scottish uveitis national managed clinical network ... treatment guideline... · scottish. uveitis...
TRANSCRIPT

Scottish
Uveitis National Managed Clinical Network
Treatment Guidelines
Uveitis NMCN Treatment Guidelines Revised September 2010
1

Introduction ..................................................................................................4
Uveitis Treatment Pathways.........................................................................5
When to immunosuppress ?.........................................................................9
Which immunosuppressive agent to use ?...................................................9
Immunosuppressive Therapy .....................................................................12
Prednisolone.....................................................................................................13
Azathioprine......................................................................................................15
Methotrexate.....................................................................................................17
Mycophenolate mofetil......................................................................................19
Ciclosporin........................................................................................................21
Tacrolimus ........................................................................................................23
Alkylating Agents........................................................................................25
Cyclophosphamide ...........................................................................................25
Biological therapies ....................................................................................28
Tumour necrosis factor (TNF) alpha inhibitors..................................................29
Adalimumab......................................................................................................30
Infliximab ..........................................................................................................33
Interferon α .......................................................................................................36
Daclizumab.......................................................................................................40
Campath (Alemtuzumab)..................................................................................43
Uveitis NMCN Treatment Guidelines Revised September 2010
2

Rituximab..........................................................................................................46
Anakinra ...........................................................................................................49
Other biological therapies .................................................................................51
Summary of use of second line and biologic agents.........................................52
Combination Therapy.................................................................................54
Appendices ................................................................................................55
Appendix 1: Posterior Uveitis requiring early immunosuppressive therapy ......55
Appendix 2: Treatment of Inflammatory choroidal neovascularization (CNV)...58
Appendix 3: Management of uveitis-associated glaucoma...............................60
Appendix 4: Management of uveitis in the perioperative period .......................61
Appendix 5: Immunosuppression during pregnancy.........................................62
Appendix 6: Paediatric guidelines.....................................................................68
Appendix 7: Guidelines for Screening for Uveitis in Juvenile Idiopathic Arthritis
(JIA) ..................................................................................................................76
Appendix 8: Membership of NMCN treatment guideline development group and
stakeholders group ...........................................................................................80
Appendix 9: Evidence Base..............................................................................83
Uveitis NMCN Treatment Guidelines Revised September 2010
3

Preface
Ophthalmologists within Scotland with an interest in uveitis met in January 2005 to consider
how the care of patients with sight-threatening uveitis could be delivered in a more uniform
manner. A decision was made to develop a Scottish Uveitis Network involving clinicians and
the Uveitis Information Group, a United Kingdom based patient organisation. Since then, the
group has developed as a National Managed Clinical Network, under the auspices of
National Services Division, NHS National Services Scotland. As part of its remit it has set
out to develop guidelines for the management of uveitis.
The aim of this document is to help guide ophthalmologists as to which patients require
referral to a uveitis specialist and aid in the prescription of immunosuppressive therapy for
ocular inflammatory disease.
This document does not replace the advice given by the British National Formularly, nor the advice given by manufacturers.
Introduction
Despite the relatively limited evidence for the efficacy of immunosuppressive treatment in
uveitis(1) it is generally accepted that delay in referral to a uveitis specialist, delay in
commencement of immunosuppression or inadequate immunosuppression all result in
poorer visual prognosis of ocular inflammatory disease (2)
‘Early on you regret too little, late on you regret too much’. (Andy Rees).
Central to the management of ocular inflammatory disease and the use of systemic
immunosuppression is the patient’s understanding of the disease and its treatment. All
these therapies have potentially life-threatening complications and by educating patients
about their treatment and re-enforcing the importance of regular blood tests where
appropriate, hopefully if complications do arise then they will be identified early.
All immunomodulatory drugs used in ocular inflammatory disease were initially developed
for use in other medical specialities, either as chemotherapeutic agents or for
immunosuppression in transplant medicine. Although all these medications are licensed for
other indications none are currently licensed for ocular inflammatory disease and are used
at the discretion of the prescribing consultant. It is important that the patient is aware and
accepting of this prescribing situation.
Uveitis NMCN Treatment Guidelines Revised September 2010
4

Immunomodulatory drugs have different side effect profiles and so the treatment regime
needs to planned for each patient aiming to produce a treatment regimen that is well
tolerated and is able to to suppress the ocular inflammation.
The document is intended as a guideline rather than a set of protocols. The aim is to assist
the ophthalmologist in making decisions about when to initiate treatment and which type of
treatment is appropriate. It is expected that ophthalmologists will refer on to a uveitis
specialist or ask for assistance from physician colleagues if they do not feel competent to
move on to the appropriate step in the treatment pathway.
Although the guidelines are primarily intended for the use of ophthalmologists, they may be
found helpful by some patients, general practitioners and optometrists in gaining a greater
understanding of uveitis management.
The majority of patients with uveitis will have acute anterior uveitis which settles promptly
with topical treatment. However, the guidelines appropriately cover in greater detail the
minority who require systemic therapy and who generally have more sight threatening
disease.
These guidelines do not apply to infectious uveitis, which should always be considered,
along with malignancy, in patients presenting with uveitis.
In unilateral disease intra-orbital or intra-vitreal steroid may be considered as an alternative
to systemic steroids.
The points emphasised in the treatment pathways such as macular oedema, retinal
vasculitis and steroid dose should be considered ‘red flags’ highlighting indicators of sight
threatening uveitis and of systemic complications of therapy.
Uveitis Treatment Pathways
The following flow diagrams aim to simplify and demystify the treatment of uveitis. By
providing a clear route for treatment we would hope to identify those patients with sight-
threatening uveitis at any earlier stage. These pathways are intended for use by
ophthalmologists involved in the management of patients with uveitis. This will allow prompt,
appropriate referral to a uveitis specialist for consideration of systemic immunosuppression.
These pathways are not applicable to infectious uveitis
Uveitis NMCN Treatment Guidelines Revised September 2010
5

.
Anterior Uveitis
No
Posterior synechiae
Systemic and topical steroids
Topical mydriatic
Yes No
Topical steroid Topical mydriatic
Try staged mydriasis. If fails
then subconjunctival
steroids and Mydricaine.
Macular oedema
Yes
Taper therapy
Resolving?
No Yes
Uveitis NMCN Treatment Guidelines Revised September 2010
6

Uveitis NMCN Treatment Guidelines Revised September 2010
7
Intermediate Uveitis
Macular oedema
No Yes
Vitritis causing reduced vision Systemic
steroids
No
Intra-orbital or
intravitreal steroids
Topical steroids
Observation only

Posterior/Panuveitis
Yes
Macular oedema
Non-occlusive
Vitritis causing reduced vision
Occlusive
Yes
No Systemic steroids
Retinal vasculitis
No
Observation may be appropriate
Central
If observation not appropriate
Peripheral No
Uveitis NMCN Treatment Guidelines Revised September 2010
8

When to immunosuppress ?
Which immunosuppressive agent to use ?
Immunosuppressive therapy should be considered in the following situations:
• All patients requiring chronic steroid therapy greater than 7.5mg a day (osteoporosis
guideline) should be considered for immunosuppressive therapy to allow reduction in
the steroid therapy.
• Most patients requiring systemic steroid therapy who relapse on steroid withdrawal
will require systemic immunosupression to reduce long-term steroid exposure.
• Early indications for immunosuppression would be ineffect of prednisolone despite
adequate dosing.
• Reactivation while reducing the steroid therapy usually requires an increase in the
prednisolone dosage to ensure rapid control of the disease.
• Immunosuppression is recommended at the outset in a number of inflammatory eye
diseases due to the chronicity and potentially poor prognosis that these conditions
have if untreated.
• Patients requiring ongoing systemic steroid therapy do so because they have
disease that is either steroid-dependent, steroid-resistant or relapsing disease.
• When starting immunosuppression it is important to determine whether the patient
requires a steroid sparing agent or an agent to induce remission of disease as
agents differ in their ability to induce disease remission.
Uveitis NMCN Treatment Guidelines Revised September 2010
9

Summary of side effect profiles
Immunosuppressive agent Pred AZA MTX MMF CSA TAC CphosCirculatory system Hypertension ● ● ● Hypercholesterolaemia ● ● ● Heart failure ● Atherosclerosis ● ● ● Cardiomyopathy ● Digestive System ● ● ● ● ● ● Liver dysfunction ● ● ● ● ● ● Gum hyperplasia ● Endocrine system Diabetes ● ● ● Adrenal suppression ● Integumentary system Hirsutism ● Immune system Infection ● ● ● ● ● ● ● Bone marrow ● ● ● ● ● ● Musculoskeletal system Osteoporosis ● Nervous system Mood disorder
●
Tremor ● ● Reproductive system Infertility ● Teratogenic
● ● ●
Respiratory system ● Urinary system
Renal impairment ● ● Cystitis ● Risk of malignancy ●
Uveitis NMCN Treatment Guidelines Revised September 2010
10
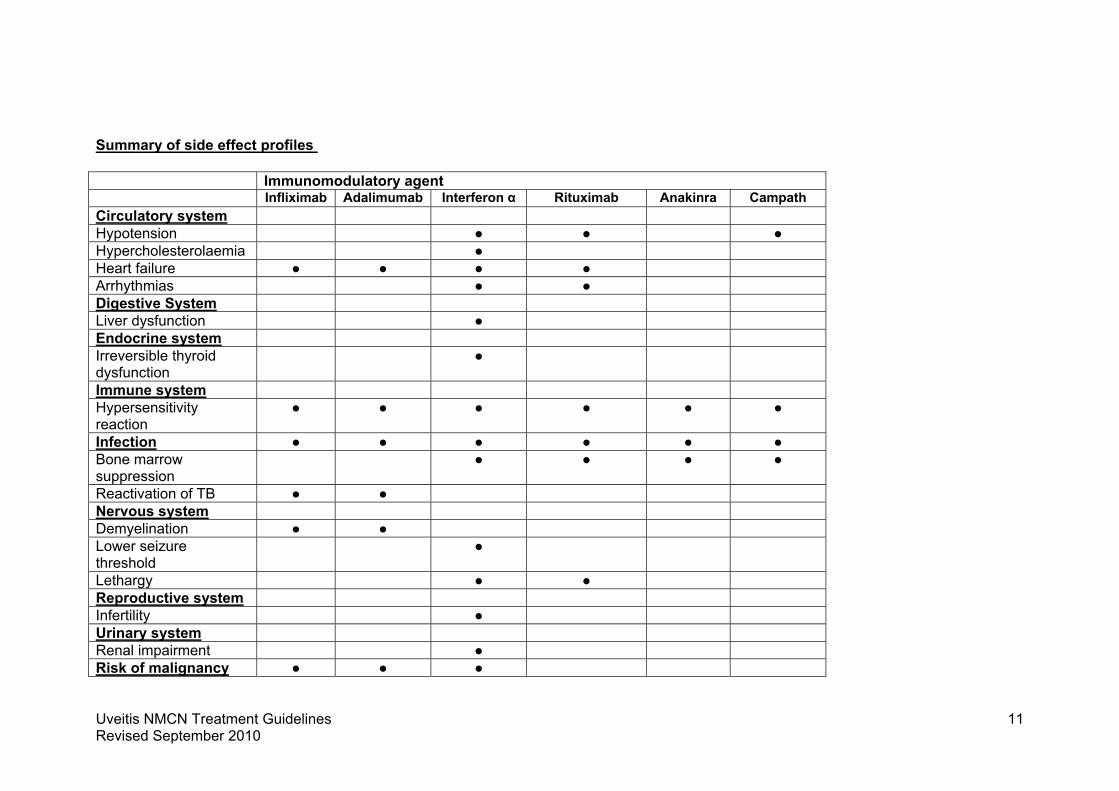
Summary of side effect profiles Immunomodulatory agent Infliximab Adalimumab Interferon α Rituximab Anakinra Campath Circulatory system Hypotension ● ● ● Hypercholesterolaemia ● Heart failure ● ● ● ● Arrhythmias ● ● Digestive System Liver dysfunction ● Endocrine system Irreversible thyroid dysfunction
●
Immune system Hypersensitivity reaction
● ● ● ● ● ●
Infection ● ● ● ● ● ● Bone marrow suppression
● ● ● ●
Reactivation of TB ● ● Nervous system Demyelination ● ● Lower seizure threshold
●
Lethargy ● ● Reproductive system Infertility ● Urinary system Renal impairment ● Risk of malignancy ● ● ●
Uveitis NMCN Treatment Guidelines Revised September 2010
11
Immunosuppressive Therapy
• Immunosuppressive therapy may be effective in the longer term management of
inflammatory eye disease for some patients. The aim of therapy is to allow a
reduction in the steroid dosage while maintaining disease control. Most drugs are
well tolerated but all carry a small risk of severe side effects which may be
potentially life-threatening.
• As most immunosuppressive drugs take several weeks to be effective, reduction of
the oral prednisolone, even in patients with controlled ocular inflammation may need
to be deferred for several weeks after commencement of the immunosuppressive
agent.
• In active disease, high dose prednisolone is often required at the same time as
commencing immunosuppressive therapy.
• Pregnancy and breast feeding are relatively contraindicated while on
immunosuppressive therapy.
• It is important to ensure adequate contraception being used. See appendix for
teratogic risks.
• To minimize the risk of skin cancer, exposure to sunlight and UV light should be
limited by wearing protective clothing and using sunscreen with a high protection
factor.
• Once a treatment plan is agreed this should be actioned as promptly as possible.
• If an agent is not effective, provided an adequate period of treatment has been
adhered to, then there should not be unnecessary delay ( max 2 Weeks) in either
switching or adding further therapy.
• When a decision is made to commence biologic therapies, treatment should begin
within 2 weeks of that decision.
This document does not replace the advice given by the British National Formularly, nor the advice given my manufacturers.
Uveitis NMCN Treatment Guidelines Revised September 2010
12

Prednisolone
Indications
Corticosteroids are the initial mainstay of treatment in inflammatory eye disease. Almost all
patients with sight-threatening uveitis will require systemic steroids at some point.
Systemic steroids are effective in the short and longer term management of inflammatory
eye disease. They are usually well tolerated, but do have a number of side-effects, most of
which are predictable .
What to do
• Consult BNF.
• Ensure no potential interaction with other medications.
• Check baseline U+E, LFTs, FBC, serum glucose, urinalysis and blood pressure.
• Consider what is the most appropriate route of administration (Steroids may be
administered topically, intra-orbitally, intra-vitreally or systemically).
• Initial treatment may depend on consultant and patient preference.
• Many authors would advocate initial dosing of prednisolone at 1mg/kg, however it is
our experience that a starting dose between 40mg and 60mg is usually required for
patients with uveitis, depending on severity and type of uveitis.
• If rapid disease control is required then methylprednisolone may be given at a dose
of 1g pulses per day over 3 consecutive days. This would be followed by high-dose
oral prednisolone.
• High dose oral steroid therapy does not increase the risk of ulcer disease(3,4) and
therefore the routine use of proton pump inhibitors (PPI) or histamine H2 blockers is
not necessary. However many patients complain of dyspepsia when commenced on
steroids and PPIs or H2 blockers may have a role in these patients. Patients should
be started on a PPI if they are also taking non-steroidal anti-inflammatory drugs
(NSAIDS) as this combination of therapy has been associated with a fourfold
increased risk of gastric ulceration.(4)
Uveitis NMCN Treatment Guidelines Revised September 2010
13

• Bone densiometry should be considered for any patient on any dose of oral
prednisolone for longer than three months or where the patient is likely to require
prednisolone for at least three months due to the risk of osteoporosis. The college of
physicians guidelines are summarized on the following website
http://www.rcplondon.ac.uk/pubs/books/glucocorticoid/
• Patients on corticosteroid for longer than 3 weeks, treatment must not be stopped
abruptly. Adrenal suppression can last for a year or more after stopping treatment
and the patient must mention the course of corticosteroid when receiving treatment
for any illness or injury
• Unless patients have had chickenpox, patients receiving oral or parenteral
corticosteroids should be regarded as being at risk of severe chickenpox.
Manifestations of fulminant illness include pneumonia, hepatitis and disseminated
intravascular coagulation; rash is not necessarily a prominent feature.
Passive immunisation with varicella–zoster immunoglobulin is needed for exposed
non-immune patients receiving systemic corticosteroids or for those who have used
them within the previous 3 months. Confirmed chickenpox warrants specialist care
and urgent treatment. Corticosteroids should not be stopped and dosage may need
to be increased.
• Mood and behaviour changes. Corticosteroid treatment, especially with high doses,
can alter mood and behaviour early in treatment—the patient can become confused,
irritable and suffer from delusion and suicidal thoughts. These effects can also occur
when corticosteroid treatment is being withdrawn. Medical advice should be sought if
worrying psychological changes occur.
• Steroid Treament Cards should be issued to all patients.
Side Effects
Side effects include acne, atherosclerosis, avascular necrosis of femoral head, cataract,
delay in pubertal growth, diabetes mellitus (up to 30%)(5), dyslipidemia (up to 30%)(6,7), heart
failure, hypertension (up to 85%) (6), infection, osteporosis, raised intraocular pressure
(IOP), serious psychosis (up to 5%) (8,9), sleep disturbance.
Uveitis NMCN Treatment Guidelines Revised September 2010
14

Antimetabolites
Azathioprine
Indications
Azathioprine may be used as a steroid sparing agent.
Evidence in Inflammatory Eye Disease
• A recently published retrospective cohort study found 69% of patients with
intermediate uveitis, 44% of patients with posterior or panuveitis and 24% of patients
with anterior uveitis patients had control of their ocular inflammation within 6 months
of treatment with azathioprine(10).
• The only randomized, placebo-controlled, double-blind trial of azathioprine was in
patients with Behcet disease. This trial found azathioprine to be effective in the
treatment of chronic uveitis and in reducing incidence of second eye involvement
when used in combination with prednisolone(11).
• Azathioprine has also been shown to provide effective long-term control of uveitis
associated with Behcet disease (12,13) but newer drugs are likely to be more effective.
See section on interferon alpha and tumour necrosis factor alpha inhibitors.
• There are a number of case series illustrating the efficacy of azathioprine in the
treatment of chronic uveitis in patients with eye disease (13,14,15).
• Azathioprine has been shown in case series to be useful in the treatment of
serpiginous choroiditis, multifocal choroiditis tubulointerstitial nephritis and panuveitis
when combined with prednisolone or ciclosporin A(16,17,18,19).
What to do
• Consult BNF.
• Ensure no potential interaction with other medications.
• U&E, LFT and FBC should be checked before commencing therapy, then weekly for
the first month of therapy and at least three monthly thereafter.
Uveitis NMCN Treatment Guidelines Revised September 2010
15

• The enzyme thiopurine methyltransferase (TPMT) metabolises azathioprine; the risk
of myelosuppression is increased in those with a low activity of the enzyme,
particularly in the very few individuals who are homozygous for low TPMT activity.
Normal levels: normal dose. Medium levels (heterozygous for TPMT mutation):
reduce dose. Very low levels (homozygous for TPMT mutation): low dose or avoid
use.
• If Allopurinol is co-prescribed the dose of Azathioprine should be reduced by 75%.
• If on warfarin then close monitoring of INR is advised as azathioprine may alter
anticoagulant effect.
• Azathioprine may be started at a dose of 50mg/day and if tolerated increased to
100mg after a week.
• Dosing usually needs to be adjusted based on the clinical response and side effects.
• Dose may be increased to a maximum of 2.5mg/kg/day.
• In practice, this will rarely exceed 150mg/day.
Side effects
Side effects are common and in one study 24% patients stopped azathioprine due to
side effects (10). These include generalised muscle aches, fatigue and headache. Slow
titration of the dose reduces the chance of these side effects and if they do occur then
dose reduction is often enough for symptoms to resolve. Regular blood monitoring is
required to identify liver dysfunction and bone marrow suppression. These effects
usually resolve on stopping the azathioprine. Gastrointestinal upset is relatively
common. A recent retrospective review would suggest that there is no increased cancer-
related mortality in patients treated with azathioprine for ocular inflammatory disease(20).
Uveitis NMCN Treatment Guidelines Revised September 2010
16

Methotrexate
Indications
• Most frequently used in disease in association with connective tissue disorders as a
steroid sparing agent.
• May be used in combination with infliximab for idiopathic inflammatory eye disease.
Evidence in Inflammatory Eye Disease
• Methotrexate has been show in several large studies to be effective in the treatment
of uveitis(18,22,23,24,25,26,27) with one large study showing remission in 76% patients (22).
• A recently published retrospective cohort study found 55.6% of patients with anterior
uveitis, 47.4% of patients with intermediate uveitis and 24% of patients with posterior
or panuveitis had control of their ocular inflammation within 6 months of treatment
with methotrexate (21).
• This however appears not to be the case in Scottish clinical practice and
methotrexate is rarely used except in patients requiring some form of
immunosuppression while on infliximab and all other immunosuppressants have
been either ineffective or not tolerated.
What to do
• Consult BNF.
• Ensure no potential interaction with other medications.
• Full blood count and renal and liver function tests before starting treatment and
repeated weekly until therapy stabilised, thereafter patients should be monitored
every 2–3 months.
• A baseline CXR is required.
• Patients should be advised to report all symptoms and signs suggestive of infection,
especially sore throat
• Not suitable for patients with either significant renal or liver disease.
Uveitis NMCN Treatment Guidelines Revised September 2010
17

• 16% patients (21) are intolerant of this drug.
• Commence at 7.5mg/week (as single dose).
• Dose may be increased by 2.5mg increments every 6-8 weeks (available in strengths
of 2.5mg and 10mg).
• The maximum dose is usually 15-25mg/week.
• Nausea, diarrhoea and mouth ulcers may respond to folic acid 5mg once a week 3
days after methotrexate.
• Respiratory symptoms should be investigated with a CXR and pulmonary function
tests as there is a risk of pulomary fibrosis.
• Side effects
• Regular blood monitoring is important as hepatoxicity and bone marrow suppression
may occur. These usually resolve on stopping the methotrexate. Nausea, diarrhoea
and mouth ulcers are relatively common but usually respond to treatment.
Conception must be avoided for at least 3 months after administration has ceased for
both males and females. May cause reversible sterility in males. Hair loss or rash
may occur. It is important to get medical review urgently if a rash develops. Hair loss
generally improves on stopping methotrexate. Irreversible lung changes may occur
(interstitial disease).
Uveitis NMCN Treatment Guidelines Revised September 2010
18

Mycophenolate mofetil
Indications
Used as a steroid sparing agent.
Evidence in Inflammatory Eye Disease
• In a number of published case series mycophenolate mofetil appears to be effective
in the treatment of ocular inflammatory disease (28,29,30).
• In one retrospective case series 64.3% patients achieved long term disease control
with mycophenolate mofetil (31).
• A recently published retrospective cohort study showed mycophenolate was
associated with a greater level of treatment success at six months than azathioprine
and methotrexate (70%, 58%, 42% respectively)(32) .
What to do
• Consult BNF
• Ensure no potential interaction with other medications.
• U&E, LFT, lipid profile and FBC should be checked before commencing therapy.
• FBC should be checked weekly for the first month, then twice a month for the second
and third months, then every month in the first year. Thereafter monitoring every two
to three months may be appropriate.
• U&E, LFTs and blood pressure should also be monitored regularly.
• Avoid clozapine and mycophenolate together as there is an increased risk of
agranulocytosis.
• Use cautiously in renal impairment or gastrointestinal disorders.
• Commence orally at 1g twice a day.
• May be increased up to 1.5g twice daily if clinically indicated.
• A negative pregnancy test is essential prior to commencement of therapy.
Uveitis NMCN Treatment Guidelines Revised September 2010
19
• Patients should be warned to report immediately any signs or symptoms of bone
marrow suppression e.g. infection or inexplicable bruising or bleeding
• Mycophenolate should not be prescribed concomitantly with azathioprine.
Side effects
Side effects include generalised muscle aches, fatigue and headache and
gastrointestinal upset. May be reduced by titrating the dose slowly. If side effects do
occur then dose reduction is often enough for symptoms to resolve. Regular blood
monitoring is important to identify liver dysfunction and bone marrow suppression.
These effects usually resolve on stopping the drug. A recent retrospective review would
suggest that there is no increased cancer-related mortality in patients treated with
mycophenolate for ocular inflammatory disease (20) .
Uveitis NMCN Treatment Guidelines Revised September 2010
20

T-cell inhibitors/Calcineurin Inhibitors
Ciclosporin
Indications
Ciclosporin may be used as a steroid sparing agent.
Evidence in Inflammatory Eye Disease
• Case series have suggested that cyclosporin is an effective monotherapy for the
treatment of uveitis at a dose of 10 mg kg/day (33). This is much higher dose than that
currently used.
• Several studies in uveitis have shown its efficacy and safety (34,35,36,37,38,39,40).
• In a randomized controlled trial involving 56 patients with uveitis, ciclosporin had
similar efficacy to oral steroids (41), though greater efficacy was noted in combination.
What to do
• Consult BNF.
• Ensure no potential interaction with other medications.
• Baseline FBC, LFTs, U&E (x2), lipids, urinalysis and blood pressure.
• U&E, LFTs and FBC should then be checked fortnightly until dose stable for 3
months, then monthly thereafter.
• Lipids should be checked every six months.
• BP should be checked at each monitoring visit.
• There is no indication for routine monitoring of serum concentrations of the drug as
they do not correlate well with efficacy. May be useful if compliance in question.
• Because of differences in bioavailability, the brand of oral ciclosporin to be dispensed
should be specified by the prescriber
• Doses given for Neoral.
Uveitis NMCN Treatment Guidelines Revised September 2010
21
• Commence at 2mg/kg twice a day (4mg/kg/day) orally.
• Dose adjusted dependent upon clinical response and side effects.
• Nephrotoxicity is relatively uncommon on doses of 2-5mg/kg/day. Treatment
contraindicated in patients with evidence of moderate or severe renal impairment.
• Do not prescribe concomitantly with tacrolimus.
• The concomitant use of nifedipine or colchicine should be avoided.
• Potassium sparing diuretics, ACE inhibitors, Angiotensin-II receptor antagonists and
potassium salts should be used with caution.
• Grapefruit juice should not be taken at the same time as ciclosporin.
Side effects
• Frequently causes hirsutism and therefore less favoured in women. Not generally a
problem in men
• Gum overgrowth may occur. Does not generally resolve on stopping ciclosporin and
may require surgery to correct.
• Regular blood monitoring usually allows early identification of liver or kidney
impairment. These effects may resolve on stopping the ciclosporin.
• High blood pressure and high cholesterol may result in an increased risk for stroke
and heart disease. Both of these side effects are monitored for and are potentially
treatable with further medication.
• Low magnesium levels may occur with ciclosporin. Occasionally these may cause
muscle aches or numbness. If these are problematic then the magnesium levels
usually return to normal on stopping the ciclosporin.
• Pregnancy and breast feeding relatively contraindicated while on ciclosporin.
• Tremor if not well tolerated may require cessation of treatment.
• Mild nephrotoxicity often responds to dose reduction. Ciclosporin should be stopped
if nephrotoxicity moderate or worse. Nephrotoxicity (42). All patients on 10mg/kg/day
Uveitis NMCN Treatment Guidelines Revised September 2010
22

will develop evidence of nephrotoxicity. This is significantly reduced on doses of 2-
5mg/kg/day.
Tacrolimus
Indications
Used as a steroid sparing agent.
Evidence in Inflammatory Eye Disease
• Small case series have suggested tacrolimus is effective in the treatment of uveitis,
achieving between 62% to 76% control (43,44,45,46).
• One prospective randomized controlled trial has shown tacrolimus to be as
efficacious as ciclosporin but with a better side effect profile (47).
What to do
• Consult BNF
• Ensure no potential interaction with other medications.
• Baseline FBC, LFTs, U&E and creatinine, lipid profile, blood glucose, coagulation
screen and ECG.
• Once on treatment U&E, creatinine, LFTs, FBC and blood pressure, should be
checked weekly for 4 weeks then fortnightly for 2 months then monthly.
• Lipid profile and blood glucose should checked regularly.
• Monitoring the blood concentration of tacrolimus is not essential when using low
doses. However, trough tacrolimus levels are useful when considering increasing the
tacrolimus dose, for ensuring that maintenance doses are not toxic and as a
measure of compliance.
Recommended doses given for Prograf
• An initial dosage of 0.05 mg per kg per day may be effective for uveitis.
• Usual effective dose 1-2mg twice daily.
Uveitis NMCN Treatment Guidelines Revised September 2010
23

• Dosing should be based on achieving disease control with minimal side effects.
• Do not prescribe concomitantly with ciclosporin.
• Grapefruit juice should not be taken at the same time as tacrolimus.
• Potassium sparing diuretics and potassium salts should be used with caution.
Side effects
• Regular blood monitoring usually allows early identification of liver or kidney
impairment. These effects may resolve on stopping the tacrolimus.
• May cause hypertension and hypercholesterolaemia which potentially may result in
an increased risk of stroke and ischaemic heart disease. Both of these side effects
are monitored for and are potentially treatable with further medication.
• Tacrolimus is associated with diabetes.
• Low magnesium levels may occur with tacrolimus and may result in muscular aches.
If these are problematic then magnesium supplements may be tried. The magnesium
levels usually return to normal on stopping the tacrolimus.
• Gastrointestinal upset including abdominal pain, nausea, vomiting, and diarrhoea
may occur. Slow dose increase reduces the chance of these side effects and if they
do occur then dose reduction is often enough for symptoms to resolve.
• Tremor occurs in some patients but stops with treatment cessation.
• Due to reports of reversible cardiomyopathy in children receiving tacrolimus following
cardiac transplant, it is recommended that children have regular echocardiograms
(reference to BNF). However, screening is generally not undertaken in adults.
• Occasionally headache can be a problem.
• Pregnancy and breast feeding relatively contraindicated while on tacrolimus. Avoid
steroid based contraceptive agents as tacrolimus may alter their metabolism.
• Adverse effects generally resolve or improve when tacrolimus is stopped or when the
dosage is reduced.
Uveitis NMCN Treatment Guidelines Revised September 2010
24
Alkylating Agents
Cyclophosphamide
Indications
Essential therapy in some forms of inflammatory disease especially if systemic disease
involvement. Used as an induction therapy.
Evidence in Inflammatory Eye Disease
• The majority of data on cyclophosphamide use in ocular inflammatory disease
comes from uncontrolled case series (50,51,52,53).
Intravenous pulsed cyclophosphamide has fewer side effects, but is less efficacious than
the preferred oral route (52).
What to do
• Consult BNF
• Ensure no potential interaction with other medications.
• U&E, LFT, FBC and urinalysis and pregnancy test (if appropriate) before
commencing treatment.
• Once treatment commenced, U&E, LFT, FBC and urinalysis weekly for the first
month, two weekly for the second and third month and then monthly thereafter.
• Doses given for oral route of administration.
• Starting dose orally, 1 to 3 mg/kg/day.
• Usual starting dose 100-150mg/day.
• Use with caution in elderly population (start at 50mg/day).
• Dose may be adjusted depending on response and toxicity.
• If toxicity occurs, dose may be decreased by 25 to 50 mg.
• Dosage reduction may be necessary in renal impairment.
Uveitis NMCN Treatment Guidelines Revised September 2010
25

• Should not be given concurrently with allopurinol as this increases bone marrow
suppression, or sulphonylureas due to the increased risk of hypoglycaemia.
• Opportunistic infections are more common with oral daily cyclophosphamide
compared to intravenous “pulse”, with 30% of patients on oral regimen developing
Pneumocystis carinii pneumonia in one study (48). Intermittent intravenous
administration is increasingly favoured by rheumatologists (49).
• Pneumocystitis carinii pneumonia prophylaxis should be considered for all patients
commencing cyclophosphamide. Septrin 960mg three times a week is
recommended. (see BSR guidelines)
• Patients should be asked about the presence of sore throat, rash, abnormal bruising
or oral ulceration at each visit.
• If a patients has haematuria on a urine dipstick they should be advised to increased
fluid intake. Monitor closely.
• If a patient develops macroscopic haematuria or haematuria with dysuria the drug
should be stopped.
Side effects
• Bone marrow suppression is dose dependent, reversible and more common in the
elderly.
• It is important that the patient is aware of signs and symptoms of bone marrow
suppression. They should be instructed to stop the cyclophopsphamide and to seek
urgent medical advice if they develop a sore throat, rash, abnormal bruising or oral
ulceration.
• Relative increased risk of cancer (especially bladder and bone cancer), however
most patients receiving this treatment do not develop cancer.
• Hair loss, usually recovers.
• Cystitis due to cyclophosphamide irritating bladder (high fluid intake reduces risk).
• Blood in urine, may be microscopic or macroscopic and is more common in patients
with inadequate fluid intake. Patients should stop treatment and seek medical advice
immediately if macroscopic haematuria occurs.
Uveitis NMCN Treatment Guidelines Revised September 2010
26

• Nausea and vomiting.
• Cyclophosphamide is contraindicated during pregnancy and lactation and should be
withdrawn at least 3 months prior to conception.
• Amenorrhoea and azoospermia may occur in patients taking cyclophosphamide.
• May result in primary ovarian failure in over 70% patients (53,54,55,56).
• Patients should be offered sperm banking/ cryopreservation of oocytes.
Uveitis NMCN Treatment Guidelines Revised September 2010
27

Biological therapies
Biologic therapies currently have a role in treating sight threatening uveitis refractory to
conventional immunosuppression. They may be used as steroid sparing agents or where
other immunosuppressive agents are poorly tolerated as well as when ocular inflammation
remains uncontrolled. There remains some uncertainty about the long term consequences of
biologic therapy and so they should not be used as first-line treatment at present. There are
considerable cost implications to these therapies, but they may be sight-saving, and in
patients where the more ‘traditional’ approaches have failed, expense should not prevent
appropriate treatment. Common and important side effects of medication are discussed here
but please consult the British National Formulary and product datasheets for more complete
information.
The aim of biological immunosuppressive therapy is to control ocular inflammation and allow
the oral prednisolone dosage to be reduced below 7.5mg. The overall duration of treatment
is dependent on the individual and their disease. At present there are no large studies
comparing biological treatments in inflammatory eye disease. The use of biological therapy
for treating inflammatory conditions is changing rapidly and as our understanding of immune
mechanisms contributing to ocular inflammation improves we should aim to target our
therapies more precisely.
Uveitis NMCN Treatment Guidelines Revised September 2010
28

Tumour necrosis factor (TNF) alpha inhibitors
The tumour necrosis factor (TNF) alpha inhibitors comprise adalimumab, infliximab and
etanercept. Adalimumab and infliximab are being used for the short and long term treatment
of refractory ocular inflammatory disease and are discussed below but etanercept appears
to be ineffective. Adalimumab offers the advantage of being delivered via a subcutaneous
injection whereas infliximab is given as an infusion. However, there is currently more
experience with infliximab than with adalimumab in treating uveitis.
The anti-TNF therapies can:
• Can unmask previously unidentified multiple sclerosis.
• May reactivate tuberculosis.
• Allergic-like reaction may occur during infusion (infliximab). Slowing infusion or pre-
treating with hydrocortisone often effective in preventing this during further infusions.
• Sudden death has been reported in patients with known heart problems.
• Pregnancy and breast feeding relatively contraindicated.
• Injection site reactions may occur. It has been reported that cooling the site prior to
administering the injection reduces pain associated with the injection.
• Infection including histoplasmosis and other invasive fungal infections.
• SLE and lupus like syndrome.
• Hepatitis B reactivation has been reported in patients on infliximab.
• Patients with hepatitis B should be referred to a gastroenterologist to consider
antiviral prophylaxis prior to starting anti TNF alpha therapy.
• Lymphoma has been reported but the incidence was not higher than would be
expected for that population.
• Haematologic reactions including pancytopenia and aplastic anaemia are rare.
• Although adverse effects may be severe, they are relatively rare and should be
compared with those associated with other immunosuppressive agents.
Uveitis NMCN Treatment Guidelines Revised September 2010
29

Adalimumab
Indications
• It is recommended that adalimumab should be used as an adjunctive therapy for
refractory cases of uveitis rather than as a first-line treatment.
• Can be used as either a steroid sparing agent or an inducing agent.
• Adalimumab has not been licensed for use in inflammatory eye disease
Evidence in Inflammatory Eye Disease
• There are a number of moderate sized case series, and one open label prospective
trial looking at adalimumab in paediatric uveitis. These have reported an
improvement in ocular inflammation (57,58,59,60), reduction in the use of topical and
systemic medication (57,59) and a low rate of uveitis flares (61) in children, the majority
of whom had juvenile idiopathic arthritis associated uveitis.
• There is one open label prospective trial of patients with uveitis refractory to therapy
treated with adalimumab for 12 months. This reported a reduction in macular
oedema, ocular inflammation and immunosuppression but 42% of patients had
relapses requiring periocular steroid injections (62).
• There is one small case series showing maintenance of remission of Bechet’s uveitis
in patients on adalimumab (63).
Practical Considerations
Prior to commencing therapy:
• Consult BNF.
• Ensure no potential interaction with other medications.
• Medical history and examination looking for evidence of infection or malignancy.
• Full blood count (FBC), urea and electrolytes (U+E), liver function tests (LFTs), C-
reactive protein (CRP), erythrocyte sedimentation rate (ESR), antinuclear antibodies
(ANA), double stranded DNA (dsDNA).
• Consider testing for hepatitis B.
Uveitis NMCN Treatment Guidelines Revised September 2010
30

• Consider investigating for central nervous system (CNS) demyelination in patients
with intermediate uveitis or a history of optic neuritis.
• Chest X-ray (CXR) to exclude tuberculosis (TB). Patients with an abnormal CXR,
history of TB or TB treatment should be referred to a TB specialist.
• Patients at high risk of TB eg. black African aged over 15 years and all South Asians
born outside the UK should be considered for TB chemoprophylaxis.
• Urinary pregnancy test as appropriate.
Short and longer term
• Usual adult dose is 40mg subcutaneous administered 2 weekly. May be increased to
40mg weekly if required. There is no data looking at the optimum dose of
adalimumab in uveitis.
• Dose for child ≤30kg is 20mg 2 weekly. Child ≥30kg is 40mg 2 weekly.
• Patients may be taught to self-administer adalimumab.
• Blood monitoring (FBC, U+E, LFT, CRP and ESR) should be performed 4 to 8
weekly.
Adalimumab as a monotherapy
• Adalimumab has been successfully used as a monotherapy in patients with ocular
inflammatory disease (59,61) although in the majority of reported cases it has been
used in combination with systemic steroids and/ or other immunosuppressive agents.
• In rheumatoid arthritis, a combination of methotrexate and adalimumab has been
found to be superior to adalimumab alone (64).
• There is currently no data on anti-adalimumab antibody formation in patients with
uveitis.
Contra-Indications/drug interactions
• Avoid concomitant use of adalimumab with other biological therapies.
• Avoid live vaccines (www.humira.com)
Uveitis NMCN Treatment Guidelines Revised September 2010
31
• Breast feeding. It is not known whether adalimumab is excreted in breast
milk (www.humira.com)
• Pregnancy. The effect of adalimumab on the fetus is unknown. (www.humira.com)
• Active infection including tuberculosis (www.humira.com)
• Demyelinating CNS disorders (65).
Side Effects
• Injection site reactions (10.6%). It has been reported that cooling the site prior to
administering the injection reduces pain associated with the injection (61).
• Infection including histoplasmosis and other invasive fungal infections (65,66) .
• Reactivation of tuberculosis (61).
• Demyelinating disease (61).
• SLE and lupus like syndrome (61) .
• Hepatitis B reactivation has been reported in patients on infliximab (66,67). Patients
with hepatitis B should be referred to a gastroenterologist to consider antiviral
prophylaxis prior to starting anti TNF alpha therapy (68).
• Lymphoma has been reported but the incidence was not higher than would be
expected for that population (65).
• Congestive cardiac failure (65). Use with caution in patients with known cardiac failure
(www.humira.com).
• Haematologic reactions including pancytopenia and aplastic anaemia are rare
(www.humira.com).
Uveitis NMCN Treatment Guidelines Revised September 2010
32

Infliximab
Indications
• It is recommended that infliximab should be used as an adjunctive therapy for
refractory cases of uveitis rather than as a first-line treatment.
• Can be used as either a steroid sparing agent or an inducing agent.
Evidence in Inflammatory Eye Disease
• In one prospective open label trial infliximab in patients with refractory uveitis, clinical
success was achieved in the majority of patients (17 out of 23 patients) at 10 weeks
although by one year the numbers of patients considered a success had fallen to 7
out of 14 patients (69).
• There are a number of prospective open label trials of patients with refractory
Behcet’s uveitis showing rapid control of inflammation with infliximab (70,71,72), a
significant reduction in uveitis flares (72,73) and of systemic steroid dose in patients
treated with infliximab compared with the pre-treatment period (73).
• There are case series reporting success in controlling ocular inflammation in
childhood uveitis (60,74,75,76).
Practical Considerations
• Consult BNF.
• Ensure no potential interaction with other medications.
• Hepatotoxicity has been reported. Infliximab should be stopped if liver function tests
become elevated to >5 times normal levels.
• Haematologic reactions including pancytopenia and aplastic anaemia are rare.
• Infusion hypersensitivity reaction – 10% of patients. May be severe and delayed.
• Although adverse effects may be severe, they are relatively rare and should be
compared with those associated with other immunosuppressive agents.
Uveitis NMCN Treatment Guidelines Revised September 2010
33
Prior to commencing therapy:
• Medical history and examination looking for evidence of infection or malignancy .
• FBC, U+E, LFTs, CRP, ESR, ANA, dsDNA.
• CXR to exclude tuberculosis (TB). Patients with an abnormal CXR, history of TB or
TB treatment should be referred to a TB specialist.
• Patients at high risk of TB eg. black African aged over 15 years and all South Asians
born outside the UK should be considered for TB chemoprophylaxis.
• Consider testing for hepatitis B
• Consider investigating for CNS demyelination in patients with intermediate uveitis or
a history of optic neuritis.
Short and longer term
• Usual dose is 5mg/kg administered as an intravenous infusion but doses of up to 20
mg/kg may be given.
• After the initial dose a second dose may be given after two weeks and then at 6
weeks.
• Further doses may be given up to 6 to 8 weekly dependent upon clinical response.
• Blood monitoring (FBC, U+E, LFT, CRP and ESR) should be performed 4 to 8
weekly.
Infliximab as a monotherapy
• Infliximab has been used successfully as a monotherapy in uveitis (71,72), although in
the majority of reported cases it has been used in combination with systemic steroids
and/ or other immunosuppressive agents.
• Studies of patients with rheumatoid arthritis have shown that the formation of anti-
infliximab antibodies is greater in patients on infliximab alone compared with those
on infliximab combined with methotrexate (77). The formation of anti-infliximab
antibodies has been associated with a loss of clinical response and an increased
rate of infusion reactions (78).
Uveitis NMCN Treatment Guidelines Revised September 2010
34
• There is currently no data on anti-infliximab antibody formation in patients with
uveitis. However, it is recommended that infliximab is used in combination with
another immunosuppressive agent where this is tolerated.
Side Effects
• Infusion hypersensitivity reaction – 10% of patients (79). May be severe and delayed.
• Infection, including histoplasmosis and other invasive fungal infections.
• Reactivation of tuberculosis (80).
• Demyelinating disease (81) .
• Optic neuropathy (82).
• SLE and lupus like syndrome (83).
• Hepatitis B reactivation (66,67). Patients with hepatitis B should be referred to a
gastroenterologist to consider antiviral prophylaxis prior to starting infliximab (68).
• Lymphoma has been reported but it is unclear whether the incidence is higher than
that in the general population (84).
• Congestive cardiac failure. Both exacerbation of existing heart failure and new-onset
heart failure reported (85,86) .
• Hepatotoxicity has been reported. Infliximab should be stopped if liver function tests
become elevated to >5 times normal levels (www.remicaide.com).
• Rare reports of haematologic disorders including leucopenia, neutropenia,
thrombocytopenia and pancytopenia (www.remicaide.com).
Uveitis NMCN Treatment Guidelines Revised September 2010
35

Interferon α
Indications
• It is currently recommended that Interferon-α is used only in cases of uveitis
refractory to conventional immunosuppressive therapy.
• Can be used as either a steroid sparing agent or an inducing agent.
Evidence in Inflammatory Eye Disease
• Both interferon alpha 2a (Roferon A®) and interferon alpha 2b (Intron A®,
Viraferon®) have been used in uveitis.
• A large prospective case series of patients with Behcet’s disease reported that 92%
patients responded to treatment. This effect appears to be prolonged with 40%
remaining inactive for 7 to 58 (mean 29.5) months after stopping treatment (87).
• Interferon alpha has been used to treat children with uveitis associated with Behcet’s
disease, and a corticosteroid sparing effect has been reported in one case series (88).
• Case series of patients with idiopathic uveitis, predominantly posterior and
panuveitis, refractory to conventional immunosuppression have demonstrated a
beneficial effect of interferon-α on uveitis in 59 to 83% of patients (89,90).
• Refractory uveitic cystoid macular oedema responded to interferon alpha with
complete resolution in 6 out of 8 patients in a prospective pilot study (91).
What to do
Pre-treatment
• Consult BNF.
• Ensure no potential interaction with other medications.
• Medical history and examination, including history of mental illness.
• Prior to administration of the first dose, the following investigations should be
performed: FBC, U+E, LFTs, CRP, ESR, thyroid function tests (TFT), autoantibodies
Uveitis NMCN Treatment Guidelines Revised September 2010
36
including dsDNA and thyroid autoantibodies, coagulation screen, lipid profile, urinary
pregnancy test as appropriate.
• The patient’s weight should be recorded.
• Base line ECG for patients with cardiovascular disease.
• Chest X-ray.
• Steroid dose should be no greater than 15 mg prednisolone daily when interferon
treatment commenced, and ideally reduced to 10mg or less.
• Other immunosuppressive drugs should be stopped prior to starting interferon
therapy.
Short and longer term
• Starting dose 3 million units once daily for Intron A.
• Maximum dose of Intron A used in ocular inflammatory disease is nine million units
daily.
• Administered as a subcutaneous injection daily before bed as patients may feel tired
after the injection.
• Paracetamol should be given 500mg tds for days 1-3.
• The following blood tests should be monitored during treatment at weeks 1, 2, 4, 8
and every month thereafter: FBC, U+E, LFTs, CRP, ESR, TFT and lipid profile
• Weight should be recorded at each clinic visit.
Contra-Indications/drug interactions
• Avoid concomitant use of interferon alpha with other immunosuppressive agents.
Low doses of steroids may be used in combination with interferon alpha.
• Avoid live vaccines.
• Breast feeding. It is not known whether interferon alpha is excreted in breast milk.
(http://www.introna.com).
Uveitis NMCN Treatment Guidelines Revised September 2010
37

• Pregnancy. The effect of interferon alpha on the fetus is unknown.
(http://www.introna.com).
• History of severe depression.
• Hypersensitivity to interferon alpha (http://www.introna.com).
• Autoimmune hepatitis (http://www.introna.com).
• Decompensated liver disease (http://www.introna.com).
• Uncontrolled thyroid disease (http://www.introna.com).
Side Effects
• Flu-like illness (fatigue, headache, arthralgia, fever) occurs in almost all patients(87,88)
( http://www.introna.com). It is most predominant in the first two weeks of therapy
and may be improved by taking regular paracetamol (http://www.introna.com).
• Fatigue may persist during therapy (90).
• Anorexia and weight loss - 33% (90).
• Bone marrow toxicity resulting in myelosupression (87,89) and rarely aplastic anaemia
(http://www.introna.com).
• Injection site reaction. 25% (90) - 100% (87).
• Alopecia. 24% (96). Hair growth returns when interferon alpha is stopped
(http://www.introna.com).
• Hepatotoxicity (91). If the ALT rises to greater than 5 times normal, interferon should
be withheld. It may be later re-introduced at 50% of the initial dose. If the ALT rises
to greater than 10 times normal, interferon should be stopped and not re-started
(http://www.introna.com).
• Regular blood monitoring usually allows early identification of liver disturbance and
bone marrow suppression. These effects should resolve on stopping the interferon.
• Depression may be dose related and improve as the dose is reduced (89). Selective
serotonin re-uptake inhibitors have been used to treat interferon-induced depression
in a case series of patients (92). Depression may be severe and suicidal ideation has
Uveitis NMCN Treatment Guidelines Revised September 2010
38

been reported (88,90). Patients with severe or worsening depression should have their
therapy stopped (92).
• Pruritis 24% (87)
• Diarrhoea
• Hypertriglyceridaemia, which may cause pancreatitis (http://www.introna.com).
• Cardiovascular problems – Hypotension, hypertension and arrhythmias. Use
cautiously in patients with known cardiovascular disease (http://www.introna.com).
• Retinopathy manifesting as cotton wool spots and retinal haemorrhages (90) .
• Acute hypersensitivity reactions. Drug should be stopped if an acute reaction
develops (http://www.introna.com). The risk of development of hypersensitivity
reactions may be greater with second and subsequent treatments
• Thyroid dysfunction, which may not be reversible when the drug is stopped
(http://www.introna.com).
• Psoriasiform rash (90)
• Seizures (87)
• Interferon alpha may impair fertility (http://www.introna.com).
• The patient should be made aware of the possibility of delayed adverse reactions
and should be advised to report any symptoms which may give them cause for
concern.
• Not recommended in pregnancy or breast feeding.
• Women of childbearing age should use effective contraception during treatment and
for four months after.
Uveitis NMCN Treatment Guidelines Revised September 2010
39

Daclizumab
Indications
• It is recommended that Daclizumab is used only in cases of uveitis refractory to
conventional immunosuppressive therapy.
• Humanised IgG monoclonal antibody that binds CD25 of the human IL-2 receptor.
• Mechanism of action may be via induction of natural killer (CD56bright) cells.
Evidence in Inflammatory Eye Disease
• Daclizumab has been found to be effective in the treatment of intermediate and
posterior uveitis in a small open label study. Eight out of ten patients maintained
remission of uveitis over 4 years and were able to withdraw concomitant
immunosppressive medications with 2 to 4 weekly infusions of daclizumab (94).
• High dose intravenous daclizumab has been used successfully as an induction
therapy for active sight-threatening uveitis in a small open label study with control of
uveitis in 4 out of 5 patients at 4 weeks (95). Standard dose daclizumab (1mg/kg)
improved ocular inflammation in 59% of eyes in one case series (96).
• Two-weekly subcutaneous administration of daclizumab has also been shown to be
effective in maintaining remission of uveitis in a small 26 week open label trial (61,97).
• A retrospective case series of patients with birdshot retinochoroidopathy showed an
improvement in clinically observed ocular inflammation with daclizumab, but
electroretinography parameters declined in some patients (98).
• Three out of five children with ocular inflammatory disease responded to daclizumab
in one series but there were a number of adverse events with three children
developing transient leukopenia, one nausea, and one myalgia and fatigue (60).
• A small randomised controlled trial of daclizumab use in patients with Behcets
disease did not show any benefit of intravenous daclizumab over placebo in
preventing ocular attacks of Behcet’s disease (99).
Uveitis NMCN Treatment Guidelines Revised September 2010
40

Practical Considerations
• Consult BNF.
• Ensure no potential interaction with other medications.
• Infusion hypersensitivity reaction. If a severe reaction occurs, daclizumab should be
discontinued.
• Fatigue may occur.
• Infection. An increased risk of death from sepsis was observed in a trial using
daclizumab for cardiac transplantation but these patients were on up to 5
immunosuppressive agents (93).
• Skin rash, liver disturbance, painful muscles, lymphadenopathy and leucopenia have
been reported.
• An increased risk of malignancy has not been found in studies of renal transplant
patients, but there is a theoretical increased risk of malignancy with
immunosuppression.
• Side effect profile should be discussed explaining that although adverse effects may
be severe, they are relatively rare and should be compared with those associated
with other immunosuppressive agents.
• Prior to commencing therapy:
• Medical history and examination looking for evidence of infection or malignancy .
• U+E, LFTs, CRP, FBC, ESR
• CXR to exclude tuberculosis (TB). Patients with an abnormal CXR, history of TB or
TB treatment should be referred to a TB specialist.
• Urinary pregnancy test as appropriate.
Short and longer term
• Blood monitoring (FBC, U+E, LFT, CRP and ESR) should be performed 2 to 4
weekly prior to administering infusion.
Uveitis NMCN Treatment Guidelines Revised September 2010
41

Daclizumab as a monotherapy
• Daclizumab has been used effectively as a monotherapy for uveitis. In a four year
open label study, patients were tapered off other immunosuppressive agents and
maintained on daclizumab alone (94).
Side Effects
• Infusion hypersensitivity reaction. If a severe reaction occurs, daclizumab should be
discontinued (http://www.rocheusa.com/products/zenapax/)
• Infection. An increased risk of death from sepsis was observed in a trial using
daclizumab for cardiac transplantation but these patients were on up to 5
immunosuppressive agents (93).
• Skin rash (100).
• Hepatic dysfunction (98).
• Leucopenia (96,98).
• Lymphadenopathy (94).
• Fatigue (60).
• Myalgia (60).
• An increased risk of malignancy has not been found in studies of renal transplant
patients (101), but there is a theoretical increased risk of malignancy with
immunosuppression (http://www.rocheusa.com/products/zenapax/)
Short and longer term
• The dose regime for transplantation is an intravenous infusion of 1mg/kg two weekly
for 5 doses.
• In uveitis, induction doses of 8mg/kg have been used intravenously with a second
dose of 5mg per kg at 14 days (95).
• Maintenance intravenous dose is 1mg per kg (up to 100mg). Administer 2-4 weekly (94).
Uveitis NMCN Treatment Guidelines Revised September 2010
42
• Although subcutaneous daclizumab has been used in trials at a dose of 1 to 2mg/kg,
2 to 4 weekly (maximum 200mg) (94,96) there is not currently a commercial product for
subcutaneous use.
Campath (Alemtuzumab)
Indications
• It is currently recommended that Alemtuzumab is used only in cases of uveitis
refractory to conventional immunosuppressive therapy.
• Can be used as either a steroid sparing agent or an inducing agent.
• Is a humanised mAb which binds to CD52, the pan-lymphocyte antigen.
Evidence in Inflammatory Eye Disease
• One case series of ten patients showed Campath-1H to be effective in the treatment
of refractory ocular inflammatory disease with initial improvement in all patients.
Eight patients had control of ocular inflammation lasting 5 months or longer (102).
• Campath-1H has also been used effectively in the treatment of a Mooren’s ulcer (103).
• A case series of patients with Behcet’s syndrome were treated with Campath using a
total of 134mg administered over 5 days. Details of eye involvement is limited in the
paper but there were four patients with active ocular disease prior to receiving
Campath, and at 6 months two were in remission and two in ‘partial remission’ (104).
Practical Considerations
What to do
Pre-treatment
Prior to commencing therapy:
• Consult BNF.
• Ensure no potential interaction with other medications.
Uveitis NMCN Treatment Guidelines Revised September 2010
43
• Medical history and examination looking for evidence of infection or malignancy.
• FBC, U+E, LFTs, CRP, ESR
• Baseline cytomegalovirus serology.
• CXR to exclude tuberculosis (TB). Patients with an abnormal CXR, history of TB or
TB treatment should be referred to a TB specialist.
• Consider HIV test.
• Urinary pregnancy test as appropriate.
• Ensure adequate contraception is used for at least 6 months following the infusions.
Short and longer term.
• Patients should be pre-treated with steroid, paracetamol and anti-histamine e.g. 1g
oral paracetamol, 100mg hydrocortisone and 10ml chlorpheniramine 30 minutes
prior to the infusion.
• Patients should receive anti-infective prophylaxis against Pneumocystis jiroveci
pneumonia (e.g. trimethoprim/ sulfamethazole 1 tablet twice daily, 3 times weekly)
and an oral anti-herpes agent such as famiciclovir 250mg bd while on therapy and
following treatment for a minimum of two months after treatment or until the CD4+
count has recovered to 200 cells/μl (whichever occurs later). (www.campath.com).
• Patients should have daily monitoring of full blood count and platelet count during
therapy with Campath and at 1, 2 and 4 weeks post therapy and at intervals
thereafter until haematological indices have recovered. Thyroid function should be
monitored.
Contra-Indications/drug interactions
• Breast feeding. It is not known whether Campath is excreted in breast milk
(http://emc.medicines.org.uk/).
• Pregnancy (http://emc.medicines.org.uk/).
• Active infection (http://emc.medicines.org.uk/).
• HIV (http://emc.medicines.org.uk/).
Uveitis NMCN Treatment Guidelines Revised September 2010
44

• Use with caution in patients with ischaemic heart disease, angina and patients on
antihypertensives. (http://emc.medicines.org.uk/). Mycocardial infarction following
a Campath infusion has been reported (104).
• Avoid live vaccines (www.campath.com)
Side Effects
• Infusion reactions due to cytokine release causing rigors, fever, nausea, vomiting
and skin rashes are common. Severe reactions with bronchospasm, syncope, acute
respiratory distress syndrome, myocardial infarction and death have been reported.
Infusion reactions may be minimised by dose-escalation and by pretreatment with
oral antihistamines, paracetamol, and corticosteroids
(http://emc.medicines.org.uk/).
• Haematological toxicity. Lymphopenia occurs in all patients. Neutropenia,
thrombocytopenia (106), anaemia (www.campath.com), and coagulopathy (107) may
occur.
• Severe infections, some resulting in death, have been reported in patients with
haematological malignancies treated with Campath, although these patients received
higher doses than are used for ocular disease and had received other
immunosuppressive agents. Opportunistic infections included cytalomegalovirus,
aspergillosis, cerebral toxoplasmosis and progressive multifocal leukencephalopathy (108). There have been no reports of significant opportunistic infections in patients
treated with Campath for ocular inflammatory disease but experience of Campath
treatment in ocular disease is limited (109). Patients should be advised to report
symptoms of infection e.g. pyrexia (www.campath.com).
• Myocardial infarction post-infusion has been reported in the oncology literature (105).
• Hypothyroidism developed in 2 out of 18 patients with Behcet’s disease following
Campath infusions (http://emc.medicines.org.uk/). Thyroid dysfunction, usually
associated with thyroid autoantibodies, developed in 22% of patients with multiple
sclerosis and occurred up to 30 months after the last infusion. Some patients
required long term treatment for thyroid disease (110).
Uveitis NMCN Treatment Guidelines Revised September 2010
45

• Campath is administered as an intravenous infusion over 2 hours
(www.campath.com). The reported regimen for ocular inflammatory disease is daily
infusions for five days (102).
• The initial dose is 3mg. If tolerated this may be increased to 5 mg on the second day
and then up to 10mg. The maximum reported dose for treating ocular inflammatory
disease is 10-12 mg daily (102).
• One paper on Campath use in systemic Behcet’s disease, which included patients
with ocular disease, used an escalating regimen of 4mg,10mg, 40mg, 40mg and
40mg infusions on consecutive days (104). Doses of up to 30mg daily or 90mg weekly
are used for B cell chronic lymphocytic leukaemia (www.campath.com).
• If blood products are required following Campath therapy, these should be irradiated
while the patient remains lymphopenic because of the risk of graft versus host
disease (http://emc.medicines.org.uk/).
Rituximab
Indications
• Can be used as either a steroid sparing agent or an inducing agent.
• Is a monoclonal antibody that binds to CD20 on mature B lymphocytes.
• Depletes CD20+ B cells by antibody-dependent cellular cytotoxicity, complement-
dependent cytotoxicity and apoptosis.
• Significant reduction in peripheral blood B lymphocytes occurs for 6 to 12 months.
Evidence in Inflammatory Eye Disease
• There are isolated case reports showing a benefit in anterior uveitis(112), scleritis
associated with Sjögrens syndrome (113), and scleritis (114) and peripheral ulcerative
keratitis (115) associated with Wegener’s granulomatosis. Rituximab has been used in
the treatment of retinal vasculitis (116).
• A number of small uncontrolled studies and case reports suggest that rituximab may
be effective in systemic lupus erythematosus (117) and systemic vasculitis (118).
Uveitis NMCN Treatment Guidelines Revised September 2010
46

Practical Considerations
What to do
Pre-treatment
• Consult BNF.
• Ensure no potential interaction with other medications.
• U&E, LFT, FBC before commencing treatment.
• Four rituximab infusions (375mg/m2) intravenously at 4 weekly intervals effective in
treatment of anterior scleritis. So far no information or data for its use in uveitis. It
may be that this could be reduced further.
• Administration of IV administration of corticosteroids prior to the first dose of
rituximab reduces the incidence of infusion reactions. Infusion reactions less
common after the second rituximab dose, compared with the first.
• It may be that this could be reduced even further as an on-going dose-ranging trial
for the use of Rituximab in RA suggests dosing at day 1 and 15 at either 500mg or
1000mg proved efficacious (111) .
Short and longer term
• U&E, LFT, FBC weekly for the first 2 months and 4 weekly thereafter.
• Human antichimaeric antibodies against rituximab have been detected, although
despite these patients were successfully retreated.
• Regular blood monitoring usually allows early identification of liver impairment and
bone marrow suppression with increased risk of infection and bleeding.
Contra-Indications/drug interactions
• Breastfeeding.
• Recent MI.
• Severe arrhythmias.
Uveitis NMCN Treatment Guidelines Revised September 2010
47

• Uncontrolled CCF.
• Women of childbearing age should use effective contraception during treatment and
for twelve months after.
Side Effects
• Up to 94% patients have reported adverse events during clinical trials for Rituximab (119).
Infusion related reactions
• Transient flu-like symptoms during first infusion (50-87%). Normally resolves within 3
hours. May require paracetamol and/or antihistamine (120,121,122,123,124,125).
• Up to 10% patients also experienced bronchospasm, hypotension or severe cytokine
release syndrome during first infusion.
• Generally treatment can be completed after symptoms resolved.
• Administration of IV corticosteroids prior to the first dose of rituximab reduced the
incidence of infusion reactions. Infusion reactions less common after the second
rituximab dose, compared with the first (121,123).
• Fatalities following severe cytokine release syndrome (characterised by severe
dyspnoea) and associated with features of tumour lysis syndrome have occurred 1–2
hours after infusion of rituximab (0.04–0.07% of patients) in patients treated for AML
and CLL.
• In the vast majority of cases these adverse effects are reversible with interruption or
discontinuation of rituximab along with supportive care severe consequences of
infusion-related reactions have been reported, including pulmonary infiltrates, acute
respiratory distress syndrome and cardiovascular events. Multi-organ failure can
occur. Infusion- related fatalities with rituximab have been rare (126).
• Transient hypotension frequent during infusion. Recommend withholding
antihypertensives for 12 hours prior to infusion.
• Cardiac arrhythmias (2%) (121) .
• Angina pectoris.
Uveitis NMCN Treatment Guidelines Revised September 2010
48

• Syncope.
• Anaphylaxis.
• Urticaria (127).
• Stevens-Johnson syndrome (127).
• Human antichimaeric antibodies (HACA) against rituximab were detected in <1%
and patients were successfully re-treated with the drug after developing HACA (124).
• Anaemia (Hb<10 g/dl) (10%) (121).
• Thrombocytopenia (2%) (121).
• Leucopenia (121).
• Neutropenia (0.5-1.5x109 cells/L) (10%) (121).
• These mild haematological abnormalities resolved spontaneously in 4 to 8 days
(relationship to treatment not reported) (121).
• All side effect information available is for use in AML and CLL therapy where dosing
regimens more aggressive and therefore we would hope the type and severity of
adverse reactions would be much less with this dosing regimen.
• Two dose-ranging studies have shown no relationship between side effects and
administered dose (120,122).
Anakinra
Indications
• May be used as a steroid sparing agent or an inducing agent.
Evidence in Inflammatory Eye Disease
• Anakinra is an anti-IL-1 agent.
• There is one case report of successful treatment of a child with uveitis associated
with the CINCA syndrome using anakinra (128). There is also a report of scleritis
responding to anakinra in two patients with rheumatoid arthritis (129).
Uveitis NMCN Treatment Guidelines Revised September 2010
49

• Although anakinra has been shown in several randomized, controlled, double-blind
clinical trials to be effective in the treatment of rheumatoid arthritis, there are no
human studies for its use in ocular inflammatory disease (130,131).
Practical Considerations
What to do
• Consult BNF.
• Ensure no potential interaction with other medications.
• Monitor neutrophil count before treatment, then every month for 6 months, then
every 3 months—discontinue if neutropenia develops.
• Dose 100mg subcutaneous once a day.
• Alternating injection site recommended.
• Supplied in pre-filled syringe.
• Use cautiously in patients with a history of asthma (risk of serious infection).
• Patients should be instructed to seek medical advice if symptoms suggestive of
neutropenia (such as fever, sore throat, infection) develop.
Contra-Indications/drug interactions
• Predisposition to infections.
• History of asthma (risk of serious infection).
• Renal impairment. Manufacturer advises caution if creatinine clearance 30–
50 mL/minute; avoid if creatinine clearance less than 30 mL/minute.
• Despite animal model studies suggesting a benefit of combination therapy with
anakinra and anti-TNF-α in inflammatory arthritis, a safety study, though showing
increased efficacy, identified a high rate of adverse effects(132). A further study looked
at the additional benefit of anakinra and etanercept versus etanercept alone in
patients with rheumatoid arthritis but didn’t show any additional clinical benefit (133).
Combination therapy is therefore not recommended.
Uveitis NMCN Treatment Guidelines Revised September 2010
50

Side Effects
• Injection site reactions (70%) (http://www.kineretrx.com/#).
• Serious infection (mainly bacterial) (http://www.kineretrx.com/#).
• Neutropaenia (<1 x109/L) (0.4%) (http://www.kineretrx.com/#).
• Increased lymphoma (3.6 fold increase) and melanoma rates (3 fold increase)
(http://www.kineretrx.com/#).
• Unlike anti-TNF-α therapies, there has been no report of increased incidence of
tuberculosis or opportunistic infections in patients treated with anakinra.
• Regular blood monitoring usually allows early identification of bone marrow
suppression with increased risk of infection.
• Patients should be instructed to seek medical advice if symptoms suggestive of
neutropenia (such as fever, sore throat, infection) develop.
• Relative increased risk of cancer (especially lymphoma and melanoma), however
most patients receiving this treatment do not develop cancer.
Other biological therapies
Etanercept
Etanercept appears to be ineffective as an agent for the treatment of uveitis. While an early
report suggested a benefit in children with uveitis (134) the majority of these patients had an
incomplete treatment response and small randomised controlled trials looking at the role of
etanercept in preventing relapse of uveitis (135), controlling juvenile idiopathic arthritis
associated uveitis (136) and ocular sarcoidosis (137) have shown no benefit over a placebo.
Retrospective comparison of infliximab and etanercept in controlling uveitis have found the
former to be superior (138,57). There are also case reports of new onset uveitis occurring in
patients on etanercept for other conditions (139,140). Etanercept is not currently recommended
for use as treatment for eye disease.
Uveitis NMCN Treatment Guidelines Revised September 2010
51

Summary of use of second line and biologic agents
• The aim of immunosuppressive therapy is to control disease and allow the oral
prednisolone dosage to be reduced to 7.5mg or less.
• Cystoid macular oedema is the leading cause of visual loss in uveitis and systemic
treatment should be considered in ALL patients with cystoid macular oedema.
• Having achieved disease control, immunosuppressive therapy is usually continued
for at least 6 months.
• The overall duration of treatment is dependent on the individual and disease activity
• Treatment may be required in the long-term or possibly even life-long depending on
the underlying condition.
• Once the prednisolone dose below 7.5mg and provided ocular inflammation remains
controlled then immunosuppressive therapy is slowly withdrawn.
• Dosage reductions are usually made every 4 to 6 weeks. and complete withdrawal of
therapy may take up to 12 months.
• At present there are no large studies comparing treatment efficacies.
• Individual treatment plans often initially the result of a patients preferred side effects
rather than on evidence-based decisions.
• Mycophenolate or tacrolimus are often the first choice agents with the choice of
agent based on likely efficacy and tolerability.
• T-cell inhibitors (ciclosporin or tacrolimus) are often the first choice agent for T-cell
mediated disease (retinal vasculitis, Vogt-Koyangi-Harada disease, sympathetic
ophthalmitis).
• Frequent review and early identification of treatment failure is important to allow
appropriate therapeutic changes to reduce morbidity and improve long-term visual
outcomes.
• The aim of biological immunosuppressive therapy is to control ocular inflammation
and allow the oral prednisolone dosage to be reduced below 7.5mg.
Uveitis NMCN Treatment Guidelines Revised September 2010
52

• Biological therapies are associated with significant systemic side effects. The long
term effects of biological therapies are still unknown and so these drugs should not
be used as first line agents.
• The overall duration of treatment is dependent on the individual and their disease.
• At present there are no large studies comparing biological treatments.
• The use of biological therapy for treating inflammatory conditions is changing rapidly
and as our understanding of immune mechanisms contributing to ocular
inflammation improves we should aim to target our therapies more precisely.
Uveitis NMCN Treatment Guidelines Revised September 2010
53

Combination Therapy
• As with all treatments for inflammatory eye disease, the concept of combination
therapy was adopted from allied specialities.
• This strategy has a long and proven history in the treatment of cancer.
• Due to the many pathways involved, a ‘two-pronged’ approach affecting different
parts of the immune system may be more effective than individual therapies.
• As the drugs have different side effect profiles, combination therapy may allow lower
individual doses to be used and so may be better tolerated than monotherapy.
• Alhough in other specialities large randomized controlled trials have been
undertaken to show the benefits of combination immunosuppressive therapy over
monotherapy (141,142,143), there are currently no randomized clinical trials making such
comparisons (1).
• In practice, immunosuppressive therapy is usually prescribed in combination with
oral prednisolone, the exception being interferon, where it is felt that combination
therapy actually reduces its efficacy. If prednisolone is used in combination with
interferon then the dose of prednisolone should be 10mg or less.
• In one case series combining methotrexate, ciclosporin and corticosteroid was
shown to be beneficial (144).
• Triple therapy in the form of azathioprine, cyclosporine and corticosteroid appears to
be more effective than monotherapy in the treatment of serpiginous choroidopathy (16).
Uveitis NMCN Treatment Guidelines Revised September 2010
54
Appendices
Appendix 1: Posterior Uveitis requiring early immunosuppressive therapy
Immunosuppression is recommended at the outset in a number of inflammatory eye
diseases due to the chronicity and potentially poor prognosis that these conditions have if
untreated. These conditions include ocular Behçet’s disease, birdshot retinochoroidopathy,
multifocal choroiditis with panuveitis, serpiginous choroidopathy, Vogt-Koyangi-Harada
disease and Sympathetic ophthalmitis
A number of these specific conditions and their treatment guidelines are presented below.
Where possible evidence for the efficacy of therapy is provided but due to the relative
scarcity of some of these conditions the evidence base is limited. It is important to realise
that many of these conditions have been treated under the blanket of sight-threatening
uveits, the individual conditions being lost within the study’s statistics. In practice therefore
where evidence doesn’t exist for specific disease-directed therapy then the therapy should
be directed by the disease activity.
Behçet’s disease
Treatment guidelines
• The acute presentation should be controlled with high dose oral prednisolone (1 to
1.5 mg/kg/ day).
• Sight-threatening disease may warrant urgent high dose pulsed methylprednisolone
of 1g per day for 3 days.
• Corticosteroids rarely prevent recurrences and are therefore used in combination
with immunosuppressive agents (145,146,147).
• Second line immunosuppresion should be started as soon as the diagnosis is
confirmed.
• Treatment choice will depend on the individual patient circumstances and disease
activity, both ocular and systemic.
• Chlorambucil and cyclophosphamide are effective in disease control in this condition (148) (case series). Chlorambucil is usually commenced at 0.1 mg/kg/day (149) and it
may take up to 3 months to be effective.
Uveitis NMCN Treatment Guidelines Revised September 2010
55

• Both ciclosporin and tacrolimus have been used widely for the treatment of uveitis in
patients with Behçet’s disease (34,150,44,46). Ciclosporin has been shown to be more
effective than colchicine and cyclophosphamide in the treatment of ocular Behçet’s
disease (151,52,36).
• Tacrolimus may be effective in patients with posterior uveitis refractory to ciclosporin (151) .
• Ciclosporin and tacrolimus are not recommended in patients with central nervous
system involvement as they may potentiate this (152).
• Azathioprine (dose of 2.5 mg per kg per day), has been shown to be effective
(controlled trial), although 22% patients developed disease while on azathioprine (11).
Other groups have also reported favourable results (153).
• Biologic agents, specifically interferon α and infliximab have recently been shown to
be effective in the treatment of ocular Behcet’s disease (154,155,156,157,70,96).
• Interferon α has been shown to produce remission, even in previously refractory
disease (96). In one study 92% patients with previously refractory disease responded
to treatment. This effect appears to be prolonged with 40% remaining inactive 14
months after stopping treatment (96).
• The results of infliximab in ocular Behcet’s disease appear very promising. In one
study, 24 of 25 patients had went immediate remission after a single treatment (70)
and remission was attained for over six months in 60% patients who had further
dosing. Numerous other studies have shown favourable results for the use of
infliximab in ocular Behcet’s disease (155,156,158,159).
• Infliximab should be used as an adjunctive therapy for refractory cases rather than
as a first-line treatment (70,159). Etanercept has not been shown to be effective (135).
• For refractory ocular disease biologic agents should be considered.
Birdshot Retinochoroidopathy
Treatment guidelines
• Ciclosporin may be effective in the treatment of birdshot retinochoroidopathy (36,160,161)
(case series, no controlled trials).
Uveitis NMCN Treatment Guidelines Revised September 2010
56

• Ciclosporin is more efficacious than corticosteroid therapy alone. Disease control
was achieved in 85% patients compared to 46% respectively over a follow up period
of between 24 and 48 months (160).
• Another case series has shown in individual patients ciclosporin, mycophenolate
mofetil, azathioprine, methotrexate, and daclizumab to be effective (162).
Multifocal Choroiditis with panuveitis
Treatment guidelines
• Oral corticosteroids are effective in up to 50% patients (163) in treatment of cystoid
macular oedema, dense vitritis or macular choroidal neovascular membrane (164).
• Consider immunosuppressive therapy, although there is no evidence at present to
suggest the efficacy of this (165).
Serpiginous Choroidopathy
Treatment guidelines
• Ciclosporin in combination with oral prednisolone has been advocated for early
treatment of this condition (166,167).(Case series, no controlled trials)
• Other authors have found this treatment ineffective (168) and some have
recommended a triple therapy regimen (16,17) involving concurrent administration of
prednisone, ciclosporin and azathioprine.
• Alkylating agents have been shown to be effective in an uncontrolled case series (169)
.
Uveitis NMCN Treatment Guidelines Revised September 2010
57

Appendix 2: Treatment of Inflammatory choroidal neovascularization (CNV)
Inflammatory choroidal neovascularization (CNV) is a comparatively rare complication of
uveitis, occurring in 1.9% of patients with uveitis (12 of 648) in one large retrospective
review (170) . However, inflammation is the third most common cause of choroidal
neovascularization, after age related macular degeneration (AMD) and pathological myopia,
and CNV of any aetiology can lead to severe visual loss (170).
Inflammatory conditions with a high incidence of CNV include punctate inner choroidopathy
(PIC), multifocal choroiditis with panuveitis, ocular histoplasmosis, serpiginous choroiditis,
Vogt-Koyanagi-Harada disease and ocular toxoplasmosis. CNV can develop during an
episode of active uveitis or in eyes with signs of previous uveitis but no active inflammation
at the time of visual loss from the CNV. In a recent multicentre treatment study of
inflammatory ocular neovascularization, 26% of eyes (26 of 99) had signs of active uveitis,
whereas in 74% of eyes (73 of 99) the uveitis was inactive (171).
The following treatments for inflammatory CNV have been used either as monotherapy or in
combination: argon laser photocoagulation, surgical excision, corticosteroids (local injections
or systemic), second line immunosuppressive agents, photodynamic therapy (PDT) and
intravitrel anti-vascular endothelial growth factor (VEGF) agents.
Laser photocoagulation of subfoveal CNV causes immediate loss of vision and is therefore
counterproductive. In cases of juxtafoveal or extrafoveal CNV, laser photocoagulation can
reduce the risk of severe loss of vision; however, enlargement of the subsequent scar, and
recurrence of neovascularization at the edge of the scar, often causes late visual loss (172).
The Submacular Surgery Trials Research Group presented a randomized comparison of
surgery vs observation for subfoveal CNV in eyes with ocular histoplasmosis or idiopathic
cause (173). At the 24-month follow-up, median BCVA was 6/75 (20/250) in the observation
arm and 6/48 (20/160) in the surgery arm. CNV recurred in 58% of surgically treated eyes.
Overall this study did not show a significant benefit for surgical excision.
A tapering course of high dose oral prednisolone monotherapy has been shown to stabilize
or improve vision, in the short term, in the majority of patients with inflammatory CNV due to
PIC or multifocal choroiditis (174). However, some patients fail to respond to systemic
immunosuppression (175), or develop recurrences when immunosuppression is reduced.
The Verteporfin in Ocular Histoplasmosis Study treated 22 patients showing subfoveal CNV
with an average of 3.9 sessions of PDT (176). At the 24-month examination, the median
Uveitis NMCN Treatment Guidelines Revised September 2010
58
improvement was 1.2 lines. PDT has been used to reduce CNV activity and improve vision
when initial treatment with systemic immunosuppression has failed. In a small study of 5
patients with CNV secondary to PIC, combination therapy with PDT and systemic
corticosteroids, led to an average improvement of 9 ETDRS letters at 12 months follow up (177).
Multiple recent studies have reported a beneficial effect with intravitreal bevacizumab
(Avastin) for inflammatory CNV (171,178) . A large multicentre retrospective study of 99 eyes
with inflammatory ocular neovascularization treated with intravitreal bevacizumab has
recently reported 12 month and 24 month results (171) . (6 out of 99 eyes had new vessels at
the disc or elsewhere rather than CNV). Forty-one patients (44 eyes) were also taking oral,
periocular, or intraocular corticosteroids or other immunosuppressive agents. Thirty-three
eyes received 0.1ml (2.5 mg) of intravitreal bevacizumab and 66 eyes received 0.05 ml
(1.25 mg). The majority of centres treated with single intravitreal injections as required,
although some centres gave a monthly injection for 3 visits and then subsequent injections
as required. Ninety-five eyes completed the 12-month follow-up with a mean gain of 2.5
lines and an average of 2.3 (+/- 1.8) bevacizumab injections (range 1–12). Best corrected
visual acuity (BCVA) worsened in 14 eyes (14.7%). So far 27 eyes have completed the 24-
month follow-up with a mean gain of 2.2 lines and an average of 3.6 (+/- 4.2) bevacizumab
injections (range 1–21). BCVA worsened in 5 eyes (18.5%).
In summary, recent evidence suggests that anti-VEGF therapy provides superior results at 2
years than previous therapies. The most commonly used protocol is to give single injections
of 0.05ml (1.25mg) of bevacizumab (Avastin) on an as required basis depending on activity
of the CNV. If there is active uveitis then concurrent treatment with systemic steroids or
other immunosuppressive agents should be included in the regime. If there is no active
uveitis then monotherapy with intravitreal bevacizumab is reasonable. There have been no
reports of intravitreal ranibizumab (Lucentis) therapy for inflammatory CNV, but on the basis
of the wet AMD trials there is likely to be a similar treatment effect. For patients who decline,
are not suitable for, or fail to respond to anti-VEGF therapy, PDT is a reasonable alternative.
It must be remembered no drug treatments have been licensed for the treatment of
inflammatory CNV and patients should be counseled to this effect. Many patients with
inflammatory CNV are young women and all of the above drug treatments should be
avoided, if possible, in pregnancy or when breast-feeding.
Uveitis NMCN Treatment Guidelines Revised September 2010
59

Appendix 3: Management of uveitis-associated glaucoma
Glaucoma in association with uveitis is relatively common. One retrospective study
identified a prevalence of 22.3% in patients with chronic uveitis at 10 year follow up (179).
Glaucoma is commoner in specific uveitic syndromes including Fuchs’ heterochromic cyclitis (180) , sarcoidosis, herpes simplex keratouveitis (181), and herpes zoster associated uveitis (181).
Most of the ocular hypotensive agents can be used for the treatment of uveitis-associated
glaucoma, in some patients topical carbonic anhydrase inhibitors appear be very effective (182). Prostaglandin analogues are relatively safe and appear to increase the uveitis activity in
only a minority of patients (183,184,185). They should however be used with caution in patients
with a history of cystoid macular oedema (186,187,188) or herpetic disease (189,190). Cyclodiode
laser has a high rate of hypotony in uveitis (19%) (191).
Laser iridotomy may provide temporary relief in secondary angle closure glaucoma,
although longer term failure rate is relatively high due to on-going inflammation. Surgical
iridectomy may be necessary. Filtration surgery is appropriate if intraocular pressure
remains high despite maximum medical therapy (192,193,194,195) .
Ideally, ocular inflammation should be controlled prior to any surgery. Anti-proliferative
agents should be used with trabeculectomy. Good results have been obtained with
glaucoma drainage implant devices (196,197,198,199).
Uveitis NMCN Treatment Guidelines Revised September 2010
60

Appendix 4: Management of uveitis in the perioperative period
Ideally ocular surgery should only be performed when the inflammation has been controlled
for a period of at least 3 months. Control may mean 1+ cells in the anterior chamber. Ensure
intraocular pressure is adequately controlled prior to surgery.
Although most uveitis specialists would agree that the use of steroid perioperatively is
efficacious, there currently doesn’t appear to be any consensus as to what this should entail.
Whether this should be oral or intravenous, pre, peri, or post-operative and if oral steroids
should be continued for a prolonged post-operative period.
One study involving 40 patients found that a two week course of oral prednisolone prior to
surgery resulted in less blood aqueous barrier break down than a single dose of intravenous
methylprednisolone in the perioperative period (200) .
One author recommends 2 hourly steroid drops for the 2 weeks preceeding surgery for
patients with relatively inactive anterior segment disease. In patients with chronic
inflammation whether or not they are already on systemic immunosuppression, he
recommends intensive topical corticosteroids as above plus a pulse of iv methylprednisolone
500mg in the immediate pre-operative period. Post-operatively 2 hourly topical
corticosteroids for a minimum of 4 weeks before considering a slow reduction. Early regular
review is important (201).
Another opinion is that in general old anterior uveitis that has been quiet for years requires
no treatment. If quiet posterior/intermediate uveitis off immunosuppression, give one dose of
500mg IV methylprednisolone intraoperatively. Patients with uveitis on immunosuppression
give 3 doses of IV methylprednisolone 500mg day before, day of and day after surgery.
Uveitis NMCN Treatment Guidelines Revised September 2010
61
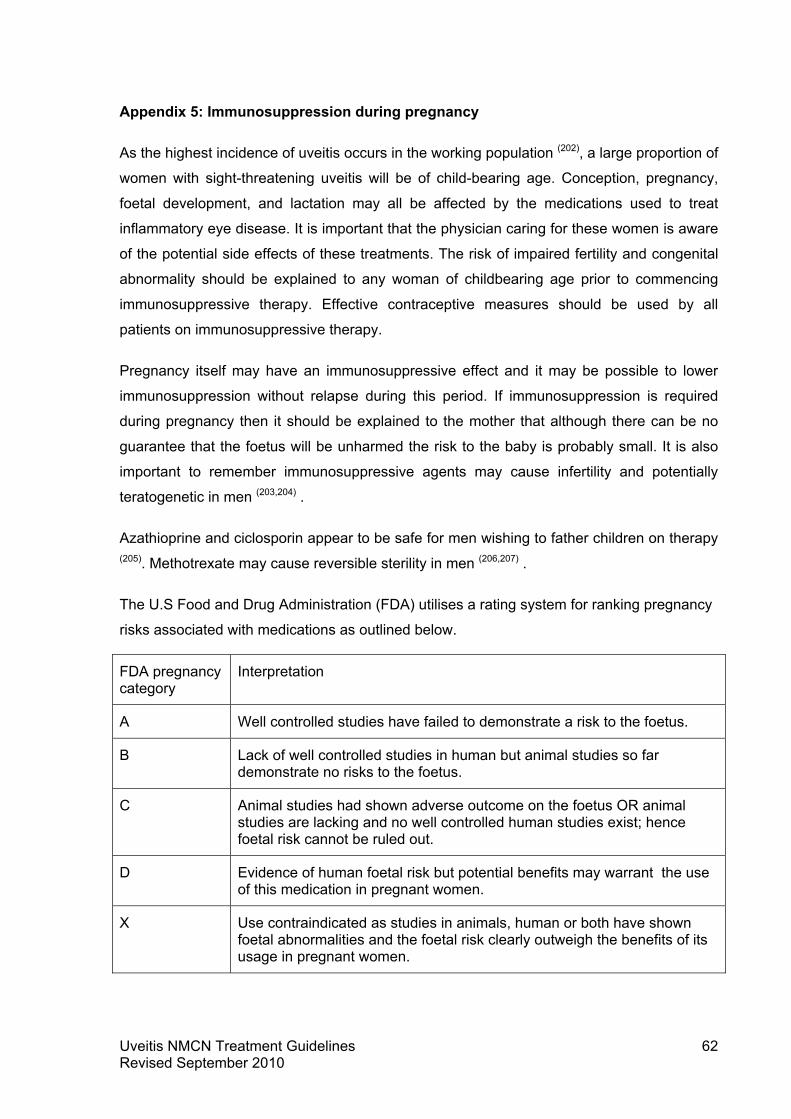
Appendix 5: Immunosuppression during pregnancy
As the highest incidence of uveitis occurs in the working population (202), a large proportion of
women with sight-threatening uveitis will be of child-bearing age. Conception, pregnancy,
foetal development, and lactation may all be affected by the medications used to treat
inflammatory eye disease. It is important that the physician caring for these women is aware
of the potential side effects of these treatments. The risk of impaired fertility and congenital
abnormality should be explained to any woman of childbearing age prior to commencing
immunosuppressive therapy. Effective contraceptive measures should be used by all
patients on immunosuppressive therapy.
Pregnancy itself may have an immunosuppressive effect and it may be possible to lower
immunosuppression without relapse during this period. If immunosuppression is required
during pregnancy then it should be explained to the mother that although there can be no
guarantee that the foetus will be unharmed the risk to the baby is probably small. It is also
important to remember immunosuppressive agents may cause infertility and potentially
teratogenetic in men (203,204) .
Azathioprine and ciclosporin appear to be safe for men wishing to father children on therapy
(205). Methotrexate may cause reversible sterility in men (206,207) .
The U.S Food and Drug Administration (FDA) utilises a rating system for ranking pregnancy
risks associated with medications as outlined below.
FDA pregnancy category
Interpretation
A Well controlled studies have failed to demonstrate a risk to the foetus.
B Lack of well controlled studies in human but animal studies so far demonstrate no risks to the foetus.
C Animal studies had shown adverse outcome on the foetus OR animal studies are lacking and no well controlled human studies exist; hence foetal risk cannot be ruled out.
D Evidence of human foetal risk but potential benefits may warrant the use of this medication in pregnant women.
X Use contraindicated as studies in animals, human or both have shown foetal abnormalities and the foetal risk clearly outweigh the benefits of its usage in pregnant women.
Uveitis NMCN Treatment Guidelines Revised September 2010
62

NSAIDS
• Can be used during pregnancy until the last 6 weeks of gestation (208,209).
• Felt to be safe while breast feeding (210,211).
Prednisolone
• FDA pregnancy category B.
• Increased risk of cleft lip and cleft palate (212).
• Important to limit to the lowest effective dosage or if possible, avoid during the first
trimester while hard palate is forming.
• After the first trimester, can be used for sight-threatening disease.
• Require “stress doses” of hydrocortisone for any emergency surgery, caesarean
section or prolonged labour.
• Monitor babies in the neonatal periods for infection or possible adrenal insufficiency
(213).
• Not contraindicated in breast feeding (214).
• Avoid breast feeding for 4 hours immediately following maternal ingestion will reduce
the amount of glucocorticoid in the milk (214).
Antimetabolites
Azathioprine
• FDA pregnancy category D.
• No significant teratogenic effect on the foetus (215).
• Prematurity, foetal growth restriction, adrenal hypoplasia and reduced serum
immunoglobulin levels have been reported (216,217,218).
• Transient neonatal leucopenia and thrombocytopenia. Reduction of dosage at 32
weeks’ gestation may decrease the risk.
Uveitis NMCN Treatment Guidelines Revised September 2010
63

• Felt to be safe in breast feeding (219,220,221,222).
Methotrexate
• FDA pregnancy category X.
• Teratogenic and therefore absolutely contraindicated in pregnancy (223,224,225)
• Reversible sterility in males.
• Discontinue at least 3 months prior to conception (214).
• If conception occurs while on treatment, methotrexate should be stopped
immediately and patient given folic acid to reduce risk of neural tube defects.
• Contraindicated in breast feeding.
Mycophenolate mofetil
• FDA pregnancy category D.
• Associated with congenital malformations and spontaneous abortions (226,227).
• Contraindicated in pregnancy.
• A negative pregnancy test is essential prior to commencement of therapy.
• FDA recommends the use of 2 reliable forms of contraception 4 weeks prior to
treatment, during treatment and 6 weeks after discontinuation of treatment.
• Contraindicated in breastfeeding.
T-cell inhibitors/Calcineurin inhibitors
Ciclosporin
• FDA pregnancy category C.
• No specific pattern of congenital malformations detected (205).
• No significant increased risk of foetal malformations (228).
• Acceptable immunosuppressant in pregnancy (229).
Uveitis NMCN Treatment Guidelines Revised September 2010
64

• The American Association of Paediatrics warns against breast feeding while on
treatment.
Tacrolimus
• FDA pregnancy category C.
• Small increase in foetal malformations but no consistent pattern (230).
• Incidence of gestational diabetes and transient neonatal hyperkalaemia reported (231).
• Transient neonatal immunosuppression.
• Safe to be used during pregnancy at therapeutic level (232).
• Secreted in breast milk and no adequate studies to determine the safety of breast
feeding, therefore breast feeding not recommended.
Alkylating agents
Cyclophosphamide
• FDA pregnancy category D.
• Teratogenic therefore contraindicated in pregnancy (233).
• Discontinue at least 3 months prior to conception.
• May result in primary ovarian failure in over 70% patients (53,56).
• Cryopreservation of oocytes should be considered.
• Contraindicated in breast feeding (234).
Biologics
Knowledge of the safety of these agents in human pregnancy is very limited and therefore
only consider these agents if benefits outweigh the potential risks.
Infliximab
• FDA pregnancy category B.
Uveitis NMCN Treatment Guidelines Revised September 2010
65

• Felt to be safe in pregnancy based on limited data.
• No increased risk of teratogenicity (TREAT registry and Infliximab Safety Database) (235).
• Should be stopped during the 3rd trimester when transplacental transfer is at its
greatest (237).
• Reports of decreased sperm motility and morphology (235).
• Infliximab is undetectable in breast milk of nursing mother, felt to be safe in breast
feeding (236,237).
Adalimumab
• FDA pregnancy category B.
• Limited data but the OTIS registry and published case reports do not suggest an
increased risk for adverse pregnancy outcomes during the 1st trimester exposure (238,239,240).
• Limited data on breast feeding, but case report shows no adverse effects to infant
whose nursing mother was on medication during pregnancy and post delivery (239).
Rituximab
• FDA pregnancy category C.
• Few case reports show low levels of B lymphocytes during the first 6 months of life,
but no reported adverse pregnancy outcome (241).
• Should only be used if benefits outweigh risks.
• Limited data on breast feeding, therefore breast feeding not recommended.
Interferon alpha
• FDA pregnancy category C.
• Limited human case reports which demonstrate no increased risk of teratogenicity (242).
Uveitis NMCN Treatment Guidelines Revised September 2010
66

• Reported cases of neonatal lupus and intrauterine growth restriction (243).
• Compatible with breast feeding (214).
Campath
• FDA pregnancy category C.
• Contraindicated in pregnancy.
• FDA suggests that women and men should use effective birth control during
treatment with Campath and for 6 months after stopping treatment.
• FDA warns against breast feeding during treatment and 3 months after stopping
treatment.
Anakinra
• FDA pregnancy category B.
• Animal studies show no evidence of foetal harms but no controlled data in human
pregnancy, therefore only recommended when benefits outweigh risks.
Uveitis NMCN Treatment Guidelines Revised September 2010
67

Appendix 6: Paediatric guidelines
Scottish Uveitis Network and Scottish Paediatric and Adolescent Rheumatology Network Joint Management and Screening Guideline for Juvenile Idiopathic Arthritis associated Uveitis, Idiopathic Paediatric Uveitis and other rare causes of uveitis in children.
This document gives guidance on the screening for Juvenile Idiopathic Arthritis associated
Chronic Anterior Uveitis (JIA CAU), and the management of JIA CAU and idiopathic
paediatric uveitis (IPU).
Very rarely uveitis occurs in children with other disease associations, such as Behcet’s
disease, sarcoid, inflammatory bowel disease, and other rare causes. The management of
these conditions is poorly evidence based, and is best done by experts with the greatest
possible knowledge of these conditions, but it is expected the management should adhere to
the principles of good uveitis and paediatric care and care pathways inherent in this
document.
Rationale
Asymptomatic CAU associated with JIA has long been recognised as an important cause of
visual loss in childhood (244,245) with high levels of complications compared to other forms of
anterior uveitis. The incidence of bilateral disease is between 67-85% (246,247,248,249) , and
complications are reported in 20-40% of children at presentation and steadily accumulate
over the first two decades of life, especially in those with persistently active disease (247,248,249,250,251,252) . In order to reduce the ocular complications early, regular, screening by
slit lamp examination has been recommended for many years, but the incidence of a poor
visual outcome remains high (16-38%) (246,247,253,254) . The current screening advice (255) ,
albeit based on limited evidence is the basis for the current screening guidance in this
document, and is in line with other guidance (256) . It has not been possible to demonstrate
unequivocally that screening programmes have reduced the frequency of either
complications at presentation, or long-term visual loss (257,258,259) , but it is becoming clearer
that early diagnosis, and early immunosuppression with an aggressive approach to removal
of inflammation are important (1, 246, 251, 253, 260, 261, 262, 263, 264, 265, 266) . Some medication choices
may be important risk factors for developing uveitis (61, 57, 134, 135, 136, 137, 138, 139, 140, 267, 268, 269, 270)
. Other risk factors are not yet clearly elucidated, poorly controlled uveitis and chronicity of
inflammation themselves presents a significant risk of cataract and glaucoma in 10- 50% of
patients in many series, and are increasingly common with longer follow-up (47, 251, 253, 261, 263,
Uveitis NMCN Treatment Guidelines Revised September 2010
68

266, 271, 272, 273, 274, 275) . Persistent ongoing application of topical steroid is also associated with
cataract and glaucoma (246, 251, 253, 261, 263, 264, 265) . There is growing evidence for the value of
early introduction of disease modifying anti-rheumatic therapies (DMARD), particularly
methotrexate (276, 277) and mycophenolate (278, 279, 280, 281) , and for early introduction of
biologic therapies, namely infliximab (57, 74, 75, 76, 282, 283, 284) or adalimumab (58, 59, 60, 62, 269) . The
majority of children with uveitis have JIA, and paediatric rheumatology services in Scotland
already manage and prescribe these drugs for the other organ manifestations of JIA. This
includes access to specialist paediatric nurses with a remit to manage and educate about
these drugs for children and parents.
These guidelines are based on an agreement between SPARN and the Uveitis Network that
joint working between these teams is a useful way forward, and that paediatric rheumatology
services are happy to support the use of these complex drugs in all children with uveitis,
including those who do not have JIA, including providing paediatric nurse specialist support
for ophthalmology services. Whilst the networks accept this guidance is not fully evidence
based they are current best practise and are adopted by both networks until more definitive,
evidence based guideline is developed.
Core principles:
Communication
In each region key personnel caring for paediatric uveitis and providing screening should
be clearly identified through both SPARN and the uveitis network.
• For eye screening identified paediatric ophthalmologists would usually be the key
lead for each region.
• The management of paediatric uveitis is expected to be undertaken by an
ophthalmologist who has expertise in the management of uveitis, but who should
be properly supported by paediatric services, including specialist paediatric
nursing support in line with current standards of care (286, 287,288) . This will usually
be through the local paediatric rheumatology service. In some regions the same
individuals may provide both screening and uveitis care. It is essential that all
children are seen in an appropriate paediatric environment supported by
appropriately trained paediatric staff, even where occasional component of care
takes place unavoidably in an adult setting. In many regions paediatric
Uveitis NMCN Treatment Guidelines Revised September 2010
69

ophthalmologists may do the screening, day to day uveitis care, liasing with
uveitis experts as required.
• Rapid, consistent and complete two way communication between the
ophthalmologist and the paediatric rheumatologist / paediatric rheumatology services
is key to an effective screening service. Both services will need to have good
knowledge of the screening guidelines, with awareness of decisions that alter the
screening requirements for an individual patient.
• Uveitis care requires the same high level of communication.
• Planned transition to adult services aims to involve both adult rheumatology and
ophthalmology services (285) .
• The following is considered a core set of information to be included in all
correspondence, or immediately accessible from shared clinical notes, from both
ophthalmologists and rheumatologist includes:
o Next planned appointment
o All systemic and topical medication, whether or not given for eyes. Systemic
treatment given for JIA or other systemic disease association should be
recorded in the ophthalmology notes whether or not it is given for eye
complications.
o All changes in systemic and topical medication particularly cessation of
treatments.
o Ophthalmologists should record at each visit in the clinical notes, and where
the clinical notes are not shared with the rheumatology team, communicate
the following to the rheumatology team in numerical values, vague or
descriptive terms should be avoided: visual acuity, the presence and absence
of uveitis, and the severity of uveitis using the SUN criteria (289) recording the
actual number of cells using a 1mm circular beam set at 45 degrees, bright
light and high magnification. Flare should be recorded. For the
measurement of intraocular pressures proxymetacaine should be used and a
gentle examination performed. Goldman is preferred (290) . This may be
difficult in the very young and the failure to record pressures should be
documented. The appearance of the optic disc, and the macular if the vision
Uveitis NMCN Treatment Guidelines Revised September 2010
70
o Those providing screening should be able to provide rapid access to
examination under anaesthetic where examination is difficult in line with
current standards of care (255) . To minimise the number of general
anaesthetics ideally a shared general anaesthetic with rheumatology services
providing joint injections wherever possible.
o Rheumatologists should urgently highlight to the ophthalmologist any
changes in medication or diagnostic details that materially alter the screening
programme required (255) . The paediatric rheumatologist should be aware of
the implication to the management of the eyes that changes in treatment for
other aspects of JIA care will make, and where this is unclear should make
this decision in conjunction with the ophthalmologist.
o It should be avoided that ophthalmologists and rheumatologists are both
prescribing disease modifying drugs (DMARDS) or biologics for different
aspects of JIA care. The lead clinician for prescribing should be formally
identified, and should normally be the paediatric rheumatologist unless
otherwise agreed in writing, and appropriate paediatric nursing support
provided.
o All communication should be sent within two weeks of clinical review in line
with current guidance.
Uveitis Screening
JIA CAU Screening guidelines have been produced jointly by BSPAR and the RCPOphth in
2006 (255) (appendix 7). Whilst these are not fully evidence based they are current best
practise and are adopted by both networks until more definitive, evidence based guideline is
developed. Both rheumatology and ophthalmology services should be aware of these
guidelines, and ensure changes in diagnosis or management are effectively communicated
to the other services to facilitate adherence to these guideline. In Scotland geographical
issues are not an acceptable barrier to meeting screening needs. Where screening is
provided by training ophthalmology doctors they should be aware of their responsibilities
under the screening guidelines, and should not deviate from the screening guideline unless
this is a consultant led decision and communicated to the paediatric rheumatology team.
Uveitis NMCN Treatment Guidelines Revised September 2010
71
Management of JIA CAU and IPU
The management of paediatric uveitis differs from adult uveitis in that an earlier and more
aggressive approach to the introduction of DMARDS and biologics is found (47, 57, 58, 59, 60, 62, 74,
75, 76, 140, 259, 269, 271, 272, 273, 276, 277, 278, 280, 281, 282, 283, 284) . The algorithm demonstrates the key
pathways agreed includes time lines for rapid progression through treatment regimes but
acknowledges the lack of evidence base for this (1, 246, 251, 253, 261, 262, 263, 264, 265, 266, 271) . Key
red flags for concern are considered to be:
o Persistent requirement of topical steroids after 4 months, with or without a DMARD
o Presence of macular oedema or posterior involvement.
Detailed discussion points from the algorithm:
Differences between the management of uveitis in adults and children include:
1) Steroids
a. In children a very cautious approach to even low dose topical steroid is
usually taken (because of the risk of glaucoma and cataract) (135, 246, 251, 253, 261,
263, 264, 291, 292) . In severe inflammation where high dose frequent application
of topical prednisolone is required earlier introduction of DMARDS or more
rapid progression through the algorithm is appropriate.
b. Once control is achieved it is expected that low dose topical and systemic
steroid will be withdrawn before weaning off the second line agent. The
second line agents are usually given for a longer time period than is usual in
adult uveitis, and may be required indefinitely.
2) Biologics: In children progress to a biologic agent is usual after the first second-line
agent has failed.
Paediatric Nursing Care
Children receiving DMARDS or biologic agents are expected to have
o Access to identified trained paediatric nursing care with expertise in the management
of these drugs including skills in education, monitoring and training of families
appropriate for the care of children (286, 287, 288) .
Uveitis NMCN Treatment Guidelines Revised September 2010
72
o The paediatric nurse has a key role in coordinating both the PR and ophthalmology
teams. One team (usually paediatric rheumatology because of their role in prescribing
immunosuppression for other organ involvement) is formally responsible for the
monitoring and prescribing of these drugs.
Drug Monitoring
DMARDs and biologics are expected to be formally monitored. The BSPAR and RCN
guidelines on the use of these drugs, including doses and monitoring guidelines, are
appropriate guidance to follow for these patients (287, 288, 293) .
Choice of DMARD
The usual choices of DMARD would be methotrexate or mycophenolate (259, 276, 277, 278, 279, 280,
281) . The rationale for the choice may be influenced by the other features of JIA, such as
joint involvement where methotrexate is usually the preferred choice, mycophenolate has
poorer efficacy for synovitis (281) , whereas where eye features predominate mycophenolate
may be the preferred choice. Whichever is chosen first if the response to DMARD treatment
is unacceptable a biologic would usually be the next choice rather than the other DMARD.
Methotrexate is also used as the first choice in conjunction with the biologic agents
infliximab and adalimumab to reduce allergic reactions, and may improve the efficacy of
these drugs for JIA and uveitis (57, 61, 269) although adalimumab is licensed for use on it’s own.
Choice of Biologic
The current first choices for which there is evidence of efficacy are of an anti-TNF. The
choice is between infliximab (75, 76, 282, 283, 284) or adalimumab (57, 58, 59, 60, 61, 62, 76, 269, 282, 283) .
There is a current lack of evidence base to guide choice between either of these, and
practical or patient related issues around administration often influence the choice. The
licences suggest these should be given with a DMARD, usually methotrexate. Where the
response to one is inadequate or significant side-effects occur the other may be tried. The
anti-TNF etanercept should be avoided in uveitis because of lack of efficacy and some
suggestion that it might worsen inflammation in uveitis (57, 61, 135, 136, 137, 138, 139, 140, 252, 267, 268, 269,
270) .
Macular oedema
The assessment of macular oedema is difficult in children. If the vision is reduced it is
appropriate to assume that macular oedema is present, until proven otherwise. Initially oral
steroid can be given, but in severe cases intravenous pulsed methylprednisolone may be
Uveitis NMCN Treatment Guidelines Revised September 2010
73

most appropriate. Concurrent commencement or escalation of DMARDS or biologics is
appropriate.
Time lines for moving through the algorithm
These are the longest time periods felt acceptable before moving through the algorithm.
Where severe disease persists, vision is threatened, glaucoma has developed, or
unacceptable doses of topical or systemic steroids are required it is appropriate to move
more rapidly to the next stage of the algorithm.
Uveitis NMCN Treatment Guidelines Revised September 2010
74
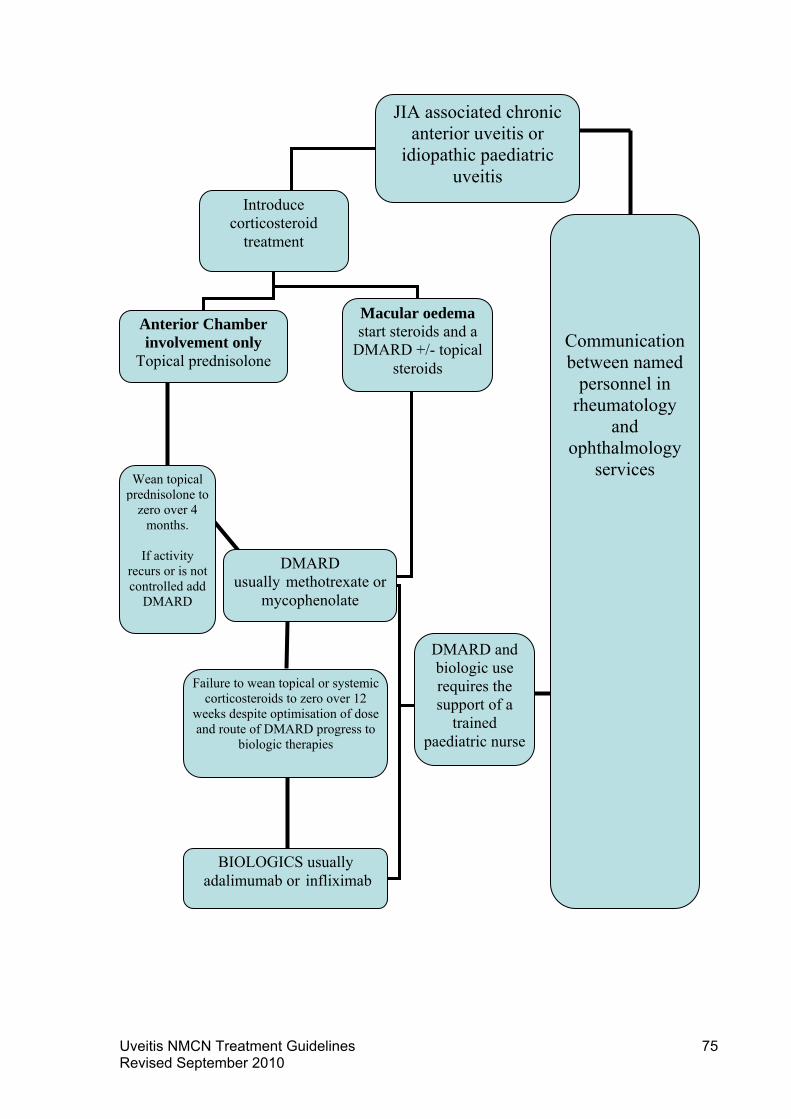
JIA associated chronic anterior uveitis or
idiopathic paediatric uveitis
Introduce corticosteroid
treatment
Communication between named
personnel in rheumatology
and ophthalmology
services
Failure to wean topical or systemic corticosteroids to zero over 12
weeks despite optimisation of dose and route of DMARD progress to
biologic therapies
BIOLOGICS usually adalimumab or infliximab
DMARD and biologic use requires the support of a
trained paediatric nurse
Wean topical prednisolone to
zero over 4 months.
If activity
recurs or is not controlled add
DMARD
Macular oedema start steroids and a
DMARD +/- topical steroids
DMARD usually methotrexate or
mycophenolate
Anterior Chamber involvement only
Topical prednisolone
Uveitis NMCN Treatment Guidelines Revised September 2010
75

Appendix 7: Guidelines for Screening for Uveitis in Juvenile Idiopathic Arthritis (JIA)
Produced jointly by BSPAR and the RCPOphth 2006
Aim of the screening programme
To reduce the incidence of visual impairment among children and young people with juvenile
idiopathic arthritis (JIA) by early detection through screening allowing for early intervention.
Background
The prevalence of uveitis in JIA overall is approximately 8-30%, but in young oligoarticular
onset group (ie arthritis in which up to 4 joints are involved) it may be as high as 45-57%.
The annual incidence of JIA in the UK is 1:10,000 with a prevalence of 1:1000. The type of
arthritis and age at onset dictates the risk of developing uveitis. Only the highest risk groups
are included in the regular screening recommendations below. However, late onset of first
uveitis can occur even in young adults and cases have been reported in systemic JIA so it is
important to make clinical referrals for ophthalmology assessment in patients where there
are clinical concerns even if the patient is not specifically covered by these screening
guidelines.
The uveitis in JIA is asymptomatic and therefore screening by slit-lamp is essential for
diagnosis. Visual impairment arises mainly from complications of the uveitis including
cataract, glaucoma, macular oedema and hypotony. Once complications have arisen they
are often irreversible. Early detection and treatment can prevent the development of
complications and can prevent permanent visual impairment. These complications are more
frequent and more severe in younger children and are often asymptomatic. The most
frequent cause of avoidable morbidity remains missed or inadequate examinations in the first year of disease and all efforts must be made to achieve early and thorough early examinations.
Principles
1) Initial screening examination Uveitis often starts soon after onset of arthritis but may
also start before the arthritis. The initial screening examination is therefore a clinical priority and should occur as soon as possible and no later than 6 weeks from referral. (
Reference the BSPAR Standards of Care.)
2) Symptomatic patients or patients suspected of cataracts or synechiae should be seen
within a week of referral.
Uveitis NMCN Treatment Guidelines Revised September 2010
76

3) Difficult examinations If the patient is uncooperative at initial screening or for an urgent
symptomatic examination in a young child an examination under anaesthetic should be
considered.
4) Parent information Parents and carers of children with JIA need to be fully informed
about the possibility of uveitis and that this is usually an asymptomatic condition until
complications arise. They need to be told that a high street optician assessment is not an
adequate examination to exclude uveitis. They should be instructed to seek medical
assessment urgently if their child develops visual symptoms or signs. These include red
eyes, photophobia, abnormal pupils, corneal clouding, or visual impairment. In younger
children this may be manifest by unusual blinking, eye rubbing, visual inattention or
preferential attention on auditory signals, or a new onset squint.
5) Missed appointments Parents and carers must be fully informed about the method of
screening and the need to attend for specific uveitis screening examinations on a regular
basis. Arrangements need to be in place to give priority to rebooking of any missed
appointments in this group with a system of contacting non-attenders.
6) Training Ophthalmologists and other health professionals carrying out uveitis screening
should be appropriately trained and experienced. They should have facilities to audit the
outcomes of their screening program.
7) Older patients Older teenage patients need to be told to return quickly should they
become symptomatic. If there is concern about their reliability, e.g. in developmental delay,
then they should be considered for longer term less frequent screening. After discharge from
the screening programme an annual check by an optometrist is a useful adjunct to self-
monitoring for symptoms.
8) On stopping immunosuppressant treatment such as Methotrexate
Patients who have been treated with methotrexate for their arthritis may not have developed
uveitis due to drug suppression. However after methotrexate is stopped uveitis may flare.
Screening should therefore restart at 2 monthly intervals after stopping Methotrexate or any
other immunosuppressant therapy during the period of maximum risk for 6 months before
reverting to the previous screening arrangements.
Scottish addition: Where a child is started on etanercept alone in the absence of
methotrexate the ophthalmologist should be aware of the possible increased risk in
Uveitis NMCN Treatment Guidelines Revised September 2010
77

developing uveitis, or worsening severity of pre-existing uveitis and return to 2 monthly
screening for 6 months.
Specific Screening Schedules
These schedules are the best recommendation possible with current data and are focused on the highest risk groups.
First screening within 6 weeks of referral
Two monthly intervals from onset of arthritis for 6 months
Scottish simplification: Then 3-4 monthly screening until their 12th birthday.
Older patients presenting for the first time after the age of 11, should undergo one year of
screening.
When a patient is discharged from the regular screening program it is vital to stress to
them that they and the family are now deemed able to detect any changes in their vision
which may signify a new onset or flare of uveitis. It does NOT mean that their risk of uveitis
has gone completely. A tip for family self monitoring is to remind the young person to check
his or her vision uniocularly- eg by reading small print with each eye once a week.
Monitoring may need to continue indefinitely if there are other reasons such as learning
difficulties or treatment non-compliance when the young person may be unable to detect a
change in vision or unwilling to seek re-referral.
Systemic onset JIA and definite rheumatoid factor positive polyarticular JIA patients are at
very low risk of uveitis. However, there may be delay in being certain about the diagnosis or
exact category of JIA, and overlaps between groups do occur. For this reason an initial
screening examination may be indicated.
Some important facts about uveitis in JIA
Boys do get severe uveitis
ANA negative patients get significant uveitis
Uveitis does occur in young patients with psoriatic arthritis
Patients with polyarticular JIA do get uveitis.
Uveitis NMCN Treatment Guidelines Revised September 2010
78

Patients with enthesitis related arthritis may get chronic as well as acute iritis.
Scottish modification Nov 2009
Uveitis NMCN Treatment Guidelines Revised September 2010
79

Appendix 8: Membership of NMCN treatment guideline development group and stakeholders group
Uveitis national managed clinical network treatment guideline development group
Dr Graeme Williams Consultant Ophthalmic Physician, Gartnavel General Hospital,
Glasgow
(Chair)
Dr John Olson Consultant Ophthalmic Physician, Aberdeen Royal Infirmary
(NMCN Lead Clinician)
Ms Frances Philip, MCN Support Manager, Woolmanhill Hospital, Aberdeen
(NMCN Support Manager)
Dr Neil Basu Honorary Consultant Rheumatologist, Aberdeen Royal Infirmary
Dr Chee Peng Cheng Medical Ophthalmology Specialty Registrar, Gartnavel General
Hospital, Glasgow
Dr Nicholas Fluck Consultant Nephrologist, Aberdeen Royal Infirmary
Dr Janet Gardner-Medwin Senior Lecturer in Paediatric Rheumatology, Royal Hospital
for Sick Children, Glasgow
Dr Catherine Guly Medical Ophthalmology Specialty Registrar, Aberdeen Royal
Infirmary
Dr Fraser Imrie Consultant Ophthalmologist, Gartnavel General Hospital, Glasgow
Uveitis national managed clinical network stakeholders group
Dr Stuart Roxburgh Consultant Ophthalmologist, Ninewells Hospital Dundee
(Chair)
Dr John Olson Consultant Ophthalmic Physician, Aberdeen Royal Infirmary
(NMCN Lead Clinician)
Mrs Lorraine Urquhart, Managed Clinical Network Manager, Woolmanhill Hospital,
Aberdeen
(NMCN Manager)
Uveitis NMCN Treatment Guidelines Revised September 2010
80

Ms Frances Philip, MCN Support Manager, Woolmanhill Hospital, Aberdeen
(NMCN Support Manager)
Dr Neil Basu Honorary Consultant Rheumatologist, Aberdeen Royal Infirmary
Mr Donald Cameron Independent Optometrist, Optometry Scotland
Professor Bal Dhillon Consultant Ophthalmologist, Princess Alexandra Eye Pavilion,
Edinburgh
Dr Suzanne Brannan Consultant Ophthalmologist, Queen Margaret Hospital,
Dunfermline
Dr Brian Fleck Consultant Ophthalmologist, Princess Alexandra Eye Pavilion,
Edinburgh
Professor Forrester Professor of Ophthalmology, University of Aberdeen
Dr Janet Gardner-Medwin Senior Lecturer in Paediatric Rheumatology, Royal Hospital
for Sick Children, Glasgow
Dr Catherine Guly Medical Ophthalmology Specialty Registrar, Aberdeen Royal
Infirmary
Mr Phil Hibbert Founder, Uveitis Information Group
Dr Simon Hewick Consultant Ophthalmologist, Raigmore Hospital, Inverness
Dr Fraser Imrie Consultant Ophthalmologist, Gartnavel General Hospital, Glasgow
Ms Angela James Ophthalmology Pharmacist, Princess Alexandra Eye Pavilion,
Edinburgh
Mr Allan Jones Edinburgh & The Lothians Operations Manager, RNIB Scotland
Dr Lucia Kuffova Senior Lecturer in Ophthalmology, University of Aberdeen
Mr John Legg Director of RNIB Scotland
Mrs Ali McAllister Project Office Standards Development Team, NHS Quality
Improvement Scotland
Mrs Gill Ogden Uveitis Nurse Specialist, Queen Margaret Hospital, Dunfermline
Uveitis NMCN Treatment Guidelines Revised September 2010
81

Dr Sheila Paterson-Brown Associate Specialist in Ophthalmology, Princess Alexandra
Eye Pavilion, Edinburgh
Miss Vanessa Sandison Clinic Nurse Manager, Aberdeen Royal Infirmary
Dr Angus Scott Consultant Ophthalmologist, Stirling Royal Infirmary
Miss Caroline Smith Patient Representative
Mrs Fiona Smith Patient Representative
Mr James Stephen Programme Manager, National Services Division, NHS National
Services Scotland
Dr Mohan Varikkara Consultant Ophthalmologist, Ayr Hospital
Dr Meena Virdi Consultant Ophthalmologist, Hairmyres Hospital, East Kilbride
Mrs Carri-Anne Walker Director of Fundraising, Uveitis Information Group
Dr Graeme Williams Consultant Ophthalmic Physician, Gartnavel General Hospital,
Glasgow
Dr Imran Zaheer Consultant Ophthalmologist, Dumfries Infirmary
Uveitis NMCN Treatment Guidelines Revised September 2010
82
Appendix 9: Evidence Base
1. Jabs DA, Rosenbaum JT, Foster CS et al. Guidelines for the use of
immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations
of an expert panel. Am J Ophthalmol 2000; 130 : 492–513.
2. Dana M, Merayo-Lloves J, Schaumberg DA, et al. Prognosticators for visual outcome
in sarcoid uveitis. Ophthalmol 1996;103:1846-1853.
3. Conn HO, Blitzer BL. Nonassociation of adrenocorticosteroid therapy and peptic
ulcer. N Engl J Med 1976;294:473–479.
4. Piper JM, Ray WA, Daugherty JR, Griffin MR. Corticosteroid use and peptic ulcer
disease: role of nonsteroidal anti-inflammatory drugs. Ann Intern Med 1991;114:735– 740.
5. Fujikawa LS, Meisler DM, Nozik RA. Hyperosmolar hyperglycemic nonketotic coma.
A complication of short-term systemic corticosteroid use. Ophthalmology. 1983;90:1239–
1242.
6. Covar RA, Leung DY, McCormick D, et al. Risk factors associated with
glucocorticoidinduced adverse effects in children with severe asthma. J Allergy Clin
Immunol. 2000; 106:651–659.
7. Sholter DE, Armstrong PW. Adverse effects of corticosteroids on the cardiovascular
system. Can J Cardiol. 2000;16:505–511.
8. Patten SB, Neutel CI. Corticosteroid-induced adverse psychiatric effects: incidence,
diagnosis and management. Drug Saf. 2000;22:111–122.
9. Wolkowitz OM, Reus VI, Canick J, et al. Glucocorticoid medication, memory and
steroid psychosis in medical illness. Ann NY Acad Sci. 1997;823:81–96.
10. Pasadhika, S., Kempen, JH., Newcomb, CW., Liesegang, TL., Pujari, SS.,
Rosenbaum, JT., Thorne, JE., Foster, CS., Jabs, DA., Levy-Clarke, GA., Nussenblatt, RB.,
Suhler, EB. Azathioprine for Ocular Inflammatory Diseases. Am J Ophthalmol 2009;148:500
–509.
11. Yazici H, Pazarli H, Barnes CG, et al. A controlled trial of azathioprine in Behcet’s
syndrome. N Engl J Med. 1990;322:281–285.
Uveitis NMCN Treatment Guidelines Revised September 2010
83

12. Hamuryudan V, Ozyazgan Y, Hizli N, et al. Azathioprine in Behcet’s syndrome:
effects on long-term prognosis. Arthritis Rheum. 1997;40:769–774.
13. Newell FW, Krill AE. Treatment of uveitis with azathioprine (Imuran). Trans
Ophthalmol Soc UK. 1967;87:499–511.
14. Andrasch RH, Pirofsky B, Burns RP. Immunosuppressive therapy for severe chronic
uveitis. Arch Ophthalmol 1978; 96:247–251.
15. Azici J, Pazarli H, Barnes CG, et al. A controlled trial of azathioprine in Behcet’s
syndrome. N Engl J Med 1990;322: 81–285.
16. Hooper PI, Kaplan HJ. Triple agent immunosuppression serpiginous choroiditis.
Ophthalmology 1991;98:944 –951.
17. Akpek EK, Baltatzis S, Yang J, et al.: Long-term immunosuppressive treatment of
serpiginous choroiditis. Ocul Immunol Inflamm 2001, 9:153–167.
18. Michel SS, Ekong A, Baltatzis S, et al. Multifocal choroiditis and panuveitis:
immunomodulatory therapy. Ophthalmology. 2002;109:378–383.
19. Gion N, Stavrou P, Foster CS. Immunomodulatory therapy for chronic
tubulointerstitial nephritis-associated uveitis. Am J Ophthalmol. 2000;129:764–768.
20. Kempen, JH., Daniel, E., Dunn, JP., Foster, CS., Gangaputra, S., Hanish, A.,
Helzlsouer, KJ., Jabs, DA., Kaçmaz, RO., Levy-Clarke, GA., Liesegang, TL., Newcomb,
CW., Nussenblatt, RB., Pujari, SS., Rosenbaum,JT., Suhler, EB., Thorne, JE. Overall and
cancer related mortality among patients with ocular inflammation treated with
immunosuppressive drugs: retrospective cohort study. BMJ 2009;339:b2480
21. Gangaputra, S., Newcomb, CW., Liesegang, TL., Oktay Kaçmaz, R., Jabs, DA.,
Levy-Clarke, GA., Nussenblatt, RB., Rosenbaum, JT., Suhler, EB., Thorne, JE., Foster, CS.,
Kempen, JH. for the Systemic Immunosuppressive Therapy for Eye Diseases Cohort Study.
Methotrexate for Ocular Inflammatory Diseases. Ophthalmol 2009;116:2188–2198.
22. Samson CM, Waheed N, Baltatzsis S, et al. Methotrexate therapy for chronic non-
infectious uveitis: analysis of a case series of 160 patients. Ophthalmology. 2001;108:1134–
1139.
23. Bom S, Zamiri P, Lightman S. Use of methotrexate in the management of sight
threatening uveitis. Ocul Immunol Inflamm. 2001;9:35–40.
Uveitis NMCN Treatment Guidelines Revised September 2010
84

24. Van Gelder RN, Kaplan HJ. Immunosuppression in uveitis therapy. Springer Semin
Immunopathol. 1999;21:179–190.
25. Dev S, McCallum RM, Jaffe GJ. Methotrexate treatment for sarcoid-associated
panuveitis. Ophthalmology. 1999;106:111–118.
26. Weiss AH, Wallace CA, Sherry DD. Methotrexate for resistant chronic uveitis in
children with juvenile rheumatoid arthritis. J Pediatr. 1998;133:266–268.
27. Holz FG, Krastel H, Breitbart A, et al. Low-dose methotrexate treatment in non-
infectious uveitis resistant to corticosteroids. Ger J Ophthalmol. 1992;1:142–144.
28. Larkin G, Lightman S. Mycophenolate mofetil. A useful immunosuppressive in
inflammatory eye disease. Ophthalmology 1999;106:370 –374.
29. Kilmartin DJ, Forrester JV, Dick AD. Rescue therapy with mycophenolate mofetil in
refractory uveitis. Lancet 1998; 352:35–36.
30. Lau CH, Comer, M, Lightman S. Long-term efficacy of mycophenolate mofetil in the
control of severe intraocular inflammation. Clinical Exp Ophthalmol 2003; 31: 487–491
31. Thorne, JE., Jabs, DA., Qazi, FA., Nguyen, QD., Kempen, JH., James P. Dunn, JP.
Mycophenolate Mofetil Therapy for Inflammatory Eye Disease. Ophthalmol. 2005; 112:1472–1477.
32. Galor, A., Jabs, DA., Leder, HA., Kedhar, SR., Dunn, JP., Peters III, GB.,Thorne, JE.
Comparison of Antimetabolite Drugs as Corticosteroid-Sparing Therapy for
Noninfectious Ocular Inflammation. Ophthalmol 2008;115:1826–1832.
33. Nussenblatt RB, Palestine AG, Chan CC. Cyclosporine A therapy in the treatment of
intraocular inflammatory disease resistant to systemic corticosteroids and cytotoxic agents.
Am J Ophthalmol 1983;96:275–282.
34. Whitcup SM, Salvo EC Jr, Nussenblatt RB. Combined cyclosporine and
corticosteroid therapy for sight-threatening uveitis in Behcet’s disease. Am J Ophthalmol.
1994;118:39–45.
35. Walton RC, Nussenblatt RB, Whitcup SM. Cyclosporine therapy for severe
sightthreatening uveitis in children and adolescents. Ophthalmology. 1998;105:2028–2034.
Uveitis NMCN Treatment Guidelines Revised September 2010
85

36. Nussenblatt RB, Palestine AG, Chan CC, et al. Effectiveness of cyclosporine therapy
for Behçet’s disease. Arthritis Rheum 28:672, 1985.
37. Nussenblatt RB, de Smet MD, Rubin B, et al. A masked, randomized, dose-response
study between cyclosporine A and G in the treatment of sight-threatening uveitis of
noninfectious origin. Am J Ophthalmol. 1993;115:583–591.
38. de Vries J, Baarsma GS, Zaal MJ, et al. Cyclosporin in the treatment of severe
chronic idiopathic uveitis. Br J Ophthalmol. 1990;74:344–349.
39. Caspers-Velu LE, Decaux G, Libert J. Cyclosporine in Behcet’s disease resistant to
conventional therapy. Ann Ophthalmol. 1989;21:111–116, 118.
40. Vitale AT, Rodriguez A, Foster CS. Low-dose cyclosporin A therapy in treating
chronic,noninfectious uveitis. Ophthalmology. 1996;103:365–373.
41. Nussenblatt RB, Palestine AG, Chan CC, et al. Randomized double-masked study of
cyclosporine compared to prednisone in the treatment of endogenous uveitis. Am J
Ophthalmol 1991;112:138 –146.
42. Palestine AG, Austin HA III, Balow JE, et al. Renal histopathologic alterations in
patients treated with cyclosporine for uveitis. N Engl J Med 1986;314:1293–1298.
43. Mochizuki M, Masuda K, Sakane T, et al. A clinical trial of FK506 in refractory uveitis.
Am J Ophthalmol 1993;115: 763–769.
44. Ishioka M, Ohno S, Nakamura S, et al. FK506 treatment of noninfectious uveitis. Am
J Ophthalmol 1994;118:723– 729.
45. Kilmartin DJ, Forrester JV, Dick AD. Tacrolimus (FK506) in failed cyclosporine A
therapy in endogenous posterior uveitis. Ocul Immunol Inflamm 1998;6:101–109.
46. Sloper CM, Powell RJ, Dua HS. Tacrolimus (FK506) in the treatment of posterior
uveitis refractory to cyclosporine. Ophthalmology 1999;106:723–728.
47. Murphy CC, Greiner K, Plskova J, Duncan L, Frost NA, Forrester JV, Dick AD.
Cyclosporine vs Tacrolimus Therapy for Posterior and Intermediate Uveitis. Arch
Ophthalmol 2005; 123: 634-641.
Uveitis NMCN Treatment Guidelines Revised September 2010
86

48. Lacki JK, Schochat T, Sobieska M. Immunological studies in patients with
rheumatoid arthritis treated with methotrexate or cyclophosphamide. Rheumatol
1994;53:76–82.
49. Lapraik, C., Watts, R., Bacon, P., Carruthers, D., Chakravarty, K., D’Cruz, D.,
Guillevin, L., Harper, L., Jayne, D., Luqmani, R., Mooney, J., Scott, D. BSR and BHPR
guidelines for the management of adults with ANCA associated vasculitis. Rheumatology
2007;46:1–11.
50. Buckley CE, Gills JP. Cyclophosphamide therapy of peripheral uveitis. Arch Intern
Med 1969;124:29 –35.
51. Buckley CE 3rd, Gills JP Jr. Oral cyclophosphamide in the treatment of uveitis. Trans
Am Acad Ophthalmol Otolaryngol. 1970;74:505–508.
52. Ozyazgan Y, Yurdakul S, Yaziei H, et al. Low dose cyclosporin A versus pulsed
cyclophosphamide in Behçet’s syndrome: a single masked trial. Br J Ophthalmol.
1992;76:241–243.
53. Boumpas DT, Austin HA, Vaughn EM, Yarboro CH, Klippel JH, Balow JE. Risk for
sustained amenorrhea in patients with systemic lupus erythematosus receiving intermittent
pulse cyclophosphamide therapy. Ann Intern Med. 1993;119:366-369.
54. Blumenfeld A, Avivi I, Ritter M, Rowe JM. Preservation of fertility and ovarian
function and minimizing chemotherapy- induced gonadotoxicity in young women. J Soc
Gynecol Invest 1999;6:229 –239.
55. Blumenfeld A, Avivi I, Linn S, Epelbaum R, Ben-Shahar M, Haim N. Prevention of
irreversible chemotherapy-induced damage in young women with lymphoma by a
gonadotropin- releasing hormone agonist in parallel to chemotherapy. Human Reproduction
1996;11:1620 –1626.
56. Slater CA, Liang MH, McCune JW, Christman GM, Laufer MR. Preserving ovarian
function in patients receiving cyclophosphamide. Lupus. 1999;8:3-10.
57. Tynjälä P, Lindahl P, Honkanen V, Lahdenne P, Kotaniemi K. Infliximab and etanercept
in the treatment of chronic uveitis associated with refractory juvenile idiopathic arthritis. Ann
Rheum Dis. 2007 Apr;66(4):548-50.
58. Tynjälä P, Kotaniemi K, Lindahl P, Latva K, Aalto K, Honkanen V, Lahdenne P.
Adalimumab in juvenile idiopathic arthritis-associated chronic anterior uveitis.
Uveitis NMCN Treatment Guidelines Revised September 2010
87

Rheumatology (Oxford). 2008 Mar;47(3):339-44.
59. Vazquez-Cobian, LB, Flynn T, Lehman TJ. Adalimumab therapy for childhood
uveitis. J Pediatr 2006;149:572-5
60. Gallagher M, Quinones K, Cervantes-Casteneda RA et al. Biological response
modifier therapy for refractory childhood uveitis Br J Ophthalmol 2007;91:1341-1344.
61. Biester S, Deuter C, Michels H, Haefner R, Kuemmerle-Deschner J, Doycheva D,
Zierhut M.Adalimumab in the therapy of uveitis in childhood. Br J Ophthalmol. 2007
Mar;91(3):319-24.
62. Diaz-Llopis M, Garcia-Delpéche S, Salom D et al. Adalimumab therapy for refractory
uveitis: a pilot study J Ocular Pharm Therapeut 2008;24:351-361.
63. Mushtaq B, Saeed T, Situnayake RD et al. Adalimumab for sight threatening uveitis
in Behects disease Eye 2007 ;21:824-825
64. Breedveld F, Weisman MH, Kavanaugh AF et al. A multicentre, randomised double
blind clinical trial of combination therapy with adalimumab plus methotrexate versus
methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid
arthritis who had not had previous methotrexate treatment. Arthritis Rheum 2006;54:26-37
65. Schiff MH, Burmester GR, Kent JD et al. Safety analyses of Adalimumab (HUMIRA)
in global clinical trials and US post-marketing surveillance of patients with rheumatoid
arthritis. Ann Rheum Dis 2007;66:2-26.
66. Esteve M, Saro C, González-Huiz F et al. Hepatitis B reactivation following infliximab
therapy in Crohn’s disease patients: need for primary prophylaxis Gut 2004;53:1363-1365.
67. Ostuni P, Bostios C, Punzi L et al. Hepatitis B reactivation in a chronic hepatitis B
surface antigen carrier with rheumatoid arthritis treated with infliximab and low dose
methotrexate. Ann Rhem Dis 2003;62:686-687.
68. Nathan DM, Angus PW, Gibson PR. Hepatitis B and C infections and anti-tumor
necrosis factor-α therapy: Guidelines for clinical approach. J Gastroenterol Hepatol
2006;21:1366-1371
69. Suhler EB, Smith JR,Wertheim MS, Lauer AK, Kurz DE, Pickard TD, Rosenbaum JT.
A Prospective Trial of Infliximab Therapy for Refractory Uveitis. Preliminary Safety and
Efficacy Outcomes. Arch Ophthalmol. 2005;123:903-912.
Uveitis NMCN Treatment Guidelines Revised September 2010
88
70. Sfikakis PP, Kaklamanis PH, Elezogiou A, et al. Infliximab for recurrent, sight
threatening ocular inflammation in Adamantiades-Behcet disease. Ann Intern Med.
2004;140:404–406.
71. Benitez-del-Castillo JM, Martinez-de-la-Casa JM, Pato-Cour E. Long term treatment
of refractory posterior uveitis with anti-TNFα (inflximab). Eye 2005;19:841-845.
72. Niccoli L, Nannini C, Bennuci M et al. Long term efficacy of infliximb in refractory
posterior uveitis of Behcets disease: a 24 month follow up study. J Rheumatol
2007:46:1161-1164.
73. Tugal-Tutkun I, Mundun A, Urgancioglu M et al. Efficacy of infliximab in the treatment
of uveitis that is resistant to treatment with the combination of azathioprine, cyclosporin, and
corticosteroids in Behcets disease. Arthritis Rheum 2005;52:2478-2484.
74. Kahn P, Weiss M, Imundo LF et al. Favourable response to high-dose infliximab for
childhood uveitis. Ophthalmology 2006;113:860-864
75. Ardoin SP, Kredich D, Rabinovich E et al. Infliximab to treat chronic non-infectious
uveitis in children: retrospective case series with long term follow up. Am J Ophthalmol
2007;144:844-849.
76. Rajaraman RT, Kimura Y, Li S et al. Retrospective case review of pediatric patients
treated with infliximab. Ophthalmology 2006;113:308-314.
77. Maini RN, Breedveld FC, Kalden JR. Therapeutic efficacy of multiple intravenous
infusions of anti-tumor necrosis factor α antibody combined with low dose weekly
methotrexate in patients with rheumatoid arthritis. Arthrit Rheum 1998;41:1552-1563
78. de Vries MK, Wolbink GJ, Stapel SO et al. Decreased clinical response to infliximab
in ankylosing spondylitis is correlated with anti-infliximab antibody formation. Ann Rhem Dis
2007;66:1252-1254.
79. Cheifetz A, Smedley M, Martin S et al. The incidence and management of infusion
reactions to infliximab: A large centre experience Am J Gastroenterol 2003;98:1315-1324.
80. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a
tumour necrosis factor alpha-neutralizing agent. N Eng J Med 2001;345:1098–104.
81. Mohan N, Edwards ET, Cups TR et al. Demyelination occurring during anti-tumor
necrosis factor α therapy for inflammatory arthritides Arthritis Rheum 2001;44:2862-2869.
Uveitis NMCN Treatment Guidelines Revised September 2010
89

82. Tusscher MP, Jacobs PJ, Busch MJ, et al. Bilateral anterior toxic optic neuropathy
and the use of infliximab. BMJ 2003;326:579.
83. Klapman JB, Ene-Stroescu D, Becker MA et al. A lupus-like syndrome associated
with infliximab therapy. Inflamm Bowel Dis 2008;9:176-178.
84. Brown SL, Greene MH, Gershon SK et al. Tumour necrosis factor antagonist therapy
and lymphoma development. Arthritis Rheum 2002;46:3151-3158.
85. Chung ES, Packer M, Hung Lo K et al. Randomised double blind placebo controlled
pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-α, in patients
with moderate to severe heart failure. Results of the anti-TNF therapy against heart failure
(ATTACH) trial. Circulation 2003;107:3133-3140.
86. Kwon HJ, Coté TR, Cuffe MS. Case reports of heart failure after therapy with a tumor
necrosis factor antagonist. Ann Intern Med 2003:138:807-811.
87. Kotter I, Zierhut M, Eckstein AK, et al. Human recombinant interferon alfa-2a for the
treatment of Behcet’s disease with sight threatening posterior or panuveitis. Br J
Ophthalmol. 2003;87:423-431
88. Guillaume-Czitrom S, Berger C, Pajot C et al. Efficacy and safety of interferon-α in
the treatment of corticodependent uveitis of paediatric Behcet’s disease. Rheumatol
2007;46:1570-1573.
89. Bodaghi B, Gendron G, Weschler B et al. Efficacy of interferon alpha in the treatment
of refractory and sight threatening uveitis: a retrospective monocentric study of 45 patients.
Br J Ophthalmol 2007;91:335-339.
90. Plskova J, Greiner K, Forrester JV. Interferon-α as an effective treatment for non-
infectious posterior uveitis and panuveitis. Am J Ophthalmol 2007;144:55-61.
91. Deuter CME, Koetter I, Guenaydin I et al. Interferon alpha-2A: a new treatment
option for long lasting refractory cystoid macular oedema in uveitis? A pilot study. Retina
2006;26:786-79130.
92. Scalori A, Pozzi M, Bellia V. Interferon-induced depression: prevalence and
management. Digestive and Liver disease 2005;37:102-107.
93. Hershberger RE, Starling RC, Eisen HJ et al. Daclizumab to prevent rejection after
cardiac transplantation. New Eng J Med 2005;352:2705-2713.
Uveitis NMCN Treatment Guidelines Revised September 2010
90

94. Nussenblatt RB, Thompson DJS, Li Z et al. Humanised anti-interlukin-2 (IL-2)
receptor alpha therapy: long term results in uveitis patients and preliminary safety and
activity data for establishing parameters for subcutaneous administration. J Autoimmun
2003;21:283-293.
95. Yeh S, Wroblewski K, Bruggage R. High-dose humanised anti-IL-2 receptor alpha
antibody (daclizumab) for the treatment of active, non-infectious uveitis. J Autoimmunity
2008;31:91-97.
96. Papaliodis GN, Chu D, Foster CS. Treatment of ocular inflammatory disorders with
daclizumab. Ophthalmology 2003;110:786-789.
97. Nussenblatt RB, Peterson JS, Foster CS. Initial evaluations of subcutaneous
daclizumab treatment for non-infectious uveitis. A multicentre non-comparative
interventional case series. Ophthalmology 2005;112:764-770.
98. Sobrin L, Huang JJ, Christen W. Daclizumab for treatment of birdshot
chorioretinopathy. Arch Ophthalmol 2008;126:186-191.
99. Buggage RR, Levy-Clarke G, Sen HN et al. A double-masked randomised placebo
controlled trial to investigate the safety and efficacy of daclizumab to treat the ocular
complications related to Behcet’s disease. Ocular Immunol Inflamm 2007;15:63-70.
100. Nussenblatt RB, Fortin E, Schiffman R. Treatment of non-infectious intermediate and
posterior uveitis with the humanised anti-Tac mAb: a phase I/II clinical trial. Proc Natl Acad
Sci USA 1999;96:7462-7466.
101. Webster AC, Playford EG, Higgins G et al. Interleukin-2 receptor antagonists for
renal transplant recipients: a meta-analysis of randomised trials. Transplantation
2004;77:166-176.
102. Dick ADD, Meyer P, James T, et al. Campath 1-H in refractory ocular inflammatory
disease. Br J Ophthalmol 2000;84:107-109.
103. van der Hoek J ,Azuara-Blanco A, Greiner K. Mooren’s ulcer resolved with campath-
H. Br J Ophthalmol 2003;84:924-5.
104. Lockwood CM, Hale G, Waldman H. Remission induction in Behcets disease
following lymphocyte depletion by the anti-CD-52 antibody CAMPATH-1H. Rheumatology
2003;42:1539-1544.
Uveitis NMCN Treatment Guidelines Revised September 2010
91

105. Basquiera AL, Berretta AR, Garcia JJ. Coronary ischaemia related to alemtuzumab
therapy. Ann Oncol 2004;15:539-540.
106. Lundin J, Kimby E, Björkholm M. Phase II trial of anti CD-52 monoclonal
antibody alemtuzumab (Campath-1H) as first line treatment for patients with B-cell
chronic lymphocytic leukaemia (B-CLL). Blood 2002;100:768-773.
107. Ku G, Ting WC, Lim STK. Life-threatening coagulopathy associated with use of
Campath (alemtuzumab) in maintenance of steroid-free renal transplant given before
surgery. Am J Transplant 2008;8:884-886.
108. Martin SI, Marty FM, Fimara K. Infectious complications associated with
Alemtuzumab use for lymphoproliferative disorders. Clin Infectious Dis 2006;43:16-24.
109. Mould DR, Baumann A, Kuhlmann J. Population pharmacokinetics-
pharmacodynamics of Alemtuzumab (Campath) in patients with chronic lymphocytic
leukaemia and its link to treatment response. Br J Clin Pharmacol 2007; 64:278-291.
110. CAMMS223 investigators. Alemtuzumab vs interferon beta-1a in early multiple
sclerosis. New Eng J Med 2008;359:1786-1801
111. Emery P, Fleischmann Roy M, Filipowicz-Sosnowska A. The Efficacy and Safety of
Rituximab in Patients With Active Rheumatoid Arthritis Despite Methotrexate Treatment:
Results of a Phase IIb Randomized, Double-Blind, Placebo-Controlled
112. Tappeiner C, Heinz C, Specker C et al. Rituxumab as a treatment option for
refractory endogenous anterior uveitis Ophthalmic Res 2007;39:184-186.
113. Ahmadi-Simab K, Lamprecht P, Nölle B Ai M, Gross WL. Successful treatment of
refractory anterior scleritis in primary Sjögren’s syndrome with rituximab. Ann Rheum Dis
2005;64;1087-1088.
114. Cheung CMG, Murray PI, Savage COS. Successful treatment of Wegener’s
granulomatosis associated scleritis with rituxumab. Br J Ophthalmol 2005;89:1542.
115. Freidlin J, Wong IG, Acharya N. Rituximab treatment for peripheral ulcerative
keratitis associated with Wegener’s granulomatosis. Br J Ophthalmol 2007;91:1414.
116. Sadreddini, S., Noshad, H., Molaeefard, M., Noshad, R. Treatment of retinal
vasculitis in Behc¸et’s disease with rituximab. Mod Rheumatol (2008) 18:306–308.
Uveitis NMCN Treatment Guidelines Revised September 2010
92

117. Leandro MJ, Edwards JC, Cambridge G, et al. An open study of B lymphocyte
depletion in systemic lupus erythematosus. Arthritis Rheum 2002; 46 (10): 2673-7.
118. Lamprecht P, Lerin-Lozano C, Merz H, et al. Rituximab induces remission in
refractory HCV associated cryoglobulinaemic vasculitis. Ann Rheum Dis 2003; 62 (12):
1230-3
119. Szczepanski L, Szechinski J, Filipowiczs-Sosnowska A, et al. Safety data from 48
weeks follow-up of a randomised controlled trial of rituximab in patients with rheumatoid
arthritis [abstract]. Arthritis Rheum 2003; 48 Suppl. 1: S121.
120. Maloney DG, Liles TM, Czerwinski DK, et al. Phase I clinical trial using escalating
single-dose infusion of chimeric anti- CD20 monoclonal antibody (IDEC-C2B8) in patients
with recurrent B-cell lymphoma. Blood 1994 Oct 15; 84: 2457-66.
121. McLaughlin P, Grillo-López AJ, Link BK, et al. Rituximab chimeric anti-CD20
monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a
four-dose treatment program. J Clin Oncol 1998 Aug; 16: 2825-33.
122. Maloney DG, Grillo-López AJ, Bodkin DJ, et al. IDEC-C2B8: results of a phase I
multiple-dose trial in patients with relapsed non-Hodgkin’s lymphoma. J Clin Oncol 1997a
Oct; 15: 3266-74.
123. Maloney DG, Grillo-López AJ, White CA, et al. IDEC-C2B8 (rituximab) anti-CD20
monoclonal antibody therapy in patients with relapsed low-grade non-Hodgkin’s lymphoma.
Blood 1997b Sep 15; 90: 2188-95.
124. Davis T, Levy R,White CA, et al. Retreatments with RITUXAN (rituximab, Idec-C2B8)
have significant efficacy, do not cause hama, and are a viable minimally toxic alternative in
relapsed or refractory non-Hodgkin’s lymphoma (NHL) [abstract no. 2269]. Blood 1997 Nov
15; 90 Suppl. 1, Part 1: 509.
125. Coiffier B. Rituximab in diffuse large B cell and mantle cell lymphomas [abstract no.
020]. Ann Oncol 1998; 9 Suppl. 3: 27.
126. Plosker GL, Figgitt DP. Rituximab A Review of its Use in Non-Hodgkin’s Lymphoma
and Chronic Lymphocytic Leukaemia Drugs 2003; 63 (8): 803-843.
127. Foran JM, Rohatiner AZS, Cunningham D, et al. Immunotherapy of mantle cell
lymphoma (MCL), lymphoplasmacytoid lymphoma (LPC) and Waldenstrom’s
Uveitis NMCN Treatment Guidelines Revised September 2010
93

macroglobulinemia (WM), and small lymphocytic lymphoma (SLL) with rituximab (IDEC-
C2B8): preliminary results of an ongoing international multicentre trial [abstract no. O-0586].
Br J Haematol 1998 Jul; 102 (1): 149.
128. Teoh SBC, Sharma S, Hogan A et al. Tailoring biological treatment: Anakinra
treatment of posterior uveitis associated with the CINCA syndrome. Br J Ophthalmol
2007;91:263-264
129. Thonhofer R, Uitz E, Graninger W. Efficacy of the IL-1 receptor antagonist, anakinra
for the treatment of diffuse anterior scleritis in rheumatoid arthritis. Report of two cases.
Rheumatology 2007;46:1042-1043
130. Bresnihan B, Alvaro-Gracia JM, Cobby M, et al. (1998) Treatment of rheumatoid
arthritis with recombinant human interleukin-1 receptor antagonist. Arthritis Rheum 41,
2196–204.
131. Cohen S, Hurd E, Cush J, et al. (2002) Treatment of rheumatoid arthritis with
anakinra, a recombinant human interleukin-1 receptor antagonist, in combination with
methotrexate: results of a twenty-four-week, multicenter, randomized, double-blind, placebo-
controlled trial. Arthritis Rheum 46, 614–24.
132. Schiff MH, Bulpitt K, Weaver AA, et al. (2001) Safety of combination therapy with
anakinra and etanercept in patients with rheumatoid arthritis. Arthritis Rheum 44, S79.
133. Genovese M, Cohen S, Moreland L, et al. (2004) Combination therapy with
etanercept and anakinra in the treatment of patients with rheumatoid arthritis who have been
treated unsuccessfully with methotrexate. Arthritis Rheum 50, 1412–9.
134. Reiff A, Takei S, Sadeghi S, Stout A, Shaham B, Bernstein B, Gallagher K, Stout T.
Etanercept therapy in children with treatment-resistant uveitis. Arthritis Rheum. 2001
Jun;44(6):1411-5.
135. Foster CS, Tufail F, Waheed NK, Chu D, Miserocchi E, Baltatzis S, Vredeveld CM.
Efficacy of etanercept in preventing relapse of uveitis controlled by methotrexate. Arch
Ophthalmol. 2003 Apr;121(4):437-40.
136. Smith JA, Thompson DJ, Whitcup SM, Suhler E, Clarke G, Smith S, Robinson M, Kim
J, Barron KS. A randomized, placebo-controlled, double-masked clinical trial of etanercept
for the treatment of uveitis associated with juvenile idiopathic arthritis. Arthritis Rheum. 2005
Feb 15;53(1):18-23.
Uveitis NMCN Treatment Guidelines Revised September 2010
94
137. Baughman RP, Lower EE, Bradley DA, Raymond LA, Kaufman A. Etanercept for
refractory ocular sarcoidosis: results of a double-blind randomized trial. Chest. 2005
Aug;128(2):1062-47.
138. Galor A, Perez VL, Hammel JP, Lowder CY. Differential effectiveness of etanercept
and infliximab in the treatment of ocular inflammation. Ophthalmology.2006
Dec;113(12):2317-23.
139. Reddy AR, Backhouse OC. Does etanercept induce uveitis? Br J Ophthalmol
2003;87:925.
140. Kaipaiainen-Seppanen O, Leino M. Recurrent uveitis in a patient with juvenile
spondlyloarthropathy associated with tumour necrosis factor alpha inhibitors. Ann Rheum
Dis 2003;62:88-89.
141. O’Dell JR, Haire CE, Erikson N, et al. Treatment of rheumatoid arthritis with
methotrexate alone, sulfasalazine and hydroxychloroquine, or a combination of all three
medications. N Engl J Med 1996;334:1287–1291.
142. Tugwell P, Pincus T, Yocum D, et al. Combination therapy with cyclosporine and
methotrexate in severe rheumatoid arthritis. The Methotrexate-Cyclosporine Combination
Study Group. N Engl J of Med 1995;333:137–141
143. Weinblatt MEK, Bulpitt KJ, Fleischmann RM, et al. A trial of etanercept, a
recombinant tumor necrosis factor receptor: Fc fusion protein, in patients with rheumatoid
arthritis receiving methotrexate. N Engl J Med 1999;340:253–259.
144. Pascalis L, Pia G, Aresu G, Frongia T, Barca L. Combined cyclosporine A-steroid-
MTX treatment in endogenous non-infectious uveitis. J Autoimmun 1993;6:467– 480.
145. O’Duffy JD, Robertson DM, Goldstein NP. Chlorambucil in the treatment of uveitis
and meningoencephalitis of Behçet’s disease. Am J Med 1984;76:75– 84.
146. Abdalla MI, Bahgat Nour E. Long-lasting remission of Behçet’s disease after
chlorambucil therapy. Br J Ophthalmol 1973;57:706 –711.
147. Tessler HH, Jennings T. High-dose short-term chlorambucil for intractable
sympathetic ophthalmia and Behçet’s disease. Br J Ophthalmol 1990;74:353–357.
Uveitis NMCN Treatment Guidelines Revised September 2010
95

148. Buckley CE, Gills JP. Cyclophosphamide therapy of Behcet’s disease. J Allergy
1969;43:273–283.
149. Tabbara KF. Chlorambucil in Behçet’s disease: a reappraisal. Ophthalmology
1983;45:265.
150. Binder AI, Graham EM, Sanders MD, et al. Cyclosporin A in the treatment of severe
Behçet’s uveitis. Br J Rheumatol. 1987;26:285–291.
151. Masuda K, Nakajima A, Urayama A, Nakae K, Kogure M, Inaba G. Double-masked
trial of cyclosporine versus colchicine and long-term open study of cyclosporine in Behçet’s
disease. Lancet 1989;1:1093–1096.
152. Kotake S, Higashi K, Yoshikawa K, et al. Central nervous system symptoms in
patients with Behcet disease receiving cyclosporine therapy. Ophthalmology. 1999;
106:586–589.
153. Bietti GB, Cerulli L, Pivetti-Pezzi P. Behçet’s disease and immunosuppressive
treatment. Mod Probl Ophthalmol 1976; 16:314.
154. Wechsler B, Sablé-Fourtassou R et al. (2004) Infliximab in refractory panuveitis due
to Behcet’s disease. Clin Exp Rheumatol 22, S14–6.
155. Triolo G, Vadala M, Accardo-Palumbo A et al. (2002) Antitumour necrosis factor
monoclonal antibody treatment for ocular Behcet’s disease. Ann Rheum Dis 61, 560–1.
156. Joseph A, Raj D, Dua HS, Powellt PT, Lanyon PC, Powelit RJ (2003) Infliximab in
the treatment of refractory posterior uveitis. Ophthalmology 110, 1449–53.
157. Morris DS, Gavin MP, Sturrock RD (2003) The effect of antitumor necrosis alpha
(Infliximab) on sight-threatening uveitis in a patient with Behcet’s Disease. Adv Exp Med Biol
528, 557–9.
158. Munoz-Fernandez S, Hidalgo V, Fernandez-Melon J, et al. Effect of infliximab on
threatening panuveitis in Behcet’s disease. Lancet. 2001;358:1644.
159. Ohno S, Nakamura S, Hori S, et al. Efficacy, safety, and pharmacokinetics of
multiple administration of infliximab in Behcet’s disease with refractory uveoretinitis. J
Rheumatol. 2004;31:1362–1368.
Uveitis NMCN Treatment Guidelines Revised September 2010
96

160. Vitale AT, Rodriguez A, Foster CS. Low-dose cyclosporine therapy in the treatment
of birdshot retinochoroidopathy. Ophthalmology 1994;101:822– 831.
161. LeHoang P, Girard B, Keray G, et al. Cyclosporine in the treatment of birdshot
retinochoroidopathy. Transplant Proc 1988;20(suppl 4):128 –130.
162. Kiss S, Ahmed M, Letko E, et al. Long-term follow up of patients with birdshot
retinochoroidopathy treated with corticosteroid-sparing systemic immunomodulatory therapy.
Ophthalmol. 2005;112:1066–1071.
163. Morgan CM, Schatz H. Recurrent multifocal choroiditis. Ophthalmology
1986;93:1138 –1147.
164. MacLaren RE, Lightman SL. Variable phenotypes in patients diagnosed with
idiopathic multifocal choroiditis. Clin Exp Ophthalmol. 2006; 34: 233–238.
165. Nussenblatt RB, Whitcup SM, Palestine AG. White-dot syndrome. In. Nussenblatt
RB, Whitcup SM, Palestine AG, editors. Uveitis: fundamentals and clinical practice. St.
Louis: Mosby, 1996:371–384.
166. Christmas NJ, Oh KT, Oh DM, Folk JC. Long-term follow-up of patients with
Serpiginous Choroiditis. Retina 2002; 22, 550-556.
167. Secchi AG, Tognon MS, Maselli C. Cyclosporine-A in the treatment of serpiginous
choroiditis. Int Ophthalmol 1990; 14:395–399.
168. Laatikainen L, Tarkkanen A. Failure of cyclosporine A in serpiginous choroiditis. J
Ocul Therap Surg 1984;3:280– 283.
169. Akpek EK, Jabs DA, Tessler HH, et al. Successful treatment of serpiginous
choroiditis with alkylating agents. Ophthalmology. 2002;109:1506–1513.
170. Perentes Y, van Tran T, Sickenberg M, Herbort CP. Subretinal neovascular
membranes complicating uveitis: frequency, treatments, and visual outcome. Ocul Immunol
Inflamm 2005;13:219 –224.
171. Mansour AM, Arevalo JF, Ziemssen F. Long-term Visual Outcomes of Intravitreal
Bevacizumab in Inflammatory Ocular Neovascularization. Am J Ophthalmol 2009 May 8.
(Epub ahead of print)
Uveitis NMCN Treatment Guidelines Revised September 2010
97
172. Shah SS, Schachat AP, Murphy RP, Fine SL. The evolution of argon laser
photocoagulation scars in patients with the ocular histoplasmosis syndrome. Arch
Ophthalmol 1988;106:1533–1536.
173. Hawkins BS, Bressler NM, Bressler SB, et al, Submacular Surgery Trials Research
Group. Surgical removal vs. observation for subfoveal choroidal neovascularization, either
associated with the ocular histoplasmosis syndrome or idiopathic: I. Ophthalmic findings
from a randomized clinical trial: Submacular Surgery Trials (SST) Group H Trial: SST Report
No. 9. Arch Ophthalmol 2004;122:1597–1611.
174. Flaxel CJ, Owens SL, Mulholland B, Schwartz SD, Gregor ZJ. The use of
corticosteroids for choroidal neovascularization in young patients. Eye 1998;12:266 –272.
175. Leslie T, Lois N, Christopoulou D, Olson JA, Forrester JV. Photodynamic therapy for
inflammatory choroidal neovascularisation unresponsive to immunosuppression. Br J
Ophthalmol. 2005 Feb;89(2):147-50.
176. Rosenfeld PJ, Saperstein DA, Bressler NM, et al, Verteporfin in Ocular
Histoplasmosis Study Group. Photodynamic therapy with verteporfin in ocular
histoplasmosis: uncontrolled, open-label 2-year study. Ophthalmology 2004;111:1725–1733.
177. Fong KC, Thomas D, Amin K, Inzerillo D, Horgan SE. Photodynamic therapy
combined with systemic corticosteroids for choroidal neovascularisation secondary to
punctate inner choroidopathy. Eye. 2008 Apr;22(4):528-33.
178. Chan WM, Lai TY, Liu DT, Lam DS. Intravitreal bevacizumab (Avastin) for choroidal
neovascularization secondary to central serous chorioretinopathy, secondary to punctate
inner choroidopathy, or of idiopathic origin. Am J Ophthalmol 2007;143:977–983.
179. Neri P, Azuara-Blanco A, Forrester JV. Incidence of Glaucoma in Patients with
Uveitis. J Glaucoma 2004;13:461–465.
180. La Hey E, de Vries J, Langerhorst CT, et al.: Treatment and prognosis of secondary
glaucoma in Fuchs heterochromic cyclitis. Am J Ophthalmol 1993, 116:327–340.
181. Miserocchi E, Waheed NK, Dios E, et al.: Visual outcome in herpes simplex virus
and varicella zoster virus uveitis: a clinical evaluation and comparison. Ophthalmology 2003,
109:1532–1537.
Uveitis NMCN Treatment Guidelines Revised September 2010
98

182. Sung VCT, Barton K. Management of inflammatory glaucomas. Curr Opin
Ophthalmol 15:136–140.
183. Patelska B, Greenfield DS, Liebmann JM, et al.: Latanoprost for uncontrolled
glaucoma in a compassionate case protocol. Am J Ophthalmol 1997, 124:279–286.
184. Warwar RE, Bullock JD, Ballal D: Cystoid macular edema and anterior uveitis
associated with Latanoprost use: experience and incidence in a retrospective review of 94
patients. Ophthalmology 1998, 105:263–268.
185. Smith SL, Pruitt CA, Sine CS, et al.: Latanoprost 0.005% and anterior segment
uveitis. Acta Ophthalmol Scand 1999, 77:668–672.
186. Callanan D, Fellman RL, Savage JA: Latanoprost-associated cystoid macular
edema. Am J Ophthalmol 1998, 126:134–135.
187. Heier JS, Steinert RF, Frederick AR: Cystoid macular edema associated with
Latanoprost use. Arch Ophthalmol 1998, 116:680–682.
188. Ayyala RS, Cruz DA, Margo CE, et al.: Cystoid macular edema associated with
latanoprost in aphakic and pseudophakic eyes. Am J Ophthalmol 1998, 126:602–604
189. Kaufman HE, Varnell ED, Thompson HW: Latanoprost increases the severity and
recurrence of herpetic keratitis in the rabbit. Am J Ophthalmol 1999, 127:531–536.
190. Wand M, Gilbert CM, Liesegang TJ: Latanoprost and herpes simplex keratitis. Am J
Ophthalmol 1999, 127:602–604.
191. Murphy CC, Burnett CA, Spry PG, et al.: A two centre study of the dose response
relation for transscleral diode laser cyclophotocoagulation in refractory glaucoma. Br J
Ophthalmol 2003, 87:1252–1257.
192. Towler HMA, Bates AK, Broadway DC, et al. Primary trabeculectomy with 5-
fluorouracil for glaucoma secondary to uveitis. Ocular Immunol and Inflamm 1995, 3:163–
170.
193. Ceballos EM, Beck AD, Lynn MJ: Trabeculectomy with antiproliferative agents in
uveitic glaucoma. J Glaucoma 2002, 11:189–196.
194. Prata JA, Neves RA, Minckler DS, et al.: Trabeculectomy with Mitomycin C in
glaucoma associated with uveitis. Ophthalmic Surg 1994, 25:616–620.
Uveitis NMCN Treatment Guidelines Revised September 2010
99

195. Wright MM, McGehee RF, Pederson JE: Intraoperative mitomycin-C for glaucoma
associated with ocular inflammation. Ophthalmic Surg Lasers 1997, 28:370–376.
196. Valimaki J, Airaksinen PJ, Tuulonen A: Molteno implantation for secondaryglaucoma
in juvenile rheumatoid arthritis. Arch Ophthalmol 1997, 115:1253–1256.
197. Molteno AC, Sayawat N, Herbison P: Otago glaucoma surgery outcomestudy: long-
term results of uveitis with secondary glaucoma drained by Moltenoimplants. Ophthalmology
2001, 108:605–613.
198. Da Mata A, Burk SE, Netland PA, et al.: Management of uveitic glaucoma with
Ahmed glaucoma valve implantation. Ophthalmology 1999, 106:2168– 2172.
199. Ceballos EM, Parrish RK, Schiffman JC: Outcome of Baerveldt glaucoma drainage
implants for the treatment of uveitic glaucoma. Ophthalmology 2002, 109:2256–2260.
200. Meacock WR, Spalton DJ, Bender L, Antcliff R, Heatley C, Stanford MR, Graham
EM. Steroid prophylaxis in eyes with uveitis undergoing phacoemulsification. Br. J.
Ophthalmol. 2004;88;1122-1124.
201. Murray PI. Cataract Surgery in Patients with Uveitis. Eye news 2002;9; 24-32.
202. Miettinen R. Incidence of uveitis in Northern Finland. Acta Ophthalmol (Copenh)
1977;55:252–60.
203. Watson AR, Rance CP, Bain J. Long-term effects of cyclophosphamide on testicular
function. BMJ. 1985;291:1457-1460.
204. Russell JA, Powles RL, Oliver RTD. Conception and congenital abnormalities after
chemotherapy of acute myelogenous leukemia in two men. BMJ. 1976;1:1508.
205. Kitridou RC. The mother in systemic lupus erythematosus. In: Wallace DJ, Hahn BH,
eds. Dubois' Lupus Erythematosus. 5th ed. Baltimore, Md: Williams & Wilkins; 1997:967-
1002.
206. French AE, Koren G. Effect of methotrexate on male fertility. Canadian Family
physician.2003;4:577-578.
207. Sussman A, Leonard JM. Psoriasis, methotrexate, and oligospermia. Arch Dermatol.
1980;116:215-217.
Uveitis NMCN Treatment Guidelines Revised September 2010
100

208. Brooks PM, Needs CJ. The use of antirheumatic medication during pregnancy and in
the puerperium. Rheum Dis Clin North Am. 1989;15:789-806.
209. Ostensen M. Safety on nonsteroidal anti-inflammatory drugs during pregnancy and
lactation. Immunopharmacology. 1996;4:31-41.
210. Needs CJ, Brooks PM. Antirheumatic medication during lactation. Br J Rheumatol.
1985;24:291-29
211. Ostensen M, Ostensen H. Safety of nonsteroidal anti-inflammatory drugs in pregnant
patients with rheumatic diseases. J Rheumatol. 1996;23:1045-1049.
212. Park-Wyllie L, Mazzotta P, Pastuszak A. Birth defects after maternal exposure to
corticosteroids: prospective cohort study and meta-analysis of epidemiological studies.
Teratology. 2000;62:385
213. Cote CJ, Meuwissen HJ, Pickering RJ. Effects on the neonate of prednisone and
azathioprine administered to the mother during pregnancy. J Pediatr. 1974;85:324-328.
214. American Academy of Pediatrics. The transfer of drugs and other chemicals into
human milk. Pediatrics. 1994;93:137-150.
215. Rudolph J, Schweizer R, Bartus S. Pregnancy in renal transplant patients.
Transplantation. 1979;27:26-29.
216. Penn I, Makowski E, Droegemueller W, et al. parenthood in renal homograft
recipients. JAMA. 1971;216:1755-1761.
217. Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation. 5th ed.
Baltimore, Md: Williams & Wilkins; 1998.
218. Little BB. Immunosuppressant therapy during gestation. Seminars in Perinatology.
1997;21:143-148
219. San A, Clarke S, Bass J, et al. Azathioprine and breastfeeding : is it safe? Br J
Obstet Gynaecol. 2007;114:498-501
220. Moretti ME, Verjee Z, Ito S, et al. Breastfeeding during maternal use of azathioprine.
Ann Pharmacother. 2006;40:2269-2272.
Uveitis NMCN Treatment Guidelines Revised September 2010
101
221. Moskovitz DN, Bodian C, Chapman ML, et l. The effect on the fetus on medications
used to treat pregnancy inflammatory bowel disease. Am J Gastroenterol. 2004;99:656-661.
222. Fran Cella A, Dyan A, Present DH, et al. the safety of 6-mercaptopurine for
childbearing patients with inflammatory bowel disease: A retrospective cohort study.
Gastroenterol. 2003;124:9-17
223. Milunsky A, Graef JW, Gaynor MF. Methotrexate-induced congenital malformations.
J Pediatr. 1968;72:790-795.
224. Powell HR, Ekert H. Methotrexate-induced congenital malformations. Med J Aust.
1971;2:1076-1077.
225. Del camp M, Kosaki K, Bennett FC, et al. Developmental delay in feta
aminopterin/methotrexate syndrome. Teratology. 1999;60:10-12.
226. Sifontis NM, Coscia LA, Constantinescu S, et al. Pregnancy outcomes in solid organ
transplant recipients with exposure to mycophenolate mofetil or sirolimus.
Transplant.2006;812:1698-1702.
227. Le Ray C, Coulomb A, Elefant E, et al. Mycophenolate mofetil in pregnancy after
renal transplantation: a case of major fetal malformations. Obstst Gynecol.2004:103:1091-
1094.
228. Bar Oz B, Hackman R, Einerason T, et al. Pregnancy outcomes after ciclosporin
therapy during pregnancy: a meta-analysis. Transplantation. 2001;71:1051-1055.
229. Ostenten M, Khamashta M, Lockshin M, et al. Anti-inflammatory and
immunosuppressive drugs and reproduction. Arthritis Res Ther. 2006;8:209.
230. Kainz A, Hcrabacz I. Cowlrick IS, et al. Review of the course and outcome of 100
pregnancies in 84 women treated with tacrolimus. Transplantation. 2000;70:1718-1721.
231. Jain A, Venkataramanan R, Fung JJ. Pregnancy after liver transplantation under
tacrolimus. Transplantation. 1997;64:559-565.
232. EBPG Expert Group in Renal transplantation: European best practice guidelines for
renal transplantation. IV.10. Longterm management of the transplant recipient. Nephrol Dial
Transplant. 2002;17;50-55.
Uveitis NMCN Treatment Guidelines Revised September 2010
102

233. Nicholson HO. Cytotoxic drugs in pregnancy: review of reported cases. J Obstet
Gynaecol Br Commonw. 1968;75:307-312.
234. Wiernik PH, Duncan JH. Cyclophosphamide in human milk. Lancet. 1971;1:912-914.
235. O’Donnell S, O’Morain C. Use of antitumour necrosis factor therapy in inflammatory
bowel disease during pregnancy and conception. Aliment Pharmacol Ther.2008;27:885-894.
236. Dana CM, Charles NB. Drug therapy for inflammatory bowel disease in pregnancy
and the puerperium. Best Practice and Research Clinical Gastroenterology. 2007;21:835-
847.
237. Kane S, Ford J, Cohen R, et al. Absence of infliximab in infants and breast milk from
nursing mothers receiving therapy for crohn’s disease before and after delivery. J Clin
Gastroenterology.2009;0:1-4.
238. Chambers CD, Johnson DL, Jones KL. Adalimumab and pregnancy outcome: the
OTIS autoimmune diseases in pregnancy project. Am J Gastro. 2006;101:5421-5422.
239. Mishkin DS, VanDeinse W, Becker JM, et al. Successful use of adalimumab for
crohn’s disease in pregnancy. Inflamm Bowel Dis. 2006;12:827-828.
240. Vesga L, Terdiman JP, Mahadevan U. Adalimumab use in pregnancy.
Gut.2005;54:890.
241. Lima XT, Seidler EM, Lima HC, et al. Long term safety of biologics in dermatology.
Derm Ther. 2009;22:2-21.
242. Sakata H, Karamitsos J, Kunclaria B, et al. Case report of interferon alpha for
multiple myeloma during pregnancy. Am J Obstet Gynecol.1995;171:217-219.
243. Fritz M, Vats K, Goyal RK. Neonatal lupus and IUGR following alpha-interferon
during pregnancy. J Perinatology. 2005;25:552-554.
244. Kanski J. Uveitis in juvenile chronic arthritis: incidence clinical features and prognosis
Eye1988 2 641-5.
245. Kanski JJ. Screening for uveitis in juvenile idiopathic arthritis. Br J ophthalmology 1989
73 225-8.
Uveitis NMCN Treatment Guidelines Revised September 2010
103
246. Edelsten C, Lee V, Bentley CR, Kanski JJ, Graham EM. An evaluation of baseline risk
factors predicting severity in juvenile idiopathic arthritis associated uveitis and other chronic
anterior uveitis in early childhood. B J Ophthalmology 2002 86 51-56.
247. Woreta F, Thorne JE, Jabs DA, Kedhar SR, Dunn JP. Risk factors for ocular
complications and poor visual acuity at presentation among patients with uveitis associated
with juvenile idiopathic arthritis. Am J Ophthalmol. 2007 143 647-55.
248. Kodski SR, Rubin SE, Milojevic D, Ilowite N, Gottlieb B. Time of onset of uveitis in
children with juvenile rheumatoid arthritis. J AAPOS 2002 6 373-6.
249. Kump LI, Castaneda RA, Androudi SN, Reed GF, Foster CS. Visual outcomes in
children with juvenile idiopathic arthritis-associated uveitis. Ophthalmology. 2006 113 1874-
250. Kotaniemi, K, Kotaniemi H, Karma A, Aho K. Occurrence of uveitis in recently
diagnosed juvenile chronic arthritis. Ophthalmology 2001 108 2071-2075.
251. Cabral DA, Petty RE, Malleson PN, Ensworth S, McCormick AQ. Arth Rheum (S) D93
1992. Visual prognosis in children with chronic anterior uveitis and arthritis. J Rheumatol.
1994 Dec; 21(12) :2370-5.
252. Saurenmann RK, Levin AV, Feldman BM, Rose JB, Laxer RM, Schneider R, Silverman
ED. Prevalence, risk factors, and outcome of uveitis in juvenile idiopathic arthritis: a long-
term follow up study. Arthritis Rheum. 2007 56 647-57.
253. de Boer J, Wulffraat N, Rothova A. Visual loss in uveitis of childhood. Br J Ophthalmol
2003 87 879-884.
254. Ozdal PC, Vianna RN, Deschenes J. Visual outcome of juvenile rheumatoid arthritis-
associated uveitis in adults. Ocul Immunol Inflamm. 2005 13 33-8.
255. Royal College of Ophthalmologists 2006. Guidelines for screening for uveitis in
juvenile idiopathic arthritis. Produced jointly by BSPAR and the RCPOphth 2006 available
at http:// www.rcophth.ac.uk/docs/publications (2006) (accessed 18th June 2007).
256. Cassidy J, Kivlin L, Linddsley C et al. Ophthalmological examination in children with
juvenile rheumatoid arthritis Pediatrics 2006: 117:1843-5.
257. Chia A, Franco, V Lee, EM Graham, C Edelsten Factors related to severe uveitis at
diagnosis in children with juvenile idiopathic arthritis in a screening program. Am J
Ophthalmol. 2003 135 757-62.
Uveitis NMCN Treatment Guidelines Revised September 2010
104

258. Carvounis PE, Herman DC, Cha S, Burke JP. Incidence and outcomes of uveitis in
juvenile rheumatoid arthritis, a synthesis of the literature. Graefe’s Arch Clin Exp
Ophthalmology 2006 244 281-290.
259. Yu EN, Meniconi ME, Tufail F, Baltatzis S, Foster CS. Outcomes of treatment with
immunomodulatory therapy in patients with corticosteroid-resistant juvenile idiopathic
arthritis-associated chronic iridocyclitis. Ocul Immunol Inflamm. 2005 Sep-Oct;13(5):353-60.
260. Adib N, Hyrich KL, Thornton J, Lunt M, Baildam E, Foster H, Gardner-Medwin J,
Davidson J, Wedderburn L, Thomson W. Association between symptoms at presentation to
paediatric rheumatology and the delay from disease onset. Results from the Childhood
Arthritis Prospective Study (CAPS) Rheumatology 2008 47 991-5.
261. Marvillet I, Terrada C, Quartier P, Quoc EB, Bodaghi B, Prieur AM. Ocular threat in
juvenile idiopathic arthritis. Joint Bone Spine. 2009 Jul;76(4):383-8.
262. Hamade I H, H N Al Shamsi, H Al Dhibi et al. Uveitis survey in children. Br J
Ophthalmol 2009 93: 569-572.
263. Sabri K, Saurenmann RK, Silverman ED, Levin AV. Course, complications, and
outcome of juvenile arthritis-related uveitis. J AAPOS. 2008 Dec;12(6):539-45.
264. Dana M, Merayo-Lloves J, Schaumberg DA, et al. Prognosticators for visual outcome in
sarcoid uveitis. Ophthalmol 1996; 103:1846-1853.
265. Foster HE, Eltringham MS, Kay LJ, Friswell M, Abinun M, Myers. Delay in access to
appropriate care for children presenting with musculoskeletal symptoms and ultimately
diagnosed with juvenile idiopathic arthritis. Arthritis Rheum. 2007 57 921-7.
266. Edelsten C. Reconsidering treatment options in childhood uveitis. Br J Ophthalmol.
2007 91 133-4.
267. Schmeling H, Horneff G. Etanercept and uveitis in patients with juvenile idiopathic
arthritis. Rheumatology 2005 Aug ;44 (8): 1008-11.
268.Prince FH, Twilt M, ten Cate R, van Rossum MA, Armbrust W, Hoppenreijs EP, van
Santen-Hoeufft M, Koopman-Keemink Y, Wulffraat NM, van Suijlekom-Smit LW. Long-term
follow-up on effectiveness and safety of etanercept in juvenile idiopathic arthritis: the Dutch
national register. Ann Rheum Dis. 2009 May;68(5):635-41.
Uveitis NMCN Treatment Guidelines Revised September 2010
105

269. Saurenmann RK, Levin AV, Rose JB, Parker S, Rabinovitch T, Tyrrell PN, Feldman
BM, Laxer RM, Schneider R, Silverman ED. Tumour necrosis factor alpha inhibitors in the
treatment of childhood uveitis.Rheumatology (Oxford). 2006 Aug;45(8):982-9.
270. Tauber T, Turetz J, Barash J, Avni I, Morad Y. Optic neuritis associated with etanercept
therapy for juvenile arthritis. J AAPOS. 2006 Feb;10(1):26-9.
271. Edelsten C, M Ashwin Reddy, MR Stanford, EM Graham. Visual loss associated with
pediatric uveitis in english primary and referral centres. Am J Ophthalmol 2003 135 676-80
(2003).
272. Yim JL, Jalila JL, Lavy T, Gardner-Medwin J. Chronic Active Uveitis In JIA: Lessons
From A Clinical Screening Service. Paediatric Rheumatology European Society 2007,
Istanbul.
273. Hudson B., Clarke M., Strong N., Abinun M., Craft AW, Foster HE. An audit of
screening for chronic anterior uveitis in juvenile chronic arthritis. Br J Rheumatol 1997 36
Abstract presentation BSR AGM 1997.274. Thornton J, Lunt M, Ashcroft DM, Baildam E,
Foster H, Davidson J, Gardner-Medwin J, Beresford M, Symmons D, Thomson W, Elliott
RA. Costing juvenile idiopathic arthritis: examining patient-based costs during the first year
after diagnosis Rheumatology (Oxford). 2008 Jul;47(7):985-90.
275. Maini R, O'Sullivan J, Reddy A, Watson S, Edelsten C. The risk of complications of
uveitis in a district hospital cohort. Br J Ophthalmol. 2004 88 512-7.
276. Foeldvari I, Wierk A. Methotrexate is an effective treatment for chronic uveitis
associated with juvenile idiopathic arthritis. J Rheumatol. 2005 Feb;32(2):362-5.
277. Alsufyani K, Ortiz-Alvarez O, Cabral DA, Tucker LB, Petty RE, Malleson PN.
The role of subcutaneous administration of methotrexate in children with juvenile idiopathic
arthritis who have failed oral methotrexate J Rheumatol. 2004 Jan;31(1):179-82.
278. Doycheva D, Deuter C, Stuebiger N, Biester S, Zierhut M. Mycophenolate mofetil in the
treatment of uveitis in children. Br J Ophthalmol. 2007 Feb;91(2):180-4. Epub 2006 Jul 6.
279. Thorne JE, Jabs DA, Qazi FA, Nguyen QD, Kempen JH, Dunn JP. Mycophenolate
mofetil therapy for inflammatory eye disease. Ophthalmology. 2005 Aug;112(8):1472-
7.PMID: 16061096.
Uveitis NMCN Treatment Guidelines Revised September 2010
106

280. Daniel E, Thorne JE, Newcomb CW, Pujari SS, Kaçmaz RO, Levy-Clarke GA,
Nussenblatt RB, Rosenbaum JT, Suhler EB, Foster CS, Jabs DA, Kempen JH.
Mycophenolate mofetil for ocular inflammation. Am J Ophthalmol. 2010 Mar;149(3):423-
32.e1-2. Epub 2009 Dec 30.
281. Sobrin L, Christen W, Foster CS. Mycophenolate mofetil after methotrexate failure or
intolerance in the treatment of scleritis and uveitis. Ophthalmology. 2008 Aug;115(8):1416-
21, 1421.e1.
282. Murphy CC, Ayliffe WH, Booth A, Makanjuola D, Andrews PA, Jayne D. Tumor
necrosis factor alpha blockade with infliximab for refractory uveitis and scleritis.
Ophthalmology. 2004 Feb;111(2):352-6.
283. Mangge H, Heinzl B, Grubbauer HM, El-Shabrawi Y, Schauenstein K. Therapeutic
experience with infliximab in a patient with polyarticular juvenile idiopathic arthritis and
uveitis. Rheumatol Int. 2003 Sep;23(5):258-61.
284. Richards JC, Tay-Kearney ML, Murray K, Manners P.Infliximab for juvenile idiopathic
arthritis-associated uveitis.Richards JC, Tay-Kearney ML, Murray K, Manners P.
Clin Experiment Ophthalmol. 2005 Oct;33(5):461-8.
285. RCN Adolescent Transitional Care 2004.
http://www.rcn.org.uk/__data/assets/pdf_file/0011/78617/002313.pdf
286. BSPAR Standards of Care 2010. BSPAR Standards of Care for JIA
http://www.bspar.org.uk/downloads/clinical_guidelines/Standards_of_Care.pdf
287. Royal College of Nursing (2004) Subcutaneous Methotrexate in Inflammatory Arthritis.
London: RCN. Available at www.rcn.org.uk. Lead Paediatric Author, Polly Livermore.
288. Royal College of Nursing (2003) Assessing, Managing and Monitoring Biologic
Therapies; guidance for rheumatology practitioners. London:RCN. Available at
www.rcn.org.uk Lead Paediatric Author, Liz Hutchison.
289. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature
(SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data.
Results of the First International Workshop. Am J Ophthalmol 2005;140:509-516.
Uveitis NMCN Treatment Guidelines Revised September 2010
107
Uveitis NMCN Treatment Guidelines Revised September 2010
108
290. Goldmann H Schmidt T. Über Applanationstonometrie. Ophthalmologica
1957;134:221–42.
291. Jonas JB, Degenring RF, Kreissig I, Akkoyun I, Kamppeter BA. Intraocular pressure
elevation after intravitreal triamcinolone acetonide injection. Ophthalmology.
2005;112(4):593-598.
292. Smithen LM, Ober MD, Maranan L, Spaide RF. Intravitreal triamcinolone acetonide and
intraocular pressure. Am J Ophthalmol. 2004;138(5):740-743.
293. BSPAR Clinical Guidelines for DMARDs and Biologics
http://www.bspar.org.uk/downloads/clinical_guidelines