school failure. etiology of school failure why does he read saw for was? can’t he see the...
TRANSCRIPT

SCHOOL FAILURE

Learning disabilitiesAttention deficitsMental retardationSensory impairmentEmotional disturbanceChronic illnessTemperamental dysfunctions
Intrinsic conditions
Family dysfunctionSocial problemsIneffective schooling
Extrinsic conditions
ACADEMIC UNDERACHIEVEMENT (SCHOOL FAILURE)

Etiology of School Failure
Cause Approximate Prevalence (In over-all population)
Mental Retardation Learning Disability Attention Deficit Disorder Emotional Disturbance Chronic Illness Ill-Defined Factors
2% - 3% 7% - 10%
5% 5% - 10%
5% ?


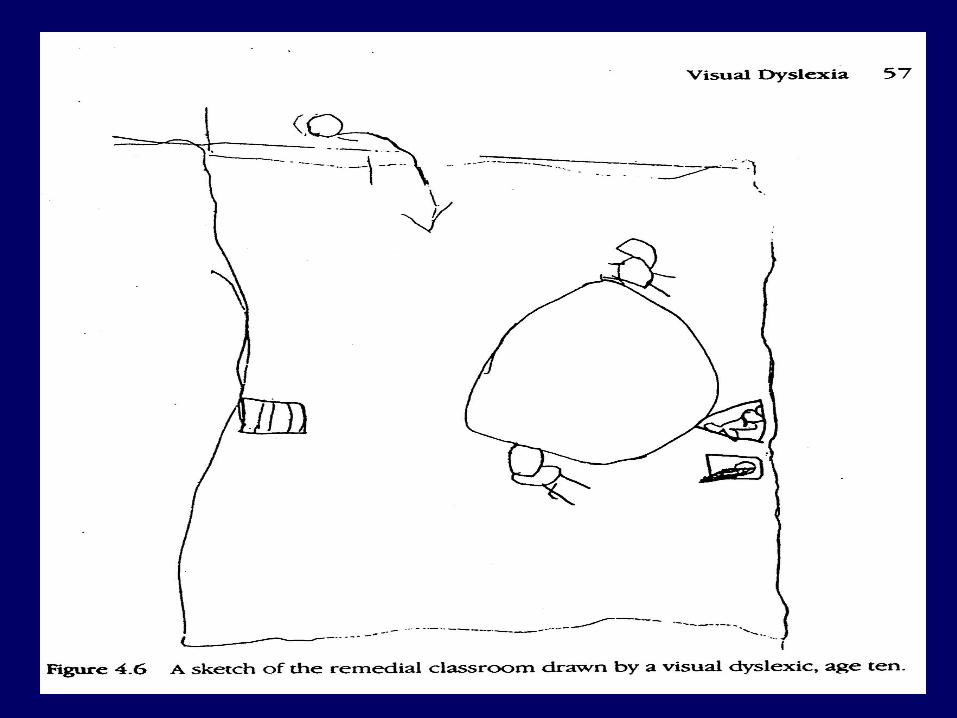
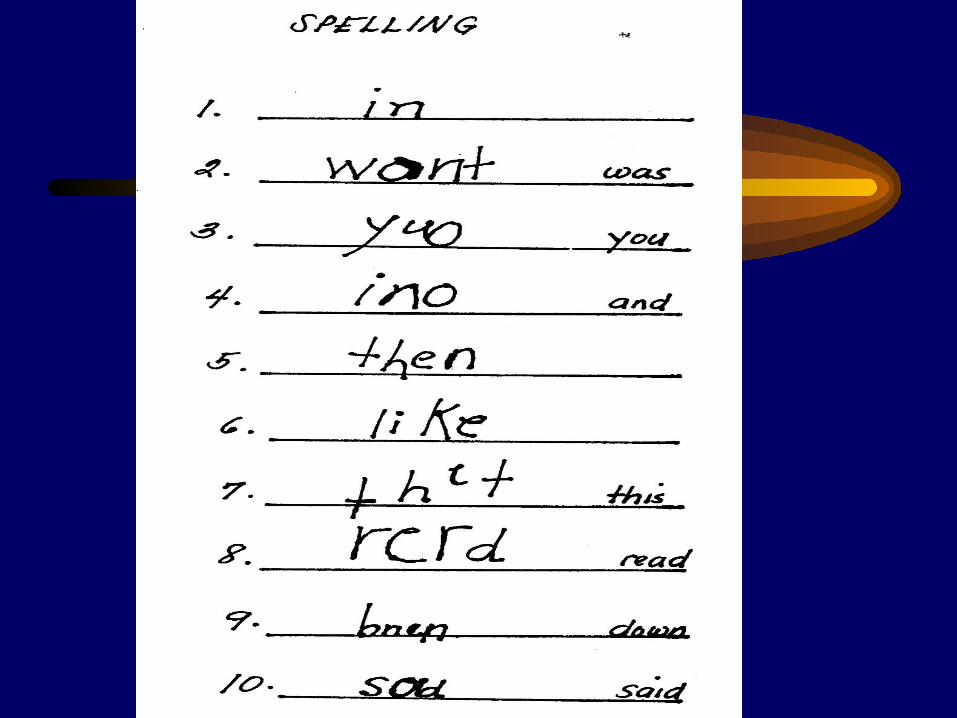
Why does he read SAW for WAS?Can’t he see the difference between b and d?
How come she read all these words
yesterday, and she can’t read them today?Will he never learn the days of the week?

Can’t he stop talking for 5 minutes?
Why won’t he behave at school?
He’s so good and he tries so hard, why can’t he learn?
How could she put down the same answer to four different arithmetic problems?

Who is this child?

• Generic term referring to a heterogenous group manifested as significant difficulties in the acquisition and use of listening, speaking, reading, writing, reasoning, or mathematical skills.
• Disabilities are intrinsic and are presumed to be due to CNS dysfunction.
• Co-morbid factors (emotional, sensory, cultural, etc) not the direct cause
LEARNING DISABILITIES

LEARNING DISABILITIES
• Of the basic 3 “Rs”of learning (reading, ‘riting’ and ‘rithmetic’), reading difficulty is usually easily recognized.
• Becomes manifest at the end of the 1st grade

Etiology
• Unknown• ? Developmental alterations of CNS• In early years, difficult to state
whether the problem is due to neuromaturational lag or true LD
• Genetic factors play an important role, there is often a strong FH of LD











Presentation of Learning Disability in the Different Grade Levels
Motor problems (especially fine motor)Sequencing difficultyLanguage dysfunction (including
articulation)Hyperactivity/aggressiveness
Kindergarten

UnderachievementWritingReading comprehensionBehavior
Decoding
Behavior
Behavior
Early Primary
Late Primary
Middle school

Clinical Evaluation
• Specific attention to child’s language skills (ordinary conversation)
• Academic and intellectual screening tests• Reading (word recognition and comprehension)• Mathematics (verbal and written)• Spelling (verbal and written) and writing• Constructional abilities (Bender and Beery)• Draw - A - Person• General information, abstract reasoning,
vocabulary
Further Assessments
• Psychometric testing - very important• Others depend on symptomatology
• Language problems - Speech and language evaluation and therapy
• Blood tests, karyotyping, metabolic screening - no clinical value
• EEG- not routine, only when seizures are present or strongly suspected;
• Childhood Absence Epilepsy is most frequently mistaken for LD
• Neuroimaging - more academic than practical

Patient: 12-year old with learning disability
Result of WISC Test:
Verbal IQ 128
Performance 88
Full Scale IQ 108

Verbal testsInformation 14Similarities 15Arithmetic 9Vocabulary 17Comprehension 13
Performance testsPicture Completion 8Picture Arrangement 10Block Design 7Object Assembly 10Coding 3

Impression
Verbal IQ – superior
Performance IQ – low-average
Visual-perceptual, visual-sequencing, visual abstraction, visual memory, fine motor & visual motor disabilities

Psychosocial Problems for the Child with Learning Disabilities
Emotional/Social problems
Withdrawal
Regression
Displacement and Projection
Weak Self-image

Prognosis
• Most LD improve in time• Complete recovery to normality does not
appear to happen• Reading disabled will be able to read but
slowly and laboriously (6th grade, sufficient for everyday living and even for college
• Spelling, writing and arithmetic deficits are rather resistant and pervasively persist

Treatment
• Educational intervention - cornerstone of treatment for LD
• Educational settings -• Structured• Private tutorial sessions• Resource rooms
• While no single best approach or specific treatment is most specific for LD, every effort should be made to fit the needs of the child

Treatment
• Unrecognized LD, often already with emotional problems and may be more difficult to treat,
counseling is a must.• Explain to the child that his
problems are however not his passport to completely neglect his
academics.

Treatment
• Since most LD are resistant to remediation, and up until specific teaching methods are available, perhaps a good way of teaching these children is bypassing the deficits