school re-entry after traumatic brain injury: for educators anne bradley, ph.d sarah powell, m.ed....
TRANSCRIPT
School Re-Entry after Traumatic Brain Injury:
For Educators
Anne Bradley, Ph.D
Sarah Powell, M.Ed. CCC-SLP
Roger C. Peace Rehabilitation Hospital
Traumatic Brain Injury Program
Goals
• Understanding Traumatic Brain Injury• Returning to School• Identification and Assessment• Intervention and Classroom
Accommodations• Advocacy and Resources
Preview of Section 1: Understanding Brain Injury
• Appreciate the under-reported nature of TBI
• Learn what a brain injury is• Learn how to identify the
level of severity of a brain injury
• Be able to generally predict the early course after injury

Disguised as a Low Incident Disability…
• Each year, an estimated 1.7 million people sustain a TBI annually. Of them: – 52,000 die, – 275,000 are hospitalized, and – 1.365 million, nearly 80%, are treated and
released from an emergency department.
– The number of people with TBI who are not seen in an emergency department or who receive no care is unknown.
Incidence and Prevalence
• Children aged 0 to 4 years, older adolescents aged 15 to 19 years, and adults aged 65 years and older are most likely to sustain a TBI.
• Almost half a million (473,947) emergency department visits for TBI are made annually by children aged 0 to 14 years.
• Only 200 of every 100,000 cases go to the hospital.
Parts of the Brain
Definition of TBI
• Acquired Brain Injury• Congenital and Perinatal Brain Injury• Traumatic Brain Injury
– Open Head Injury– Closed Head Injury
Acquired Brain Injury
• Brain Injury incurred after a period of normal development– Internal causes– External causes
Congenital and Perinatal Brain Injury
• No period of normal development• Congenital- a condition a child is born with
such as a chromosomal abnormality• Perinatal- a condition that develops
around the time of birth such as a perinatal stroke
Traumatic Brain Injury
• An acquired injury to the brain caused by an external physical force, resulting in total or partial functional disability or psychosocial impairment or both, that adversely affects a child’s educational performance.
Effects of Brain Injury
• Injury to brain tissues at the site of damage
• Shearing and tearing of neurons throughout the brain
• Bleeding, swelling, and lack of oxygen to the brain
• Possible coma
Severity of Brain Injury
• Mild• Moderate• Severe
Mild Traumatic Brain Injury: AKA Concussion - Definition
• Any period of loss of consciousness• Any loss of memory for events
immediately before or after the accident• Any alternation in mental state at the time
of accident• Posttraumatic amnesia is no greater than
24 hours• Signs of concussion nausea and
vomiting, headache, fatigue, dizziness

Concussion: Sports related injuries
Immediate Presentation: Delayed effects:
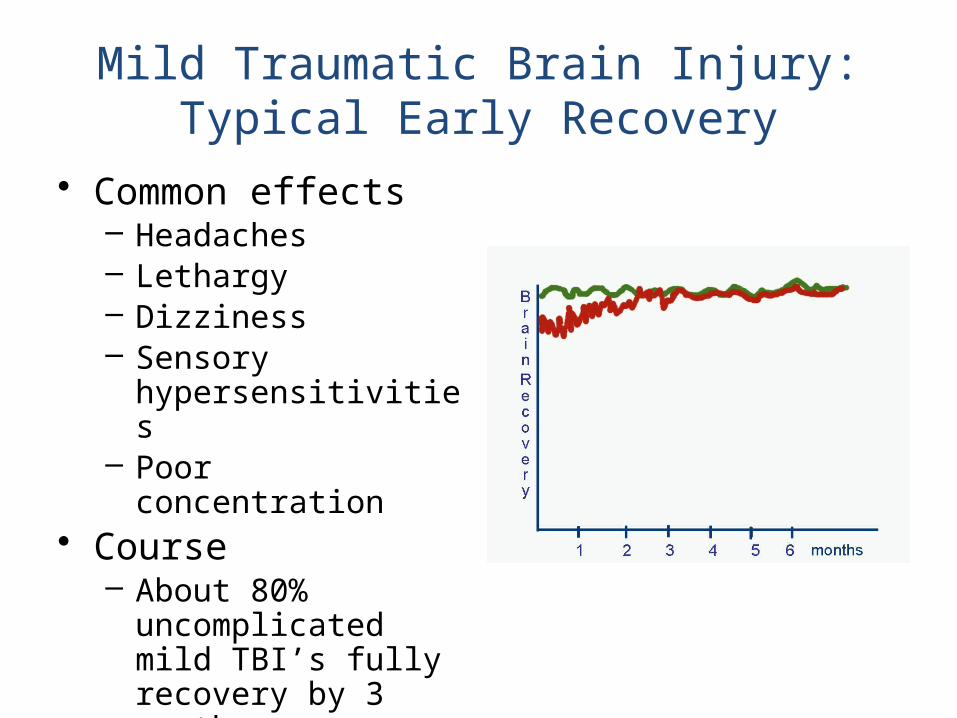
Mild Traumatic Brain Injury:Typical Early Recovery
• Common effects– Headaches– Lethargy– Dizziness– Sensory
hypersensitivities– Poor concentration
• Course– About 80%
uncomplicated mild TBI’s fully recovery by 3 months
Mild Traumatic Brain Injury: Treatment
• Estimated 80% of concussions are not treated
• Most often seen in the emergency room or by pediatrician and sent home
• Out of school perhaps a day or two, up to a couple weeks
Moderate Traumatic Brain Injury: Definition
• Coma less than 24 hours duration• Post traumatic amnesia 1-24 hours• Neurological signs of brain trauma
– Tissue damage– Bleeding
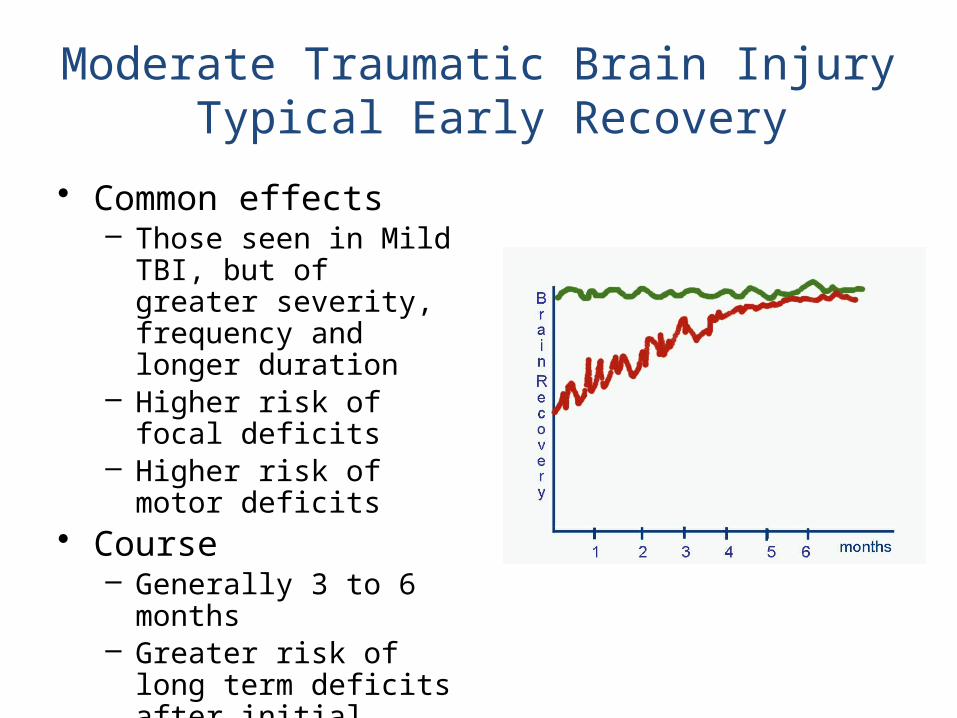
Moderate Traumatic Brain Injury Typical Early Recovery
• Common effects– Those seen in Mild TBI,
but of greater severity, frequency and longer duration
– Higher risk of focal deficits
– Higher risk of motor deficits
• Course– Generally 3 to 6 months– Greater risk of long term
deficits after initial recovery
Moderate Traumatic Brain Injury: Treatment
• Most often seen in the emergency room or by pediatrician and sent home
• Occasionally hospitalized on an acute care medical unit for days to a couple weeks
• Rarely receive inpatient rehabilitation• More frequently receive outpatient
therapies (most often if there is a deficit in physical functioning)
Severe Traumatic Brain Injury:Definition
• Coma more than 24 hours• Post Traumatic Amnesia more than 1 day
Severe TBI sustained in a snowboarding accident: Recovery after a 2 month coma
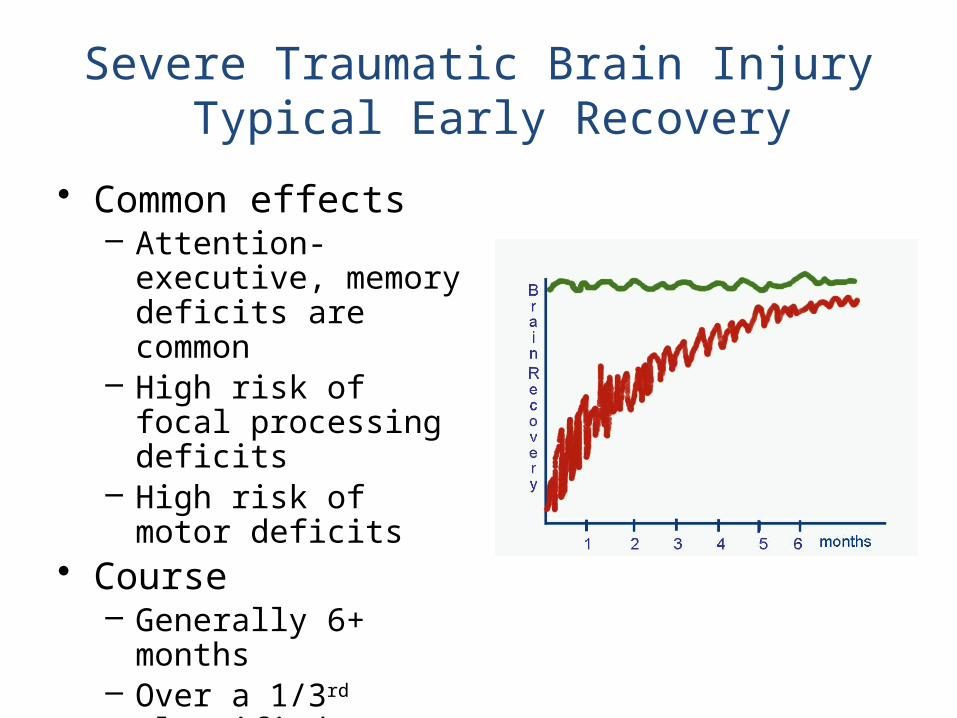
Severe Traumatic Brain Injury Typical Early Recovery
• Common effects– Attention-executive,
memory deficits are common
– High risk of focal processing deficits
– High risk of motor deficits
• Course– Generally 6+ months– Over a 1/3rd classified
as disabled after initial recovery period
Severe Traumatic Brain Injury: Treatment
• Short to very long stays in ICU/PICU/ NeuroICU’s
• More likely to get inpatient rehabilitation, but more frequently seen by therapists in an acute medical care setting
• Average inpatient rehabilitation stays are 2 to 4 weeks
• The younger they are the less likely referred to inpatient rehabilitation and the quicker they are discharged home
• Most likely to be referred to outpatient therapy
Review of Section 1: Understanding Brain Injury
• Appreciate the under-reported nature of TBI
• Learn what a brain injury is• Learn how to identify the
level of severity of a brain injury
• Be able to generally predict the early course after injury.
Preview of Section 2: Returning to School
• Identify what actions need to be take to facilitate school re-entry after brain injury
• Identify common physical and cognitive sequelae of brain injury
• Assess issues that distinguish TBI from other diagnoses
• Identify means by which the student’s needs can be assessed
The Process of School Re-entry:Who, When and How?
School Re-entry Who
How
When
The Process of School Re-entry:Who
Family
ChildSchool
Medical staff
The Process of School Re-entry:When
At Injury
Hospital
Stay
Discharge
Home
The Process of School Re-entry:Moderate to Severe Brain Injury - How
Medical Staff
Families
• Identify a family and medical contact person to receive and provide information
• Focus on the provision of medical care
• Integrate the family into the patient’s care
Educational Staff
• Participate in their child’s medical care
• Make their wishes known regarding visits and other contacts
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Moderate to Severe Brain Injury
Medical Staff• Identify a school contact person• Provide updates on progress and needs• Provide information needed for the school
to evaluate the student’s needs and form a reasonable school re-entry plan
• Educate family and school staff
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Moderate to Severe Brain Injury
Educational Staff• Request updates from medical contact
person• Identify appropriate members of school re-
entry team• Share information about student’s prior
achievement and behavior with medical contact person
• Educate medical staff regarding local education resources and procedures
• Update others as needed
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Moderate to Severe Brain Injury
Family
• Consent to allow communication between school and medical staff
• Facilitate contact between appropriate staff members
• Participate in education provided by medical staff
• Make wishes known regarding support needs
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Moderate to Severe Brain Injury
Medical Staff• Inform family and school of discharge date• Provide discharge summaries• Provide summaries of treatment and recommendations• Complete appropriate paperwork to support
recommendations (e.g., homebound, therapies at school, Early Childhood referral)
• Maintain ongoing collaboration with schools as proceeds through outpatient therapies
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Moderate to Severe Brain Injury
Educational Staff• Educate family about homebound, Section 504, and/or
special education process• Refer for special education services if appropriate• Obtain medical records• Arrange for staff education (don’t forget homebound
teachers)• Meet to determine if more evaluation is needed, and/or
what is the appropriate immediate school plan for re-entry
• Maintain ongoing collaboration with outpatient therapies
At Injury
HospitalStay
Discharge Home
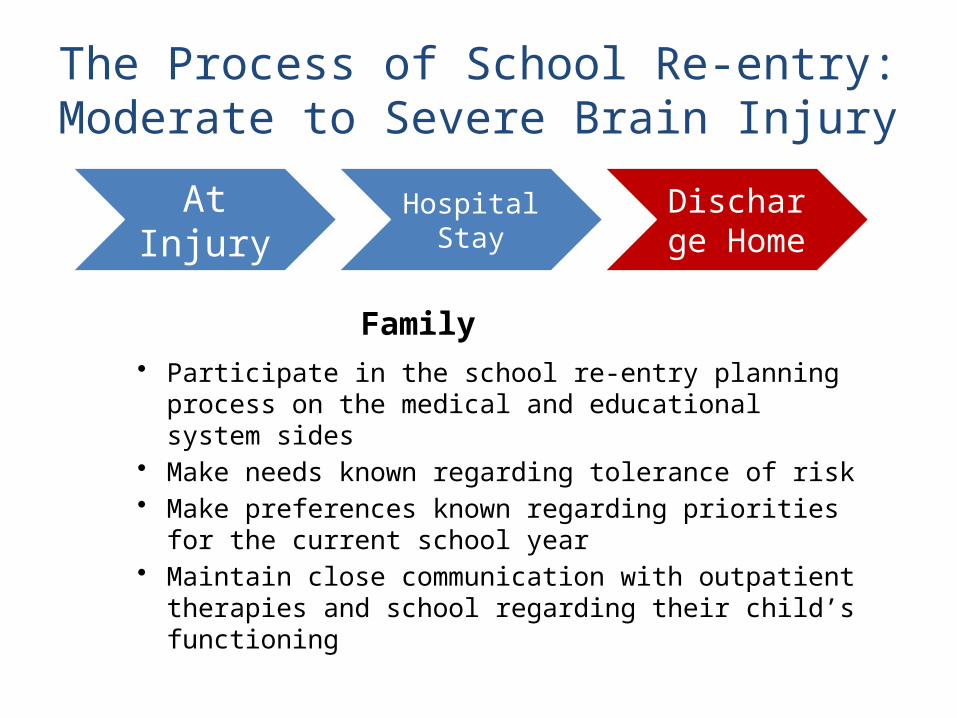
The Process of School Re-entry:Moderate to Severe Brain Injury
Family
• Participate in the school re-entry planning process on the medical and educational system sides
• Make needs known regarding tolerance of risk• Make preferences known regarding priorities for
the current school year• Maintain close communication with outpatient
therapies and school regarding their child’s functioning
At Injury
HospitalStay
Discharge Home
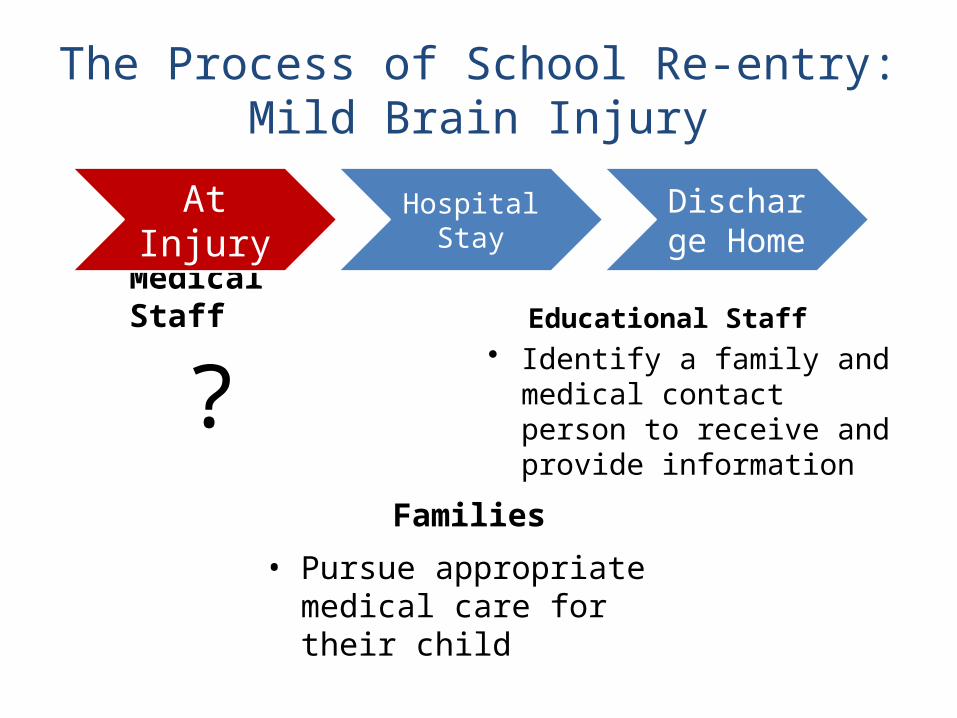
The Process of School Re-entry:Mild Brain Injury
Medical Staff
Families
• Identify a family and medical contact person to receive and provide information
?Educational Staff
• Pursue appropriate medical care for their child
At Injury
HospitalStay
Discharge Home
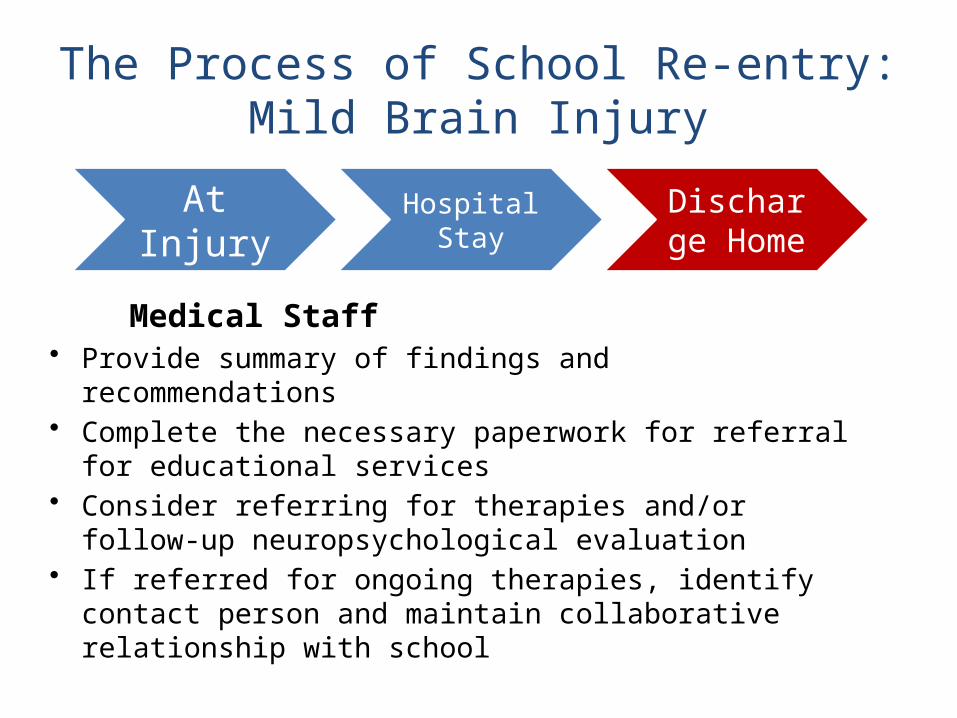
The Process of School Re-entry:Mild Brain Injury
Medical Staff• Provide summary of findings and recommendations• Complete the necessary paperwork for referral for
educational services• Consider referring for therapies and/or follow-up
neuropsychological evaluation• If referred for ongoing therapies, identify contact
person and maintain collaborative relationship with school
At Injury
HospitalStay
Discharge Home
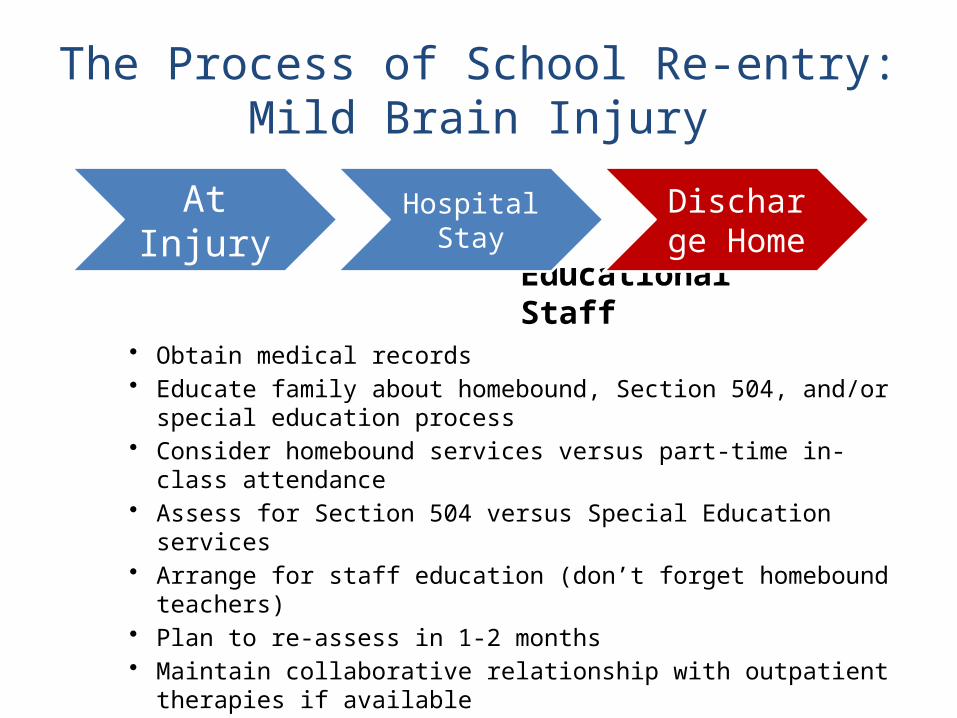
The Process of School Re-entry:Mild Brain Injury
Educational Staff• Obtain medical records• Educate family about homebound, Section 504, and/or
special education process• Consider homebound services versus part-time in-class
attendance• Assess for Section 504 versus Special Education services• Arrange for staff education (don’t forget homebound
teachers)• Plan to re-assess in 1-2 months• Maintain collaborative relationship with outpatient therapies if
available
At Injury
HospitalStay
Discharge Home
The Process of School Re-entry:Mild Brain Injury
Family
• Participate in the school re-entry planning process on the medical and educational system sides
• Make needs known regarding tolerance of risk• Make preferences known regarding priorities for
the current school year• Maintain close communication with outpatient
therapies and school regarding their child’s functioning
At Injury
HospitalStay
Discharge Home
TBI Students
• Identification• Assessment/Evaluation
Which student has a TBI?
• Can you tell?
Common Problems of Students with TBI
• Anticipating these difficulties can facilitate successful re-entry to school
• Problems can be physical/medical, cognitive, sensory, motor, social, emotional, and behavioral
Physical/Medical Problems
• Problems– Seizures– Fatigue– Headaches– Swallowing/Eating– Self-care activities
• Medication issues
Most Common Physical Deficits:
• Physical Endurance• Mental Endurance• Headaches
Motor Problems
• Apraxia• Ataxia• Coordination problems• Paresis or paralysis• Orthopedic problems
• Spasticity• Balance problems• Impaired speed of movement
Most Common Motor Problems:
• Balance• Fine Motor Dexterity• Motor Speed
Sensory/Perceptual Problems
• Visual deficits– field cuts– tracking (moving and stationary objects)– spatial relationships– double vision (diplopia)
• Neglect / Inattention• Auditory sensory changes• Tactile sensory changes
Most Common Sensory/Perceptual Issues:
• OVERSTIMULATION!• Double Vision• Neglect / Inattention• Hypersensitivities
Cognitive-Communication Problems
• Executive functions • Memory• Attention• Concentration• Information processing• Sequencing
• Problem solving• Comprehension of abstract language• Word retrieval• Expressive language organization• Pragmatics
Most Common Cognitive-Communication Deficits:
• Slowed Processing Speed• Intolerance of Complexity• Attention• Memory
Emotional & Behavioral Problems
• Irritability• Impulsivity• Disinhibition• Perseveration• Emotional Lability• Insensitivity to social cues• Low frustration tolerance
• Anxiety• Withdrawal• Egocentricity• Denial of deficit/lack of insight• Depression• Peer conflict• Sexuality concerns• High risk behavior
Most Common Emotional-Behavioral Problems:
• Fragile Emotional Control• Poor Awareness• Impulsivity• “Just don’t get it”
4 Facts about Identification
• Each student will vary greatly, no 2 will be alike• Changes are unlikely to disappear fully over time• Negative consequences may not be seen
immediately but emerge when developmental demands reveal problems
• An injured brain is less likely to meet the increasingly complex tasks all children face as they get older
Misclassified or Missed Altogether
• Poor transitional services between hospitals and schools
• Timing of injury• Mild TBI slips thru the cracks• Traditional approaches to assessment fail to
provide necessary insight into how cognitive deficits impact school
• Special Ed for TBI vs. LD vs. ED looks different• Deficits are not always immediately apparent
How is TBI different from LD?
• TBI is not “just a learning disability”• Students with TBI cannot be dealt with as
if they have something similar• Although similar, the differences are
important• The impairments are different, as are the
implications for educators
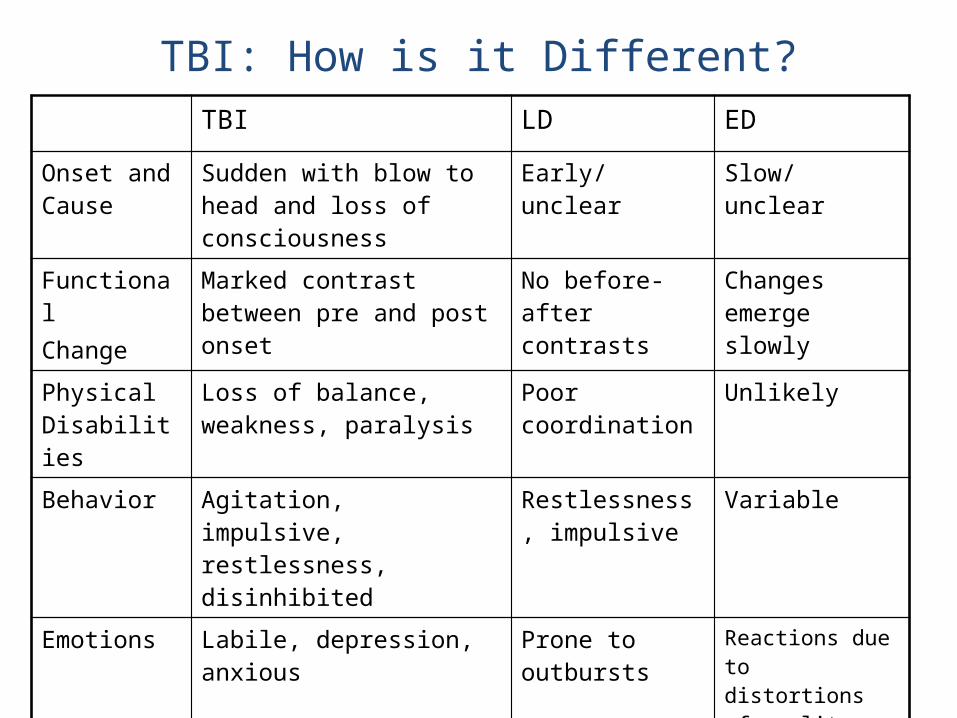
TBI: How is it Different?TBI LD ED
Onset and Cause
Sudden with blow to head and loss of consciousness
Early/ unclear Slow/ unclear
FunctionalChange
Marked contrast between pre and post onset
No before-after contrasts
Changes emerge slowly
Physical Disabilities
Loss of balance, weakness, paralysis
Poor coordination
Unlikely
Behavior Agitation, impulsive, restlessness, disinhibited
Restlessness, impulsive
Variable
Emotions Labile, depression, anxious Prone to outbursts
Reactions due to distortions of reality
Academic Deficits
Based on disrupted cognition
Based on type of learning disability
Not based on impaired cognition
Difficulties with Learning
Old info easier to recall than new info
New learning can be linked with old learning
New learning can be linked with old learning
Information to Determine Needs
• Obtain all medical information you can• Information about areas of functioning
– Cognition and memory– Speech and language; communication– Sensory and perceptual abilities– Motor abilities– Psychosocial impairments– Physical functions/safety– Academic skills
Challenges to Evaluation: Student Factors
• Rapidly changing skills (especially during first 6-12 months)
• Communication, physical, sensory, motor, emotional, and behavioral difficulties may interfere with assessment
• Uneven skill profile (some higher skills preserved with lower skills lost)
• Performance influenced by state and situation• Problems may emerge later
Other Challenges to Evaluation
• The family is probably in distress• Initial assessment is probably conducted
outside school in a setting unlike the classroom
• Much assessment information is needed from other professionals (who are busy)
• Medical reports may be difficult to interpret• Assessment requires IEP team
coordination and planning
What can be done to address these challenges?
• Use classroom data to guide instruction• Use observation, curriculum-based
measures, work samples, trial teaching• Assess across content, time, settings• Invite parents to provide information• Ask medical personnel for assistance• Plan team evaluations• Share information
Cognitive Assessment…is the student?• Processing Speed
– Accurate but slow? • Memory
– Retaining new info from day to day?– Benefiting from context?– Benefiting from repetition?
• Executive Function– Prioritizing? Following through? Staying organized? – Using problem solving strategies?– Shifting from 1 task to another?
• Attention– Able to concentrate? Hold onto information?– Attending to more than 1 thing at a time?– Accurate when carrying out complex tasks?
How can I gather more info?
• Record review (school and medical)• Direct observation (school or hospital)• Student interview (if possible)• Teachers/service provider interviews• Criterion-referenced assessment• Curriculum-based assessment• Rating scales and checklists• Neuropsychological assessment (if available)• Identify cognitive strengths and weaknesses
Review of Section 2: Returning to School
• Identify what actions need to be take to facilitate school re-entry after brain injury
• Identify common physical and cognitive sequelae of brain injury
• Assess issues that distinguish TBI from other diagnoses
• Identify means by which the student’s needs can be assessed
Preview of Section 3:Interventions for Students with TBI• Identify the domains in which you can
intervene.• Identify how common physical, cognitive
and emotional/behavioral sequelae are expressed in the classroom.
• Identify several avenues of intervening to address the impact of sequelae on the student’s ability to benefit from the educational environment.
Intervention
• Environment (space and time)• Instruction and materials• School staff• Peers• Student• Family
Most Common Physical Deficits:
• Physical Endurance• Mental Endurance• Headaches
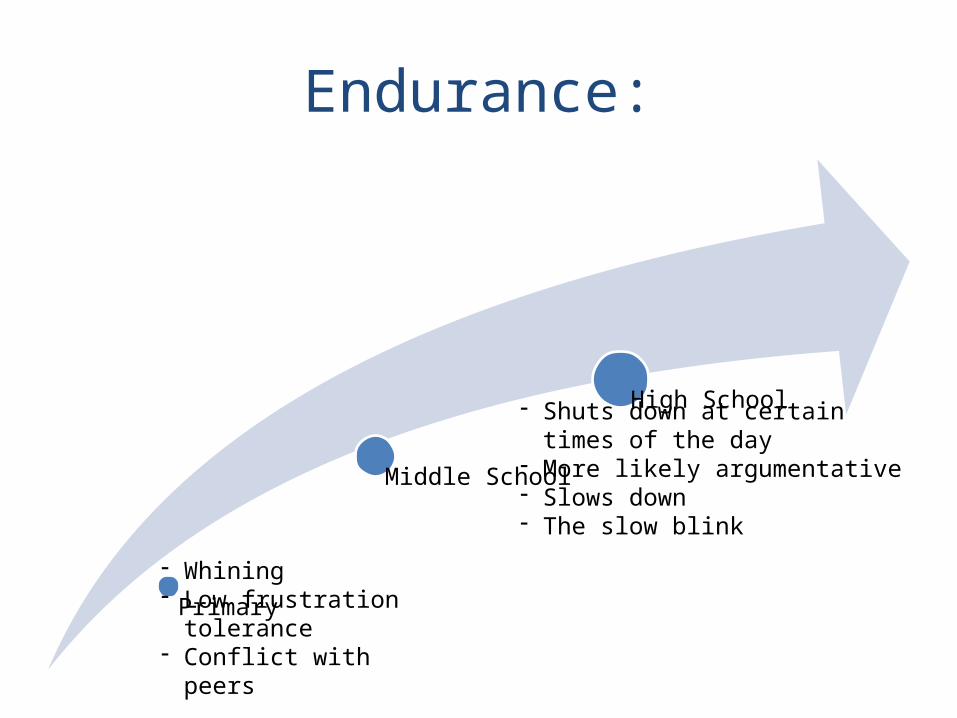
Endurance:
Primary
Middle School
High School
- Whining- Low frustration tolerance- Conflict with peers
- Shuts down at certain times of the day
- More likely argumentative- Slows down- The slow blink
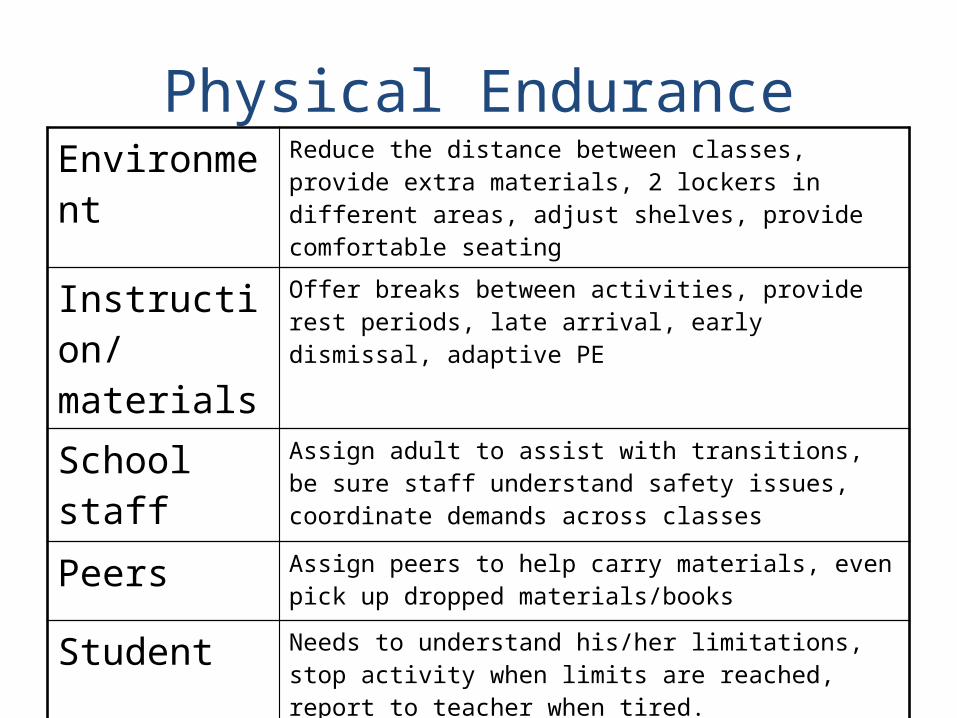
Physical EnduranceEnvironment Reduce the distance between classes, provide extra
materials, 2 lockers in different areas, adjust shelves, provide comfortable seating
Instruction/materials
Offer breaks between activities, provide rest periods, late arrival, early dismissal, adaptive PE
School staff Assign adult to assist with transitions, be sure staff understand safety issues, coordinate demands across classes
Peers Assign peers to help carry materials, even pick up dropped materials/books
Student Needs to understand his/her limitations, stop activity when limits are reached, report to teacher when tired.
Family Educate on importance of sleep and routine, adjust medications if need be
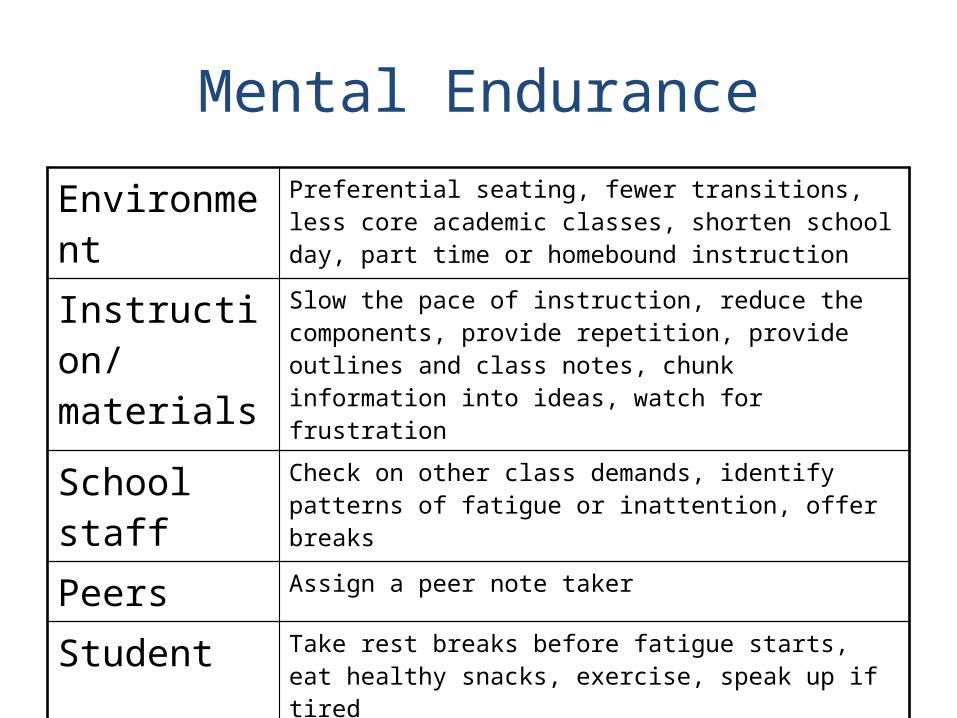
Mental Endurance
Environment Preferential seating, fewer transitions, less core academic classes, shorten school day, part time or homebound instruction
Instruction/materials
Slow the pace of instruction, reduce the components, provide repetition, provide outlines and class notes, chunk information into ideas, watch for frustration
School staff Check on other class demands, identify patterns of fatigue or inattention, offer breaks
Peers Assign a peer note taker
Student Take rest breaks before fatigue starts, eat healthy snacks, exercise, speak up if tired
Family Educate on importance of sleep and routine, adjust medications if need be
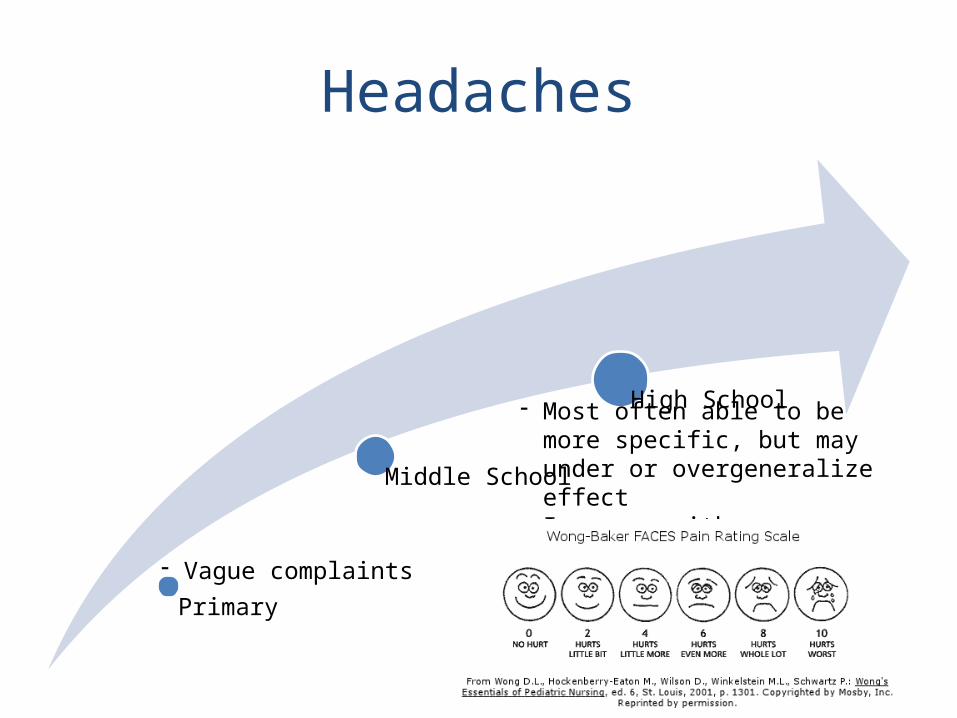
Headaches
Primary
Middle School
High School
- Vague complaints
- Most often able to be more specific, but may under or overgeneralize effect
- Increase with mental/physical exertion
Physical Signs of Severe Pain:
• Pallor• Sweating• Shallow breathing• Elevated pulse• Dilated pupils• Sensory hypersenstivities• Preoccupation• Lethargy
Headaches
Environment Allow student to leave and go to comfortable place to lay down in quiet and darkness; limit noise in classroom
Instruction/materials
Break components down, slow pace of instruction,Provide rest breaks, use intermittent teaching to avoid exacerbation
School staff Educate other staff
Peers Education
Student Encourage student to speak up at first sign of headache
Family Explore medications, consult with family or rehab doctor
Most Common Motor Problems:
• Balance• Fine Motor Dexterity• Motor Speed
Balance
Primary
Middle School
High School
- Higher rate of falls- Clumsy, bumps into things, trips- Slow and extra careful/fearful
- Dynamic balance issues- Multi-tasking while walking- Worse when tired- When burdened
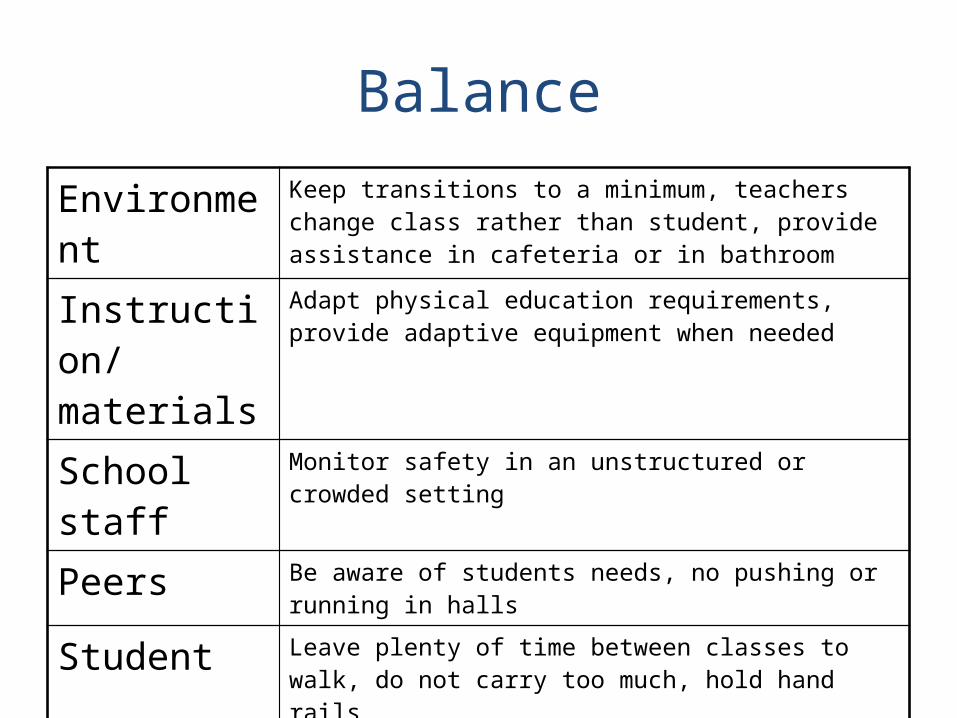
Balance
Environment Keep transitions to a minimum, teachers change class rather than student, provide assistance in cafeteria or in bathroom
Instruction/materials
Adapt physical education requirements, provide adaptive equipment when needed
School staff Monitor safety in an unstructured or crowded setting
Peers Be aware of students needs, no pushing or running in halls
Student Leave plenty of time between classes to walk, do not carry too much, hold hand rails
Family Consult with family on strategies used at home
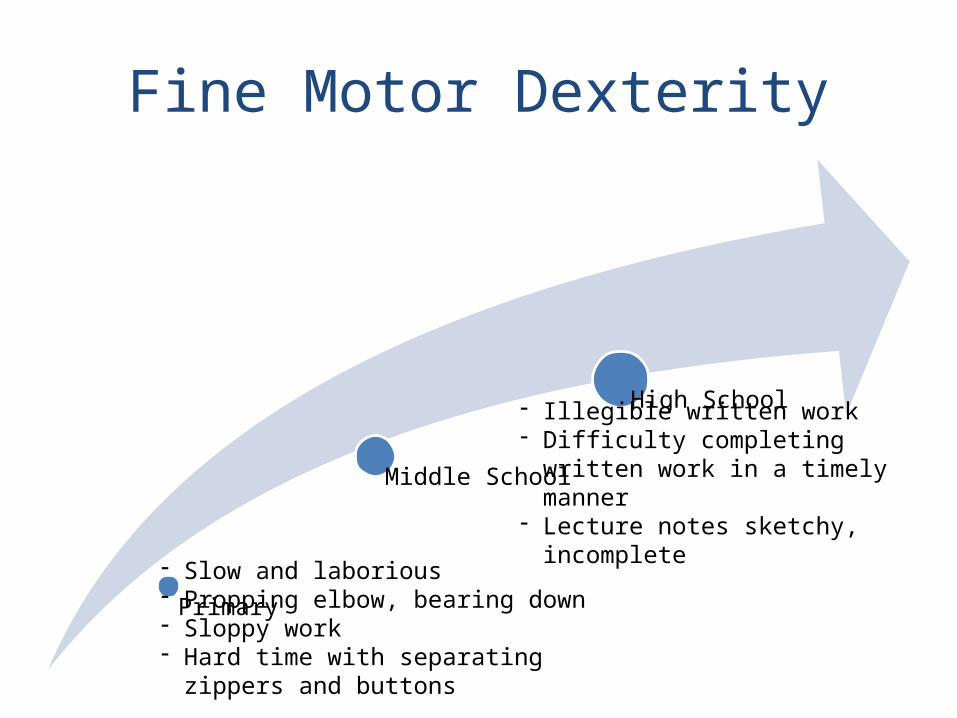
Fine Motor Dexterity
Primary
Middle School
High School
- Slow and laborious- Propping elbow, bearing down- Sloppy work- Hard time with separating zippers and
buttons
- Illegible written work- Difficulty completing written work
in a timely manner- Lecture notes sketchy, incomplete
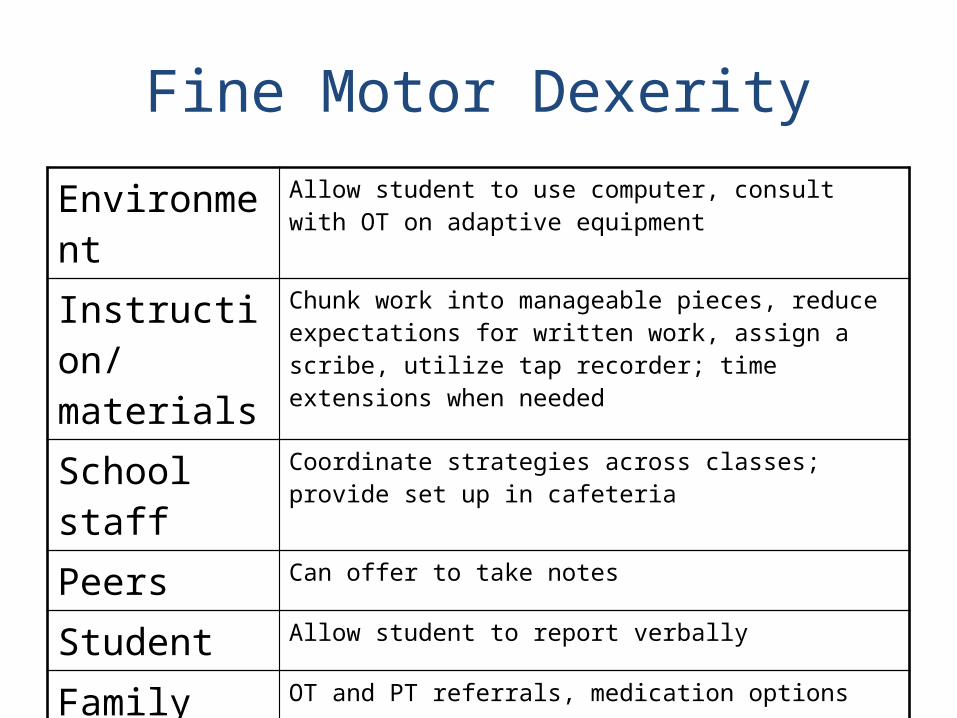
Fine Motor Dexerity
Environment Allow student to use computer, consult with OT on adaptive equipment
Instruction/materials
Chunk work into manageable pieces, reduce expectations for written work, assign a scribe, utilize tap recorder; time extensions when needed
School staff Coordinate strategies across classes; provide set up in cafeteria
Peers Can offer to take notes
Student Allow student to report verbally
Family OT and PT referrals, medication options
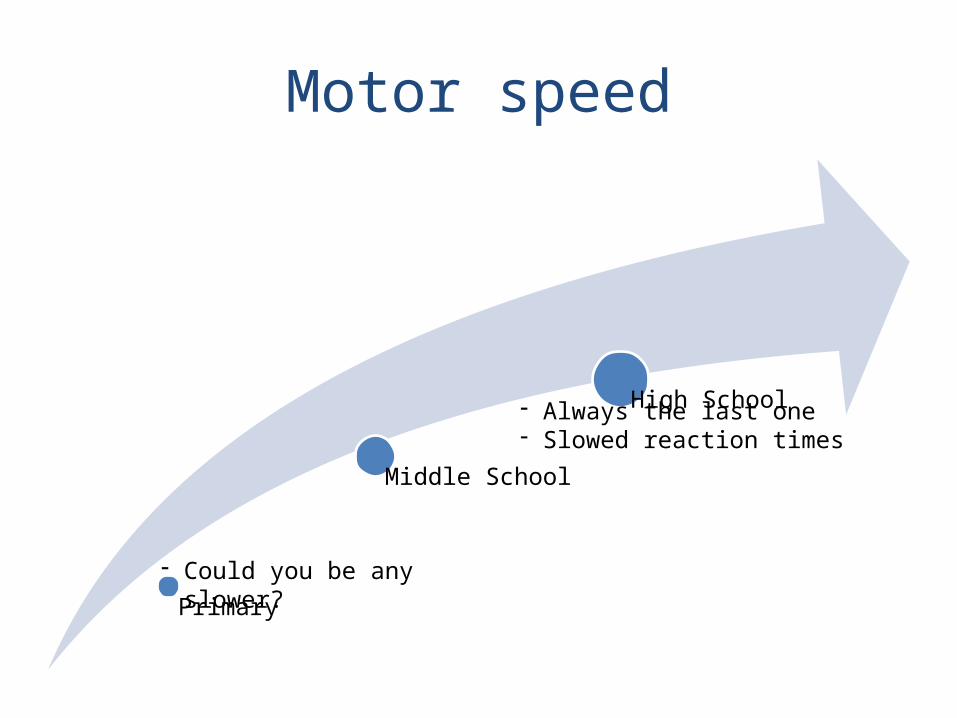
Motor speed
Primary
Middle School
High School
- Could you be any slower?
- Always the last one- Slowed reaction times
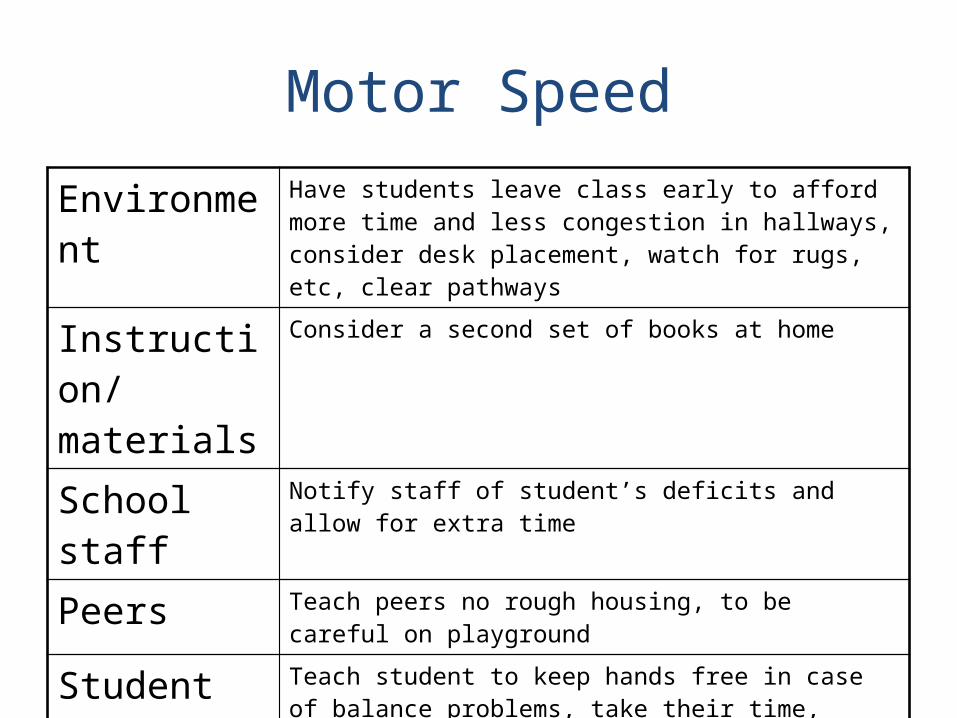
Motor Speed
Environment Have students leave class early to afford more time and less congestion in hallways, consider desk placement, watch for rugs, etc, clear pathways
Instruction/materials
Consider a second set of books at home
School staff Notify staff of student’s deficits and allow for extra time
Peers Teach peers no rough housing, to be careful on playground
Student Teach student to keep hands free in case of balance problems, take their time,
Family Allow extra time for morning and homework routines
Most Common Sensory/Perceptual Issues:
• OVERSTIMULATION!• Double Vision• Neglect / Inattention• Hypersensitivities
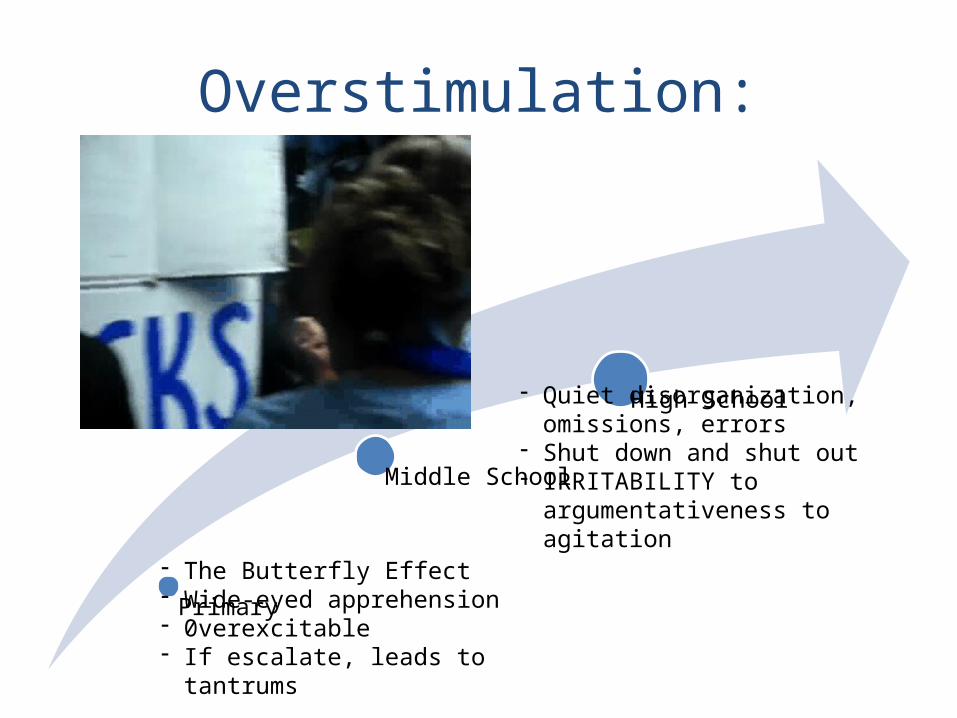
Overstimulation:
Primary
Middle School
High School
- The Butterfly Effect- Wide-eyed apprehension- 0verexcitable- If escalate, leads to tantrums
- Quiet disorganization, omissions, errors
- Shut down and shut out- IRRITABILITY to
argumentativeness to agitation
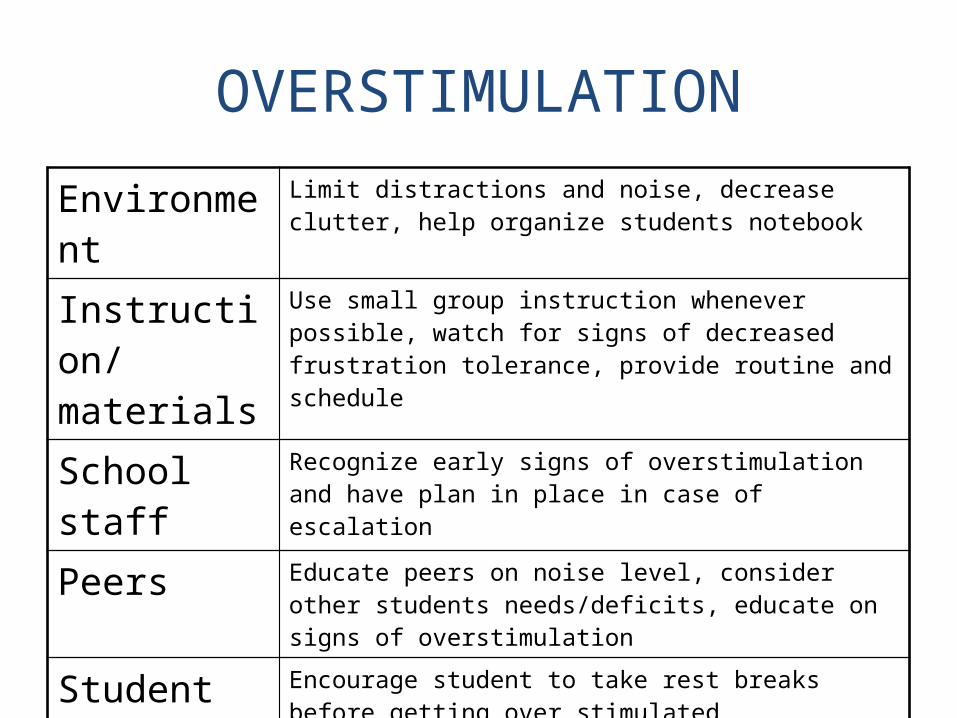
OVERSTIMULATION
Environment Limit distractions and noise, decrease clutter, help organize students notebook
Instruction/materials
Use small group instruction whenever possible, watch for signs of decreased frustration tolerance, provide routine and schedule
School staff Recognize early signs of overstimulation and have plan in place in case of escalation
Peers Educate peers on noise level, consider other students needs/deficits, educate on signs of overstimulation
Student Encourage student to take rest breaks before getting over stimulated
Family Explore medications
Double Vision
Primary
Middle School
High School
- Holding materials up to one eye- Head hovering over materials- Poor hand-eye coordination
- May or may not wear eye patch as prescribed
- Overreaching- Worn out- “lead with one eye”
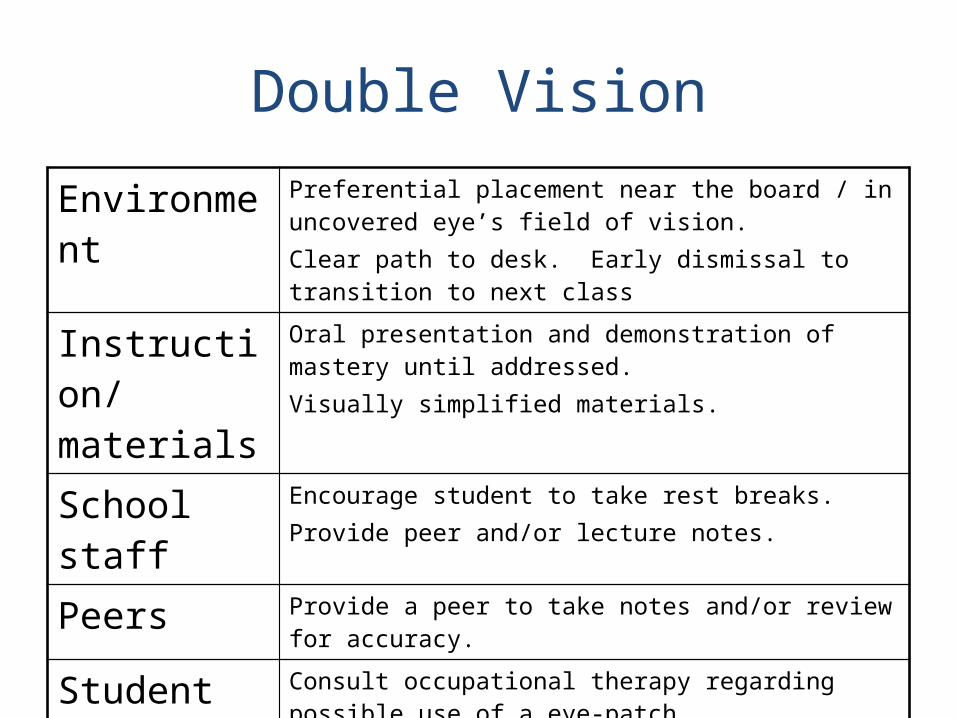
Double Vision
Environment Preferential placement near the board / in uncovered eye’s field of vision.Clear path to desk. Early dismissal to transition to next class
Instruction/materials
Oral presentation and demonstration of mastery until addressed. Visually simplified materials.
School staff Encourage student to take rest breaks. Provide peer and/or lecture notes.
Peers Provide a peer to take notes and/or review for accuracy.
Student Consult occupational therapy regarding possible use of a eye-patch.
Family Encourage referral to neuro-ophthalmology consultation.
Inattention / Neglect
Primary
Middle School
High School
- Loses things /takes a long time to find things
- Complains that others move things
- Runs into things on the left
- Miss information when reading!!
- Miss information from the left side of the classroom
- Can’t follow scantrons- Mix up math signs- Lose track of organization of
math problems
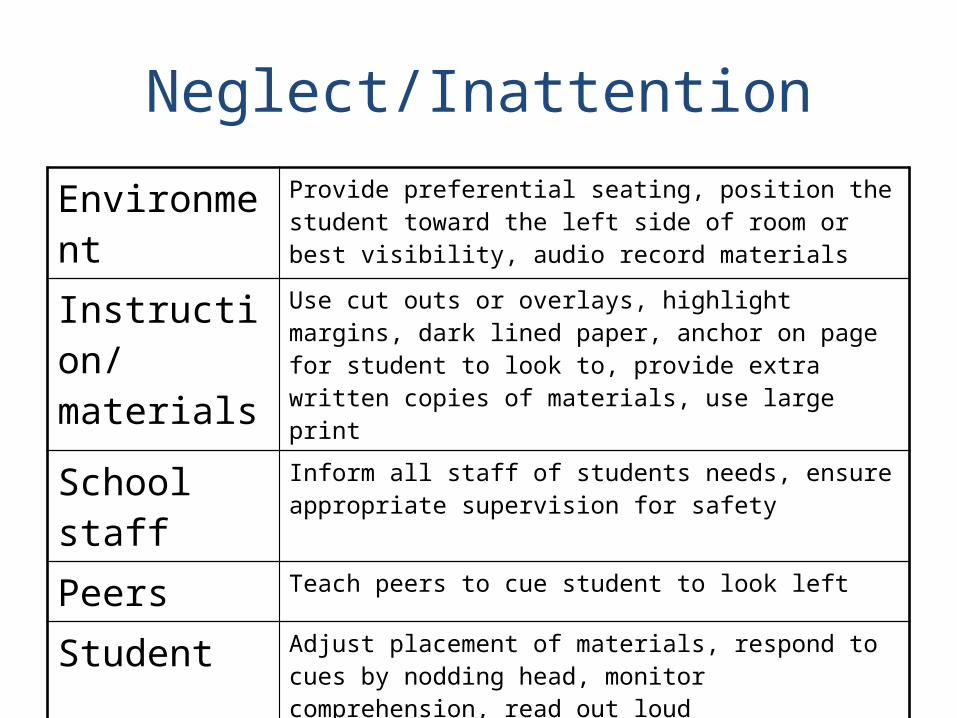
Neglect/Inattention
Environment Provide preferential seating, position the student toward the left side of room or best visibility, audio record materials
Instruction/materials
Use cut outs or overlays, highlight margins, dark lined paper, anchor on page for student to look to, provide extra written copies of materials, use large print
School staff Inform all staff of students needs, ensure appropriate supervision for safety
Peers Teach peers to cue student to look left
Student Adjust placement of materials, respond to cues by nodding head, monitor comprehension, read out loud
Family Ask the family what strategies are used at home that can be generalized to the classroom
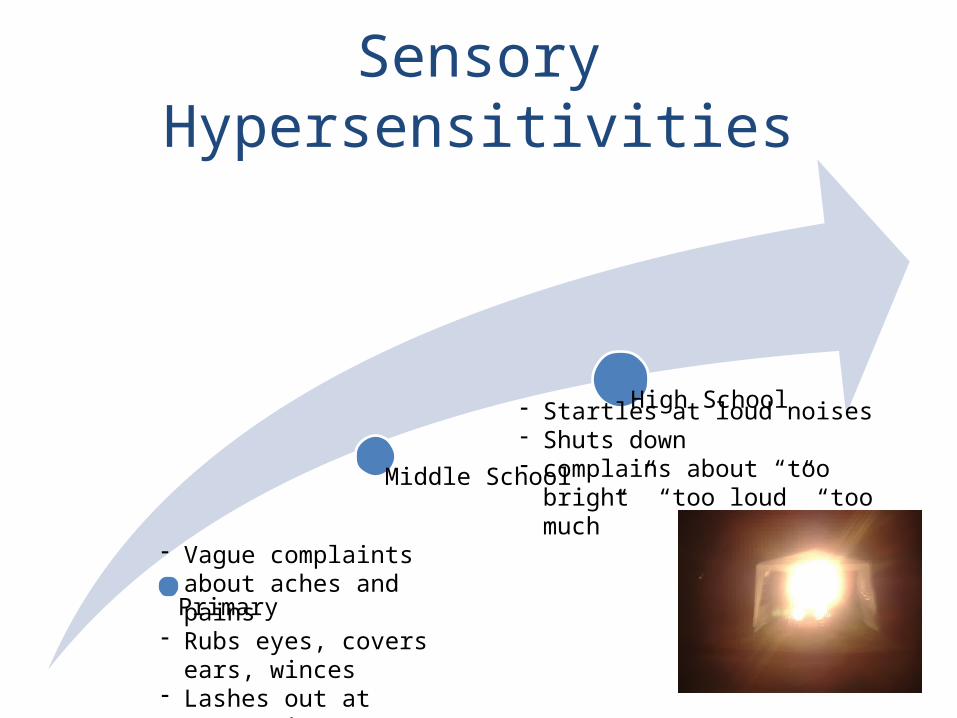
Sensory Hypersensitivities
Primary
Middle School
High School
- Vague complaints about aches and pains
- Rubs eyes, covers ears, winces
- Lashes out at energetic peers
- Dislikes being touched
- Startles at loud noises- Shuts down- complains about “too bright” “too
loud” “too much”
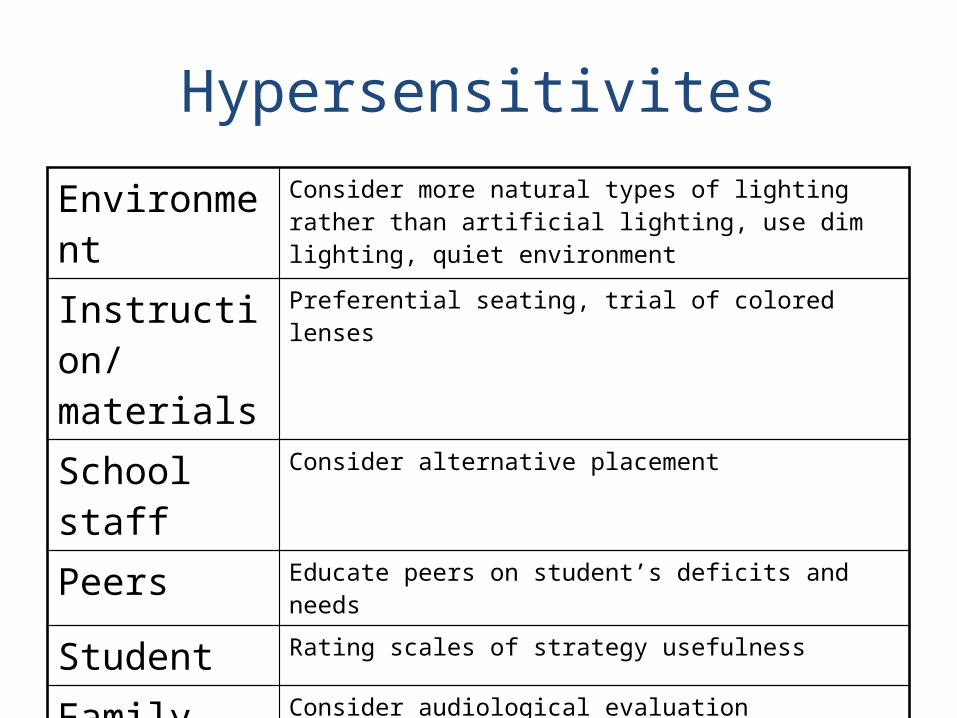
Hypersensitivites
Environment Consider more natural types of lighting rather than artificial lighting, use dim lighting, quiet environment
Instruction/materials
Preferential seating, trial of colored lenses
School staff Consider alternative placement
Peers Educate peers on student’s deficits and needs
Student Rating scales of strategy usefulness
Family Consider audiological evaluation
Most Common Cognitive-Communication Deficits:
• Slowed Processing Speed• Attention• Intolerance of Complexity• Memory• Reasoning and Problem-solving
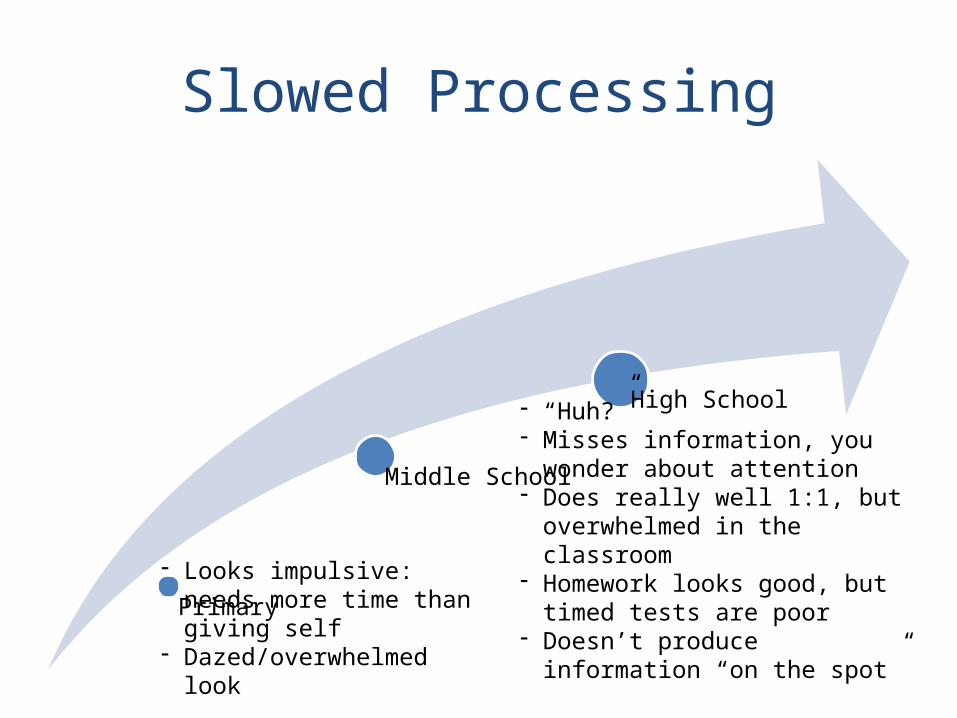
Slowed Processing
Primary
Middle School
High School
- Looks impulsive: needs more time than giving self
- Dazed/overwhelmed look
- “Huh?”- Misses information, you wonder
about attention- Does really well 1:1, but
overwhelmed in the classroom- Homework looks good, but timed
tests are poor- Doesn’t produce information “on
the spot”
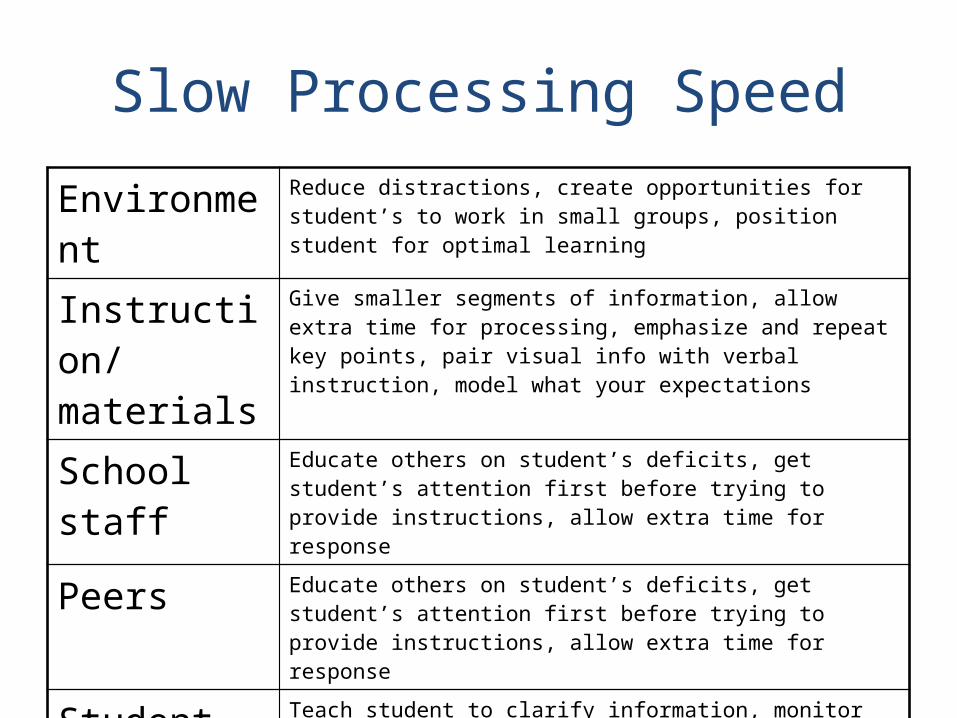
Slow Processing Speed
Environment Reduce distractions, create opportunities for student’s to work in small groups, position student for optimal learning
Instruction/materials
Give smaller segments of information, allow extra time for processing, emphasize and repeat key points, pair visual info with verbal instruction, model what your expectations
School staff Educate others on student’s deficits, get student’s attention first before trying to provide instructions, allow extra time for response
Peers Educate others on student’s deficits, get student’s attention first before trying to provide instructions, allow extra time for response
Student Teach student to clarify information, monitor comprehension, ask questions or give a signal when he/she doesn’t understand, watch others, examine sample
Family Educate others on student’s deficits, get student’s attention first before trying to provide instructions, allow extra time for response
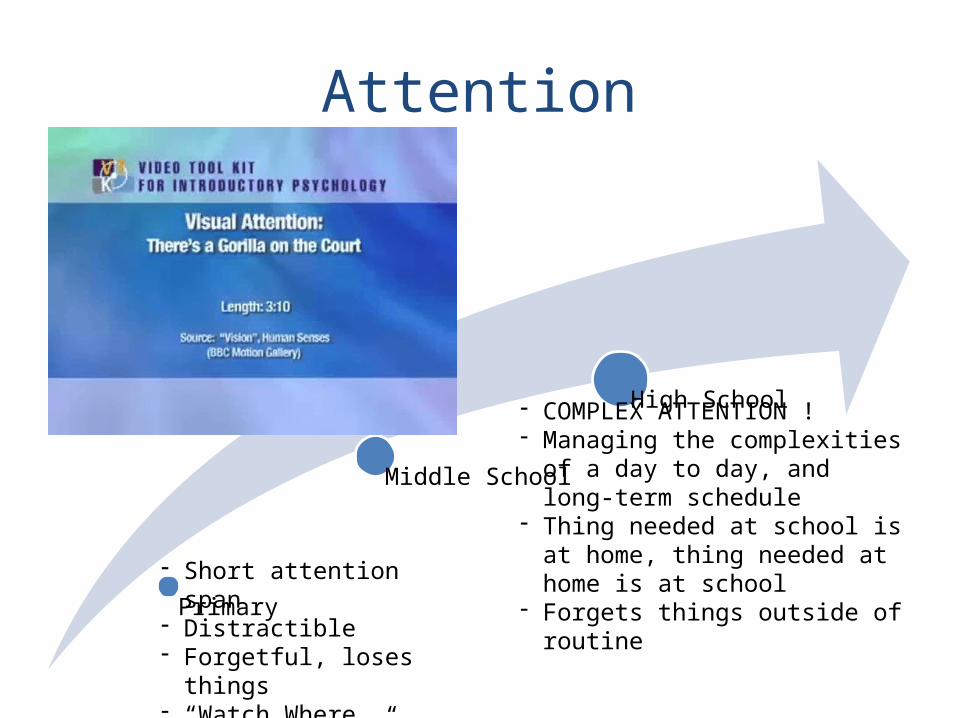
Attention
Primary
Middle School
High School
- Short attention span- Distractible- Forgetful, loses things- “Watch Where You’re
Going!”
- COMPLEX ATTENTION !- Managing the complexities of a
day to day, and long-term schedule
- Thing needed at school is at home, thing needed at home is at school
- Forgets things outside of routine
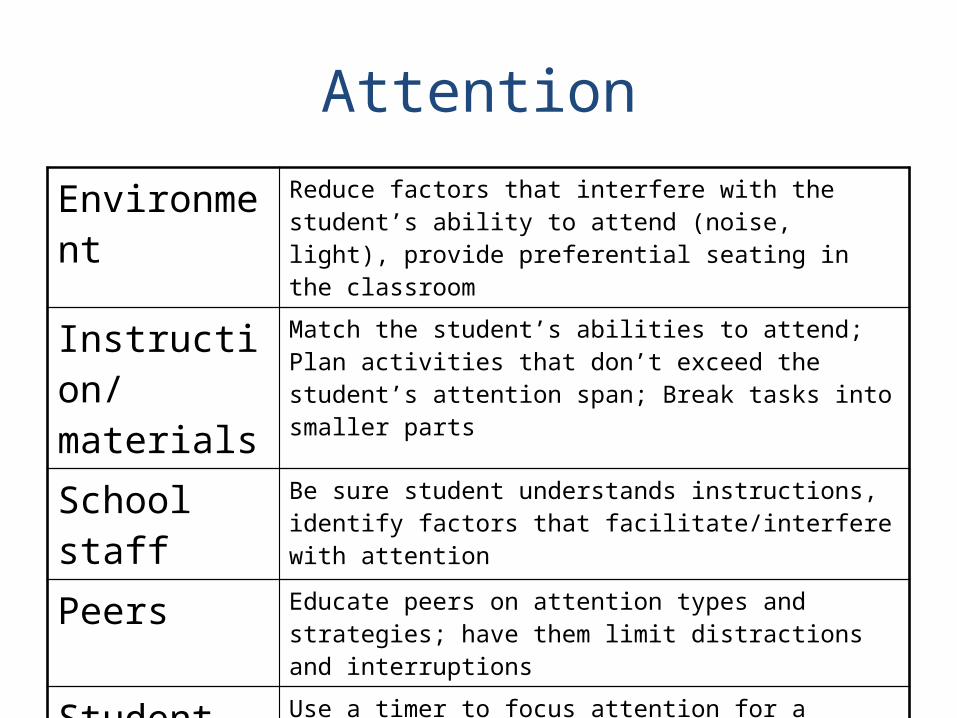
Attention
Environment Reduce factors that interfere with the student’s ability to attend (noise, light), provide preferential seating in the classroom
Instruction/materials
Match the student’s abilities to attend; Plan activities that don’t exceed the student’s attention span; Break tasks into smaller parts
School staff Be sure student understands instructions, identify factors that facilitate/interfere with attention
Peers Educate peers on attention types and strategies; have them limit distractions and interruptions
Student Use a timer to focus attention for a specific period of time, monitor attention to task, complete a pre-determined amount of work and then take a break; have student clarify information
Family Discover student’s interests, encourage good study habits
Complex attention
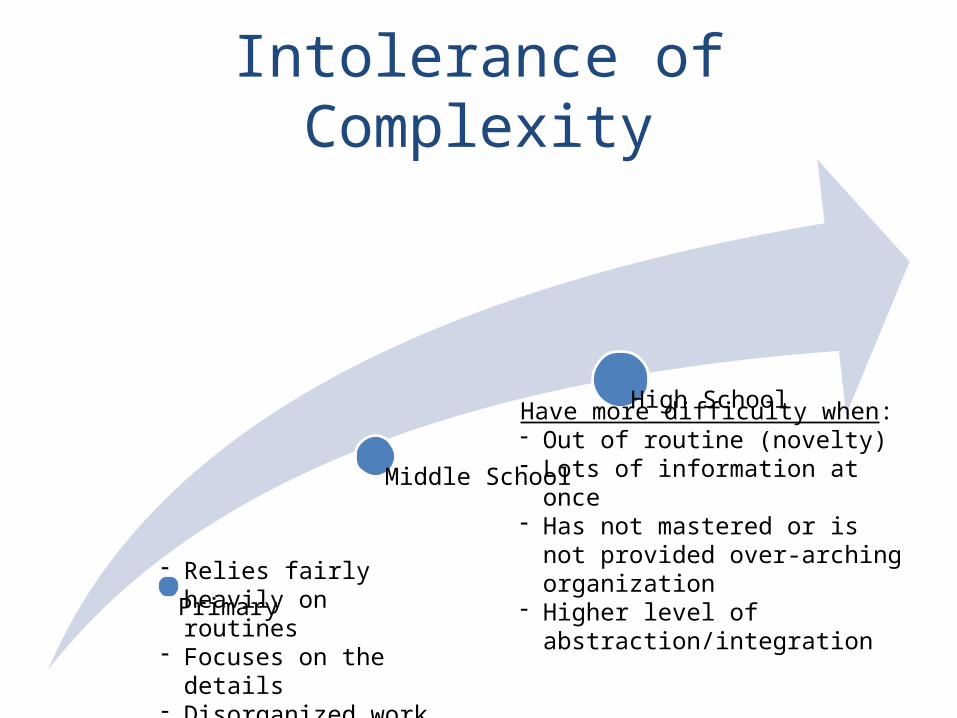
Intolerance of Complexity
Primary
Middle School
High School
- Relies fairly heavily on routines
- Focuses on the details- Disorganized work
Have more difficulty when:- Out of routine (novelty)- Lots of information at once- Has not mastered or is not
provided over-arching organization
- Higher level of abstraction/integration
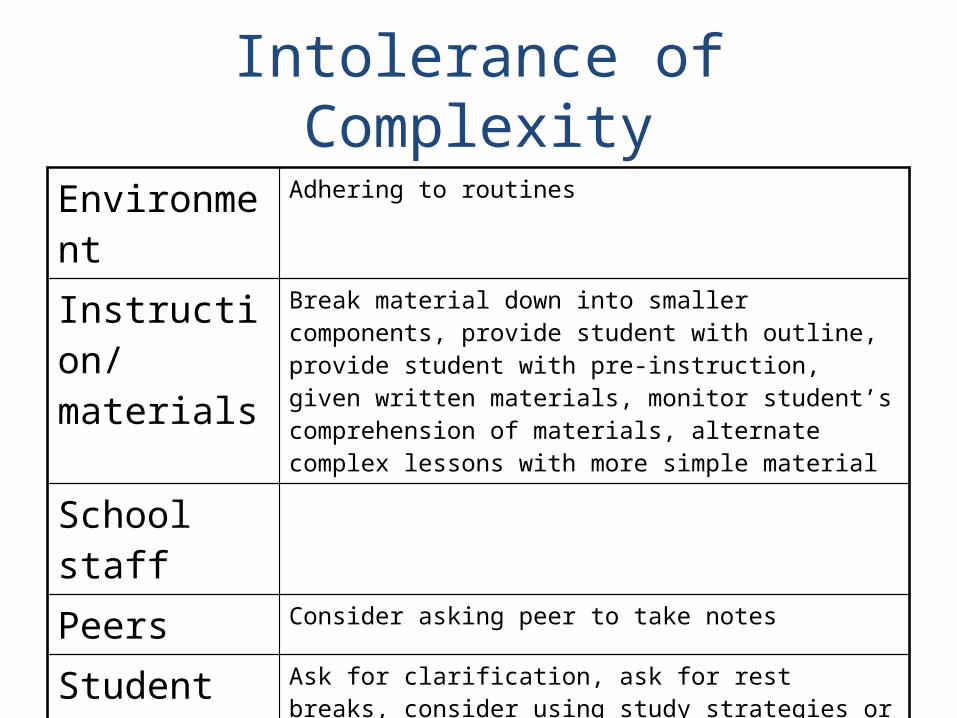
Intolerance of Complexity
Environment Adhering to routines
Instruction/materials
Break material down into smaller components, provide student with outline, provide student with pre-instruction, given written materials, monitor student’s comprehension of materials, alternate complex lessons with more simple material
School staff
Peers Consider asking peer to take notes
Student Ask for clarification, ask for rest breaks, consider using study strategies or alternative ways to organize/study, teach time management
Family Consider a tutor
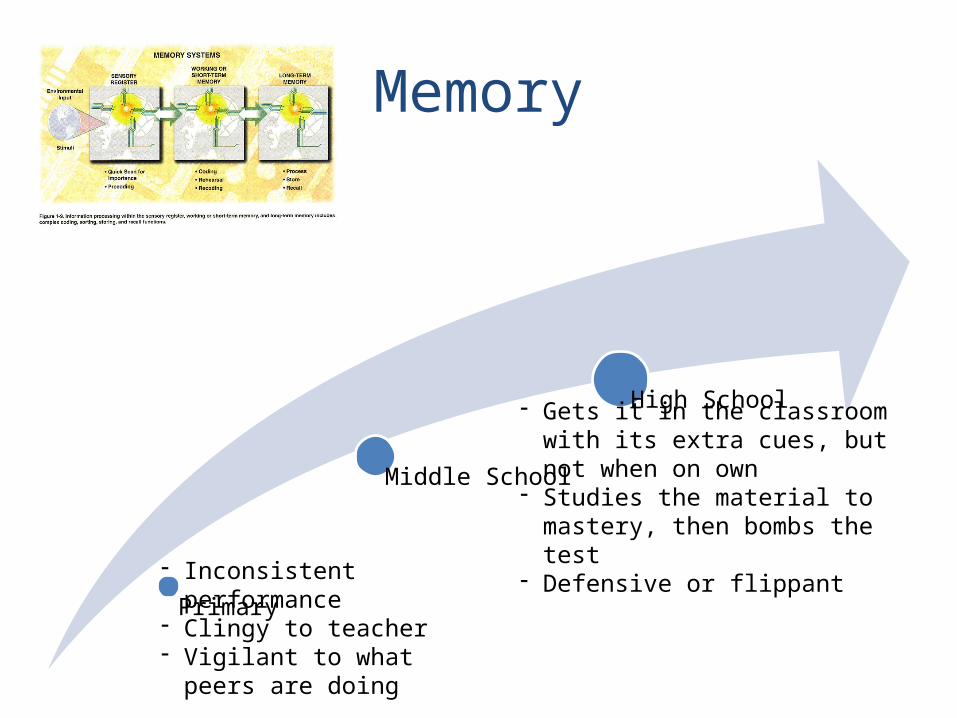
Memory
Primary
Middle School
High School
- Inconsistent performance- Clingy to teacher- Vigilant to what peers are
doing
- Gets it in the classroom with its extra cues, but not when on own
- Studies the material to mastery, then bombs the test
- Defensive or flippant
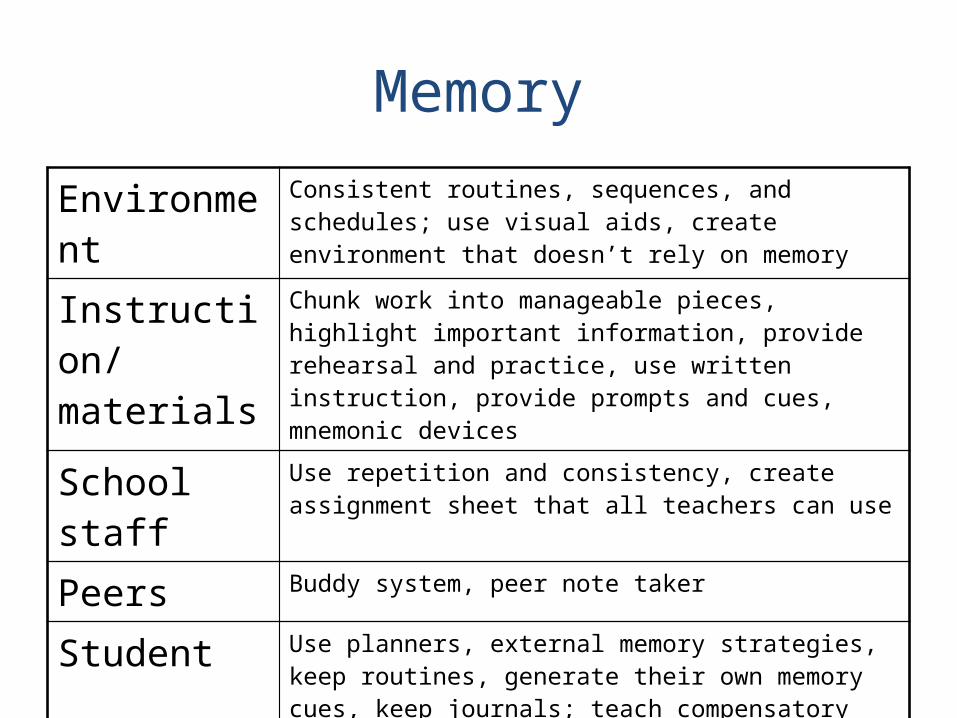
Memory
Environment Consistent routines, sequences, and schedules; use visual aids, create environment that doesn’t rely on memory
Instruction/materials
Chunk work into manageable pieces, highlight important information, provide rehearsal and practice, use written instruction, provide prompts and cues, mnemonic devices
School staff Use repetition and consistency, create assignment sheet that all teachers can use
Peers Buddy system, peer note taker
Student Use planners, external memory strategies, keep routines, generate their own memory cues, keep journals; teach compensatory strategies; awareness training
Family Generalize strategies from home to school and vice versa
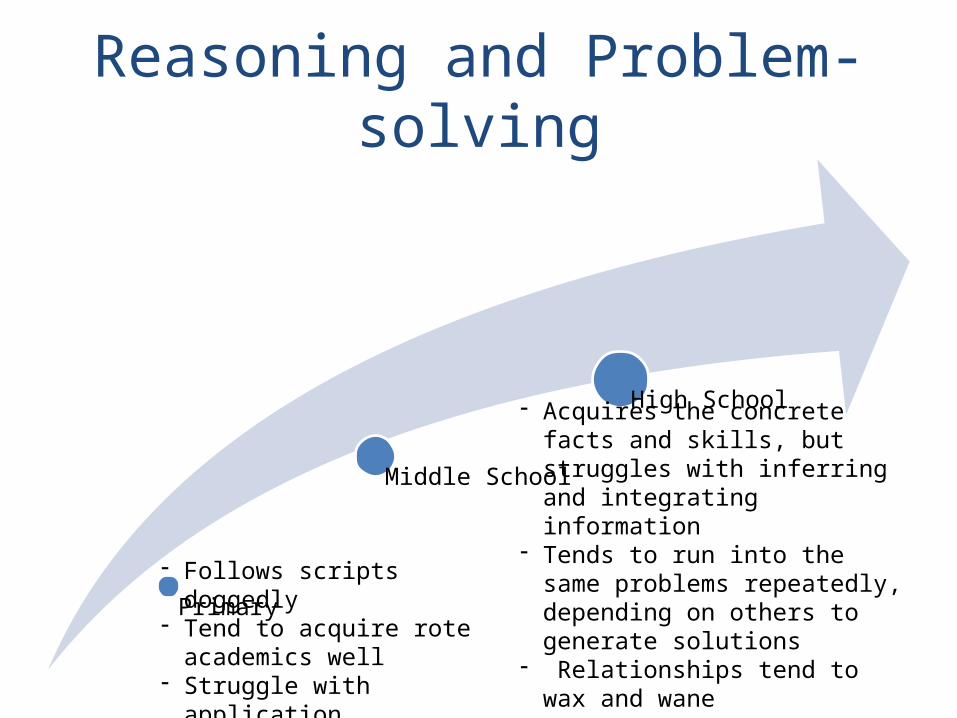
Reasoning and Problem-solving
Primary
Middle School
High School
- Follows scripts doggedly- Tend to acquire rote
academics well- Struggle with application
- Acquires the concrete facts and skills, but struggles with inferring and integrating information
- Tends to run into the same problems repeatedly, depending on others to generate solutions
- Relationships tend to wax and wane
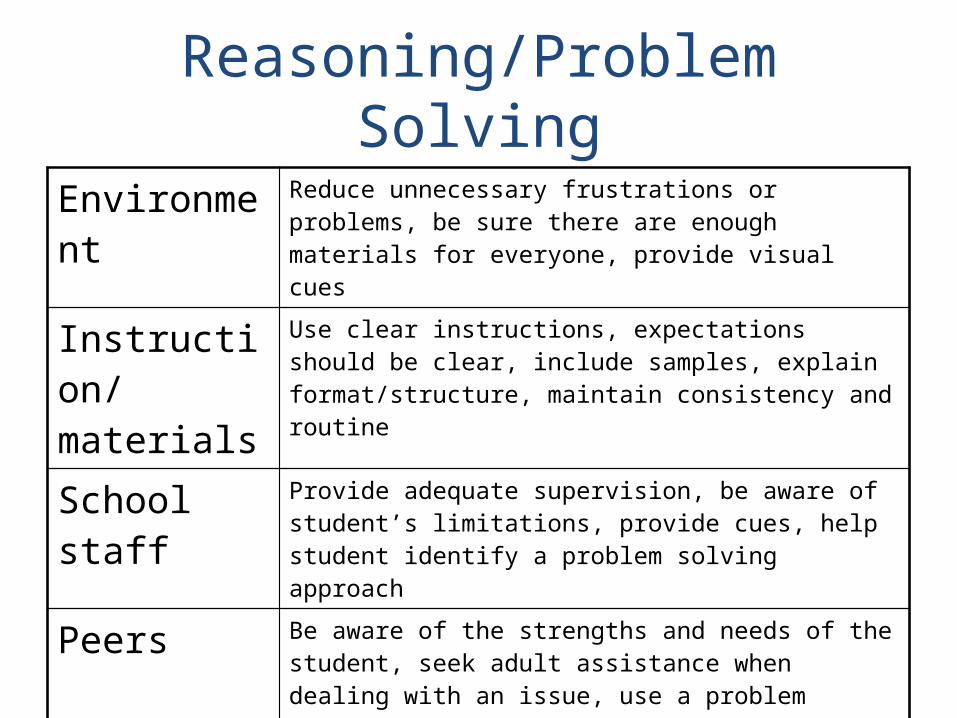
Reasoning/Problem Solving
Environment Reduce unnecessary frustrations or problems, be sure there are enough materials for everyone, provide visual cues
Instruction/materials
Use clear instructions, expectations should be clear, include samples, explain format/structure, maintain consistency and routine
School staff Provide adequate supervision, be aware of student’s limitations, provide cues, help student identify a problem solving approach
Peers Be aware of the strengths and needs of the student, seek adult assistance when dealing with an issue, use a problem solving model/approach
Student “Stop and think,” Seek adult assistance, be aware of environmental cues, listen
Family What strategies work at home, be consistent
Most Common Emotional-Behavioral Problems:
• Fragile Emotional Control• Impulsivity• Poor Awareness• Poor Social Judgment and Pragmatics
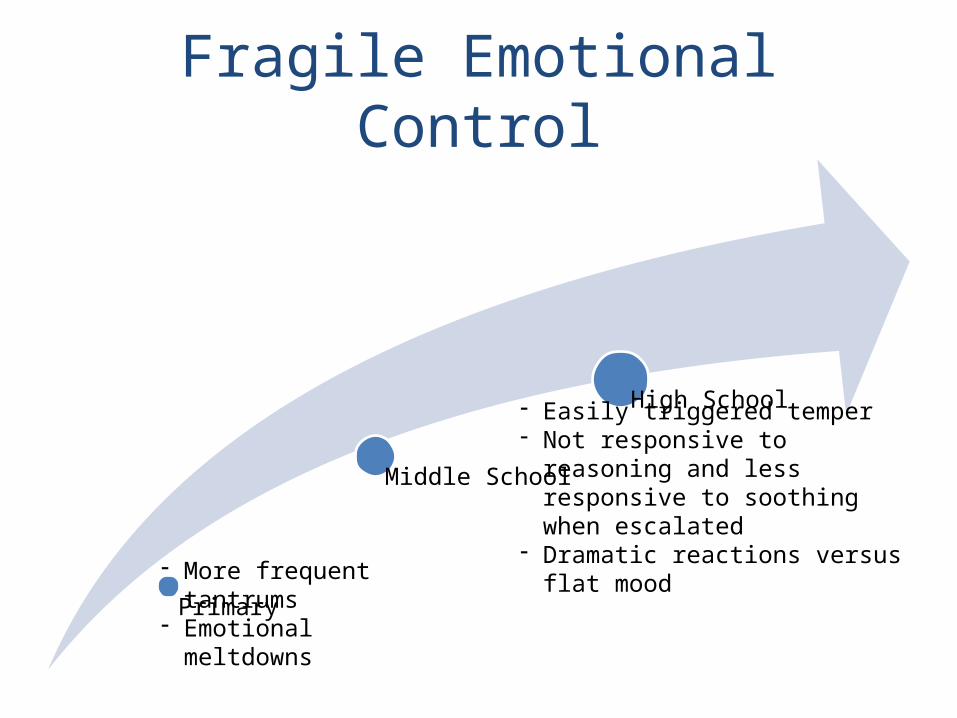
Fragile Emotional Control
Primary
Middle School
High School
- More frequent tantrums- Emotional meltdowns
- Easily triggered temper- Not responsive to reasoning and
less responsive to soothing when escalated
- Dramatic reactions versus flat mood
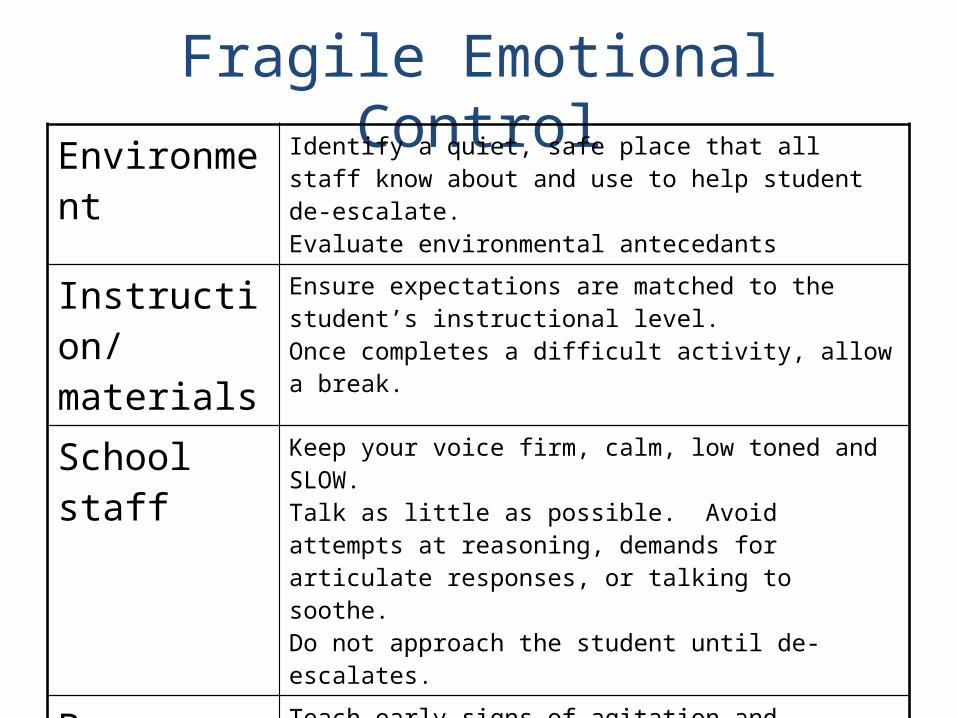
Fragile Emotional ControlEnvironment Identify a quiet, safe place that all staff know about and
use to help student de-escalate.Evaluate environmental antecedants
Instruction/materials
Ensure expectations are matched to the student’s instructional level.Once completes a difficult activity, allow a break.
School staff Keep your voice firm, calm, low toned and SLOW.Talk as little as possible. Avoid attempts at reasoning, demands for articulate responses, or talking to soothe.Do not approach the student until de-escalates.
Peers Teach early signs of agitation and appropriate response.Enforce intolerance of intentional provocation.
Student Teach routine of behaviors and consequences.Teach self-soothing strategies and reinforce use.Reward positive behavior, particularly ability to tolerate frustrations and disappointments.
Family Assess external events that may be having an impact on well-being. Collaborate on carry through at home.
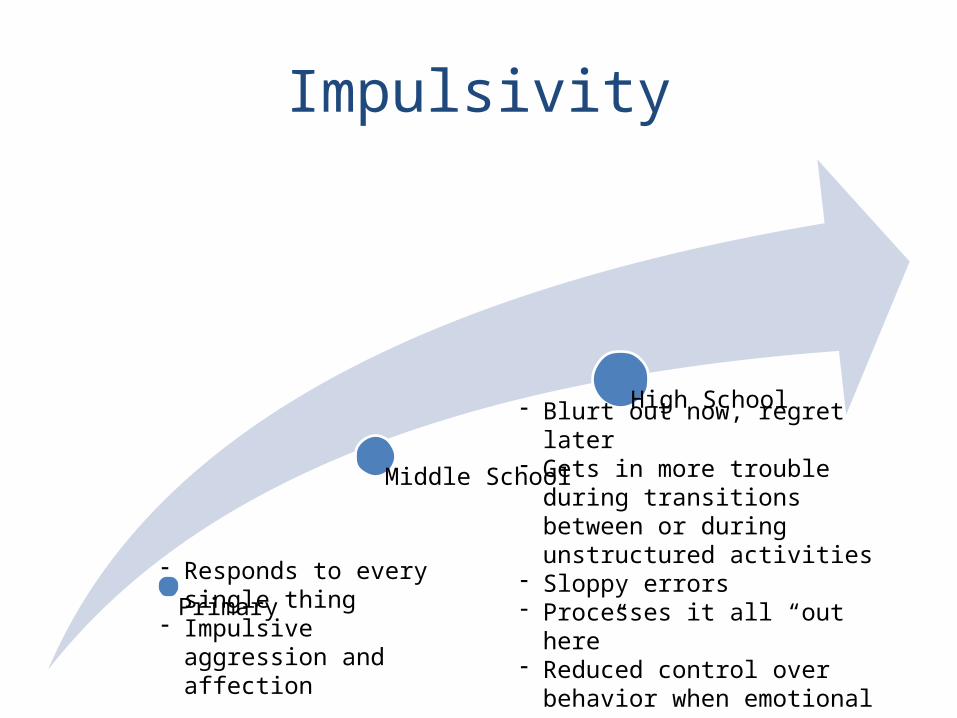
Impulsivity
Primary
Middle School
High School
- Responds to every single thing
- Impulsive aggression and affection
- Blurt out now, regret later- Gets in more trouble during
transitions between or during unstructured activities
- Sloppy errors- Processes it all “out here”- Reduced control over behavior
when emotional
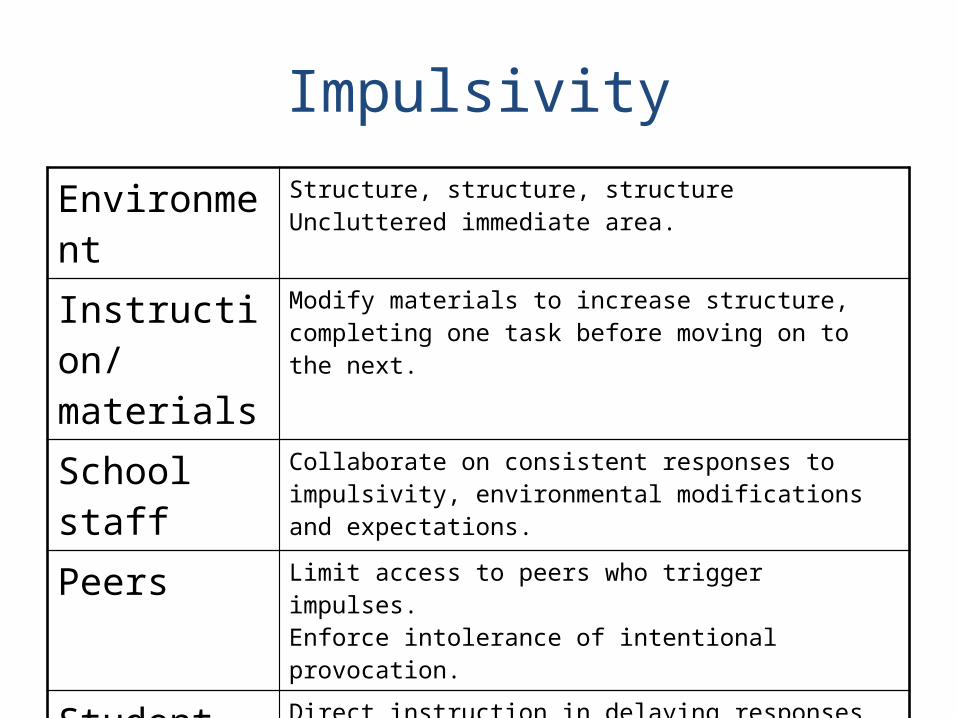
Impulsivity
Environment Structure, structure, structureUncluttered immediate area.
Instruction/materials
Modify materials to increase structure, completing one task before moving on to the next.
School staff Collaborate on consistent responses to impulsivity, environmental modifications and expectations.
Peers Limit access to peers who trigger impulses.Enforce intolerance of intentional provocation.
Student Direct instruction in delaying responses and reinforce use of this strategy across all staff.
Family Collaborate on consistent responses to impulsivity, environmental modifications and expectations.
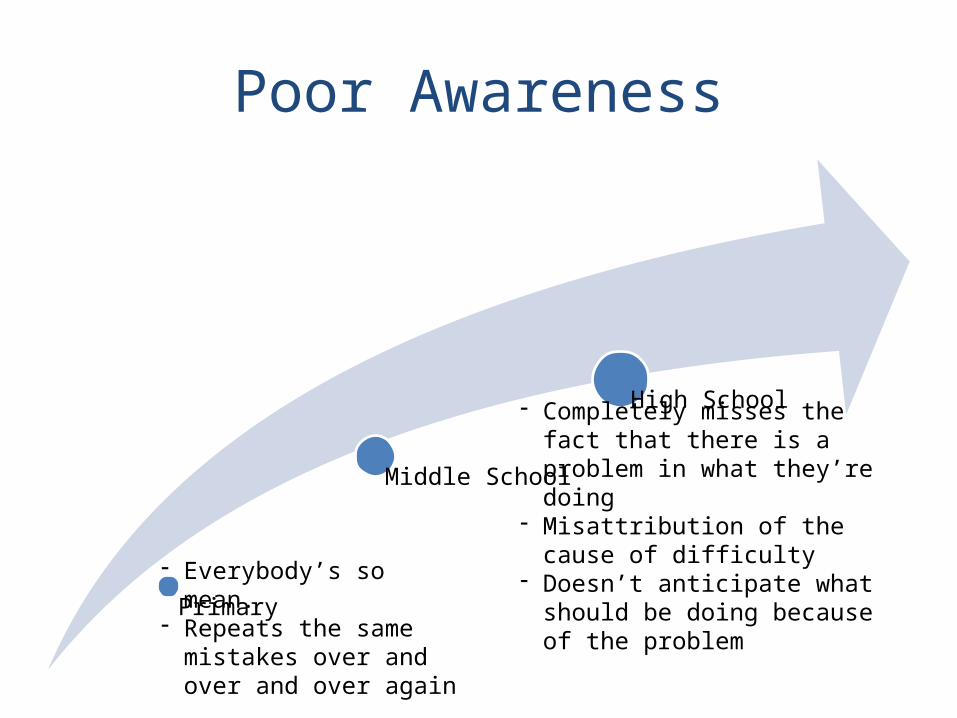
Poor Awareness
Primary
Middle School
High School
- Everybody’s so mean.- Repeats the same
mistakes over and over and over again
- Completely misses the fact that there is a problem in what they’re doing
- Misattribution of the cause of difficulty
- Doesn’t anticipate what should be doing because of the problem
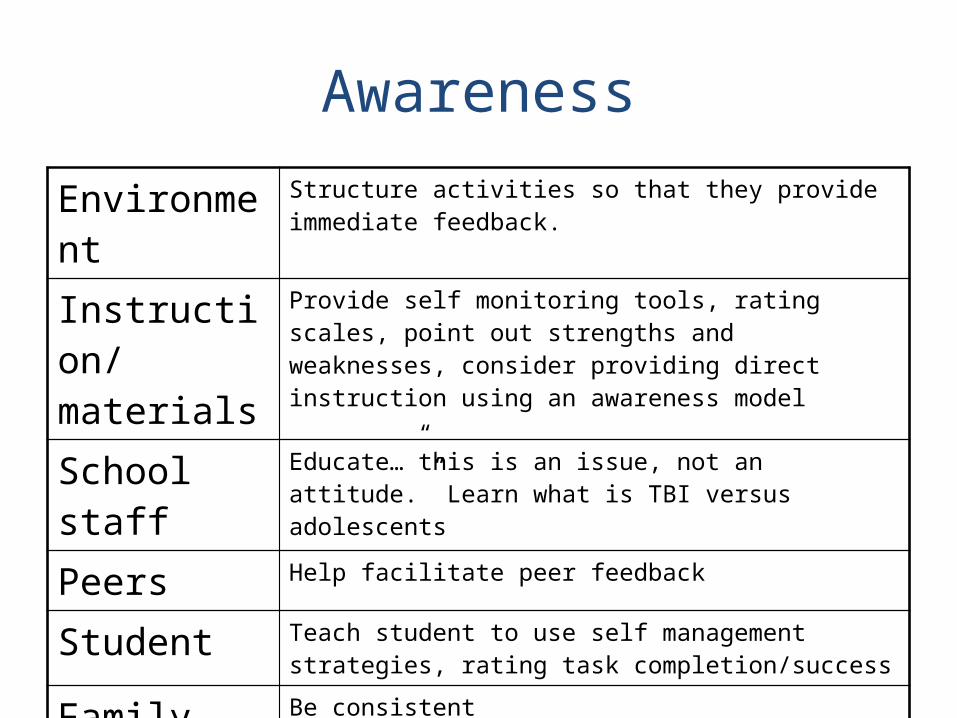
Awareness
Environment Structure activities so that they provide immediate feedback.
Instruction/materials
Provide self monitoring tools, rating scales, point out strengths and weaknesses, consider providing direct instruction using an awareness model
School staff Educate…”this is an issue, not an attitude.” Learn what is TBI versus adolescents
Peers Help facilitate peer feedback
Student Teach student to use self management strategies, rating task completion/success
Family Be consistent
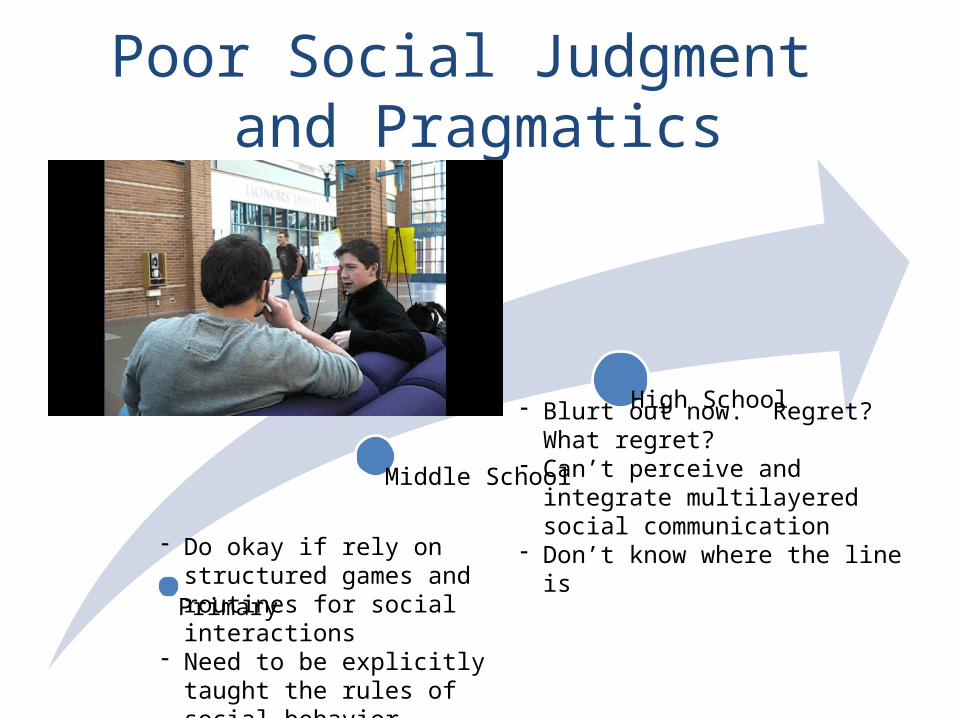
Poor Social Judgment and Pragmatics
Primary
Middle School
High School
- Do okay if rely on structured games and routines for social interactions
- Need to be explicitly taught the rules of social behavior
- Rely on social rules rigidly
- Blurt out now. Regret? What regret?
- Can’t perceive and integrate multilayered social communication
- Don’t know where the line is
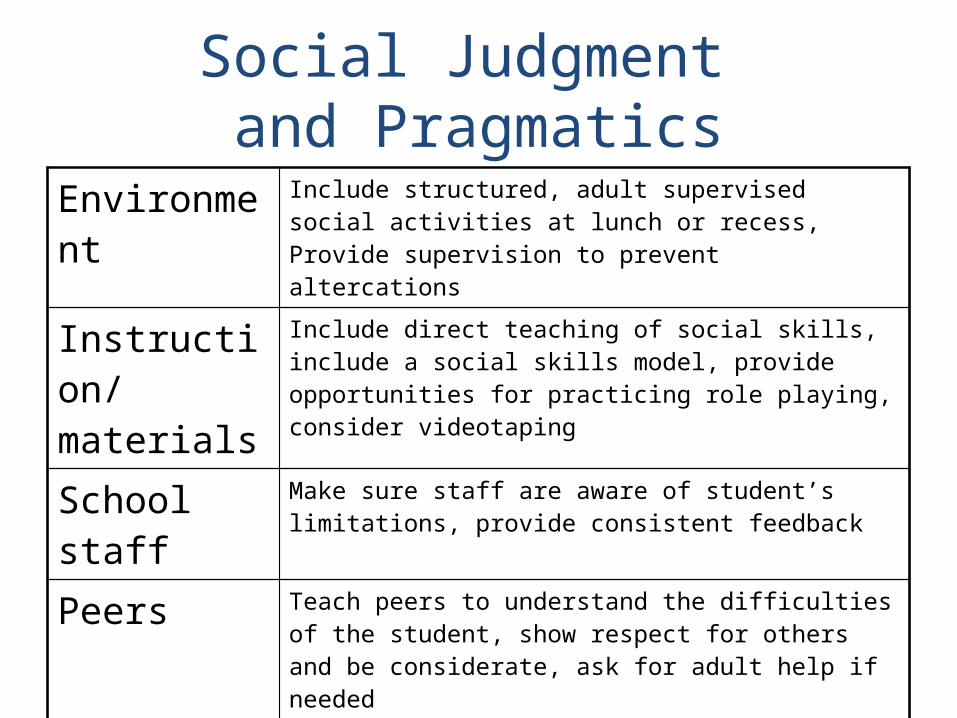
Social Judgment and Pragmatics
Environment Include structured, adult supervised social activities at lunch or recess, Provide supervision to prevent altercations
Instruction/materials
Include direct teaching of social skills, include a social skills model, provide opportunities for practicing role playing, consider videotaping
School staff Make sure staff are aware of student’s limitations, provide consistent feedback
Peers Teach peers to understand the difficulties of the student, show respect for others and be considerate, ask for adult help if needed
Student Pay attention to social cues, be aware of strengths and weaknesses, identify social rules in specific environments, consider others perspectives
Family Provide feedback to student, generalize strateiges
Review of Section 3:Interventions for Students with TBI• Identify the domains in which you can
intervene.• Identify how common physical, cognitive
and emotional/behavioral sequelae are expressed in the classroom.
• Identify several avenues of intervening to address the impact of sequelae on the student’s ability to benefit from the educational environment.
The Lost Kids
• If so many children have brain injuries, why can’t we find them in the schools?
Preview of Section 4:Advocacy and Resources
• Be able to define advocacy• Be able to identify barriers to advocacy• Be able to identify what you can do to advocate for the
students in your class with brain injury• Be able to identify strategies to empower parents to
advocate for themselves and their child• Identify resources for deepening your understanding of
brain injury• Identify resources for expanding your skills in facilitating
school re-entry after brain injury
Advocacy… what is it?
• "Advocacy" can mean many things, but in general, it refers to taking action. Advocacy simply involves speaking and acting on behalf of yourself or others.
Barriers to Advocacy
• Attitude• Limited training• Inexperience• Funding• Shortage of programs
What can you do?
• Understand and watch for signs and symptoms of brain injury
• Recognize when to refer and who to refer to• Obtain medical/educational records• Explore accommodations and interventions with
input from other professionals• Educate school staff and auxiliary staff• Educate student and his/her peers
Advocacy Cont.
• Consult with school psychologist or guidance counselor
• Consider altering your expectations of how this student can best learn
• Consider different teaching styles– Alternative placement, homebound services
• Think about transition services• Follow up and follow through• Consider your own continuing edcuation
Talking…
• Helps change people’s attitudes• Keeps everyone on the same page• Provides education• Flushes out myths versus facts• Provides opportunities for brainstorming• Allows for sharing and giving examples• Gives a chance to say thank you
Advocacy and Parents
• Communicate with family regularly• Set expectations for family as a member of
the team• Remember, when looking for an advocate,
many parents overlook the most obvious place …the school
• Keep in mind….they don’t speak your language…IEP, 504, “eval”
Parents…
“I need to be careful how I say this…it’s almost like it would’ve been better if the injury were severe enough that we would’ve had to have gotten help. With TBI, the moderate to mild, it’s invisible. People don’t see it and then people don’t get the help they need.”
~Parent
Resources, Who can You call?
• Family• School Psychologist• Resource Teacher• Guidance Counselor• Speech Therapist• Neuropsychologist• Hospital Case Manager• Peers and Friends
Educator Resources…at your fingertips
• Educating Educators about ABI– www.abieducation.com
• BIA NY Learnet– www.projectlearnet.org
• Brainline– www.brainline.org
• Project BRAIN– http://www.tndisability.org
• Brain Injury Navigator– www.binav.org
• TBI Educator– www.tbied.org
In the Library• An Educator’s Manual: What Educator’s Need to
Know about Students with Brain– Ron Savage and Gary Wolcott
• Parents as Educators and Partners– Marilyn Lash and Bob Cluett
• Making the IEP Process Work for Students with TBI– Ann Glang, McKay Moore Sohlberg, and Bonnis Todis
• Signs and Strategies for Educating Students with Brain Injuries– Marilyn Lash, Gary Wolcott, and Sue Pearson
Resources in South Carolina
• 4 counties house traveling libraries• Contact the following:
– In Charleston County– In Greenville County– In Horry County– In Richland County
Review of Section 4:Advocacy and Resources
• Be able to define advocacy• Be able to identify barriers to advocacy• Be able to identify what you can do to advocate for the
students in your class with brain injury.• Be able to identify strategies to empower parents to
advocate for themselves and their child• Identify resources for deepening your understanding of
brain injury• Identify resources for expanding your skills in facilitating
school re-entry after brain injury
Provide…
• An ear to listen• A safe environment• Clear structure and routine• Consistency• Immediate feedback and praise• Reinforcement• Cueing and modeling