scaling up art in sénégal: specifics needs for strategic information
DESCRIPTION
Scaling up ART in Sénégal: specifics needs for strategic information. Mame Awa Toure MD, MSc AIDS/STI Division, MOH Senegal. Introduction. Senegal: a west African country Area: 196.722 km² Population estimated to 10 millions 11 regions and 30 departments/ provinces. - PowerPoint PPT PresentationTRANSCRIPT

Scaling up ART in Sénégal: specifics needs for
strategic information
Mame Awa Toure MD, MScAIDS/STI Division, MOH Senegal

Introduction
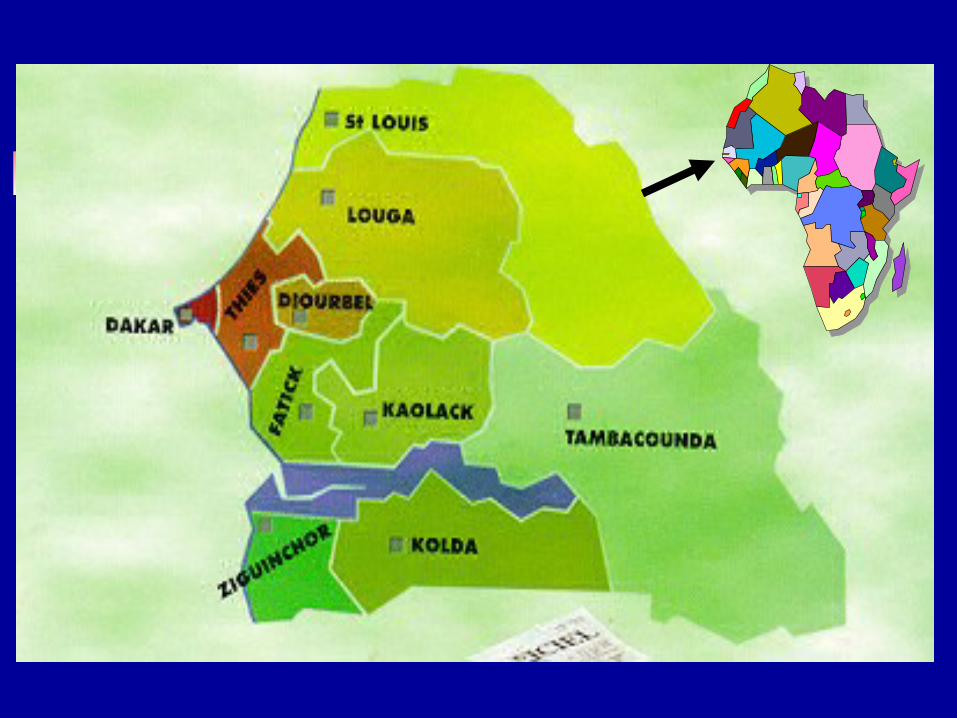
Senegal: a west African country Area: 196.722 km² Population estimated to 10 millions 11 regions and 30 departments/ provinces. Resources constrained settings: GDP of 500$
US. Concentrated HIV epidemic
Low HIV prevalence in general population less than 2%
5-20% in high risk group
The Senegalese Initiative for Access to ARVs : ISAARV
A Governmental initiative late 1997 Political commitment : increasing annual subsidy Collaboration of ANRS: technical support, project
design First step : Pilot study
Building up a model according limited resources Evaluation before extension (collaboration with ANRS)
Second step : scale up for nationwide access

2000- 2006Accelerating phase of ISAARV
Political comittement Government subsidy increased Subsidy included to the national budget line Credit IDA : MAP
Expanding Fund and Partnership for ARV program government, WB, GF, USAID/FHI, UE, GTZ, UN agencies…
Decrease of the of financial participation Increasing demand

Increasing government budget
250 millions
1475 millions
0
1000
2000
3000
4000
5000
1998 1999 2000 2001 2002 2003
BudgetTotal
Financial participation
Government subsidy con’t October 2000: ACCESS Program Levels of financial participation
SES assessed by a social workers team A package including drugs, CD4 count and viral load
Low income: $30- $7 per month Government officers $60- $15
About 80% of patients treated free of charge

ISAARV managerial structures
Health facilities level: hospital/treatment centers Medical committees
Enrollment and medical follow up PEP documentation and management
Psycho-social support committees Adherence support, accompaniment counseling… PLWHA clubs
Coordination level: HIV/AIDS Division, MOH Drugs and reagents management committee PMTCT management committee VCT piloting committee
Services delivery package
District level : operational level Counseling, certain OI management, * PMTCT services, Referral functional system, Monitoring ARV (next step)
Hospital level : district + ARV ARV entry point
Rapid functionality of structures
Needs, coverage ISAARV components
prior Conditions: HIV testing available/ VCT ARV Treatment Centers Counseling, treatment of OI, use of Cotrimo… Laboratories capacity : CD4, routine exams Training of health personals ARV monitoring committees
Needs, coverage (2)
Monitoring ART Adults, Children,
PMTCT Post Exposure Prophylaxis Psycho-social and adherence support Supportive research:
Monitoring drugs resistance Promoting clinical trials

Chain of distribution
National procurement pharmacy
Treatment centers Regional procurement pharmacy
Fann Pharmacy Regional hospital/ Districts
HPD, IHS
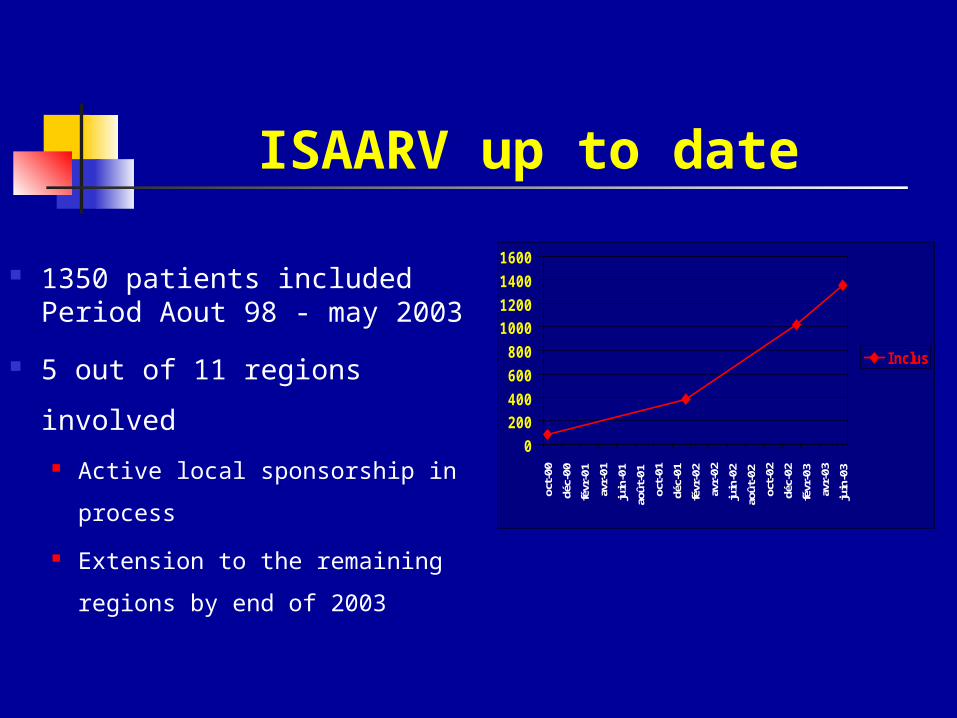
ISAARV up to date
1350 patients included Period Aout 98 - may 2003
5 out of 11 regions involved Active local sponsorship in
process Extension to the remaining
regions by end of 2003
0200400600800
1000120014001600
oct-00
déc-
00fé
vr-0
1av
r-01
juin
-01
août
-01
oct-01
déc-
01fé
vr-0
2av
r-02
juin
-02
août
-02
oct-02
déc-
02fé
vr-0
3av
r-03
juin
-03
Inclus
How does the data collection work?
Patient monitoring Detailed patient data base for the first
100 naives patients enrolled to the pilot phase,
Database on 80 patients enrolled in the two clinical trials ANRS1204/ ANRS1206
Few initiatives on the remaining Data not being collected regularly
Lack of systematized data collection
Strategic objectives Nationwide access to ARV drugs planned
Strenghten capacities in the 11 regions Increasing number of PLWHA treated
7000 patients by 2006 M&E system urgently needed!!!
Weak part of the program to be improved
M&E approach M&E system already in place
For other priority diseases except HIV/AIDS new strategies (PMTCT,
ART..)
Building up process for HIV/AIDS: Capacity building**
M&E Unit: NACA, MOH, and other ministries Strengthening technical resources: training
M&E approach (2)
M&E plan developed Workshop in June 2003: set of indicators
for each components ** (UNGASS/MAP) M&E tools and Operational guidelines to
be developed training Data collection plan

M&E approach (5)
O the r Public S e c torE duca tion
YouthW om en a nd s oc ia l deve lopm e nt, W ork a nd E m ploym e nt
HIV E p ide m io logic a l S urve i l la nc eM O H
C ivi l soc ie ty orga niza tions , pr iva te s e ctorC BO, NG O s , F BO s
NA C AM & E Unit

M&E approach(4)next steps by end of 2003
Workshop series Update and reinforce competencies in M&E within
targeted sectors (health, education, youth…) Priority for the Health sector TOT, training series
M&E tools development Data collection plan Data collection forms Defining evaluation system and calendar
M&E sub- units to be set up at the regional level,
Contracting services ???

Specifics needs
Lack of technical resources : Urgent need to
Strenghten HR capacities in M&E Recruit human resources for M&E units at each
level More use of available data
Systematisation of information, Regular data collection
For patient monitoring and program monitoring

Specifics needs
ARV delivery system to be improved Logistical issues
Better planning of Evaluations for all ISAARV components Evaluation of the pilot phase (ANRS 02) More in-dept Cost-effectiveness analysis
External expertise needed