scapular resting position - azata winter meeting/progressive... · •resting position •17 muscle...
TRANSCRIPT

Progressive Therapeutic Exercise Strategies for Shoulder Dyskinesis
Scapulothoracic Joint
• Resting position
• 17 muscle attachments
• Force couples of the shoulder
• Normal vs abnormal Scapulohumeral rhythm
Scapular Resting Position
Clinical Importance of Multiple Muscle Attachments
• 17 muscles
• Stabilize
• Move
Scapulohumeral Rhythm
• Setting Phase
• Preserves length-tension relationship of GH muscles
• Prevents impingement between humerus and acromion
Force Couples of Shoulder

Why is Scapular Function Important
• Scapular upward rotation and axial rotation was impaired in subjects with chronic impingement syndrome. Endo K, et al. J Orthop Sci 2001
• Serrated dysfunction evidenced by decreased upward rotation and increased anterior tipping and winging in patients with impingement syndrome. Ludwig et al. Phys Ther 2000
• Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: an evidence-based review Ellenbecker et al. Br J Sports Med 2010
What is Scapula Dyskinesis
• Altered scapulohumeral rhythm
• Decreased scapular upward rotation, posterior tilt, and lateral rotation
• Can cause shoulder impingement, instability, neck pain
Causes of Scapular Dysfunction
• Nerve impingement
• Lack of Soft tissue flexibility
• Abnormal scapular position
• Dysfunctional movement patterns
• Poor strength and motor control

Clinical Manifestation of Scapular Dyskinesis
• Kibler, et al 2002
• Type I - increased anterior tilting
• Prominent inferior angle
Clinical Manifestation of Scapular Dyskinesis
• Type II - Prominence of entire medial scapular border
• Common in patients with glenohumeral instability
Key Components of Therapeutic Interventions for Scapular Dyskinesis
• Alignment
• Soft tissue restrictions
• Altered Scapular movement patterns
• Strength and Motor Control
• Kinetic Chain
• Cools, et al 2013
Soft Tissue Restrictions
• Short pectoralis minor
• Posterior GH tightness
• Latissimus dorsi
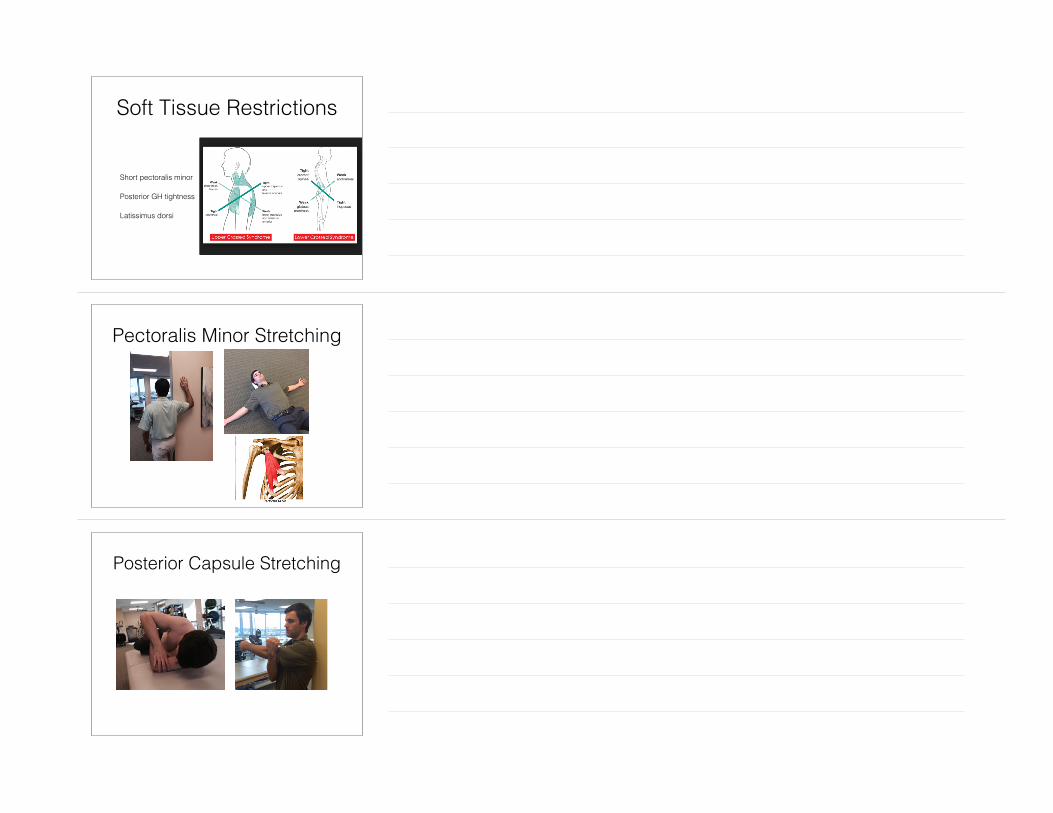
Pectoralis Minor Stretching
Posterior Capsule Stretching

Altered Muscle Performance
• Lack of co-contraction and force couple activity
• Strength deficits
Emphasize Dynamic and Neuromuscular Control
• Efficient dynamic stabilization and neuromuscular control of glenohumeral joint is necessary to avoid injury
• Scapular strength and stability are essential for proper function of the glenohumeral joint
• Rhythmic stabilization
• Reactive neuromuscular control drills
• Closed kinetic chain drills
• Plyometric exercises
• Reinold,et al 2010
Conscious Muscle Control• Improve proprioception and
normalize scapular resting position
• Mottram, et al 2009 found that it is possible to teach a normal subject to consistently reproduce movements of the scapula into a posterior tilt and upward rotation.
• Corrective exercises should be performed prior to dynamic movements

Dynamic Motor Control• Continue to challenge
dynamic stabilization/neuromuscular control
• Open vs closed chain activities
• Hardwick, et al 2006 demonstrated that wall slide exercise produces similar SA activity as wall push up with plus
Quadruped rock-back

Strength Training• Focus on strengthening weak
scapular muscles without increasing activity of hyperactive muscles
• Low UT/LT, UT/MT, and UT/SA ratios
• Goal to strengthen SA and LT
• Reinold, et al 2009
Best Strengthening Exercise for Serratus Anterior
• Push up with plus on physioball
• Dynamic hug
• Serratus punch at 120 degrees

Best Strengthening Exercise for the LT
• Prone full can
• Prone ER at 90 degrees Abduction
• Prone Horizontal Abduction at 90 degrees ER
Best Strengthening Exercise for Suprapinatus
• Full can with scapular retraction below 60 degrees
• Prone full can
Best Strengthening Exercise for Infraspinatus/Teres Minor
• Side lying ER with towel
• Prone ER at 90 degrees Abduction
• Standing ER at 45 degrees scapular Abduction

Best Strengthening Exercises for Subscapularis
• IR at 0 degrees Abduction
• IR at 90 degrees of Abduction
• Push up with plus on ball
• Dynamic hug
Integration of Kinetic Chain
• Implement sport-specific activities
• Perform plyometric and eccentric exercises
• Core/Proximal hip strengthening

Do's and Dont's• Avoid anterior humeral glide
• Avoid over stretching anterior capsule in swimmers and throwers
• Postural alignment
• Be careful with prone ball exercises
• "Down and back"
Other Things to Consider
• Breathing Patterns
• Pelvic position
• Taping/postural shirts
• NMES
Conclusion• Many factors contributing to
altered scapular kinematics
• Need to have good understanding of scapulohumeral rhythm
• Select most appropriate exercise
• Integrate Kinetic Chain

Thank you