screening genetici per individuare ipercolesterolemia ... solo cuore... · screening genetici per...
TRANSCRIPT

Di.M.I. University of Genoa
IRCCS AOU SAN MARTINO-IST
Screening genetici
per individuare
ipercolesterolemia
familiare
Livia Pisciotta

CASO CLINICO
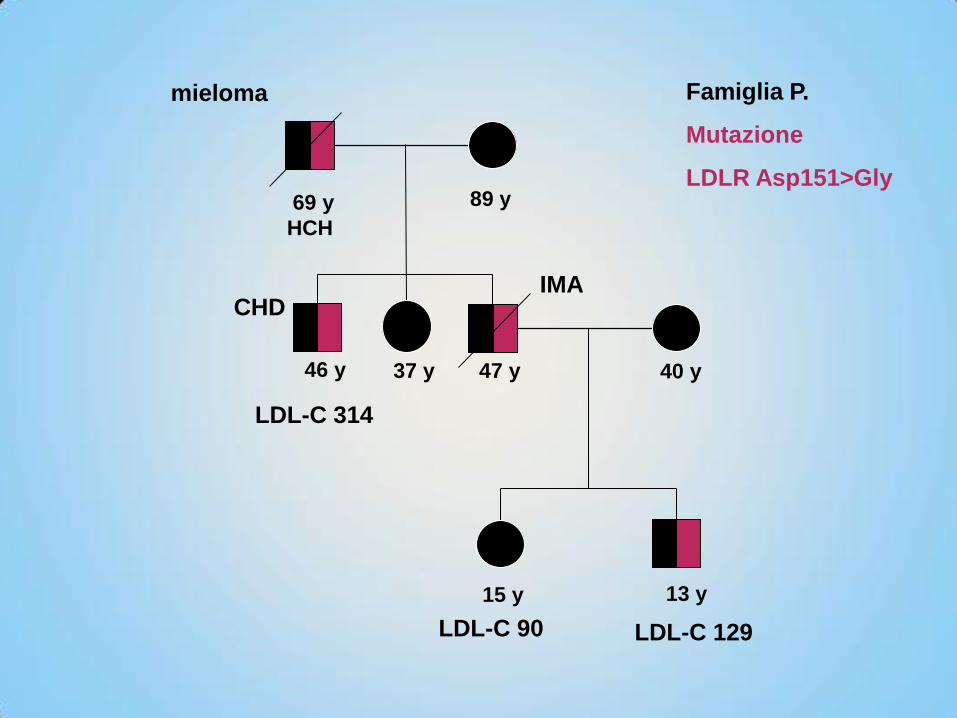
Il sig. PM di anni 47 in buona salute, non fumatore,
normoteso, normopeso. Una sera esce di casa per
andare a correre…
REFERTO AUTOPTICO:
…Coronarie: coronarosclerosi stenosante della
coronaria sinistra (risuzione del lume di circa 90%)
coronarosclerosi della coronaria destra: riduzione del
lume di circa il 50-60%)…
La causa di morte del sig. PM è da indentificarsi in una
insufficienza cardiaca acuta con EPA terminale in
soggetto affetto da coronarosclerosi di grado severo

In seguito all’evento, il fratello, il sig. PW di anni 46
anche lui in buona salute, non fumatore, normoteso,
normopeso, decide di effettuare esami ematochimici e
cardiologici:
Viene rilevato:
colesterolo totale 410 mg/dl
HDL 60 mg/dl
LDL 314 mg/dl
TG 180 mg/dl
ECG da sforzo: positivo per ischemia inducibile
Coronarografia: coronaropatia ostruttiva per cui
viene eseguita angioplastica coronarica in elezione

i figli del sig. PM, in buona salute, normopeso,
vengono valutati:
La ragazza di 15 anni presenta:
colesterolo totale 195 mg/dl
HDL 67 mg/dl
LDL 114 mg/dl
TG 69 mg/dl
Il ragazzo di 13 anni presenta:
colesterolo totale 254 mg/dl
HDL 56 mg/dl
LDL 176 mg/dl
TG 161 mg/dl
Ripetuto dopo alcuni giorni:
colesterolo totale 213 mg/dl
HDL 58 mg/dl
LDL 143 mg/dl
ripetuto dopo tre mesi:
Colesterolo totale 173 mg/dl
HDL 73 mg/dl
LDL 90 mg/dl
TG 48 mg/dl
ripetuto dopo tre mesi:
colesterolo totale 201 mg/dl
HDL 58 mg/dl
LDL 129 mg/dl
TG 64 mg/dl
ApoB 95 mg/dl
ApoA 139 mg/dl

Si procede con l’analisi del gene LDLR mediante
sequenziamento sul sig. PW per poi effettuare
l’eventuale “screening a cascata” sui nipoti

LDL B LDL b
LDL B
LDL B
LDL B
HEPATOCYTE
PLASMA
ADH-1 ADH-2 ADH-3
PCSK9 (GOF)
LDLR
47 y
13 y
40 y
15 y
LDL-C 90 LDL-C 129
Famiglia P.
Mutazione
LDLR Asp151>Gly
IMA
46 y
LDL-C 314
mieloma
69 y
HCH
89 y
CHD
37 y


9
HeFH: DIAGNOSTIC CRITERIA

Bertolini S, Pisciotta L et al.

Probability score according to the
clinical criteria of the Dutch Lipid
Clinic Network (DLCN):
-473 subjects (46.5%): “definite ADH”
-257 (25.2%): “probable ADH”
-288 (28.3%): “possible ADH”

In the group of 1018 index subjects, mutations in the
candidate genes were detected in 832 individuals (809
Italians and 23 of different ethnicities) with a mutation
detection rate of 82%.
-811 (97.4%): LDLR mutations (ADH-1),
-18 (2.2%): APOB mutations (ADH-2)
-3 (0.36%): PCSK9 mutations (ADH-3),
Mutation detection rate stratified according to DLCN score
“definite ADH” 435/473 (91.9%) 8.1% NO GEN.DIAGNOSIS
“probable ADH” 197/257 (76.6%)
“possible ADH” 200/288 (69.4%)
RESULTS: Mutation detection

Of 14 subjects classified as “definite HE-ADH” :
i) 12 resulted homozygotes (HO) or compound
heterozygotes (CHE) for mutations in LDLR
gene (8 HO and 4 CHE, respectively)
ii) 2 resulted double heterozygotes for
mutations in APOB and LDLR genes (one
subject) or for mutations in PCSK9 and LDLR
genes (one subject).

Prevalence and clinical impact of FH variants in a large U.S. clinical care cohort.
Noura S. Abul-Husn et al. Science 2016;354:aaf7000
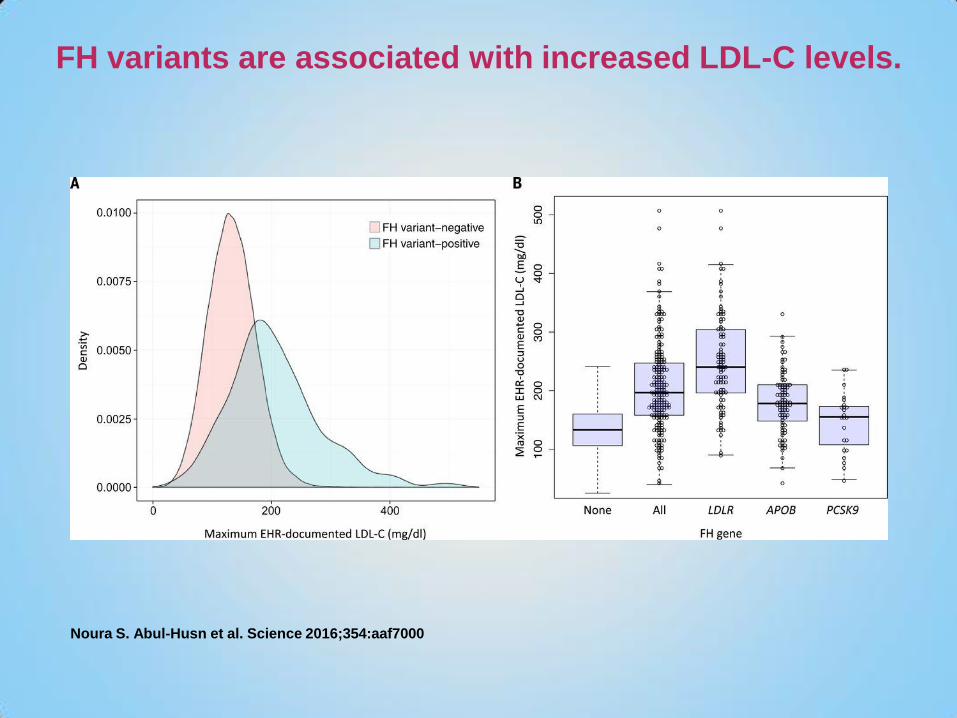
FH variants are associated with increased LDL-C levels.
Noura S. Abul-Husn et al. Science 2016;354:aaf7000

FH variants are associated with increased risk of CAD.
Noura S. Abul-Husn et al. Science 2016;354:aaf7000

Presequencing likelihood of FH diagnosis with DLCN criteria.
Noura S. Abul-Husn et al. Science 2016;354:aaf7000

When genetic diagnosis
can be useful ?

In homozygous phenotype

1. Plasma LDL-C level >13 mmol/L
(500 mg/dl)
2. Tendon and cutaneous xanthomas
in infancy
3. Hystory of hypercholesterolemia in
both parents
CLINICAL CRITERIA FOR HO-FH

EAS Consensus Panel statement on homozygous FH Stock J. Atherosclerosis 2015; 242: 323-6
*

In heterozygous phenotype

LDL-C levels in 1250 genetically characterized
heterozygous FH patients (values are adj. for gender and age)
LDL-C (mg/dL)
<150 175 200 225 250 275 300 325 350 375 400 425 450 475 500 >500
Bertolini S. 2011
Median 273.4 mg/dL
10th p. 205.5 mg/dL
25th p. 234.8 mg/dL
50th p. 273.4 mg/dL
90th p. 358.4 mg/dL
75th p. 317.6 mg/dL
5th p.189.3 mg/dL
95th p. 391.0 mg/dL

Prevalence of Tendon Xanthomatosis (%)
in 1116 FH patients in relation to age
Age (years)
-

FCHL LDLR +
N. 21/143 (14.7%)
M/F 10/11
Age (years) 45.812.1
BMI (kg/m2) 27.03.6
Tc (mg/dl) 365.055.4
HDLc (mg/dl) 46.619.6
Tg (mg/dl, median, range) 247 (147-810)
Spanish FCHL subjects positive for mutations in LDLR gene

TG ≤ 200 mg/dl TG > 200 mg/dl P
N. 585 78 (11.7%)
M/F 260/325 41/37 NS
Age (years) 48.912.0 51.110.9 NS
BMI (kg/m2) 24.23.4 26.73.4 0.0001
Tx (%) 47.2 53.2 NS
CAD (%) 30.6 39.7 NS
TC (mg/dl) 375.763.9 413.370.1 0.0001
LDL-C (mg/dl) 302.163.4 324.166.2 0.004
HDL-C (mg/dl) 51.313.9 42.410.6 0.0001
TG (mg/dl,
median, range) 112 (31-200) 244 (202-432) 0.0001
Comparison between FH subjects over 30 y of age with
pathogenic LDLR gene mutations according TG levels

Factors involved in TG
increase
Mutations in the LDLR repeat 5 (IDL binding)
common variants in LPL, APOA5, APOC3
genes such as (for example D9N and N291S,
or –1131 T>C and c.56 C>G (S19W)…
APOE 2 or 4 allele
Insulin resistance
…
In recessive phenotype

GENE Disease
LDLRAP1 ARH
ABCG5/G8 Sitosterolemia
LIPA LAL-D
Familial Hypercholesterolemia
(Recessive forms)

40 y
16 y
40 y
LDL-C 171
Apo B 120
LDL-C 104
Apo B 80
76 y
43 y
72 y
LDL-C 77
Apo B 52
LDL-C 115
Apo B 78
noTx; 1V-CAD,
PTCA
LDL-C 347
Apo B 178
LDLR c.328 G>C (Ex 4)
p.Cys109Ser (repeat 3)
19 y
LDL-C 92
Apo B 72
LDL-C 318
Apo B 195
LDLR c.28 T>A (Ex 1)
p.Trp10Arg (SP)
De novo LDLR gene mutations
(differential diagnosis with ARH)

In absence of family’s data

9 y
LDL-C 162 mg/dl
SMG 9 anni adottato vietnamita
In anamnesi Epatite B
In buona salute, normopeso
ABCG5 EX 3 Val113 FS c.335_336 Ins A
ABCG5 EX 3 Leu110>Gln c.329 T>A
In corso dosaggio di sitosteroli

SANGER SEQUENCING OF CANDIDATE GENEs
GENE PRICE
LDLR (18 exons) 640 euros
APOB ex26
(1 exon) 40 euros
PCSK9 (12 exons) 480 euros
Tot. 1160 euros

NGS (NEXT GENERATION SEQUENCING)
ALL GENES 300 euros

Italian Society of Atherosclerosis, LIPIGEN e Network Italiano delle
Dislipidemie Genetiche
http://www.sisa.it/LIPIGEN/

CONCLUSIONS
DIAGNOSIS OF FH IS A CLINICAL DIAGNOSIS
THE PHENOTYPE IS DETERMINANT IN THERAPEUTICAL
DECISIONs
GENETIC DIAGNOSIS, when available, CAN BE USEFUL
in HOMOZYGOUS PHENOTYPE, IN YOUNG PATIENTs, for
DIFFERENTIAL DIAGNOSIS with FCHL, for DIFFERENTIAL
DIAGNOSIS in RECESSIVE PHENOTYPE or in ABSENCE OF
FAMILY’S DATA