scapula history - amazon web services · cole pa, schroder lk, jacobson ar. scapula and rib...
TRANSCRIPT

8/18/2015
1
Advancements
in the
Treatment of
Scapula
Fractures
Peter A. Cole, MDDepartment of Orthopaedic Surgery, University of Minnesota, Regions Hospital, St. Paul, MN
www.ScapulaInstitute.org
@PeterAColeMD
Disclosures
•Bone Foams Inc, LLC: Stock/Stock Options
•Stryker: Research support
•Synthes: Research support
Scapula History

8/18/2015
2
One Surgeon’s Journey
•Scapula fractures treated differently
•Nonoperative management the norm for all fxs
•New frontier?
Length, Alignment, Rotation
Anatomic Articular Reduction
Restore Stability
Respect Soft Tissue
Principles of Fracture
Management
AO principles of fracture management
Deformity=Dysfunction
Unless it’s a
scapula?

8/18/2015
3
Deformity
Angulation Intraarticular
SSSC
Medialization
Glenopolar angle
Studying Deformity

8/18/2015
4
Outline• Classification, Diagnosis, Radiographic
Measurements & Indications
• Diagnostic Interpretations, Perioperative Considerations & Associated Injuries
• Surgical Approaches, Reduction Techniques, implants
• Cases

8/17/2015
1
Scapula Fractures:
DiagnosisRadiographic Measurement
ClassificationIndications
Babar Shafiq, MD, MSPTAssistant Professor
Trauma Division
Department of Orthopaedic Surgery
Johns Hopkins School of Medicine
Disclosures
I have no disclosures
related to this talk
Diagnosis: History & Physical
• Blunt injury high-energy trauma
• 90% associated injuries
• Scapula fractures often overlooked– Life-threatening injuries treated first
– Detection and management often delayed

8/17/2015
2
Diagnosis: Clinical Deformities
Diagnosis: Clinical
Deformities
Diagnosis: Skin
Delay surgery until re-epithelialization 10-14 days

8/17/2015
3
Diagnosis: Associated Injuries
• Chest Wall
• Head Injury
• Cervical & Thoracic Spine Fractures
• Neurovascular
Document Neurovascular Exam
Chest, C-Spine XR or CT
Imaging
• Radiographs– Trauma Series
– True AP (Grashey)
– Axillary
– Scapular “Y”
• CT– Fine Cuts (≤2mm)
– 3D Reconstructions
Measurement Terms
Medialization(Lateral Border Off-set)
Glenopolar Angle(GPA)
Angulation
J Am Acad Orthop Surg 2012;20: 130-141

8/17/2015
4
Step-off
22mm
18mm
28mm
25mm
4mm
GPA (Glenopolar Angle)
36°
Angulation
42°

8/17/2015
5
Medialization/Lateral Border Offset
28mm
How do we interpret the injury?
Classification: Brief History
1579 – 1900s French
1723 Petit
1913 Lambotte
1984 Hardegger
1991 Ada & Miller
1998 Ideberg (Mod. Mayo)
Pare, Petit, Desault, DuVerney, Lenormant,
Dujarier, Malgaigne, Basset, Dupont, Judet,
and EvrardBodyNeck
ProcessInternal Fixation
Indications Criteria:Angulation >40 degMedialization >1cm

8/17/2015
6
90 3D-CT Scans
Scapula Maps – Inferior Glenoid Neck (n=61)
Classification: History

8/17/2015
7
Kavanagh BF, et
al.
(1993)
>2mm
Mayo KA, et al.
(1998)>5mm
Herrera DA, et al
(2009)> 4mm
Jones CB, et al
(2009)>3mm
Jones CB, et al
(2011)>3mm
Anavian J, et al
(2012)> 4mm
Articular Step-OffCurrent Expert Surgical Indications
> 4mm
Ada JR and Miller
ME
(1991)
> 10 mm
Herrera DA, et al
(2009)> 15 mm
Jones CB, et al
(2009)> 20 mm
Jones CB, et al
(2011)> 20 mm
Gauger EM, et al
(2012)> 20 mm
Cole PA, et al.
(2012)> 20 mm
MedializationCurrent Expert Surgical Indications
> 20mm
Ada JR and
Miller ME
(1991)
> 40
Jones CB, et
al
(2009)
> 45
Jones CB, et
al
(2011)
> 45
Bartoníček J
and Fric V
(2011) > 30
Cole PA, et
al.
(2012)
> 45
Gauger EM,
et al
(2012)
> 45
> 45°
AngulationCurrent Expert Surgical Indications

8/17/2015
8
GPA
Cole PA, et al.
(2012)< 22
Gauger EM, et
al.(2012)< 22
Glenopolar Angle (GPA)Current Expert Surgical Indications
< 22°
Poor Outcomes GPA < 20°
Bestard et al Contemp Ortho 12:47, 1986
Bozkurt et al. Injury, 36, 2005
Romero, Arch Ortho Trauma, 121, 2001
Pace et al. J Shoulder & Elbow, Nov/Dec, 2005
Multiple DisruptionsCurrent Expert Surgical Indications
34mm
35mm
16mmClavicle > 10mm
Scapula > 10mm
M/L > 15mm
Angular > 30°41
°
AO/OTA – 1996 (r2007)

8/17/2015
9
Glenoid Involved
73% agreementKappa 0.79
Body Fractures
82% agreementKappa 0.75

8/17/2015
10
Summary:Classification
Indications
• Multiple classification schemes– Historical– Body, glenoid & processes
• AO/OTA– In development, comprehensive– Does not help guide treatment (Yet)
• Surgical Indications– Medialization (Lateral Border Off-set) > 20mm
– Glenopolar Angle (GPA) < 22°
– Angulation > 45°
– Step-off > 4mm
GPA
Medialization
Angulation
Step

8/17/2015
1
Steven Gammon, MDOrthopaedic Trauma Surgeon
Rocky Mountain Orthopaedic Associates, Inc.
St. Mary’s Hospital Regional Medical Center
Grand Junction, Colorado
August 18, 2015
Disclosures
• I do not have any monetary or nonmonetary disclosures related to this talk.
Overview
• Significance of scapula fractures in the “Big Picture”
• Associated injuries:
– Global injuries
– Ipsilateral upper extremity injuries
• Examples

8/17/2015
2
Overall Significance
• Scapula fractures account for <1% of all fractures but are common – especially at tertiary trauma centers.
– 3-5% of shoulder girdle injuries
• The diagnosis is missed or delayed in 12.5% of multiply-injured patients
• Rarely “isolated injuries”
– >90% have associated injuries
– Always look for other injuries.
Associated Injuries
95% (n=168)
Only 4 pts with
isolated scapula fx
Ipsilateral
Shoulder
Injuries
57%Gauger, et al. “Surgical and Functional Outcomes after Operative Management of Extra-articular Glenoid Neck and Scapula Body Fractures” Presented at 2010 OTA Annual Mtg.
Associated Injuries (90-95%)
• Thoracic injuries – 80% (rib fx, pulm cont, PTX)
• Ipsilateral extremity injury – 50%
– “Superior Shoulder Suspensory Complex” (SSSC)
– Anywhere else in that ipsilateral extremity
• Head injuries – 48%
• Spine injuries – 26%
– Cervical spine or brachial plexus lesions – 15%

8/17/2015
3
Superior Shoulder Suspensory Complex (SSSC)
• A bone-soft-tissue ring that provides a stable connection of the glenoid and scapula to the axial skeleton.
– Position and orientation of glenoid in space determines shoulder function and range of motion.
Superior Shoulder Suspensory Complex (SSSC)
• Four bony landmarks:
– Clavicle
– Acromion
– Coracoid Process
– Glenoid
• Supporting ligamentous complexes
– AC joint
– CC ligament
Disruptions in SSSC
• Large disruptions in either clavicle or any components of SSSC can have major effects on normal shoulder mechanics
– Decreased ROM, pain, loss of function
• Multiple disruptions in SSSC = Floating Shoulder

8/17/2015
4
Disruptions in SSSC
• Classified as:
– Single
– Double
– Triple
– Quadruple
• Multiple disruptions lead to discontinuity or malposition of the glenohumeral joint relative to the scapula body.
Double SSSC Lesion
“The Floating
Shoulder”
Goss, JOT, 1993
Case Example 1Double Disruption – Scapula/Clavicle

8/17/2015
5
Case Example 1Double Disruption – Scapula/Clavicle
>100%Displacement
14° GPA
2.5 cm
Case Example 1Double Disruption – Scapula/Clavicle
Case Example 1Double Disruption – Scapula/Clavicle
40° GPA0mm Medialization

8/17/2015
6
Case Example 2Double Disruption – Scapula/Clavicle
*16 year old in MVA
Case Example 2Double Disruption – Scapula/Clavicle
Case Example 2Double Disruption – Scapula/Clavicle

8/17/2015
7
Case Example 3Triple Disruption – Scapula/Acromion/Coracoid
*45 year old in snowmobile
accident
Case Example 3Triple Disruption – Scapula/Acromion/Coracoid
Case Example 3Triple Disruption – Scapula/Acromion/Coracoid
*Stage One Surgery: Posterior

8/17/2015
8
Case Example 3Triple Disruption – Scapula/Acromion/Coracoid
*Stage Two Surgery: Anterior/Superior
Additional ExamplesScapula Fractures with Multiple Rib Fractures
Steven Gammon, MDOrthopaedic Trauma Surgeon
Rocky Mountain Orthopaedic Associates, Inc.
St. Mary’s Hospital Regional Medical Center
Grand Junction, Colorado
August 18, 2015

8/18/2015
1
Surgical Approaches, Reduction Techniques & Implants
Dr. Peter ColeChief of Orthopaedics: Regions Hospital
Professor, University of Minnesota
Surgical Approaches•Posterior: positioning =
lateral decubitus•Judet
•Extensile submuscular•Intermuscular window
•Straight Posterior•MIO
•Anterior: positioning = beach chair
•Deltopectoral: anterior/superior glenoid fractures
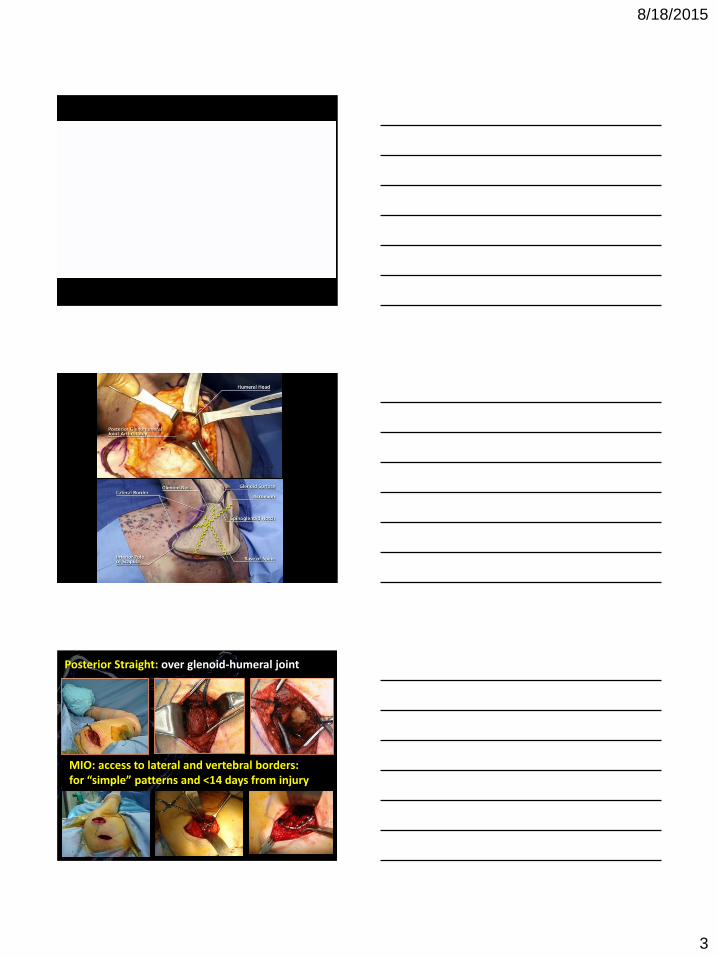
Vulnerable structures with posterior approach
Suprascapular Nerve
Ascending
Branch of
the Circumflex
Scapular Artery
Cole PA, Schroder LK, Jacobson AR. Scapula and Rib
Fractures. In: Browner B, Jupiter J, Krettek C, Anderson P,
eds. Skeletal Trauma. Fifth Edit. Philadelphia, PA:
Saunders/Elsevier; 2014.

8/18/2015
2
JudetExtensile: elevation of infraspinatus, teres minor, and
posterior deltoid
Muscular windows: infraspinatus and teres minor intervalAccess to lateral border and posterior glenoid
Judet Posterior
Approach
Deltoid
Infraspinatus
T
Minor
8/18/2015
3
Posterior Straight: over glenoid-humeral joint
MIO: access to lateral and vertebral borders: for “simple” patterns and <14 days from injury

8/18/2015
4
Reduction techniques
• Lateral border and glenoid neck = best bone stock
• Access to medial and lateral borders required
• Many deforming forces
Cole PA, Schroder LK, Jacobson AR. Scapula and Rib Fractures. In:
Browner B, Jupiter J, Krettek C, Anderson P, eds. Skeletal Trauma. Fifth
Edit. Philadelphia, PA: Saunders/Elsevier; 2014.
Tools to Aid Reduction
1. Schanz pins with T-handled chucks
2. Jungbluth clamp over screws
3. Lamina spreader between cephalad and caudad fragments
4. Shoulder Hook inside a pilot hole on the inferior lateral border an a Schanz pin in the glenoid neck
5. Once reduction attained – small pointed bone reduction forceps can maintain.
Cole PA, Schroder LK, Jacobson AR. Scapula and Rib Fractures. In: Browner B, Jupiter J, Krettek
C, Anderson P, eds. Skeletal Trauma. Fifth Edit. Philadelphia, PA: Saunders/Elsevier; 2014.

8/18/2015
5
Implants
• 2.7 mm low profile plates
–Straight 2.7 DC plate - lateral border
–Scapula spine and vertebral borders:
2.7 mm recon plates more easily
contoured.
–Superomedial angle contour requires
bending the implant in 3 planes!
Cole PA, Schroder LK, Jacobson AR. Scapula and Rib Fractures. In:
Browner B, Jupiter J, Krettek C, Anderson P, eds. Skeletal Trauma.
Fifth Edit. Philadelphia, PA: Saunders/Elsevier; 2014.

8/18/2015
6
Cole PA, Schroder LK, Jacobson AR. Scapula and Rib Fractures. In: Browner B, Jupiter J, Krettek C,
Anderson P, eds. Skeletal Trauma. Fifth Edit. Philadelphia, PA: Saunders/Elsevier; 2014.
Questions ?
Scapula
Approaches
Reduction
Techniques
Implants

8/18/2015
1
Ivan S. Tarkin, MDDivision Chief Traumatology
Department of Orthopaedic SurgeryUniversity of Pittsburgh Medical Center
21 y/o LHD M involved in altercation, hit with a pipe and ran over by a car.
Presents with bilateral scapular fractures, pneumothorax, rib fractures, grade 1 liver laceration,

8/18/2015
2
2.6cm
34 degrees

8/18/2015
3
Judet Incision

8/18/2015
4
54 y/o M laborer (road construction) s/p MCC presents with crush injury to right chest/ shoulder girdle
No relevant PMH

8/18/2015
5
Intra-op finding: suprascapular nerve entrapped in fracture site

8/18/2015
6
Back to work
Regained full ROM/Strength
Resolved weakness with external rotation (suprascapular nerve)
“Feels normal”
Intraop Photo courtesy of PA Cole

8/18/2015
7

8/18/2015
8
56 y/o M vending machine technician s/p occupational crush injury to left face, shoulder and chest.

8/18/2015
9
100% satisfied with his result
Has regained his motion and strength
Full passive and active ROM
Strength is 5/5 for abduction, forward flexion, external and internal rotation
47 y/o polytrauma pt (head, chest, abd, pelvis, extremity)
Ipsilateral scapula fx, elbow dislocation

8/18/2015
10
45 y/o M s/p MCC with multiple rib fracture, pneumothorax, scapula fracture, and liver laceration

8/18/2015
11

8/18/2015
12
36 y/o M transferred from OSH 3 days after MCC for definitive care
Injuries: right rib fractures (1-11), tension hemotopneumothorax s/p chest tube, right clavicle fracture, right scapular fracture

8/18/2015
13
28 y/o M involved in roll over MVC
Injuries to pancreas, splenic laceration s/p splenectomy, liver laceration, head blead, rib fracture, thoracic spine fracture, kidney infarct/hematoma, clavicle fracture, scapula fracture.

8/18/2015
14
53 y/o M un-helmeted MCC
Injuries: left hemopneumothorax, left 1st through 9th rib fractures, mediastinal hematoma, pilon ankle fracture, T3-8 spinousprocess fractures, T3 and T4 compression fractures, left scapula fracture

8/18/2015
15
Doing well. Only pain remaining from pilonankle fracture
Full, pain free ROM of the left shoulder
5/5 Strength in the entire left upper extremity

8/18/2015
16