophyl l inelcvcls mcasurcd rapid ly by rcsidcr-r ts in thc ED wi th a monoclonalant ibody tcst k i t .
Percenl of Patients Achieving Therapeutic, Subtherapeutic, and ToxicPlasma Theophylline Concentrations at One and Six Hours
one hour Sixhourscontrol(%) Experimental(%) Control('/.) Experimental(%)
Tox i c (>20 !g /m l ) 7 a 10 0Therapeutic ( 10 to 20 !g/ml) 26 81 37 91Sub the rapeu t i c (<10L rg /m l ) 67 19 53 I
Wc concludc that a computcr izcd dosagc predict ion protocol that
ir-rcorporatcd basclinc plasrna thcophyllinc conccntrations resultedin drar-r-ratic improvcmcnt in thc ability to achievc therapeuticplasr-r-ra t1-rcophyllinc conccntrations in ED paticnts.
111 lmpact of Portable Pulse Oximetry on Arterial BloodGas Analysis in an Urban Emergency DepartmentS Joseph, AL Kellermann, CA Cofer, BB Hackman/Divisions ofEmergency Medicine and Cardiology, University of Tennessee,Memohis
Artcrial bloocl gas (ABG) analysis is onc of thc ten most costly
cmcrgcncy dcpartmcnt tcsts bascd on cost t imes f requency or-
dcrcd. Portablc pulsc oxrmctry offcrs a simplc, noninvasive way to
asscss oxygcn saturation, but rts impact on physrcian ABG testing
and cluality of carc is unknown. For two months prcceding and twomonths following introduction of a protable pulsc oximeter in our
tcaching ED, rcsidcnt physicians rccorded, for all ABGs, their
rcason firr orclcring tht: test, primary patient problem, and planned
managcmcnt 1n rcsponse to ABG results. Following introduction of
oximctry, rcsidcnts wcrc also rcquired to obtain an oximetryrcading and attach it to each ABG rcquest that did not involve a
cardiac or rcspiratory arrest. The only educational intervention
offcrccl was a brief {fivc-minute) orientation to the use and limita-
tions of pulsc oximetry. Case records werc subscquently-reviewedby one board-certified physician blindcd to visit date to determinethc perccntage of ABGs ordered during both periods that were
indi-ated by explicit clinical criteria. Atotal of 2O,l20patientvisitswcrc notcd duiir-rg the four-month study pcriod. During the two
months pnor to introduction of oximetry, ED resident physicrans
orclcrcd (r95 ABGs, 436 (63% ) o{ which were indicated by American
Collcge of Emergency Physicians or American College oI Physi-
cians-criteria. During the two months following introduction of
oximetry, ABG usc decreascd by 43% 1�95%
CI = 34% to 52%, P <
.001). This differcnce was not explained by differences in total
Datient vislts or case mix. Residents decreased their ordering of
indicated ABGs by almost as great a degree as they reduced ordering
of unindicated tcsts, suggesting they did not reliably distinguish
between the two. However, decreased ABG test ordering was not
associated with any serious adversc patient outcomcs. Based onproiected totals, wc estimate that this device (which retails for
$2,+so1 will decreasc laboratory charges in our ED by $95,000 peryear. We conclude that portable pulse oximetry offers a highly cost
effective way to decrease ABG test use without compromistngquality of carc.
- 1 12 Aspiration During Manual Low'Frequency JetVentilation
40

EXHIBITORS
Annals is the official journal of the American College of E,mergencyPhysicians and the Society for Academic Emergency Medlcine.Editorial Board members will be on hand to answJr vour questlonsabout the journal and editorial pol icies.
Annals of Emergency MedicineP . O . B o x 6 1 9 9 1 IDallas, TX 75261-9911
Beta Medical Products, Inc.100 Lincoln StreetAkron. OH 44308
Electro-Diagnostic Instruments3401 Winona AvenueBurbank . CA 91504
Encylopaedia Britannica, USA310 South Mich igan AvenueChicago, IL 60604
Epic Sof'tware Systems, Inc.36-5 Scenic DriveAshland. OR 97520
l'enem, Inc.84 Wil l ianr StreetNew York, NY 10038
First Medic2445 l40rh Avenue N.EBellevue, WA 98005
Cenentech, Inc.2183 Manchester AvenueCardiff. CA 92007
(214) 550-091 I
(216) 253-7766
(213) 849-7701
(3t2) 341-7342
(so3) 770-t726
(212\ 248-0220
(206) 641-4774
(6r9) 632-8935
MEDphone CorporationThe Atr ium Suite 210E. 80 Route 4Paramus, NJ 07652-2647
MICROMEDEX, Inc.660 Bannock, 3rd FloorDenver, CO 80204-4506
Nonin Medical Inc.12900 Highway 55Plymouth, MN 55441
NOVA Biomedical200 Prospect StreetWaltham, MA 02254
PPG Biomedical Systems9875 WidmerLenexa. KS 66215
Weatherby Health Care25 Yan Zant StreetNorwalk, CT 06855
HPSG-McGraw Hill3562 Argonne StreetSan Diego, CA 92117 ,6l9D
274_9032Current medical books used for emergency service.
Intelligent Images, Inc.55 l0 Morehouse Drive, Suite 210San Diego, CA 92121 (619\ 4s7-ssls
Th.e Beta One x-ray trauma bed allows for diagnostic qualityradiographs within minutes of admission. I ts exceptional stabi l i iy anispecially designed operating features facilitate its use for rrauma cases.
Intelligent Images features DxTER clinical patient_care simulation.DxTER Courseware, developed by Intelligent Images, provides thehighest quality in interactive learning. By utirizing interactive videodisctechnology, the DxTER "Artificial Reality" patient_care simulationsenable physicians, residents and students to practice decision_makingand problem-solving in privacy without placing patients at risk.
Bi lateral Impedance Plethysmograph, Modcl BIp-750, l i rr the simple.non-invasive and accurate diagnosis of acute proximal Deep VeinThrombosis.
The MDphone|M System: Transtelephonic defibri l lat ion system: pa-t ient Unii with two-way speaker phone, self-adhesive electrode pads.and defibri l lator. Base stat ion with ECG display, clef ibr i l lator controland data computer. Clinician at hospital maintains 2-way communica_tion and monitoring and controls transtelephonic defibiillation of pa_tienls in relnote locatiOns.
(201) 843-6644
(303) 623-8600
(612) s53-9968
(6r7) 894-0800
(913) 894-7s31
(203) 866-1144
Encyclopaedia Britannica wil l have on display the 32 volurne edit ion,the Great Books of the Western World; plus a complete l ine of educa_tional accessories. Clinical, Industr ial and Environmental Toxicology, Occupational
Medicine, international drug information, and diseaie/trauma clinicalinlirrmation systems lbr the entire hospital medical staff. These infor_mation systems are available on: CD-ROM lirr use with Dersonal com_putcrs, computer tapes fbr use with IBM pC'S and DEX VAX Main_Itames and mocrofiche.EPIC soltware provides comprehensive, customized, altercare instruc_
turns firr emergency and ambulatory care patients. The EplC progranlis user f i iendly and tast, requir ing only 30 seconds input t ime pei pa_tient. I t is currently in use at over 40 hospitals and cl inics. There aremore than 300 separate instruct i trns in the EplC databasc which canbe printed in either Engtish or Spanish. The prograrn instructions maybe easily cuskrntized to fit your own practice needs and pref'erences.Stop by our booth to pick up our complementary demonsrrarron pro_gram diskettes.
Nonin Medical Inc. manufactures pulse oximeters that are ideally suitedfor emergency and transport applications. Features include comoactsize, lightweight, long battery life, LED displays, reusabler;enro.i fo,all patients (including new reflectance sensor), and MRI comoatabili-ty. One monibr also has an ECG synchronization system and resoira_t ion mrrn i to r ing capab i l i t y .
The FEFrM End-Tidal CO, Detecbr, a disposable device, assists inveri tying proper endotracheal intubation by u color change that variesbreath-to-breath in response to CO, levels.
NOVA's series of Stat Protile analyzers perform blood gas analysis pluselectrolytes (Na+, K+, and Cl -), ionized calcium, slucose and hema_tocrit. These autocalibrate<j analyzers use 130-250 u'i of whole blood,are easy to use, require low maintenance and utilize a self-containedreagent and waste pack that eliminates exposure to infectious waste.
First Medic is an international leader in the manufacturing of automaticdeflbrillators and medical centrol accessories. First Medic willdemonstrate the newest generation of automatic defibrillaters _ TheModel 610. Through acquisition of international businesses producing equipment
for cardiovascular and respiratory monitoring anO Oiaglosis, llCBiomedical Systerns, a new division of pittsburgh_based ppb Industries,offer products that are designed for use in the operating room, criticalcare unlts, emergency and cardiac catherization laboratories.
Activase (R) alteplase. A tissue plasminogen activator was pioneeeredby Genentech Inc. Activase is indicated for use in the manasemenrof acute myocardial infarction for the lysis of thrombi obstructi-ng cor-onary arteries, the improvement ofventricular function and reductionof the incidence of CHF.
We are a prominent physician recruiting fim wittr over 300 opportunitiesnationwide. Stop by our booth to learn more about our opportunities.
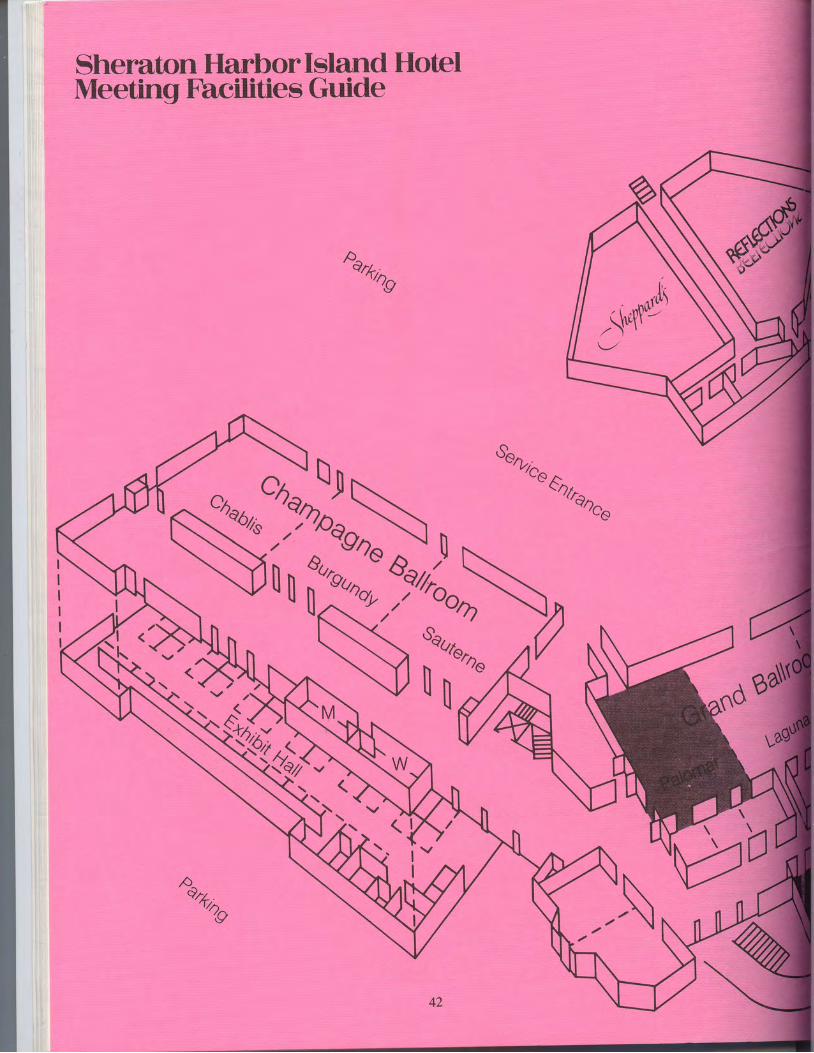
Sheraton Harbor Island HotelMeeting Facilities Guide
p^ehhT
A
%
1,,,r0\
_ ,' ,^lltL' .r ht .VI -
/ l
42

Sonntnq
"doo'l
soa
Most of the Annual Meeting functions wil l beheld at the Sheraton Harbor lsland.
May 22,23, and 24 -
General Session A: Chablis
May 22,23, and 24 -
General Session B: Burgundy
May 24 - General Session C: Palomar
May 23 - Annual Business Meeting:Burgundy
May 23 - Research Directors Luncheon:Harbor Terrace
May 23 - EMRA Resident ResearchForum: Chablis
May 23 - EMRA Reception: HarborTerrace
May 23 - SAEM Board of Directors:Chenin
May 24 - International Session: palomar
May 24 - Residency Directors: WhiteWines (Chenin, Colombard,Gamay, Riesl ing)
San Carlos
Chen inColombard
Ridding GamaY
43

Sheraton Grand Hotel
Fairbanks Ballroom
BelAire Ballroom Grrace A Grrace B Grrace C GrraceD
{ F
The Sheraton Grand Hotel wil l be the site of:
May 22, Opening Reception: Bel Aire Ballroom
May 22, Fellows Dinner: Fairbanks Ballroom
May 24and May 25, Poster Sessions l l and l l l : Del Mar, Monterey, La Jolla' and Carmel
May 25, General Session A: Bel Aire Ballroom
General Session B: Fairbanks Ballroom (Terrace A-C)
General Session C: Fairbanks Ballroom (Terrace D)

DM Yealy, MC Plewa, JJ Reed, RM Kaplan, K l lkhanipour, RDStewarVUniversity of Pittsburgh Affiliated Residency in EmergencyMedic ine; Center for Emergency Medrcine of WesternPennsylvania, Pi t tsburgh
High-frequency jet ventilation above 60 cycles/min has previ-ously been demonstrated to protect from aspiration. The recom-mended O, driving pressure of 50 psi for manual low-frequency (20cycles/min) jet ventilation commonly cxpels materials from theupper airway; however, the protective effects of manual percutanc-ous translaryngeal jet ventilation against aspiration are unknown.Seventeen anesthetized adult mongrel dogs (20 to 25 kg) werestudied in 36 t r ia ls. Group 1 (Control ) received no ai rway protec-tion; group 2 (Tube) received ventilation by a cuffed, 1ow-pressure,high-vo1ume, 8.0-mm cndotracheal tube positroned 2 cm above thecarina; group 3 (fet) received manual jet vcntilatron at a ratc oI 2Ocycles/min, I :E rat io of 1:2 and O, dr iv ing pressure of 50 psi by apercutaneous l3-gauge cannula. Half the trials were performcd at30 degrees and half at 45 degrees of head elevation. An I BF catheterplaced under direct visualization into the proximal airway I to 2 cmbelow the cords (vet above thc tube cuf{ or cannula tioi was used toinstill 250 mg Gastrograffin'" into the trachea over fivi minutes. Ananteropostenor chest radiograph was obtaincd to documcnt prcs-ence and degree of aspiration {on a 0 to 3 scale) and was rcvicwcd bya radiologist blinded to the experimental manipulations. At 30degrees elevation, none of six fet and none of six Tube anirnals hadradiographic evidence of aspiration (scores of 0), while six of sixControl animals had moderate-to-scverc aspiration (scores of 2 to3). At 45 degrees elevation, none of six Tube aminals had evidenceof aspirat ion (score of 0) , four of s ix |et anrmals showcd mi ldaspiration (scores of 1), and six of six Control anrmals showcdsevere aspiration {scores of 3). When compared with thc Controlgroup, both the Tube and the fet groups demonstrated signficantlyIess aspiration at 30 and 45 degrees lP = .0O2). We conclude that inour model standard manual low-frequency jet ventilation at 30degrees head elevatron was associated with a low risk of aspiration,comparable to that obserued with a cuffed endotrachcal tubc, withincreased risk of aspiration at greater head elevations.
- 113 Emergency Intubation in the Uncooperative TraumaPatientJJ Kuchinski, GH Tinkoff , M Rhodes, JW Becher JrlHospital of thePhiladelphia College of Osteopathic Medicine, Lehigh ValleyHospital Center, Al lentown, Pennsylvania
Emergency intubation for sedation and paralysis of agrtated, un-cooperative multiple trauma patients is being used in many traumacenters and emergency departments. The records of all traurnaadmissions requiring emergency intubation during resuscitationwere reviewed for the l8-month period from fanuary 1987 to fune1988. Patients with unambiguous documentation of intubation forreasons of agitation and combativeness were divided into highinjury severrty {HIS) and low injury severity {LIS) subgroups usingadmission Trauma Score (TS) and Injury Severity Score {ISS). HIS =TS < 13 or ISS ) 16 and LIS : TS > 13 and ISS < 16. Fif ty-sevenpatients were intubated primarily for agitation and combativeness;of these, 38 |,70%) were classi{ied as HIS and 19 ,.30%l as LIS by ourcriteria. All 38 HIS patients had significant injuries diagnosed afterintubation and paralysis, requiring further intervention. The HISgroup had a mean age of 3 1, mean ISS of 25, and mean length of stayILOS) of 20.5 days. Mortality was9o/". The mean hospital cost was$24,794, and a mean of 12.7 hours per day in nursing care wasrequired. To determine the rmpact intubation had on traumapaiients with low injury severityl the LIS subgroup was comparedwith a similar group o{ randomly selected unintubated traumapatients with TS of more than 13 and ISS of less than l6 in the samestudy period. The only mortality in these two groups occurred inthe intubated group. The cause of death was CNS anoxia due to anesophageal intubation. These groups were analyzed for statisticallysignificant differences {P < .05) in age, LOS, hospital cost, hours perday of nursing care, and percent of patients with an ETOH levelabove 100 mg%.
n rS/,ss li3l,n .o. ill,lilln 8i3llo iJ."ff"lntubated 1 9 1 5/9 23.4 6.3 1O.4 7,1 50 58Unintubated 32 1617 31.0 5.6 5.9 3.456 19P < .05 by Robusl t test.P < 0.05 by chi-square analysis.
For the majority of uncooperative, agitated multiple trauma pa-tients, emergency intubation with paralysis and sedation al1ows for
prompt diagnosis and treatment of rnjuries that might otherwise bedelayed. However, we conclude that for patients with injuries oflow severity treated in this manner, care is more costly and laborintensive than for patients of similar injury severity who are notintubated. These patients, as a group, are younger and more likelyto be legal ly intoxicated.
'114 Value of End-Tidal CO^ Measurement in theDetection of Esophageal lf i tubation During CardiacArrestAJ Sayah, WF Peacock, DT Overton/Department of EmergencyMedicine, Will iam Beaumont Hospital, Royal Oak, Michigan
Mcasurement of end-t idal CO, (ETCO,l has been used to detectinadvcrtent esophageal tube placement
- in pat icnts wi th intact
hemodynamics, but has not been studied dur ing cardiac arrest .This study sought to determrne i f ETCO, measurement coulddrst inguish t rachcal f rom csophagcal tube placement dur ing c loscd-chest massage. Twelve large dogs (avcrage weight , 23.5 kg) wcrcanesthet ized using 25 mg/kg pentobarbi ta l . Endotracheal tubeswcrc placed in the t rachea and esophagus. Placement was ver i f iedby f ibcropt ic cndoscopy. Bi lateral femoral ar tery l incs were in-serted. Ventilation was performed during the prearrest phase throughthe t rachcal tube, using a t idal volume of 15 rng/kg. Ventr icularfibrillation was induced using a (rO-Hz dischargc through a rightvcntr icular pacemakcr. Af ter four minutcs of arrcst , c losed-chestmassagc was in i t iatcd at ( r0 c/min using a Michigan InstrumcntsThumper- , and cont inucd for 20 minutes. The dogs wcrc div idcdinto two groups. Group A had t racheal vent i lat ion; group B, eso-phageal ventr lat ion. Unused tubcs wcrc rcmoved. ETCO, wascont inuously rccordcd beginnrng two l l l inutcs pr ior to arrcst .Arter ia l b lood gascs were obtained onc minutc pr ior to arrest , andonc, f ivc, and 20 minutes af ter c losed-chest massagc was in i t iated.Groups wcre compared using the Mann-Whitney U test . There wasno significant differcnce betwcen the groups mean artcrial pres-surc, weight, blood loss, IV fluid volume, or prearrcst arterial bloodgases.,ETCO, diffcrcds,ignificantly between the groups thro_ughoutc loscd-chcst rnassage (P < .001). In group A, ETCO, ranged f rom l4to 34 (avcragc, 2I) . In group B, ETCO, ranged f rom 2 to l lmm Hg
{avcragc, 5) . Measurement of ETCO, can rc l iahly d ist inguish cso-phageal from trachcal tubc placemenl during closed-chcst massageln oogs.
- 1 15 Core Temperature Measurement in HypovolemicResuscitationRW Nicholson, KV lserson/Section of Emergency Medicine,Univers i ty of Ar izona, Tucson
Accuratc corc tempe raturc mcasurcmcnt in severcly hy-povolcmrc pat ients can be di f f icul t to achievc. Currcnt ly , a l thoughboth tympanic membrane and central venous tempcratures aresaid to rcf lect corc temperature in re lat ively stable pat ients, i t isunclear whether th is is appl icable to thc acutely hypovolemicpat icnt undergoing rcsusci tat ion. A dog model was used to deter-minc a convcnicnt method of measuring core temperature duringthe rcsusci tat ivc phasc of hypovolcmia and thc accuracy of mul-trple sources of temperature measurement. Adult anesthesizcdgreyhound dogs had thcrmistor probes placcd for continuoustcmperature monitoring in thc brain, central vcin, tympanicmembrane, bladder, rectum, esophagus, and subcutancous tissue.The dogs were rapid ly b led to 65% of thci r in i t ia l rntravascularvolume. After a period of delay, and in a stepwise manner, theyreceived an autologous transfusion that had bcen cooled to 7 C.Scrial tempcraturc rcadings wcre taken during a baseline and 60-minute posttransfusion period. The readings werc analyzed usingPearson's correlation coefficient. Brain temperatures correlatedvery highly with those in the tympanic membrane throughout theanrmal 's course {r = .943i P < .0005). Rectal ( r = .9O6j P <.0005) andbladder ( r = .836; P< .0005) temperatures also correlated wel l wi thbrain tempcratures. Central venous system, however, correlatedpoorly with temperatures at a1l other sites, reflective of the markedswings in intravascular temperature caused by cold transfusions.These wide variations were damped at the other sites. Becauseintravascular hypothermra appears to be the source of the arrhyth-mias and hemostatic abnormalrties often seen during the resusci-tation of acutely hypovolemic patients, this may be the mostaccurate site for core temperature measurement. However, be-cause after the initial resuscitation organ temperatures are of primeimportance, tympanic membrane temperatures are the most usefulsource of core temperature in these patients.
45

I
'1 16 Exsanguination Cardiac Arrest in Doos:Pathophysiotogy of DyingSA Tisherman, P Safar, F Steiz, y Leonov, K Oku, W Stezoski/International Resuscitation Research Center and Departments ofAne_sthesiology and Surgery, University of pittsburgh
. Exsanguination cardiac arrcst/ common in trau-ma, has receivedl i t t le attcntion. previous studies used barbituratc ancsthcsia; how_:.i.,.1 lT ll"
study, N,O-halothane anesthesia was used. r" f7 Jogr,under l lght anesthesia, during spontaneous breathing of air, hei l lorrhage was init iatcd by an aort ic catheter. Mean art ir ial prcssure{MA^PI to 5,! mm Hg in 6Z 145_seconds, and to less than 25.;; Fi;in 100 + 4(r seconds. Carotid f low decreased rapidly, U"t p"r. i . t"8unti l mcan artcrral pressure was less than l0 mm Hg. pulselessnesscrccurrcd at 6.2 + 3 minutes with blood loss of g0 t S mf,7kg. EfCbccame depressed at MAp.50 mm Hg. After brielhyperventilationin^eight of 14 dogs, tidal volume dccrJased, and apnea occured at 6..5+ 3 minutes, srmultaneous with EEG si lence and MAf of f O mm Ugor lcss without pulsations (cl inical death). Heart ratc ini t ial lyincreased and then slowed in al l dogs. ECG activi ty contlnucd withbradycardia for 30 or more minutes during pulseiessness {electro_mechanical dissociat ion) in al l dogs; i ,nc' ieveloped rpo.rt".r"o., ,ventr icular f ibr i l lat ion. At pulseleisncss, paO, was above S0 mmHg; PaCO,, 26 ! tZ mm.Hg; pHa,7.4 r 0.1, and BD, t i .3 t 4.2 mEq/L. Hcmatdcri t dccreased troi qzx6y" to 38t gZ. in 12 of la ;&;;an agonal attcmpt at sclf-rcsuscitat ion (gasps with t iclal volurne 35dto 600, incrcascd ECG frequency, no inCicised MAp) occurrcd aftertwo to 7.5 minutcs of cl inical dcath. Dcath in exsanguination iswith clcctomechanical dissociat ion, rcsult ing from hypovolcmichypotcnsion, not hypoventi lat ion, [rypoxc-i", o, acidcmia. Theagonat state may explain "miraculous" recovcries.
'1 1 7 Exsanguination Versus Ventricular FibrillationCardiac Arrest in Dogs: Comparison of NeurologicOutcome - preliminaly DataSA Tisherman, P Safar, F Sterz, y Leonov, K Oku, W Stezoski/International Resuscitation Research Center and Departments ofAnesthesiology and Surgery, Universitv of pit tsburoh
Ncurologic re covery from_cardiac jrrest is limiicrl by thc postre _
: lscitat ign syndromc, including prolongcd mult i focal ccrclr.al hy_
popcrruslon and bl(x)d dcrangcmcnts from stasis. we hypothesizcthat bloodlcss ischcmia, as in exsanguination (EX), is bciter toler_atcd than nonnovolcmic vcntr icular f ibr i l lat ion (VF) cardiac arrcstof the samc duration. In l2 dogs, outcomc *as compared u.ing , iuidog models of VF cardiac arrest 12.5 minutes and EX cardiac arrest(six). EX involved rapid aort ic hcmorrhage of two mrnutcs ro meanartcrial prcssure lcss than 25 mm Hg, and then VF by electr ic shock.Cardiac arrest no f low was 11.5 minutcs lzere 6r I2.5 minutcs(thrcc). Rcsuscitat ion was with cardiopulmonary bypass (CpB) forf ivc minutos defibri l lat ion, intcrmittent posit ivc pressure vcnti la_tion to 20 hours, and intcnsive care ,72 to 96 hnr: ir . Outcomc wascvaluatcd as <lveral l performance categorics (OpC l, bcst; S, wo.gand ncurotogrc dcfici t sc_orcs {NDS 0,.bcst; 100, worst). pupi l laryl ight ref lex rcturned in l5 minutes or 'ress in al l animari. continu-ous EEG activi ty returncd carl icr in thc VF group (36 t 20 minutesvs 52 1.12 rninutes). Al l VF dogs achicved OpC j. One EX dog afterCA no flow of I I ..5 minutes wai OpC Z. The other five EX dod;;;;OPC 3. Best NDSs were similar 136 t2.S% after VF and 31 1 6.g%after EX). Histologically, the quantity ancl distribution of ischemicneuronal changes werc the sarre. The results of this study do notsupport the hypothesis that EX is better tolerated. N";."l.gi;outcome may not be affected by the presencc or absence of blo"odstat is during ischemia.
-118 f{qlspinephrine in Hemorrhagic Shock
ll Van Ligten, GM Messick, R Neumai J Hoekstra, CG Brown/Division of Emergency Medicine, The Ohio State University,Co lumbus
A hallmark of irreversible hemorrhagic shock is inabilitv tomaintain systemic vascular resistance. Our hypothesis was that analpha-adrenergic agonist given during he-orihag. would enhancesystemic vascular resistance, maintain vital organ perfusion, and1-h_r1q nrolone survival. We studied the effects
-oi nbrepinephrine
(NE), ql alpha-1,2 beta-l-adrenergic agonist, in the early r.rrrr"ir"_tio-n of hemorrhagic shock. Ten acutely splenectomized swine {I gto 24 kg)^were hemorrhaged through a caroiid artery catheter (l mmID x 300 mm L). After 25 minutes of uncontrolled continuoushemorrhagg, a single bolus of IV NE (0.16 mg/kg) was given to fiveanimals. The other five animals served ast-'cJntrols. Data werecollected every ten minutes until death and included hemorrhage
46
rate, cardia.c index, mean arterial pressure (MAp), left ventricularstroke.work, heart rate, and systemic vascular resrstance. Norep_rnepnnne caused a transient increase in systemic blood pressuri.At in ject ion, MAP was 51 + 3 mm Hg. MAp peaked i .O t 0.3minutes af ter in iectron iMAp, l9J , r 6 mlrr Hg). Durat ion of act ionwas bnet, wrth MAp returning to control levels by five minutes.The NE group showe d a corresponding increrse irr Lmorrhage ratewith the increase in MAp; ho*.oei, total hemorrhug" u-oirr;.adjusted for weight was significantly lower in ttre Nf gr6up {33 t 2mL/kg) compared with the controls {42 t 5 ml/kg) (p < .bl ). Survivaltime was similar in both groups, (5g t 9 minutes*for controls versus.56 r I I minutcs for NEl. There were no stat is t rcal ly s igni f icant d i f_tercnccs tor cardiac index, MAp, le{ t ventr icular st roke work,systemic vascular resistance, or heart rate when compared overtimc. While NE increased MAp in this model, tt. i,ff.ct *r,transitory; no sustained effect on systemic vascular resistance wasnotcd._Despite similar survival times, those animals,...i_"! fehad a lower total hcmorrhage volume compared *ith "orrtro'i. ,idcath. This may indicate ihat NE had a 'deleter ious ef fect ontolerancc r , hemorrhagic shock. Addi t ionar s iuJies del ineat insthcsc mcchanisms and the ef fects of cont inuous inf usions of purEalpha-adrenergic agonists are needed.
119 lsosolute Comparison of Intraosseous NaCl/GoloDextran 70{, (HSD) to lntraosseous 0.9% Normal Salinein a Hemorrhagic Shock ModelJ.4 Marx, L Hanson, EE Moore, CE Wade, D Bar-Or/Departments ofEmergency Medicine and Surgery, Denver Generi l Hospital;University of Colorado Health Sciences Center, Denver; LettermanArmy Inst i tute of Research, Division of Mil i tary Trauma, SanFrancisco, Cali fornia
Wc mcasured the efficacy of N aCI 6% Dextran 20,-, (HSD) deliv_crcd by the intraosscous route in the resuscitation of li.-;;rh;i.shock. Hampshire piglets (20 to 30 kg) were anesthetized witht%hatothanc by cone mask and bled to a mean arterial pressure of30mm Hg. Intraosseous administration_ was by an 1B-gauge spinalncedle in a proximal hind iimb tibia. The animals werJran?omizedto rcceive isosolute measurcs of HSD (a mg/kg, n=5) or normaisal ine (33.3 mg/kg, n=5)under 300 mm Hg pr. ir"?.. Hemodynamicano lnetabollc parameters were determined every l5 and 30 min_utes/ respectively for 150 minutes following institution of hemor_rhage. Data (X 1 SEM were.analyzedby unpaired r tests and analysisof variance. Intraosseous delivery of HSD'was accomplished in'6.4* 1.5 versus 37.2 L Z.4 minutes for normal sal lni (p < .001).Hemodynamic variables, including mean arterial pressure, pulmo_nary capillary wedge pressure, sysiemic vascular iesistance index,cardrac lndex/ and left ventricular stroke work index (LVSWI), werenot stat isr ical ly dif fercnt at basel ine or during the intervals ofh_cmorrhage, rcsuscitation, and observation. LVSWT was greater rnthe HSD group during the initial B0 minutes of resuscitation butnot to a significant level. Metabolic indices including serum pHand lactate, hematoc.rit, oxygen delivery, and oxygen consumptronwere not^statistically dif{erjnt between the two groups at anylnjl.url; Serum sodium (149.6 t 2.0 mEqlL), osmoLlitylsil;-i4.51, and dexrran 1403.9 ! 87.0) peaked 30 minutes following ad-ministration of HSD at 6.0 t 0..3 mEq/L, 16.8 1 0.8 mOsm/Liand3!2.9 t 30.4 mg/dl above baseline, reipectively. f" , h.-o|ih"lt.shock model, intraosseous infusion of gSO'achieved fr.*oa'y_namic and metabolic improvement comparable to an isosoluiedellvery of NS. Egress of Dextran,D from the intraosseous comDart-ment was unimpeded.
120 Rapid Correction of Severe Hyponatremia Results inMyelinolysis, Brain protein Oxidaiibn, and Altered BloodChemistriesHS Mickel, PE Starke-Reed, CN Oliver/Laboratory of ExperimentalNeuropathology, National Institute of Neurologicai Disoroers anoStroke; Laboratory of Biochemistry, National Feart, Lung, andBlood Institute, National Institutes of Health, Bethesda, Maryland
Biochemical changes were studied in the brain and blo;d of ratsundergoing rapid correction of severe hyponatremia. Myelinolysishas been demonstrated to occur in the lateral corpus striatum,external capsuie, thalamus, as well as other sites in the rat brainwithin-four days following rapid correction of severe hyponatre_mia. _Using the rat model oJ electrolyte_induced myelinolysis,blood was collected from six hyponatremic rats, 1l rais on d,iy I',five rats on days 2 or 3, and_1S,on day 4 following ,rpid correction.Marked elevarion of blood cholesterol *", ,.I.n Ly day 1 andmaintained throughout day 4. By day 4 after coffection, total

protein, albumin, globulin, calcium, phosphorus, uric acid, andcreatrnine, were,all significantly elcvaied over thc hypnnrt."rrri.varues, whr le the serum. i ron levcl was s ignt f rcant iy reduced.Soluble.brain protern oxiclation was studiecl ""ri"! tf.,. i,+ ai"iii"_phenyl-hydrazine method.for assay uf prnt" in Er. lunyt ! r , rupr.oxidation o{ proteins frorn brains *.." rtl.ri.d in rour contror rats,two rats on day l, onc rat on day 2, and four rats on day + "f,"i ."pijcorrection of hyponatrcn-ria. A significant incrcase in oxidiicclDraln protelns was observed af ter rapid corrcct ion. Control animalshad 5.6 + 0.2 ( .SEM) nmols carbonyl groups per ing solublc brarnprotein. One day af tcr corrcct ic t . r , n. , in-r" ls hacl g.q t 2.7 (SEM)lm,cyls/mS
protein, | < .03. One animal two days al ter corrcct ionna.o d.z_n.rro ls/mg protcrn. Anirnals four days af tcr correct ion hacl9- I t l . l {SEM) nrnols/mg protc in, p < .0O6. A s igni f icant oxidat ivcstrcss is demonstrated to occur in the brarn f t i l lowing thc rapiJ
: : l l : - . j l i l " c . r f sr .vcrc hyponatrcmia. Thc ce l lu lar m.chrnir_sp' iu_
oucrng th ls ( )xtdat tvc stress arc not yct c lucrdatcd, but currcnt workis focusir - rg on whether thc assocratr t l rnycl inoiysis rcsul ts f rommyel in protc in and l ip id oxi tht i r rn and pe.roxi . la i ion.
.121 Cardiovascular and Neurohumoral Responses
Following Burn lnjuryRL Crum. W Dominic, J Hansbrough, MR Brown/Departments ofSurgery and Medicine, Unrversity o-f California, San-biego, MedicalCenter
Wc reccnt ly demonstratccl changcs in thc ncurohurnural rc_sponsc t ( ) bur ' in i r ry that rnay i rnpair car t l i .vascnlar funct i . ' .LarLl tovascular lunct ion ancl ncurohumoral rcsponsc wcrc cvalu-atcd in 12 pat icnts ovcr a f ivc-day pcr iod fo l l t ,wing,30,Z, to 66,1,burn injury. Hcart r:ltc, r-r-rean aiterial p."rr|-,r. {MAlr), ccntralvcnous prcsslr rc, pulmonary capi l lary wcdgc prcssurc, cart l iacol l tp l r t / systcmic vascular rcs ist : lncc, and str . lc v. luntc wcrerccorc lcd. Plasma lcvcls of ar-rg iotcnsi i * I I (A_l l ) , at r ia l natr iurct ic
l i l , i d . . l vasop rcss i n , neu r ( , pcp r i ( l c y {N py ) , r r , , r q , i n . 1 ,h r i ne 1 N E ) ,
an r t cp rncph r i n ( . wc re I ne i r sL r red . . ( ) n r hc r l l y , r [ [ r L r r r r u ] t r r r y , \ y : _tcmic vascular rcs istancc was c lcvated, ani l s t rokc volr . rmc ant lcardiac output wcrc krw. Systcrnic v, rscular rcs istancc, st r rkc
I,lJlll.l antl cartliac t,ntput nirrmalizccl by clay a,--.r""..il 1..,y .t,rf
5 .w l t nou t changcs i n cen t_ r l l vL -n ( ) r t s l ) r ess t r r c o r n t r l r r r o r r ; r r / c r r p i l ' _lary wcdgc prcssurcr MAp antr hcart rate d i t r rot crrangc. vJs.-prcssrn/ , A- l I ,
,Npy, 1,1F, and cpinephr inc lcvcls in p lasma wcrcclcvatccl on ddmlssir )n. vas.prcssin lcvcls wcrc c lcv: i tcd 50 t i ' rcsnormal on admission and rcturncd to normal by c lays 4 ancl iPlasm:r ar tcr ia l natnurct ic pcpt ic lc lcvcls wcrc nr i rmal on aclmis_sion and incrcasccl on c lays 3 to 5. Thc rcciproc:r l r " lat i , ,n.shipbctwccn systcrnic vascular rcs istancc , r ,J- ; : ; l i ; . o l r tput anclbctwccn vasoprcssin and atr ia l natr iurot i ; p"pi i , i " - . , , . . "1" tc wi thr 'ach other fo l l rwing burn in jury a,rd ,cs,- ,s t i ia t ion. Wc concludctnat i l rc c lcv: t t ron of p lasma vasoprcssin lcvcls may contr i l l l l tc totnc rncrcasc( l systcr t r ic vascular rcsponsc : rnd c lccrc:rscd carc l iacoutput and conrract i l i ty af tcr burn in jury. Aclminist rat ion of anA vl , v I rcccpror antagonist to burn in jurcd pat icnts wi l l bc uscd totcst thts hypothcsis.
!2?.The Significance of Neutrophitia in Afebrite EtdertyPatientsEA Michelson, KR Shanabrook, C Moore, M Schneider/MontefioreHospi ta l ; Universr ty of p i t tsburgh
,Ncutrophi l ic leukocytosis occurs in rcsponse to infcct ion aswc l t as o thc r phys ioJog i c s t r esses . Whr l c y r r r r nge r n i l t i r , l r r s ( ) l t e r . lnavc l c ve r assoc ia ted w i t h s i gn i f i can t i n f cc t i on . t h i c l dc r l y r nay
l-1. ] : l l ' : r rsponsc. From pat i . . "n ts pr . r .n, i ra, , , urr ' r r lu n t cac h i ng
nosplra l cmer$ency department, I00 pat icnts ovcr age 65 wcrcprospect ivc ly idcnt i f ied as having tuta i WBC above 10k and tcm_pcraturc less than 50 C. Follow.-up was obtarned from inpaticntcharts of
-admitted patients and by phone inf"r"i.- u{ .li.chrr;;Jpatrents. Ninty-six patients had-completc records, thc average agcwas 7[3, thc mean WBC was. 13.9; l6 patients had total ncutropliii
:?:l!: 1:r. than ti,000, and werc "ril.,dc,l fru,r, f.irihe, nrrty.ir.!q1t f ; , * pcrccnr of pat icnts wirh ncurrophi l ia were admirred, 4rrto thc f Ioor and 2 I at lm i t tcd or r ransfcrred io an ICU. Twenry Srv( .n{34%)had an infect ion idcnt i f ied, but oniy 52o/o wereidcnt i f ted inthe ED. In absence of an infectious etiology, -rr-,y pnri"r-,,. still hadsigni f icant d iscase. These includt d l4 l I ' i "k) wi t i r 'acute cardiopul_monary diseasc, and 19 124%) with other significant known causesor ncutrophr l ta; a l l but one of these pat ients werc admit tcd. Of theI 7 rernaining patients, I I had sevrre pain as the only cause ol thcirneutrophilia and 82% were admittc j. No t tiology lor neutophiliawas identificd in six patients; howcver, threJ'were adrnitted.
Among pat icnts wi th infect ion, the diagnosis was apparent onchest radrograph in 307o; ur inalysis, ( t3,%i i r lood cul turcs, 'Lt%, Jf ;t issuc cxaminat ion, 15,o/ .1
^and sputum a\one, 7ok. Ainong'd is_charged pat ients, two ( lg%) weie subsequeni ly iound to havesigni f icant pathology; f .ur (3(r%) could not be contactcd af tcrmutt lp lc at tcmpts. Wc concluJc. that nul t rophi l ia in thc c ldcr lyafcbr i lc ED pat icnt identr f i r ,s a h_igh_r isk pupr l r t iu, - , . Thcsc pa'_t lents mcr i t carcfu l workr-rp {or infect ic lus as wcl l as other ser iouscl iscasc, ideal ly in an inpat icnt sct t ing.
123 Oral Labetalol Versus Oral Nifedipine inHypertensive Urgencies
!,1 lltcOon.a.!a, DM yealy, S Jacobson/Division of EmergencyMedicine, University of pit tsburgh Aff i l iated Residency inEmergency Medicine; Section of Emergency Medicine, Hospital ofthe University of Pennsylvania. pit tsbuigh
r nc.pv_rn hypertcnsivc urgencics has bccn n'ruch dcbatcd anclcornpl icatcd by thc sidc cffccts of avai lablc agcnts. In a prospcctivc,randor.nizcd, opcn-labcl study, wc ., , ,- ,rpnr", i thc usc in thc cncr_gcncy dcpartnrcnt of rral labctar. l , an alpha-bcta brockcr, with r lralnifcdipinc in hypcrtcnsivc urgcncics. paticnts with diast. l ic bloriJl lrcssl lrcs {DBP) .vcr 120 r.nm Hg wh. did n.t havc crrrcrra t.r :rl l V | ! r t e n \ r v ( c n l L r g e n e v W r . r c r - l i H i h l u . T h c J r t r g s w U r u g , l v ( n i l . t i ll { r ; l ( l i l l A l ; l s l I ( ' n w t t h r i r r s l 5 - r n . , t r r r r r n g b i r s e J o n t h c i r r r , 5 p ( . c t i V rphan lacok inc t ics un t r l : t D l lp o f I l0 n rg Hg was ob ta incd . E i thcrlabctakr l 200. 'g in i t ia l ly and a rcpcat a, i r " , i i roo t .200 r .ng at tw.hours.c lcpcnding on thc DBp, or n i f "d ip in" f O nrg f r l t . ar . rc l swal lowe vcry hour to a tota l dosc of 20 ntg was givcn. Aclcquatc contro l w: lsdcf incd as a I ) l lP. f I I 0 m nr Hg acl l icvcci .v. r" l r . r iud n, , , " " . ""a i , igfour.hours. Tcn pat icnts wcre cnrol lcd in cach grotrp; thcrc was nr is igni i icant c l i f fcrcncc in age, scx, racc, or i . . , i . t< i ry, , f previoushypcrtcnsion. Of thc 20 pat icr- r t r , l13 rcsl -urrr t lcd wi t l i no s ignf icai r id i f fcrc_ncc bctwce n groLl [s. Thc nrcarr t imc t . c ' r - r t r . l wi th I : ibctaLr lw l s 62 .5 m inu t cs , and w i t h n i f cd i p i nc was ( r 0 .0 n t i nu t cs { p = NS) .Thc nrcan_prrctrcatnrc l t t prcsslr re f t l r labctalo l was I95/ I22, . , . ,n, igand f r r r . n i f cd i p i nc was j ( ) g l l } g n rm Hg {p = NS) , wh i ch c l ec r casc ito Jn i f f tcr . t rcJrnt .cnt ,pr .e.ssl l rc for labcia io l of l54l lO{) nrnt Hg andIo r 11 ; . 1 . . 1 | [ r , r " r r f 16 ,3 / l fX ) r r r l Hg (p = NS) . Thc r . ncan dcc r c : i s c t nsystr r l rc / t l i r rs to l re h loot l prcssr l rc wtrs 42.6 f 26.5 rr r .n Hg wi t I labcta_t r ) t i l nd , J4 .9 /28 , . 4 n t n r Hg w i t h n i f cd i p i nc ( p = NS) . Mcan pu l se ra t c( lurreasc( l s tx l ) tdts l )er ut i l tutc wi th labctalo l and Ono bcat pcrn l i nu t c w i t h n i f cd i p i nc { 1 , = NS) . T l r c r l c rn c l osc o f l abc tak r l was212 n rg . a r r t l l 2 r ng w i t h n i f cd i p i r - r c , w i t h t hc r l c t l i an dosc o fI i lhctd t ( ) l hr i .g 200 ; r r r r l n i fcc l ip i 'c l 0 ntg. N. s ignrf icant s idc cf fcctsoccurrct l wj th c i thcr drug. Wc concl . ,c ic that r l ia l lu l r " t r , l . , l g iu. . - .s ' r . . th rct luct i . r . r i r - r b l . .d prcssLrrc ovcr : ln acccptablc pcr i .d ' ft i r . r c f . r E l ) usc a ' c l i s an a r t i r na t i v c t . . r a l n i f cd i p i nc i ' r i ypc r t cn -s ivc urgcncics.
'124 Cardiovascular Side Effects of Emergencylntravenous Phenytoin AdministrationPJ Donovanlleritage Hospital, Tarboro, North Caroilna,
E r r c rguncv IV phc ' y t . i n ad r r i n i s t r a t i . n i s a we l r - cs tab l i shcdtncr: tpy l (Jr p: l t iu l t ts wi th acl l tc rcpot i t tvc scizurcs and/or status cp_i lcpt icus. Prcvior . rs studics sr-rggcst that c. r r t inu, ,ur ' tV inf . , r iun ufphcr-ryto in achic.vcs rapid thcr ipcut ic lcvcls wi th minimal .u.r lp l i_cet ions. Rates of phr.nytoin infusion vary and r isks to pat icnts wi thKn{rwn c: l rL l tovascular d iscasc l ravc n<t t bccn asscssccl . Forty_twoFir t i rnts were. cv l lu; r tc t j prospcct ivc ly to stucly thc carc l ic lvasculars- ldL 'et tucts t r l l5 mg/ l<g of phcnytoin by cont inuous iV infusion.Pa t i en t s ,w t ' r u t l i v i J , . d , g roup I cons i s rU r l o I pa t ren t s j ess t i r an 5 ( Jvcd f s o l d w t t h ( )u l J l hc f ( r sc l L . r o t i c h t . i t f t r l l s t . i t s r . ; F r { ,Up 2 c r rns i s t t . r l
: l f :1 l i ' ' ] " 1 ' " rc than 50, vcars o ld.or anv indiv i i l i ia l wi th a h istory
ot athcroscl t rot ic hcart d iscasc. Infusion ratcs werc 50 rng/min ani2s
3tx/rn11, ruspccr iv l ly . pat icnts
_exper icncing braclycaid ia, sec_r)nr t - { r r th l rd-d(grr( hcart b lock, hypotcnsion, or a icohol wi th_drawal sc izurcs wcrc cxcludcd. Cardiac rhythin str ips ancl v i ta ls igr- ts wcrc obtaincd bcfore t reatmcnt ancl at l5_rninute intcrvalsunt i l onc hour af tcr infusion. No pat ient in group I (26) cxpcr iencedbradycardra, hypotcnsion, or .widcnrng ni 'qnt c iunng in lusion.Two pat icnts in group 2 (1(r) bccanre [ypotensivc (sysio l ic b looJpressurr . 100 nrrn Hg) dur ing infusion, ind one of thesc pat ient ;c levr- l .pcd a junctronal rhyth ' - r at a ratc of 50. Thcse s idc ef fcctsrcsolved wi th in onc hour af ter infusion. No pat ients dcvclopcd sei_zurcs af ter phcnytoin adrnin ist rat ion and blood rcvcrs werc thera-pcut ic . Sclect ivc administrat ion rates of phenytoin, brr .d orr rg land. h istory of atherosclerot ic hcart d iseasc ar" . f l i . " . iur l r , snf . , n.dwi thout s igni f icant cardiovascular s ide cf fects.
41

125 Supraventricular Tachyarrhythmias and Rate-Related Hypotension: Cardiovascular Effects andEfficacy of Intravenous VerapamilBE Haynes, JT Niemann, KS HaynesiUOLA School of Medicine;the Department of Emergency Medicine, Harbor-UCLA MedicalCenter, Torrance, California
Intravenous vcrapamil is the pre{erred agent for the acutc man-agcmcnt of supraventr icular tachyarrhyhmias lSVT) in the absenceof contra indicat ions to i ts usc. SVT compl icated by hypotensionhas been considered a contraindication; howcver, the efficacy of IVverapami l in thc managcment of rate-re lated hypotension has notbecn speci f ical ly addressed. The purpose of th is study was to assessthc effccts of IV verapamil in patients with SVT and artcrial hypo-tension. A retrospect ivc and prospect ive study dcsign was used. In-c lust ion cr i ter ia werc SVT (QRS durat ion < 120 ms, R-R intervalrcgular or i r regular) ; a QRS rate > 140/min; systol ic b lood pressurc(SBP) of 90 mm Hg or lcss; and a normal mental status. Weidcnt i f icd 21 cpisodcs of SVT mect ing inclusion cr i ter ia in l9pat icnts. SVT was duc to AV node reentry in 17, atr ia l f ibr i l la t ionin thrcc, and atr ia l f lu t tcr in onc. Thcrc wcrc scvcn mcn and 12women, mcan agc 52 +).7 years l t SDl. SBP pr ior to vcrapami l was70 + 2U mm Hg and QRS ratc 192 + l9/minutes. IV calcrum was notadrnin istcrcd before verapami l therapy. Af ter IV verapami l (6.5 +4.3 mg), a posi t ivc rcsponse (conversion to s inus rhythrn or vcn-t r icular ratc < 120) was notcd in l7 of 21 cpisodes ( t |0%,) . Post-t r ca tmen t SBP i nc r cascd t o 98 t l ( r mm Hg {1 r . . 005 ) andvcntr i cular rcsponsc rate decrcascd to I 12 x 39 (1, < .00 1 ) { two-ta i lcdpaire d t tcst) . In only onc study cpisodc (5 % ) was vcrapami l thcrapyfol lowcd by a decrcasc in SBP and no changc in vcntr icular rcsponseratc. Wc conclude that IV vcranami l is a safc and cf fcct ivc drue forthc r t ranagcmcnt of SVT c,rmpl icatcd by ratc-re latcd ar tcr ia l hypo-tcnslon.
.126 Efficacy of Pseudoephedrine in the Prevention ofMiddle Ear SqueezeM Brown, J Krohmer, JS Jones/Department of EmergencyMedicine, Butterworth Hospital, Michigan State University Collegeof Human Medicine, Grand Rapids
Middlc car sc lucczc {barot i t is mcdia) is thc rnost common rypeof barotrauma among scuba divcrs. Thc pain is substant ia l and maycausc tympanic mcmbrane hcmorrhagc or rupturo. Prcvious stud-ics havc shown that dccongcstants may rcducc custachian tubcblockage and al low cqual izat ion of middle ear prcssurc. Thc pur-posc of th is study was to dctcrminc thc ef f icacy and safcty ofdccongcstant prophylaxis among f i rs t - t imc scuba divcrs in thcprcvcnt ion of rn iddlc car squeezc. A prospcct ivc, doublc-bl ind t r ia lwas ccrmplctcd wrth 24 voluntccr scuba divcrs rccciving cither 60rng pscudoephcdrinc or placcbo. Following randomization, tablctswcrc administcred to each subjcct 60 mrnutes prior to diving. Signsand symptorns of middle car squeeze then were recorded. Theotoscopic appcarance of the tympanic membrane was graded ac-cording to the amount of hemorrhage in the eardrum, with gradesrunning from 0 (symptoms only) to 5 (gross hcmorrhage andrupture). Ear parn, tinnitus, and/or decreased hearing wcre prcscntin 14u1, ( two of I4) of those receiv ing pscudoephedr ine versus 40%(four of ten) of the control group. This diffcrence was statisticallys igni f icant using Fishcr 's exact test (P < .O25). Of those divers wi thcar pain, t33% (f ive of s ix) had evidence of barotrauma to thetyrnpanic membrane (mean score, 1.4). No srde effects were cn-countcred. These results suggest that usc of an oral decongestantprtor to diving may decrease the incidence of middle ear squeeze.
127 Safety Assessment ot High-Dose NarcoticAnalgesia for Emergency Department ProceduresWG Barsan, D Seger, DF Danzl, LJ Ling, R Bartlett, C Bryan/University of Cincinnati Col lege of Medicine, Cincinnati , Ohio;University of Arizona College of Medicine, Tucson; University ofLouisvi l le School of Medicine, Louisvi l le, Kenlucky; HennepinCounty Medical Center, Minneapolis, Minnesota; RichlandMemorial Hospital, Columbia, South Carol ina; Kendle ResearchAssociate, Cincinnati
Despite the availabiltiy of potent opiate compounds for therelief of pain, studies suggest that patients are undermedicated forthe degree o{ pain experienced. Fear o{ dangerous side effects, suchas respiratory depression, is an important lactor, We per{ormed aprospective trial in 70 patients evaluating the safety of high-dosenarcotic analgesia in emergency department patients undergoingpainful procedures. Mean patient age was 3l.l years (range, l8 to63). Each patient received meperidine 1.5 to 3.0 mg/kg by slow IV
infusion over l5 minutes prior to the painful procedure. Vital signsand alertness scale were performed prior to analgesia, after analge-s ia, and at 15, 30, 45, 60,90,120, 150, 180, 210, and240 minutesafter the procedure. Values from all time intervals were comparedwith bascl ine using Duncan's tcst for mul t ip le compar isons. Themean dosc of meper id ine was 2.5 rng/kg (173 mg). Al though therewere statistically significant differences in all parameters betweenbaseline and analgesra, there was little clinical significance in thediffferences. Mean respiratory rate was nevcr lower than l7 breathsper minutc, and mean systolic blood pressure was nevcr below 122mm Hg. The nadir in pulse rate was 72 bcats per minute. The lowestrespir tory rate at any t ime in any pat ient was ren, and no pat ientrcquired ventilatory assistancc or reversal with a narcotic antago-nist. No patient required fluids or drug treatment for hypotensionor bradycardia. Although paticnts were notably sedated, the lowestlevel of a ler tness in any pat ient was l0 out of 25 (0, unresponsive,25, totally alert). A11 patients wcre safely dischargcd after the four-hour observation, and a follow-up visit in 24 to 72 hours in allpatients rcvcalcd no significant late side cffects. We conclude thathigh-dose narcotic analgesia can be safely givcn in the ED prior topainful procedurcs without untoward stde cffects.
128 Intranasal Butorphanol for the Treatment ofModerate to Severe Musculoskeletal PainJ Scott, M Smith, R Shesser, R Rosenthal, J Smith, J Peterson, KGhezzi, C Feied, M Hunt, M Bourland, S Sanford/Department ofEmergency Medicine, George Washington University MedicalCenter, Washington, DC
Sevcre musculoskclctal pain is a problem faced frequently incmcrgcncy care. Treatmcnt options for such patients are limitedand includc oral narcotics, with a relatively slow onset of action, orparentcral narcotics that rcquire a physician visit for administra-tion. Aiternativc treatment modalities are needed for the manage-ment o{ such patients. We performcd an open label study of theeffcctivcncss and safety of intranasal butorphanol for the treat-mcnt of pain resulting from musculoskeletal injury. Thirty adultpaticnts with musculoskelctal pain deemed to be severe enough towarrant parenteral narcotics were administered two intranasaldoscs (0.5 mg/dose) of butorphanol. Pain relief was graded by thepatient at regular intervals during a three-hour period of observa-tion. Patients were remedicated as needed every 30 minutes to amaximum dose of 3 mg. Ninety-seven percent of patients obtainedsatisfactory pain relief with intranasal butorphanol 53 % ( I 6) withinfive minutes and 87"h {26) within 15 minutes of administration.Onc patient required supplemental intramuscular meperidine. Nomajor sidc cffects were noted, but mild sedation occurred in 70%of thc patients. Intranasal butorphanol appears to be effective,rapid, and safe when used to relieve moderate to severe muscu-loskeletal pain. Controlled studies comparing intranasal butorpha-nol to standard parenteral narcotics are indicated.
'129 Exposure of Emergency Medicine Personnel tolonizing Radiation During Cervical Spine RadiographyCM Singer, LJ Baraff, SH Benedict, EL Weiss, BD Singer/TheEmergency Medicine Center, UCLA Medical Center; The UCLARadiation Safety Office; The UCLA School ol Medicine, LosAngeles
We studied the potential hazard of ionizing radiation exposureto health care workers (HCWslwho routinely stabilize the necks oftrauma patients during cervical spine radiography. A clinical traumamodel was developed using a RANDO Phantom@ artificial torso tosrmulate an actual patient. A radiation monitor was placed atpositions of a simulaled HCW's fingers, hands, arms, and thyroidgland, and standard cervrcal spine radiographs were taken, Theexposures to the finger positions were repeated with the monitorinside a 0.5-mm lead equivalent glove. The mean exposure to thefinger for a single cross-table lateral radiograph was 174.5 mrem.The use of leaded gloves reduced this exposure to 0.3 mrem (99.9%).For a single series of lateral, AP, odontoid, and swimmer's views,the total mean measured unprotected exposure to the finger of thehand position nearest the radiograph tube was 581 mrem and230mrem to the finger of the opposite hand position. If these simulatedexposures are rndicative of actual patient situations, an HCW whoholds the head of a trauma Datient four times each week withunshielded hands would receive greater than twice the maximumallowable annual occupationai radiation exposure to the extremi-ties recommended bv the National Council of Radiation Protectionand Measurements. We conclude that HCWs who routinely stabi-lize the neck of trauma patients during cervical spine radiography
48
may incur a radlat ion exposure r isk, and that 0.5 mm lcad equrva-lent gloves provide an effective barricr to ionizing radration.
130 A Radiographic Evaluation of Various Methods ofAnkle lmmobi l izat ionJ Scott, C Martin, E Jacobs, C Miller, R Shesser, R Walls/Departmenls of Emergency Medicine and Radiology, GeorgeWashington University Medical Center, Washington, DC
Acute ankle sprarns are among thc most frequently sccn prob-lems rn the emcrgency departmcnt. Al though the managcmcnt ofthesc in jur ies is controvers ia l , thc standard o{ care in most cmer-gcncy set t ings is immcdiatc i rnrnobrhzat ion, rcst , ice, e levat ion,and orthopedic refcrral. Several mcchanisrns cxist for irnrnobiliza-t ron of in jurcd ankles, and the preferred mcthod var ies arnongemcrgency pract i t ioners. This study was performcd to radiographi-cal ly evaluatc a layerecl bulky (Joncs) drcssing, a p lastcr postcr iorspl int , and a plastcr sugar tong or st i r rup spl int for therr abi l r ty toI imi t thc most lmportant mot ions of thc in jurccl anklc p lantarf lex ion ancl invcrs ion. The studv was pcrformcd on tcn adul t r .nalcvoluntccrs wi thout antcccdcnt anl<1, : path,r l , tgy. A hascl inc latcralradiograph of the ankle was obtaincd at rcst and in rnaxir.nal plar"rtarf lex ion. Af tcr appl icat ion of cach of thc spl ints, rcpcat radiographsin r-r-raximal plantar flexion wcrc obtaincd to dctcrminc thc arnounto{ mot ion al lowcd by cach spl int . This proccclurc was rcpcatcd inthe antcr ior-postcr ior p lanc wi th maxirnal invcrs ion at bascl incand whi le wcar ing cach o{ thc spl ints. Thc bulky drcssing al lowccl94ok oI plantar flexion and [.i5'2, of invcrsion; thc postcriur splinta l lowcd 90% of p lantar f lcx ion ancl 70% of rnvcrs ion; : rnd thc sugartong spl i r - r t a l lowcd 80% of p lantar f lcx ion ancl 59"1 ' of invcrs ior . r .Only thc sugar tong splnt dcmonstratcd a stat is t ical ly s igni f icantdccrcasc in anklc movcmcnt (P < .001 ) . I f maximal immobi l izat ionis dcsircd for thc managcmcnt of acut t 'anklc s l ra ins, thc sugar tongspl int is prcfcrablc to thc postcr ior spl int or bulky c l rcssing.
-131 Radial Artery Catheterization of Crit ically l l l Patientsin the Emergency DepartmentG F Bachhuber, D W Plummer, M Lutze, E Ruiz/Department ofEmergency Medicine, Hennepin County Medical Center,Minneapolis, Minnesota
Thc succcss and cornpl icat ion ratcs of radia l ar tcry cr thctcr iza-t ion in contro l lcd, c lcct ivc sct t ings arc wcl l documcntccl ; howcvcr,thcrc is no prospcct ivc study cxamining tho ol l tcomc of cmcrgcncydcpartmcnt radia l ar tcry cathctcr izat ion in cr i t ical ly i l l pat icnts.This study dcscr ibcs thc s l roccss and cornpl icat ion ratcs of racl ia lar tery cathctcr izat ion in cr i t ical ly i l l cmcrgcncy dcpartmcnt pa-t icnts. Wc prospcct ivc ly studied 1 26 consccLl t ivc pat icnts unclcrgo-ing attcn-rptcd radial artcry cathctt:rization ovcr a onc-ycar pcriocl.Success ratc and ratcs and naturc of imn-rcdiatc ancl dclayccl com-pl icat ions werc dctermincd. Each pat icnt was cxamincd c la i ly ur-r t i lc i ther cathetcr d iscont inuat ion or dcath. Dur ins thc wcck fo lkrw-ing discont inuat ion, surv iv ing pat ients undcrwcnt scr ia l physicalcxaminat ions. Thosc wi th cvidencc of ar tcr ia l thrombosis bascd onthe Allcn's tcst underwcnt Dopplcr flow str.rdics for confirr-nation.Onc hundred twenty-s ix pat ients undcrwcnt at tcmptccl ar tcr ia lcathetcr izat ion. Six d icd dur ing resusci tat ionr howcvcr, ar tcr ia lcathctcrs were establ ishcd in I 12 of the rcmaining 120 pat icnts fora success rate of 931o. Forty- four
, .34.1)%) sustainccl inmcdiatc
minor compl icat ions, inc luding inabi l i ty to thread thc wirc ( {or thcSeldinger techniquc) in 16 pat ients 112.6" l ' ) and inabi l i ty to thrcadthc catheter in 13 (10.3%). Of the l12 pat icnts adr-r- r i t tcd to thchospital, 32 survivcd at lcast 24 hours. Dclaycd mir-ror complica-tions included insignifrcant blccding frorn thc punctlrrc sitc in I3ol 32 1a0.6%) pat icnts, ecchymosis in threc (9.3%), and localinf lammat ion in f ive {15.(r%) pat icnts, and nine 128.1 ' l , l dcvclopcdarterial thrornbosrs after cathcter cliscontinuation. No paticntsuf fered ischcmic t issue 1oss. Fivc pat ients 115.6 ' / " ) had ar tcr ia lcathcters cultured bascd on clinical suspicion of infection. Therewere two positive catheter culturcs, but neither patient dcvclopcdcatheter-rc lated sepsis. No major cornpl icat ions occurrcd, thusconcluding that radial artery cathctcfization is a useful and safcprocedure in the ED resuscitation of critically ill patients.
ORAL PRESENTATIONS132 Emergency Department Diagnosis of EctopicPregnancyT G Stoval l ,A L Kel lerman, F W Ling, L Gray/Departments ofObstetr ics and Gynecology, and Medic ine, Univers i ty ofTennessee, Memphis
The rate of ectopic pregnancy (EP) in thc Uni ted Statcs has in-crcased four{old s incc I970. To asscss thc accuracy of thc h istoryand physical examinat ion for detect ion of EP, we ident i f icd al lwomcn prcscnt ing to our cmcrgcncy departmcnt wi th a posi t rveur inc prcgnancy tcst {UCPI bctween fanuary I and Deccmber 31,I 988. Al l pat ients wcrc in i t ia l ly seen by thc ED residents or facul ty.Gynccologic consul tat ion was avai lablc on rcqucst . Serum progcs-tcror-rc (P) and c luant i tat ivc hur.nan chor ionic gonadotrophin (hCC)lcvcls wcrc obtaincd in a l l cascs whethcr thc Dat lcnt was dis-chargcd homc or admrt tcd for fur thcr evaluat i , in . Resul ts wcrcavar lablc by 2:00 PM thc fo l lowing day. Al l d ischargcd pat icntswcrc givcn fo l low-up appointments wi th in two wccks; thosc for-rndto havc a P lcss t l - ran 25 ng/ml wcrc cal lcc l to rcturn immcdiatelyfor a t ransvaginal u l t rasound and/or laparoscopic cxaminat ion andtrcatccl accorc l ing to : rn cstabl ishcd protucol . Dur ing thc studypc r i r r r l , l ( r l o f 2 , 157 ED pa t i cn t s w i t h a pos i t i v c UCG (7 .5 ' l . ) wc rcul t imatc ly founcl to havc an EP. Al l but f ivc had P lcss than 25 ng/rrL {scnsi t iv i ty ;97
"1) ; fot t r of thcsc f ivc had bccn adnt i t tcd for i rn-mcdiatc lapir roscopy c luc to syntpton-rs. Ovcral l , EL) physic iansclctectccl lJ9 of l ( r l cascs ( scnsi t iv i ty , 55.3 '2, ) on in i t ia l prcscntat ion,5.1 of which (60'2,)wcrc rupturcd at thc t intc of surgcry. Scvcnty-two EP pat icnts 144.7"1,) wcrc tholrght to havc bcnign c l rn icalprcscntat ion and wcrc scnt homc, inc luding 4l wi th vaginal b lccd-ing thor. rg l ' r t c luc to thrcatcncd abort ion. Ninc of thcsc 4l had bccnclcarccl by a gynccokrgy cunsul tant pr ior to d ischargc. Al l Z2 wcrcnotcd thc fo l lowing day to havc a P of lcss than 25 ng/mL ancl wcreaskct l to rcturn. Eig l r t of thcsc p:r t icnts wcrc found to have arLl l l turccl EP pr ior to th is fo l low-up cvaluat ion. EI) physic iar"rsrccorc lcd abscncc of an adr. rcxal l r : lss or tcndcrncss in 90'X, ofd ischargccl cascs, and tkrcumcntat ior-r o l c l in ical r isk facturs wasincon rp le t c i n 55 o f 72 cascs 176 .4 "1 , ) . Howcvc r , on l y 9 l o f l ( r lp: l t lcnts { .56.5 '2,) wi th EP ackr-rowlcclgcd onc or r lorc r is l< factors onfol low-up quost ioning. Wc conclut lc that thc standard histury andphysical cxaminat ion ( inc luding thosc pcrforr .ncd by consr. r l t ingspccia l is ts) arc insuf f icrcr-r t ly scnsi t ivc for car ly dctcct ion of unrup-turcd EP. EDs wi th h igh ratcs of EP should strongly consic lcrr-n. t ivcrsal P scrccning : rncl usc of fo l low-up algor i t l - r rn to dccrczrscLrnncccssary pat icnt n-rorbic l i ty and thc r isks of ntor ta l i ty c luc tu un-r l iagnoscci cctopic prcgnancy.
133 Mortality and Morbidity Following the 1988Earthquake in Soviet ArmeniaE K Noji lDepartment of Emergency Medicine, The Johns HopkinsHospital and School of Medicine, Baltimore, Maryland
An carthcluakc rcgistcr ing (r .9 on thc Rrchtcr scalc h i t thcnorthcrn part of thc Armcnian Rcpubl ic of thc Sovict Union onDcccmbcr 7, 1988, rcsul t ing in thousancls of dcaths and in jur ics.This study was undcrtakcn to dctcrrn inc carthquakc-rc latcd in jurypat tcrns and scvcr i ty ; to asscss factors : rssociatccl wi th surv ivalvcrsus dcath; ancl to idcnt i fy thc r -nost appropr iatc typc and t i rn ingof rcscuc. Thc study drcw or-r a populat ion-bascd survcy of thrcctowns scr iously af fccted by thc carthcluake. Data col lcctcd on s i tcby thc author dur ing thc pcr iod immccl iatc ly af tcr thc carthquakcwcrc obtainccl f rom f ic ld survcys of t l - rc dcvastated towns, d i rcctintcrv icws wi th surv ivors and of f ic ia ls of thc Arrncnian Minist ry ofHcal th, and data col lcctcd by the Div isron of Informatron Systems,Anncnian Minist ry of Heal th. Dcaths wcrc ( r8 t rmcs and in juryratcs sevcn t i rncs highcr in t rapped than in nontrappcd v ict tms.Thc possib i l i ty of escape was crucia l for surv ival and depended onthe typc of bui ld ing and occupant escape behavior . Eighty-ninepcrccnt of pcrsons found al ive werc rcscued dur ing the f i rs t 24hours. Most of thc in i t ia l rescue work and mcdical rc l ief was tota l lydisorganized and carr icd out cntrre ly by unpreparcd local people.The f i rs t outs ide assistancc f rom Soviet author i t ies d id not arr ivefor 24 hours. No ir-rternational assistancc was available for severaldays. Crush syndrome due to l imb comprcssion became a majorproblcm, wi th 23 pat ients developing acLrte renal far lure requir ingdialys is. Bccause al l hospi ta ls rn the region wcrc scverely damaged,these pat ients wcrc t ransfcrred to hospi ta ls in una{fcctcd parts ofthe country or to ncrghboring Soviet Georgia. Analysis of the datasuggcst that the emergency phasc {or medicai care wrth few excep-
49

tions was limited to the three to four days after impact. These
results point to the importance of well-organized local disaster pre-
oaredness capabilitieJ because outside assistance will invariably
arrive too lati for effective life saving.
134 Analysis ot Emergency Department Management ofSuspected Bacterial MeningitisD A Talan,J J Guterman, G D Overturf, C Singer, J R Hoffman, BLambert/Olive View-UCLA Department of Emergency Medicine,UCLA School oJ Medicine, Sylmar, Cali iorniat
Previous studies of emergency department management of bac-
terial meningitis have indicated that thcre are often long delays
or ior to in i t rat ion of ant ib iot ics. This study was to determine i f
dclays were related to specific aspects of patient management' We
rctrospcct ively reviewed { 198 I to 1988) thc medical . rccords of 122
pat ie; ts pr imar i ly evaluated in the ED and admit ted for suspected
tractcr ia l 'mcni . tg i t i t r t a univers i ty (55)and community (67) hospi-
ta l . The median t ime f rom ED registrat ion unt i l in i t ia t ion of
ant ib iot ics { t imc to ant ib iot ics) + SD was 3.0 t 2.5 hours ( range, 0 5
to l8 hours) . The t ime to ant ib iot ics was not s igni f icant ly re latcd
to thc t ime of ED registrat ion; ( )0"1, of the tota l t imc to ant ib iot ics
occurrcd fo l lowing the in i t ia l physic ian cncolrntcr ' T imc to ant ib i -
ot ics (mcdian t SD) was s igni f icant ly (1 ' � < .00005) greatcr for cases
in wlLich computed tomography scan and/r l r laboratory analysis of
ccrcbrospinal f lu id preccdcd in i t iat ion of ant ib iot ics comparcd
with cases in which ant ib iot ics administrat ion was not cont ingcnt
on thc rcsul ts of thcse proceclurcs 14.3 !2-8 hours vcrsus 1 '9 t l 9
hours, respcct ivc lyJ. Also, t ime to ant ib lot ics (mcdian t SD) was
signi{ icani ly (P . .00005) greatcr for pat icnts in whom ant ib iot ics
wcrc in i t ia ic i l on the ward as opposed to thc ED (4.5 + 3 2 hours
vcrsus 2.2 + 1. .5 hours, rcspect ivc ly) ' We concludc that in thc ED,
krng dclays cxist bcforc in i t iat ion of ant ib iot ics for cases of sus-
pcctcd bacterial rncningitis and that in gencral thcsc dclays appcar
l l be physic ian gcncraicd and to a grcat extent potent ia l ly avoid-
able.
135 Ciprofloxacin in the Treatment of Acute InfectiousDiarrheaML Neighbor, PT Cohen, D Seigel, M Newman, W Hadley' D Yakjo'O Feigal, H Larkin, MA Sande/San Francisco General Hospital 'University of Cali fornia, San Francisco
Thc cmpir ic trcatmcnt t l f acute diarrhca rcmains problcmatic in
that fcw antibiot ics cradicate al l of the commonly encountercdcnteric pathogens. Wc havc comparcd thc cf{icacy and safcty ofciprofloxacin ibF), a new quinolonc dcrivativc, with trimethoprirn/sulfamethoxazolc {TMP/SX) and placcbo in the trcatmcnt of acuteinfcct ious diarrhea. Onc hundrcd thirty-four adults prescnting tt l
thc San Francisco Gcncral Hospital emcrgcncy department com-plaining of diarrhca *"rc ctttolled in a- prospective, randomizcd,ilo.rl-rl"-bhn.tcd studv. A total of 5tl stool pathogcns wcre obtaincd:30 Campylobttcter, 22 Shigella, three Salmonella, two Yersinia'and t*<','A"romonns. Aftcr four days of trcatmont, CF successfullycradicated the stool pathogcn in 94"k of paticnts compared with60"1, [r:r TMP/SX, and 37y" {or placebo. Paticnts kept daily diaricsrccorcling thc sevcrity of their diarrhea, nausca, abdominal pain,
and fcvcl. Fifty percent of culturc-positive patients were well byclay 3 whcn treaied with CF compared with-day 4.5 and 5 0 whentreated with TMP/SX and placebo. CF was also superior to both inreducing abdominal pain and was well tolerated. These results, aswell as'the increasing incidence of TMP/SX-resistant Sfi igel la,suggest that CF should be considcred a drug of choice in the cmpirictreit-"ttt of acute in{ectious diarrhea'
136 Evaluation of Women With Possible AppendicitisUsing Technetium'99m Leukocyte Scan_PL He-nneman, TA Halt, CS Marcus, JA Butler, T Koci' N Worthen,ES Wilson/Department of Emergency Medicine; Division ol Nuclear
Medicine; Departments of Surgery and Radiology, Harbor-UCLAMedical Center, Torrance, Cali fornia
We evaluated the use of technetium-99m albumin col-loid while blood cell scan (TAC-WBCJ in women with possible
appendrcitis. One hundred nine women {mean age, 28 5 years;
ringe, S to 80) underwent I 10 TAC-WBC scans. Twen-ty-six womenhad'lristologically proven appendicitis, ten 139%) of whom had aperforated alppendii ut sutgery. Women with-appendicitis di{ferediro- -o-.tt-*ithout appindicitis only in- the frequency of pain
migration from the periumbllical region to the-right.lower quadrant(RiQ) (42% versus22Yo, respectively, P = O49l and anorexia {88%u..t.t.'ZZf , respectiveiy, l' = .OOO:41, there were no differences
with respect to age, duration of symptoms, temperature, .RLQtenderneis, RLQ rebound, cervical motion tenderness, rectal ten-
derness, or white blood cel1 count. TAC-WBC scan was indetermi-
nate for appendiceal pathology {abnormal, but nondiagnostic) in 52
women 147"t ), ntne of whom had appendicitis. Fi{ty-eight scans
werc read as positive or negative for appendiceal pathology' There
wcre I6 true-positives, frve false-posrtives, 36 true-negatives/ and
onc false-negative, resulting in a sensitivity oI94"h, aspecifrcity oI
88%, an aci racy.of 90%, i posi t ive predict ive value of 76"/o, and
a negative predictive value of 97"k. Overall, the TAC-WBC scan
was abnormal in 96"/" 125 oI 26) o{ the women with appendicitis'
The rnain value of TAC-WBC scan in women with possible appen-
dicitis is its high negative predictive val'te 197%), and the main
oroblem with the TAC-WBC scan is its high indeterminate rate
iql'k). x subgroup of 24 women also underwent graded compres-
sion ultrasound, ten of whom had appendicitis. Eleven of these
women l4(t%l had indeterminate TAC-WBC scans and ten had
indeterminatc u l t rasound (42%). TAC WBC scan was more sensl-
t ivc (100% vcrsus 25%, respect ively, P = .018), equal ly sp9! i f i9
{80% versus 70%, respect ively, P =.1) , and more acutrate \92"hvcrsus 577o, rcspectiv;ly, P = .0481 than ultrasound in diagnosing
annendicitis in these select women. Further study is needed to
de'iermine the role of TAC-WBC scan and ultrasound in women
with possib le appendic i t is .
137 Mathematical Modelof Psychosomatic Symptoms inthe Practice of Emergency MedicineR R Huang, B White/Olfice of Medical Education Research andDevelopment, College of Human Medicine; Section of EmergencyMedicine, Detroit Receiving Hospital and University Health Center'Michigan State University, East Lansing
Phiysiologic symptoms such as heartburn, loss of .appetite andheadache are sometimes a result of one's perception of the stressfulcnvironment and one's attitude toward his or her career' Thesesyrrrptoms impair performance and if the underlying causes are left.rnati"ndcd, thc su-biect may progress to even more severe problems
forcing him or her to leave the profession altogether' The purpose
of this str"rdy was to investigate this phenomeno-n- among a sampleof cmergcncy physicians and to determine possible causes of these.y-ptn-s in the context of practicing emergency medicine' Sixty-
nine physicians from six cmergency departments in the mid-Michrgan area participated in the s-tudy They were asked to
t"rpnnd to a series of well-established inventories that purport to
mcasure strcss symptoms, subiective perception of stress,- iobsatisfaction, tcdium, and feelings of professional demands; the first
being categorized as the somatic dimension and the last four beingcategori"ei as the psychologic dime,nsions fou-nd to be prilcipal
mediating variables in stress research studies. By means of linearstructurai equation rnodelling, otherwise known as causal analy-sis, scveral paradigms ihypothetical relat ional structures) to ex-nlain thc rntcractlon betwccn these varlabies were empir ical lytested for goodness of fit with the actual collected data Oneparadigm w"as found to have an adiusted goodness of fit of 0'99 {chi-.qrr".""= .01, df = l, P = .gB). Essentially, this particular paradigm
indicated that subiective stress plays a major role in determiningjob satisfaction, feelings of professional demands, and tedium'iteclings of professional demands determine job satisfaction, andfeclings of professionai demands plus tedium,.in turn, determinethe piiysioiogic outcomes (symptoms). Stated simply, how oneo".".iua, str6ss determines how demanding one perceives one'slrofession to be and how satisfied one is with one's iob These
ielationships affect the final physiologic outcome' This paradigm
contributes to the knowledge of managing the well-being of emer-gency physicians in their practices.
138 Refusing Care to Patients Who Present to anEmergency DepartmentR W DTrlet,'O ruisf iolOivlsion of Emergency Medicine and ClinicalToxicology, University of Cali fornia, Davis, School o1 Medicine'Sacramento-
In fuly 1988, the emergency departrnent- adopted a policy of
refusing io treat patients in the ED if they failed to have what was
consid&ed an emergency condition. A screening examination wasperformed by a triagl ttutse to determine if the patient was eligibleio b. seen in the ED. Patients whose vital signs fell within specific.rt.gotl.. and had one of 50 minor chief compiaints were refused
""re"in the ED and referred to a number o{ on- and of{-site clinics'The referral of these patients out of the ED {ollowing a screening ex-
amination falls within the scope of legislation governing ED care
50

r
and t ransfer {Federal COBRA, Cal i fornia SB-12 and Ti t le 22) asdetermined by thc University of California lcgal counsel. In thcf i rs t s ix months of th is new tr iage system,4, l86 pat icnts wercturned away from the ED, representing l9"k of totjl ambulatorypat ients who presented to the t r iagc area. Of the 4, I86 pat ientsrefused care, 82Yo were referred to of f -s i te nonunivers i tv c l in ics.and 18% wcre referred to c l in ics wi th in the inst i tut ion. Of th isnumber, no pat ients were rctr raged to an ED, and only 54 pat ients(1.3% ) complained about their rcferra l out of the ED. In conclusion,a select ive t r iage systcm may be used to cf fectrvc ly decomprcss anED,
139 Emergency Department Division of NonurgentPatients to an Off-Site Walk-ln Facil ityKT Sivertson, A DiGiovanna, GD Kelen/Division ofEmergency Medicine, Johns Hopkins University School ofMedicine, Baltimore, Maryland
Studies indicate that onc-thrrd or lnorc of hospi ta l cmcrgcncydcpartmcnt pat icnt vrs i ts arc for nonurgcnt problcms. A pian torcclu i rc hospi ta l EDs to d ivcr t Mcdicaid pat icr"r ts wi th r r r r r i l r rgentproblcrns to othcr faci l i t ics is bcing cvaluatcd by ncar ly a l l s tatcMcdicaid agencics. A divcrs ion plan (dcvclopcd by thc Statc Dc,partmcnt of Heal th and Mcntal Hygicnc) was r .nodclcd af tcr aprojcct in i t iatcd by thc c lcpartment o{ crnergcncy rnccl ic i r rc of aninner-c i ty univcrs i ty hospi ta l on March l , 19{ i5. Pat ients l r rsrnr-ing to the ED hacl previously bccn t r iagcd as necding pr im:rry care,i rnrncdiate care/ or cr i t rcal care. Using thc samc tr iagc cr i tcr ia,pat ients ider-r t i f icd as rcclu i r ing pr i rnary care arc scnt to an associ-atcd, but gcographical ly d istant (sevcn blocks), Lrrgent carc ccntcr .Thc number of pat icnts registcr ing for pr imary carc in t l - rc ED hasdccl ined s igni f icant ly {1, < .01, chr-squarc) f rom l4,002 in f iscal1984 l l9%,, <t f 74,141 tota l rcgist rat ions) to 5,210 in f rscal lg | f t (9, ,2,of 55, I 2 l tota l rcgist rat ions). Rcgistrat ior-rs at thc L l rgcnr carc ccntcrfor thc sarne pcr jot l rangcd f rorn 17,500 to l t { , t {00 ni l t icnr \ |cr y( . i l r .Dcrnographrcs of thc prrrnary c: l rc pat ic l ' l ts : l t thc two faci l i t ics arcsimilar with rcspcct to :rgc/ scx, ancl racc. Thc paticr-rt grollp thatcont in l rcs to rcccivc carc in thc ED is s igni f icant ly (1, <.01, chi-sc luarc j s ickcr as incl icatcd by thc propurt ion of cr i t ical carc czlsosi2.5 'k of f iscal l9f lU rcgistrat ions {1,39(r cascs) vcrsus 1.5,2, of f iscal19114 rcgistrat ions ( l ,13t i cascs), and hospi ta l ach.niss ions, 14,2, off iscal 1 9t jU rcgistrat ions ( 7,(172 adn-r iss ions) vcrsus l l ,Z, of f iscal I 9t j4rcgistratrons (( r , I52 adn-r iss ions). Wc concludc that nonurgcnt pa-t icnts can bc c l ivcr tcc l to a wal l<- in faci l i ty wi th a rcsul tant changcin carc-sccking bchavior ovcr t imc. Thcrc is a currcsl . roncl ingincrcasc in acui ty of thc pat icnt group in thc ED.
-140 Early Unexpected Deaths Following AdmissionFrom the Emergency DepartmentJG Mueller, DJ Fligner, N Wigder/Department of EmergencyMedicine, Christ Hospital and Medical Center, Oak Lawn,l l l ino is
Dcath withir-r 24 hours of adrnission has bccn suggestcd as aqual i ty assurance moni tor for emergcncy dcpartmcnts. Wc oon-ductcd a retrospcct ive rcview o{ a l } patrcnts who cxpircd wi th in thclirst 24 hours after admission frorn our ED during onc yczlr rodeterminc the val id i ty and ut i l i ty of th is rnoni tor . Each dcat l - r wasclassi f ied as ei ther expccted or uncxpectcd. An unexpcctcd c lcathwas defined as a patient for whom the final diagnosis was cliffcrcntfrom the ED diagnosis, or onc for whom the final and ED dragnoseswere the same and none of thc fo l lowing existcd: tcrminal canccr,severe c lement ia, CPR performed in thc ED, rncchanical vcnrr la-tion, appropriatc ICU admission, or a do not rcsuscitatc ordcr. Thecluality assurance assessfflent and action also were rcvicwed foreach case to determine how often thc cmergency physician wasnotified of an unexpccted death. During the l 2-monih period thcrewere 10,582 admissions througl.r the ED, of which 137 1'I.29%lexpired wi th in 24 hours; 23 (0.22%) pat icnts were found to havcunexpected mortality. Of thesc 23 patients, the emergcncy physi-cian was officially notified only two 18.7O%l times. The mean agcof pat icnts wi th unexpected morta l r ty was 75.6 years ( rangc, 44 to94), and the majority of {ina1 diagnoscs rnvolved cardiac 143.1),vascular 122%), or infect ious (26%) proccsses. We conclude that anotable number o{ patients admitted through our ED expire carlyon and unexpectedly and that the emergcncy physician involvedusually is not notified. We suggcst that ED quahty assuranceprograms notify physicians o{ all early uncxpected mortality.
*141 Use of Autopsy Results in the EmergencyDepartment's Quality Assurance PlanMC Burke, RV Aghababian, BV Blackbourne/Div is ion ol EmergencyMedicrne, The Univers i ty of Massachusetts Medical Center,Worcester
Thc autopsy is t radrt ional ly v iewed as thc ul t rmatc qual i tyassurance indicator in c l in ical mcdic ine, yct very fcw c l in i ia l dr i -partments actual ly incorporate autopsy rcsul ts in thci r formalqual i ty assurancc plan. Conscquent ly, to invest igate how autopsyresul ts could bc included in our emcrgcncy dcpartment p lan, ihccl in ical and autopsy diagnoscs of 244 pat ients wcrc comparcd toidcnt i fy condi t ions that wcre Llnapparcnt or misdiagnoscd at thct i rnc of dcath. Di f fcrcnces bctwccn c l tn ical and autopsy diagnoseswcre catcgor ized as c lass I , I I , i l I , or IV f indings. Major uncxpcctcdf indings (c lasses I and I I ) werc found in tcn (4,2,)cascs; th; mostcommonly mtsscd diagnoscs werc aort ic c l isscct ion { thrcc, 1.2%,)and pulmonary cmbolus { two, 0.8%,) . Minor uncxpcctcd f indings{c lasscs I I I and IV) wcrc d iscovcrcd rn l4 (5.8, / . )cascs. Thc rcsul tsc lcar ly ident i fy unexpcctcd f indings ancl point to thc nccd for morcaggrcssivc cvaluat ions of ccr ta in cor-rc l i t ions. Systcmat ic rcv icw ofal l topsy r- lata prcscnte c l has lcd to rncaningful changcs and c le l ivcryol carc to cmcrgcncy pat icnts. Antopsics arc a v i ta l suurcc ofol r tcorrc-bascd informat ion that shoulc l be part of cvcry ED,sr lual i ty assurancc and r isk managcrrcnt p lan.
142 DRGs and the "Negat ive"
Trauma WorkupCM Dougherty, L Flancbaum, DN Brotman, J Avedian, SZ Trooskin/Department of Surgery, UMDNJ - Bobert Wood Johnson MedicalSchool , Robert Wood Johnson Univers i ty Hospi ta l , New Brunswick,New Jersey
Ear l icr t l iagnosis ancl t rcatntcnt of l i fc- threatcning in jur ics ducto rcgional izcd t ra l lnt : l care systc l ls l " ravc rcduccd , ,prevcntal t lc
c lc: r ths" duc to i r - r jury. Concurrcut ly , cscalat ing hcal th carc cxpcn-cl i turcs havc lcc l to t l - rc inplcr .ncntat ion of programs dcsigncd tocurta i l costs. Sir - rcc 1979, a l l l - rospi ta l carc in Ncw fcrscy has bccnrcintbursccl through a pr(rsPcct ivc payntenr systum (DRGs), inwhich t l - rc casc mix of pat icr . r ts is s l rp l . rosccl to tvcragc ol l t ( ic ,"prof i ts" gaincd f rom thc carc of lcss- i l l pat icnts of fsct , , losscs, ,
i r . tcurrccl f ror .n car ing for s ickcr pat icr l ts) . Thc pr-r rposc of our stut lywas to cvr luatc thc f inar-rc ia l intpact of Dl lG rc i r lburscr .ncnt in 140consccLl t ivc t r : lu l ra pat icnts wi th ISS lcss than 9 {nOt scvcrc lvin jurccl ) aclur i t tcd bctwccn )u ly I and Dcccr.nbcr 31, l9r , t7. Thravcragc agc was 30 ycars, ancl motur vchic lc accic lcnt was thc mostcoln lnol t r .ncchanisnt of in j r - r ry ( ( r ( r '2, ) . Diagnost ic studics inc ludcd519 rrrc lographs (3(r posi t ivc , 7 ' / , ,1, 64 hcat l cr t r rputcd tomographysc:rr . rs { l I posi t ivc, 17"1,) , 60 abdont inal cumputcd tomographysczlns or d iagnost ic pcr i toncal lavagc (a l l ncgat ivc l , c ight l ivcr-splccn scans {a l l ncgat ive) , and thrcc bonc scans (a l l ncgat ivc) . Al ll rat icnts had scrccning laboratory tcsts, and 48 1 '34,k,) had ECGs.Minor opcrat ivc proccdurcs wcrc pcr forntcd in l5 pat icr- r ts ( l l ,X,) ;i r - r tcnsivc c; l rc wi ls nccdct l for 22 pat icnts { l ( r ,X,) inc iuding l5 wi thl - rcad in jur ics and s ix for ru lc-out cardiac corr tusions. Avcra{c tota llcr- rgth of stay was 3. t t days. Pat ients wcrc coclcd into 4(r scparatcDRCs . Onc hund rcd twcn t y - t h r cc pa t i cn t s { l l f l , Z , )wc re i n l i r r s ; t ' n l ythrcc pat icnts l2 ' / , ' ) wcrc h igh-t r in-r out l icrs. Thir ty- f r rur of t l i r 4(rDRCs { /47,)wcrc nct loscrs, as wcrc 94 167%,1 of thc pat icnts. TotalDRG rc imbr-rrscmcnt was $177 ,OQ f t r r r rprrat ing cosis of $259, l5Z,y ic ld ing a nct ncgat ivo contr ibut ion margin ( loss) of $ i l2, l I 5 {aver-agc, $5t17 a pat icnt) . T l - r i r ty-c ight pcrccnt of opcrat ing cosrs wcrcduc to room and board, l ( r ' lu to radio logy fccs, [J . t l ,Z, to rntcnsivecarc, 8.6"1, to laboratory tcsts, and 6.4 ' / , , t r , t pharmacy costs. Weconcludc that thc cost of appropr iatc d iagr. tost ic cvaluat ion and carcol t rauma pat ients who arc found to havc only minor in jur ics { lSS< 9) cxcccds thc DRC rc imburscmcnt. Thc currcnt DRG rc i rn-burscmcnt systcn-r c l iscouragcs, f rom a f i r - rancia l perspcct ive, thcpcrformancc of a thorough "ncgat ivc" d iagnost ic workup in t raulnapa t i cn t s .
143 Hypoxic Hazards of Paper Bag Rebreathing inHyperventilating PatientsM CallahamlDivision of Emergency Medicine, Center lorPrehospital Research and Training, University of California, SanFrancrsco
I t rs t radi t ional pract ice to t rcat acute hypervcnt i lat ion byhaving pat icnts rebreathc into a papcr bag. This t reatment, whencrroneously appl ied to pat lents who werc hypoxemic or had myo,cardral ischemia, has resul ted in death. These fata l cases promptcda study of thc effects on oxygenation of papcr bag rcbreathing in
5 l

normal volunteers. Sublects deliberately hypcrventilated to an
average end-t idal CO, conccntrat ion of 21.6 (SD, 3.2) rnm Hg-and
thcn continucd to hyperuentllate into Kraft brown papcr bags
contain ins thc cal ibraied sensors for a Hewlet t -Packard 472104
capnograph and a Teledyne TED (r0| d ig i ta l oxygcn moni t t r r '
Fourtccn mcn and s ix women, ave ragc age of 3(r ycars {SD, 6 1 J wcrc
tcsted. Resul ts, reported as mi l l imetcrs of mercury, wcre idcnt ical
I< ' r 2.25-L and 3.0-L papcr bags and are thus combincd Af ter 30
scconds of rebrcathing, mean change in O, f rom room air was - 15 9
1SD, 4.6J and mcan CCir , was 38. / (SD, 6.2) i at 6O seconds, 20 5 (6 0)
ancl '40.2 (( r .4) ; at 90 secbnds, '22\6.81and 40.5 {( r .4J; at 120 scconds,
23.6 (6.8 l r t rJ +0.7 {( r .5) ; at I 50 seconds, -25. I ( l 2) and 4l (7.3) ; and
at l i lO scconcls, 26.6 18.4J and 41.3 {7.51 A fcw subjccts achicvcd
CO. levcls as high as 50, but many ncver rcached 40 Thc rncan
r-nai imal drop in O, was 26 ( t t . t t f scvcn -sub jcctstrad dr t 'ps in oxygcn
of 2(r r-nm Hg at thrie minLrte s, for:r had drops of 34- mm Hg, and onc
hacl a drop i r f 42 rnm Hg. Thrcc subjccts rcbreathcd into an l l l -L
plast ic bag f i l lcd wi th 100'2, O,, but a l though CO, rapid ly cxcccclccl
+0, O, l .u. l . rcachccl 2 l '2, wi th in two to four tn inutcs : rncl cont in-
ucd t< i c lcc l inc to lcss than lO'2, at 1 5 minlr tcs. Bag rcbrcathing docs
not consistcnt ly c lcvatc CO, lcvcls but i t c l rcs c lccrc: ' rsc FiO,
suf f ic icnt ly to cndangcr hypt ix ic pat icnts. Addi t ional ly , hyp<rxic
rcspiratory c l r ivc is dcCrcascd l " ,y hypocapnia Paper bag-rcbrcathing
shr iu lc l r - rcvcr bc uscd unlcss t ryocardia l ischcrnia can bc ru lcd ot t t
ant l oxygenat ion has bccn di rect ly mcasurccl l ly : r r tcr ia l b loocl gascs
or oulsc oximetrv. I lccausc t l l is cannot bc achicvccl outs idc thc
hoipi ta l , i ts usc by prchospi ta l pcrsotrncl .should bc ab:rndoncd, ar-rd
in-hospi ta l usc pio i rably iht , , - , l i l bc grcat ly d iminishcd'
144 Inhaled Sodium Bicarbonate Therapy for ChlorineInhalat ion In iur iesCD Chisholm, EM Singletary, CV Okerberg, PC Langlinais/Department of Emergency Medicine, The Joint Mil itary MedicalCommand - San Antonio, Texas; The Institute for SurgicalResearch, Fort Sam Houston, Texas
Chlor inc gas l r t r ly c: l t tsc inhalat iot l i t . t j t t r ics thror-rgh cxpost l rcs
fr .1-r rnr l r - rst r i i r l s , ,u iccs, h.urc swinr .n i 'g p. . ls , . r : rc lmixt l t rcs . f
b lcach and r tcrdic c lcar l ing sol t t t i t tns. Vict i r r ls n lay rapid ly prcscnt
to thc c lncrgcl tcy c le l lar t l l lcnt wi th dyspnca, chcst p l in, not lpro-
thrct ivc c,r r - ig l - t , l t r t , t tchospi ls l l l / tachypnca, aud cvcn pt l luronary
cdc' ra. Unt i l rcccr l t ly , thc p. is indcx" rcc. . r ' rcnr lcc l 5 '2, 'cStr l izccl
NlrHCO, as i l t rcat t l lc l l t moclal i ty bascd on : rncct l r ta l rcp()r t -s/
a l th.Lrgl i thc r rost rcccl l t cdi t ion st i l tcs that " i t cann. t bc r t lut inc ly
rccr l ' - r i 'cnclcc l . " ( ) r - r r s t r . rdy was c lcs ignccl to cxaminc thc r . lc . f
ncbr: l izccl NaHCO, in thc t rcatr l lcnt of chlor inc gas inhalat i t rn
in jury t rs ing a shccf modcl . Twcnty-onc shccp I ' rad i r - r tcrnal jugular
and carot id 'ar tcry cathctcrs p laccd by c l i rcct v isual izat ion Af tcr
bcing ancsthct izcd wi th peIr i t 'harhi ta l and sr ' rcc inylchol inc, cach
shc" j . t w"t cnclotracheal ly int r - rbated r tnd cxposcd to chlor i r - rc gas
{500'ppmJ for four ur in l t tes by a c l , tscd systc l l l Thc at l iura ls thct . l
, "crc i . , , laccd.n l r Bi rc l Mark 7 vc ' t i la tor on roorn ai r . At 30 t -n i l l r t tcs
af tcr cxprtsure , t l " rc anirn:r ls wcrc d iv idccl i t - t to two gr t t t tps t t ) r tcc ive
a f ivc-r i rntr tc ncbul izcd t rcat l rc l l t (8 mL) of normal sal inc {Crot tp
A, tcn) or 4 '2, NaHCO, (Gror-rp I3, 1 l ) . Ar tcr ia l b lood gascs-wcrc
samplcd scr ia l ly at f ivc, 15, i30, ( r0, and 90.n"r inutcs and 24 hours
af tcr t rcatrncnt . Thc anir l la ls thcn wcrc cuthanlzcd ancl thc organs
tal<cn for gross : rnd l l l icr ( rsc() | ic exr t tn in; t t i t r t . t ( )nc-way ANOVA
rcve alcd n<t d i f fcrcnccs ove r t i r - r - rc wi th in gr t 'ups wi th thc cxccpt io l l
i r i t l rc GRa pO, ( f = 6.57). I - tcst . for u19u11l gr ' r r - rps rcv.c ' r le ' l
d i f fcrcnccs bciwccir groups wi th h ighcr pCO, {P < 001) and lowcr
pO, ( / ) < .05) valucs f<t t thc contro l gr<rup Thcrc was no di f fcrcncc
in i-ti,,rtolity ratcs bcforc 24 l-rours for cither group (thrcc) or in
microscopic pathology in b l indcd compar isorts Thc usc of a s inglc
in l" ra lat ion t roatmcnt of b icarbonatc c locs not apl lear to worscn
artcr ia l bkxrd gascs or a l tcr pathology in th is shccp r lodcl ancl rnay
actual ly improvc ar tcrra l b lood gas valucs.
.145 Response of Bronchial Smooth Muscle to MgCl2 'n
VitroMH Spivey, E Skobeloff , R Levin/Department of .EmergencyMedicine,-Division of Research, The Medical College ofPennsylvania, Phi ladelphia; the Department ol Urology, Universityof Pennsylvania. Phi ladelPhia
Magnesrum has becn dcmonstratcd to bc an cf lect ive bron'
chodilxor when given IV or by IM injection The rnechanism lor
ihi, i. .,t.l.rt, lrut it has becn postulated to act directly on thc
bronchial smooth muscle. Our study was dcsigned to cxamine
magnesiutn's cffect on bronchial smooth muscle Five-pound Ncw
Zealand rabbits were ancsthetized with kctamrne-xylozine and
Nernbutal". The trachea and lungs were removed surgically and
placed in oxygenated Tyrode's buffer. Three-millimcter bronchial
iir-rg, *.." disiected and placed under 1g passive stretch in a tissue
baih. Masnesium chlor id i added to the t issue bath in doses of 5, 10,
20, and 5b mM decrcased mcan + SD resting tcnsion by 60 t 23, 10
t i0, f rO + l ( r , and 105 t 44 m8, rcspect ively. Electr ical s t imulat ion
o{ 100 V, 100 ms tncreased mean tension by 1(r8 I 52 mg Magne-
sium chior idc (5, 10, and 50 mg) addcd to thc bath decreased tension
by 102, 127.5, and i(rt3 rng, respectively. Histamine (n = 4) 10 mM
incrcascd thc mean + SD tension 49O x 243 mg. Magnesium
chlor ic lc (5, 10, and 50 rnM) dccreascd thc histarnine re sponsc by 80
t 113 , 170 + 147 , and 475 t 3 I1 mg . Be thaneco l ( n : - 8 ) 5 .mM
incrcascd t -ncan + SD tension 495 t 2(r( r rng. Magnesium chlor ide {10ancl 50 mMl dccrcascd thc bethanecol- induced tension by ) '32x 122
ancl 327 t 237 n^rg,, rt: spectivcly. Magncsium chioridc produced a
ckrsc-clcpcnclent t"iatntlot-t of bronchial stnooth musclc at rest and
whcn s i imulatccl by an c lcctr ical f ic ld, h istamine, and bethanecol '
Thcsc data support ihc hypothesi s that rnagnesi t tm - induced smooth
musclc rc la"at lon is rcsponsiblc for thc c l in ical i tnprovemcnt sccn
in pat icnts who rcccivc n lagncsium for acutc bronchospasm'
146 Prospective Comparison of Inhaled Atropine andMetaproterenol in the Therapy ol Relractory StatusAsthmaticusGP Young, P Freitas/Portland Veterans Administration MedicalCenter, Olegon Health Sciences University' Portland, HighlandGeneral Hospital, Oakland, California; University of California atSan Francisco
Wc concluctcd a stucly of adul ts wi th rcf ractory status asth-
ln:rticns to cor-nparc thc rcsportsc to inhalcd anticl-rolincrgic with
that to bcta-adr incrgic solut ions. Af tcr fa i l ing to rcspond to stan-
clarcl thcrapics, 40 paticr-rts wcrc randontizccl prospcctivcly in a
dotrb lc-bl ind fashion to rcccivc cr thcr 1.5 rng atropine {AT) or l5 mg
lrctaprotcrcnol (MP) by ncbul izcr . Both groups wcrc s imi lar in
bascl inc charactcr is t ics, inc ludir - rg mcan FEV, tncasurcmcnts (0 70
L AT/0.60 L MP). Comparcd wi th bascl inc, thc- improvcrncnt in thc
FEV. f r r r thc MP,troup was stat is t ical ly srgni f icant l3 l " / ' , P = '02,
r .a i r . . l r tcst l , whercai thc improvcrncnt in thc AT group did not
icach s igni f icancc (10'2, , P = .15). Compar ing thc two groups,
statisticzilly sigr-rificant diffcrcnccs favoring MP wcrc found ir-r thc
pcrccnt itilprovcrncnt in thc FEV, ( 10'2, AT/3 I 'h, MPi P < '05, signcd
iank) arrd in thc pcrccntage of pzi t icnts in-rproving thcrr FEV,rnorc
than l0 '2, abovc bascl inc 156%' ATlS]r"1, MP; 1) < 05, chi-square) '
No patict-tts in cithcr group suffcrcd any advcrsc outcomos Wc
c,urclt cl" tl-rat for thc rlajority of adults with rcfractory bron-
c l rospasr. � iu stat l ts asthmat ic l ls , ar-r addi t ional bcta-adrcnergic
inhaiatron t rcatmcnt rcsul ts in tnorc i tnprovcmcnt than the addi-
t ion of an atropinc inhalat ion.
.147 Adjunctive Use of lpratropium Bromide in theEmergency Management of Acute AsthmaSM Tiernan, PK Cellucci, DJ Dire/Department of EmergencyMedicine, Emergency Medicine Residency Program, Darnall ArmyCommunity Hospital, Fort Hood, Texas
Our stucly was undcrtakcn to dctermine whethcr inhaled ipra-
tropiun-r brrimiclc aclds significantly to thc bronchodilation ob-
tainccl with inhalcd bcta-agonist alonc in the sctting of an acute
asthma cxaccrbation. All patict-rts who presented to our emergency
, i "pr i , - "" , wi th an acutc asthma at t ick wi th an in i t ia l FEV, of
25''/,, to 75n1, <':[ prcdictcd were evaluated {or cnro]lment in this
c loublc-bl inded s iudy. Pat icnts less than 18 ycars o id or wi th a
i.iriu.y ui glaucoma, urinary tract obstruction, chronic steroid
dcpcndencc, crnphysema, chronrc bronchitis, or cigarctte smoking
werc cxcluiecl. Ali paticnts rcceivcd 2 mg tcrbutaline with 1 mL
sairnc by a n-rinincl-rulizcr at 0, (r0, and 90 mrnutes lmmediately
aftcr th{r first dosc of terbutalinc, patients in Group A received four
puffs of ipratropiun-r bromide administered by a metcred-dose
tannistcr wi th an interposed spacing dcvice to standardize the
close. Paticnts rn Grtlup B reccived a placebo in thc same manner'
Rcpcat sprromctry was performed on all paticnts immcdiatcly alter
the 6O- 'and
9O-minutl terbutaline treatlncnts There were 20
patients in Group A who had an initial, 60-minute, and 90-minute'mean
FEV, o l 4B-.9%,63.3%, and 73.7% oI predicted,respect ively '
Thcre werb l8 patients in Group B who had an initial, 60-minute,
ar . rd 9O-minute mean FEV, of +25"k,58 0%, and 68 3% o{ pre-
clicted, respectively. The initial, 60-mrnute, and 90-minute mean
iEv, -t"f"'..
for Group A and Group B wcre not statisticaily
\')

I+Id
r-
di f ferent lP = .167, two-factor repeated measures ANOVA). Thcconcurrent use of inhaled ipratropium and terbutaline does notI.:rl, 1n
a greate r improvement in FEV, at 60 and 90 minutcs ovcrl nna teo t e rbu ta l t ne a l one .
'148 The Util i ty of Extended Emergency DepartmentTreatment of Asthma: An Analysis of lmprovement inPeak Expiratory Flow Rate as a Function of Time!.G_Murphy, RJ Zalenski, JC Raucci, N Dejneka, S Schabowski, MMcDerrnotVDepartment of Emergency Med'icjne, Cook CountyHospital; University of Health Sciences, The Chicago MedicaiSchool; Rush Medical College, Chicago, l l l inois
Wc studied thc efficacy of cxtendcd cmergcncy departmentt reatment t ime in achieving a pEFR of S0% predictcd-{pEFR..) .Ach i cvc .mr :n t_ c r f P tFR_ , , w i t h i n t h r cc t imc f r ames * r , . u . l u r r i l Jwl th ln t ( )ur , four to c ight , and eight to l2 hours of presentat ion.Entry into the study commenced when ED treatmcnt was in i t iatcc l .Thc PEFR was rccorded hour ly for up to 12 hours. pat icnts wcrecategorizcd at presentation by thc ratiir of initial pEFR to prcdictcclPEIR into group A 1.40 to .491, group B ( .30 to .39), group C ( .20 t<r29), anrJ. group D (lcss than.20). Includcd *"r. pr[i",-rt. "g"d lf, t,,45 years. Excluded were pregnant worlen, thosc hospitalir"d, thur"wl th an acute comorbid i l lness, and thosc wi th in i t ia l pEFR of morcthan PEFR.,,._The study group was 62"k rnale ancl()0,'/o black witha mean age of 2[3 years. Assignment o{ pat ients into suvcr i ty groupsy ieldcd, 4 I 122%) patients in group A, 42 123 %l in groul.r s, ai eS
;/,,Jin group.C, and 36 120%) in group D. Achicvcrncnt oi pffn .reQuircd four to cight hours for 33 I l BZ, ) pationts ancl rccluircd cigl-r'fto. 12 hours Jor sevcn (4%l pat lcnts. Group A had only onc pat icntwho ncedcd more than fuur hours tu , ih i "u. PEFR , , . GioLrp Binc l uded 34 .1 I I qo I pa r i r - n , r s who i r ch i evcd pEFR. , w i t h i n i , , u , h , , u r r ,t ivc {3%)who rcclu i rcd four to c ight hours, anJ' thrcc who nccclccie ight to l2 hours. Group C inclucicd 2S l lS, '1, ) pat icnts wi th in fourhours, . 1(r (9%) wi th in four to e ight hours, and ihrcc rcc lu i r ing c ig l . r tto 12 hours. Group D had 12 17, / , ) pat icnts who achicvcd pEfR , ,within four hours, I I _(6,/ol necding four to cight hours, and , rnly onlpat icnt .who rcclu i rcd eight to l2 hours. Ninctccn {10%,) pat icntswerc discharged f rom thc ED wi thout having achicvcd^pEFR,, . .Extcnding ED asthma trcatmcnt t lmc in uncompl icatcd asthmal '_ics for more than four hours y ic lds a substant ia l incrcasc in thcpercentagc of patients rcaching thc therapcutio goal of PEFR ,,.Only a small proportron of paticnts objcitivcly'Lcncfitcct froiilmore.than eight hours of ED treatmcnt time in this stucly gror.rp,and th<;sc who did so wcrc not prcdictablc on thc basis Jf ln i t i i iPEFR.
149 Evaluation of Brain Edema Using euanti tat iveMagnetic Resonance lmagingJE Olson, A Katz-Stein, NV Reo, FA Jolesz, RVW Dimlich/Departments of Emergency Medicine, physiology and Biophysics,and Biochemistry and The Kettering-Scoti tr/agnatic ResonanceLaboratory, Wright State University School of Medicine, Dayton,Ohio; Department of Radiology, Brigham and Women,s Hospital,fl_arvald Medical School, Boston; Departments of EmergencyMedicine and Anatomy and Cell Biology, University of Cincinnatj
Lit t le is known about the mcchani-sms of brainwate r homcosta_sis. Consequently, current therapies for brain edcma arc limited tononspccrf ic and short- l ivcd stcroidal, osmolar, and diurct ic modali_tres/ trcatmcnts that are contraindicated in many emurgcncy sitLl_atrons. In our study, wc evaiuatcd an anrmal model irf ccrcbraledema Llslng quantitative proton magnetic resonancc imaging(MRI) techniqucs. T,-weighted NMR images (TE, t30 rns; TR, l-scc jwere obtained from adult rats. After acquinng a bascline imagc,brain.edema was produced by Ip inject ibn wiih a volurnc (v) 'oidrst l t led water equivalent to l5% of the animal,s body weight.Sixty minutes later, anrrnals received I00 g/L NaCl Ip in a voluir-reequal to 0.1 (V). Control animals did not ieccive water or socl iumchloride inject ions. Thc mean (t SEM) NMR irnage intcnsity of thcbrain_in-creased by 10- 7 t f .4% 60 minutes af ter tiie water lniection{N = 5, P < .00I ) and then fell to control vah-rcs 60 minutcs aftcr thcsodium chloride rnjection. The rnean intcnsity of images fromcontrol animals did not vary over this two-hour time pcriorl. Inparal iel studies, animals were injected with cither 5% or 15%water and were sacrificed for dctermination o{ brain warer contcntby specific gravity rneasurements or were fixed for electron mrcros_copy. The mean (+ SEM) cerebral gray matter watcr content in_creased from 80.9 t 0. I % to U l .B t 0.2% {N = 12, p < .005) (r0 mrnutes
after a 5"/o water injection. Electron microscopy showed enlargedastrocyte end feet and extracel lu lar spaces. Endothel ia l cel ls , neu_ronsi axons, and myel in appeared normal . Brain water contentdecreased to contro l values 60 minutes af ter a sodium chlor idein ject ion. We conclude that MRI is a sensi t ive indicator for meas-ur ing smal l changcs in brain water content in th is animal model ofbrain edema. This technique may be used to study the t ime courseof the removal of excess water dur ing brain cdema ant l to quant i ta_t ively evaluate potent ia l speci f ic t re i tmc. , ts for brain cdema pres_cnt dur ing pathological states.
150 Effect of High-Dose Norepinephrine VersusEpinephrine on Cerebral and Myocardial Blood FlowDuring CPRJW Hoekstra, PF Van Ligten, R Neumar, HA Werman, J Anderson,CG Brown/Division of Emergency Medicine and Depanment otPreventive Medicine, The Ohio State Universitv, Columbus
Scveral studies have dcmonstratcd an impiovcrnent in ccrebralb l r rod f low {CBFI an.d myocardia l b lood f low lMnf ) wi th largc doscsof rp intphr inc (E) dur ing c loscd-chcst CpR. The cf fects o is imi lardoses of .norcpinephr inc {NE) havc not becn stut l icd. Thc purposc ofour study *{*t: .orlpr.c thc cffccts of high-dosc e ,reisui high_dosc NE on CBF and MBF dur ing CpR. Fourtccn swinc wcighingmorc. than l5 kg wcrc ancsthet izecl ancl instrumcnted fc, , rcgionaiblood f low and hcrnoclynamic mcasure rncnts. Af tcr tcn mrnutes ofvcntr icular f ibr i l la t ion CpR was l rcgun using a rncchanical thumpcr.Af tcr thrcc minutcs of CpR, thc anirnals rc ie ivcd c i thcr E 0.20 mg/kg (scvcn) or NE 0.20 ntg/kg (scvcn) through a r ight atr ia l . r th" tcr .CPR was cont inucd for an addi t ronal thrcc rn inutcs, and dcf ibr i l la_t ion was thcr . r . at tcmptcd. CI}F (nrL/min/100 g) , MBF (mL/min/100g), rnyocardia l oxygcn dcl ivcry {MDO,; rnf- O,/ rn in/ f 00 g) , myocar_dial oxygcn consurnpt ion (MVO,, mL O,/rn in/ l0O 91, and cxt .ac-t i on . r l t i o s (ER ; MV( ) . /MD( ) , 1 w r ' r c mcasu rc t l du r i ng nonna l s i nusr l t y t h rn , t l L r r r ng CPR, an t l a f t e r d ru3 adn r i n i s t r i l t t on . Thc re \u l t \dr-r r ing CPR and af tcr drug adrnin ist rat ion, inc lucl ing ratcs ofsucccssful rcsusci tat ion (SR; , / , , ) , arc c l isplaycd bckrw. 1) 'valucs forE vcrsus NE wcrc calculatcd by analysis of covar iancc, adjust ing forbascl inc c l i f fcrcr-rccs dur ing CpR.
C P R C P H + E C p R + N EcBF 1 . 0 t 1 . 3 10 .5 I 4 . 4 17 .3 1 16 9N , 4 B F 4 . 0 ! 2 . 9 6 2 . 2 ! 4 5 . 3 1 1 8 . 9 r 7 3 . 1MDO, 0 .6 t 0 . 5 9 .4 I 6 . 3 1 9 .9 1 13 .4Ni lVO, 0.6 I 0.5 2.0 t 3.8 11.9 t 8.6ER 93.6 t 5.5 78.2 x 13.0 77.O x 13.4sR 85.7 57.1
P0 .330.040.050 . 1 00.740.56
Whi lc NE improvccl MBF and MDO, ovcr E, SR ratcs wcrc lowcrwi th NE duc to postdcf ibr i l la t ion ai rhythmias in thrcc of scvcnal i rnals. Furthcr stLrdy is rcquircd to dcl incatc thc rncchanism ofthcsc arr l ry thmias wi th NE.
151 Cerebrovascular Occlusion: When Do HemorrhagicInfarcts Develop?GD de Courlen-Myers, M Kleinholz, JA Wolker, KR Wagner, REMyers/University and VAMC of Cincinnati, Ohio. Why hcmorrhagic infarcts_ dcvckrp is poor ly undcrstood cxccptfor an associat ion wi th crnbol ic s i rokcs. Ti rcy arc of intcrcstbccausc thcy may colrp l icatc f ibr inolyt ic st rokc t rcatncnt . Of 105pcrmanent ancl tcmporary middlc cercbral ar tcry (MCA) occlusionsin cats, 83 dcv_clopcd infarcts, of_which 2613l%) wcre hcmorrhagicwi th scat tcrcd petcchia l hcmurrhagcs of tcn coaicscing to smal l hc_lnatorras affecting mainly grcy mattcr. Hcrnorrhagii infarcts de_vr lopcd ovcrwhclrn ingly in hypcrglyccrnic (20 mM) cornparcdwtth ncrrrnrrg lycemic {( . rnM) cats ( ie, 25 of 58 or 45yo comparedwith onc of 25 or 4%,; P < .002 ) . Hcrnorrhagcs into infarcts occurrcdrnaxin ' ra l ly (100%) in hypcrglyccn"rrc cats wi th four and c ig l - r t hourocclusions wi th rcpcrfusion fo l lowed by 26% af ter pcrmanentocclusion._The s ingle hcrnorrhagic infarc i in a normoglyccmic catoccurred af ter an c ight-hour tcmporary occlusion. The rnean + SEMinfarct s ize (% MCA tcrr i tory)was s igni f icant ly srnal lcr (p < .05) in3B nonhemorrhagic {32 t 5 %, ) than in nine hemorrhagic infarcts i(r2+ 12"k) after pcnrancnt with cvcn grcater diffcrenccs aftc. occiu_sion fo l lowcd by re lease (20 nonhcrnorrhagic, l2 + 5%; 1(r hemor_rhagic, t33 + 9 '% j P < .001). Two factors favoi ing the dcvelopment ofhcmorrhagic infarcts cmergc: hyperglycemii and restored blooclflow after tcmporary occlusion. Hypeiglyccmia, by enhancing thet issue acidosis of ischemia, apparent ly c*n."rbni"s both cei i t ra lnervous systcm parenchymal and vascular damage, leading to
53

larser infarcts and red cell extravasation, and both processes may be
;;;;6;storing biood pressure in thc affected vcsscls'
-152 Cerebral Mult i focal Hypoperfusion After Cardiac
lrreit in Dogs, Mit igated by Hypertension and
Hemodilut ionF Sterz, P Safar, Y Leonov, D Johnson, R Latchaw' S Hecht' K
Oku/lnternational Resuscitation Research Center and Department
of Radiology, University of Pit tsburgh, Pennsylvanra" H.-,f f i" ,ron plus hypcrtcnsion plus heparinization aftcr car-
cl iac arrcst in dogs improJe'cloutcome isafar 1976) This could bc the
rcsult of a more homogcncous post-cardiac arrcst ccrcbral,11j l ;
s ion . We tnon i to r td mu l t i [ r rca l { loca l ) cc r th ra l h l { )o t l l l ( rw l l \ -Dr l
* i i f r x"-ci (Wolfson lgf l t jJ in a'dog modcl oJ vcntr icular f ibr i l la-
ii;;-;;;il. arrcst of to or iz s minutes no flow repcriusion w'ith
, , " . . " . r r . r , c rR, , r car , l i , ,pu l n tonary l l vpas-s lC PB) , ear ly .de f ib r i l la -
, ' ' . - . , " j i i ' pv t - , , . i x h , ,u r , , w i th e t 'n t r ' i l o f mean ar t ( r ia l Prc \sure
i.;il"l;,ii,^ ;;;;;i i'i,",J'g"", and tcmperaturc with normal
,. ' - ' "rn "r,". inl prcssurc and hcmatocri t after arrest (14), thc.rc was
i;h:;-;,;;;;,.,;, hyp"..-o followcd bv hvpopcrfr'rsion with rnul-
; ; ; i ; ' i , ; ; : , , i ; i . t l . i tu* (0 to 10.m1/100 g/min) and low f low (0 to
zil -lt, which wcrc not prcscnt bcforc arrcst hnmcdiatc l.rostarrcst
H; i ; i h I r , , r "p ine phr inc l . t rve r l . t t r hours {mcJn z r te r i r t l p re ss t r re '
150 to I . l0 lnm Hg l l th r tJ ( j l r ( . su l tcd in in i t ia l h . r ' tnogcntous hypcr -
cr-nia, fol lowcclby no tr icklc f low are as; with suhsequcnt norru)tcl l-
,i,in, tri"k1" f luw arcas appcarcd Howcvcr, aclditional norrnovolcmtc
iiO'',,, f-r"n",",,rcrit of I iiX, to 20,,1, starting with rcpcrfusio' (two]
i .r" i i .a in sustainccl normalization of lcBr_pattcrns and normal
sCllF values pur,rrr".r. 'Ai f ivc minutcs, al l lxain arcas had f lows
:i ' ; , ; ; . ih*; i . ' +ir '" i l roo g/r.r.r in with no tr icklc or low f low
"",. t , i i tg to six hours' No' i lypopcriusion statc was notcd Hy-
;;;.;;t; hcr.notlil'tion ,""t-,-,'''tt' bc able to prevcnt post-czlrdiac
arrcst r-nultifocal hypopcr{r'rsion
153 Cerebral lschemia and Reperfusion: - Fai lure ol
Hvperbaric Oxygen Therapy to Promote Increased
Suivival or Neurologic Protection
RE Rosentnat, J P Smiin, GH Marshall ' Jr ' RF Shesser/Department
o'f fmligency lt/edicine, The George Washington University
Medical benter, Washington, DCNcurologic i . t lury cai i t ts ' ignif ica.nt.morbrdity and n-rortal i ty in
cart l i : rc arrcst survivors Lipit l ic 'roxit lat i trn is bel icvcd to bc a rnaior
causc of ongoing r-rcurologic damagc occurring aftcr thc rcstor:rtirln
;;;;;;;il;;li,."rniiii.'lnoscf Brcathing 1.09'z' o' aitcr global
ccrcbral ischcmia has bccn shown to incrcasc l ipid pcroxidati<ln
nnJ t-t- turtr l i ,y. Paradoxical ly, hypcrbaric oxygcn.trcatmcnt ot cats
r.rfr i . . ,a. i , . 'airculatory arrest shortens t imc to EEG rccovcry and
;;;;;;;;; ccrcbral spirial flr'ricl lactatc prodr-rction c)ur studv was
clcsignccl to dcten.,rinc lh" ;il;.; of hypcrbarrc oxygon on survival
an<1 ncr.rroltlgic ini.,,y "titti"tt-'scitatitln from cardiac arrcst Malc
Wistar rats (3a'0 to 460 ;t anesth'-t izcd IP. with kctamine (36 'rg)
^"J -vl"?i. . f o.s tr. ,g), * l i t vcnti latcd with room air aftcr micl l inc
tracheototny. tn,.^.^, i i^"- i t ' lect ion of.O-+ rnL cold 1"1' KCI fol-
i,r*".l bv thoraci c com prcssi (rn in {u19{ r1 -r;rn inutc cardiac arrcst'
i ic;G;"; ;"; , ,rnpl i .h' .J * i th IACCPR {70 pcr rninutcJ svnchro-
nous with room air vcnti lat ion' Room air vcnti lat ion (a0 pc1
minute) was corltin.,eJ Lrntil spontancor'rs respiratioli ^lllYl'1,
Afi .r "t t . ,bntion {(r2 t l t3 minutcs),40:nirnals wcrc ptrced ln a
;;;il -;;t';;f
t.'vp"'r-,i. lt'n'''bti' and altcrnatclv assigncd to
,t."i-"", with hypcrbaric oxygen (2 atm absolutc IATAI] or rooln
"i, t-ii"f ii ,cia) for 90 rninutcs Animal survival was recorded
art iy '* i i r t ' " ."- l"gi. a"r i t i i t tutt t mcasurcd. in thosc animals
surviving threc ancl t"" ityt iftt'c w.?s l9 d.i{{erence in survival
between trcatnent groups ichi-squared) w-ith I I of 20 (55' l ' ) hypcr-
;; ; i ; ; ;s;"r.r , . i * l n"J ten .{ 20 {50%) room air-treated rats
surviving tcn days. N".tiofogit a"fic.it scores of survivors similarly
showed no signiticant dif{eicnces between groups at three days
(hyperbaric oxvsen = '5 8 t 8 7' room air = 6.9 x.6,6t i ; i l 11111
.i"lit tftvp"rtrtiJo"yg.tt = 2'4 ! 3 2i room air = l'3 + 2 8; t' = r4l as
*Jr.rrLatv,rr. t*u_-*-pl. r test. Hyperbaric oxygentherapy does
not appcar to promote inircascd survival or ncurologic protcctlon
after cardiac ,.r.r, ,,,i "t*ival using this expcrimcntal model for
global ccrebral ischemra'
.154 A Dose-Response Study of an Experimental lron
Cneiator for Inhibition of DNA Damage by oxygenRadicals
BC White, DM Feldman, Ll Grossman/Section of Emergency
illol.i.L, o"p"rtment oi Surgery, and Department,of Molecular
eiolo;u ;no G"netics and Center for Molecular Biology' Wayne
Siite-0niversity School of Medicine Detroit' Michigan"'-il;;;;itLrA- t'i" radical-induced DNA damage mav contrib-
",.^,"^ait".gi"irriint-t of brain ce11 nuclei during reperfusion after
."rai". ,*.'., Partial support for this.sc.heme. is provided by-the
;;;;;;;;d;;",.,rt.otio" ihat th" iron chelator dcferoxamine inhib-
i,r ..p.if"ti"" membrane injury; however, it does not appear to
"r-r,"i'..ff" in adccluatc quantities to prevent. nuclear damage'
ih*.f;, * ,,.t,iy was undertaken tb examine iron-mediated
;.;;;;';;et;;i oNn a"-^s' as wcll as t9 ch1r1c13rize the dose-
responsc for DNA protecti;n by an expcrimental iron chelator {l-
:;i';l-;;;;h;i J t.,yo'o'vpv'ic1'-4-one; EMHP), rvhose chemical
orone rt ics su,{gr: st improvctl pcne tratton- both o[ cel l memhrancs
;; i ; , i ' , -h."I . f f i ; -brain harr icr ' Supercorled closed circular DNA
ii,rti[", , ."ntitive deteciion syst;m for strand breaks One break
il'"ii;;;;,;;;; ""."11' thc oNe, giving a nickcdtrrcle form that
-ritri"t -"i. ,tn*ly nn g"t clectropiioresis Wc used a small
pi^lt"ia"ona f pBS, 2,i00 bpito studv hvdroxll r1d5ai damage pBS
ijN,t tzoo ng) was cxposcti to the normal intracellular concentra-
4." , , i fH,o, ' i :0 miciornolar) and variou-s-fer1ou1 iron concentra-
, i ,r". r t nU 7. '5. Aftcr l5 minutcs in I mM Fe2', there is extensive
ir"*t,ir,i,rr, ii,ii.l Jn-ng" n"curs at 50 nM Fe2" At the low molecu-
inirr"igflt iron conccnLration (0 4 rnM) sccn in thc brain by two
hours ot rcpcrtusron artcr a I 5-ininute cardiac arrest, all the pBS is
:#;;;l;;;i.'.a .iitt"t t'v I 5 minutes at 3 7. c and is completelv
ir^*t"".r"a fro four hours. EMHP has a molccularweight of 162 and
; ' : : ; ; i i , ; ; ' l i , . i i l . i "" iJtn 5 bctwccn n-octanol and watcr ' rhe
.r.'"i^i,ri .,r*iinr,.. ,, threc sites on iron, and all threc sites must
;; fili;A t,i r"t.t.t"t thc transition mctal inactivc in redox reactions'
Thc EMHP to Fc rat io was varicd from 0:1 to 32:1 in rcactions
concluctcd with 200 ng pBS at 37 C, pH 7 '5 in 0 4 mM Fe" and 30
;i;;;;ir H,o,. er,"i:o minutcs ind four hours of incubation'
;l.';';BS ;;; ""iti."t.,t to clcctrophorcsis Lowcr (4:1 and 8:1)
",,;";;t";;;.tr'Euip showcd somc protcctivc effcct after 30
n'linlltcs. Howcvcr, markcd damagc wai. evidcnt by four hours'
iji-rr", lro,l a,'t,t jz't1 .u.tttntt't-io"' of EMHP.protectcd com-
i-,i:ti; l;':0 ;;;";"' ;;i,;;;1.';;;.; tracc o{ darnage ryas !!il.rl;t;ili; ;; i i; i; 1,;; ;;-ple te protcction was achicved bv the 32:1closc. Howcvcr, in no casc didthc damage. seen.at thc lower ratios
;ft"ffiP;"Jth" d"io'gt in its complctc alxence EMHP has
notcntial lv supcrlor pr, 'p.t i i t t {or crtrssing thc blood-brain harr icr '
#;;;;;;i';il,i-Ir,'ErtrHp is cffectivc in prcventing in vitro DNA
lttt"g. tt'r" *.nv tf"t", dctccts thc breali of one sugar-phosphate
bond in 5,400.
155 The Relat ive Contr ibutions of Early Defibri l lat ion
""0 nCGl"terventions to Resuscitation and SurvivalFrom PrehosPital Cardiac ArrestRO Cummins, jB Gr"ret, S Horan' MP Larsen' K Crump/
ij Jp"it".t "i Medici ne, U niversitv^of w":hilg-t-ol.center f or
Lvatuation o1 Emergency Medical Servic,es'.Ktng County'
W*f'tg;., Divisio-n oi Emergency Medical Services; School of
ft f .Ji.i n"", U niversity of Washi ngton, Seattle'' -w",rtrlvr"d tht arrcst "tnid' oi B2B consccutive people resus-
citat.d fr,rm prehospital cardiac arrcst {rom 1981 through l98T to
clctcrminc the relative contributions of defibriliation and the addi-
;k-;i;;;.d cardiat life support (ACLS) interventions of en-
rlotrachcal intubation ;J.iv ;'liatrn?c9l9qy to resuscitation and
i;;-;; ;ttival. In our t*i titted EMS svstem- (EMT-D plus
;;-;;i.J; wc rlefined two groups: patients who regained a
i"ri"i".al&rrtt"g;hih''' fori.norc than six hours under the care
of EMTs traincd ,o o.{-i-1."ii1"" (EMT I Resus) and those who
,.ol in.a, tr . toin"d p. i iul ing rhyihm uuder the carc of paramedics
iNi; i i ; f f i ; i . r ." i i r", t*. i f i f iy_onc of the resuscitat ions i54%l
werc long-term ,.rruttro,, Mosi resuscitatiols (583' 70%) were
i;;;irllu;" "."tricular fibril]ation, an! mo11 long-term survlvors
;;; u*trl.nln, fibrillation (361, 80%) EMT Ds' on the anest
;;;;.;" "u.rrg. nf s'i -i""ttt beiore arrival of theparamedics'
were able to achieve z7;k \99) o{ ail ventricutq flb-:llti:19,1 t^tTl;
vors,22"/o (99) of al l long-term survlvors'.ano IrTo lrz+l ur d'
resuscitations. t_orrg t"i- lrr.vival was significantly better ]? < .0^1 )
in the EMT-D Resus group 1797n, wtth 4"/o to nursing homesl'
."-pr*J *rift ,n. m.?lt Rt"" gtottp (fov;' ,1th
B% to nursing
il;"..i. dt;;," r..o"ili- ttt't eirly arrival of de{ibrillation alone
ill:.'";:r',:: : :::]* fj ni"J,r:i;r;ti f;lij ffi i;:il'*: lf, :1;;:?;;;';"h;"t close ACLS backup The additional interventrons
54

i
ol early intubation and IV pharmacology are requirecl to achievemax imum p rehosp i t a l su r v r va l .
'156 EMT-D Survivors: The Contr ibution of Defibri l lat ionD Fark, J_LaRochelle, DW Olson, G Hendley, Tp Aufderheide, HASlue-ven/Department of Emergency Medici n'e', Milwauxee Cou ntyMedical Complex, Medical Cottege of Wisconsin, Milwaukee. Emergency rncdical technicran__defibri l lator {EMT_D) programshave irnproved surwival from preh.,spi; i ; ; ; . l i ; arrrsr In nranysettings. However, the counrershocks derivered lly EMT-Ds clo noiappear to contr ibute to the resuscitat ion of al l survivors. ln Wiscon-sin, 64 rural and suburban manual EMT_D serviccs fn.*r.a."pir.i.for rnedical review. Thc contributi"" "f a.fiLriiiiriion in the first 4+srrrvlvors rs reportcd. The arrest rhythm was ventricular fibrilla_, ion
11^11 survivors {95%) and eleciromechanicai cl issociat ion intwo l . ' r7oJ. forty-one vcntr icurar f ibr i l lat ion paticnts rcceivcdcountcrshocks and were. divided into two gru.,pr. Group l , 29patlcnts {66%1, achicvc"d a perfusing rhythin t irat pcrsistcj toprovision of advanced l i fc support (af,3). fhclr f inal countcrshocl<was del ivcred t9.9 t 5.5 minutes beforc'ALS. Group 2, l2 patients(27"/'), remained in full arrest at thc time uf aii, it ntrgt., e ight hJearl icr rcgaincd at lcast transicnt pcrfusing or clcctromcchanicaldissoc.iat ion rhythms. Ovcral l , 3l paticnts' ictu-.a ,u , t ; ; ; ; ; ; ,neurologic x^ate_(7}%l including 2 i frorn grrrup I ilzU,l and scvcntronr group 2lS8%, p = NSJ. Withi, , g.u.,p i , thc paticnts wh.returned to a prcarrcst ncurologic_statc' ira, l 'a r igr-, i f i .ontly shortcitirne from trrest to pcrfusing rhythm than thosc who clctcrioratcJid.y t ,- t .(r vcrsus lZ.f l * g.(r minutes, p < .002). In our rcvicw,dcfibrillation by EMT-Ds clearly conrib,rt..lii,-r"..,r.rtation fro,'prehcrspital cardiac arrest. in2g trt 44 survivors (6(r%,, group l) byrcstoring a pcrfusing rhythrn hc{ore ALS prtry1.i , ,n
157 Prehospital Transcutaneous Cardiac pacing _Phase l lJH Hedges, S Feero, R Easter, B Shultz, SA Syverud, WC DatseylOregon Health Sciences Unrversity, port ianO;ifrurslon CountyMedic. One, O^lympia, Wash ington ; Un iversity' ot Cirrci n nati ; Wilf orOHall Medical Center, LacklanO nfS, San nnionio, iexas
Control lcd outcome studics of prchospital trr,rr". , ,r ,- ,", , , , , anr_diac pacing (PACE) havc suggcstc,: l thoi "r. ly aJmrnistrat i .n . f!.1.1n9
i: nccdcd to improvc survival. Wc pcrforn-rccl ,, p.,,rfr".iiu.study of PACE availablc on a daily basii with coni1urisu,l t,, ahistorical
. control population of paticnts i.,iii., -ir.,.
sanc EMSsystcm with PACE avai lablc only-on an altcrnatc-dny lrrr ir . W"hyp.thcsizcd that daily availabiliiy -,r"ia,Li,"li thc ti.rc frou.rcaro lac .dcco lnpensat ion unr i l pACE lnd subscr lucn t lv i l r rp rovcsurvival. Estirnatecl survival probabil i t ics wcrc falculrrtcd'fromlogist ic. rcgrcssion rnodels of iurvivai, , i l r , ,rpiLi lamissirn anclsurvival to hospital dischargc bascd on historlcal control popula_tion charactcrist ics (144 wiincssecl arrcsts). Comparison of actualto cxpccted survival was maclc with aZ tcst. Othcr dichotomousvariables wcrc comparcd with chi_sc1"rr" ,nntv. i . . ContinuousI11tio,: : ,
werc comparcd.with,an unpaircd r test. A signif icancclevel ot l, < .U5 was used throughollt. During thc four_r_nonth stuclyperiod, 25 patients with witnesscd carclrac ,rc"umpc.,.at,u., .c-: : ' t l {- l lc i
during managernenr ol t t ," i l . pr"t . l ,oftr,r l c:rre 1gr,,up^J. I nesL. patlents wcrc comparctj with 144 witnessctl Jrrt .stpaticnts from thc control period (group B). Therc wcrc no diffcr_enccs ln mean times frorn decompensation to advancccl lifc sL,pp<,it{ALSJ, decompensation to pACL, or ALS to pAaE f, , . gr;; ; ' ;versus paced gror_rp. B patients. Howcvcr, whcn consideiing allgroup B patients,. thc _proport ion of conirols pacccl within tcnmrnutes was less than for group.A (4% versus 30y" j p < .001l. Thcgroup A survival ratc to hospital admission was not signiftcar_rtlydif ferent from the sroup B ratc (zSZ vcrsus-zi;%;, "u.r, nft",ao tus tmenr lo r par ien t charac ter is t i cs . Thc group A surv iva l ra re tonospr ta l^d lscharSs wes s rgnr f i can t ly g rca tc r rhan group B,s 124o^ye1su1 97.; P < .051. This difference wai enhanced nii". ".t1urtir,",r,Ior patlcnt arrcst characte r ist ics (Z = B.57 ) p = .0002 ). Early prchos _pital PACE can improve patient long_te; ,"r;l;;.
158 S.urvival Prognosis for the Elderly After Out_of_Hospital Cardiac ArrestMJ Bonnin, PE Pepe, p S Clark/Deparlments of Medicine andburgery, Baytor Colleqe of Medicine: City of Houston EmergencyMedical Services. Houston, Texas_^ The appropriateness of aggressive CpR of the eiderly patient (>70 years) has often been qucstioned in the medical ' f i tcrature.
However, thc out-of-hospi ta l cardiac arrest v ict im reprcscnrs adrfferen_t
.patrent population with . differcnt prit opt.,y.iotug;r" ufarrcst . We,. therefore, prospcct ively studied the outcome of a l le lder ly vrct ims of out-of-hosprta l cardiac arrest t reatcd wi th in aiTql :
l . tg: , urhan paramedic EMS systcm over a s ix_month per iodto detcrmrnc thci r overal l prognosis and to ident i {y any speci f icsurv ival factors. pat ient ,outcomus were analyzed wi th iespect tcrmul t ip le var iablcs inc ludtng agc, scxi whcther moni to.e d, *he thciwi tness.ed, bystander CpR, and bloodpressurc or cardiac . i ry , f r -^ ,_hospi ta l arnval . Outcomes evaluate, i inc ludeJ in f . lnrp i t r i ,Jrn i r_sron (resusci tatcd) and succcsstul d ischargc f rom the hospi iat(surv ival l . For thc purpo_ses of our 511i ly , pat ients whosc arrest 'was
3: :" : l i l : ! T lh in jury, hemorrhagc, o i .a 'c lear rcspiratory ct io losy
lu$/ torcrgl l body aspirat ion) werc excludcd. The resul t .s dcmon_stratcd that of l7Z consecut ive c ldcr ly cardiac arrcst vrct imscvaluated, 39 lzz%,) wcrc successful ly ics. ,sc i tatca ,"J L i - t fJ tsurv ivcd ovcral l . Of thcsc iZZ pat icnt i , 59 133,1,) had ventr icula ij]]r11!*^r.hycardia as thcirlnitial "i."rt'.hythm. rh.,.,.,rii:litiyor s l r rvrvors werc fuund. in th. is suhgroup, as 25 (a2%) of ihcsccldcr ly vcntr icular f ibr i l la t ion/ tachyiardia ' pot l .n. , wcrc resuscr_:1t . .1 l ,
dr ] ,1 n inc {15' . / " ) surv ivcd. Apart f rom h"u,ng u"ntr i . t , l r .r rnnl lat l { ' l t / rachycardia as thc in i t la l rhythn_r, bystancler CpR alsoappcarcd to contr ibutc t . bct tcr surv ival ratcs. 'Dur ing thc sarncstudy pcr iod, thcre wcrc 300 tota l carc l iac arrcst v ict ims less than70 ycars o ld, of whorn 7g 126, l ) wcrc rcsusci tatccl ant l q l f i i , lsurv ived. Thcsc data conf i rm that thc prognosis fo i c ldcr ly v ict imsof out-of-hospi ta l cardiac arrcst rs ntr t cnt i ic ly b lcak ancl , in fact , isvcry rc: rsonablc i f vcntr icular f ibr i l la t ion/ tachycardia i . i f r . l ' r " :scnt ing rhythrn.
159 Prehospital prophylactic Lidocaine Does NotFavorably Affect the Outcome of patients With ChestPain
f,Y l,?,s*r, f f Qrrggmln, HA Stueven, EM waite, JR Mareer, pHaecKer, I p Autderheide, DW olson/Department of EmergencyMedicine, Milwaukee County Medical Complex, VeOicat C5ttege otWisconsin, Milwaukee
,, , : l11". prchospit:t l pararrcclic systcn-rs acLrinistcr prcphylactic
r l r loc 'a ln ' j r ( ) a l l |at ienrs who prc,scnt w_i th chcst pain i r f iuspectcdcardiac_or ig in in hopcs of prcvcnt ing mal ignant u"ntr i .u ln. r r ' .1_,y ih_n-r ias. Al though many rcports havc bccn wr i t tcn on cf f icacy incoronary carc uni ts, prchospi ta l data l rc scarcc. A randornizct lpr()spef t ivc st l r t ly t . r f prrphylact ic l idocainc was conductccl .n a l ls t : i l ) l L ' p i l t l en t s w i t h s t r spee t rd c t r r t l i ; r c chcs t f r d i n p re \ ( , t l t i ng l o i ll l : t t , l | l ' "u, .
systcm^fr , )nr Ianuary l9 l t4 through fanJary l9 lJu. Dur_r11t1rrs pcnot l , 1,427 p; t t icnt-s wcrc cntcrcd; 204 rcccivcd l idocainc,, : , i : r , , , : : d l r t n{)r L) . ischir rgc.diagnosis inc ludcd 31,2, acurc rnyocar-( l ra l i l r larct l ( )n, ,33 '2, uDstablc angina, 7,1, othcr cardiac, uni 2r)%,noncarcl iac, wi th an ovcral l rnorta l i ty of 7.4,1, Thcrc was an cqualc l is t r ibut ion of dcaths bctwcc,n thc l idocainc (SZi r ra no l idocainc(4{31 groups. C)nly s ix cardiopulmonary arrcsts prc lospi ta l , , . . * . " , fancl I5 occurrcd in t l - rc crncigcncy dcpar,n- ,"n, i lv tn l ignant vcntncu_lar arrhyrhrnias as thc prccip i tat ing ar .cst .hyth i i i - i i pat tcnts wi thacutc_rnyocarcl ia l in{arct i . ' wcrc s imi lar fur both thc ' l idocainc and
3:::ll{yll. $roufs. Thc .incidcncc ,,i oau"rr" .ii.cts ir.rcludingt r radycardlas, sccond_ or th i rd_dcgrcc hcart b locl<s, t inni tus, ani ia l tcrcd rncntal s tatLrs wcre s imi la i in huth gr , r r , f r . i rat rcnts in thcl l l : , * 1 " "
g rou l had . r no re su l . i t c r i v r - . , , n . , p l . i n , r ' , , { . I z z rncss 12 . ( r , , uj I1] , ,y . ; ' " r l l 'u .6 'x ' 14); P.=-002) and dcvclopment of hypotcnsionl4 r { ' / u l i 4 l ve r sus 2 .4 , / " l l 7 ) r p = .00 f i )whcn comparcd w i i h t hc no_r ld()carnc group. Thert ' werc no bencf i ts rnani fesicd f rom thc usc ofprophylact ic l idocainc in pat ic t - r ts wi th stable pruhospi ta l chcstpain; thercforc, ro l l t inc use in thrs sct t ing appca;s unwarranted.
160 Comparison of TgOical Anesthetic Agents in theRepair of Facial and Scalp Lacerations in CnitOrenDS Ross, D Scroggins, J Taylor, G Muskett, B Singal, S Bernardon,K Gardner, J Fowler/University of Cincinnati Cotteg; ot Medicine;Will iam Booth Memorial Hospital. Florence, KentuZkv-
Topical ancsthet ics havc rccent ly becn used succcssful ly inminor wound carc. Their use may be of part icular benef i t in thepediatr ic populat i .n. wc cornpared three di f ferent solut ions in aprospcct ive, randonr izcd, double-bl ind study. Onc solut ion con-rarneo a comblnatron oIO.S"k tetracaine, l :15,000 adrenal inc, andl0-7_o
_c-o,caine (TAC). The sccond c.ntain ed, I'.g7% iet.acainc ancil :15,000.adrcnal ine (TAJ. Thc th i rd soiut ion contained 2,k tetra_caine only (T) . One hundred eighty-s ix chi ldrcn wi th scalp or facia llacerations were randomized tlo receivc nn. ;f th.-ih;.e solutionsin a 2-mL aiiquots on cotton applicators. The soiutrons were55

evaluated regarding their effectiveness {complete or partial versusinadequate anesthesia), use of additional injected anesthetics,parental acceptance, occurrence of side effects, and incidence ofwound infection. Parameters wete evaluated using chi-squaretesting with P < .05 denoting significant difference. TAC was foundto have no significant difference in effectiveness {87.9%) whencompared with TA BO.4%), yet both were more effective than T(54.4%1. Addi t ional in jected anesthesia was administered s igni f i -cant ly more of ten af ter TA (10.9%) and T (21%) compared wi thTAC (3.4%). Parents found the technique of topical anesthesiaoverwhelmingly sat is factory 19O.7%). The incidence of immcdiateside ef fects was low for a l l solut ions {1.8%, 2.O%, and l8%lwithout significant differences. The incidencc of wound infection
did not show a significant difference; howcver, a definite trend ofincreased erythema was noted in wounds in which TAC was used.TA may be a preferable solution because it provides nearly equalef f rcacy wi th a low incidence of infect ion and adverse react ions,whilc avoiding the high cost and negative public perception asso-ciated wi th cocaine.
161 TAC Versus Cocaine AloneAA Ernst , LH Crabbe, DK Winsemius, R Bragdon, R Link/St FrancisHospi ta l , Hart ford, Connect icut ; Univers i ty of Connect icut ,Farmington; South Louis iana Medical Center, Houma
A mixturc of tetracainc, adrenal ine, and cocaine (TAC)has been
uscd extcnsively in the repair of smal l lacerat ions, especia l ly in
children. Sevcral studies have tried tctracaine alone or tctracaineand adrenal inc for th is purpose but havc found infcr ior resul ts. Thepurpose of our study was to determine if cocaine alone wouldprovide ancsthesia equal to that of TAC, e l iminat ing both the r isk
6f tctracaine toxicity and the theoretical risk of side cffects from the
combination of cocaine and adrenalinc and simplifying prepara-
t ion. Onc hundred th i r ty-n inc pat icnts were cnrol led in a random-izcd doublc-bl ind compar ison study compar ing TAC (69 pat ients)
wi th cocaine alone (70 pat ients) . Ef fcct ivencss was rated f rom 0 to
10 by thc cmergency departmcnt staf f physic ian who appl icd the
solution. Ranks of 0 to 3 wcrc considcrcd poor ancsthe sia; 4 to 7 , Iair
anesthcsia, and 8 to 10, good ancsthesia. Using thc Wi lcoxon rank
sum tcst, TAC was found to provide significantly better ancsthcsiathan cocainc alonc (P = .005). Thc perccntagc of paticnts reccivinggood ancsthesia in the TAC group was approxima tely 72% , which
is cquivalent to thc cf f icacy found in othcr studics. Good anesthcsiawas obtained in 52% of thc cocainc-alone group. No side effcctswcrc rcportcd in either group. No incrcased ratc of infection was
f<lund in cithcr group. In summary, TAC was {ound to be a bettcrtooical ancsthctic than cocainc alonc. Neither was associated with
s i gn i f i can t comp l i ca t i ons .
- 162 Safety Practices and Living Condit ions of Low'lncome Urban ChildrenLJ Santer, CB Stocking/Department of Pediatrics, Case WesternReserve University School of Medicine, Rainbow Babies andChildrens Hospital, Cleveland, Ohio; Department of Medicine,Pritzker School of Medicine, Center for Cl inical Medical Ethics'Chicago. l l l inois
Iniuries rcmain the leading cause of mortality in children. Priorinjury prevention efforts have targeted specific injury modes andprimarily private patients, neglecting low-income urban children.i.r ,n atte-pt to assess the injury problem in this population,caregrvers of indigent children less than 6 years old enrolled in anurban pediatric clinic were interviewed regarding living condi-tions, transportation, household configuration, and previous iniu-ries. Of the 133 adults approached, 89% agreed to be interviewed.The median age of patients and parents was 9 months and 25 years,rcspectively. Thirty-eight percent of homes were single-parenthomes. The number of injuries or poisonings per household aver-aged .08 (range, 0 to 4), with 40% of households experiencing oneor more incidents. Eleven percent oi households had a poisoningepisode. Eighteen percent of respondents were cognizant of ipecac,with ipecac available in only 8.5% of homes. Medicine and poisonstorage were rnadequate in 427" and 5 I % of homes, respectively' Ifa child ingested something the respondent believed. might bepoisonous, 5l% would have gone to an emergency departmentbefore calling {or advice. While the frequency of automobile usewas low, unrestrained rides were common with 63% of childrenusually inappropriately restrained. Match or lighter storage wasinadeouatein 78% of homes. Functional smoke detectors and fireextinguishers were present in 75% and27% of homes, respectively.The slorage of knives or scissors was inadequate in 68% of homes,
and firearms were present in 6%. Additionally , 89ok of children 35to 69 months old and 6% o{ those less than 3 vears old sometimesbathed without adult supervision. These findings indicate thedramatic need for injury prevention programs focused on low-income urban children. Specific concerns include exposure tohazardous transportation, chemicals, firearms, burns, and drown-ing. Lack of information and isolated caregivers may result in poorsupervision and responses to life-threatening iniuries.
'163 Undiagnosed Abuse in Children Less Than 3 YearsOld With Femoral FracturesHJ Dalton, T Slovis, RE Helfer, J Comstock, S Scheurer/WayneState University School o1 Medicine, Detroit , Michigan; Children'sHospital of Michigan; Departments of Radiology and Pediatrics/Human Development, Michigan State University, Ypsi lanti
Retrospective evaluation of 138 children who presented con-secutively to an emergency department in one of three ma)orMichigan hospitals was completed. All hospital records and radio-graphs were reviewed. Initial data were evaluated by three pediatri-cians to classify the cases into one o{ four categories: accident (3 I ),abuse (12), underlying bone pathology (12), and uncertain et iology(83). These 83 uncertain cases were handled as follows: 36 werereferred to Hospital Social Services, 29 of whom were subsequentlyreported to Protective Services. Abuse was confirmed in 20 oI 29169%l of these cases. Thus, a total of 32 cases of femoral fracturewere secondary to confirmed abuse. The remaining l6 of 35 caseswere assessed by Hospital Social Services and abuse ruled out as thecause of the fracture. In the remaining 47 children from theuncertain group, no attempt was made to determine the etiology ofthe fracture. A total of 63 children left the hospital without anetiologic diagnosis of their femoral fracture. A review of the stateregistry revealed that seven of 63 {11%) undiagnosed cases weresubsccluently listed as victims of abuse. There was no fracture typecharacteristic for any specific etiology. The high incidence of abuse{32 of 138, 23/ol as the etiology of femoral fracture and of subse-cluent abuse in "uncertain etiology" cases suggests that _everyyoung child with a femoral fracture whose cause is not absolutelyccrtain should be admitted to the hospital for an epidemioiogiccvaluation by a multidisciplinary team consisting of medical andsocral service personnel.
164 Outpatient Management of Febrile Infants 28 to 90Days Old With Intramuscular CeftriaxoneMN Baskin, GR Fleisher, EJ O'Rourke/Division of EmergencyMedicine and InJectious Diseases, Harvard Medical School,Children's Hospital, Boston, Massachusetts
A bacterial focus is demonstrated in 3% to 8% of nontoxicfebrile infants I to 3 months old despite a benign clinical examina-tion. Traditional management includes admission and parenteralantibiotics pending bacterial culture results. We conducted a pro-spcctive study of intramuscular ceftriaxone for the outpatientmanasement of febrile in{ants 28 to 90 days old, with fever morethan 58 C and no source on physical examination or screeninglaboratory tests. After blood, cerebral spinal fluid, and urine wereobtained for culture, if peripheral white blood cells were less than20,0OO, cerebral spinal {luid white blood cells were Iess than lO, andurine dipstick white blood cells were esterase negative, febrileinfants received 50 mg/kg intramuscular ceftriaxone and were senthome. A second dose was administered 24 hours later, and febrilein{ants were followed-up by telephone at two and seven days. Over20 months, 223 iebrrle infants were enrolled. Fourteen febrileinfants (6.3 % I had a bacterial focus identified (group I l, and 209 didnot (group 2). There were no significant differences in mean age (8.4weelis [gioup 1], 7.4 weeks [group 2]), Yale observation scale (6.5versus 6.6), WBC x 103 { 1 1.2 versus 10.6J, or percent polymorphonu-clear ceIIs {32 versus 33). The two groups had significant difierencesin temperature (39.1 versus 38.8 C), and percent bands i9 versus 5)and approached a significant di{{erence in total band count (924,rersui 542; P : .06). o{ 79 febrile infants with 6% or more bands,ten (13%l had bacterial {oci eventually identified, whereas onlythree 127") of 138 febrile infants with less than 6% bands ever hadbacterial {oci identified (P = .004). Of the 14 febrile infants withbacterial foci, four had bacteremia (one case each, Pneumococcus,group B Streptococcus, N meningitid.is, and E co-li). All-feb-rileinfants *ere-afebrile with sterile blood cultures obtained whenrecalled and were well at follow-up. Nine febrile infants hadbacterial gastroenteritis without bacteremia Eight were followedat home, ind one required hospitaltzatron due to increasing bloodydiarrhea without dehydration or toxicity. One febrile in{ant had
56

urinary tract in{ection without bacteremia. Of the 209 febrileinfants without bacterial focus, 200 were managed as outpatientsand were well at seven-day follow-up. Nrne were admitted to thehospi ta l f ive hours to ten days af ter study enrol lment. A11 were wel lat fo l low-up. We conclude that for nontoxic febr i le infants 28 to 90days old, who after a full sepsis workurr do not have an idcntifiablebacterial source by physicil examrnaiion or screeninSl laboratorytests, intramuscular ceftriaxone for two days with telephonc fol-low-up may be an alternativc to hospital adrnission.
165 Outcome in Highly Febrile Nonbacteremic ChildrenJ Burg, L Etzwiler, S Petrycki, GR Fleisher/ Harvard MedicalSchool, Boston, Massachuseus
Thc incidence and comrr l icatrons of occul t bacteremia in chi l -dren have been well describcd; howevcr, tht're is scant informationon s imi lar cohorts of h ighly fcbr i le chi ldren who havc ncgatrvcin i t ia l b lood cul tures. We uncler took an investrsat ion of thc out-comc of thesc nonbacteremic par icnts. Wc studicd 253 chi ldrcn 3to 3ar months old seen in th i cmergency department betwccnNovembcr 1987 and func lgt l t l who were fcbr i le to 39 C or h ichcrand had no apparent bacter ia l source of rn{cct ion. Blood cul turcswcre ol l ta ined on al l pat icnts. Thc chi ldren rcccivcd ei thcr oralamoxic i l l in for two days or a s inglc dosc of int ramuscular ccf t r iax-onc as part of an ongoing study of thc t rcatmcnt for prcsunrptrvebactcremia. A11 nonbactercrnic pat icnts wcrc analyzccl . Subsc-quent infect ions werc documcr-r tcd c lur ing tc lcphonc fo lkrw-up oron repcat examinat ion. Thc mcan agc of thc pat icnts was 14 + 8months, and 47% wcrc boys. Tcmperaturc range was 39.0 to 41.3C with a mcan of 39.U 1 0.5 C. Tl-re n-rcan Yalc obscrvation scorc w:rs7.0 1 I .U. Thc mcan whi tc b lood ccl l count was 14,200 + (r ,850/mml(rangc, 2,500 to3t t ,000/mmr) wi th a mcan bancl count o[ 7.6 ! 6.5, ,1, .Ccrcbral spinal { lu id was obtainecl in 16%, of pat icnts and wasnormal in a l l . Posi t ivc cul ture rcsul ts inc ludcd two of ( r2 13,2, ) ur inclonc E coli, <>ne () vaginalis); thrcc of 12 125,/,) stool {tw(r.S(r1r?rlne|la, onc Cttmpylobacter); onc throat {group A Streyttococctts).Chi ldrcn wi th a bactcr ia l infcct ion on fo l low-r-rp inc l r - rdccl l4 o l253(5.5%) ot i t is rncdia; l4 of 253 (5.5%,) minor bactcr ia l infcct ions{throc bactcr ia l gastrocntcr i t is , threc urrnary t ract infcct ion, twopharyngitis, four pneumonra, onc sinusitis, onc ir-r-rpctigo). Twopat icnts rcquircd hospi ta l izat ion wi th in 4f i hours, onc for dchyclra-t ion and onc wi th H lnf luenzac B bactercmia. In conclusion, h ighlyfebr i lc nonbactcrcmic young chi ldrcn rnay dcvclop rn inor bactcr ia linfcct ions or sor ious compl icatrons of v i ra l d iscasc. In addi t ion, asinglc ncgatrvc blood cul turc docs not c l in inatc thc possib i l i ty ofbactcrcmia. Unl ikc thci r col lntcrparts wi th bactcrcr .n ia, howcvcr,nonbactcrcmic chi ldrcn appoar to bc at rn in i rnal r isk for subsc-ql lcnt scr ious focal bactcr ia l infcct ions such as mcninxi t is .
166 Cat Bi te Wounds: Risk Factors for Infect ionDJ Dire lDepar lment of Emergency Medic ine, Emergency Medic ineResidency Program, Darnal l Army Communrty Hospi ta l , Fort Hood,Texas
In thc last tcn ycars, many cmergcncy mccl ic inc spccia l is ts havcstudicd anrmal b i tc wounds. Most authors ' recommcndat ions forthe t rcatmcnt of cat b i tc wounds havc becn bascd on anccdotalexpcr ienccs, studics of dog bi tc wounds, or onc smal l , contro l lcd,prospcct ive study of cat b i tcs (which had only 1 1 pat icnts) . Todetcrmine r isk factors for wound infcct ion, wc prospcct ivc ly col-lccted data on 216 consccut ivc cat br te or scratch wounds thatoccurred rn 185 pat ients who prescntcd to our cmcrgcncy dcpart-ment ovcr a two-ye ar per iod. Of the wounds, 150 {( r9 %, ) wcrc part ia lth ickncss and 62 129%) wcre fu l l th ickness. Twcnty- four {13%,)patients had clinical evidencc of wound infcction on arrival to thcED. Five (3%) pat ients developcd c l in ical cv idcncc of woundinfect ion dcspi te ED treatment. None of thc 1a (8%)pat icnts wi thonly "c law" in jur ics developcd a wound infcct ion. Thc ovcral lpat ient lnfcct lon ratc {or thosc wi th cat "b i tcs" was I7"1, . Factorsassociated wi th an increascd l ikel ihood of wound infcct ions in-c luded oldcr age (P < .005 j , longer t ime intervals unt i l ED trcatment(P < .05), wounds inf l ic ted by "pet" cats (P = .0018), patrcnts whoattcmpted wound care at home lP = .0041, paticnts having a singlcbi te wound {P = .1903), and pat icnts having morc severe wounds {p= .00771 or dccper wounds (P = .000I) . Data f rom I4{3 of thcscpatients who had only "bite" wounds and did not havc clinicalevidencc of infection on prescntation to thc ED were also analyzedfor infection risk factors. Wound infections wcre more likcly tcrdevelop in patients with lower extremity wounds who did notreccive prophylact ic oral ant ib iot ics (P : .01871 and those wi thpuncturc wounds who did not reccive prophylactic oral antibiotics
\P : .O21.In our study, the wound type and wound depth were themost important factors in determining the l ikc l ihood of developinginfection regardlcss of whether the patient was prescribcd prophy-lact ic oral ant ib iot ics.
167 The Use of Oral Acyclovir in the Treatment ofHerpetic WhitlowEA Davis, MR Sayre/Medical College of Pennsylvania - AlleghenyCampus, Pittsburgh
Herpct ic whi t low is an rnfcct ion of thc d ig i t (s) by herpcs s im-plcx v i rus type I or I I . Thosc at h ighcst r isk rnclude mcdicalpcrsonncl . Due to thc infcct ious nature of thc d iseasc, thoscaf f l ic tcd rnust avoid d i rcct patrent contact unt i l thc lcs ions crustovcr, usual ly rn two to s ix weeks. Trcatmcnt has t radi t ional ly bccnsymptomat ic; howcver, rcccnt ly oral acyclovi r has bccn shown todccrcasc hcal ing t tmc in other forms of hcrpet ic infcct ion. Thepurposc of our study was to cxaminc rhc i f fcct ivcncss of oralacyclovi r in dccrcasing thc durat ion of syrnptoms and thc infect ivcper iod of hcrpctrc whi t low. In the f i rs t mul t ip lc casc study s ince1959, wc retrospcct ivc ly rcv iewcd al l cascs of cul turc-provcnl"rerpct ic wl-r i t low prcscnt ing to thc cmploycc hcal th c l rn ie in ourcmcrgcncy dcpartmcnt f rom May 191J3 to May l9 l i l t . Twcnty-ninccascs wcrc idcnt i f icd, wi th scvcn cxclusions. Thc rcn"rain inc 22pat icnts wcrc cvcnly d iv idcd betwccn thosc rcccrv ing oral lcy-c lovi r (200 mg f ivc t i rncs a day for tcn days) and thosc wi th ncrt rcatmcnt. Thc samc physic ian cxamincd al l pat icnts at rcgularintcrvals ancl , using thc samc cr i tcr ia for cach pat icnt , dctcrrn incdwhcn thcy coulc l rcturn to work. Thc groups wcrc not stat is t ical lyc l i f fcrcnt in scx, agc, prcccdrng dig i ta l i r - r j r - r ry, or c lominant hancl ordig i t involvcd. Data for thc two grol lps wcrc analyzcd curnpar ingt iurcs f rom in i t ia l prcscntat ion to rct l l rn to wor l< using thc Mann-Whitncy tcst . Thc acyckrv i r group rcturncd to work car l icr {mcan,I 1.33 vcrsus I 7.5(r days, P = .OO47l , and, subjcct ively, thc i r syn-rp-toms wcrc lcss scvcrc. Wc also founcl a h ighcr (17 of 22) propurt ionof pat icnts wi th prccccl ing in jury than prcviously rcportcd. Rccog-niz ing thcrc wcrc l imi tat ions to th is typc of stucly, wc rccornrrcndoral acycluvi r as cf fcct ivc in t rc: r t ing hcrpct ic whrt low.
168 Screening for Syphilis in the EmergencyDepartment: RPRs in Patients With Suspected SexuallyTransmitted DiseasesA Ernst , JD Samuels, DK Winsemius/Saint Francis Hosoi ta l andMedical Center, Hart ford, Connect icut ; Univers i tv of Connect icutHeal th Center, Farmington
Our str - rc ly was intcnclcd to dcmonstratc thc cost-cf fcct ivcncssof syphi l is scrccning in a h igh-r isk group of cne rgcncy r lcpartme ntpat icnts. Ovcr a four-month pcr iod, 2(r0 pat icnts wi th suspcctedscxr-ra l ly t ransl l i t tcd discascs {othcr than syphi l is) hat l rapid p lasntarcagins (RPRs) drawn to dctcrminc thc inc idcncc of ur-rs l rspcctcdsyph i l i s . Twcn t y - two pa t i cn t s ( 13 ' 2 , ) had pos i t i v c RPRs . O f t hcsc , l ( r(6 '2,) a lso hacl posi t ivc FTA-ABS. Of I 1(r pat icnts wi th posi t ivc GCcul turcs, c ight a lso had posi t ivc RPRs; of 2t l pat icr- r ts wi th posi t ivcChluntydiu ant ibody tcsts, f ivc had posi t ivc RPRs. Thc study groupwas comparccl wi th two smal lcr contro l groLrps in whorn syphi l isscrccning is rout incly donc at our hospi ta l . In a randomly choscnn- lonth c l l r r ing thc stucly pcr iod, 55 ncw hospi ta l crnpkryccs and 90rrcw obstctr ics c l in ic pat icnts had bccn scrccncd, and nonc hadposi t ivc RPRs. Thc di f fcrcncc was highly s igni f icant l1) < .001). Thccost for thc RPR scrccning camc to $104.90 for cach pat ient wi th aposi t ivc FTA,ABS. Wc concludc that scrccning for syphi l is in ahigh-r isk populatron i t - r thc ED is cost cf fcct ivc.
169 HTLV-1 Infection in an Inner-City EmergencyDepartment Populat ion: The Next Retrovirus Epidemic?GD Kelen, T DiGiovanna, L Loty, L Bisson, D Kalainov, KTSivertson, TC Quinn/Divisions of Emergency Medicine andInfectious Diseases, The Johns Hopkins School of Medicine; JohnsHopkins University School of Medicine, Balt imore, Maryland;Laboratory of lmmunoregulat ion, NlAlD, NlH, Bethesda, Maryland
Thc human T-ccl l lcukemia virus (HTLV-11 rs thc causativcagcnt of the adult T-ccl l leukcmia (ATL) and HTLV-l associatedrnyelopathy lHAM). Whilc HTLV-1 is cndemic in ccrtain parts ofthc world, with an cst imated gcncral populat ion rate of .03%, i t hasnot been considcrcd to be widcly prevalcnt in the United Statcs.Becausc coinfection with HIV has been demonstrated, wc undertook this study to examine the epidcmiology of HTLV-I in apopulation known to have a high ratc of HIV infcction. OI 2,544consccutive serum samples drawn from adult patients prcsenting
57

to an inner-city emergency department, 30 ll.2%l were Western
Blot seroposi t ive to HTLV-1. Whi le 152 of the pat ients (6 0%)were
Western Blot seroposrtive to the human immunodeficiency virus
{HIV- l } , only three pat ients (a l l IV drug users) had concurrent
infect ions. The age dist r ibut ion of HTLV-1 infected indiv iduals
matched that of the patient population in contrast to HIV, which-
was concentrated among pat ients 25 to 44 years old (P < .05). Hal f
of thc HTLV- 1 infectcd patients were more than 50 years old. Of the
30 seropositive paticnts, 93% l28J were black, whereas blacks made
up only 77% ol the pat ient populat ion {P < .05) Only l5 patre-nts
{50y.) had an identificd risk factor; ten were IV drug users and five
were t ransfusion recip icnts. Only one pat lent 's potent ia l source of
infect ion was sexual exposure to an HlV- infected partner. Al l but
one of the seroposi t rve pat ients l ived in the surrounding neighbor-
hood, imply ing that migrat ion f rom cndemic areas was not l ikely
a pr incip i l fac ior for infect ion. We conclude that HTLV-1 may be
mire pievalent than previously thought among US rcsidents.
Sexual t ransmission did not seem to play a major ro ic in HTLV-1
infect ion. The data support thc hypothcsis that HTLV-1 and HIV
are indcocndent lv t ransmit ted diseascs. Whi lc nosocomial infec-
t ion wi th HTLV-l has not becn demonstratcd, th is may bc due to
a low lcvcl of survei l lancc.
170 Multicenter Human lmmunodeficiency Virus andHepatitis B Seroprevalence StudYJ Jui, B Wayson, J Schriver, P Stevens, S Modesitt , S Hulman, DFleming/Emergency Medicine Research Counci l of GreaterPort land, Oregon Health Sciences University, Oregon State HealthDivision, Port land
Prior singl: inst i tut ional invcstigations havc found unrecog-nized human irnmunodeficicncy virus (HIV) seroprcvalcncc incmcrgency dcpartmcnt patients to range from 03U% trt 4'k. Aprospcctive, anonymous study of HIV and hcpati t is B scroprc-valencc was pcrformcd on cxccss scrum of al l ED patients over two4tl-hour pcri6ds in May and August 19tlti, from scvcn hospitals ina major northwcstern city (populat ion, approximatcly onc mil l ion) 'Dcrnographics wcre known for 33ti of 444 {76'2, } paticnts. Forty-sixp"rcc.t i wcrc male and U5'X, werc whitc, with a mcdian agc groupi,f aO tn 39 ycars. Ambulance transport-trauma; clothes and cquip-mcnt contaminatcd with blood; prcscntat ions rcquir ing EDproccdurc(s); and acuity result ing in intensivc carc admission wcrcpr"."nt f<tr i l " l , ,10"1,,7'k,34%, and 14% of paticnts, rcspcctivcly'two of 444 10.45"1' l patients werc HIV posit ivc, onc previouslyundiagnoscd. Fif ty-f ivc <tf the 444 l l2' /"1 and threc of 444 10'6%)r"-pi. . werc posit ivc for hcpati t is B corc antibody (HBcAB) andhepati t is B surfacc antiScn {HBsAC), rcspectivcly. Asscssmcnt otr isi factors was possiblc on 180 of 444 l4O%) paticnts. HBcABscroprcvalcncc corrclatcd with racc {1' < .001) and IV drug usc (P -<.001l, but thcse cri tcr ia were sensit ive in detectrng only 14% andl8% of HBcAB-posit ive patients, rcspcctivcly. HBcAB was notassociatcd with the fol lowing factors: scx, arca of rcsidencc,prescncc of blood on clothing and ecluipmcnt, trauma, acuity ofillness, Eo procedures, and mode o{ transport. Thesc data stronglysupport the usc of universal body fluid precautions. Hepatiti's Bpoies a significant and clistinct risk to all emergency care providersthat has bcen understatcd because of the HIV exposure concerns'Henatitis B vaccination should bc strongly advocatcd for all EDhealth care workers. Emergcncy mcdicrnc multicenter studles areboth dcsirablc and fcasiblc io follow trcnds rn the seroprevalence ofin{ectious agcnts in the ED.
171 Hepati t is B Infection and Human lmmunodeficiencyVirus Inlection in Emergency Department PatientsKT Sivertson, GD Kelen, TA DiGiovanna, T Brothers, TC Quinn/
Div is ions of Emergency Medic ine and Infect ious Diseases, The
Johns Hopkins Univers i ty School of Medic ine, Bal t imore, Maryland;
Laboratory of lmmunoregulat ion, Nat ional Inst i tute of Al lergy and
Infect ious Disease, Bethesda, MarylandBoth hcoatitis B virus and human immunodeficiency virus
(HIV) have been identified as exposure risks for emergency- health
workers. Some municipal emergency medical services stili fail to
vaccinate personnel agiinst hepatitis B virus,- arguing that the use
of universal precautio;s to auold contact with the blood and body
fluids o{ patients wr11 prevent infection with either virus' Sera
coilected during a previous study oi HIV infection in emergency
department patienti was tested to characterize the prevalence and
diitribution o{ hepatitis B virus infection' Adequate sera was
available to test 2,i i6 patients by ELISA (Abbott Laboratorres) for
the presence of hepatitis B virus surface antigen. Of the 2,116
patiants, 83 13.9%l were infected with HIV only -One hundred nine
i5.2%l *rre infectious with hepatitis B virus only Frfteen patients
i0.7%)*. . . in fect ious wi th both v i ruses. Thus,207 pat ients (9.8%)
were infectious with one or both viruses. Hepatitis B infection was
uniformly distributed across age, sex, and race strata. Statistically
signi{icant di{ferences (P < .05, chi-square) existed-between hepati-
tiJ B and HIV inlection in patients 55 years and older (hepatitis B,
32 cases or 297oi HIV, {our cases or 4.8%), female sex (hepat i t is B,
59 cases or 547o;HIV, 23 cases or 27.7"h), andwhi terace {hepat i t isB, 24 cascs or 22"ki HIV, ten cases or 12"/"1' Arrival by ambulance
was the same for both hepat i t is B {25 or 22.9%) and HIV {24 or
28.9%)pat ients. Given the smal l ovcr lap and the di { {erent d ist r ibu-
tion of thcse two infectious viruses in the same ED patient popu-
lation and the availability of a 1ow-rrsk and highly effective vaccine
for hcpatitis B virus, the substitution of unrversal precautions Jor
hcpatiiis B immunization is not iustified and increases the proba-
bility of emcrgency health workcr infection with infectious blood
and body fluid-borne virus.
172 The Effects of Fructose'1,6-Diphosphate onMyocardial Necrosis During Coronary Artery OcclusionTG Janz, JE Leasure, JE Olson, GC Hamilton/Wright StateUniversity, School of Medicine, Dayton, Ohio
We cvaluated the abil ity of fructose-1,6-diphosphate {FDPJ tolimit myocardial ischemia and necrosis during acute occlusion ofa coronary artery. Thrombosis of the left antcrior descending arterywas induced in dogs by a closed-chest technique. After coronaryocclusion produced significant S-T segment elevations, dogs werethen injccied intravenously with 90, 175, or 350 mg/kg FDP ornormal salinc (controls). Hemodynarnic parameters, ECG changes,ancl scrum levcls of creatinc kinase, creatine kinase-MB, and lacticdchydrogenasc were evaluated at baseline and at 30 minutes andfoui hours after ECG changes. Four hours after acute coronaryocclusron, the animals were sacrificed and cross-sectional areasand weights o{ ischemic and necrotic myocardial tissue wereouantified in uniform heart sections, using a histologic-stainingmcthod. The animals treated with FDP demonstrated a significantrcduction in weight and area of necrotic myocardium comparedwith control animals (1' < .001); however, there were no significantdiflerenccs bctween control and treated animals in biochemical,hemodynamic, or ECG parameters. In control animals, 13, !3% ofthc cardiac tissue was necrotic by weight and 24 t 4% by cross-scctional arca o{ thc histologic sections. Animals treated with FDPhad an avcrage ol 4 t2% necrosis by weight and l0 t 3% by cross-scctional arei, with the I 75 mg/kg group showing the best results'Significant reductions also were seen in the weights and cross-scctional areas of ischemrc myocardium of the treated dogs iP <
.001). These data suggest that FDP reduces the amount-of myocar-dial ischernia and necrosrs after acute coronary artery thrombosis'
173 High-Energy Phosphate Metabolism DuringVentricular FibrillationH Neumar, CG Brown, P Van Ligten, J Hoekstra, R Altschuld/
Div is ions of Emergency Medic ine and Cardio logy, The Ohio State
Univers i ty , ColumbusPast studies of mvocardial ischemia have shown an association
between high-energy phosphate (HEP) depletion, the on-set of
irreversible -yocatdir[ i.tjury, and the degree of myocardial func-
tional recoverv after reper{usion. These studies, however, were of
nonfibrillatory regional and global myocardial ischemia Because
approximately 50% to 7O% of patients with prehospital.cardlac
"ir"rt ^.. found in ventricular fibrillation, we studied the time
course of HEP metabolism during ventricular fibrillation' Five
immature swine weighing 23.0 t 3.2 kg were studied. After thora-
cotomy, 4-mm diametei transmural myocardial biopsies were
taLe.t in vivo during normal sinus rhythm (NSR) and at designated
times durinq ventricular fibrillation. Biopsies were frozen within
two secondJ in chilled isopentane and then transferred to liquid
nitrogen. Chemical analysii for HEP was done using high-Per{orm-
ance"liquid chromatography The results, expressed in pmol/g
proteln, are listed below:
NormalSinus Duration of Ventricular Fibrillation (min)Hhythm 5 10 15 20 30
ATP 39.0i2.3 18.2t5.9 12.813.5 10.7L3.4 7.9+2.3 3.813 4
ADP 8.2!1 .7 10.4!2.7 10.8 1.2 10j !2.4 9.511 .8 5.4L28AMP O.7tO.4 2.510.3 3.2t0.5 3.611.1 4.7!0.9 9 515.7
TAN 48.1!3.2 31.018.1 26.8L4.3 24.2 '154 22'2!34 188135
58

TAN, tota l adenine nucleot ides (ATp + ADp + AMp)Aftcr 20 minutes of ventricular fibrillation, an avcrage 203% ol
NS_R myocardial ATP remains. Previous studies of myocardialrschcmia have shown that when ATP is equal to or greatcr than20o/o of c,rlntrol, myocardial inlury is revcrsible, and the myocar-dium will ultimately recover function rf adequatcly reperiusecl.Additional study of ATP rcgeneration and myocardial functionalrecovery after repcrfusion may help further define the limits ofacute myocardia l rcsusci tat ion af tcr prolongcd ventr icular f ibr i l la-t1on.
.174 Evaluat ion of Direct Mechanical Ventr icular
Assistance At ter 15 Minutes of Ventr icular Fibr i l la t ionMP Anstadt , R Neumar, P Van Ligten, HA Werman, GL Anstadt ,CG Brown/Department of Surgery, Duke Univers i ty Medical Center,Durham, North Carol ina; Div is ion of Emergency Medic ine, The OhioState Univers i ty , Columbus; and The Biosciences Center, MiamiVal ley Hospi ta l
Prcvious studics ustng di rcct mcchanical vcntr icular assistancc{DMVA) af tcr tcn minlr tcs of vcntr icular f ibr i l la t ion and thrccminl l tcs of CPR resul tcd in successful myocardia l rcsusci t ; r t ion offour out of scven aminals. Thc purposc of t rur st t rdy w:rs to cv:r luatcthc cf fect ivcr-re ss of DMVA af tcr l5 minl r tcs of vcntr icular f ibr i l lat ion. Scven immat luc swinc wcighing24.O ! 3.4 l<g wcre instr r r -mentcd for rcgional b lood f low and hcmoclynarnic rncasurcnrcnts.Af tcr 15 minutcs of vcntr icular f ihr i l l r l t i ( )n, stanr larc l r -nccl"ranicalCPR was pcrformccl for thrcc minutcs. DMVA was thcn annl icc l forthrcc minutcs (DMVA I ) . Af tcr DMVA I , in tcrnal dcf ihr i l le i ion wasattcrnptcd. I f def ibr i l la t ion dic l not rcsr . r l t in thc rctnrn of spontanc,ous c i rculat ion, DMVA was rcappl icd for an adcl i t ional tcn minutcs1DMVA2), af tcr which dcf ibr i l la t ion was again at tcmptcd. Rcgionalt issuc blood f low and hcmodynamic mcasurcmcntJ arc d isplaycdbclow:
CPR DMVA] DMVA1 -- DN,,IVA2 Pn = 7 n = 7 n = 5 n = 5 p t p z
MBF- 2.1 !1 .3 78.4 ! 32 84.0 r 37.3 76.2 t47.g < .005 > .1EN/EP 0.2 10.1 1.2 t 0.6 .1.4 t 0.6 0.6 r 0.3 < .005 > .005c B F 0 . 7 1 0 . 8 2 . 3 + 2 . 7 1 . 1 r 1 . 1 1 . 2 1 0 . 8 < . 0 5 > . 1MVO, 0.28+0.17 9.4!4.4 10.7!4.6 5.6!2.4 <.005 >.05E R 8 8 . 9 1 6 . 7 7 1 . 6 t 1 1 . 8 7 7 . 9 t 5 . 9 5 7 . 7 1 1 6 . 6 < . 0 1 > . 0 5A o D P 1 0 . 3 1 8 . 9 3 1 . 6 r 1 0 . 0 2 7 . 7 t 6 . 5 2 6 . 1 t . l 1 . 8 < . 0 0 5 > . j- l \ ,48F, myocardia l b lood f low (mL/min/100 S); EN/Ep, endocardia l /epicardia lb lood f low rat io; CBF, cerebral cor t ical b lood f low (ml/min/100 g) ;MDO2,myocardia l oxygen del ivery (mL O,/mrn/100 g) ; MVO,, myocardia l oxygenconsumpt ion (mL Orlmin. 100 g1: ER. myocardia l oxylen extracuon rar io:AoDP, aort ic d iastol ic pressure (mm Hg); p l , compar ison of CpR andDMVAI t P2, compar ison of DMVAI , (animals that subsequent ly receivedDMVA2) and DMVA2.
DMVA providcs MBF and MDO, slrperior to star-rdard CpR aftcrprolongcd vcntr ic l r l : l r { ibr i l la t ion; howevcr, cercbral b loocl fkrwstcmain poor. Af tcr l5 minutcs of vcntr icular f ibr i l la t ion and thrccminlltcs of CPR, rnyocardial rcsuscitation r:ltc is p(x)r cvcr-r witl-rthrcc to 13 n-rinutcs of DMVA.
175 lmproved Resuscitation and Limited Myocardiallnfarct Size Following Cardiopulmonary BypassReperfusionM Angelos, M Gaddis, G Gaddis, J Leasure, S Orebaugh/Department of Emergency Medicine, Wright State University Schoolof Medicine, Dayton, Ohio
Resusci tat ion wi th cardropulmonary bypass was comparcd wi thstandard CPR advanccd l i fe support (ALSI wi th a dog modcl of acutcn-ryocardial infarction followcd by vcntricr"rlar fibnllation. Sixtccnmongrcl dogs were randomly assigncd to reccivc CpR-ALS {groupi ; n = f3)or CPB (group 2; n: f i ) . A coi l was placcd in the lc f t anier icxdesccnding coronary artery under fluoroscopic gurJancc. Anin"ralswerc fibrillated aftcr the appearancc of I mm S-T clcvatron. CpRwas star ted af ter e ight minutcs of ventr icular f ibr i l la t ion. Epincph-r inc (0.05 mg/kg) and HCO. ( lmEc1/kg) wcre admir . r is tercd at icnminutes. Group I reccived in i t ia l dcf ibr i l la t ion at tcmpts at l2minutes. Croup 2 received CPB bcginning at 12 minutes: dcf ibr i l -lat ion at 14 minutes and bypass for one hour. Ischemrc and necrot icareas wcre detcrmined with flourescein and triphenvl tctrazoliumhistochcmical sta in ing techniques rn surv ivors. There was nosignificant difference betwccn prearrest variables {heart rate, mcanarterial prcssure, right atrial pressure, dp/dt, or timc to infarct).Four of eight group 1 and cight of cight group 2 animals wereresuscitated with two of eight and six of eight surviving to fourhours, respectively {P < .05). Group I required significanily moreeprnephrine, Iidocaine, countcrshocks, and joulcs per kilograrn
than group 2 dur ing resusci tat ion. Aort ic d iastol ic and coronarypertuslon prcssures were s imi lar dur ing CpR but s ignl f icant lyhighcr in group 2 af ter the onset of CPB. Group I surv ivois (n=a) hada mcan infarct s ize of 17.65 X8.26% vcrsus group 2 surv ivors (n =6), 5.24 ! 6.03% (P < .05). The rat io of necrotrc to ischcmic t rssucwas s igni f icant ly greatcr in group 2 {p <.05). Af ter lc f t antcr iordesccnding occlusion, cardropulmonary bypass reperfusion af tcrcardiac arrcst rcsul tcd in srgni f icant ly bet tcr resusci tat ion andsn'ra l ler infarct s izcs. Cardiopulmonary bypass rcpcrfusion mayl in ' r i t in farct s izc dur ing thc in i t ia l postrcsusci tat ion phasc.
.176 Comparison of Epinephrine and Dopamine in CpRKH Lindner, FW Ahnefeld, lM Bowdler/ Universitv Clinic ofAnaestheslology, University of Ulm, Ulm, West Germany
Epincphr inc and doparr"r inc inducc by a vasoconstr ic t ron an in-crcascd diastol rc b looci prcssurc and hcncc : rn improvccl rnyocardia lpcr fusion c i r - r r ing CPR. Wc havc, thcrcfore , cornrrarcd thc actron ofcprncphr inc and dop:u-nine rn an asphyxral and eicctr ical ly induccdcardiac arrcst n-roclc l . Asphyxia l arrcst was induccd in 2 l p igs byclar-nping thc cndotrachcal tubc. Af tcr a thrce-rninute pcl i r ld <i farrcst / cxtcrn: l l chcst cor lprcssion and vcnt i lat ion wcrc appl icd.Scvcn animals rcccivcd 45 pg/kg epincphr inc; a fur thcr ievcnanirnals rcccivcd 2.5 mg/kg dop:rrn inc; and thc rcmaindcr rcccivcdno r l rug thcrapy. Twcnty-c ight p igs wcrc rcsusci tatcd af tcr a fotr r -r r inutc pcr iod of vcntr icular f ibr i l la t ion. Scvcn animals wcrccicf ibr i l la tcd wi t l . rout c i thcr r .ncchanic:r l mcaslr rcs or drug thcrapy.Af tcr star t ing mcchanical mcasl l rcs, thc fo lkrwing du, tcs wcicgivcn bcforc dcf ibr i l la t ion to scparatc groups of sevcn i rnrmals cach:a5_ pg/kg cpincphnnc, 2.5 nrg/ l<g c lopar.r . r inc, or l0 nrL physio logicsal inc. Asphyxir l arrcst rcsul tecl . Al l thc anir ra ls g ivcn Jpincphr incc<rtr lc l bc rcsusci tatct l t r f tcr 174 ] 53 scconds. With dorrani inc. aspor. l t : lncol ls c i rculat ior . r could bc rcst t l rcd in 0nly thrcc of scvcnan in ta l s a f t c r 4 t JZ t ( r 3 sce r rnds . W i t ho r - r t d rug t he rapy , no c i r cu l a -t i on was cs tab l i shcd . Vcn t r i cu l a r f i b r i l l a t i on occu rcc l . I n t hc ab -scr . rcc of c i thcr t lnrg or r lcchanical nte asl r re s, only two of scvcn, ant lwi th urcchanical r lcasurcs only, four of scven rn i r .nals coulc l bcdcf ibr i l la tcd. In r ro casc could a spontancol ls c i rculat ion bc estab-l i shcc l . A f t c r i n i c c t i on o f cp i neph r i n r , t l c f i b r i l l i r t i on and r cs to ra t i o l . )of a spontancous c i rculat ior . r wcre achicvccl in s ix of scvcn animalstr l tcr 667 + 2l ( r scconcls, whcrcas wi th ckrpaminc, a l l animals couldbc s r , r cccss f r - r l l y r csusc i t l t c t l i n t he s i gn r f r can t l y sh ( ) r t c r t imc o f I 741 l l5 scconds. As r .ncasurcr l by thc rcsusci tat ion t in1c, cpincphr incis r .norc cf fcct ivc than ckrparrrr . rc in thc nranagcrncnt o i asphyxia larrcst . I l t contrz lst , a l l anir .nals i r - r which vcntr icular f ibr i l la t ion hadbccn inclucct l coulc l bc rcsusci t : r tcc l wi th dopan-r inc in a s igni f i -c : rnt ly shortcr t ime , possib ly bccausc tkrpaminc pcnctratcs sympa-thct ic ncrvc cndings i rnt l c : r t rscs thc rc le asc of s iorccl n, t r "1r i . t "p l . r -r inc. Simi lar rcsul ts wcrc obtainccl in a prcvious study r . rs ing norcp-incpl . r r ine .
177 Monitoring End-Tidal Carbon Dioxide as aPrognostic Index During CPB in Human BeingsAB Sanders, KB Kern, CW Otto, MM Milander, GA Ewy/College ofMedicine, University of Arizona, Tucson
Thc cf fcct ivencss of ongoing CPR cf for ts is d i f f icul t to cvaluate.Rcccrr t s tudics sul lgcst that carbon dioxidc cxcrct io l t may bc auscful noninvasive int l icator of rcsusci tat ion f rorn cardiac arrcst . Aprospcct ivc c l intcal stucly was donc to dctcrminc whcthcr cnd-t ic la lcarbon dioxidc moni tor ing dur i r - rg CPR could bc usccl as a prognos-t ic int l icator of rcsusci tat ion and surv ival . Thir ty- f ivJ cardiacarrcsts in 34 p:r t icnts wcrc r -nonrtorcd wi th capnornctry dur ing CpRovcr a ( )nc-ycar pcnod. Ninc pat lcnts who werc succcssful ly rcsus-c i tatcd had highcr avcragc cncl- t idal carbon c l iox ide part ia l Drcs-sures {P, , .CO,) dur ing CPR than 2(r pat icnts who c i ,u ld not brr csusc i t a t cd (15 + 4 vc r sus 7 + 5 mm Hg , / r . . 001 ) . Th rec pa t i cn t swho surv ivcd to lcave thc hosprta l had a highcr average p, ,CO,than t hc 32 nonsu rv i vo r s { 17 + a ) vc r sus l J + 5 mm Hg , p . . 05 } . A l 1ninc pat icnts who wcrc succcssful ly resusci tated had an avcragc
fr ,90, value_ of 10 mm Hg or more. No pat icnt wi th an rucrrg.Pr rCO, less than 10 mm Hg was resusci tated. Data f rom th is pro-spect ivc c l incral t r ia l indicate that cnd-t idal carbon t l iox idc rn i rn i -tor ing dur ing CPR is corrc lated wi th resusci tat ion and surv ivalf rom cardiac arrest .
-178 A Prospective Study of Helmet Usage on MotorcycleTraumaPJ Kelly, TG Sanson, GR Strange, EM Orsay/Division ofEmergency Medicrne, University of l l l inois, Chicago; LutheranGeneral Hospital, Park Ridge, l l l inois
59
Trauma resulting from motorcycle accidents accounts for a drs-proportionate amount of death and disability in motor vehicleaccidents. In our state, f rom 1982 to l9B5 motor cycle accidentsaccounted for 1.75"/o of all motor vehicle accidents while theyacounted Ior 12.6% of all fatal motor vehicle accrdents. We under-took th is study to def ine the ef fect of motorcycle helmet usage onthe morbid i ty , morta l i ty , and f inancia l impact associated wi thmotorcycle t rauma.Three hundred ninety pat ients were entere d inthc study who wcrc an avcragc agc of 26.5 years old, wi th 88.7%bcing male. Fi f ty-s ix 114.4%l pat ients were helmetcd vcrsus 334(85.6%) nonhelmeted. Nonhelmeted motorcycl is ts had s igni f i 'can t l y h i ghe r ISS ( l l . 0 l t 0 . 95 vs 6 .73 ! L46 , P = .037 ) . Pa t i cn t s whowcrc not hclmetcd suf fcrcd a disproport ionatc number of head andncck in jur ics (P =.013) and cxtrcmity-pclv ic g i rd le in jur ics (P =
.018). Nonhelmctcd pat icnts had a nonsrgni f icant t rend towardhighcr heal th carc costs {$6,623 vs $5,427,1 = .31). Of thc mostsever ly in jured pat icnts { lSS, 15), nonhelmeted motorcychsts hadsigni f icant ly longer hospi ta l izat ions and incurrcd grcatcr hcal thca rc cos t s t han hc lme ted cyc l i s t s {P = .0006 and P = .0001 , r cspcc -t ivc ly) . Thcrc wcrc 2(r fata l i t ics in thc study, of whom 25 wcrc nothclmctcd. Thc rcsul ts demonstratc that motorcyclc helmcts rc-duce the scver i ty of in jury and thc incidence of head and neckin jur ics as wcl l as cxtrcmity-pclv ic g i rd le rn jur ies. Further, heal thcarc costs and lengt l " r of hospi ta l s tay in the rnore scvcrc ly in jurcdpat icnts arc s igni f icant ly lowered by thc use of rnotorcylcc hcl -r -ncts. Final ly , our study demonstrated thc nccd of cmcrgcncyphysic ians to provic le thc publ ic and lcgis lators concrctc data t<rs l lpport mandatory safcty lcgis lat ion in our casc, thc usc ofmutorcyclc hclmets.
179 Comparison of Different Definit ions of Crit icalTrauma PatientsM Smith, K Cooper, D Morabito, C MayiDivision of Trauma,Highland General Hospital, The Bay Area Trauma Registry,Oakland, California
Thc opt i r -nal c lcf in i t ion of a cr i t ical t rauma pat ient , for cpidcmi-ologic as wcl l as qual i ty assLlranco purposcs/ is unclcar. Wc testcdthc fo l lowing proposcd def in i t ions of cr i t ical t rauma pat icnts onol l r cnt i rc populat ion of t rauma pat icnts t rcatcd dur ing a l2-monthpcr iod: 1 ) ISS rnore than I 5 or ISS of l0 or morc wi th a LOS of morcthar-r thrcc c lays or pcnctrat ing and ISS of l0 or mr)rc;2) ISS morcthar-r l 5; 3) AIS of 3 or rnorc for any body rcgron; 4) any pcnctrat ingtraulra proxi l r ra l to c lbow or kncc or AIS of 3 or morci 5) probabi l i tyof surv ival {POS) .90 or lcss {using TRISS rncthodology).
Del in i t ions
cause the risks, benefits, and time required to accomplish it remainunknown. We studied 70 consecutive patients with penetratingcardiac injuries to ascertain the relationships among prehospitalprocedures, time consumed in the field, and ultimate patientoutcomc. Thirty-one patlents sustained gunshot wounds, and 39sustained stab wounds. The mean Revised Trauma Score was 2.8 t0.5. Paramcdics spent an average of 10.7 t 0.5 minutes at the scene.Scvcnty-one percent o{ patients underwent endotracheal intuba-tion;93Y" had at least one IV line inserted, and57"/" had two IV linesinscrtcd. Twenty-one (30%) survived. There was no correlationbctwccn on-scene time and either the total number of orocedures(R = .17, P = . I7 l or the number of IV l ines establ ished {R = .06; P =
.(r). On-scene times did not di{fcr whether endotracheal intubationor pneumatic antishock garment applications were applied. Weconclude that well-trained urban paramcdics can perform multiplelrfc support procedures with very shott on-scene times and a highrate of patient survival and that prehospital trauma systcms rcquirea minimum obligatory on-scene time to locate patients and preparethcm for transport. Endotracheal intubation, IV cannulation, andpncumatic antishock garment application, performed in accor-dancc with advanced trauma life support protocols, do not addapprecrably to thc t imc elapsed in the f ie ld.
- 181 lmpact of Interhospital Air Transport on Mortality ina Rural Trauma SystemRC Campbell, K Corse, CR Boyd/ Department of Surgery, MemorialMedical Center, Inc, Savannah, Georgia
Air transport for thc seriously injured patient has long beenrccognized as an effective rnode of transportation to get patients todcfinitivc carc. Fcw studics, however, have examined the rmpact ofrntcrhospital air transport on mortality of the rural trauma patient.Wc rctrospcctively rcvicwcd l(r8 survivablc major trauma patientsdcf incd as having an In jury Scvcr i ty Score i ISSI bctwccn l5 and 60;pcdiatric pationts wcrc cxcluded. Trauma Scorc and ISS wcreobtaincd on cach paticnt. The probability of survival for eachpaticnt was dcfincd using thc TRISS mcthod of the Major TraumaOutcomc Study. Actual rnortality was compared with predictedmortal i ty . Pat icnts wcrc then div ided into outcome probabi l i tybins to cxaminc thc impact of air transport with respect to the lcvelof injury scvcrity. Our total patient population of l68 had a meanTrauma Scorc of 1 I and a mcan ISS of 29. The mcan probability ofsurv ival was 0.697. Fi f ty deaths were cxpcctcd, wi th 3 l observed.This 38.9'2, rcduction in mortality was significant to P < .00I lZ =4.64). Thc grcatest single reduction in mortality occurred in themost scrrously in jurcd probabi l i ty b in (ps < 0.25). Nineteen deathswerc obscrvcd in this group with27 expected, a 30% reduction inrnorta l i ty (P < .001, Z = 4.76). We conclude that a i r t ransport is ancffcctivc componcnt of prehospital care in the survivable, criticallyinjurcd paticnt. Air transport would seem to have its greatest effecton thosc paticnts who are most seriously injured.
182 The lmpact of a Regionalized Trauma System onTrauma Care in San Diego CountyFT Meyer, DA Guss, TS Neuman, WG Baxt, JV Dunford Jr, LDGriff ith, SL Guber/University of California, San Diego, MedicalCenter
Within thc last decade. manv communities across the UnitedStatcs havc introduccd {ormalized systems for the management oftrauma victin-rs. Thcsc systems have evolved in part as a conse-quence of several studies that have identified a high percentage ofprcvcntable death among trauma victims in communities withouttrauma programs. To assess thc impact of the trauma systemintroduccd in San Diego County in 1984, a review of the autopsyreports on all traumatrc deaths during the I986 calendar year wasperf ormed. All deaths occurring before or within one hour of arrivalat a hospital werc cxcluded, leavrng 21 1 cases for review. After ailreferenccs to hospital name and treating physician were removedfrom the rccord, a panel of six physrcians analyzed each autopsyrcport to determine if a death was preventable. When five of sixreviewers independently concurred that the death was preventable,it was so classified. Results were compared with a study of traumadeaths during the 7979 calendar year that used the same method-ology and physic ian reviewets. In 1986, two of 211 ( i%) t raumadeaths wcrc classified as preventable compared with 20 ol \77
l I I .4%) in 1979 (P < 001). One of 149 10.7%l centra l nervoussystem-rclated deaths was assessed as preventable in l9B5 com-pared wi th four of 94 (5%) in 1979 lP < .10). Of the 62 non-centra lnervous system-related deaths in 1986, one was believed to beprcventable compared with l6 of 83 non-central nervous system-
60
No. Pat ients 665Average ISS 21Average POS(%l 80No. deaths 142l\ilortalty (%) 21Operating room< 24 hours 254No. intensivecare admits 281Average intensive
2
38128
66 83 89139 142 1423 6 1 8 1 2
163 271 257
206 290 298
3 4 5 A t lPatientsTreated
787 1 ,193 161 2 ,1801 9 1 4 3 6 I
26 94121 1457 5 7
5 7 3 1 3
72 343
care days 1.86 2.91 1.58 1.05 3.03 0.60Blunt orpenetrat ing 1.00 0.93 1.28 0.59 0.53 1.90Average hospitalhospi ta l days 8.26 9.16 7.42 5.28 6.32 3.48lSS, Injury Severity Score; AlS, Abbreviated Injury Scale
Overall mortality for the e ntirc population w as7 "/"; yetttrungedfuom 7 5'k to 1 2 % depenciing on the dcfinition used. Also, wide dif -
ferences in acui ty, cnt ical resourcc ( intcnsive care and operat ingroom)usc, and ovcral l t rauma act ivr ty wi l l be perceivcd in the samepopulat ion depending on the def in i t ions uscd. Concensus needs tobc rcached on a standard definition if meaningful comparisonsbetween trauma centers as well as Datient care standards are to bcmade.
180 Prehospital Advanced Trauma Life Support forPenetrating Cardiac WoundsB Honigman, K Rohweder, EE Moore, SR Lowenstein, PT Pons/University of Colorado Health Sciences Center, Denver; DenverGeneral Hospital
Prehospital advanced trauma life support is controversial be-

re lated deaths in 1979 (P < .0051. Dur ing the interval between l9Z9and I986, a formal ized system of t r rurni care was introduccd in SanDiego County. Analysis of traumatic deaths occurring frvc yearsbefore the institution of the trauma system compared with deathsoccurring two years after the introduction o{ the system revcaled adrop in the preventable death rate f rom l l .4"k to I .0%.
-183 Comparison of Cimetidine and Diphenhydramine inthe Treatment of Acute UrticariaR Moscati, G Moore/Department of Emergency Medicine, DarnallArmy Community Hospital, Fort Hood, Texas
Recent case reports have suggestcd that H, antihrstamines, usccla lone, may be ef fect ive in the t reatment of acute ur t icar ia, acommon emcrgency departmcnt complaint . This contradicts ac-cepted doctr inc on thc t reatmcnt of acute ur t tcar ia. Bascd ontheor ies of H, - and H, - reccptor intcract ion at the cel lu lar lcvel , i t hasbeen stated that H,
-b lockadc before H, b lockadc may cxaccrbatc
s_ymptoms. Thc puiposc rrf our study was t() colnparc diphenhy-dramine, an H, b locker, and c i rnet id ine, an H, b locker, rn a iandorn-izcd, prospcct ivc, douhlc-bl ind c l in ical t r ia l . Nincty- thrce pat icntsprcsent ing to thc ED wi th c l in ical cv idcncc of acute ur t rcarra wcrctreated wi th c i ther 50 mg diphcnhydraminc or 300 mg ci rnct id incIM. Pat ients ' s igns and symptoms wcrc quant i tatcd on a numcr icalscalc before rcceiv ing medicat ion ancl 30 minutcs af tcr t rcatmcnt.Parameters measured includcd degre c of i tchi r - rg, rntcnsi ty of whcals,dcgree of sedation, extcnt of whcals, ancl l.rcrception of ovcralitmprovcment. Usrng analysis of var iancc for stat is t rcal cvaluat ion,both rncdications provided signifrcant relief of itching and whcaiintensi ty (P = .000 1 ) . Scdat ion was causcd by both diphcnhydran-r inc(P = .0001 ) and c imc t i d i nc ( 1 , = .00051 . Howcvc r , t l . r c dcg rcc o fsedat ion causcd by diphcnhydraminc was s igni f icant ly grcatcr thanthat caused by c imct ic l inc {P = .0001). Thc perccpt ion of ovcral llmprovcmcnt was grcatcr wi th c imct id inc (P = .0t t21), wi t l - r l lZ,Z, ofthcsc pat icnts rcport ing somc improvcmcnt, wh|rc76, '1, of d iphcnhy-draminc-t rcatcd pat icnts rcportcd imptovcmont. Our resul ts indi-catc that c i rnct id inc is cf f icacious as thc in i t ia l t rcatmcnt of acl r tcurticaria and has less tcndcncy towarcl scdation. Furthcn.norc, untlcrc losc obscrvat ion, c imct id inc drd not cal lsc any cxaccrbat ion ofsymptoms or untoward s ic ic cf fccts. Wc advocatc considcrat ion () fc imctrd inc as a rapid, lcss-scdat ing antrh istaminc for usc i r - r thcin i t ia l t rcatmcnt of acutc ur t icar ia. I ts usc may cncouragc grcarcrcornpl iancc ancl lcss rncdicolcgal r isk in thc arnbulat() ry par ieut .
184 Cimetidine in the Treatment of Acute AllergicReactionsJW Runge, JC Martinez, EM Caravati, SG Will iamson, SC Hartsell/Department of Emergency Medicine, Charlotte Memorial Hospitaland Medical Center, Charlotte, North Carolina
Cimct id inc, an H, b lockcr, has bccn rcportcd to bc an cf fcct ivctreatmcnt alonc or in combination with dirrhenhvclraminc for ircutcal lcrg ic rcact ions. Wc studict l 39 pat icnts in a randornizccl c loublc-bl ind protocol to assess thc cf f ic tcy o{ c inrct id inu comparcd wi thdiphcnhydramine. Mcdicat ions wcre givcn intravcnously: Group I(N = 14), d iphcnhydraminc 50 mg and placcbo; group 2lN = l2) ,cimctidine 300 mg and placebo; and group 3 (N = lg), dipl.rcnhydrarn-ine 50 mg and cimetidine 300 mg. Patrcnts ancl examincrs asscsscdsymptons and s igns of a l lcrg ic react ions using an l l -cm visualanalog scale (VAS) be{orc and 30 rn inutes af tcr t rcatmcnt. I tchinsand urt icar ia occurred wi th suf f icrent f rcc lucncy for stat isr iealevaluation. A significant symptom was dcfiniJ as .l cm or morc onpretreatment VAS and relief as a decrcasc of 2.5 cm or rnorc aftcrtreatment. Mean drffcrences in VAS score s wcrc analyzctl usir-rg thctwo-way Student 's f tcst , and prcsencc of rc l ic f was tcstcd using thcFisher 's exact tcst . Of thc 35 pat icnts wi th i tching, I2 oI lZ l I00%)receiving diphcnhydramine-placcbo had rclicf cornparcd with six often (60.0%) of thc pat ients rcceiv ing c imet id inc-pl iccLro (r tost , 1) =.02; Fis l rer 's , 1r = .029). Al though I 1 of 12191.7"1,)rcceiv ing diphcnhy-dramine-cimetidine had rclief, thc differencc betwccn ihis comhi-nation drug group and the single drr-rg groups was not significant{Fishcr 's , P =. I2) . Of 33 patrents wi th ur t icar ia, f ivc of 1 l (45.5%)receiving diphenhydramine-placebo had relief compared with cightof ten (80.0%) receiv ing c imct id ine-placebo {NS; Fisher,s, p = . i8) .Of those receiv ing diphenhydramine-cimet id ine, l l of 12 (91.7"/ , , )had relicf, significantly bctter than diphenhydrarnrnc alone (r tcst,P = .006) Fisher 's , P = .O27). We conclude that in pat ients wi th acutcallergic reactions for itching, cimctidine alone or in cornbrnationwith diphenhydramine is no more effective than diphenhydraminealone; and {or urticaria, cimctidine is cffective, and its combination
with d iphenhydramine is bet ter than diphenhydramine alone.
185 Early Detection of Acute Myocardial Infarct ion:lmmunochemical Determination of CreatinePhosphokinase-MB Versus Standard ElectrophoresisWB Gibler, LM Lewis, RE Erb, WB Campbell , R Vaughn, AVBiagini, J Blanton/Division of Trauma and Emergency Medicine,Section of Surgical Sciences, Vanderbi l t University School ofMedicine; Departments of Pathology and Cardiology, St ThomasHospital, Nashvi l le, Tennessee
Thrcc immunochemrcal methods for dctcct ion of creatinephosphokinasc (CPK)-MB and standard e lcctrophorcsis werc cvalu-atcd for thcir abi l i ty to diagnose acutc rnyoiardial infarct ion inpaticnts prcscnting to the emcrgency departmcnt with chcst pain.Serum samplcs werc analyzcd for CPK-MB by the four mcthods(Corning Magic Litc- , Baxtcr Stratus" f luororrctr ic inrrnunoassav,Hybritcch Tandcm-E-, and Hclcna REP- at zero hours lprcsenta-t ior-r to thc ED) and at thrcc hours aftcr prcscntat ion on 200 totall )a t i t .n ts . A [ tc r exe ]ud ing r rans fer nn tL ED d ischarge p l r ren ts ,curnplctc data wcrc avai lablc on 90 patrents. Using the hospitaldischargc sumn-rary as thc standard, 13 of t l -rc 90 wcre posit ivc foracutc myocardial rnfarct ior"r. Thc fol lowinc tablc summarizes thcclat:r for zcro :rncl thrcc hours, wit l"r scnsit ivi tv and spccif ici tv asnotccl:
Sensitivity Specif icityMethod (0 hr) (0 hoCorning 61.5% 97.4kBaxter 61 .5% 87.0"kHybr i tech 53.8% 97A%Helena 46.1"k 98.7"k
Sensitivity Specif icity(3 hr) (3 hr)100ak 94.80k100% 85.71"100% 91 .0%
61 .50/" 98.7"k
Thc scnsi t iv i ty of a l l i r lmunochcmical rncthocls was 100,2, atthrcc hours cor"nparcd wi t l - r ( r l .5"1, lor c lcctrophurcsts. A 100,2,ncgat ivc prccl ic t ivc valuc was obtai r - rcd by thc thrce intn lunrr-chcrnical l rc thods at thrcc hours af tcr prcscntat ion. As thc hospi-ta l d ischargc diagnosis of acutc n.ryocarcl ia l infarct ion was basc. lon c lcctrophorct lc analysis of CPK-Mi l , i t is possib lc sourc of thc"fa lsc-posi t ivc " dctcrnt ina t i , rns by the rr r t r r t i srnsi t rvc l l lmLlno-chcrnical l rc thocls actual ly dctcctcd srnal l in farct ions. Rarr ic lt lc tcct ion of : lcutc uyocardia l infarctron of fcrs r .nany poteni ia laclvantagcs to thc cnlcrgcncy physic ian. Ear ly d iagnosis, whi lc thepat icnt is in thc ED, woulc l a l low appropr iatc d isposi t iun of thcpatrcnt wi th acutc n ' ryocarcl ia] infarct ion to t l rc intensivu carcsct t ing. Potcr-r t ia l ly , c l iagn<ts is ( } f : rcutc r l lyocarc l ia l infarct ion wi th ina_ s ix-hour pcr iocl af tcr syutptoln onsct r ray al low thron-rbolyt icthcrapy to bc givcr-r to pat icnts wi t l - r acutc my0carcl ia l infarct i ( ) r - rn ( ' t h i l v i r ' r g t l i agno : t i c FCCs .
-186 Use of Indomethacin Suppositories in theTreatment of Ureteral ColicS Melanson, S Weitzel, J Gil len, D Kapoor, J Mowad/Departmentsof Emergency Medicine and Urology, Geisinger Medical Center,Danvil le, Pennsylvania
Urctcral col ic can bc a di f f icul t pat icnr nan: lgcrrcnt problcmin thc cmcrgcncy c lcpartntcnt . Prcscnt t rcat lncnt consists of hy-c l rat ion ancl symptomat ic pain contro l wi th narcot ic analgcsics.Urctcral obstruct ion causcs rc lcasc of prostaglandins that increascrcnal b lood f low ancl g lorncrular f i l t rat ion, thcrcby incruasingurcte ra l wal l tcr . ts ton proximal to thc obstruct ion and causing thcpain of urctcral col ic . By inhib i t ing prostaglandin synthcsis, in-domcthacin b locks th is cf fcct and has bccn shown to bc cf fcct ivcin rc l rcv ing urctcral col ic wl-rcn givcn IV in Europcan studics. Wccondtrctcd a prospoct ivc, dt 'uhlc- t r l ind, p lacch, , - iontro l lcd studycxamining thc cf f icacy of indomethacin sul . rposi tor ics in ru l icv ingcol ic seconclary to radiographical ly documcntcd urctcral calcul i rnan outpat icnt set t ing. Patrents wcrc randomized to rcccive surr-posrtor ics {e i thcr indorncthacin or p laccbo) evcry c ight ht '115 2p6supplcmcntal narcot ics (acetarninophcn-oxycodonc) to L lsc asnccded. Pain cor-r t ro l was assessed by the numbe r of supplementalnarcot ic tablcts used by cach pat icnt each 24 hours. Forty-oncpat icnts wcrc entercd into thc study protocol wi th cornplctcfo l low-up avai lablc or-r 2(r pat icnts. Al l 13 pat ients in the contro lgroup had recl l r rcnt cpisodcs of col ic , n ine of thcsc having morethan onc episode. Five of thc l3 contro l pat ients rcquired hoip i ta l i -zatron for pai n contro l . Four of thc I 3 pat icnts in thc indomcthacingroup had recurrcnt colic, witl-r only one having more than oneepisode. No patrent in thc indomcthacin group requircd hospi ta l i -
6 l

zation for pain control. Overall, the ratio of supplemental narcot-
ics used by the placebo group versus thc indomethacin group was
7.6: l lP. ' .OOSJ. The mian t ime to calculus passage was s l ight ly
shorter in the indomethacin group (ti2 versus 89 hours), but this
dif{crencc was not statistically significant. Our results support the
use o{ indomethacin suppositories in the treatment of recurrent
colic secondary to ureteral calculi.
187 Indomethacin for Rel ief of Acute Renal Col ic
AB Wotfson, DM Yealy/Hospital of the University of Pennsylvania;
Univers i ty of Pi t tsburgh Af f i l ia ted Residency in Emergency
Medic ine; Center for Emergency Medic ine of Western
Pennsylvania, Pi t tsburghEaily studies have suggcsted that indomethacin can relieve
renal colic by a mcchanism of action different from that of narcot-
ics. If effcctivc, indomethacin would offer the potential advantagc
of avoiding narcotic side cffects such as alteratlon of mental status'
We prospcct ively adrnin istcred oral indomcthacin (50 mgJ to 25
nonvomiting patients with acutc renal colic due to a documcnted
stonc. Elcven pat ients (group l ) recclved indomethacin in an
unblindcd, noniandomized fashion aftcr failure of oral or paren-
teral narcot ics to re l icve pain. In I4 addi t ional pat ients (group 2) ,
indon-rcthacin was givcn as the only initial trcatmcnt. Pain inten-
s i ty bcforc and af te i t rcat lnent was rcported using a 1 - to-10 scalc '
I n g roup I pa t i cn t s ,pa indcc reascd f rom 5 .U12 .7 to3 . ( r t 3 U (1 '< 02 ) '
Six'of the I 1 paticnts rcportcd a dccrease in pain intensity of 50.o1',
or morc, whi ih occurrcd wi th in 25 + 1i minutes. In no pat ient d id
pain incrcasc. In five of thc six obtaining rclicf, pain dccrcased to a
b or 1 lcvcl. Among the I 4 paticnts in group 2, pain decrcascd from
7.(r i 1.5 to 4.6 + +.0 ( t ' . .00S). Eight of the 14 roportcd a dccreasc
in pain intcnsi ty of 50'2. or morc, which occurrcd wi th in 40 + 14
minutcs. In f ivc of thc e ight , pain dccrcascd to a 0 or 1 lcvcl ln no
nat icnt c l id pain incrcasc; fur thcr analgcsia was rcclurrcd in the s ix
nat i "nts whosc pain d id not rcspond to indomethacin. Pat icnts who
icsp,rnclcd to indotncthacin werc dischargcd on oral indorncthacin '
Al i wcrc able to cont inuc wi th dai ly act iv i t ics; oniy onc had
returncd for further pain control at onc wcck follow-up - Two
pat icnts succcssful ly t ieatcd fur ther cpisodes of rcnal col ic at homc
with oral indomcthacin. Thcse promrsing preliminary observa-
t ions suggcst that p laccbo-contro l led studics arc warrantcd to
dcfinc ttLc appropriaic rolc {or indomethacin and similar agcnts in
thc managcmcnt of acutc rcnal col ic .
-188 Stabil ization of Unstable Pelvic Ring Fractures WithMilitary Anti-Shock Trousers: A RadiographicAssessmentCC Huerla, G Polando, J Shall, J Glauser/Emergency MedicineResidency Program, Departments of Orthopaedic-Research andOrthopaeiic Surgery, trl i Sinai Medical Center oi Cleveland, Ohio
The benefits irf military anti-shock trousers (MAST) in hcmody-rlarnically unstablc paticnts with pclvic ring fracturcs arc wcll
du..rrrr"r,t.,1. Howcvcr, this literature and EMS guldclines also
advocatc the use of MAST as a skclctal stabilization devicc lt is
bclicvcd that MAST imrnobilizes the pclvic ring by acting as a large
air splint. No study documcnts, eithcr quantitativcly or- quaiita-
tivcly, evidencc that MAST can adequatcly perform this function'
Furthermorc, the potential for creating new darnage, or thc-agg{a-
vation o{ n.gnn "ni soft tissue injurics, has not been asscssed This
.trl,ly "*a-incs radiographically- whethcr bonv stability o{ thc
nclv is is achicved by MAST A cat laver ic modcl was dcvelopcd-and
i.ruu.n ,o sitnulate a human unstable pelvic ring {racture Thrcc
iudaue.s found by radiographic examination to be {rcc of pelvic
bone disease o, fiactr.trc-serrred as models. Five types of unstable
pelvic ring fractures, simulating worst casc instability, were surgi-
cally induccd. For ihe most unstablc fractures, both blunt and
obliquc anglc bone cuts were produced. External leg rotation to 90'
and abduction to 50'{rom midline were used to represent extremes
of expected prehospital motion. Anterior-posterior and inlet views
*ith'r.tpp1.-entaioutlet view documented pelvic ring instability'
Radiogr'aphic assessment of pelvic ring motion was carried out
beforc" and at end-manrpulaiion, both with and without each
cadaver in MAST. EMS personnel aided in the application and
inflation of MAST to ensure conformity with current protocols'
Radiographic evaluation proved MAST was- effective in reducing
and siabilizing each unstable pelvic ring fracture With proper
MAST inflatio*n, pelvic ring staEility under extreme manipulation
was maintained. in every fracture type, bony distraction of up to 6
cm was completely reduced with MAST. In addition, with MAST
inflated, even extreme manipulative force failed to reproduce
fracture end-distraction. At no time during MAST use was the
fracture ovcrreduced or did pelvic ring collapse result. The authors
find radiographic evidence fo s.tppott the use of MAST in stabiliz-
ing the unstable pelvic ring fracture.
189 Neutrophi l-Mediated Microvascular InjuryDL Carden, JK Smith, RJ Korthuis/Department of Physiology andBiophysics, Louisiana State University Medical Center; Cl inicalDepartment of Emergency Medicine, Schumpert Medical Center,Shreveport, Louisiana
Recent studies implicatc polymorphonuclear neutrophils in the
microvascular injury that occurs on reperfusion of ischemic tissue'
Bcfore tissuc extravasation and microvascular injury, circulatingneutrophils adhcre to the microvascular endothelium and become,"tivrt d. Thc purpose of our study was to delineate the role of
ncutrophils in producing microvascular injury in isolated canine
lracilii mrlscl. after a frolonged ischemic insult The effect ofncutropenia was examined using specific antisera raised againstcaninc neutrophils. The antineutiophil serum reduced theperiph-cral white blood cell count to less than 5% of control values' In
addition, the rolc of neutrophil adherence was addressed by admini-stcrins a monoclonal aniibody specific for the B-chain o{ theneutrdphi l CD18 complex (IB.). Bv binding with the CD18 com-plcx, IB. interfercs wiih ncutrophi l adherence and. extravasation'.fhe'snliret'tt drag reflection cocfficient (o) was used as an index ofthe scverity of riiicrovascular injury and is a sensitive measure of
changes ininicrovascular permeability. The o was determined {or
the fJllowlng conditions: control (no ischemia), reperfusion after
four hours oi-ischemia, reperfusion a{ter four hours o{ ischemia in
ncutropcnic dogs, and reperfusion a{ter four hours of ischemia in
dogs trcated with IBo.
GroupControllschemia/reperf usion (l/R)l /R, (neutroPhi l dePlet ion)r/R, (rB")
o0.99 r .08U , O U f , U Z
0.99 t .051 .0 r . 03
Rcpcrfusion aftcr {our hours of ischemia resulted in a significantdcircasc in o, indicating a dramatic increase in microvascular
fcrmeability. Neutrophil depletion or preventron o{ neutrophil
ndh"..n". prevented ihe inciease in microvascular permeability
sccn in untrcated animals. The results of our study indicate that
ncutrophils mediate postischemic microvascular injury and that
t.ntto-phil adherence to the microvascuiar endothelium is a pre-
recluisile for the production of this injury.
190 The Detrimental Effects of lv crystalloid AfterAortotomy in the SwineWH Bickell,- SP Bruttig, CE Wade, P Maningas, GA Millnamow/Letterman Army Institute of Research, Presidio ol San Francisco,Cali fornia; Trauma Service, Saint Francis Hospital, Tulsa,
Oklahoma- ihe obiective of our study was to test the hypothesis that after
aortotom, attempting to iapidly replace the estimated blood
unl,r-. a.ii"lt *iitt IV crystailoid will increase hemorrhage and
decrease survival. Sixteen anesthetized Yorkshire swine under-
went splenectomy and statnless-steel wire placement in the ante-rior in{rarenal aoita and were instrumented with Swan-Ganz and
carotid artery catheters. The wire was pulled, producing a-S-mm
aortotomy and spontaneous intraperitoneal hemorrhage' The ani-mals were randomly assigned to tlie untreated control group (eight)
or the lactated Ringer's group (eight), which received 80 ml/kg
Rinser's IV. The lactatedhinger's in{usion was initiated 6'5 min-
utes after aortotomv and infused at a rate o{ 8 ml/kg/min lrom
lasel ine to f ive minutes after aortotomy, there was a profound
decrcase in cardiac output, mean arterial pressure, and mean
oulmonarv artery pressure in both groups. The administration of
iactatcd Ri.tg.t ' t produccd a biphasic hemodynam-ic response as
cardiac output, meatt artetial pressure/ and mean.pulmonary afterypi.rr".. sign#icantly {P < .05), increased, and then subsequentlyFell srsnific;ntlv (P <'.05] below that of untreated control animals'ih. ,iolrr-. of'hemorrhage and the mortality rate were signifi-
cantly (P < .05) increased in the Ringer's treatment group 12,142 !
178 veisus 783 t 85 mL, and eight of eight versus zero o{ eight,
iespectively). From these data, we conclude that in this model of
r,rttcotrtroll.d arterial hemorrhage resulting from abdominal aorto-
tomy, the rapid administration of IV lactated Ringer's signilicantly
62

increases hemorrhage and mortality.
-191 An Evaluation of the Diagnostic Capabil it ies ofMagnetic Resonance lmaging With a Comparison toComputerized Tomograptty in Acute Spinit ColumnInjuryA E Flanders, M A LevitVEmergency Service, Thomas JeffersonUniversity Hospital, Philadelphia, pennsylvania
Recently, magnetic resonance (MR) imaging has become auseful adyunct in diagnostic evaluation of suTt t]rr.rc pathology.Plain radiographic and computed tomographic (Cf) scanning iiethc prcsent standard of care in evaluation of spinal column inlury,.Where CT scanning demonstrates presence ,rr,l "*terrt of skcletalinjury better than plain radiography, both have been limitecl inprovldrng rnlormation regarding prcsence and extent of soft tissueinjury, primarily concerning the spinal cord and intervertebraldiscs. Our study_was conducted to evaluate the diagnostic capabili_ties of MR in the sctting of acutc spinal column injury and tocompare these results with those oJ CT scanning. Our studyinstitution is a Lcvel I and regional spinal cord trauma ccnter. Thesample population included 49 patie;ts undergoing MR to cvaluatesuspected spinal column injury. Thirty-thrce-of th-esc paticnts haclboth MR and CT_cvaluation, and resJlts wcre con-rpaied. Level oirnjury as imaged by MR and CT scanning ranged from C2 through
!]r.Sgven percent (five) of the injuries -brc ai'C2, Z% {fivc) at i3,
20% l l 4 l at C4, 37 % 126l at CS, 23 % l l7 ) at C(r , and S y" l f our ' I at C7' .Seventy-one injuries were idcntificd by MR imaging. Thesc inju-ries were classificd as fracture-dislocation (2 I ), disc herniation (29),and spinal cord cdema-contusion-t ransect ion (21). Diagnost i iimaging results of patients undergoing CT scanning and MR werccompared. CT scanning dcmonitratcd 22 hactiie_dislocationscompared with ten on MR. MR demonstratcd l9 disc protusionscompared with seven on CTscanning. Additionally, MR imagcd l3cord injuries comparcd with zero by CT scanning. f t wcightcdechospin sequcnce imaging provcd'bcst for osscous injury an<ihemorrhage. T2-weighted echospin sequcncc imaging dcrnonsira tcdspinal cord edema best. GRASS imaging p.uu".l-bcst for discherniation with its myelogramlikc cfJeci.
'MR irnaging provcrl
superior in demonstrating spinal cord pathology and intcrvcitcbraldlsc hcrniation. CT scanning was supcrior to MR in dcmonstratinsosscous in jury. CT imaging and MR imaging can l re uscf u l togcthc:rrn dctcrmining prcscncc and cxtcnt of spinal column in iury.
.192 Effect of Hypertonic Versus NormotonicResuscitation on Intracranial pressure After CombinedHead lnjury and Hemorrhagic ShockCB lrvin, SA Syverud, SC Dronen, CR Chudnofsky/Department ofEmergency Medicine, Universily of Cincinnati Medical Center
Vigorous fluid resuscitation of hemorrhagic shock may rncreasccerebral cdema in patients with concomitant closed_he.d ir.ryr,.y.Because hypertonic resuscitation (HTRJ results in fluid shift iromthe extravascular to thc intravascular compartmcnt/ lcss ccrebraiedema and lower intracranial prcssurc (fil1 migni be observcdwhen compared with normotonic rcsuscitation (Nfn). Immatureswine (15 to 20 kg) werc instrumented under halothane ancsthcsiaand splenectomized. Aortic, central venous, and intracranial pres_sures were monitored. At t : 0, blunt injury to the right cerebralhemispherc was induced with a fluid percuision dcvice. Simulta_neously, hemorrhagic shock was induced by rol lcr purnp with_clrawal trom the arterial catheter of 307" oI blood volume bver 30minutes. At t : 35, resuscitation was initiated with 0.9% saline 3ml/k_g/rnin (NTf., n = 4) or Dextran 7O,t' - 7.5"/o saline 0.36 mLlkglmin (HTR,-n = 4) for 20minutes. Both groups were hypotensive it!!q 9"d of hemorrhage (mean arterial pi.srrr. range, 40 to 60 mmHg) but n-o_rmotensivc by t = 45 (rnean arterial pr.rr'rr" range, 90 to-t]! mm.Hg) Ar t : 45, ten minutes after the siart of resuscitation,ICP in the NTR group (63 I 2l mm Hg) was significantly higherthan.in the HTR group l2Z ! t4 mm Hg) {p < .05, unpaired r Gst).Cerebral perfusion pressure was signifiiantly highei in the HTRgro-up at t : 45 174 t 9 versus 47 ! 17 mm Hg) (p < .051. Thesedif{erences gradually resolved during subsequeni ieinfusion of shedblood. I hese ollservations suggest that HTR may decrease cerebralede.ma during fluid resuscitaiion of combined hemorrhagic shockand closed-head injury.
193 Effect of Ghemical interventions on Cerebral EdemaFormation After Head Trauma in Rats
IrlH Biros, R Nordness/Department of Emergency Medicine,Hennepin County Medical Center, Minneapol is , Minnesota
, Morhidity af ter significant head trauma depencls in part on the
degrte ol cerebral edema that develops in the period immediatelya{ter the injury. The goal o{ our research was to compare the effectsof var ious chcmical intervent ions on reduct ion of ierebral edemaaftcr head trauma in the rat. Adult male Spraguc_Dawley ratsweighing 350 ro 450 g were anesthetized with kelamine { l0b mg/kg IP,) and underwcnt right ternporoparietal craniotomy. A 2_cml.ength ot polyethylene tubing ( ID, 5.8 mm) was posi t ioned perpen-dicular. to the exposcd intact dura through the cranrotorny srte,secured wrth methyLncthacrylate, and filled with normal ialine.Animals were al lowed to stabi l ize for ten to 15 minutes. Hcadtral r rna was then produced by a f lu id pcrcussion systcm at tachcd tothe trauma cathcter that delivcred aitandarcl pr".rr,r. wave {prcs_surc, 0.5 atm) to the under ly ing brain t issue. Exper in-rental ani inalsreceived one o{ thc fo l lowing drug t rcatmcnt i : dcxamcthasone(DM), 0.30 rng/kgIV; d ichloroacctate (DCA), 25 mg/kg Ip { reduccst issuc lactate product ion and accumulat ion), 1. . ; -Uutanediol (BD),47 nmlkg, IP (rcduccs t issue lactatc product ion and is osmot ical lyact ivc) , manni to l , I g/kg IV. Ip and IV in jectrons werc del ivcred tenminutcs and immediately beforc t raunta, respcct tve ly . The cxper i_mental t reated animals (srx) wcrc "ntop"r id wi th t raumat izcdcontrol animals that reccived thc samc volumc of normal salnc{NS) placebo by the same routc and wi th nontraumat ized contro lanimals that rcccrvcd thc samc study drug or NS. Six hours af tcrhcad t rauma, thc anin-ra ls wcrc k i l icd, and cort ical t issuc washarvcstccl for mcasurc of t issuc spcci f ic gravi ty. Samplcs wcrecollcctcd from tl-rc trauma sitc and fiorn a crirrcsp<inding arca of thcopposi tc cortex. Nonc of the study drugs af fcctcd ihc spcci f icgravi ty of cort ical t issuc in nontra l lmat izcd t rcatcd animals. Thcspcci f tc gravi ty of cort ical t issuc f rorn thc contracoup s i tc oft raumat izcd animals d id not d i f fcr f rorn thc spcci f ic g iavi ty oft issuc f rom nontraumat izcd t rcatcd or contro l animals. '
Experimental ConditionWith Study Drug(N = 6 for each group)Trauma + drug intervention
Trauma - drug intervent ion
Significance (ANOVA)( N o n t r a u m a + N S = 1 . 0 4 0 )
Trauma Site Specilic Gravity (g/mL)
DM DCA BD Manni to l1 .035 1 .037 1 .039 1 .037
1 .033 1 .033
P = N S P < . 0 5
1 ,033 1 .033
P < . 0 5 P < . 0 5
-t"
Highcr spcci f ic gravi ty of cort ical t issuc f rom anin-ra ls t rcatcd wi thmanni to l , DCA, and BD indicatcs lcss watcr contcnt of thcsctissucs and suggcsts a protcctivc cffcct of thcsc drugs frorn dcvclop_mcnt of ccrcbral cdcna six hor-rrs aftcr hcad trauma in rats.
194 Oral lntubation in the Multipty tnjured patient: TheRisk of Exacerbating Spinal Corci DamageKJ Rhee, W Green, JW Holcroft, JAA Mangil i/Division ofEmergency MedicineiOlinical Toxicology, D,epartments of InternalMedicine and Surgery, University of Caiifornia, Davis, MedicalCenter, Sacramento
The use of oral intubation during the resuscitation of seriouslyin jurcd pat icnts has bccn discouragcd bccause of thc fear that th istcchnique may lcad to cervical cord darnagc. Our abstract reportsthe. 18-month cxpertcnce of an erncrgency dcprrt-"rrt in whichoral intubation was the usual rnethod nf uii."ny.u.rtrol for victimsof blunt trallma. There were 237 injured paticnts intubated in theED; 2l pat icnts {8.9% ) had ccrv ical cord oi bone rn jury. Thcre wercno paticnts in whon a neurologic loss followed an airway mancu_ver. Oral intubat ion was the dcf in i t ive ai rway maneuvcr in 213p.at ients {89.9%1, nasal intubat ion in I Z pat icnt s 17.2%), and cr ico_thyrotomy or tracheotomy in scven paticnts li.q"/"l. Ot d1c Zlpatients with cervical injury, oral intubation was the definitrvcairway maneuvcr in l7 pat ients (81.0%), nasal intubat ion in twopat ients 19.5%), and cr icothyrotomy in two pat icnts (9.5%). Thesetwo cricothyrotomies were performed because nasal and oral intu_bation had failed. The risk of spinai cord injury ,..ondrry tn orrlin t r rbx66l in thc ser iously in jurcd pat ient ls low. Select ion of themcthod ior dctinitive airway_control should be based primarily onthe operator's particular skills and cxperience rather than the fearof inflicting cervical cord damage.
195 Factors lnfluencing Neurologic Recovery AfterCardiac Arrest
63

N Abramson, P Safar, K Detre, the Brain Resuscitation Clinical Trail
(BRCT) ll Study Group/lnternational Resuscitation Research
benter, University ot Pittsburgh; 20 hospitals in eight countries
Neurologic damage has been reported to occur rn 20y" to 4O"/o
of lone-term-cardiac arrest survivors' The recent completion of the
seconl ohase of an international randomized clinical trial of brain
resuscitation provides additional in{ormatron. Data from 5l(r
comatose t.t.uivott of cardiac arrest, including details concerning
baseline medical history, brain insult, and the resuscitation proc-
ess, were analyzed to identify independent predictors of subse-
quent neurologic recovery. Mortality was,,9}"k 1423 oI 516). Of
ihose who survived the entire six-month follow-up perio d' 7 6% 17 |
of 93) were able to function independently Good neurologic func-
t ion was recovered by 23% { 121 of 516) of the ent i re study popula-
t ion at some t ime dur ing fo l low-up. An addi t ional 9% 147 of 516l
awakened but never achieved good neurologic function. Thc re-
maining 667" 1342 o{ 516) never regained consciousness. Factors
positiveiy associated with good neurologic recovery/ in both uni-
variate and multivariate analyses, were cardiac cause of arrest,
arrest t ime of less than f ive minutes, and CPR t ime of 15 minutes
IaI1 P =.01). These resul ts conf i rm the f indings of our previous
clinical trial, parallel reported predictors of mortality after cardiac
arrcst, and trlggcst areis for improvement in the treatment of
carolac arrcst .
.196 Coronary Perfusion Pressures During CPR AreHigher in Patients With Eventual Return of SpontaneousCirculationTJ Appleton, N Paradis, GB Martin, D Bovell, MG Goetting, EPRivers, RM Nowak/Departments of Emergency Medicine andPediatr ics, Henry Ford Hospital, Detroit , Michigan
Work in animal models of cardiac arrcst has demonstratcd thatthc aortic to right atrial pressurc gradicnt during CPR rclaxationphasc (Ao-RAl is the co.unaty perfryr91 pre.ssure. It has been
nositivcly corrclatcd with myocirdial blood {low and return ofipunt".t.ir.tt circulation (ROSC). Thc purpose of our study was tomeasurc Ao-RA during cardiac arrest and compare this in pationtswith antl without subicqucnt ROSC. Adult medical cardiac arrcstpaticnts ((r 1 J, of a mcan age of (r3 + 1(r years, had aortic arch and rightcathetcrs placccl and simultaneous prcssurcs recorded. Mean init ialand maximal Ao-RA gradients wcrc mcasurcd and compared(studcnt 's t tcst {or unpi ire d samplcsJ. Down t ime avcragcd 15 t l4minutcs. Timc from arr ival to cathctcr placemcnt was 14 + 5minutes. Fif tv-one patients had no ROSC; ten had ROSC'
millimeters of mercury for patients in whom catheter placementwas con{irmed radiologically (two). Baseline Ao-RA was 4.9 + 6 6before standard dose, and 5.6 t 8.4 before high dose (not statisticallydi{ferent, P = .54, Student's t test paired samples). The meanmaximai increase in these gradients was 3.4 + 5 (range, 2to l2l afterstandard dose and 1 1.8 t 10.7 (range, 0 to 45) after the high dose (P= .001). Four Datients had ROSC after receiving high-dose therapy.High-dose epinephrine significantly increases the Ao-RA gradientduiing CPR in human beings, which may improve myocardialblood flow and rates of ROSC.
198 Extreme Systemic and Cerebral Oxygen ExtractionDuring Human CPRMG Goetting, EP Rivers, NA Paradis, GB Martin, T Appleton/Departmenti of Pediatrics and Emergency Medicine, Henry FordHospital, Detroit , Michigan
We quantified systemic and cerebral oxygen (Or] extra.ction in19 adulis undcrgoing CPR for cardiac arrest. fugular bulb, rightatrial, and aortii arch catheters were inserted during CPR withposition conlirmed later radiographically. CPR was performedaccording to advanced cardiac life support guidelines. Patients withhemoglo6in of iess than 9.O gldL or arterial hypoxia (SaO, < 0.80)were excluded. O. tensions and saturations and hemoglobin weremcasured directly from samples obtained simuitaneously from allcatheters. Systemic and cerebral O, extraction ratios were calcu-lated using standard formulae. Mean age was 67.8 t 15.6 years'
Time to CFR averaged 7.5 minutes in l4 and was unknown in four'Total t ime of CPR unti i blood sampling was 38' l + 16.1 minutes'SaO, was 0.961 t 0.043 and hemoglobin was 11.2 t 1.6 gldL'
O- Extraction Ratio CPR NormalSys temic 0 .808t0103 0 .23 '032Cerebral 0.755 10.151 0.28 - 0.35
Systemic cxtraction ratio was greater than brain extraction ratio inipn l l ' : .015, paired t test). These data ref lect inadequate systemicand cerebral o*yg.tt delivery during CPR despite adequate arterialoxygen content. The markedly elevated extraction ratio suggeststhai-delivery-dependent oxygen consumption is occurring. Thesedata aiso indicat-e that aerobic metabolism continues during severeand prolonged global ischemia. The Iower cerebral extraction ratiomay be due to preferential brain per{usion during CPR'
199 Cerebral Lactate Uptake During Prolonged Global
lschemia in Human BeingsEP Rivers, NA Paradis, GB Martin, MG Goetting, TJ Appleton, RMNowak/Departments of Emergency Medicine, Surgery, andPediatrics, Henry Ford Hospital, Detroit, Michigan
Animal data indicate that cerebral metabolism may be fueled bylactate during ischemia. We measured lactate levels across thecerebral circulation in human beings during cardiac arrest.Forty-two patients (57 t I 5 years old) had iugular venous bulb, aortic arch,and iieht atrial catheters inserted during CPR. Lactate levels weredrawn immediately after catheter placement (t = 0) and ten minutes{t = l0l later. Patients were managed by advanced cardiac lifesupport guidelines. Lactate was measured by the Du Pont ACA.tr"y-^ii. "ttry and is reported in millimeters per liter' Time fromarrest until arrival in the emergency department was 20 + 10minutes. Time {rom arrlval in the ED until sampling was 14 + 5minutes. Mean lactate levels for aortic arch, iugular venous bulb,and r ight atr ial were 17.O x 5.6 (t = 0) and 17.7 t 5.2 (t = l0), 16'0 t4 .7 l t =0 l and 16 .3 t 4 .3 ( t = 10) , and 15 .7 t4 .6 ( t = 0 ) and 17 015 '3(t = 10), respectively. At t = 0, mean aortic arch to iugular venoustulb lactate dif ference was 1.0 x 3 4lP = .03J; at t = 10, the meanaortic arch to iugular venous bulb difference was I 46 ! 4'OZ lP =
.018). Of the 4i patients, 29 had decreasing lactate levels across thebrain with differences as high as 18 4 in one patient' Sixty-nineDercent of all patients showed decreasing lactate levels across thetrain. This is the first evidence suggesting lactate uptake duringprolonged global ischemia in human beings.
200 Lidoflazine Administration to Survivors of Cardiac
ArrestN Abramson, P SaJar, K Detre, the Brain Resuscitation Clinical Trial(BRCT) ll Study Groupilnternational Resuscitation Researchbenter, University ot Prttsburgh; 20 hospitals in eight countries
Twenty hospitals in eight countries,participated in this ran-
domized iti.ri.rt trial testing whether administration of lidoflaz-ine, an experimental calciumentry blocker, would improve neurol-
64
No ROSC (mm Hg)ROSC (mm Hg)
lnitial Ao-RA0.8 I 9.31 4 . 5 t 1 0
Maximal Ao-RA9 . 5 t 1 1 . 826.8 ! 7 .7
ROSC versus no ROSC difference signi{icanl at P < .001 .
No nat ient wi th a maximal Ao-RA of less than 17 had ROSC' A
gradicnt above this did not prcdict ROSC, howcver, as l3 pa-tients
*ho fril".i to devclop ROSC had gradients above 17. This substan-
tiates previous animal work and indicates there is a higher mean
Ao-RA gradient in patients with ROSC than in those who fail to
dcvclop"hcmodynamics. Measurement of Ao-RA may predict
outcome and serve as an index for ef{icacy of therapeutic intervcn-
t1()ns.
- 197 High-Dose Epinephrine and Coronary Perfusion
Pressure During Cardiac Arrest in Human BeingsNA Paradis, GB Martin, EP Rivers, J Rosenberg, TJ Appleton' RMNowak/Department oJ Emergency Medicine, Henry Ford Hospital,Detroit , Michigan
Work in inimal models of cardiac arrest indicates that the
optimal dose of epinephrine may be larger than that used clinically'Tie aortic to right alrial pressure gradient (Ao-RA) during CPRrelaxatron phasei. the coronary perfusion pressure in the arrestedheart and is positively correlated with return of spontaneouscirculation (ROSC]. The study population was adults in medicalcardiopulmonary arrest who had failed to respond to prolongedstandard ACLS therapy. Aortic arch and right atrial catheters wereplaced and simultaneous pressures recorded. The maximum rise inAo-RA af ter a standard I -mg dose o{ epinephrine and a high dose-of0.2 mg/kg (ie, 14 mg in a 70-kg patient)-were measured during the
five minrites after IV administiation. The protocol was sequentialrn that each patient served as his own control receiving standard
dose followed by high dose. Patient mean age was 59 + 16 years'
Time from arrival to high dose was 25 + B minutes. Pressures are rn

ogic recovery after cardiac arrest. Informed consent was obtainedfrom next of kin, usually with a "deferred consent mechanism.Patrents w5,r1y1doqly assigned to receive placcbo (STD) orhdollazine (LIDO) in addition to protocol_defined standarcl therapyand were followed for six months. Results are available for 505 ofthe 5 l6 patients entered into thc study. Mean age was 6 3 years j 62o/ol3 l1 of 505) were male; 66% l3BS oi SOS) of arrests were cardiaccaused; and 60% ,303
oI 505) occurred out of hospital. Mean arrcsttime^wa-s 4.6 minutes (range, one to 2Z minutcsl. Mean CpR timcwas 23.9 minutes (range, one to 180 minutes). Treatmcnt groupswere,comparable except for greater incidence of history of Jonges-trve heart ia i lure in.STD (p = .05). Compar ison of morta l i ty indncurologrc rccovery betwcen treatment groups revealed:
factors) . The s ix factors were l imb- lead eRS interval of 0.10seconds or more, a l tcred.mental status, re ip i ratory depression,seizures, arrhythmias, and hypotension. Subsequent ciinical courseand occurrence of any compiications were th;n evaluatcd. Fortv-seven pat ients were entered into the study. Al l had the p. . r . r r . . ofa tricyclj c antidepressant con{irmed by toxicologic scrcenrng. Noneof the l8 low-r isk and nine of the 29 high_r isk pat ients h"a io-pf l -cat ions (P < .05 by chi-square). Compi icat ions werc judged l i fe_threatening (eg, hypotcnsion, arrhythmias) in five f-rigt ?irL put ients and_ ser ious (evidencc of aspirat ion pneumoni t rs) in four.Review of the data rcvealed that nerther eRS interval nor anisolated clinical finding alonc would havc performcd rd.q,_rat.ly nir isk c lassi f icat ion. I t was concluded thai combinccl pai i .nt , r rdECC cvaluat ton for the prescnce of spcci f ic factors in thc ED can beuscd to assess t r icycl ic ant idepressant overdosc pat ient r isk.
'203 Hypervent i lat ion in Tr icycl ic Ant idepressant Toxic i ty
H Desai, D Seger, A Sanders/Section of Emergency Medicine,Col lege of Medic ine, Univers i ty of Ar izona, Tuclon;-EmergencyMedic ine, Vanderbi l t Univers i ty , Nashvi l le , Tennessee
Sodir-rn-r bicarbonatc is the drug of choicc for the treatment ofQRS-widcning cardrac dysr l - rythmias sccondary to t r icycl rc ant idc_prcssant tor ic i ty . Al tcrat ion of p lasma pH wi th a subsccluenrchangc in the protc in b inding of the drug is thought to bc thcmcchanism of act iun. I t is unknown whe thcralkal in izat ion throughhypcrvcnt i lat ion rcvcrscs eRS wide ning. Our str . rdy was concluctcdin an animal modcl cvaluatrng thc cf fect of hypcrvent i lat ion onrevc rs i ng QRS w i t l cn i ng . duc t o t r i c yc l r c an t i dep rcssan r t ( l x i e t t y .. lwc t vc p l gs {mcan wc igh t , 1U .214 .3 kg ) wc rc ancs thc t i zed w i t hhalr) t l tanc and nr t rous oxide, intubatcd, and rncchanical ly vcnt i -latcd. Nortr ipty l inc was aclministcrcd intravcnously t , , cach anin-ra l unt i l thc QRS complcx widcncd to 120 n-rs or lnorc. A mcan of7. .75 J: | .13 rug/kg nort r ipty l inc was administcrcd to cach animal .Thc QRS width incrcascd f rorn a bascl inc oI 47.5 + I1.4 n-rs to thctox i c s t a t c w id th o f 150 1 .21 .3 ms . Oncc t ox i c i t y was ach i cvcd ,vcnt i lat ions wcrc incrcascd f ron-r 10.(r t L7/r-n in t , , tq.S t 4.5/min.Hypcrvcnt i lat ion rcsnl tcd in a narrcwir . rg of thc eRS complcx f rornI50 t 21.3 to 91.6 + I5.1.1 ms. This rcprcscntcd a s igni f icant changcby thc paircd Studcnt 's I tcst l1) . .0 iJ. Artcr ia l b loocl gascs .h,r* ! , Ia rcspiratory a lkalosis af tcr hypcrvcnt i lat ion. Basci inc pH andpCO, valucs changcd | rorn 7.42 t 0.04 and 35.5 12.3 rnm Hg,rcspoct ivoly, to posthyporvcnt i lat ion valucs of 7 .50 X0.07 an<l1,27' it 2.6 mm Hg, rcspcct ivc ly (1, < .01). Scrr . rm catccholaminc lcvcls ofcpinelhr i nc and nor. -p incphr inc wcrc rncasurcd at bascl inc, postnor_tr ipty l ine, ,and f ( )sthypervcnt i lat i1tn; hgwcvcr, no stat is t ical ly s ig_ni f icant changcs in lcvcls wcrc obscrvcd. In a porc inc mocic l i r ft r icycl ic ant ic lcprcssant toxic i ty , s igni f icant narrowing of wic lcQRS complcxcs was obscrvccl wi t l - r hypcrvcnt i lat ion and rcspira_tory a lkalosis. Furthcr studics on thc usi of hypcrvcnt i lat ion fo; thctrcatntc l t t of wic lc QRS carc l iac dysrhythn-r ias are warrantcd.
-?-04 The Effect of Alpha, Acid Glycoprotein onNortriptyline Toxicity in SwineDC Seaberg, LD Weiss, DM yealy, RM Kaplan, Ep Krenzelok/U,niversity of Pittsburgh Affiliated Residency in EmergencyMedicine, Center for Emergency Medjcine
-ot Westeri
Pennsylvania, PittsburghTricycl ic . ant idoprcssant toxic i ty is a f rcc lucnt ly cncountcrccl
problcr-n in thc. cr-ncrgcncy departmcnt. Wc dciigncci a pruspe ctivc,contro l lcd t r ia l to. invcst igatc thc cf fcct of a lpha, acic l g lycr iprotc in(AAG.), an acutc phasc rcactant , on thc c l in iCal and phaimacologicmani fcstat ions of nort r ipty l ine toxic i ty . Fourtccn swinc (10 to- i3k, l l wcrc g iven a tcn-minutc loading dose fo l lowcd by a 45_rninutclnaintenancc infusion of nort r ipty l inc to achicve a levcl , based onp r t ' v i ous l y
. e : r l cuh t cd . pha r rnaco l< i nc t i c s , o | app rox im l t e l y 1 ,0 { J0ng /d l . A r r hc cnd r r l t hc i n f us ron , sevcn con r ro i r n i r na l s 1C) wc rcgivcn 50 mL 0.9%, sal inc and scvcn AAG_trcated animals wercgrvcn.50 rn l l0%, AAG, both ovcr 15 minutcs. Hcart rate, eRSdurat ion, QTc interval , b lood pressure, ar tcr ia l b lood gases, 'a l iumin, and serum {rcc and bound nort r ipty l inc levcls wcre measuredat basdinc and cvery hour aftcr for five iours. Data were analyzedusing l ishcr 's cxact , two-ta i lcd t tcsts, and repeated , -neasures cr fANOVA with thc alpha error set at 0.05. One dei th was notecl in thcAAG group and none in thc control group {p = NS). Mean totalnortriptylinc levcls after infusion in the control group were 1,240t 498 ng/dl and in the AAG group, 804 t 73 "glar il = NS). Nosignificant differcnces werc found in the serum fric to iotal nortrip_tylinc ratios bctwecn groups at any timc intcrval. Howevcr, signifi_cant ly shorter QTc intervals were found dur ing t reatment; i th
O.utcome at 6lvlos (%) Best Function During Foltow_Up (%)LIDO STD LIDO ST-D(n = 253) ( n = 252) (n = 253) (n =2s2)12 .0 12 .5 18 .9 1 8 .3
2.7 0.4 5.0 4.7
NormalModeratedisabilitySeveredisabilityComaDeath[,4issing
0 .40 .88 1 . 5
2 .7
1 . 9082.5
2 .7
9.3 8.966.8 67.7
Lidoflazinc has not been shown to excrt a statistically significantbrain-bcnefitting effcct on comatose carcliac arrcst survlvors.
-201 Glucagon: Prehospital Therapy lor HypoglycemiaRB Vukmir, DM Yealy/University ot pittsburgh Afiiiiated-Residencyin Emergency Medicine, pittsburgh
. Wc prospectiv_cly studied the efficacy of glucagon for thc prchos_pital trr.atment of hypoglycemia whcn IV line ,"i"r, *r, .,r,i,l-,ta,,-r_ablc. . .The study populat ion consisted of 50 consccut ivc pat icntscnrolled ovcr a six-month period in a busy urban advanccd lifcsupport.system who presented with documcntccl hypoglyccrnia ( <80 mg/dl by Chcmstr ip, BG) and symptoms of dccicasccl lcvcl ofconscrousncss/ s_yncopc/ or seizurcs. After a mcan of Ltili failcd IV
] i9" 9, j t -O.. , .g lucagon was administercd c i thcr int ramuscular ly{46 of 50) or subcutancously ( four of 50). A dosc of 1.0 , r rg *r , . , r . ifor adul ts and 0.5 mg for chi ldren 2 ycars or youngcr. Data col lcctcdrnclur lcd.prctreatment (by Chcmstr ip, ) and post_trcau-ncnr scr l lnrglucosc (by in-hospi ta l assay) levcls, as wcl l as prctrcat lnont andpost-trcatment assessrrlcnt of lcvcl of c,_rnsciousncss by GlasgowComa Score (GCS) and a 0 to 3 qual i tat ivc scalc. Data wcic analyzcclusing two-ta i lcd rank-sum and Stuclcnt s I tcst as wcl l as Fishcr,sexact tcst . Thc per-cxpcr imcntal a lpha crror was sct at 0.05.Twcnty-four malc paticnts and 26 fcrnalc patients wcrc stucliccl,with a mean agc of 56.8 years (range, 4 months to 92 ycarsl. Tl-rcmean prctreatment blood glucosc was 33.2 t 2.3.3 mg/dl, ancl thcpost- t rcatment rose to 133.3 t 52.3 rng/dl {P < .0001). er . ra l i tat ivclevel of consciousne ss rose f ro m 1 .26 tO.96 to 2.42 t0.O9 p < .0001 )and GCS rosc f rom a mean of 9.0 + 4.19 to 13.041 3.6U (p < .0001).The mean t ime unt i l responsc was B.B rn inutcs in thosc whore.sponded by both lcvel of consciousncss criteria l4I oI 50, g2%).There was no diffcrence in responsc rate between malc and'fcrnalcpatients/ initial level of consciousness scorcs/ or thosc with antlwithout a history of diabetes. Headaches occurred in two patlcntsl4%| no other sidc effccts were notcd. Wc concludc that gir-rcagonis a safe and effective trcatmcnt for syn-rptomatic hypoglyien-ria inthc prchospital setting when IV line.aciess is diffi;;lt.-
'
202 Accurate Prediction of Tricyclic AntidepressantOverdose Complications Using ED presentation: AProspective StudyGE FoulkelDiv is ions of Emergency Medic ine/Cl in ical Toxtcotogyand Pulmonary/Cr i t ical Care Medic ine, Univers i ty of Cal i fornia i 'Davis, Medical Center, Sacramento
Identifying the subgroup, of tricyclic antideprcssant_ovcrdoscpatients who are at rrsk of subsequent complications and thereforewarrant use of hospital-critical cat. tcsu.,.c.. is an important but:oTpi:* emergency department task. previous retrospective stucl_res indicate that a constellation of clinical and ECG findings n-rightbe used to identi{y this subgroup. A prospective study of'all suchpaticnts presentlng to our ED was peiformed during ihc perio<i ofMarch l987 through April I988. Ali patients *.rc urscss.d fo, thcpresence or absence of six risk factors and classed as high risk{presence of one or more factors) or low risk {absence of-all six
65

r
i
AAG compared with controls (P < '05)' In addition' a trend toward
i;;#':;t;ot" ftooa press're and shorter- QRS duration was
noted during treatment with AAG No significant changes were
shownbetweensroupst*.:{::?'"':"*f :,:ln,"ifi',*}l?""1ilff d;fi it"illl"f'li'ii'ru;t;;;;;;;;h".rinicarparameters;ici;:;,;;;;r, qRd a"'r;-;, and svstolic blood pressure and that
further research is warranted'
-205 The Evaluation of Cocaine' lnduced Choa"t Pain
G Tokarski, P Paganussr, R Urbanski, D Carden' C Foreback' M
Tomlanovich/Department of Emergency Medicine' Henry Ford
Hospital, Detroit , Michigan
-l.tln",lt*l;r::::#:1rlltrJ#ft "J,1:il:ff .:'-Til'id:
;ct i;; ililtii". "t,.*t iniury or ischemia To determine the
;J;;i .re^ti.,e kinase isocnzymes (CK-I) in this populatioll,Y:
cvaluated 42 patients presentingto thcID with chest pain w1th1n
six hours clf cocaine use and liho h^d normal or nondiagnostic
ECGs at presentation. 6r-i*ttt obtained at presentation and
;;;r,J ti;;;a It hn..-'i ' l 't"t, ECGs wereabtained simultane-
ously. Forty-twu p",t.rrr, *iiit ^ -""t agc of 28 5 years completcd
our study. Mean time tn ptt't"ttt',tion after cocaine use was 135
-in.,,",. Ei ght pati cnts ti: ll ":i*nf xil::il ;ffif "t'-.t f iiffi :i':ij1$"'it",lTi";;.i,;;";, ;hi.( i con jid'rccr diagnos-;i;;;;;; ;y;.r'aia lnil"t'on si* patients (1a%) had eiev-atcd;;;icii;;J6r-i o" tt'" initial determination onlv; seri'lttt;!f,ir i*-r"a 12 hours werc within normal l imits' .EC
i*f :*i""'Tf 't:11.1',tffi '[.?"i1rt..""*,i[:i,I:'!:tl',^t'#f,lJl t*:'?3L:
-,:;1':5r' 3::il""'"?T:' |ffl p a, i e n i s w c r e
*';l**1,i::n*"1i,*jli"r' j::';:,1$:x,:lf niT:i,ili;..;;;;;;i;;,t -r-',ia.i"inp-thest pain.after cocaine use and havc
","*"r <ir non<liagnostic ECCs' This injurv *"tti:HilT:fffi;il;;J*i infarciion or transient mvoc:rdial.isc
duc to coronar y Ntery;;;;;;, '"itittt t"t" been reported with
cocainc usc). Singlc ut ttilinottal-nondiagnostic ECGs' there-
fore, do not rule nut itti-tt*iu or injury .in ihis situation These
iiilil*j:*i',ft l'1r".',Tl*,m*:ln:lff ffi H""?:lx'ficlctcrmination of CK-I in the ED'
*206 Severe Oral Phenytoin Intoxication: Lack of
cardiovascular Morbidityv Department, Detroit Receiving
fi 3.yJJf '#i
fl"'#E["'n""., Med ici ne, Department or su rserv'Wayne State University, Detroit , Michigan .-,^-
To facilitatc treatment of hvpotension "t Utt:?:|il,T; ;1TJ
,.rtho.iti.t advocate management in a monitor
il;;;t;h ,.u.r. ph.ttytuin poisoning' To evaluate this strategy'
;;';';;;-irt.-ti'.aiJti records of .51 patients admitted to our
institutlon o,r., ".*u-ylrr perlod with peak_phenytoin levels of 40
;;i;;";;;;. l.t"rtl"s irom inge-stion - M',t' peak phenvtoin
illl"t t^, 49.4 t 7 .7 pg/ml (range, 40,to 7 6 us/ml)' Mean age was
44.1 + 1(r.8 )ears;56;;; i ; ; ' t ( isr) haa a historv of seizures'-54
(95%) were ,rr.i"g ptJtttitta-ptt"i-tvtoi"' and six {11%) had a
iriri.iv oi r't.rtt diri"it pitt*ting complaints included ataxia {36'
2,a '/. ), ;;;;;;;ir"t. ( tt", -r
s i' 1 ; ttie"tnl -ttatus
chan ges' y:i'Y:t:'
and visual symptoms (each nine, l6%Ji and gastrointestinal prob-
i;t (f;;, 9't )' Sulcide was mentioned as a motive in seven cases
iilni:'::l'#:,ru*;f l'e1;?"""r?:i'.',"'ff #ix'i:;""":iil;t;i""t;"^';; ivttrtvt[,,'i^ requiring .l':1tT""t
Twelve-lead
:.#iiflt[t];ir#:W::.r,';if35:t:3,ffi '''ftn!
i:*:#i:t".'":';illl'"ff :i::::tY;1ry:*:.Tfi iilft ii'"!increase in p-n intervaitlur, f S t iO -t) when toxic' while six had
a decrease (M,17 t l0 ms) in comparison to nontoxic records' No
:t::;ii*ff :;1."1';?llilliji?l;il,x';ffi i:iSft x.",T:',f i;sustained a llp laceratil-r4 tft*t i"*9 t'o t"diou"trllar complica-
tions and no deaths. wt-'to""f"at that in many cases setr-ele ^oral
;[;y.il poisoning may be safeiy managed in an unmonltoreo
settinq.
207 Decreased Inllammatory Reaction (Enhanced Burn
ivo""a fr""iing) in Nonionii Surfactant-Treated RatsPW Paustian, RR Haase, . lC McPherson Jr ' TH Hguyen' DF Ward'
iC U"Fn"rton l l l /Department of Cl inical Investigation and
i'if'o'io gv-, Ei t"n now'e r.nrmy M ed ical Center' Fort Gordo n'
Georqia; Department or surgeryiEmergency Medicine' Medical
College of Georgia. AugustaWe havc discovered a oramatic improvement in burn wounds in
,".t.i.ri.a with a nonioni" t"tf"t"ttt, Pluronic.I-127 (F 127)' ln
""?-"a.i, z+ ̂ ".rtt.,.tir.J-'i" rats (300 to 320 g) received a third-
ilil;;; by i--"*lott-oithe antetior chest wall' 8% bodv
surface area, for 12 seconds in a 70 C waterbath' Burn wound area
;;;;;;;;;;!a t--.di^t.iv after immers.ion' Thirtv minutes later'
rrrri "iirr" ,"i-als received either g ml/kg body wt saline or F-127
iit -r"riif uto.,gh the t"iiu"i" All animlls were eating' voiding'
;;i;;;ilr;;;;it'i" rz hours' rhere were no fatalities Animals
*.t. -r.rli.J
^? 48 hours ""a tnt burn wound area measured' At
autopsy, the gross "pp.,t^tt"" of the F-127-treated animal wounds
;;#;t;;U. ir'"v !r'"*"J a significant (P < 05) reduction in the
;;;"t;; ;i"*;;nd contraction Tie wound,contraction was 15%
#;;;;; iil" .rli,t"-,t""t.J""i-"tt Histologicallv-' the degree of
i,r "il;;;;;";t llu.it't J"potition, p-erivascular f ibrosis' edema'
;J;;ebi;"d ..ii "*t,"""'"tion in the dermis' submucosa'-and
;;;;; *.r" gr.r,., in the saline-treated animal's versus those
;;""*tdF"iti. w" b.li."t these data show a p.ositive therapeutic
;;i;;;if 127 on the initial burn-induced inflammatorv process
that may imProve wound healing'
208 Effect ol Povidone'lodine and Saline Soaking on
a;;iitdi"; Bacterial wound Tissue Gounts in Acuteiraumatic Contaminated Woundsnl-L"tt"i., nZ Fourre, M Callaham, T Boone/Valley Medical.
i".iJt, o.plttment of Etetgency Medicine',and U-niversity of
6"iit.i.ii, 5"" Francisco, rr"esno; Division of Emergency Medicine'
University of Cali{ornia, San FranciscoIt is common pr""t'""-fo soak acute traumatic wounds in dilute
o""iao"'.i"Ji"" iol.,tio"-befli" *ottnd irrigation and toilet' The
efficacv of this practic. jt ""1"o*" We s6ught to determine if
lo.i.ft ;;;;'Id; air"tt p*'ao"t-iodine iolution would de-
crease quantitative wounJiissue bacterial counts {previously shown
;;;;;;t predict wound infection) as companed with no treat-
-.* "t t"rflilg *i,ft t'fi"t Patients were eligible iot st1a1{ tl;1
*"i" t"." in ihe emergency department with.acute traumatlc
;;t;i;";;d, t"tt tttin ti' hours old that had sienificant con-
tamination and ,eq,,i'eJ-i"b'idt-"ttt' Patients weie excluded if
ifr'iy #.i" iri.iel"-.-i -ai"t, r"I^d taken antibiotics within five davs'
or refused consent o, tt tlJtt *"t no subsequent bacterial growth
i'-- "r.,i,rrr". Before any treatm-ent, 6 to, l0 mL visibly-contami-
nated tissue w", ,.-ouJd {'om the wound surface and subjected to
il;;ri,;il ;-.". ."ri"*"-it'e wound-was th.en randomized to
r e c e i v e a t e n - m i n u t e s o a k i n l % p o v i d o n e - i o d i n e , s a l i n e , o r n oir."rr*", ,i "ff . afte, the ir"rtment period,,a second set of tissue
:;fii;;rd;;t-to-the first sites waJtaken for repeat cuiture' and
;il;ilil;;1Len t"'ted itt a standardized {ashion' charts were
reviewed to determine ;;;";" and incidence o{ wound in{ection
Thirty-three patlents *iitt sJ;o""as were entered into the study;
three in the saline g,ot'i *Jtt e*cludtd due tono bacterial growth'
i'h;;;;b""teria'i co"ttt per gram of tissue decreased 9'19 x 106
isp, i.ii " io;f ,it.t pouiao'".-i"oii"" to"k, 6 a 1 Ip5 (1'68 x 106)after
lio-lori., ^"a irr"r""r.d 3.eg x 10' (1.05 x 10s) after a saline soak.
Wounds with counts o{ iess than lb, organisms per gram.of tissue
;;";;itk;t to become infected' Multiple regression analvsis was
;;il;';;"i1he changes in bacterial count after treatment as a
Iunction of "*p.rl-.ti?l gi""p ""a initial bacterial count' There
;ffi;.ilii:r.ti-oltitt"itt between the-control and povidone-
ioaj"" sto""p.. Howevet, the saline group^had a sienificant trend
toward increase tn bacterial count after treatment 1i" = 'OO0t1' and
this eftect was greater at higher initial bacterial contamination
i1.".f..'rnt """8f"a" tt"t siatti"g acute traumatic wounds in
;"";d;";-i"i;" ."i"rii" ptl"ides-no ben'fit in decreased wound
tissue bacterial counts and that saline soaks may actually increase
such counts.
-209 Tetanus lmmunization Status and lmmunologic-n""pon"Jto a Booster in an Emergency Department
Geriatric PoPulation; c;;";, nieoy, D williams/university of roronto' Toronto'Ontario, Canada
66

Although effective procedures for the prevention of tetanushave long been available, serosurvcys done since I97Z dcmonstratcthat 49T" to 66T' of the elderly population lacks a protcctiveantitoxin level (less than 0.01 IU/mL). Our study was undertakcnto assess t he t c t anus immun i za r i on s ta tus o f ge r i a t r i c pa t i un l spresenting to a tertiary care emergency department with a break inthe skin barrier and to evaluatc their immunologic responsc to atetanus booster . From February to Septembcr 1988, 80 pat ientsmore than 65 years old wcre enrol led. At cach pat ient ,s in i t ia lpresentation/ pertinent dernographrc data and tetanlls irnmuniza-tion history were recorded, an antitoxin titcr was determined on aserum sample by ELISA, and a booster was administcred if requiredby the Advisory Con-rmittce of Immunization practiccs (ACIp)criteria. Scrum antitoxin assays were repeatcd on days Z, 1 4, and 2 Iaf ter the in i t ia l v is i t unt i l seroconversion { t i tcr , morc than 0.01 ru/mL). Forty- four pat ients (55%) had protcct ive levcls at in i t ia lpresentat ion and, in 36 las%), the lcvels wcrc unprotcct ive. Agcand sex wcre not predictivc of protcction. past n-riliiary scrvicc anda dcfinite history of threc or morc previous ilnrnLrnrzatrons wcrcgood predictors of protection. Of thc 36 paticnts who wcrc followcds.erially for-unprotective initial titers, 19 153"1,) scroconvcrtcd byday 14, whi lc I5 142%)did not seroconvert . Two patrents ( .5%) wcrclost to follow-up at day 7. Patients who did noi seroconvcn wcrcmore l ikely to be oldcr ( / r <.05). In conclusion, a considcrablcnumber of c lder ly pat ients lacked an in i t ia l protcct ivc levcl oftctanus antitoxin in this study. Of these, 42% Iailed to scroconvcrtwi th in l4 days and potent ia l ly carr ied a r isk of dcvcloping tctanusdespite prophylaxis.
.210 Util i ty of Contrast Duodenography in the Detectionof Proximal Small Bowel Injury Following Blunt TraumaJM Edney, JA Marx, EE Moore/Departments of EmergencyMedicine and Surgery, Denver General Hospital and University ofColorado Health Sciences Center, Denver
We comparcd contrast duodenography with a cliagnostrc pcrrro-ncal lavagc and computed tomography (CT) in thc clctcrminaiion oftraumatic small bowel pathology. Contrast duodcnography wasperformcd on 104 paticnts whri sustaincd major blunt rncchanisrnwith midthoracoabdominal impact . Six (5. t i%) t ruc-posrt ivc stud-ics demonstratcd burst jc junum ln = 2) , pcr forat ion of thc th i rdportion of thc duodcnum, or duodcnal hcmatorna {n = 31. Thcremaining 96 had true-ncgativc contrast duodcnography by clinicaloutcofire critcria. In patients with hollow viscus pcrforatior-r, lapa-rotomy confirmcd isolatcd injury. Scrum arnylasc was norrnaf incach. Diagnostic peritoncal lavagc was pcrforrncd within twohours of injury and standard diagnostic pcritoncal lavagc criteria forred blood ccl ls , whi tc b lood ccl ls , and amylasc wcrc not cxcccdcd.However_, white blood cells wcre equivocal in two of thrcc paticnts,and amylasc ranged from 20 to 56 U/L. CT was obtaincd in twopatients and was unrernarkable. In patients with duodcnal hc-matoma, initial serum amylasc was markcdlv c-lcvatcd in two ofthrec. Diagnostic peritoneal lavage mcasurcmL.ltts wcrc normal.CT was negativc, not perforrned, and confirmatory of contrast duo-denography findings, respcctively. Diagnosis of proximal smallbowel injury is problematic. In our expcrience, iontrast duodc-nography is a sensitive method of dctcciion when comparecl withdiagnostic peritoneal lavage and CT. Subthreshold elevations ofwhitc blood cclls and amylasc in the immediatc postiniury periodmay reflect pcrforation of thcsc structurcs.
-211 Computed Tomography in the Evaluation of BluntAbdominal TraumaWC Pevec, AB Peitzman, AO Udekwu, W Straub/Trauma/Emergency Services, Presbyterian-University Hospital, University ofPittsburgh School of Medicrne_ . The efficacy of computed tomography {CT) for thc diagnosis ofblunt abdominal injury remains controversial. The purpoic of ourstudy was to further define the role of CT in the acuteivaluationof blunt abdominal trauma. Methods: CT scans were performed on325 consecutive patients sustalning significant blunt abdorninaltrauma with these indications: equivocal physical findings, dc-creased level of consciousness, spinal cord injury, hematuria, orpelvic fracture. Unstable patients and those with indication forrmmediate surgical exploration were excluded. Results: Onehundred twenty scans 137%l revealed abdominal rnjuries; S5 t 20minutes were requrred to perform the CT scans. Diagnostic accu-racy was 97.5%, with two {aise-positrve and thrcc false-negativescans. Thirty patients {9%) underwent laparotomy based on CTfindings. Ten laparotomies {33%) were nontherapeutic. Twenty
splcnic in jur ics were dctected; c ight of n ine werc successful lymanaged nonoperattvely, and eight of I I rcquired operation. Onesplenic in jury was mrssed on the in i t ia l scan and diasnoscd on asubscquent scan. Both fa lse-posrt ive scans were read as showingsplcnic in jur ics. Sixteen hepat ic lacerat ions were diagnosed; twowcrc repaired antl 14 wcre managed nonoperatively. Of 20 rcnalin jur ies, thrce were rcpaired, and I7 werc managed nonoperatrvely.Two of f ive pancrcat ic in jur ics were not detected by thc in i t ia l CTscan. Six of n inc laparotomies performed for f ree per i toneal f lu idon CT scan wcre nonthcrapeut ic. Conclusions: Thc rate of nonth-erapeut ic laparotomy (33%) bascd on CT was s imi lar to thatrcported for pentoncal lavagc; CT cvaluatron of blunt abdon-rrnalin jury a l lowed nonoperat ivc managcment of splenic, hepat ic, andrcnal in jur ics; CT was unrel iablc in thc cvaluat ion of pancreat icin j r" r ry; and thc major shortcomings of CT in the cvaluat ion of theblunt t rauma vict im wcre i ts a l rsolutc rc l iancc t rn exoer icncedintcrprctat ion ancl the rcqurred commitmcnt of t imc and pcrsc,n-nc l .
-212 A Comparative Rewarming Trial of Gastric VersusPeritoneal Lavage in a Hypothermic ModelMA Levitt, V Kane, J Henderson, M Dryjski/Thomas JeffersonUniversity Hospital, Philadelphia, Pennsylvania
Pcr i toncal Iavagc and gastr ic lavagc z l rc two mcthods of intcrnalrcwarnt ing that can vcry rapid ly bc appl icd in thc cmcrgcncy dc-partment. Wc comparcd thcsc two commonly uscd rncthods ofrcwartn ing in thc sct t ing of a hypothcrmie rahbi t modcl . Af tcrobtain ing basel inc l rcasurclncnts of rnci rn ar tcr ia l b lood prcssurc.hcart_ ratc, tympanic mcmbranc tcntpcraturc/ and est iphagca)/rccta l tcrnpcratLl rc, thc cool ing phasc was in i t iatcd. Dialysatccoolcd to 4 C was cont inual ly c i rculatcd through pcr i toncal lavagccathctcrs r - lnt i l a body corc tcmpcraturc as dctcrnt incd by t l tcmcmbranc tcmpcraturc probc () f 25 C was achicvcd and rnainta incdfor tcn minutcs. Rcwanning was thcn accompl ishccl wi th 40 C;c l ia lysatc by gastr ic lavagc (N = 5) or pcr i toncal lavagc {N = 6) .Rabbi ts unclcrgoing gastr ic lavagc hacl cont inuous rcctal andtrrcmbranc tc lnpcraturo mcasl l rc lncnts. Rabbi ts ur-rdcrgoing pcr i -toncal lavagc had cont inuor.rs csophagcal ancl mcmbranc rcmpcra-t l l rc mcaslrrcmcnts. I loth gr<tups had c()nt inuous hcart ratc, r .ncanartcr ia l b lood prcssurc, and ECG r.noni tor ing. Thc mcan cool ingt imc for our study was 1i9.09 t23.43 minutcs. Mcar-r cool inc t i rnafrr r thc pcr i toncal lavagc groups was L)6.67 !2[ i .05 minutcs ancl forthc gastr ic lavagc groul . r was i lO + 14.14 n-r inutcs lP = .24). Thc mcanrcwarming t i r .nc for thc pcr i toncal lavagc groul . r was 131.7 !27.1)nl inutcs. Thc mcan rcwarming t imc for thc gastr ic lavagc groupwas 136.0 + 25.1 minutcs (nor-rs igni f icant by r tcst) . In th is hypoth-crmic modcl , gastr ic lavagc ancl pcr i toncal lav:rgc achicvcd s i in i larrcwarming ratcs that dcmonstratcd no stat is t ical d i f fcrcncc. Gooclcorrc lat ion was found bctwecn tyntpanic mcmbranc tcmpcratLl rcand rcctai tcmpcrat l l rc (wi th gastr ic lavagc) and csophagial tcrn-pcraturc (wi th pcr i toncal lavagc).
213 Protocols for the Use of a Portable HyperbaricChamber for the Treatment of High-Altitude DisordersRL TaberlDepartment of Emergency Medicine, St Luke's Hospital,Denver, Colorado
_ Dcspi tc a rcccnt cxplosior-r in rcscarch on high al t i tude i l lncss,desccnt rcmains thc dcf in i t ivc t rcatment. Howevcr, in a lnrncset t ings of nore than 10,000 f t whe re thcse problcms ar ise, rn i rne -d iatc cvacuat ion rs of tcn unpossib le. Rcccr-r t ly , a portablc, l ight-weight (7 kg) hypcrbar ic bag has been dcvclopcd capablc of wi th-standing a prcssure of 2 psi . Thc bag's usc has becn reportedanecdotal ly in thc past few years as a mcans of s i rnulat ing desccntand thereby act ing as a t rcatnent modal i ty . Howevcr, no work hasbcen conducted to dcterrnrnc thc optirnal length of trmc of treat-mcnt in thc bag to achicve resolut ion of symptoms and to preventrecurrcncc once thc patient is or-rt of the prcssurized bag and'rcturns" to a l t i tude. This was cvaluated at the Himalayan RescueAssocrat ion 's a l t i tudc rcsearch c l in ic in Phcr iche, Ncpal , at I4,1.50f t . At th is a l t i tude, rnf lat ion of the bag to 2 psi ef fect i a descent of8,200 f t . By provid ing such descent, dramat ic improvcments couldbe secn wi th thc symptoms cr f acute -ountr ln s ickncss, h ighaltitudc pulmonary cdema, and cerebral cdema {HApE and HACE,respect ively) . At thc c l in ic, pat ients werc evaluatcd and diagnosedaccordingly and thosc with potcntrally fatal HAPE and HACE werearranged for immediate evacuation. At times, this was not feasibleand these patients werc put in thc bag. Repeat serial observation ofsymptoms and recovery revealed that wi th l5 acute mountainsickness, nine HAPE, and seven HACE patients, time frames of
67

two, {our, and six hours, respectively, were required to provideresolution of the symptoms with no subsequent complications ordeterioration. The author advocates the role of the bag as aneffective adiunctive and temporizing measure for the treatment ofHAPE and HACE.
214 A Novel Strategy for Therapy of Acute lronPoisoningJR Mahoney Jr, PE Hallaway, JW Eaton, BE Hedlund/Departmentsol Surgery and Laboratory Medicine and Pathology, and DightLaboratories, University oJ Minnesota Medical School; BiomedicalFrontiers, Inc, Minneapolis, Minnesota
Iron poisoning from accidental ingestion of iron supplements isan impoitant form of poisoning in young children and is still lethalin some cases. Present therapy involves IV and oral administrationof deferoxamine. Unfortunately, large IV doses of this drug causeprofound hypotension, which rs additive with the hypotensiveiffect of iron poisoning per se. Thercfore, the maximum IV dose o{deferoxamine is limited by its toxicity. To circumvent this thera-peutic problem, we synthesized a novel class of high molecularweight derivatives o{ deferoxamine by covalent attachment of thefree drug to various polysaccharides. The derivatives used in ourexperiments were prepared on backbones o{ either dextran orhydroxyethyl starch. Importantly/ these high molecular weightderivatives of deferoxamine maintain high affinity for iron of theparent drug but lack detectable hypotensive effects. Eighty-onepercent of male Swiss-Webster mice {25 to 30 g} given ferroussulfate by gavage i lO;rmol/g body wt and I mL l0% dextran orstarch in NaCl, IV) die within 24 hours {n = 16). Immediate IVadministration of the maximum tolerable dose of free deferoxam-ine (0.15 gmol/g in NaCl with 10% dextran or starch) does notreduce mortali ty 1'78%; n = 9). Larger doses of free deferoxamine i0.3Urnol/g) are lethal even in the absence of precedent oral ironadministration {n = l0}. By contrast, administration of eitherdextran-deferoxamine or starch-deferoxamine (equivalent to 1.25or 0.75 gmol free deferoxamine/g body wt) immediately or 60minutes after oral iron administration saves 100% of iron-poisonedanimals (n = 22 and f ive, respectivelyi P <.001). we conclude thatthese high molecular weight derivatives of deferoxamine ate, inlargc doses, much less toxic than free deferoxamine. This greatlydimlnished toxicity, in turn, permits the use of higher and moreeffective IV doses of iron chelator in cases of acute iron poisoning.
215 Combination Therapy With Cimetidine, Penici l l in,and Ascorbic Acid for Alpha Amanitin Toxicity in MiceSM Schneider, GJ Vanscoy, EA Michelson/University of Pittsburgh
Amanitin is the primary toxin of the mushroom Amanitaphalloides. High doses of cimetidine, penicillin, and ascorbic acidas single agents have been shown to attenuate amanitin toxicity inmice. We looked at this effect using combinations of these agents.Female Swiss mice were divided into nine groups. Croups Ithrough l5 were treated with alpha amanitin 0.6 mg/kg IP andsubsequently treated in four hours with saline I mL IP, cimetidine
120 mg/kg IP, a combination of cimetidine 120 mg/kg and penicil-lin 250 mg/kg IP, a combination of cimetidine 120 mg and ascorbicacid 600 mg/kg IP, or the combination of cimetidine, penicillin, andascorbic acid in above doses, respectively. Groups 6 through 9received saline and at four hours cimetidine, cimetidine+penicillin,cimetidine+ascorbic acid, or the combination of all three drugs inthe doses previously given. Half of the animals in each Sroup wereobserved seven days for survival. The other animals were sacrificedat 48 hours, and blood was withdrawn for hepatic enzymes, andlivers was harvestedfor histopathology. Analysis included ANOVA,Kaplan-Meier, and lisher's exact tests. Results revealed a length-ened survival in all treatment groups. However, only the combina-tion therapy increased ultimate survival {P < .01). Seven-day sur-vival in Group 1 was 31.6"/o; Group 2, 36.8%; Group 3,47.5%iGroup 4, 42.I%; and Group 5, 73.7%. ln the second half of theexperiment, three animals from group 1 failed to survive 48 hours.Mean SGOT (U/L) values (P < .00011 of surviving animals were:
Group 1 Group 2 Group 3 Group 4 Group 517,693+3,639 11 ,962+2,222 6 ,907 +2,646 5 ,100+ 1 ,697 1 '742+846
Control SGOT ranged from a mean of 60 to 236UlL. Histopathol-ogy results paralleled the enzymatic results. We conclude that thetliree-drug combination of high-dose cimetidine, penicillin, andascorbic acid provides significant protection in mice exposed toalpha amanitin in toxic dosages.
.216 Contribution of Sorbitol Combined With ActivatedCharcoal in Prevention of Salicylate AbsorptionRE Keller, RA Schwab, EP Krenzelol</Department of EmergencyMedicine and Susquehanna Poison Center; Geisinger MedicalCenter, Danvi l le, Pennsylvania Poison Center, Children's HospitaloJ Pittsburgh
The use of cathartics and activated charcoal in toxic ingestionshas become a standard treatment modality. Sorbitol has beenshown to be the most rapidly acting cathartic, but its therapeuticsignificance has been debated. Using a previously described aspirinovtrdose model, ten healthy volunteers participated in this cross-over design study, which investigated the efiect of activated char'coal alone versus activated charcoal and sorbitol in preventingsalicylate absorption. In phase I of the study, subjects consumed 2.5g aspirin followed by 25 gactivated charcoal one hour later. UrinewaJcollected for 48 hours and analyzed for quantitative salicylatemetabolites. Phase II was identical to phase I, except that 1.5 g/kgsorbitol was consumed with the activated charcoal. The meanamount of aspirin absorbed without the use of sorbitol was 1.25 g
{r 0.15), while th mean absorption was 0.912 g (t 0.18) with theaddition of sorbitol. This amounts to a 28T" decrease in absorptionof salicyiates attributable to the use of sorbitol' The difference issignificant at P < .05 using the paired Student's t test. Our studydemonstrates that the addition of sorbitol significantly decreasesdrug absorption in a simulated drug overdose model. Effects onabsorption in actual overdose situations and effects on patientoutcome should be the subiect of further study.
68

BEST ORALBASIC SCIENCE
1988- Sandra M. Schneider, MD, Universityof Pittsburgh, "Amanita PhalloidesPoisoning: Mechanism of CimetidineProtection"
1987- Eric Davis, MD. Ohio State Univer-sity, "The Comparative Effects ofMethoxamine versus Epinephrine onRegional Cerebral Blood Flow DuringCPR' '
1986- Peter A. Maningas, MD, LettermanArmy Institute of Research, "Use of7.5 % NaCll6 % Dextran 70 for Treat-ment of Severe Hemorrhaeic Shock inSwine"
1985- Michel le H. Biros, MD, MS, Univer-sity of Cincinnati, "Post Insult Treat-ment of Ischemia-Induced CerebralLactic Acidosis in the Rat"
BEST ORALCLINICAL SCIENCE
1988- William G. Baxt, MD, University ofCalifornia, San Diego, "The Inabilityof Prehospital Trauma Prediction Rulesto Classify Trauma Patients Accu-rately' '
1987- Ranjan Thakur, MD, Medical Collegeof Wisconsin, "A Randomized Studyof Epinephrine versus Methoxamine inPrehospital Ventricular Fibrillation"
1986- Stuart A. Malafa, MD, ButterworthHospital, Grand Rapids, "Prehospital
Index: A Multicenter Trial" andJoseph F. Waeckerle, MD, BaptistMedical Center, Kansas City, "A Pro-spective Study IdentiS/ing the Efficacyof Clinical Findings and Sensitivity ofRadiographic Findings in CarpalNavicular Fractures"
1985- Harlan A. Stueven, MD, Medical Col-lege of Wisconsin, "Bystander/
First Responder CPR: Ten Years Ex-per ience in a Paramedic Sys-tem"
BEST ORAL METHODOLOGY
1988- Phillip L. Henneman, MD, Harbor-UCLA, "Attending Coverage in Aca-demic Emergency Medicine: A Nation-al Survey"
VADE MECUM
BEST SCIENTIFIC POSTER
1988- David L. Schriger, MD, UCLA,"Defining Normal Capillary Refill:Variation with Age, Sex, and Temper-ature"
1987- Ruth Dirnlich, PhD, University of Cin-cinnati, "Effects of Sodium Dichloro-acetate on ATP and Phosphocreatine inIshchemic Rat Brain"
1986- Mark Howard, DO, Henry Ford Hos-pital, "Improvement in Coronary Per-fusion Pressures After Open Chest Car-d iac Massage in Humans: APreliminary Report"
BEST METHODOLOGY POSTER
1988- Frank J. Papa, DO, Texas College ofOstcopathic Medicine, "A Computer-Assisted Lraming Tool Designed to Im-prove Clinical Problem Solving Skills"
BEST RESIDENT PAPER
1988- Douglas Sinclair, MD, Victoria GeneralHospital, "The Evaluation of SuspectedRenal Colic: Ultrasound Scan vs. Ex-cretory Urography"
1987- Robert L. Muelleman. MD. TrumanMedical Center, "Blood Pressure Ef-fects of Thyrotropin-Releasing Hor-mone and Epinephrine in AnaplylacticShock. "
1986- Steven Chernow, MD, University ofArizona, "Use of the EmergencyDepartment for HypertensiveScreening"
1985- William C. Dalsey, MD, and Scott A.Syverud, MD, University of Cincinnati,"Transcutaneous and Transvenous Car-diac Pacing For Early BradyasytolicCardiac Arrest"
1984- Gerard B. Martin, MD, Henry FordHospital, "Insulin and Glucose LevelsDuring CPR in the Canine Model"
1983- Jeffrey A. Sharff, MD, Oregon HealthSciences University, "Effect of Time onRegional Organ Perfusion During TwoMethods of Cardiopulmonary Resus-citation"
BEST RESIDENT POSTER
1988- Katherine M. Hurlbut. MD. Universi-ty of Arizona, "Reliability of ClinicalPresentation for Predicting SignificantViper Envenomation"
1987- Gert-Paul Walter, MD, Michigan StateUniversity, "Emergency IntraosseousInfusions in Children: A PracticalMethod of Teaching PrehospitalPersonnel"
BEST PEDIATRIC ACUTECARE AND TRALIMA
1988- Peter Arlian, MD, Valley MedicalCenter, "Endotracheal Intubation ofPediatric Patients bv Paramedics"
BEST EDUCATIONALPRESENTATIONSSelected to represent EmergencyMedicine ^t the AAMC AnnualMeeting.
1988- Frank J. Papa, DO, Texas College ofOsteopathic Medicine, "A Computer-Assisted Tool Designed to ImproveClinical Problem Solving Skills"
Charles E. Saunders, MD. VanderbiltUniversity, "Videotape Review of Car-diac Arrest Resuscitation: Analysis ofElements of Resuscitation Team Per-formance"
1987- David Plummer, MD, Hennepin Coun-ty Medical Center, "Emergency
Department Critical Care Registry"
BEST PAPER
1984- Charles G. Brown, MD. Ohio StateUniversity, "Injuries Associated withthe Percutaneous Placement ofTransthoracic Pacemakers"
1983- Charles F. Babbs, MD, PurdueUniversity, "Improved Cardiac OutputDuring Cardiopulmonary Resuscitationwith Interposed Abdominal Compres-sions' '
1982- Carl D. Winegar, MD, Wayne StateUniversity, "Early Amelioration ofBrain Damage in Dogs After FifteenMinutes of Cardiac Arrest"
1981- Blaine C. White, MD, Wayne StateUniversity, "Correction of CanineCerebral Cortical Blood Flow andVascular Resistance Post Arrest UsingFlunarazine, A Calcium Antagonist"
1980- Blaine C. White, MD, Wayne StateUniversity, "Mitochondrial 0, Useand ATP Synthesis: Kinetic Effects ofCa-- and HPO. Modulated by Gluco-corticoids"
69
1979- Albert E. Cram, MD, University of
Iowa, "The Effect of Pneumatic Anti-
Shock Trousers on IntercranialPressure in the Canine Model"
1977- Lawrence B. Dunlap, MD, Josephine
General Hospital, Grants Pass,Oregon, "Percutaneous TranstrachealVentilation During CardiopulmonaryResuscitation"
BEST PRESENTATION
1984- Paul M. Paris, MD, University of
Pittsburgh, "The Prehospital Use of
Transcutaneous Cardiac Pacing"
1983- Sandra H. Ralston, MD, Purdue Uni-
versity, "Intrapulmonary EpinephrineDuring Prolonged CardiopulmonaryResuscitation: Improved Regional Blood
Flow and Resuscitation in Dogs"
1982- Stephen R. Boster, MD, University of
Louisville, "Translaryngeal Absorb-
tion of Lidocaine"
l98l- Robert W. Strauss, MD, University of
Chicago, "Expanded Role of the
Bar ium Enema in the Acute
Abdomen"
1980- Jacek B. Franaszek, MD, and Harold
A. Jayne, MD, UniversitY of I l l inois,"Medical Preparations for an Outdoor
Papal Mass"
KENNEDY LECTURERS1973-Fraser N. Gurd. MD1974-Oscar P. HamPton, Jr., MD
1975-Curt is P. Artz, MD1976-John G. Wiegenstein, MD
1977-Peter Safar. MD1978-Senator Alan M. Cranston1979-Alexander J. Walt, MD1980-Eugene L. Nagel, MD
l98l-C. Thomas ThomPson, MD
1982-R Adams CowleY, MD
1983-Ronald L. Krome, MD
1984-David K. Wagner, MD
1985-Richard F. Edl ich, MD, PhD
1986-Henry D. Mclntosh, MD
1987-Robert D. Sparks, MD
1988-Gail V. Anderson, MD
1989-D. Kay Clawson, MD
HONORARY MEMBERS
1973-Robert H. KennedY, MDtFraser N. Gurd, MD
C. Barber Mueller. MD
1974-John G. Wiegenstein, MD
Alexander J. Walt, MD1975-Oscar P. Hampton, MDt
N. H. McNal ly , MDtCurt is P. Artz, MDI
1976-Anita M. Dorr, RNtEugene L. Nagel, MD
19'77-Peter Safar, MD
1978-Eben Alexander, Jr., MD
1979-David R. Boyd, MD, CM
198 l-R Adams CowleY, MD
1982-Carl Jelenko, I I I , MD
HAL JAYNE ACADEMICEXCELLENCE AWARD1985-James T. Niemann, MD
1986-Glenn C. Hamilton, MD
1987-Charles G. Brown, MD
1988-Jerris R. Hedges, MD
1989-Richard F. Edl ich, MD, PhD
ACADBMIC LEADERSHIPAWARD1989-Ronald L. Krome, MD
SILVER TONGUE ORATORDEBATE AWARD1979-Ann L. Harwood-Nuss, MD
1980-Peter Rosen, MDl98l-Jerome L. Hoffman, MD
1982-Glenn C. Hamilton, MD
1983-Frederick B. EPstein, MD
1984-Marcus L. Mart in, MD
1985-Paul M. Paris, MD
1986-Daniel Danzl, MD
1987-Nicholas Benson, MD
1988-Daniel Danzl, MD
PASTUA/EM
l97O-19'1 l-Charles FreY, MD
l97I-1972-Alan R. Dimick, MD
1972-1973-Probert B. Rutherford, MD
1973-1974-James R. Mackenzie, MD
197 4-19'7 s-George Johnson, Jr', MD
1975-19'76-Leslie E. Rudolf, MD
1976-1977-David K. Wagner, MD
l9'77-1978-Carl Jelenko, III, MD
1978-1979-Ronald L. Krome, MD
1979-1980-Kenneth L. Mattox, MD
1980-1981-W. Kendall McNabneY, MD
1981-1982-Joseph F. Waeckerle, MD
1982-1983-Barry W. Wolcott, MD
1983-1984-Jack B. Peacock, MD
1984-1985-Richard C. LevY, MD
1985-1986-steven J. Davidson, MD
1986-1987-Richard M. Nowak, MD
1987-1988-Ernest Ruiz, MD
PRESIDENTSSTEM
1975-1976-Robert H. DaileY, MD
197 6-197'7 -Peter Rosen, MD
197'7-19'78-C. C. Roussi, MDt
1978-1979-G. Richard Braen, MD
1979-1980-HarveY W. Meisl in, MD
1980-1981-Frank J. Baker, I I , MD
l98l-1982-John R. LumPkin, MD
1982-1983-Harold A. JaYne, MDf
1983-1984-Kenneth V. Iserson, MD
1984-1985-Glenn C. Hamilton, MD
1985-1986-Daniel Schelble, MD
1986-1987-Thomas O. Stair, MD
1987-1988-Mary Ann CooPer, MD
1988-1989-Gabor D. Kelen, MD
SAEM
1988-1989-James T. Niemann, MD
IMAGO OBSCURA AWARD1976-Norman E. McSwain. Jr.. MD1977-Sung Rock Lee, MD1978-G. Patrick Lilja, MD1979-Stephen Karas, MD1980-Jack Goldberg, MDl98l-Robert Knopp, MD1982-Blaine C. White, MD1983-Richard C. Levy, MD1984-Glenn C. Hamilton, MD1985-Jerris R. Hedges, MD1986-David DuBois, MD1987-Norman Abramson, MD1988-Charles G. Brown, MD
MACKENZIE AWARD1976-James R. Mackenzie, MD1977-Cyril T. M. Cameron, MDf1978-John H. Hughes, MD1979-Joseph F. Waeckerle, MD1980-Kenneth L. Mattox, MD198l-Barry W. Wolcott, MD1982-Hubert T. Gurley, MD1983-Ronald L. Krome, MD1984-Charles F. Babbs, MD1985-Blaine C. White, MD1986-James T. Niemann, MDI 987-Arthur Kellermann. MD1988-Richard E. Burney, MD
Charter MeetingNovember 18, 1970Denver, Colorado
lst Annual MeetingM a y 1 4 - 1 5 , l 9 7 lAnn Arbor, Michigan
2nd Annual MeetingMay 12-13, 1972Washington, D.C.
3rd Annual MeetingMay 23-25, 1973Hamilton, Ontario
4th Annual MeetingMay 28-June l , 1974Dallas, Texas
5th Annual MeetingMay 20-24, 1975Vancouver, British Columbia
6th Annual MeetingM a y l l - 1 5 , 1 9 7 6Philadelphia, Pennsylvanra
PAST ANNUAL MEETINGS
7th Annual MeetingMay 15-18, 1977Kansas City, Missouri
8th Annual MeetingMay l8-20, 1978San Francisco, Cali fornia
9th Annual MeetingMay 24-26, 1979Orlando, Florida
10th Annual MeetingApri l 20-23, 1980Tucson, Arizona
l lth Annual MeetingA p r i l l 3 - 1 5 , 1 9 8 1San Antonio, Texas
l2th Annual MeetingApri l 15-17, 1982Salt Lake City, Utah
l3th Annual MeetingJune 1-4, 1983Boston, Massachusetts
l4th Annual MeetingMay 22-25, 1984Louisville, Kentucky
l5th Annual MeetingMay 2l-24, 1985Kansas City, Missouri
16th Annual MeetingMay 13-15, 1986Portland, Oregon
lTth Annual MeetingMay L9-21, 1987Philadelphia, Pennsylvania
l8th Annual MeetingMay 24-26, 1988Cincinnati, Ohio
l9th Annual MeetingMay 22-25, 1989San Diego, California

ANNUAL BUSINESS MEETING AGENDA
l. Amendments to the constitution and Bylaws, Louis Ling, MD, Secretary/Treasurer
The following five amendments have been proposed and approved by the constitution and Bylaws committee and the Board of Directors and
have been submitted to the membership vii the March isiue of the SAEM newsletter for consideration. The Constitution and Bylaws (with
the proposed changes ln italics and the proposed deletions crossed out) is provided in this program' Only active members of the organization
ure eligible to vote on amendments to the Constitution and Bylaws'
Amendment l: Article III, Section 2,3 (a) of the constitution. This amendment changes the criteria for emeritus membership from l0
years of service to the organization and an age of 60 years to 15 years of service and an age of 65'
Amendment 2: Article II, Section 2, (a) of the Bylaws. This amendment would change the criteria for election of the vice-president position
so that candidates for this position are not required to be a current or a past member of the Board of Directors'
Amendment 3: Article II, Section 4 of the Bylaws. This amendment would change the criteria for election of the program chairman so
that candidates for this posiiion are not required io be current members of the Program Committee' This amendment would also allow nomina-
tions from the floor for the position of program chairman'
Amendment 4: Article II, Section 6 of the Bylaws. This amendment would change the criteria for the convening of Board of Directors
meetings so that the Secretary/Treasurer would need to inform members of the Board of meetings 7 days in advance, instead of requiring
the SeJretary/Treasurer to inform all members 60 days in advance of Board meetings'
Amendment 5: Article III, Section I of the Bylaws. This amendment would make consistent the establishment of a quorum at the annual
business meeting so that a quorum would be a majority of the active members present and voting. This quorum is already established for
the amendment of Constitution and Bylaws changes in Article VII and Article VIII of the Constitution'
2. Elections, Louis Ling, MD, Secretary/Treasurer
The slate of nominees is listed below and photos and biographical information on each candidate is provided in this program. only active members
of the organization are eligible to vote in the elections'
President-Elect - (one l-year position)
Jerris R. Hedges, MD
Board of Directors - (three 2-year positions)
William G. Barsan, MDNicholas H. Benson, MDLouis Binder, MDMary Ann Cooper, MDDaniel Danzl, MDLewis R. Goldfrank, MDRichard M. Nowak, MD
Research Committee Chairman - (one 2-year position)
William H. Spivey, MD
3. Secretary/Treasurer's Report, Louis Ling, MD, Secretary/Treasurer
A. Membership at APril 28, 1989: 1,494Active: 902Associate: 248
B. Finance Report - Year Ending December 31,
RevenuesDues
Annual Meeting
Symposium
EMRA
Interest
Mailing List Sale
EMF Contributions
Other
TOTAL
Program Committee Chairman-Elect - (one 3-year term to begin May
1990)
Gary Krause, MDJames T. Niemann, MD
Nominating Committee Members - (two 2-year positions)
John A. Marx, MDPaul Pepe, MDDaniel T. Schelble, MDJ. Douglas White, MD
Constitution and Bylaws Committee Member - (one 3-year position)
Marcus L. Martin, MDJames D. Woodburn, Jr ' , MD
Emeritus: l3Honorary: 12
1988
r74,59937,84516,125?5 n?t *
t6,7131,6254,465
580
$286,984
83,50647,44116,34820,523*34,63129,97l**16,948r<+*
$249,368
Expenses
Salaries, Wages and PaYroll Taxes
Annual Meeting
Symposium
EMRA
Postage and TelePhone
Other Administration
Committees and RePresentattves
TOTAL
*EMRA newsletter and 1989 Job Catalog (profit belongs to EMRA)**office rent and insurance, newsletter printing, g"n"J p.iiting, accounting, bank charges, depreciation, computer' and photocopying expenses'
,r**Annalssubscriptions, AAMC, EMF, AMA Commission on-BUS, EMRA representative, STEM, 6th world congress, EMRS' Committees'
and Board exPenses.
1)

STEM Annual Business Meeting, Robert Prosser, MD, STEM Secretary/Treasuter
The active membership of STEM are eligible to vote on the following two resolutions which will complete the nearly two-year process of
amalgamating the Society of Teachers of-Emergency Medicine and the University Association for Emergency Medicine into the Society for
Academic Emergency Medicine.
BE IT RESOLVED that the Board of Directors of the Society of Teachers of Emergency Medicine is instructed to dissolve the organization
as soon as possible after satisfying all legal requirements. Thls amendment supersedes all other provisions of the Constitution and Bylaws of
the Society.
BE IT RESOLVED that the Board of Directors of the Society of Teachers of Emergency Medicine will transfer all assets of the Society and
all debt liability to the Society for Academic Emergency Medicine immediately before dissolving the Society. This amendment supersedes all
other provisions of the Constitution and Bylaws of the Society.
American Board of Emergency Medicine Report, Judith E. Tintinalli, MD, ABEM President
Annals of Emergency Medicine Report, Joseph F' Waeckerle, MD, Editor
President's Address, James T. Nietnann, MD
8' Introduction of New President: Arthur B' sanders' [{dD' rarnes T' Niemann' MD
9. New Business
Adjournment
iilt lI
riiiiil r
l ,
,!c
;*i

SLATE OF
PRESIDENT-ELECT
Jerris R. Hedges, MD, MS
Jerris R. Hedges, MD, MS, is anassociate professor of EmergencYMedicine in the Division of EmergencyMedicine and the Director of ResearchPrograms at the Oregon Health SciencesUniversity in Portland, Oregon. Dr.Hedges has been a member of UA/EMsince 1977 and a member of STEM since1980. He is currently a member of theSAEM Board of Directors (1986-1989)and has served on the UA/EM LongRange Planning Committee (1984- 1987),the UA/EM Program Committee(1985-1989), and as Chairman of theUA/EM Prosram Commi t tee
(1986-1989). Dr. Hedges has served on the STEM Faculty Develop-ment Committee (1983-1988). Dr. Hedges was a moderator at the 1988UA/EM-IRIEM Research Symposium. In 1988, Dr. Hedges was therecipient of the Harold Jayne Academic Excellence Award. Dr. Hedges
has been an item writer for the American Board of Emergency Medicinesince 1986. He is a member of the Editorial Board of the Annals of
Emergency Medicine, Joumal of Emergency Medicine , and Emergen-cy Medicine and Ambulatory Care News. He is a guest reviewer for
the American Journal of Emergency Medicine and Resuscitation' Heis a 1976 graduate of the University of Washington School of Medicine
and he completed his Emergency Medicine Residency in 1979 at theMedical College of Pennsylvania.
BOARD OF DIRECTORSWilliam G. Barsan. MD, is an associateprofessor at the Department of Emer-gency Medicine at the University of Cin-cinnati. Dr. Barsan has been a memberof UA/EM since 1980 and was a memberofthe Executive Council, from 1985 to1988. Dr. Barsan was a member of theSTEM Program Committee from1982-84 and served as chairman in1983-84. He served on the UA/EM Pro-gram Committee from 1982-85 and onthe Constitution and Bylaws Committeefrom 1981-84. He was the chairman ofthe 1988 UA/EM-IRIEM Research Sym-posium on Emergency ThrombolYtic
NOMINEES1988 STEM Debates. He serves as a consulting reviewer for the
American Journal of Emergency Medicine and contributing editor of
the Aero Medical Journal. He graduated from the University of SouthDakota School of Medicine and in 1983 completed an emergency
medicine residency at the University of Illinois Affiliated Hospitals'
He is currently an assistant professor and Vice Chairman of the Depart-
ment of Emergency Medicine at East Carolina University.
, Louis Binder, MD' is an assistant pro-
,.ir,' fessor in the Division of Emergencyr.,,t Medicine at the Texas Tech University
. Regional Academic Health Center at El
,,,,.., Paso, and is also the Assistant Dean for'
. Graduate Medical Education and StudentAffairs at that institution. He graduatedfrom the University of Minnesota Medi-cal School in 1980 and comPleted anEmergency Medicine residency in 1983at Truman Medical Center. He is thechairman of the SAEM UndergraduateCommittee, was elected to the Constitu-tion and Bylaws Committee in 1988, andwill be moderating a panel discussion at
the 1989 SAEM annual meeting. He is a member of the Education
Committee, the Public Relations Committee, and the Committee on
Academic Departments, and has been a member of SAEM since 1982'
He was a participant in the STEM Goals and Objectives Project, and
was a member of the UAEM Membership Committee in 1986 and the
Scientific Consensus Committee in 1986' He is an examiner for the
American Board of Emergency Medicine, and a reviewer for Annals
of Emergency Medicine and the American Journal of Emergency
Medicine.
Mary Ann Cooper, MD, is an assistantprofessor and director of research at theDivision of Emergency Medicine at theUniversity of Illinois. She has been amember of UAEM since 1977, servingon the Constitution and Bylaws Commit-tee, Program Committee and the Exec-utive Council where she served as an at-large member from 1982 to 1988 andsecretary/treasurer from 1985 to 1988.She was local arrangements Chairmanfor the 1984 Annual Meeting inLouisville. She has been a member of theJoint Academic Affairs Task Force since1986. She has also been an active
member of STEM having served on its Board of Directors since 1980
as well as newsletter editor from 1983 to 1986. She was President of
STEM in 1988 and was a member of the Amalgamation Task Force.
She has been an ABEM examiner since 1982, on the editorial boardof the Journal of Emergency Medicine and a grant reviewer for the
Australian Research Council. The Emergency Medicine Residents'
Association awarded her its Excellence in Teaching Award in 1988.Dr. Cooper graduated from Michigan State University College of
Human Medicine in 1975 and completed an Emergency MedicineResidency Program at the University of Cincinnati in 1978.
Emergencies. He has been a moderator at the 1983, 1984, 1985 and
1987 Annual Meetings. He has been a member of the American Jour-nal of Emergency Medicine editorial board and a guest reviewer of
Journal of Emergency Medicine since 1983 and an examiner for ABEMsince 1983. Dr. Barsan graduated from Ohio State University Collegeof Medicine in 1975 and completed an Emergency Medicine residen-cy in 1979 at the University of Cincinnati.
Nicholas H. Benson, MD, has been amember of UA/EM since 1984 and amember of STEM since 1983. He is cur-rently a member of the STEM Board ofDirectors having been elected in 1988.He has been a member of the EMSEducators Committee since 1986 andserved as its chairman until 1988. He hasserved on the Publications Task Forcesince 1987. He was a member of theSTEM Undergraduate Curriculum Pro-motion Committee from 1983-87' In
1987 he won the STEM Silver TongueOrator Award and participated in the
Louis Binder, MD
Mary Ann Cooper, MD
1$l
+'
editorial board member of the American Jourrutl of Emergency Mer)icinesince 1984 and a reviewer for Journal oJ Emergency Medicine since1987. Since l98l he has also served as a reviewer for Annals oJEmergency Medic:ine. He was a moderator at the l9g3 and lggg An-nual Meetings. He was also a faculty member at the t9g7 and lgggUA/EMIIRIEM Research Symposiums. He is a 1976 graduate of OhioState University and he completed his entergen.y . ."di. in. residencyin 1979 f iom the University of Louisvi l le.
Daniel Danzl, MD, is an associate pro-fessor in the Department of EmergencyMedicine at the University of Lousiville.Dr. Danzl has been a member ofUA/EM since 1979 and is currently amember of the SAEM Board of Direc-tors, having been elected to a one yearterm in 1988. He was the winner of the1986 and 1988 STEM Silver OratorAward. He served on the UA/EM In-dustrial/Governmental Relations Com-mittee from 1984-85 and a member ofthe Nominating Committee unti l 1988.Dr. Danzl has been an examiner forABEM since 1982. He has been an
Lewis R. Goldfrank, MD, is anassociate cl inical professor of InternalMedicine at the New York UniversitySchool of Medicine. He is the Directorof the Departments of EmergencyMedicine at Bel levue Hospital Centerand New York University MedicalCenter. He is also the Medical Directorof the New York City Poison ControlCenter. Dr. Goldfrank has been amember of UA/EM since 1974. He hasbeen an Ad Hoc reviewer in toxicologyfbr the 1987, 1988, and 1989 AnnualMeetings as well as serving as a
Richard M. Nowak, MD, is the chairof the Department of EmergencyMedicine at Henry Ford Hospital and aclinical assistant professor in the sectionof emergency medical services at theUniversity of Michigan. Dr. Nowak isa past president of UA/EM and has beena member of UA/EM since 1976. Dr.Nowak served on the Executive Coun-ci l from l98l to 1988 and served on theAmalgamation Task Force. He is cur-rently the chairman of the International
Nowak was a member of the UA/EM Nominating Committee in1979-8 I and chair of the Joint Academic Affairs Task F:orce since 19g6.He has been an examiner for ABEM since 1983 and is a reviewer forJAMA and Annals of Emergency Medicirze, as well as a member ofthe editorial board of the American Journal of Emergency Medicine.He has been a moderator at the 1984, 1985, and 1986 Annual Meetinss.He graduated from the University of Toronto Medical School in 1972,completed postgraduate training in Internal Medicine at MontrealGeneral Hospital in 1973 followed by research fellowship in the clinicalscience division at the University of Toronto in 1975.
RESEARCH COMMITTEE CHAIRMANWilliam H. Spivey, MD, is an assistantprofessor in the Department of Emergen-cy Medicine at the Medical College ofPennsylvania where he serves as Assis-tant Clinical Director and Director ofResearch. Dr. Spivey is currently thechairman of the Research Committee andwas appointed chair in 1988. Dr. Spiveyhas been a member of UA/EM since1982 and is currently a member of theConstitution and Bylaws Committee. Hewill chair the Constitution and BylawsCommittee 1989-90. He has been an adhoc reviewer for the Program Commirtee since 1987 and was a moderator dur-
ing the 1986 Annual Meeting and participated as a debator in the l9g6STEM Debates. He is a reviewer for the Annals of Emergency Medicineand a member of the Journal of Emergency Medicine Editorial Board.Dr. Spivey graduated fiom East Carolina University Medical Schoolin l98l and completed an emergency medicine residency at the medicalcol lege of Pennsylvania in 1985.
PROGRAM COMMITTEE CHAIRMANGary Krause, MD, is an assistant pro_fessor in the section of EmergencyMedicine at Wayne State University. Hehas been a member of UA/EM sincel98l and is currently a member of theProgram Committee. He has served asan ad hoc abstract reviewer and as amoderator for the 1987 and 1988 AnnualMeetings and will be a moderator at the1989 Annual Meeting. He is a memberof the Resuscitation Editorial Board andis a reviewer for Annals of EmergencyMedicine. Dr. Krause graduated fromWayne State University School of Medi_cine in l98l and completed a residency
Wayne State University in 19g4.
James T. Niemann, MD, is an associateprofessor of medicine at UCLA. Dr.Niemann has served on the UA/EM Ex_ecutive Council since 1985 and is thecurrent president of SAEM. He has beena member of the Editorial Board ofAnnals of Emergency Medicine since1982 and is also a member of the Edi_torial Board of Critical Care Medicine.He is a manuscript consultant/reviewerfor Annals, the American Journal ofEmergency Medicine, as well as foimany other joumals including./,4M1 andCirculation. He was the first recipient of
rhe U n i ve rs i ty or B ru xer r es,#:LT['Jr',Ll ?:ti #;, tjij Hilfi:j:a residency in Internal Medicine at Montefiore Hospital and MeclicalCenter in 1973. He has been an examiner fbr ABEM since l9g5 andthe American Board of Medical Toxicology since 19g3. He is areviewer for the American Journal of Emergenr:y Medicine and anEditor for the.journals of Clinicat Toxirnlogy, and Mer)ical Toxicrfutgyand Adverse Drug Experience.
Gary Krause, MD
in emergency medicine at
Richard M. Nowak, MD Committee and is collaborating with the6th World Congress on Emergency andDisaster Medicine and a co-sponsored
meeting with the Emergency Medicine Research Society. He was thesecretary/treasurer of UA/EM in 1984-85 and has served on theNominating Committee. He has been a member of STEM since 1975and was a member of the STEM Board of Directors in lggl-g3. Dr.
/ J
James T. Niemann, MD

the Hal Jayne Academic Excellence Award in 1985 and served three
years on the UA/EM Constitution and Bylaws Committee, serving as
chair in 1987-1988. Dr. Niemann served on the Amalgamation Task
Force, the Academic Affairs Task Force, and in 198l-1982 on the
STEM Public Education Committee, as well as the UA/EM Educa-tion Committee in 1984. He has been a member of STEM since 1980
and a member of UA/EM since 1981 and served on the STEM Board
of Directors in 1981-1982. Dr. Niemann graduated from the Univer-
sity of California School of Medicine in 1976 and completed his resi-
dency in 1979 at Los Angeles County Harbor-UCLA Medical Center'
NOMINATING COMMITTEEJohn A. Marx, MD, is an associate Pro-fessor in the Department of Surgery,Section of Emergency Medicine andTrauma at the University of ColoradoHealth Sciences Center. He is AssistantDirector of the Department of Emergen-cy Medicine at Denver General Hospitaland has been Research Coordinator forthe Denver Affiliated Emergency Medi-cine Residency Program since 1980. Heattended Stanford Medical School andtrained in the Denver Affiliated Residen-cy in Emergency Medicine from 1978 to1980. Dr. Marx has been a member ofUA/EM since 1981 and has been amoderator at two annual meetings
and will be a moderator at the 1989 Annual Meeting. Dr. Marx is the
Section Editor for Original Contributions for the "/ou rnal of Emergen-
cy Medicine. He has been a guest editorial reviewer for JAMA and
the American Journal of Emergency Medicine.
Paul Pepe, MD
Paul Pepe, MD, is an associate Pro-fessor of medicine and surgery at BaylorCollege of Medicine and director of theHouston EMS system. He has rePre-sented UA/EM on the AMA Commis-sion on EMS for the last four years andwas a moderator at the 1987 AnnualMeeting. Dr. Pepe has been a memberof UA/EM since 1983. In 1976 hegraduated from the University of Califor-nia School of Medicine, completed an in-ternal medicine residency in 1979 andthen several clinical and researchfellowships in pulmonary-critical care,trauma, and surgical critical care'
Daniel T. Schelble' MD, is an associateprofessor in Emergency Medicine atNortheastern Ohio Universities Collegeof Medicine. He is currently a memberof the Nominating Committee, havingbeen elected to a one year term in 1988'Dr. Schelble served on the STEM Boardof Directors from 1982-87 and was thepresident of STEM in 1985-86. He hasalso coordinated the Hal Jayne AcademicExcellence Award since its inception in1986. He served on the Joint AcademicAffairs Task Force from 1985-87 andwas a member of the Faculty Develop-ment Committee. He was the STEM
Daniel T. Schelble, MD
gency Medicine at Akron General Medical Center.
,!u,.,..i11!ju'' r;llhl'l 'liiirlr'rrl J. Douglas White, MD' clinical direc-
to r o f Emergency Med ic ine a tGeorgetown University Medical Center,is a graduate of Yale University Schoolof Medicine. He completed a residencyin internal medicine at Bellevue-NewYork University, followed bY fel-lowships in clinical emergency medicineat Massachusetts General Hospital andresearch at Harvard Medical School. Dr.White is currently editor of TheAmerican Journal of EmergencYMedic ine . He is a lso D i rec torof Research in the DePartment ofEmergency Med ic ine and is an
J. Douglas White, MD
associate professor of emergency and internal medicine at GeorgetownUniversity. A member of UA/EM since 1980, Dr. White was chair-
man of the Governance Committee from 1986-88, and is currently
chairman of the Governmental Affairs Committee. He is currently a
member of the Nominating Committee. He represented UA/EM on
the Joint Academic Affairs Task Force, and served three years on the
Constitution and Bylaws Committee'
CONSTITUTION AND BYLAWS COMMITTEEMarcus L. Martin, MD, is an associateprofessor of Emergency Medicine at theMedical College of PennsYlvania,A l leghney Campus, EmergencYMedicine Residency Director andAssociate Director of Emergency Ser-vices at Allegheny General Hospital' Dr.Martin has been a member of STEM andUAEM since 1984 and has participatedin the STEM Goals and Objectives pro-iect. He was a member of the STEMPublic Relations Committee 1984- 1985.Dr. Martin was the winner of the 1984STEM Silver Tongue Orator Award, and
and also participated in the 1988 STEMDebate. He has been a reviewer for the
Annals of Emergency Medicine since 1985. As a charter member, Dr'
Martin graduated in 1976 from Eastern Virginia Medical School and
completed residency training in Emergency Medicine at the Universi-
ty of Cincinnati in 1981.
James D. Woodburn,Jr., MD' MS
James D. Woodburn, Jr., MD, MS,was the co-chairman of the 1989UA/EM-IRIEM Research SYmPosiumon Technology Applications. He was acontributing editor to the STEM newslet-ter in 1987 and 1988 and is currently amember of the Publications Task Force,as well as an ad hoc abstract reviewerfor the 1989 Annual Meeting' Dr.Woodburn served as the EMRA rePre-sentative to STEM and UA/EM from1985 to 1987. In 1986 he coordinated thefirst Resident Research Forum whiqh isheld at the Annual Meeting and in 1987he received the EMRA National Leader-
representative to the AAMC in 1983 and has been a member of UAEM
since 1984. He graduated from the University of Wisconsin School
of Medicine in 1972 and in 1977 completed a residency in Emer-
ship Award. Dr. Woodburn graduated from the University of Wisconsin
School of Medicine in 1983 and completed an Emergency Medicine
residency at Hennepin County Medical Center in 1987, which was
followed by a fellowship in Emergency Medicine which was completed
in August, 1988. Dr. Woodburn is currently an emergency physician
at HeilthEast Hospital Corporation in St. Paul and also at the Hen-
nepin County Medical Center.
a))) .:..:ilal::::' t:..1
llii;i11q
: ;
CONSTITUTION OF THE SOCIETYFOR ACADEMIC EMERGENCY MEDICINE
I7
ARTICLE I - NAMEThe name of this organization shall be, "The Society for
Academic Emergency Medicine," hereinafter referred to as,"The Association. "
ARTICLE II - OBJECTIVESSection 1: The objective of this Association is to improve the
emergency, urgent, or critical care of the acutely ill or injuredpatient by promoting research, by educating health care pro-fessionals and the public, by fostering relationships with organ-izations with a similar purpose, and by supporting the special-ized or multidiscipline care of such patients through researchand education. The Association will function as a scientific andeducational organization as defined in Section 501(c) (3) oftheInternal Revenue Code, as amended.
Section 2: The Association shall pursue its purpose by: l)sponsoring forums for the presentation of peer-reviewed scien-tific and educational investigations, 2) convening and sponsor-ing educational programs for health care professionals and thelay public, 3) promoting academic development and educationof its membership through specialized programs, 4) serving asan academic, university-based, and/or teaching hospital repre-sentative for the care of the acutely ill or injured patient, 5)developing l iaison with other organizations with a similar pur-pose, and 6) publishing research and educational data in thescientif ic and educational l i terature and other media availableto the lay public.
Section 3: A. This corporation is organized exclusively fbreducational and scientif ic purposes, including, fbr such pur-poses, the making of distributions to organizations that qualifyas exempt organizations under Section 501(c) (3) of the Inter-nal Revenue Code of 1954 (or the corresponding provision ofany future United States Internal Revenue Law).
B. No part of the net earnings of the col.poration shall inureto the benefit of, or be distributable to its members, Directors,Officers or other private persons, except that the corporationshall be authorized and empowered to pay reasonable compen-sation for services rendered and to make payments and distribu-tions in furtherance of the purposes set forth in paragraph Ahereof. No substantial part of the activities of the corporationshall be the carrying on of propaganda, or otherwise attemptingto influence legislation, and the corporation shall not participatein, or intervene in (including the publishing or distribution ofstatements) any political campaign on behalf of any candidatefor public office. Notwithstanding any other provision of thesearticles, the corporation shall not carry on any other activitiesnot permitted to be carried on (a) by a corporation exempt fromFederal Income tax under Section 501 (c) (3) of the InternalRevenue Code of 1954 (or corresponding provision ofany futureUnited State Revenue Law) or (b) by a corporation, contribu-tions to which are deductible under Section 170(c) (2) of theInternal Revenue Code of 1954 (or the corresponding provisionof any future United State Internal Revenue Law).
ARTICLE III _ MEMBERSHIPSection l: Classifications. There shall be seven classes of
membership: active, associate, emeritus, resident/fellow, hon-orary, and international active and international associate.
Section 2: Qualifications. (1) Candidates for activemembership shall be individuals with an advanced degree (MD,PhD, DO, PharmD, DSc, or equivalent) who hold a medicalschool or university faculty appointment and who actively par-ticipate in acute, emergency, or critical care in an administrative,teaching, or research capacity, (b) individuals with similardegrees in active military service (U.S. or abroad) who activelyparticipate in acute, emergency, or critical care in an ad-ministrative, teaching, or researih capacity. (c) Individuals whootherwise meet qualifications for active membership as definedabove but who do not hold a university faculty appointment maypetition the Membership Committee for consideration for ac-tive membership status, if desired. (2) Candidates for associatemembership shall be health professionals, educators, govern-ment officials, members of lay or civic groups, or membersof the public at large who may have an interest or desire to par-ticipate in pursuing the purposes and objectives ofthe Associa-tion. (3) Candidates for emeritus membership shall be (a) ac-tive members who seek such status and who have given *&/5continuous years of active service to the Association and haveattained the age of6U65 years (b) other active members whounder special circumstances are invited fbr such emeritus statusby the Membership Committee. (4) Candidates for resi-dent/fellow membership must be resident(s) or f-ellows in resi-dency training program(s) who have an interest in emergencymedicine. (5) Candidates fbr honorary membership shall be indi-viduals who have made outstanding research or educational con-tributions to the purpose and objectives of the Association. (6)Candidates for international membership shall be individualswho reside outside the U.S. and who meet qualif lcations fbractive or associate membership as described above. Such can-didates may apply for active, associate, or other membershipin the Associat ion.
Section 3: Member Rights and Privileges. All members mayhave the privilege of the floor and of serving on the commit-tecs of the Association. All members of the Association mayserve on the Board of Directors or as a committee Chairper-son. Only active members shall have voting rights and shallserve as officers of the Association.
Seoion 4; The Association shall not discriminate, with respectto its membership, on the basis of race, sex, creed, religionor national origin.
ARTICLE IV _ OFFICERSSection .1: The officers of this organization shall be the presi-
dent, Vice-President, and Secretary-Treasurer.
Section 2: Board of Directors shall serve as the governingbody of the Association. The Board of Directors shall consistof the above officers, the Program Committee Chairman, theimmediate past president, and five Councilmen-at-Large. Bothactive and associate members may serve on the Board of Direc-brs, but only active members may be officers of the Association.
ARTICLE V - COMMITTEESThe standing committees of the Association shall be: (l) Nom-
inating Committee, (2) Membership Committee, (3) programCommittee, (4) Constitution and Bylaws Commiffee, (5) Educa-tion Committee, (6) Research Committee, (7) Liaison Committee
77

to the Association of American Medical Colleges, (8) Govern-mental Affairs Committee, and (9) Committee on InternationalAffairs. Additional committees may be created by the Boardof Directors and ad hoc committees may be created by the Presi-dent to aid in the Association's efforts to achieve and furtherits goals.
ARTICLE VI - ANNUAL MEETINGSection 1.' There shall be an annual meeting of the Associa-
tion. This meeting shall consist of an educational and scientificprogram and a business session.
Section 2: The Board of Directors, by majority vote, maycall, upon 30 days notice, a special meeting of the membershipor standing committee to conduct any business that the Boardof Directors shall place before the membership or standingcommittee.
Section 3: The Board of Directors may call and conduct anyspecial meeting by mail. For purposes of notice, the meetingdate shall be a date set for the return of mail ballots and it shallbe called the voting date. Adoption of any proposal, resolutionor amendment by mail ballot shall be achieved by affirmativevote of a majority of voting active members unless otherwiseprovided by another provision of this constitution. Only thosemail ballots received at the business office of the Associationwithin 30 days subsequent to the voting date shall be counted.
ARTICLE VII _ BYLAWSSection 1: Bylaws may be adopted or amended at any annual
or special meeting of the membership.
Section 2; Proposed amendments to the bylaws shall be sub-mitted in writing to the Secretary/Treasurer by three membersat least 60 days prior to the meeting at which they are to beconsidered. The Secretary/Treasurer shall mail the proposedamendments to the membership at least 30 days prior to thatmeeting.
Section 3; The Board of Directors may, by resolution, pro-pose amendments to the bylaws; provided the proposed amend-ments are mailed to the membership at least 30 days prior tothe meeting at which they are to be considered.
Section 4: Adoption of a bylaw amendment shall be by amajority vote of the active members present and voting at anyannual or special meeting.
ARTICLE VIII - ADOPTION OF THEAMENDMENTS TO THE CONSTITUTION
Section 1; The constitution may be adopted or amended atany annual or special meeting of the membership.
Section 2; Proposed amendments to the constitution shall besubmitted in writing to the Secretary/Treasurer by three mem-bers at least 60 days prior to the meeting at which they are tobe considered. The Secretary/Treasurer shall mail the proposedamendments to the membership at least 30 days prior to thatmeeting.
Section 3.: The Board of Directors may, by resolution, proposeamendments to the constitution; provided the proposed amend-ments are mailed to the membership at least 30 days prior tothe meeting at which they are to be considered.
Section 4; Adoption of a constitution amendment shall be bya majority vote of the active members present and voting at anyannual or special meeting.
ARTICLE IX _ DISSOLUTIONUpon the dissolution of the corporation, the Board of
Directors shall, after paying or making provision for the pay-ment of all of the liabilities of the corporation, dispose of allofthe assets ofthe corporation exclusively for the purposes ofthe corporation in such manner, or to such organization ororganizations organized and operated exclusively for charitable,educational, religious or scientific purposes as shall at the timequalify as an exempt organization or organizations under Sec-tion 501(c) (3) of the Internal Revenue Code of 1954 (or thecorresponding provision of any future United States InternalRevenue Law), as the Board of Directors shall determine. Anysuch assets not so disposed of shall be disposed by a Court ofCompetent Jurisdiction in the Council in which the principaloffice of the corporation is then located exclusively for suchpurposes or to such organization or organizations, as said courtshall determine, which are organized and operated exclusivelyfor such purposes.
Section 2: Dues. Annual dues for active, associate, resi-dent/fellow, and international members will be established bythe Board of Directors. Honorary and emeritus members willnot pay dues. Membership in the Association may be terminatedfor nonpayment of dues.
Section 3: Rights and privileges. All members have the priv-ilege of the floor at business meetings of the Association andmay serve as a committee member, committee chair, orMember-at-Large of the Board of Directors. Only active mem-bers may vote and serve as officers. Any member may submitagenda items for consideration by the Board of Directors.
BYLAWS OF THE SOCIETY FORACADEMIC EMERGENCY MEDICINE
ARTICLE I _ MEMBERSHIPSection l: Application Process. Membership application forms
may be obtained from the Secretary/Treasurer through the Ex-ecutive Director of the Association. The Applicant must returnthe completed application forms and supporting letters to theExecutive Director of the Association at least one month priorto Board of Directors meeting in order to be considered formembership at that time. The qualifications of applicants formembership will be reviewed by the Membership Committeeat each meeting of the Board of Directors. Approval of ap-plicants by the Council Board shall constitute election to oneof the membership categories, effective immediately.

ARTICLE II -BOARD OF DIRECTORS
Section l: Members. The Board of Directors shall consist ofthe President, Vice-President (President-Elect), the Secretary/Treasurer, the Immediate Past president, the program Chair,and five Members,at-Large.
Section 2: Election of Officers. (a) The Vice-president shallbe elected for a term of one year with automatic succession fromVice-President to President the following year. During this twoyear period, the elected member will serve as an officer of theAsso_ciation. Following terms of Vice-president (president_elect)and President, this member will automatically assume the posi_tion of Immediate Past president. Election as Vice-presidentshall confer Board of Directors membership for a minimum ofthree years. Nominees for this office will be selected by theNominating Committee,
+ne+oar+ofBiteetors, and must have agreed to stand for elec_tion prior to formal nomination for election at the business ses_sion of the annual meeting. Alternative nominationsofequaHy
@willbe acceptecl from the ilooi.Such nominees must also agree to stand for election. Electionshall be by majority vote of the active members present andvoting at the business session of the annual meeting. The Vice_President may also be elected or appointed as Chair of otherstanding or ad hoc committees, with the exception of the pro_gram Committee, and shall be an ex-officio member of all stand_ing committees. (b) The Secretary/Treasurer shall be electedto a three year term. An active member may serve only oneterm as Secretary/Treasurer. Nominees for this office shall beselected by the Nominating Committee and must have asreedto stand for election prior to their formal nomination fbr"elec_tion at the business session of the annual meeting. Alternativenominations may be offered from the floor. Such nominees mustalso agree to stand for election. Election shail be by majorityvote of the active members present and voting at the buiines.ssession of the annual meeting. The Secretary/Tr"arure, rnuyalso be elected or appointed as the Chair of standing or ad holcommittees, with the exception of the Nominating tommitteeand Program Committee, and may serve as a member of allcommittees.
Section 3 : Election of Members-at-lnrRe. Members_at_Larseshall be electcd ro two year rerms. the t-rms being ,tugg.."i.Members-at-Large may only be elected for two consecutlveterms. Nominees for the above offices shall be selected by theNominating Committee and must have agreed to stand for elec_tion prior to their formal nomination for election at the businesssession of the annual meeting. Alternative nominations may beoffered from the floor. Such nominees must also agree to standfor election. Election shall be by majority vote of the activemembers present and voting at the business session of the an_nual meeting.
Members-at-Large may also be elected as Chairs of standinscommittees, with the exceptions of the Nominating and prolgram Committees, appointed as Chairs of ad hoc committees,or serve as a member of standing or ad hoc committees, withthe exception of the Nominating Committee.
Section 4: Election of Program Committee Chair. The pro_gram Committee Chair shall be elected to a three year term.Norin"esfirmberq and must have agreed to stand forilection prior totheir formal nomination for election at the business session ofthe annual meeting. Alternative nominations willtstbe acceptedfrom the floor. Such nominees must also agree to ,tond yo,
election.Election shall be by majority vote of the active memberspresent and voting at the business session of the annual meetins.The Program Committee Chair shall not be eligible for oth6relected positions within the Association, but may serve as an ap-pointed member of other standing or ad hoc committees.
Section 5: Terms of Office. Terms of office will begin at theconclusion ofthe annual business meeting. The president shallappoint eligible Association members to fill vacancies and unex_pired terms on the Board of Directors and standing and ad hoccommittees until the next scheduled election.
Section 6: Meetings of the Boctrd of Directors. Meetings ofthe Board of Directors will be convened at least twice durinsthe term of the President of the Association. Additional meetineimay be convened at the President's discretion or by petitiJnof six members of the Board of Directors. A final notice of timeand place of such meetings shall be sent to all members of the
-Asseeiafier+ Bo a rd by the Sec retary /Treasu rer at I east 5& Z day sbefore the meeting. Six members of the Board of Directors willconstitute a quorum. Members of the Association, regardlessof membership category, may submit agenda items. Such itemsmust be submitted within 30 days of the meeting date. Meetingsof the Board of Directors are open to all members of the Associa-tron and to the public. Closed meetings of the Association'sofflcers and Executive Director may be convened by order ofthe President.
.Section 7: Duties of the President. The president shall pre_side over both the educational program and business sessionof the annual meeting of the Association, and the meetinss ofthe Board of Directors. It shall be the duty of the preside-nt tosee that the rules of order and decorum aie properly enforcedin all deliberations of the Association, to sign the approvedminutes of each meeting, and to execute all documents whichmay be required for the Association, unless the Board of Direc_tors shall have expressly authorized some other person to per_fbrm such execution. The president shall serve as Chair of theBoard of Directors and shall serve as an ex-officio member ofall committees. The President shall appoint members to fi l lvacancies and unexpired terms on the Board of Directors andstanding and ad hoc Committees unti l the next scheduledelect ion.
Section 8: Duties of the Vice-president (presiclent-Elect). TheVice-President shall preside in the absence ofthe president. TheVice-President shall serve as Chairman of the Nominatins Com_mittee and ex-officio member of all committees.
Section 9: Duties of the Secretary/Treasurer. It shall be theduty ofthe Secretary/Treasurer to preside in the absence ofboththe President and Vice-President. The Secretary/Treasurer shallkeep a true and correct record ofthe proceedings ofthe annualbusiness meeting and meetings of the Board of birectors, shallpreserve documents belonging to the Association and issuenotice of the annual business meeting and meetings of the Boardof Directors 60 days prior to such meetingr. ih" Secretary/Treasurer shall keep an account of the Association with its mem_bers and maintain a current register of members with dates oftheir election to membership and preferred mailing address, thelatter to be circulated annually to the membership w;thin 30 daysof the annual business meeting. The SecretaryiTreasurer shallbe re^sponsible for reporting unfinished business requiring ac-tron from previous meetings of the membership oi Boaid ofDirectors and will be responsible for the agenda of the annualbusiness meeting and meetings of the Board of Directors. TheSecretary/Treasurer shall collect the dues of the Association.make disbursements of expenses, and maintain the financial ac_counts and records of the Association.
79
The financial record will be presented to the membership at theannual business meeting, biannually to the Board of Directors,and at such times as requested by the President of the Associa-tion. The financial records of the Association shall be reviewedannually by two other members of the Board of Directorsappointed by the President, or a certified accountant or finan-cial consultant retained by the Board of Directors of theAssociation.
Section I0: Duties of Board of the Directors, Members-at-lnrge. Members-at-Large shall assume whatever duties areassigned by the Officers of the Association or by Articles inthe Bylaws of the Association.
Section I I: Duties of Program Committee Chair. Actingunderthe auspices of the President and Board of Directors of the Asso-ciation, the Program Committee Chair shall be responsible forthe Association's annual research and education meeting, as wellas other symposia or meetings sponsored or co-sponsored bythe Association to meet its purpose. The duties of the ProgramCommittee Chair shall include but not be limited to: (l) selec-tion of committee members, (2) selection of meeting sites, (3)designation of ad hoc committee members specifically selectedfor review of materials to be presented at the annual meetingor other Association meetings, (4) peer-review and selectionof papers to be presented at meetings or forums sponsored orco-sponsored by the Association, (5) publication of call-for-abstract notices, and (6) scheduling activities at the Associa-tion's annual meeting or other meetings sponsored or co-sponsored by the Association. Recommendations from the Pro-gram Commiffee Chair must be approved by the Board of Direc-tors by majority vote.
Section l2: Duties ofthe Past President. The Past Presidentshall assume whatever duties are assigned by the President orby articles in the Bylaws of the Association.
Section I 3: Absenteeism/termination of ffice. Absences canbe approved or excused only by the President. Two unexcusedabsences from scheduled Board of Directors meetings, annualbusiness meeting, or special meetings of the Board of Direc-tors during any term as a member of the Board of Directorsshall constitute a resignation. Such resignation shall be effec-tive two weeks after notification by the President. Any mem-ber of the Board of Directors may voluntarily resign and suchresignation will become effective immediately.
Section 14: Special meetings of the Board of Directors.Special, unscheduled meetings of the Board of Directors or theOfficers of the Association may be convened by the President,or by any six members of the Board of Directors. Upon peti-tion by 100 or more active members of the Association, statingthe reason(s) for calling a special meeting of the Directors orOfficers, the Secretary/Treasurer shall call such a meetingwithin 30 days of receiving the petition to be convened at a timeand place designated by the President.
ARTICLE III - MEETINGSSection l: Annual business meeting. An annual business meet-
ing of the membership of the Association shall be convened an-nually and in conjunction with the annual scientific and educa-tional meeting of the Association.@A majoriry of the active and voting members in good standingand in attendance shall constitute a quorum. Business itemspresented as informational or for vote by active members shallinclude but not be limited to: (1) a financial report from theSecretary/Treasurer, (2) amendments to the Constitution andBylaws of the Association, (3) election of officers, members
of the Board of Directors, and the Chairs and members of stan-ding committees of the Association, (4) reports of committeeactivities, (5) transaction of other business which may comebefore the membership, and (6) a "State of the Association"address by the President. Where dictated by the Constitutionand Bylaws, the Association shall be governed by a majorityvote of active members in attendance at the anriual businessmeeting. The President of the Association shall preside overthe meeting and the Secretary/Treasurer will circulate agendaitems to the membership 30 days before the annual businessmeeting. The Chairs of the Constitution and Bylaws Commit-tee and Nominating Committee will preside over the respec-tive parts of the annual meeting. The annual business meetingshall be held at a time and place determined by the Board ofDirectors of the Association approximately one year in advanceof the convocation.
Section 2: Between annual business meetings, within the pol-icies established by the Association's membership and the Con-stitution and Bylaws, the Association shall be governed by theBoard of Difectors. Actions of the Board of Directors shall bedetermined by a majority vote of those of its members presentat its meeting, six members constituting a quorum.
Section 3: Annual scientific and educational assembly. TheAssociation shall sponsor an annual scientific and educationalmeeting or assembly to meet its purpose and objectives. Thismeeting will include but not be limited to: (l) presentation oforiginal research in the sciences and educational methodology,(2) educational/research forums, (3) special programs for themembership as determined by the purpose and objectives of theAssociation, and (4) meetings of the standing and ad hoc com-mittees of the Association. The research and educational pro-grams of the annual meeting shall be open to the public andthe general membership of the Association in good standing.All meetings of standing and ad hoc committees are open tothe public and members of the Association in good standing,Programs for the annual meeting shall be arranged by the Pro-gram Committee and approved by the Board of Directors ofthe Association. A final notice of the time, place, and programof the annual assembly shall be sent to all members of theAssociation by the Secretary/Treasurer at least 30 days beforethe meeting.
Section 4: Special meetings sponsored or cosponsored by theAssociation. The Association may sponsor or cosponsor otherscientific or educational meetings of interest te the member-ship to meet its purpose and objectives. Such meetings shallbe convened by the President, Board ofDirectors, and ProgramCommittee Chair and publicized 30 days in advance by theSecretary/Treasurer.
ARTICLE IV - FINANCESSection,/r The annual membership dues for all members shall
be determined by the Board of Directors. The annual member-ship will be payable within 30 days of request by the Secre-tarylTreasurer. The Board of Directors may establish proce-dures and policies regarding non-payment of dues andASSESSMENTS.
Section 2: The Board of Directors shall adopt such member-ship schedules as is necessary to encourage participation by theinterested public.
ARTICLE V _PARLIAMENTARY AUTHORITY
Rule of order. Any question oforder or procedure not spe-cifically delineated or provided for by these bylaws and subse-

quent amendments shall be determined by parliamentary usageas contained in Robert Rules of Order (Revised).
ARTICLE VI _ STANDING COMMITTEESSection I: Nominating Committee. The Nominating Commit-
tee shall consist ofthe Vice-President, as Chair, the past presi-dent, a member of the Board of Directors elected for a one yearterm by the board, and three elected members who may notbe members of the Board of Directors. The latter shall servestaggered two year terms. It shall be the task of this committeeto select a slate ofofficers to fill the naturally occuring vacan-cies on the Board of Directors and elected positions on the stand-ing committees of the Association not otherwise designated andprovided for by these bylaws. The Nominating Committee willseek the candidates approval for formal nomination and shallplace their names in nomination before the membership for elec-tion at the business session of the annual meeting TheNominating Committee will also provide slates for any awardsoffered by the Board of Directors.
Section 2: Membership Committee. The Board of Directorsshall constitute the Membership Committee. It shall be theSecretary/Treasurer's duty to review the qualifications andrecommendations of each applicant, for presentation and ap-proval by the majority of the Membership Committee.
Section 3: Program Committee. The Program Committee shallbe composed of a Chair, elected by the membership for a threeyear term, two members appointed by the President to staggeredthree year terms, and two members appointed by the commit-tee Chair to staggered three year terms. The Research Com-mittee chair and the Education Committee chair will be membersof the Program Committee. None of the appointed membersof the committee can be members of the Board of Directors.The duties of the committee shall be to arrange, in conformitywith instructions from the Board of Directors, the program forall meetings and select the formal participants.
Section 4: Constitution and Bylaws Committee. The Constitu-tion and Bylaws Committee shall consist of a Chair and twoother members, elected for staggered three year terms so thatthe member with the least remaining tenure shall serve as Chairduring their final year on the Committee. This Committee shallstudy the potential merits, adverse consequences and legal im-plications of all proposed constitutional amendments or changesin the bylaws and report their findings and recommendationsto the President and Board of Directors prior to the time of for-mal consideration of the proposed changes by the membership.The members of the Committee may themselves suggest ap-propriate constitutional amendments and bylaws changes to thePresident and Board of Directors upon study of problems aris-ing out of the existing constitution and bylaws.
Section 5: Education Committee. The Education Committeeshall consist of a chair, elected to a three year term by themembership, and six other members appointed by the commit-tee Chair for staggered two year terms. The committee Chairand appointees may be members of the Board of Directors orother Association committees. The Chair shall create ad hoceducation subcommittees with the approval of the Board of
Directors. The Committee shall foster education in emergencymedical care and assume duties and tasks as determined bv theBoard of Directors.
Section 6: Research Committee. The Research Committeeshall consist of a Chair, elected to a three year term by themembership, and six other members appointed by the commit-tee Chair for staggered two year terms. The committee Chairand appointees may be members of the Board of Directors orother Association committees. The chair shall create ad hocresearch subcommittees with the approval of the Board of Direc-tors. The Committee shall foster research in emergency medicalcdre and assume duties and tasks as determined by the Boardof Directors.
Section 7: Liaison Committee to the Association of AmericanMedical Colleges (AAMC). The Committee shall consist of aChair, appointed to a five year term by the Board of Directors,and three members appointed by the committee Chair for stag-gered three year terms. The official emergency medicinedelegates to the AAMC will be members of this committee. Thecommittee Chair and appointees may be members of the Boardof Directors or other committees of the Association. Only cur-rent or past members of the committee will be nominated bythe Nominating Committee for election to Chair. The Committeeshall develop programs fbr the Association to be presented atthe annual meeting of the AAMC and assume other duties andtasks of similar purpose as determined by the Board of Directors.
Section 8: Gctvernmental Affairs Committee. The Committeeshall consist of a Chair, elected to a three year term by themembership, and three members appointed by the committeeChair for staggered three year terms. The committee Chair andappointees may be members of the Board of Directors or othercommittees of the Association. Only current or past membersof the committee wil l be nominated by the Nominating Com-mittee for election to Chair. The Committee shall assume dutiesand tasks as determined by the Board of Directors to foster fed-eral and state support of research and education in emergencymedical care.
Section 9: Committee on International Afrttirs. The Commit-tee shall consist ofa Chair, elected to a three year term by themembership, and three members appointed by the committeeChair for staggered three year terms. The committee Chair andappointees may be members of the Board of Directors or othercommittees of the Association. The committee shall assumeduties and tasks as determined by the Board of Directors to fosterinternational recognition ofeducation and research ln emergencymedical care.
ARTICLE VII - DISSOLUTIONOF THE ASSOCIATION
Section /: Dissolution of this Association can only be initiatedby a majority vote of all members of the Board of Directorsand must be approved by two-thirds of the active membershippresent and voting at any annual or special meeting.
Section 2: Dissolution shall be achieved in compliance withArticle IX of the constitution.
8 1
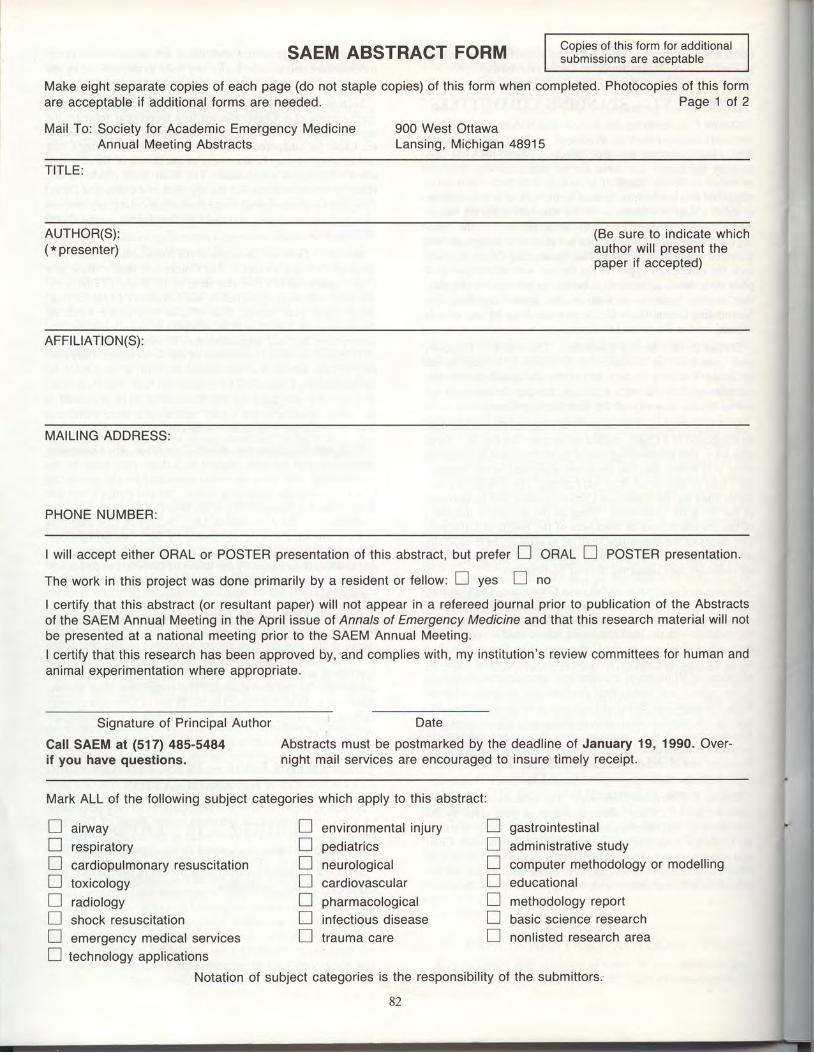
Copies of this form for additionalsubmissions are aceptable
Make eight separate copies of each page (do not staple copies) of this form when completed. Photocopies of this formare acceptable if additional forms are needed.
Mail To: Society for Academic Emergency Medicine 900 West Ottawa
Page 1 of 2
Annual Meeting Abstracts Lansing, Michigan 4891 5
SAEM ABSTRACT FORM
TITLE:
AUTHOR(S):( * presenter)
(Be sure to indicate whichauthor will present thepaper if accepted)
AFFTLTATTON(S):
MAILING ADDRESS:
PHONE NUMBER:
I will accept either ORAL or POSTER presentation of this abstract, but prefer I Onnl I pOSfen presentation.
The work in this project was done primarily by a resident or fellow: I yes E no
I certify that this abstract (or resultant paper) will not appear in a refereed journal prior to publication of the Abstractsof the SAEM Annual Meeting in the April issue of Annals of Emergency Medicine and that this research material will notbe presented at a national meeting prior to the SAEM Annual Meeting.
I certify that this research has been approved by, and complies with, my institution's review committees for human andanimal experimentation where appropriate.
Signature of Principal Author
Call SAEM at (517) 485-5484if you have questions.
Date
Abstracts must be postmarked by the deadline of January 19, 1990. Over-night mail services are encouraged to insure timely receipt.
Mark ALL of the following subject categories which apply to this abstract:
L_l arrwayn respiratoryLJ cardiopulmonary resuscitationLJ toxicologyL--J radiologyn shock resuscitationLJ emergency medical servicesI technology applications
n environmental in juryL-l pediatricsL--l neurologicalLJ cardiovascularLl pnarmacologrcalI in,fectious diseasetr trauma care
Ll gastrointestinal
L-l administrative studyI computer methodology or modellingLJ educationalI methodology reportI basic science researchtr nonlisted research area
Notation of subject categories is the responsibility of the subrnittors.
82

SAEM ABSTRACT FORMMake eight separate copies of each page (do not staple copies) of this form when completed.
:..Mail To: Society for Academic Emergency Medicine' Annual Meeting Abstracts
Copies of this form for additionalsubmissions are acceptable
Page 2 ot 2
900 West OttawaLansing, Michigan 48915
TITLE:
BODY OF ABSTRACT: (The abstract must be typed double-spaced and include no more than 3OO words. lt must belimited to the space on this page and be of a type size no smaller than used on this form. Donot include references, illustrations, or funding sources. Tables, when appropriate, are accept-able.) Do not list authors or institutions on this page.
Abstracts that do not conform to the instructions will be returned to the author without review. lt wil be the author's respon-sibility to re-submit the abstract by the postmark deadline of January 19, 1990. There will be no extension of the deadlinefor re-submissions.
83
SAEM MEMBERSHIP APPLICATION
Please complete and send, with the appropriate dues and initiation payment, to:
Society for Academic Emergency Medicine . 900 West Ottawa . Lansing, Michigan 48915 o (517) 485-5484(517) 48s-0801 FAX
Name
Home
Tit le: DO MD PhD Other
Address
Business Address
Preferred Mailing Address (please circle): Home Business
Home ( )
Birthdate
Business: ( )
Sex: M
Telephone:
lnstitution
Faculty Appointment
Positions currently held in Emergency Medicine:
1 .
2 .
3 .
Department Chairman
Check the appropriatemembership category: _Active -Associate -Resident/Fellow -lnternational Active -lnternational Associate
Active membership is open to (a) individuals with an advanced degree who hold a medical school or university faculty appointment and who actively
participate in acute, emergency, or critical care in an administrative, teaching or research capacity; (b) individuals with similar degrees in active military
,"i"i.J "it.l ihdividuals iho otherwise meet qualifications but who do not hold a taculty appointment and who petition the Membership committee'
Annual dues are g195 ptus a $15 init iat ion fee payable when the application is submitted. The application must be accompanied by a curr iculum vitae
and a letter verifying tfie faculty appointment. Membership benefits include a subscription to Annals of Emergency Medicine, the off icial SAEM iournal;
a subscription to the SAEM newsletter; free SAEM Annuai Meeting registration and banquet ticket; and reduced registration tees to other SAEM educa-
tional meetings.
Associate membership is open to health professionals, educators, government officials, members of lay or civic groups, or members of the public
at large who have an interesi in Emergency Medicine. Annual dues are $175 plus a $15 initiation fee payable when the application is submitted' The
application must be accompanied by a curriculum vitae. Membership benefits include a subscription to Annals of Emergency Medicine, the official SAEM
journal; a subscription to the SAEM newsletter; a free SAEM Annual Meeting registration and banquet ticket; and reduced registration fees to other
SAEM educational meetings.
Resident/Fellow membership is open to all residents or fellows interested in Emergency Medicine. Annual dues are $50 plus a $15 initiation fee payable
when the application is submitted. The application must be accompanied by a letter from the director verifying that the applicant is a resident or fellow
and the anticipated graduation date. Membership benefits include a subscription to Annals of Emergency Medicine,lhe otticial SAEM journal; a subscription
to the SAEM newsletter; a free SAEM Annual Meeting registration; and reduced registration fees to other SAEM educational meetings.
lnternational active and international associate membership is open to individuals who meet the criteria for SAEM active or associate membership
but do not reside in the united States. Annual dues are $95 plus a 915 (u.S. funds) ini t iat ion fee, payable when the application is submitted. The ap-
plication must be accompanied by a curriculum vitae and a letter veritying the faculty appointment, if appropriate. Membership benefits include a subscription
to Annals of Emergency MedicrL, tne official SAEM journal; a subscription to the SAEM newsletter; a free SAEM Annual Meeting registration and ban-
quet ticket; and reduced registration fees to other sAEM educational meetings.
My signature certifies that the information contained in this application is correct and is an indication of my desire to become
a SAEM member.
Signature of apPlicant Date
Apri l 1989
84
This form can be photocopied if additional copies are needed.

Society for Academic Emergency Medicirre900 West Ottawa
Lansing, Michigan 48915(s17) 48s-s484
FAX number: (517) 485-0801