schistosomiasis
TRANSCRIPT

SCHISTOSOMIASIS/
BILHARZIOSISBY:
INUSAH ADAMS
4th yr med. Student
TDMU, Ukraine
DEC, 1ST, 2012
TDMU

Bilhazia in Ghana

PLAN OF PRESENTATIONDEFINITION
EPIDEMIOLOGY
ETIOLOGY
MODE OF TRANSMISSION/LIFE CYCLE
PATHOGENESIS
SIGNS &SYMPTOMS
DIAGNOSIS
DIFFERENTIALS
TREATMENT
COMPLICATIONS
PROGNOSIS

DEFINITION
• Schistosomiasis is a chronic, parasitic
disease caused by blood flukes
(trematode worms) of the genus
Schistosoma
• Also, called snail fever

EPIDEMEOLOGYThe disease is found in Africa, South
America, East Asia and Middle East
Over 230 million people require treatment for schistosomiasis yearly
90% of those requiring treatment for schistosomiasis live in Africa.
More than 200,000 deaths per year are due to schistosomiasis in sub-Saharan Africa

ETIOLOGY• Parasitic worms of schistosoma species
Main species are;
a. Schistosoma haematobium
b. Schistosoma mansoni
c. S. japonicum
d. S. mekongi and
e. S intercalatum

Two forms of schistosomiasis exist
1. Intestinal schistosomiasis and
2. Urogenital schistosomiasis

SCHISTOSOMA MANSONI (lateral spine)

SCHISTOSOMA HAEMATOBIUM(terminal spine)
• TT

RISK FACTORS• wading or swimming in lakes, ponds and
other bodies of water which are infested
with the snails
• Fishing (both men and women)
• Women washing clothes in infested water
are at risk
• People with STIs

LIFE CYCLE• : parasite eggs are released(by way of urination
or defecation) into the environment from infected
individuals.
• The eggs hatch on contact with fresh water to
release the free-swimming miracidium
• Miracidium penetrates a water snail tissue where
it develops into cercaria
• Cercaria is release into the water from the snail
• cercaria penetrates the skin of human (definitive
host), circulate to organs (GIT, urinary tract)
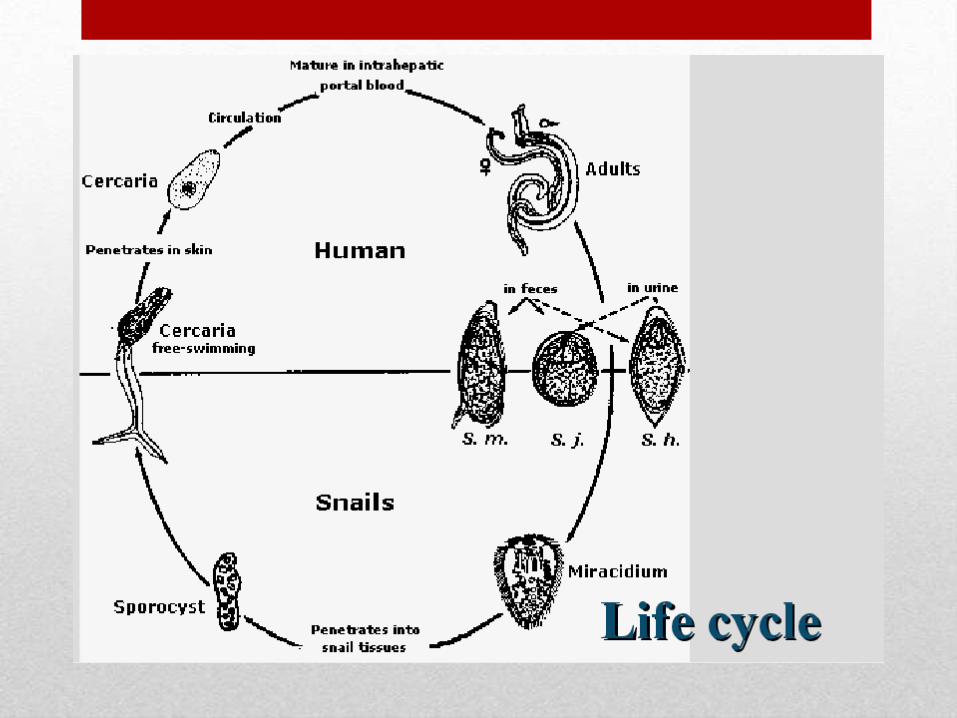

LIFE CYCLE
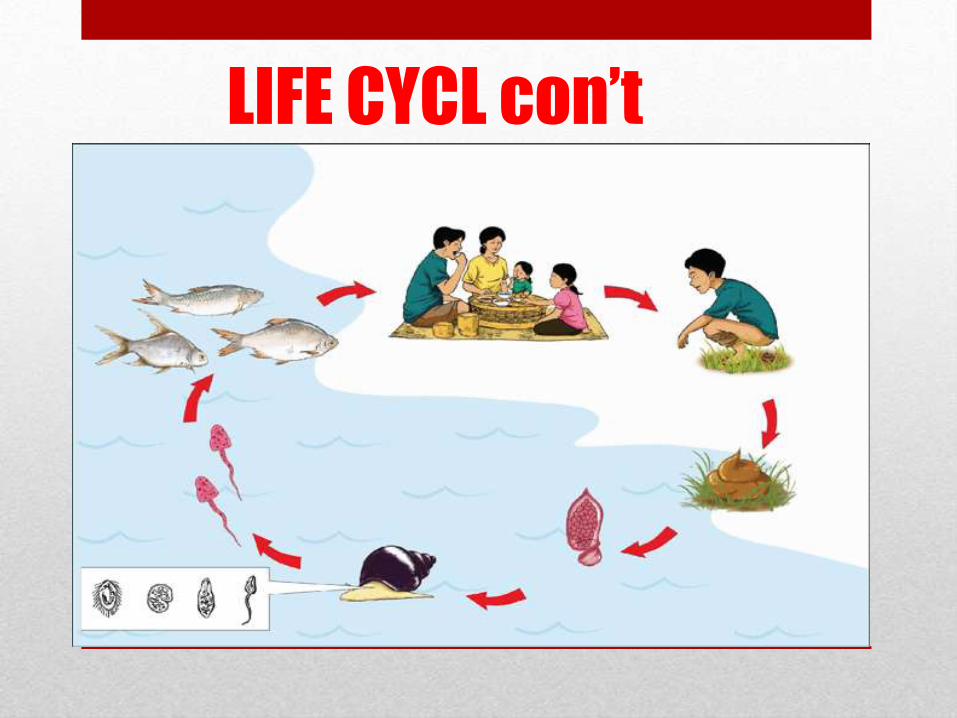
LIFE CYCL con’t


Schistosoma dermatitis or “swimmers itch”

PATHOGENESIS1. People become infected when larval forms of the
parasite – released by freshwater snails – penetrate
their skin during contact with infested water.
2. the larvae develop into adult schistosomes
3. Adult schistosomes live in the blood vessels where
the females release eggs
4. Some of the eggs are passed out of the body in the
faeces or urine to continue the parasite life-cycle
5. Others become trapped in body tissues (intestinal
and urinary system), causing an immune reaction
and progressive damage to organs.
SIGNS & SYMPTOMS• Clinical picture: low grade fever. Fatigue, weight loss and
anemia
• INTESTINAL SCHISTOSOMIASIS
1. Abdominal pain
2. Diarrhea
3. Blood in stool, fresh or melena
4. Hematemesis
5. Liver enlargement
UROGENITAL SCHISTOSOMIASIS
1. Hematuria (terminal)
2. dysuria
3. Frequent need to urinate (polykauria)
4. In females; genital lesions, vaginal bleeding, pain during sexual intercourse and nodules on the vulva, irregular menstruation

DIFFERENTIAL DIAGNOSISUROGENITAL SCHISTOSOMIASIS
• Renal tuberculosis ("golf-hole" (gaping) ureteral orifice is seen during cystoscopy, Yellow raised nodules) surrounded by a halo of hyperemia in bladder)
• Urogenital tract cancer ( total hematuria, hematuria may stop and recur in a week, month or year time)
• Urolithiasis (colicky pain)
INTESTINAL SCHISTOSOMIASIS
• Peptic ulcer disease (heartburns, GERD,
endoscopically, ulcer in GIT)
• Pancreatitis (H-like pain, vomiting that is worsened with eating, high diastase level, etc.)
• cutaneous leishmaniasis (non-healing raised, scaling lesions on the skin)

DIAGNOSTIC PLAN
1. stool examination for S. mansoni and ova
2. Urinalysis and urine for S. hematobium and ova
3. General blood analysis:
4. Serological: hemagglutination test; reaction is positive @ a dilution of 1: 16 or more
5. BUN and creatinine level
6. Ureterocystoscopy
7. Biopsy of rectum or urinary bladder
8. Plain abdominal X-ray: chronic cases may show calcification and fibrosis of ureters, urinary bladder, ascites
9. Intravenous urography: may show the level of ureter stricture
10. Ultrasound of abdomen: hepatosplenomegaly, bilharzial hepatic fibrosis, ascites
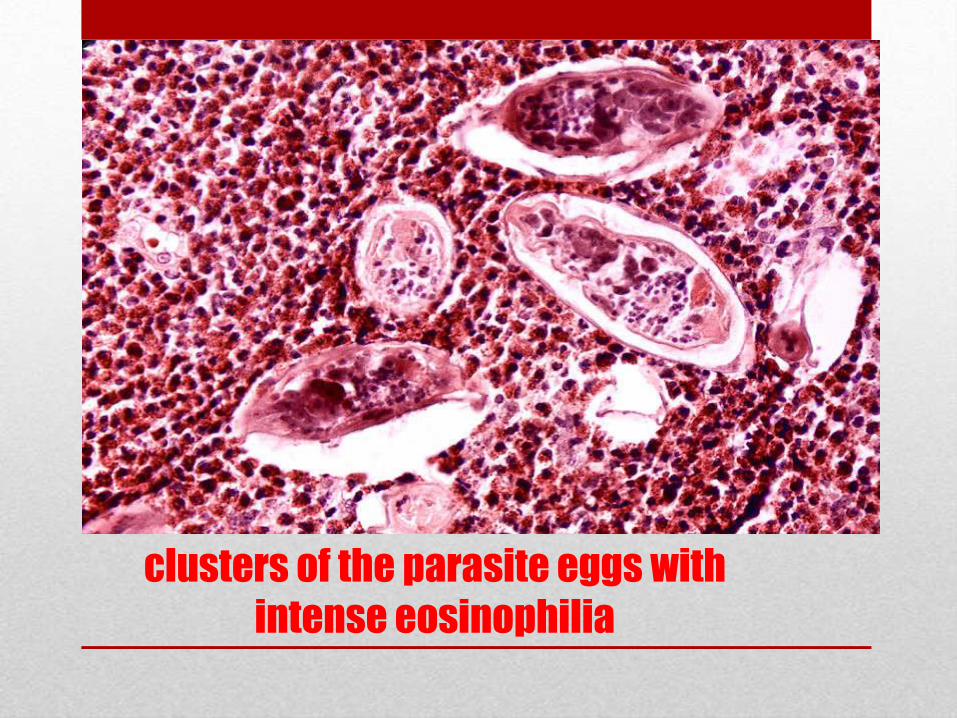
clusters of the parasite eggs with
intense eosinophilia

Calcification of the urinary bladder



Yellow raised nodules surrounded by a
halo of hyperemia (TB of bladder)

Cystoscopy in tumor of kidney
(gross hematuria)

TREATMENT
• Drug: Prazequnatel
Dose: 40mg/kg single oral dose
60mg/kg in 2 divided doses if
quantity of ova is high
Review in 2 weeks

COMPLICATIONS
Urogenital schistosomiasis
1. cystitis
2. Urinary bladder cancer
3. Polyps, ulcers of urinary bladder
4. Hemospermia
5. Infertility
6. Spontaneous abortion
7. Renal failure
8. anemia
Intestinal schistosomiasis
1. Liver fibrosis
2. Intestinal cancer
3. Portal hypertension/Pulmonary hypertension/ Cor pulmonale
4. Ascites
5. Esophageal varices
6. Malnutrition

PROGNOSIS
• Always good especially with prompt
diagnosis and treatment

PREVENTION
Education
Eliminating the water-borne snails which are natural reservoirs for the disease
Annual dose of prazequantel
adding niclosamide, acrolein, copper sulfate, etc., to the water sources in order to kill the snails.
Avoid swimming and contact with fresh water in endemic areas
Boiling water for 1 minute will kill the parasite. (Filtration of drinking water )

• GHANA AND BILHARZIA
