santa clara county nov...santa clara county tis 101 trainers cross systems collaboration •maretta...
TRANSCRIPT

SANTA CLARA COUNTY
Imagine Trauma Free Communities... Bay Area communities working together to change the way we understand, respond to, and heal trauma

T²: TRAUMA TRANSFORMED SYSTEM OF CARE
2
Santa Clara San FranciscoSanta Cruz Contra CostaAlameda San MateoMarin
“Nobody can go back and start a new beginning, but anyone can
start today and make a new ending.”
– Maria Robinson

In July 2013 Regional Directors of County Behavioral Health
systems began planning to launch a Regional Trauma Informed
System of Care initiative designed to:
• Develop a regional understanding and shared approach to our
response to trauma and its effects,
• Embed leaders including youth and parent peers to be
champions of change within and across our systems serving
children and youth,
• Support and maintain change efforts through deploying experts
and consumer voices within our region.
• Address common and pervasive patterns of disproportionality
with respect to historical trauma and fragmented service delivery
systems.
HISTORY WALK
3

TRAUMA INFORMED SYSTEMS (TIS): ORIGINS
4
SAMHSA
SFPHD
TIS
7 Bay Area Counties Behavioral Health Directors
T² Regional Center
Local County TIS

TRANSFORMING STRESS AND
TRAUMA:FOSTERING WELLNESS AND RESILIENCE
Trauma-Informed Systems Initiative
Healing Organizations: Trauma Transformed

OVERARCHING GOALS
6
Transform the regional, overlapping systems into a coordinated, trauma-informed, youth-guided and family driven, evidence-based system of care. With the SAMHSA grant:
T2 Regional Center: Develop a regional center to support and sustain a system of care that is trauma-informed, youth-guided, family-driven, and culturally competent.Training: Develop training resources for dissemination to county staff, providers, and consumers.Coordination of Care: Establish a regional model to provide coordinated services for youth and children placed out of county, and children, youth, and families served by multiple systems within counties.Policy and Practice Sustainability: Develop and sustain promising practices from the project and incorporate them throughout the region.

Children ages Birth to 5
Juvenile Justice
Dually Involved Youth
Foster Care
LGBTQ
TAY
Victims of Violence
TARGET POPULATIONS
7

TRAUMA AND STRESS ARE A PUBLIC HEALTH CONCERN
8
• Stress and Trauma linked to 6 leading causes of death• Heart disease, cirrhosis of the liver, accidents ,
COPD, cancer, suicide• Trauma impacts more than just the individual
• Ripple effect• Some communities disproportionally affected
• Racism + Urban Poverty + Trauma = Toxic• Intergenerational transmission of trauma• Systemic preventative approach is needed

CASUALTIES OF CHILDHOOD
CHRONIC AND TOXIC STRESS
9
Statistically, the home is one of the most violent places in America.
All children are shaped by their early life experiences.
In the absence of repetitive, patterned, and enriching experiences, they may develop in disorganized or even dysfunctional ways.
Their emotional, behavior, cognitive, social, and physical development can become arrested and delayed.
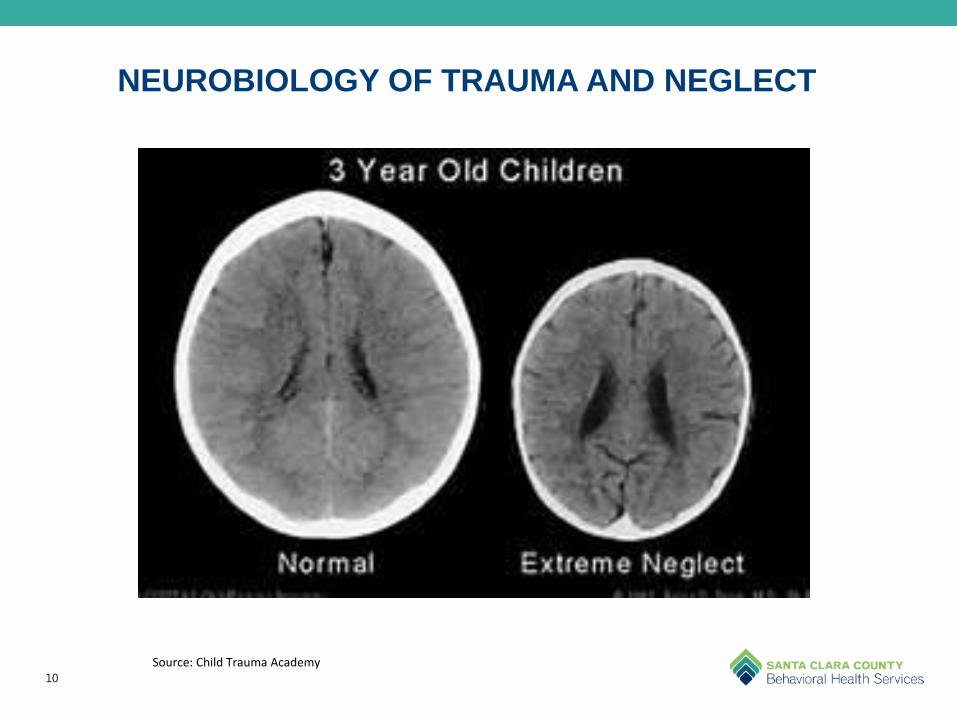
NEUROBIOLOGY OF TRAUMA AND NEGLECT
10
Source: Child Trauma Academy

A PUBLIC HEALTH CRISIS
ADVERSE CHILDHOOD EXPERIENCES-ACES
11
ACEs affect people from all backgrounds, regardless of race, income, education, or geography.
Occurring in childhood, exposure to chronic adversity during the most formative years has the potential to reap long term and far reaching consequences of ACEs on adults.
ACEs are traumatic experiences that have a profound impact on the child’s developing brain and physiology with lasting impact on their health and well being as an adult.
Sources: Center for Disease Control; Center for Youth Wellness

THREE TYPES OF ACES
12
Abuse
Physical
Emotional
Sexual
Neglect
Physical
Emotional
Household Dysfunction
Mental illness
Divorce
Domestic Violence
Incarcerated relative
Substance Abuse
Adverse Childhood Experiences-ACEs

KEY FINDINGS
13 Sources: Center for Disease Control
1. 1 of 3 reported no ACEs.2. 87% likelihood that at least 1 additional category was present.3. 21% were sexually abused.4. 19% had a parent with mental illness5. 28% were physically abused.6. 27% had a member in the household who was an alcoholic or substance abuser.7. 23% were not raised by both biological parents.8. Women were 50% more likely to have experienced 5 or more ACES9. Significant health outcomes:
a. Those with an ACEs score of 4 were 2x more likely to develop heartcondition or cancer.
b. Those with 5 or more ACEs were 8x more likely to become alcoholic.c. Those with 6 or more ACEs are at risk of their lifespan being shortened
by 20 years. d. ACEs will still have a profound effect 50 years later.

ACES IN CALIFORNIA
14 Sources: Center for Disease Control; Center for Youth Wellness

ACES IN CALIFORNIA
15 Sources: Center for Disease Control; Center for Youth Wellness

COUNTIES WITH THE
HIGHEST NUMBER OF ACES
BUTTE: 76.5% OF RESIDENTS
HAVE 1 OR MORE ACES
MENDOCINO & HUMBOLDT:
75.1% OF RESIDENTS HAVE 1 OR
MORE ACES
16
COUNTIES WITH THE LOWEST
NUMBER OF ACES
SANTA CLARA: 53.4% OF
RESIDENTS HAVE 1 OR MORE
ACES
SAN MATEO:
53.9% OF RESIDENTS HAVE 1 OR
MORE ACES
• A tool to recognize and understand ACEs as a hidden
epidemic and public health issue
• Opportunity for healing.
• Build hope
• Promote wellness and recovery
ACES ARE NOT A DESTINY
17

TRAUMA INFORMED CHILD SERVICE SYSTEMS
Child
Primary Care/
VMC
BHSD
Child Welfare
Juvenile Justice
Criminal
Justice
Education
Public Health
Faith Based Community
FIRST 5
Consumer/
Youth Voice

DEVELOPING TRAUMA INFORMED PRACTICES
• Trauma-informed care approach, which involves looking at all practices through a trauma lens
• Trauma-informed practices are not interventions but are approaches that are infused through all levels of the organization.
• Trauma-informed practices include, among others, creating a safe, supportive, welcoming, and respectful environment; educating and training all staff including administrators, direct care staff, case managers, and support staff about the impact of trauma; implementingscreening and assessment tools and procedures to identify clients who have experienced trauma and determine the impact of that trauma; and training clinical staff in trauma-specific treatments.
• It is essential that providers are aware of their own cultural attitudes and beliefs, as well as those of their clients, and provide culturally relevant approaches

Trauma-informed practice is more about the overall essence of
the approach, or way of being in the relationship, than a
specific treatment strategy or method.
Trauma Informed
THE 4 R’S OF A TRAUMA-INFORMED SYSTEM
SAMSHA defines “a program, organization, or system that is trauma-informed as one that:
• Realizes the widespread impact of trauma and understands potential paths for recovery;
• Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system;
• Responds by fully integrating knowledge about trauma into policies, procedures, and practices; and
• Seeks to actively resist re-traumatization.”
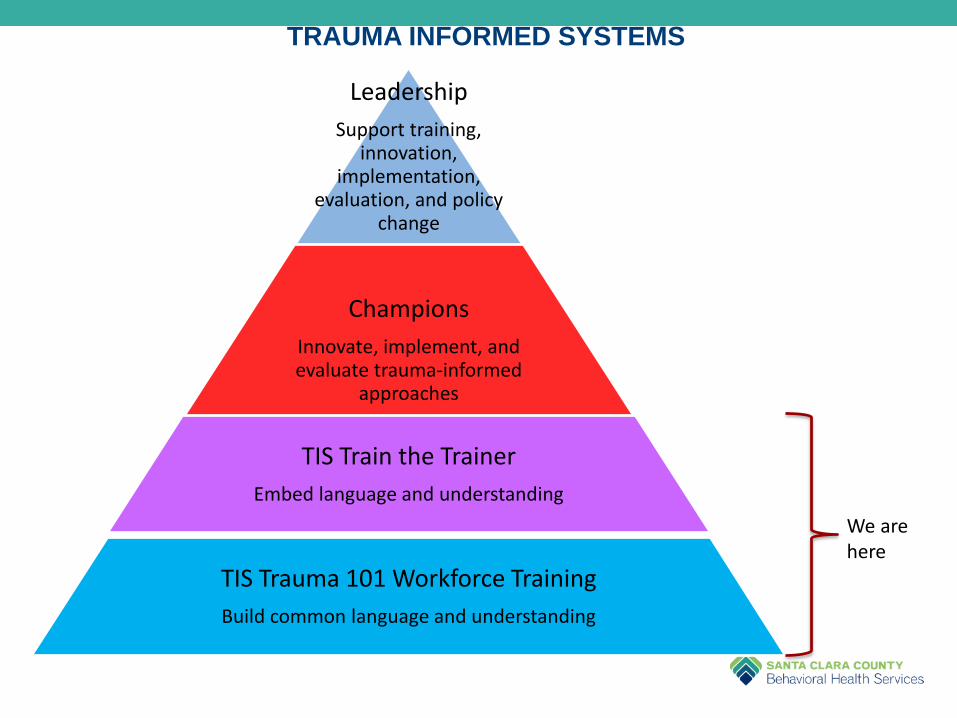
TRAUMA INFORMED SYSTEMS
Leadership
Support training, innovation,
implementation, evaluation, and policy
change
Champions
Innovate, implement, and evaluate trauma-informed
approaches
TIS Train the Trainer
Embed language and understanding
TIS Trauma 101 Workforce Training
Build common language and understanding
We are here

CHAMPIONS OF CHANGE
• Providing leadership
• Building awareness
• Trauma informed organizational self assessment
• Trauma informed training
• Clarity that this process is not just about increasing individual trauma knowledge but about setting the stage for organization-wide change.
• Knowing what it means to be trauma-informed and what it will take to begin the transformation
“We must become the change we want to see.”
– Mahatma Gandhi

Adapted from UCSF Healthy Environments and Response to Trauma in Schools (HEARTS) Curriculum by
Joyce Dorado, Ph.D.
Director, UCSF HEARTSChild and Adolescent Services
UCSF-San Francisco General Hospital
Lynn Dolce, MFT
Director, Foster Care Mental HealthChildren Youth and Families System of Care
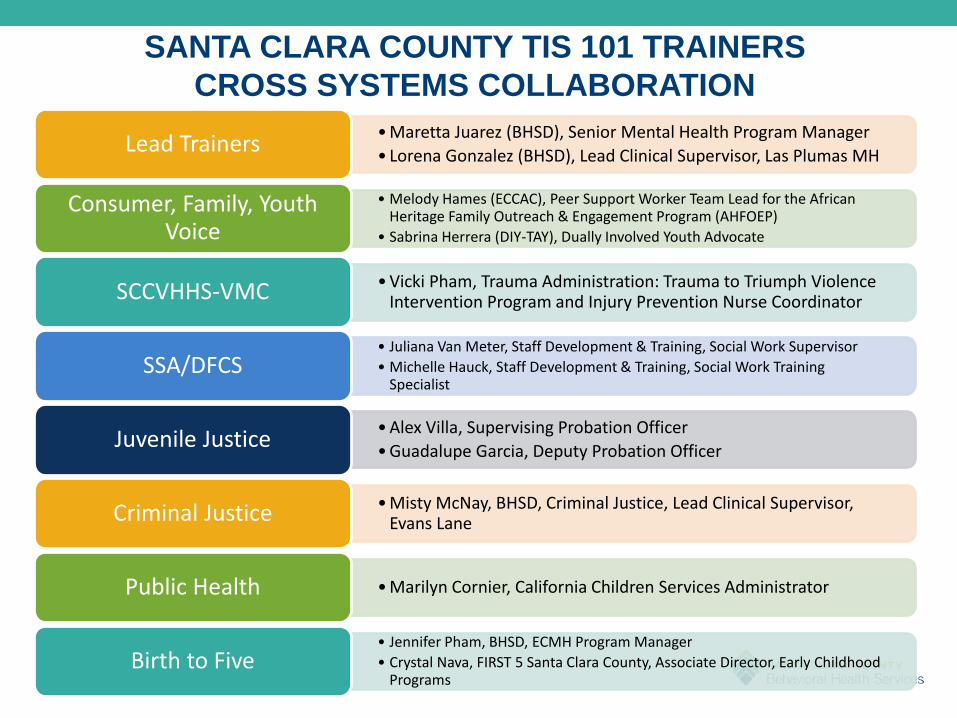
SANTA CLARA COUNTY TIS 101 TRAINERS
CROSS SYSTEMS COLLABORATION
• Maretta Juarez (BHSD), Senior Mental Health Program Manager
• Lorena Gonzalez (BHSD), Lead Clinical Supervisor, Las Plumas MHLead Trainers
• Melody Hames (ECCAC), Peer Support Worker Team Lead for the African Heritage Family Outreach & Engagement Program (AHFOEP)
• Sabrina Herrera (DIY-TAY), Dually Involved Youth Advocate
Consumer, Family, Youth Voice
• Vicki Pham, Trauma Administration: Trauma to Triumph Violence Intervention Program and Injury Prevention Nurse CoordinatorSCCVHHS-VMC
• Juliana Van Meter, Staff Development & Training, Social Work Supervisor
• Michelle Hauck, Staff Development & Training, Social Work Training Specialist
SSA/DFCS
• Alex Villa, Supervising Probation Officer
• Guadalupe Garcia, Deputy Probation OfficerJuvenile Justice
• Misty McNay, BHSD, Criminal Justice, Lead Clinical Supervisor, Evans LaneCriminal Justice
• Marilyn Cornier, California Children Services AdministratorPublic Health
• Jennifer Pham, BHSD, ECMH Program Manager
• Crystal Nava, FIRST 5 Santa Clara County, Associate Director, Early Childhood Programs
Birth to Five

BHSD T² WORKGROUPS
• Amanda Vierra, Standards of Practice Coordinator
• Lorena Gonzalez, Lead Clinical Supervisor, Las Plumas Mental HealthWorkforce Development/Training
• Renee Marquett, BHSD Contracts Manager
• Carol Guerrero-Urbanski, Clinical Lead Supervisor, Juvenile HallNeeds Assessment/Focus Groups
• Melody Hames, Ethnic & Cultural Communities Advisory Committee
• Sabrina Herrera, Dually Involved Youth Program, AdvocateConsumer/Youth Stakeholder
Voice/T2 Advisory Council
• Jennifer Pham, Early Childhood Mental Health Program Manager
• Lily Vu, Lead, School Linked ServicesService Delivery and Care
Coordination
• Carolina Cervantes, Lead Clinical Supervisor, RAIC
• Veronica Robles, TAY System of Care Manager
• Karin Kalk (consultant) to BHSDMeasurement System
• Rhoda Blankenship, Public Health Department
• Wendy Kinnear, Department of Family and Children Services
• April Kihara, PEI/SLS/SOS Program ManagerACESConnection
• April Kihara, PEI/SLS/SOS Program ManagerTrauma Services Inventory
(Time limited group)
• Yuki Ascue, Lead Clinical Supervisor, Sunnyvale Mental Health
• Betsy Ramirez, Licensed Clinical Social Worker, BHSD AdminCommunication
•TIS 101 Community of Learning Collaborative training
calendar
•Standardized Readiness Assessment
•Continued spread of Reflective Practice
•T² Trauma Transformed Advisory Council of Santa Clara
County
•Continue cross systems collaboration for collective impact
•Paper Tigers screening
NEXT STEPS
27

• BHSD Website
– https://www.sccgov.org/sites/mhd/Providers/Pages/Trauma-Transformed.aspx

Santa Clara County T2 Operations
Maretta Juarez, LCSW
Senior Mental Health Program Manager
Behavioral Health Services Department
408-794-0768