screening guidelines for procedural sedation
TRANSCRIPT
SCREENING GUIDELINES FOR PROCEDURAL SEDATION
Use these guidelines to determine whether your patient is appropriate for “Anesthesia Supervised RN Sedation” or “General Anesthesia” 1. Does the patient have pulmonary signs and symptoms? Oxygen saturation levels below 92% on room air at baseline Uses Oxygen continuously or at night Has difficulty breathing when lying supine Has been recently diagnosed with Pneumonia or RSV (less than 6 weeks ago) Has been diagnosed with Obstructive sleep apnea Parents have noted periods of apnea at night, or disturbed sleep in their child? 2. Does your patient have a potentially difficult airway? Receding or small jaw Small mouth opening Short and/or thick neck Decreased neck mobility/instability History of difficult airway Syndromes associated with a difficult airway (Treacher collins, Pierre Robin, Hunter-Hurler etc) (Presence of a tracheostomy does not preclude ability to sedate patient) 3. Does your patient have cardiac signs and symptoms? Congenital heart disease, Uncorrected Corrected congenital heart disease but has minimal activity level and/or low oxygen saturations (less than 92% on room air) Unstable cardiac condition (chest pain, Shortness of breath, critical aortic stenosis, congestive heart failure etc) 4. Did your patient experience a previous failed sedation with the Anesthesia supervised sedation team? 5. Does your patient have any involuntary movements / tremors? 6. Does the procedure(s) for which sedation is required likely to last longer than 3 hours? 7. Is your patient less than one year of age? If you have answered “NO” to all questions please book case as an “Anesthesia Supervised RN sedation” case. If you have answered “YES” to any of the questions above, or have any other related questions, please contact the Procedural Sedation Team (49099 or pager 7760). The Sedation team will help in assigning your patient to “General Anesthesia” or “Anesthesia Supervised RN Sedation”. Once the sedation team gives information about assigning the case as “Anesthesia Supervised RN Sedation” or General Anesthesia, it is still the responsibility of the schedulers of any service to book the case in the respective category. (The RN Sedation team does not schedule cases themselves) For SEDATION cases only, please make sure that you have also made arrangements for the “recovery phase” of your patient. You may contact the RN sedation team to help direct you to the right personnel to help with this important phase of care of your patient.

Procedural Sedation – Process Guidelines Department of Radiology
1. Patient to report to CT or MRI reception area.
2. Receptionist to page sedation team nurse on pager # 7760 when patient arrives (even if there’s a plan to try without sedation, so they can put EMLA cream on – just in case sedation is needed after the trial).
3. Sedation team nurse to call CT command center or MRI tech to communicate that patient is ready to start sedation med (10 minutes till scan). If any unplanned issues arise (i.e. scanner down), sedation plan to be negotiated. If scanners are down, CT or MRI should contact sedation team to make them aware.
4. Recovery – first MRI pediatric patient out of sedated scanner to be recovered in MRI, if more than one recovery at a time, the second patient to go to Nuc med recovery area on 3rd floor. In this scenario, page the Radiology charge nurse prior to leaving MRI.
5. Pediatric patients under 3 months of age or an ASA status of 3 need to have arrangements made to be recovered in the PSC.
6. If patient is being sedated by the PST for an IR procedure, a Radiology nurse will be involved in the initial prep to facilitate any procedure specific nursing tasks (i.e. antibiotics, etc).
Contact numbers:
Sedation team pgr: #7760
CT Command Center: 4-6167
MRI: 6-2236
CT Reception: 6-1901
CT Prep Room (Radiology RN): 6-1253
Radiology Charge Nurse pgr: #3802
Nuc Med Recovery Room: 4-6796
Sue Small (IR sedation questions): 6-2203
IR Scheduling pgr: #4644

Guidelines for Medication Administration for Procedural Sedation for Pediatric Patients
If there are contraindications, for any of the medications listed below, consult with staff to develop an
alternative plan.
GI Procedures: Age 10 yrs or older:
Propofol Infusion: Propofol (10mg/ml) Dose = 150mcg/kg/min. Infusion is to be started after pt monitoring has begun. Propofol infusion to run throughout the procedure or until notified by the proceduralist that there is less than 5 minutes remaining in the procedure, then at the discretion of the PST RN or Staff the propofol infusion may be discontinued.
Propofol Boluses: Propofol (10mg/ml) Dose = 0.5mg/kg. Administer boluses to achieve/maintain
Rikers of 2. Boluses may be given 30 seconds apart based on pt. sedation level. Additional boluses may be given throughout the procedure for breakthrough periods during procedure.
Versed: (1mg/ml) Dose = 0.1mg/kg (Max dose 2mg). 50% of full dose to be given to pt before
leaving recovery room area. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2mg/ml) Dose = 0.005mg/kg (Max dose 0.2mg). Glycopyrrolate should be
administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.
Age 0-9 yrs:
Propofol: (10mg/ml)/Ketamine (50mg/ml) Infusion: Dose = 125mcg/kg/min. Infusion is to be started after pt monitoring has begun. Propofol infusion to run throughout the procedure or until notified by the proceduralist that there is less than 5 minutes remaining in the procedure, then at the discretion of the PST RN or Staff Propofol, infusion may be discontinued.
Propofol Boluses: Propofol (10mg/ml) Ketamine: (50mg/ml) Dose = 0.5mg/kg. Administer boluses to achieve/maintain Rikers of 2. Boluses may be given 30 seconds apart based on pt. sedation level. Additional boluses may be given throughout the procedure for breakthrough periods during procedure
Versed: (1mg/ml) Dose = 0.1mg/kg (Max dose 2mg). 50% of full dose to be given to pt before
leaving recovery room area. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2mg/ml) Dose = 0.005mg/kg (Max dose 0.2mg). Glycopyrrolate should be
administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.
Bronchoscopies:
Propofol: Infusion: Propofol (10mg/ml) Dose = 150 mcg/kg/min. Infusion is to be started after pt monitoring has begun. Propofol infusion to run throughout the procedure or until notified by the proceduralist that there is less than 5 minutes remaining in the procedure. Infusion may be discontinued at the discretion of the PST RN or Staff at that time. The infusion rate may need to be adjusted down, at the discretion of the PST RN or Staff, to achieve sedation goal for exam.
Propofol Boluses: Propofol (10 mg/ml) Dose = 0.5 mg/kg. Administer boluses to achieve/maintain sedation necessary to achieve desired exam. Boluses may be given 30 seconds apart based on pt sedation level. Additional boluses may be given throughout the procedure for breakthrough periods.
Versed: (1mg/ml) Dose = 0.1 mg/kg (Max dose 2 mg). 50% of full dose to be given to pt once monitoring is started. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2 mg/ml) Dose = 0.005 mg/kg (Max dose 0.2 mg) Glycopyrrolate should be administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.
Renal Biopsies, PICC Lines, Ortho Procedures, Bone Marrow Biopsies/Aspiration, Interventional Radiology Procedures, Ultrasound/Fluro Procedures or any Invasive/Stimulating/Painful Procedure Age 10 yrs or older:
Propofol Infusion: Propofol (10mg/ml) Dose=150mcg/kg/min. Propofol infusion to run
throughout the procedure or until notified by the proceduralists that there is less than 5 minutes remaining in the procedure. Infusion may be discontinued at the discretion of the PST RN or Staff at that time.
Propofol Boluses: Propofol (10mg/ml) Dose= 0.5mg/kg Administer boluses to achieve/maintain
Rikers of 2. Boluses may be given 30 seconds apart based on pt. sedation level. Additional boluses may be given throughout the procedure for breakthrough periods.
Versed: (1mg/ml) Dose= 0.1mg/kg (Max dose 2mg). 50% of full dose to be given to pt before
leaving recovery room area. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2mg/ml) Dose=0.005mg/kg Max dose 0.2mg Glycopyrrolate should be
administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.
Age 9 yrs or less:
Propofol/Ketamine Infusion: (10mg/ml) / Ketamine (50mg/ml): Dose=125mcg/kg/min. Infusion is to be started after pt monitoring has begun. Propofol infusion to run throughout the procedure or until notified by the proceduralist that there is less than 5 minutes remaining in the procedure. Infusion may be discontinued at the discretion of the PST RN or Staff at that time.
Propofol Boluses: Propofol (10mg/ml) Dose= 0.5mg/kg Administer boluses to achieve/maintain
Rikers of 2. Boluses may be given 30 seconds apart based on pt. sedation level. Additional boluses may be given throughout the procedure for breakthrough periods.
Versed: (1mg/ml) Dose= 0.1mg/kg (Max dose 2mg). 50% of full dose to be given to pt before
leaving recovery room area. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2mg/ml) Dose=0.005mg/kg (Max dose 0.2mg). Glycopyrrolate should be
administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.

MRI/CT/Nuclear Medicine/ PET or Non-Invasive/Non-Stimulating Procedures < 60 Minutes
Dexmedetomidine Bolus: (4 mcg/ml). Give initial bolus of 3 mcg/kg for MRI, Nuc Med, PET over 10 minutes; bolus of 2 mcg/kg for CT over 10 minutes. If desired sedation level, Rikers of 3 is not achieved; a 2nd bolus may be given with the above parameters.
Dexmedetomidine Infusion: (4 mcg/ml). Infusion to be started after required sedation level achieved at 2 mcg/kg/hr for MRI, Nuc Med, PET; 1.5 mcg/kg/hr for CT. Infusion to continue until scan/procedure is complete.
Ketamine: Dose = 1 mg/kg. Ketamine should be used if the Dexmedetomidine is not effective. Ketamine must be diluted to a concentration of 5 mg/ml (1 ml of ketamine (50 mg) in 9 cc of sterile normal saline = final concentration of 5 mg/ml).
Normal Saline Infusion: Dose = 20 ml/kg. Infusion should be completed prior to discharge of patient if possible.
MRI/CT/Nuclear Medicine/ PET or Non-Invasive/Non-Stimulating Procedures – IF procedure is prolonged > 60 minutes or is combined with Invasive procedure, Propofol may be used instead of Dexmedetomidine after consulting with Staff.
Propofol Infusion: Propofol (10 mg/ml) Dose = 150 mcg/kg/min. Infusion is to be started after pt monitoring has begun. Propofol infusion to run throughout the procedure and may be reduced at the discretion of the PST RN or Staff, or until notified by the proceduralists that there is less than 5 minutes remaining in the procedure. Infusion may be discontinued at the discretion of the PST RN or Staff at that time.
Propofol Boluses: Propofol (10 mg/ml) Dose = 0.5 mg/kg. Administer boluses to achieve/maintain Rikers of 2. Boluses may be given 30 seconds apart based on pt sedation level. Additional boluses may be given throughout the procedure for breakthrough periods.
Versed: (1 mg/ml) Dose = 0.1 mg/kg (Max dose 2 mg). 50% of full dose to be given to pt before leaving Recovery Room area. The last 50% of full dose should be given prior to the start of the procedure.
Glycopyrrolate: (0.2 mg/ml) Dose = 0.005 mg/kg (Max dose 0.2 mg). Glycopyrrolate should be administered 10-15 minutes prior to procedure start time or as soon as possible before procedure begins.

Protocol – Intranasal (IN) Dexmedetomidine Procedural Sedation Team Indication: Short CT scans – usually < 3 minute scans – 60 min for entire
procedure
For whom: Children < 1 year of age
Dose: 2 mcg/kg IN through mucosal atomizer. Wait 20 minutes. If needed give an additional bolus of 1-2 mcg/kg IN.
Concentration: 100 mcg/ml. This preparation of Dexmedetomidine allows for atomization of volumes less than a milliliter.
Comments:
IN administration is effective with a smooth and predictable onset and with high patient acceptability [1, 2]. Onset is delayed compared with IV dosing. When adequate time is allowed, the clinical effect produced is comparable to that of IV and IM administration. Atomized particles of 10 to 20 µm are better distributed on the nasal mucosa, whereas drop solutions are primary deposited on the ciliary surface of the nose. Bioavailability of atomized sprays has been found to be superior to administration of drops into the nose [3]. Dexmedetomidine administered as atomized particles intranasally is effective in inducing observable sedation within 15-30 minutes of administration [3]. Significant sedation occurs 45-60 min after IN administration of drops of Dexmedetomidine. Sedative effect peaks after approximately 90-105 min [1, 2]. References:
1. Yuen, V.M., et al., A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia; a double-blinded randomized controlled trial. Anesth Analg, 2008. 106(6): p. 1715-21.
2. Yuen, V.M., et al., A double-blind, crossover assessment of the sedative and analgesic effects of intranasal dexmedetomidine. Anesth Analg, 2007. 105(2): p. 374-80.
3. Talon, M.D., et al., Intranasal dexmedetomidine premedication is comparable with midazolam in burn children undergoing reconstructive surgery. J Burn Care Res, 2009. 30(4): p. 599-605.
Merete Ibsen, 6/2/2010
Dea
r co
lleag
ues
Thi
s pr
oble
m h
as p
lagu
ed u
s fo
r ye
ars
and
the
Rad
iolo
gy d
ep
art
me
nt w
ould
be
real
ly a
ppre
ciat
ive
if w
e ca
n co
me
to
an
agre
emen
t on
thi
s.
Ple
ase
Not
e: A
ny
CT
tha
t is
ord
ered
as
ches
t/ab
dom
en/p
elvi
s o
r ab
dom
en/p
elvi
s a
lmo
st a
lway
s re
quire
s or
al c
on
tra
st (
in
addi
tion
to IV
con
tras
t).
If y
ou a
re n
ot s
ure,
ple
ase
text
pag
e 33
45 fo
r co
nfir
mat
ion
the
day
bef
ore
the
stu
dy o
r co
nta
ct
4614
7/8
(CT
con
trol
cen
ter)
to
conf
irm
wh
eth
er
this
pat
ient
will
nee
d or
al c
ontr
ast.
In o
rde
r th
at t
he i
mag
ing
qual
ity is
ade
quat
e an
d in
kee
ping
with
wh
at w
ould
be
cons
ider
ed "
safe
" w
e ha
ve c
om
e u
p w
ith
the
follo
win
g p
roto
col
SE
DA
TIO
N C
AS
ES
: N
PO
as
pe
r an
esth
esia
gui
delin
es.
The
pat
ient
is g
iven
on
e h
ou
r to
dri
nk
this
vol
ume,
but
we
enco
urag
e th
e pa
rent
to h
ave
the
child
dri
nk
the
conc
octio
n a
s fa
st a
nd a
s m
uch
as
poss
ible
. M
ost
chi
ldre
n e
ithe
r gul
p it
dow
n o
r st
op d
rinki
ng a
fte
r aro
und
10 m
inut
es.
Eve
n if
the
child
do
es n
ot d
rin
k th
e w
hole
or
requ
ired
amou
nt,
we
still
con
tinue
with
the
sed
atio
n:
We
wai
t fo
r O
NE
HO
UR
aft
er t
he la
st
aliq
uot i
s d
run
k an
d th
en w
e st
art
the
seda
tion.
Qua
ntity
of o
ral c
on
tra
st b
y ag
e:
Pre
emie
: 30
ml
0-1
year
: 8
0 m
l 2-
5 ye
ars:
12
0m
l 5-
10 y
ears
: 2
00
ml
10 y
ears
and
up:
25
0m
l
GE
NE
RA
L A
NE
ST
HE
SIA
CA
SE
S:
NP
O a
s p
er
an
est
he
sia
gui
delin
es.
Aft
er in
tuba
tion,
a N
G t
ube
is p
lace
d. I
t is
like
ly th
at la
rger
qua
ntiti
es th
an t
hat f
or
seda
tion
is g
iven
(so
me
time
tw
ice
the
am
ount
), t
hrou
gh t
he
NG
tube
. T
he c
hild
is p
lace
d ri
ght s
ide
dow
n fo
r 1
0-2
0 m
inut
es to
fac
ilita
te e
mpt
ying
of t
he s
tom
ach.
T
he i
mag
ing
stu
die
s ar
e th
en d
one.
The
res
idua
l am
ou
nt o
f co
ntr
ast
is s
ucke
d o
ut a
nd t
hen
the
pa
tien
t can
be
wok
en u
p a
nd
ext
ubat
ed.

Preparing Medications Propofol (10 mg/ml) – Draw up from vial at vial concentration. See individual procedures for Dosing. Propofol (10 mg/ml) / Ketamine (50 mg/ml) Mixture
20 ml Bottle P:K = 10:1 Propofol = 200 mg of 10 mg/ml Ketamine = 20 mg of 50 mg/ml P-K total volume = 20 ml + 0.4 ml
= 20 ml = 0.4 ml = 20.4 ml
1 ml of P/K = 10:1 contains 9.8 mg P + 0.98 mg K Propofol conc. = 9.8 mg/ml Ketamine conc. = 0.98 mg/ml
50 ml Bottle P:K = 10:1 Propofol Ketamine P-K total volume
= 500 mg of 10 mg/ml = 50 ml = 50 mg of 50 mg/ml = 1 ml = 50 ml + 1 ml = 51 ml
1 ml of P/K = 10:1 contains 9.8 mg P + 0.98 mg K Propofol conc. = 9.8 mg/ml Ketamine conc. = 0.98 mg/ml
Versed: (1 mg/ml) Draw up at vial strength. Dose = 1 mg/kg (Max dose 2 mg).
Glycopyrrolate (0.2 mg/ml) Draw up at vial strength. Dose = 0.005 mg/kg (Max dose 0.2 mg).
Ketamine: (50 mg/ml) Ketamine is supplied by pharmacy in 1 ml pre-drawn syringes. Ketamine must be diluted, when used in MRI/CT as an adjunct to Precedex, to a concentration of 5 mg/ml. (1 ml of ketamine (50 mg) in 9 cc of sterile normal saline = final concentration of 5 mg/ml). Dose = 1 mg/kg.
Fentanyl: (100 mcg/ml) Draw up at vial strength. Dose = 0.5 mcg/kg.
Precedex: (4 mcg/ml) Precedex is supplied in pre-mixed patient labeled Bags from pharmacy.
Dexmedetomidine Bolus: (4 mcg/ml). Give initial bolus of 3 mcg/kg for MRI, Nuclear Med, PET over 10 minutes; 2 mcg/kg for CT over 10 minutes.
Dexmedetomidine Infusion: (4 mcg/ml). Infusion to be started after required sedation level achieved at 2 mcg/kg/hr for MRI, Nuclear Med, PET; 1.5 mcg/kg/hr for CT.
ALL MEDICATION IS TO BE DRAWN UP USING ASEPTIC TECHNIQUE IN DESIGNATED AREAS AND DOUBLE CHECKED FoR ACCURACY BY ANOTHER RN.
Policy and Procedure Manual
Nursing Sedation Team N-SED-01.000 Policy
DRAFT REVISIONS – FORMAL APPROVAL PENDING
SUBJECT: Guidelines for Procedural Sedation Nurses Trained in the Department of Anesthesia
PURPOSE: Procedural sedation administered by the Procedural Sedation Nursing under the
supervision of an Anesthesia LIP. These guidelines apply only to those Registered Nurses who are trained and supervised by the Department of Anesthesia for Procedural Sedation.
Anesthesia trained personnel will provide sedation for patients following American Society of Anesthesiologists (ASA), The Joint Commission, and American Academy of Pediatrics (AAP) guidelines.
POLICY: A. SUFFICIENT AND QUALIFIED PERSONNEL
The person administering sedatives and monitoring the patient is responsible for the sedated patient and cannot be involved in other procedural activities. At a minimum, one Procedural Sedation Nurse will attend to each patient during sedation. A sedation-designated anesthesiologist will be immediately available to assist as needed. Procedural sedation team nurses who are responsible for sedation must be familiar with the medications and reversal agents, dosages, physiologic and adverse effects.
1. Credentialing/Competency Verification:
a. All procedural sedation nurses will be certified bi-annually in Basic Life
Support. b. All procedural sedation nurses responsible for sedation will be certified in
either PALS or ENPC, and in ACLS within 6 months of hire date or as soon as hospital-based classes are available. All procedural sedation nurses will re-certify every other year as required by PALS/ENPC and ACLS certification.
Continued Subject: Page 2 of 18
c. All procedural sedation nurses will take the UIHC PSRC Sedation Program
test online and pass it annually. d. All procedural sedation nurses will attend a pediatric sedation lectures
annually given by a member of the anesthesia sedation team faculty and will take the UIHC PSRC Pediatric Sedation Simulation Test and pass it annually.
e. All procedural sedation nurses shall be evaluated at least once a year on
airway skills in the operating room setting and complete the required minimum of 5 adult mask airway, 5 pediatric mask airway and place at least 2 LMAs (in both adults and pediatric patients depending on availability)
B. EQUIPMENT REQUIREMENTS
The following equipment and supplies must be readily available in the sedation room or area:
Crash cart Defibrillator Appropriate sized artificial airway, mask, and Ambu bag Bedside cardiac monitor/cable/electrodes Blood pressure cuff Hospital-approved crash cart Capnography or End Tidal CO2 monitoring using Salter cannulas Pharmacologic sedation agent Pulse oximetry monitor and sensor Suction source Supplemental oxygen source/supplies Complete supply of different size facemasks Flumazenil and Narcan must be readily available
C. PATIENT SELECTION CRITERIA PRESEDATION EVALUATION NOTE: CMS guidelines §482.52(b) (1). The Anesthesia Sedation team RN can complete a presedation evaluation note for moderate sedation. An Anesthesia LIP is required to complete a presedation assessment for all deep sedations/MAC/ and Gen Anesthesia.
1. Appropriate Patients:
All patients who will receive procedural nurse-administered sedation will be assessed by the procedural sedation nurse and by an anesthesiologist for their physical status according to the ASA Physical Status Classification. Please see link for the ASA physical status.
ASA Physical Status Classification (From http://www.asahg.org/clinical/physicalstatus.html)
Continued Subject: Page 3 of 18
NOTE: Patients with ASA Status 1 and 2 may be sedated if they meet sedation
guidelines. Patients with ASA Status 3 may be sedated only after approval by the
anesthesiologist.
2. Age criteria:
a. Infants under one month of age and ex-premature infants less than 60 weeks gestation are more prone to sedation complications such as apnea, and must be admitted to the hospital on an apnea monitor for a minimum of 12 apnea-free hours after sedation. When possible, imaging studies are conducted without sedation (e.g., during normal sleep). Elective studies should be deferred until the infant is over one month of age. Anesthesia LIP can make a clinical determination in exceptional cases
b. For patients between 1 and 12 months of age, the administration of oral
pentobarbital is an option only if the patient does not have IV access and will not require an IV for contrast. Exceptions to this guideline are made at the discretion of an anesthesiologist. Candidates for oral sedation will be scheduled in the mornings, with the last scheduled appointment made at 11:30 AM. Oral sedation must be administered before 12:00 PM if the patient is an outpatient. In most cases there is a need for IV placement as there is no guarantee that the patient would not require contrast.
NOTE: Patients receiving oral pentobarbital must be observed in the recovery area and
must meet discharge criteria or by order of the anesthesiologist before the patient can be discharged to home.
At the discretion of the sedation-designated anesthesiologist, oral pentobarbital may be administered in exceptional situation, after proper documentation of exceptional situation.
c. Patients older than 12 Months of Age: Primary sedation for patients more
than 12 months of age is IV pentobarbital, or ketamine. Midazolam may be added if the patient fails to sedate after receiving the maximum dose of pentobarbital and fentanyl, only after approval by the sedation-designated anesthesiologist. The last scheduled slot for IV pentobarbital sedation is 3:30 PM. Any patient sedated with pentobarbital protocol must be admitted overnight if any sedative (includes versed, pentobarbital, fentanyl) is subsequently administered after 4:30 PM.
NOTE: Oral midazolam is not part of the sedation protocol and should not be
administered unless under exceptional situations, at the discretion of the sedation-designated anesthesiologist.
Continued Subject: Page 4 of 18
d. Sedation with Dexmedetomidine 1) Sedation with dexmedetomidine is primarily to be used for non-
invasive radiological procedures such as MRI and CT scan. However, the anesthesiologist can use this drug for any other procedure at their discretion.
2) ‘Rescue” with pentobarbital or ketamine or midazolam to complete a study when dexmedetomidine is used as the primary drug for sedation is at the discretion of the anesthesiologist.
3) The high dose dexmedetomidine protocol is recommended for use MRI cases. There is no absolute cut-off age for using high dose dexmedetomidine. Age range can be from 0.2 to 17.9 years. However Dexmedetomidine sedation using the CT or MRI protocol is primarily for patients greater than one month or age
4) The dexmedetomidine sedation protocol is primarily to be used in the pediatric age group (up to 18 years).
5) The anesthesiologist should determine the appropriate dexmedetomidine dose for older adults using their clinical judgment.
6 7) It is not recommended to reverse bradycardia with glycopyrrolate
since there have been instances of significant hypertension post administration. Most children tolerate bradycardia. Please consider fluid bolus (total of 20ml/kg) for hypotension.
8) All patients who will be ambulating post sedation must have orthostatics done prior to discharge. Total fluid administration should be at least 20 ml/kg (unless contraindicated) prior to discharge
INTRANASAL Dexmedetomidine: This is suggested for short procedures that do not require the use of an IV line: example CT scans. The relative contraindications to use of dexmedetomidine are underlined below. The anesthesiologist can override any relative contraindication of dexmedetomidine based on their clinical judgment and needs for the procedure: 1) Active, uncontrolled gastro esophageal reflux 2) Active, uncontrolled vomiting 3) Current (or within the past 3 months) history of apnea requiring an
apnea monitor 4) Active, current respiratory issues that are different from the baseline
status (pneumonia, exacerbation of asthma, bronchiolitis, respiratory syncytial virus
5) Unstable cardiac status (life-threatening arrhythmias, abnormal cardiac anatomy, significant cardiac dysfunction)
6) Craniofacial anomaly, which could make it difficult to effectively establish mask airway for positive pressure ventilation if needed
7) Current use of digoxin, beta blockers, or calcium channel blockers
Continued Subject: Page 5 of 18
8) Moyamoya disease 9) Non-onset stroke Reference: High dose dexmedetomidine as the sole sedative for pediatric MRI: Mason et al : Pediatric Anesthesia 2008 18: 403–411
3. Special cases:
Any deviations from the following criteria must be approved by a staff anesthesiologist responsible for sedation.
a. Pentobarbital Sedation
1) If a patient requires a second radiological sedation with pentobarbital within 18 hours of initial medication administration, anesthesia must approve the patient for sedation.
2) Pentobarbital sedation may be administered on consecutive days
following an 18 hour interval between administrations. 3) The patient may receive a second radiological sedation on the same
day with different sedation protocols. These protocols may include dexmedetomidine, pentobarbital and ketamine. [Examples: 1) sedated with ketamine in Interventional Radiology followed by pentobarbital for MRI; 2) sedated with ketamine in Nuclear Medicine followed by pentobarbital for MRI.]
b. Patients with Acute Respiratory Issues
1) Patients with a cold or upper respiratory infection (URI): Patients
with an isolated nonproductive cold, cough, or clear runny nose are appropriate for sedation provided the patient is afebrile, has clear breath sounds, and remains at baseline appetite and activity level.
2) Patients with a history of asthma exacerbation, bronchiolitis, or
bronchitis are required to be at baseline respiratory status for at least six weeks before receiving sedation by PST nursing staff. This does not apply to patients who require bronchoscopy
3) Patients with respiratory syncytial virus (RSV): Any patient with a
clinical diagnosis of RSV or positive REV titer (even if clinically asymptomatic) may be sedated six weeks after the resolution of RSV. This does not apply to patients who need a bronchoscopy.
4) Patients with a history of pneumonia, empyema, or cystic fibrosis
are required to be six weeks from the resolution of the active process before scheduling for sedation by PST nursing staff. This does not

Continued Subject: Page 6 of 18
apply to patients who require a bronchoscopy. The anesthesiologist makes the final decision to proceed.
5) Patients with strep throat may be sedated following 24 hours of
appropriate antibiotic treatment as long as patient otherwise meets sedation criteria.
6) A patient who has had a tonsillectomy within past 8 weeks may be
approved only at the discretion of the anesthesiologist.
NOTE: Before the time of MRI or CT scan scheduling, if the patient has a cardiac
history, the results of the cardiac echo, chest x-ray and EKG results should be available so the procedural sedation nurse can include those results in the work-up for the sedation-designated anesthesiologist’s review. The sedation-designated anesthesiologist will determine if the child meets nurse-administered sedation criteria or requires a general anesthesia consult.
The EKG, chest x-ray and/or echo may be waived if the attending physician documents in the medical record that the patient is not at risk of cardiac disease.
Any additional exceptions to the above must be approved by the sedation-designated anesthesiologist. The sedation-designated anesthesiologist will document the clinical indication and any added risk related to the deviation from the guidelines in the medical record.
Any additional risks will be explained to the parents/guardians and added to the informed consent prior to sedation and parent/guardian signature.
c. Oral Midazolam
1) The use of oral midazolam is not recommended within the set
protocols of the other sedation medications. Nonetheless anesthesia personnel can use their own judgment to use this for anxiety. Protocol doses of subsequent medications may need to be adjusted due to the prolonged activity of oral midazolam.
D. SCHEDULING AND SCREENING OF RADIOLOGICAL EXAMINATIONS THAT
REQUIRE SEDATION
1. Routine Procedures:
All elective cases must be scheduled using the current UIHC scheduling system. Once a case is scheduled, a Procedural Sedation Nurse will screen the patient by reviewing documentation in the electronic medical record and will complete a pre-sedation assessment: a. By telephone interview with the patient/parent for outpatients.
Continued Subject: Page 7 of 18
b. On the inpatient unit for admitted patients. c. All relevant consultations, studies, and laboratory values must be attached to
the patient work-up if available.
NOTE: Non-urgent procedures must be scheduled during routine hours and preferably
before NOON on the day prior to the scheduled procedure.
2. Emergency Procedures:
Patients referred for urgent sedated procedures (e.g., CT, MRI, NM, and interventional radiology) are generally not being done by the procedural sedation team. If the need arises, an evaluation is done on a case-by-case basis and it is to the discretion of the anesthesiologist to consider nurse-administered procedural sedation for the procedure. Patients who do not meet the criteria for nurse administered procedural sedation will be referred to the Department of Anesthesia for further management. It should NOT be the expectation that the procedural sedation team carries out the necessary phone calls or appointments to schedule a case for general anesthesia. However, every effort to help to facilitate this process shall be made.
E. PRE-SEDATION GUIDELINES
1. Before the Patient Arrives:
a. Initial Assessment
A Procedural Sedation Nurse obtains the patient’s medical history from the parent/guardian and/or the patient, including:
1) Current and past medical history, current medications/herbs/dietary
supplements taken within the past two weeks including name/dose/frequency (including seizure medication, sedation and anesthesia). The procedure sedation nurse documents these findings on IPR.
2) NPO status. 3) Allergies. 4) Prior experiences with sedation/anesthesia. 5) Review of the medical record – including relevant laboratory values,
consultations, and any OUTSIDE studies. 6) If the patient is an inpatient, prior to scheduling the patient for
sedation, the procedural sedation nurse must perform a physical assessment. The results of the assessment will be shared with the
Continued Subject: Page 8 of 18
anesthesiologist for his/her use in determining the medical appropriateness for sedation.
b. Patient Fasting Guidelines
UI Hospital Fasting Guidelines as written by the Department of Anesthesia are followed: http://anesthesia.uihc.uiowa.edu/proceduralsedation3/adult/Fasting.asp
2. Before the Patient Procedure:
Considerations: Pediatric patients are accompanied to the procedure area by the parent or legal
guardian. Patients scheduled for body CT requiring oral contrast medium and sedation will
follow the fasting guidelines. In addition, the patient may be given oral water-soluble contrast as needed (based on the current agreed guideline set up between anesthesia and radiology) prior to sedation. Patients needing abdominal CT and MRI may undergo sedation for CT first, followed by MRI, providing 2 hours have elapsed between administration of oral contrast and placement in MRI scanner.
a. If no one is available to accompany the patient home, appropriate
arrangements for transportation home must be made before the patient is sedated.
b. The LIP and procedural sedation nurse (independently) must perform a
physical assessment of the patient with emphasis on the airway, respiratory, and cardiovascular systems.
c. The procedural sedation nurse completes the Sedation Monitoring Record
information on IPR including:
1) Prior sedation history 2) Medication history 3) Physical findings 4) Additional information if required
d. The LIP and procedural sedation nurse independently reviews the electronic
medical record for relevant medical information and clinical laboratory values and records this information on the Sedation Monitoring Record. Pertinent information may include EKG, CXR, cardiac echo, and other consult reports.
NOTE: If additional information or clarification about the case is required,
Anesthesiologist responsible for the sedation may contact the referring physician to request additional information.
Continued Subject: Page 9 of 18
e. The Procedural Sedation Nurse takes the patient’s vital signs UPON ARRIVAL to the procedural area and records them on the Sedation Monitoring Record (Anesthesia monitoring record) to include the following:
1) Blood pressure (syst/diast and Mean Arterial BP when necessary) 2) EtCO2 3) Heart rate 4) Oxygen saturation 5) Respiratory rate 6) Temperature 7) Weight in kilograms - may be from the most recent patient visit 8) Height in centimeters when clinically indicated
f. The procedural sedation nurse obtains written informed consent for sedation
from parent/legal guardian. The consent must be counter-signed by the anesthesiologist/provider.
g. The procedural sedation nurse consults with the anesthesiologist to review
the pertinent assessment information and history obtained from patient/parents or guardian. The medication plan is identified and discussed by the anesthesiologist and the procedural sedation nurse. Dosages are calculated, orders are written as defined per protocol and the anesthesiologist signs electonically.
h. Medications are administered following all applicable UIHC policies and
procedures, including the policy for high alert/high-risk medications if appropriate (insert correct title and link).
i. The anesthesiologist prescribing sedation drugs must be immediately
available by pager and respond as necessary
THE SUPERVISING PHYSICIAN NEEDS TO BE CONTACTED PRIOR TO INITIATION OF ANY SEDATION EVENT. PERMISSION TO START SEDATION MUST BE SOUGHT BY SEDATION NURSE PRIOR TO INITIATION OF SEDATION FOR ANY PATIENT.
F. PATIENT SEDATION PROCEDURES
1. Vital Sign Monitoring-Intra Procedure:
a. All patients receiving sedation must be monitored continuously by pulse oximetry.
b. Transcutaneous oxygen saturation is recorded every five minutes during
the procedure and every 15 minutes during recovery.
Continued Subject: Page 10 of 18
c. Blood pressure and heart rate baseline measurements should be obtained prior to sedation and then frequently during the onset of sedation or within 2-3 minutes. Documentation should be made at least every 5 minutes or more frequently if significant changes occur. In pediatric cases where measurement of the blood pressure may disturb the child and interrupt the procedure, the monitoring interval may be adjusted to the needs of the patient, at least every 15 minutes or intervals further increased with documented reasons. All patients must have a blood pressure reading recorded prior to discharge from the recovery area.
d. Oxygen via blow-by or nasal cannula at 2 liters is administered routinely to
sedated patients. e. End-tidal carbon dioxide monitoring is required for all sedated patients,
non-invasively by nasal/oral cannulas and results recorded at 5-minute intervals. Is this being used for other areas using conscious sedation? Not currently required being encouraged.
f. EKG monitoring is required on all sedated patients.
Note: Placement of monitors can be difficult prior to sedation of a child. All efforts are to be made to use ALL standard ASA monitors during the sedation process. The use of at least pulse oximetry before the child becomes sedated enough to allow for placement of all other monitors is HIGHLY recommended. Once the child is adequately sedated all standard ASA monitors should be used for the procedure.
2. Management of Adverse Effects of Sedation:
The anesthesiologist will be contacted immediately when a patient exhibits any adverse effect of sedation.
a. Hypoxemia
In the case of a drop in oxygen saturation, the procedural sedation nurse will institute basic resuscitation techniques (e.g., open airway, head repositioning, oxygen administration via face mask or ambu bag, suctioning). If the patient does not respond immediately to basic resuscitation techniques, Anesthesia will be summoned via stat page (3911) and the Anesthesia LIP be contacted directly by cell phone. Also, a Code Blue is called if patient has gone into cardiopulmonary arrest or is in impending arrest.
b. Paradoxical Reaction to IV Pentobarbital
Protect the patient from injury by holding the patient or padding the bed. Patients demonstrating “rage” or other aggressive behavior after awakening WILL NOT BE offered a caffeine-containing beverage (e.g., Coca Cola or Mountain Dew) nor any other oral intake during the rage episode. The anesthesiologist may consider the use of midazolam if the “rage” episode does not subside.

Continued Subject: Page 11 of 18
Any patient, who has had a history of rage for 30 minutes or more, is referred to anesthesia for management of future imaging studies, or other alternate sedation medications may be considered. The family is informed of the adverse reaction and instructed to list this as an adverse reaction when relaying the child’s history to any health care professional. The nurse caring for the patient describes the adverse event in the patient’s medical record and documents it in the electronic documentation system. The Procedural Sedation Committee views all paradoxical reactions as an adverse event.
G. POST SEDATION RECOVERY AND DISCHARGE
1. Patient Recovery Discharge criteria are based on current PACU guidelines (link). Following the procedure, patients are observed and monitored in the recovery area until discharge criteria are met or a discharge order is received from the sedation-designated anesthesiologist.
NOTE:
A patient may be transferred to the PACU only if approved by a staff anesthesiologist.
Patients who have received sedation must be escorted home by the parent/guardian or, in the case of patients over 18 years of age, by another responsible adult.
All patients who receive dexmedetomidine must get a total crystalloid fluid dose of 20 ml/kg for the whole procedure and prior to discharge. Patients who are ambulating post dexmedetomidine sedation must have orthostatics done prior to discharge. If patient’s standing systolic blood pressure is 20% below baseline, patient needs to get another 10ml/kg bolus and orthostatics measured again prior to discharge. Fluid management for patients with cardiac disease must be discussed with the supervising physician and and order obtained prior to administration. Discharge of patient from recovery area is based on prespecified criteria. The recovery nurse does not need to contact supervising physician unless these specific discharge criteria are not met by the patient
a. If the patient is transferred to the PACU
Upon transfer of the patient to PACU, the PACU physician will assume ongoing responsibility for the care of the patient. The procedural sedation nurse will give a verbal nurse-to-nurse report to the PACU nurse upon the patient’s arrival in the PACU. When discharge criteria are met, the patient
Continued Subject: Page 12 of 18
may be sent home or sent to the appropriate nursing unit after a full verbal report is given to the unit nurse and a discharge order written.
b. Unanticipated admission to the hospital
1) If the patient’s referring physician has admitting privileges at UIHC,
the patient will be admitted to referring MD’s service. 2) If the patient’s referring physician does not have admitting privileges,
the patient will be admitted using the following guidelines:
a) If a patient is older than 18 years and might require admission to an internal medicine service, call the internal medicine triage officer who is always on pager 5025. This will be a faculty physician who is responsible for accepting admissions to Medicine.
b) If the patient is older than 18 years and requires ICU care, the
patient can be admitted under Anesthesia in the Surgical ICU. Please call the triage officer for further assistance.
c) If a child (less than 18 years) requires admission to a general
pediatrics floor, call the senior pediatric resident on pager 3920. They will admit on the general pediatrics service or subspecialty if indicated. The pediatric service shall provide guidance about pediatric attending on call and accepting team.
d) If a child (less than 18 years) needs admission to intensive
care, please call the PICU pager at 3433 for further assistance.
c. Inpatients
1) When recovery discharge criteria are met, the procedural sedation nurse will provide report to the inpatient nurse. An RN will accompany all inpatients back to the unit following the procedure and a hand off report will be given.
NOTE: ALL patients will have at minimum pulse oxymetry monitoring done during transport.
2) Inpatients who receive nursing administered pentobarbital sedation
after 4:00 PM must have written orders from the anesthesiologist for 12 hours of pulse oximetry and apnea monitoring. These orders must be co-signed by the physician covering the inpatient service for the patient.
Continued Subject: Page 13 of 18
3) Inpatients from the Newborn ICU, Pediatric ICU, Cardiac ICU and Emergency Department will be recovered in the area of origin after transport by an RN and hand off report given.
H. SEDATION OF PEDIATRIC PATIENTS AT THE PEDIATRIC SPECIALTY CLINIC
1. Department of Anesthesia Fasting guidelines shall be followed on all patients: http://anesthesia.uihc.uiowa.edu/proceduralsedation3/adult/Fasting.asp
a. Exception to the above rule is for patients who are undergoing colonoscopic
procedures who require a bowel regimen prior to procedure. Since they are on a liquid diet at least 48 hours prior to procedure, the patients will follow DDC fasting guidelines (link).
b. Procedural Sedation Nurses shall interview parents, guardians or patients as
appropriate by telephone if possible, prior to the date of procedure. c. IV placement will be placed by the procedural sedation nurse or PSC nurse in
the pediatric specialty clinic if necessary.
d. Vital signs monitoring before and after procedure follows the same protocol as for procedural sedation in the radiology department.
e. The patients shall be taken to the recovery room in the recovery area and
handed over to the pediatric specialty clinic recovery nurse with a verbal report.
f. Anti-emetic medications can be given to the patients as appropriate prior to
the sedation procedure. g. Same day cases can be added on at the discretion of the anesthesiologist and
will be based on availability of the procedural sedation nurse and the type of concurrent cases and location of cases for that day.
2. Propofol use by the Sedation Team
a. Propofol can only be administered to patients (for procedural sedation) who are not intubated by nurses who are specifically trained and supervised by the Department of Anesthesia.
b. Propofol is to be administered on patients following the protocol developed
by the Department of Anesthesia. Any deviation from the protocol is to be cleared by the supervising member of the anesthesia team or the intensivist.
c. All procedural sedation nurses who administer propofol on non-intubated
patients have maintained advanced airway skills as set by the Department of Anesthesia.
Continued Subject: Page 14 of 18
d. As far as possible, all imaging studies should be performed with dexmedetomidine as the main sedative agent. Deviation from this or the use of propofol for imaging studies must be cleared by the anesthesiologist.
e. Concurrent propofol sedations in different locations must be cleared by the
anesthesiologist or intensivist who is supervising sedation. Anesthesia cans use their discretion to stagger cases if locations are not in contiguous locations.
f. The supervising physician must be immediately available for all propofol
sedations but not necessarily in continuous attendance of the sedation event. g. The use of end tidal CO2 must be mandatory for all sedations that use
propofol of propofol ketamine mixture and for all deep sedation procedures (level 3)
h. Propofol boluses must be administered according to protocol to attain the
level of sedation. The use of an infusion dose of propofol is recommended for all procedures greater than 10 minutes.
POST SEDATION EVALUATION (PRIOR TO DISCHARGE) (§ CMS 482.52
(b) (3)) An Anesthesia LIP needs to assess the patient prior to discharge and must complete
the assessment on EPIC within 48 hours. This applies to all patients who receive MAC, Gen Anesthesia, or Deep Sedation. (Dexmedetomidine is considered moderate sedation and therefore does not require a post sedation note to completed)
I. QUALITY IMPROVEMENT INDICATORS
All patients or guardians will be called by telephone by the next working day or on Monday (if the procedure occurred on Friday) and a post-sedation questionnaire will be completed by the procedural sedation team. Questions about somnolence, irritability, hyperactivity, nausea, vomiting, and IV site problems are addressed. Three attempts will be made and messages clearly indicating that the sedation team has called shall be left on the answering machine. The Sedation Committee reviews and monitors adverse events related to sedation. The following adverse events and their definitions are associated with sedation: 1. Quality assurance parameters are divided into sedation related events and
adverse events.
a. AIRWAY/Ventilation related problems: Abnormal oxygen saturation: Less than 90% saturation or decrease in saturation greater than 5% of baseline for greater than 60seconds (not applicable to patients with congenital heart disease) not amenable to usual interventions such as blow by oxygen,
Continued Subject: Page 15 of 18
position change, jaw thrust, short duration (less than 5 minutes) of bag mask ventilation.
1) Stridor (not applicable to pulmonary/bronchoscopy patients) 2) Wheezing (not applicable to pulmonary/bronchoscopy patients) 3) Aspiration (clinical diagnosis with or without chest x-ray findings)
b. Obstruction: Persistent loss of end tidal CO2, required jaw thrust or need for
oral airway throughout and immediately after procedure (not applicable to pulmonary/bronchoscopy procedures), to maintain ventilation (need for jaw thrust with GI endoscope placed in mouth is not to be considered a sedation related event unless jaw thrust is necessary even after GI scope has been removed for more than a minute).
c. Adverse event: Oxygen saturation less than 90% (or less than 5% of baseline) for greater than 60 seconds that does not respond to blow by oxygen, position change, jaw thrust, oral airway, removal of foreign body such as a bronchoscope and needs positive bag mask ventilation for more than 5 minutes for reversal. Patient requiring intubation is considered an adverse event unless decision to intubate was due to patient's underlying morbidity, example: poor respiratory reserve, aspiration risk, known obstructive sleep apnea on CPAP at home.
2. Medication related events
a. Prolonged sedation:
1) Dexmedetomidine: recovery greater than 3 hours after infusion was stopped.
2) Propofol and propofol/ketamine: recovery greater than 1.5 hours after infusion was stopped.
3) Midazolam/fentanyl: recovery greater than 1.5 hours after last dose of medication.
4) Ketamine only: greater than 3 hours after infusion of drug was stopped.
5) And patient does not reach baseline status within 24 hours.
b. Somnolence: Persistent sleepiness/drowsiness noted after discharge (at home) and within 24 hours of sedation event by parent or patient (note that sedation with drugs such as pentobarbital, due its long half-life can lead to persistent drowsiness for at least 18 hours and should not be reported as such).
c. Delirium: Irritability, agitation, dysphoria, hallucinations noted within 24
hours of a sedation event by parent or patient. d. Nausea and or vomiting during or after sedation and within 24 hours of the
sedation event.
Continued Subject: Page 16 of 18
e. Cardiovascular compromise:
f. Blood pressure: Systolic blood pressure less than or greater than 30% of
baseline sustained over 5 minutes and requires pharmacological therapy for reversal even after fluid bolus of 20 ml/kg.
g. Respiratory rate: RR less than or greater than 30% of baseline or apnea
(with loss of end tidal C02) for more than 30 seconds that is not amenable to position change or jaw thrust, or oral airway.
h. Inadequate sedation: Conditions for procedure suboptimal but procedure
nonetheless completed. (Example: Physician performing procedure complains that patient is moving too much or imaging quality is sub optimal but acceptable).
1) Inadequate sedation on recommended dose and despite rescue
doses of medications per protocol.
a) Adverse event: Patient required admission due to prolonged sedation Reversal agent required Inadequate sedation on recommended dose: procedure had
to be discontinued/cancelled due to suboptimal sedation conditions (If physician decides to change to MAC/GA to complete procedure then it is not considered as adverse event. It should be reported as a sedation related event).
b) Drug error: wrong drug, wrong dose regardless of whether patient was affected or not
3. Other
a. IV problem: greater than 3 attempts or IV mechanical problem identified that affected delivery of medication (extravasation of medication).
b. Unexpected admission: if it is directly related to sedation (example prolonged
sedation), then it should be reported as an adverse event. c. Change to MAC or General Anesthesia after procedure has started and
sedation deemed inadequate for procedure to continue safely. d. Allergic reaction: not to be confused with known side effects of medication.
(Rash is to be reported). e. Contrast related allergic reaction: difficulty breathing, hemodynamic
compromise temporally related to administration of IV contrast.
Continued Subject: Page 17 of 18
Any adverse event is to be reported to Anesthesia Clinical Conference Director for consideration for presentation at the Clinical Case Conference. All sedation related clinical conference presentations are mandatory for sedation nurses.
Date Created: 8/07 revised 9/2013
Source: Department of Anesthesia
Approved: Department of Anesthesia, 8/07
PNP, 11/11
Pharmacy and Therapeutics Subcommittee, 2/12
Effective Date: 2/12
Date Reviewed:
Date Revised: References: 1. American Society of Anesthesiologists Task Force on, S. and N.-A. Analgesia by, Practice
guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology, 2002. 96(4): p. 1004-17.
2. Apfelbaum, J.L., et al., Practice Guidelines for Postanesthetic Care: An Updated Report by the American Society of Anesthesiologists Task Force on Postanesthetic Care. Anesthesiology, 2013. 118(2): p. 291-307 10.1097/ALN.0b013e31827773e9.
3. Arlachov, Y. and R.H. Ganatra, Sedation/anaesthesia in paediatric radiology. British Journal of Radiology, 2012. 85(1019): p. e1018-e1031.
4. Bayman, E.O., et al., National Incidence of Use of Monitored Anesthesia Care. Anesthesia & Analgesia, 2011. 113(1): p. 165-169.
5. Candiotti, K.A., et al., Monitored Anesthesia Care with Dexmedetomidine: A Prospective, Randomized, Double-Blind, Multicenter Trial. Anesthesia & Analgesia, 2010. 110(1): p. 47-56.
6. Cauldwell, C., Anesthesia risks associated with pediatric imaging. Pediatric Radiology, 2011. 41(8): p. 949-950.
7. Commission, J., Sedation and anesthesia care standards. Joint Commission. 2010. 8. Coté, C.J., Safety After Chloral Hydrate Sedation of Former Preterm and Term Infants for
Magnetic Resonance Imaging: Are the Data Clear? Anesthesia & Analgesia, 2010. 110(3): p. 671-673.
9. Couloures, K.G., et al., Impact of Provider Specialty on Pediatric Procedural Sedation Complication Rates. Pediatrics, 2011. 127(5): p. e1154-e1160.
10. Cravero, J.P., et al., The Incidence and Nature of Adverse Events During Pediatric Sedation/Anesthesia With Propofol for Procedures Outside the Operating Room: A Report From the Pediatric Sedation Research Consortium. Anesthesia & Analgesia, 2009. 108(3): p. 795-804.
11. Delegates, A.H.o., Distinguishing Monitored Anesthesia Care ('MAC") from Moderate Sedation/Analgesia (Conscious Sedation). October 2009.
12. Delegates, A.H.o., Continuum of Depth of Sedation: Definition of General Anesthesia and Levels of Sedation/Analgesia. October 2009.
Continued Subject: Page 18 of 18
13. Delegates, t.H.A.H.o., Statement on Granting Privileges to Non Anethesiologists Physicians for Personally Administering or Supervising Deep Sedation. Oct, 2006, Amended on Oct 2012.
14. Eichhorn, V., D. Henzler, and M.F. Murphy, Standardizing care and monitoring for anesthesia or procedural sedation delivered outside the operating room. Current Opinion in Anesthesiology, 2010. 23(4): p. 494-499 10.1097/ACO.0b013e32833b9c9f.
15. Gaitan, B.D., et al., Sedation and Analgesia in the Cardiac Electrophysiology Laboratory: A National Survey of Electrophysiologists Investigating the Who, How, and Why? Journal of Cardiothoracic and Vascular Anesthesia, 2011. 25(4): p. 647-659.
16. Havidich, J.E. and J.P. Cravero, The current status of procedural sedation for pediatric patients in out-of-operating room locations. Current Opinion in Anesthesiology, 2012. 25(4): p. 453-460 10.1097/ACO.0b013e32835562d8.
17. Heuss, L.T., et al., Risk stratification and safe administration of propofol by registered nurses supervised by the gastroenterologist: A prospective observational study of more than 2000 cases. Gastrointestinal Endoscopy, 2003. 57(6): p. 664-671.
18. Hoffman, G.M., et al., Risk Reduction in Pediatric Procedural Sedation by Application of an American Academy of Pediatrics/American Society of Anesthesiologists Process Model. Pediatrics, 2002. 109(2): p. 236.
19. Mayr, N.P., et al., Should an Anesthesiologist Be Present on Site During Cardiologic Interventions? Journal of Cardiothoracic and Vascular Anesthesia, 2011. 25(6): p. e51.
20. McFadyen, J.G., N. Pelly, and R.J. Orr, Sedation and anesthesia for the pediatric patient undergoing radiation therapy. Current Opinion in Anesthesiology, 2011. 24(4): p. 433-438 10.1097/ACO.0b013e328347f931.
21. Metzner, J. and K.B. Domino, Risks of anesthesia or sedation outside the operating room: the role of the anesthesia care provider. Current Opinion in Anesthesiology, 2010. 23(4): p. 523-531 10.1097/ACO.0b013e32833b7d7c.
22. Tantri, A., et al., Anesthesia monitoring by registered nurses during cataract surgery: Assessment of need for intraoperative anesthesia consultation. Journal of Cataract & Refractive Surgery, 2006. 32(7): p. 1115-1118.
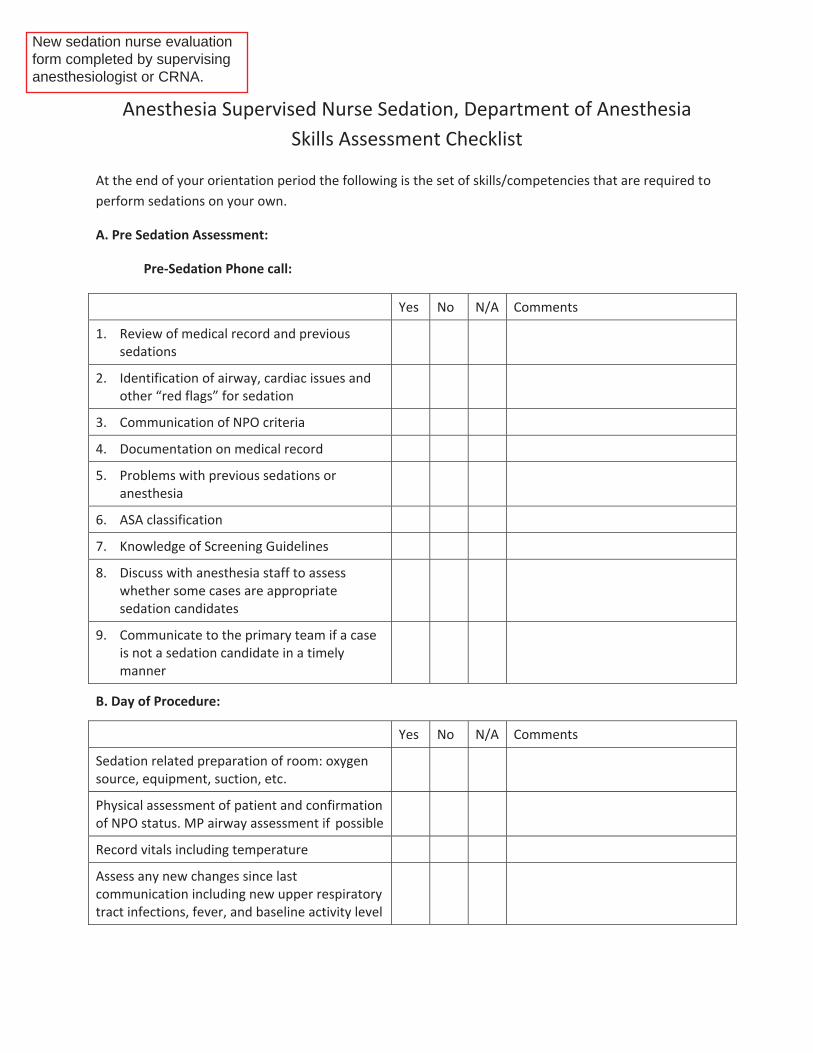
Anesthesia Supervised Nurse Sedation, Department of Anesthesia Skills Assessment Checklist
At the end of your orientation period the following is the set of skills/competencies that are required to perform sedations on your own.
A. Pre Sedation Assessment:
Pre-Sedation Phone call:
Yes No N/A Comments
1. Review of medical record and previous sedations
2. Identification of airway, cardiac issues and other “red flags” for sedation
3. Communication of NPO criteria
4. Documentation on medical record
5. Problems with previous sedations or anesthesia
6. ASA classification
7. Knowledge of Screening Guidelines
8. Discuss with anesthesia staff to assess whether some cases are appropriate sedation candidates
9. Communicate to the primary team if a case is not a sedation candidate in a timely manner
B. Day of Procedure:
Yes No N/A Comments
Sedation related preparation of room: oxygen source, equipment, suction, etc.
Physical assessment of patient and confirmation of NPO status. MP airway assessment if possible
Record vitals including temperature
Assess any new changes since last communication including new upper respiratory tract infections, fever, and baseline activity level
New sedation nurse evaluation form completed by supervising anesthesiologist or CRNA.

B. Day of Procedure (continued):
Yes No N/A Comments
Place LMA/LMX at the appropriate time and on strategic areas of the body of patient
Place an IV on the patient as necessary
Always talk to the anesthesia staff prior to administration of any medication
Know the set-up of pumps
Double check concentration and doses of drugs (using another nurse or faculty)
Follow protocol for medications used in sedation
Always contact the anesthesia staff if there are deviations from protocol
Identify level of sedation
Make appropriate adjustments to medications for under- and over-sedation
Identify airway and hemodynamic issues in a timely manner and take corrective actions as necessary
Have the required airway skills to handle potential airway problems like obstruction, apnea, hypoventilation and hypercarbia
Monitor patient’s vital signs continuously and record the vitals as per anesthesia regulations
Address potential hemodynamic issues by appropriate doses of fluid boluses as necessary
Know “When to call for the Anesthesia Staff or 3911”
Have knowledge of initial resuscitation of patient if patient decompensates, institute first steps and call for help
Follow UIHC guidelines for handling of scheduled medications

C. Post Procedure:
Yes No N/A Comments
1. Assess if safe to handover patient to the recovery nurse.
2. Handover the patient to the recovery staff after placing patient on recovery monitors and provide specified information to the recovery nurse
3. Complete medication record and complete medical record as scribe so that anesthesia staff can complete the medical record
4. Post procedure phone call and completion of the anesthesia database for sedation
5. Address assignments for subsequent sedations, paperwork, phone calls, and restocking of materials as recommended by the sedation team charge nurses
D. Other Responsibilities:
Yes No N/A Comments
1. Attend sedation meetings
2. Discuss ways to improve sedation satisfaction, efficiency and safety
3. Bring any issue related to sedation and human interaction to the Director and the Nurse Manager
4. Attend Anesthesia Clinical Case Conference for sedation related cases
5. Attend any lectures or presentations provided by anesthesia staff on sedation
6. Know how to start the anesthesia machine and set up for nitrous oxide
7. File PSNs as necessary
8. Complete airway requirements in the OR on a yearly basis
9. Attend simulation sessions
10. Read the information on sedation related topics on the Anesthesia Procedural Sedation Website on a yearly basis
1
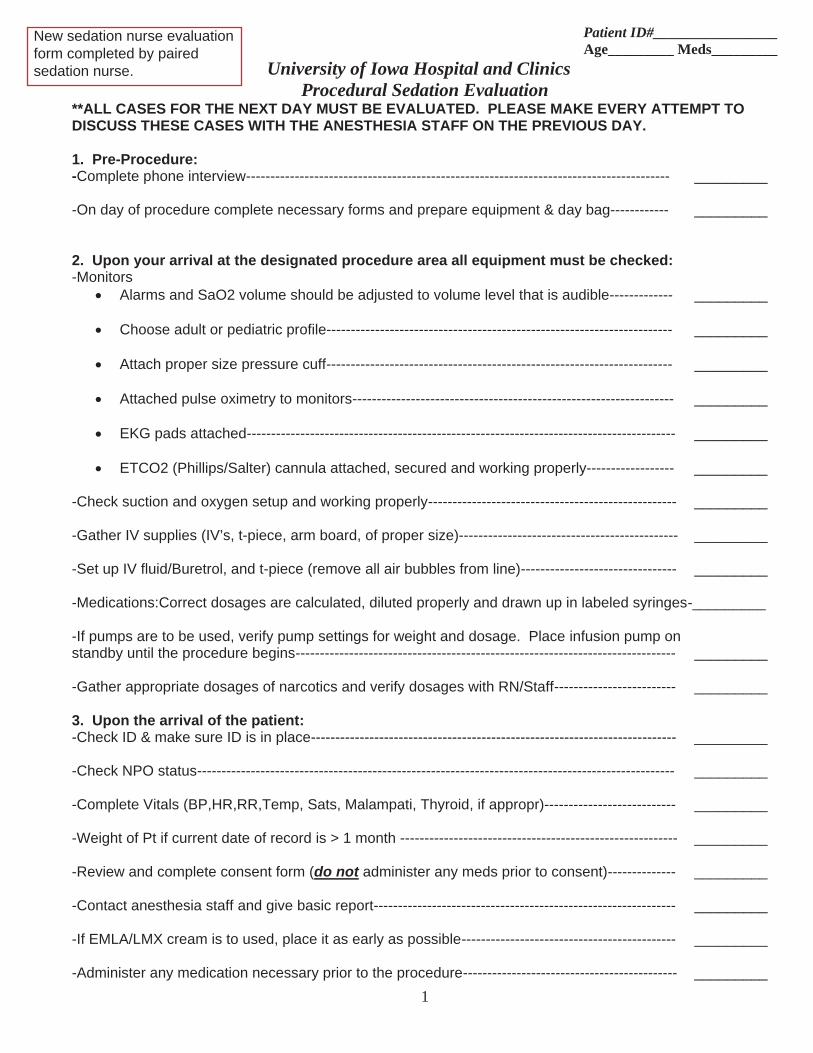
Patient ID#_________________ Age_________ Meds_________
University of Iowa Hospital and Clinics Procedural Sedation Evaluation
**ALL CASES FOR THE NEXT DAY MUST BE EVALUATED. PLEASE MAKE EVERY ATTEMPT TO DISCUSS THESE CASES WITH THE ANESTHESIA STAFF ON THE PREVIOUS DAY. 1. Pre-Procedure: -Complete phone interview--------------------------------------------------------------------------------------- _________ -On day of procedure complete necessary forms and prepare equipment & day bag------------ _________ 2. Upon your arrival at the designated procedure area all equipment must be checked: -Monitors
Alarms and SaO2 volume should be adjusted to volume level that is audible------------- _________ Choose adult or pediatric profile----------------------------------------------------------------------- _________
Attach proper size pressure cuff----------------------------------------------------------------------- _________
Attached pulse oximetry to monitors------------------------------------------------------------------ _________
EKG pads attached---------------------------------------------------------------------------------------- _________
ETCO2 (Phillips/Salter) cannula attached, secured and working properly------------------ _________
-Check suction and oxygen setup and working properly--------------------------------------------------- _________ -Gather IV supplies (IV’s, t-piece, arm board, of proper size)--------------------------------------------- _________ -Set up IV fluid/Buretrol, and t-piece (remove all air bubbles from line)-------------------------------- _________ -Medications:Correct dosages are calculated, diluted properly and drawn up in labeled syringes-_________ -If pumps are to be used, verify pump settings for weight and dosage. Place infusion pump on standby until the procedure begins------------------------------------------------------------------------------ _________ -Gather appropriate dosages of narcotics and verify dosages with RN/Staff------------------------- _________ 3. Upon the arrival of the patient: -Check ID & make sure ID is in place--------------------------------------------------------------------------- _________ -Check NPO status-------------------------------------------------------------------------------------------------- _________ -Complete Vitals (BP,HR,RR,Temp, Sats, Malampati, Thyroid, if appropr)--------------------------- _________ -Weight of Pt if current date of record is > 1 month --------------------------------------------------------- _________ -Review and complete consent form (do not administer any meds prior to consent)-------------- _________ -Contact anesthesia staff and give basic report-------------------------------------------------------------- _________ -If EMLA/LMX cream is to used, place it as early as possible-------------------------------------------- _________ -Administer any medication necessary prior to the procedure-------------------------------------------- _________
New sedation nurse evaluation form completed by paired sedation nurse.
2
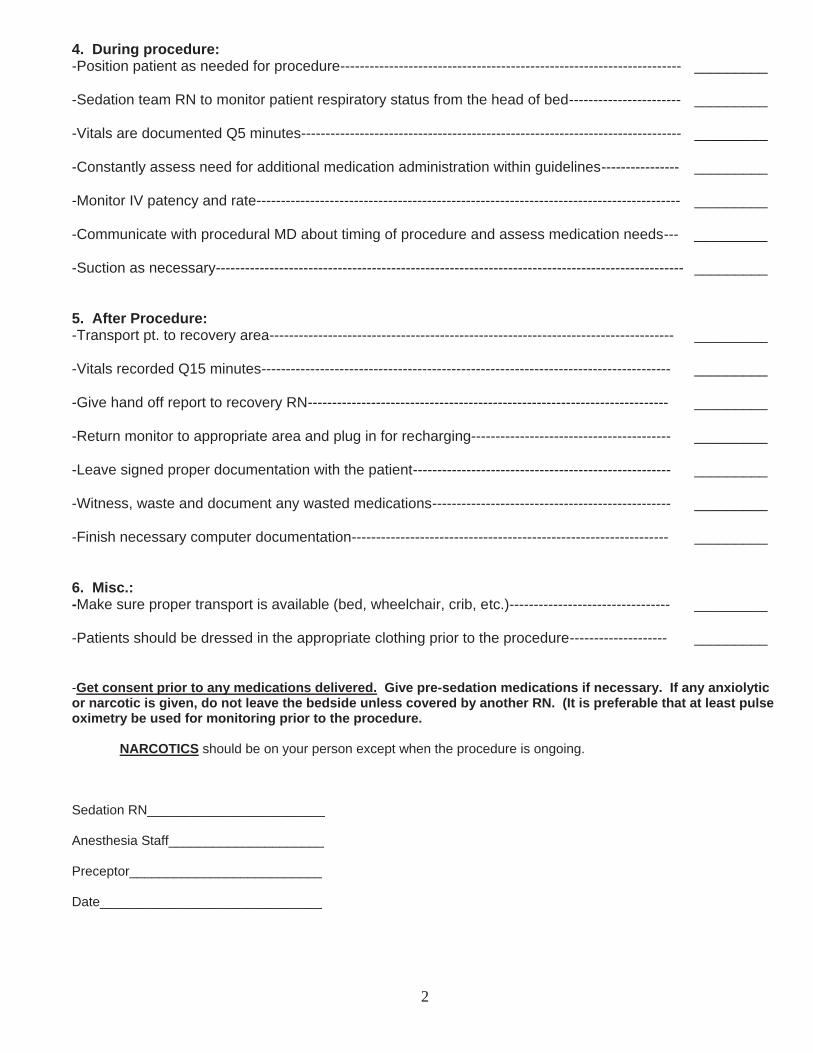
4. During procedure: -Position patient as needed for procedure---------------------------------------------------------------------- _________ -Sedation team RN to monitor patient respiratory status from the head of bed----------------------- _________ -Vitals are documented Q5 minutes------------------------------------------------------------------------------ _________ -Constantly assess need for additional medication administration within guidelines---------------- _________ -Monitor IV patency and rate--------------------------------------------------------------------------------------- _________ -Communicate with procedural MD about timing of procedure and assess medication needs--- _________ -Suction as necessary------------------------------------------------------------------------------------------------ _________ 5. After Procedure: -Transport pt. to recovery area----------------------------------------------------------------------------------- _________ -Vitals recorded Q15 minutes------------------------------------------------------------------------------------ _________ -Give hand off report to recovery RN-------------------------------------------------------------------------- _________ -Return monitor to appropriate area and plug in for recharging----------------------------------------- _________ -Leave signed proper documentation with the patient----------------------------------------------------- _________ -Witness, waste and document any wasted medications------------------------------------------------- _________ -Finish necessary computer documentation----------------------------------------------------------------- _________ 6. Misc.: -Make sure proper transport is available (bed, wheelchair, crib, etc.)--------------------------------- _________ -Patients should be dressed in the appropriate clothing prior to the procedure-------------------- _________ -Get consent prior to any medications delivered. Give pre-sedation medications if necessary. If any anxiolytic or narcotic is given, do not leave the bedside unless covered by another RN. (It is preferable that at least pulse oximetry be used for monitoring prior to the procedure. NARCOTICS should be on your person except when the procedure is ongoing. Sedation RN________________________ Anesthesia Staff_____________________ Preceptor__________________________ Date______________________________
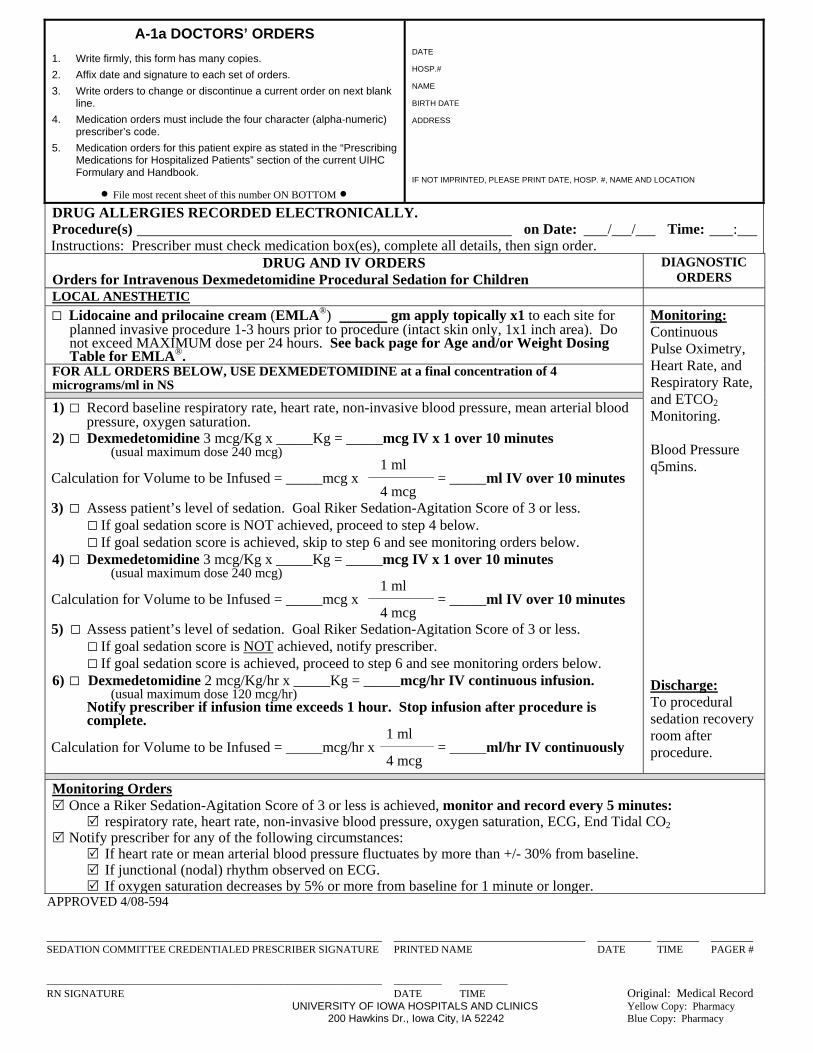
A-1a DOCTORS’ ORDERS
1. Write firmly, this form has many copies.
2. Affix date and signature to each set of orders.
3. Write orders to change or discontinue a current order on next blank line.
4. Medication orders must include the four character (alpha-numeric) prescriber’s code.
5. Medication orders for this patient expire as stated in the “Prescribing Medications for Hospitalized Patients” section of the current UIHC Formulary and Handbook.
File most recent sheet of this number ON BOTTOM
DATE
HOSP.#
NAME
BIRTH DATE
ADDRESS
IF NOT IMPRINTED, PLEASE PRINT DATE, HOSP. #, NAME AND LOCATION
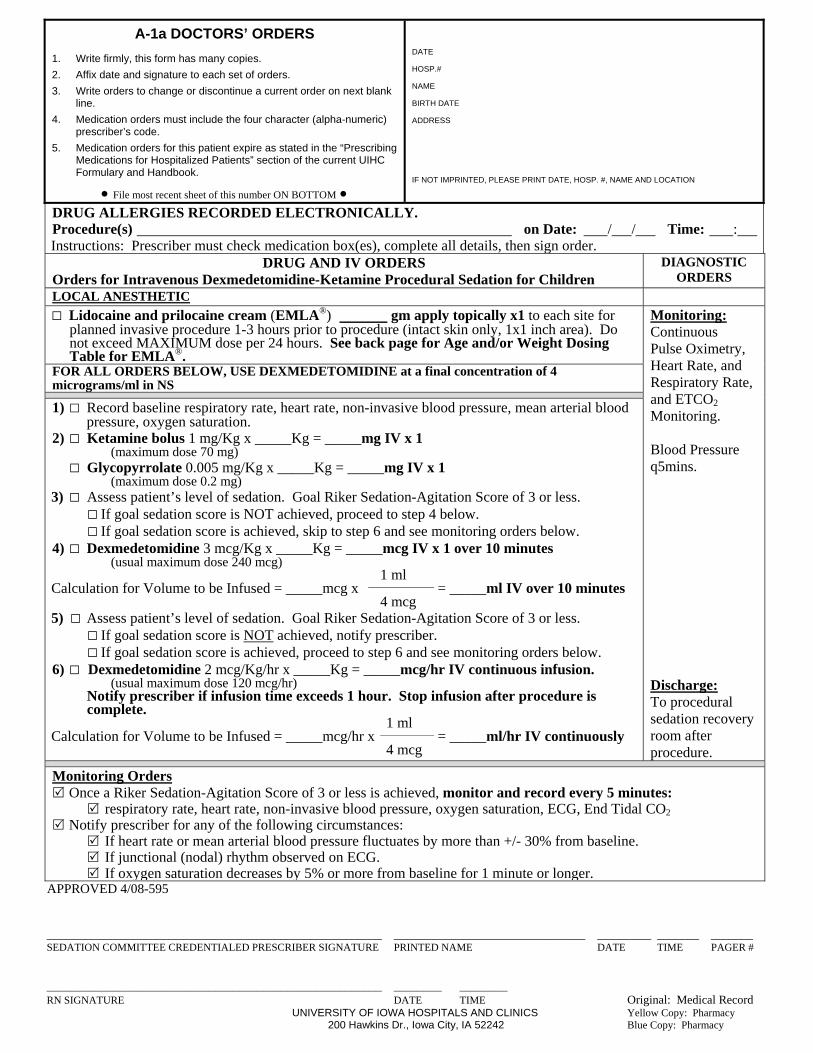
DRUG ALLERGIES RECORDED ELECTRONICALLY. Procedure(s) on Date: / / Time: : Instructions: Prescriber must check medication box(es), complete all details, then sign order.
DRUG AND IV ORDERS Orders for Intravenous Dexmedetomidine Procedural Sedation for Children
DIAGNOSTIC ORDERS
LOCAL ANESTHETIC
□ Lidocaine and prilocaine cream (EMLA®) gm apply topically x1 to each site for planned invasive procedure 1-3 hours prior to procedure (intact skin only, 1x1 inch area). Do not exceed MAXIMUM dose per 24 hours. See back page for Age and/or Weight Dosing Table for EMLA®.
Monitoring: Continuous Pulse Oximetry, Heart Rate, and Respiratory Rate, and ETCO2 Monitoring. Blood Pressure q5mins. Discharge: To procedural sedation recovery room after procedure.
FOR ALL ORDERS BELOW, USE DEXMEDETOMIDINE at a final concentration of 4 micrograms/ml in NS
1) □ Record baseline respiratory rate, heart rate, non-invasive blood pressure, mean arterial blood pressure, oxygen saturation.
2) □ Dexmedetomidine 3 mcg/Kg x _____Kg = _____mcg IV x 1 over 10 minutes (usual maximum dose 240 mcg) 1 ml Calculation for Volume to be Infused = _____mcg x = _____ml IV over 10 minutes 4 mcg 3) □ Assess patient’s level of sedation. Goal Riker Sedation-Agitation Score of 3 or less. □ If goal sedation score is NOT achieved, proceed to step 4 below. □ If goal sedation score is achieved, skip to step 6 and see monitoring orders below. 4) □ Dexmedetomidine 3 mcg/Kg x _____Kg = _____mcg IV x 1 over 10 minutes (usual maximum dose 240 mcg) 1 ml Calculation for Volume to be Infused = _____mcg x = _____ml IV over 10 minutes 4 mcg 5) □ Assess patient’s level of sedation. Goal Riker Sedation-Agitation Score of 3 or less. □ If goal sedation score is NOT achieved, notify prescriber. □ If goal sedation score is achieved, proceed to step 6 and see monitoring orders below. 6) □ Dexmedetomidine 2 mcg/Kg/hr x _____Kg = _____mcg/hr IV continuous infusion. (usual maximum dose 120 mcg/hr) Notify prescriber if infusion time exceeds 1 hour. Stop infusion after procedure is
complete. 1 ml Calculation for Volume to be Infused = _____mcg/hr x = _____ml/hr IV continuously
4 mcg
Monitoring Orders Once a Riker Sedation-Agitation Score of 3 or less is achieved, monitor and record every 5 minutes: respiratory rate, heart rate, non-invasive blood pressure, oxygen saturation, ECG, End Tidal CO2 Notify prescriber for any of the following circumstances: If heart rate or mean arterial blood pressure fluctuates by more than +/- 30% from baseline. If junctional (nodal) rhythm observed on ECG. If oxygen saturation decreases by 5% or more from baseline for 1 minute or longer.
APPROVED 4/08-594 ________________________________________________________ ________________________________ _________ _______ _______ SEDATION COMMITTEE CREDENTIALED PRESCRIBER SIGNATURE PRINTED NAME DATE TIME PAGER # ________________________________________________________ ________ ________ RN SIGNATURE DATE TIME Original: Medical Record
UNIVERSITY OF IOWA HOSPITALS AND CLINICS Yellow Copy: Pharmacy 200 Hawkins Dr., Iowa City, IA 52242 Blue Copy: Pharmacy
A-1a DOCTORS’ ORDERS
1. Write firmly, this form has many copies.
2. Affix date and signature to each set of orders.
3. Write orders to change or discontinue a current order on next blank line.
4. Medication orders must include the four character (alpha-numeric) prescriber’s code.
5. Medication orders for this patient expire as stated in the “Prescribing Medications for Hospitalized Patients” section of the current UIHC Formulary and Handbook.
File most recent sheet of this number ON BOTTOM
DATE
HOSP.#
NAME
BIRTH DATE
ADDRESS
IF NOT IMPRINTED, PLEASE PRINT DATE, HOSP. #, NAME AND LOCATION
DRUG ALLERGIES RECORDED ELECTRONICALLY. Procedure(s) on Date: / / Time: : Instructions: Prescriber must check medication box(es), complete all details, then sign order.
DRUG AND IV ORDERS Orders for Intravenous Dexmedetomidine-Ketamine Procedural Sedation for Children
DIAGNOSTIC ORDERS
LOCAL ANESTHETIC
□ Lidocaine and prilocaine cream (EMLA®) gm apply topically x1 to each site for planned invasive procedure 1-3 hours prior to procedure (intact skin only, 1x1 inch area). Do not exceed MAXIMUM dose per 24 hours. See back page for Age and/or Weight Dosing Table for EMLA®.
Monitoring: Continuous Pulse Oximetry, Heart Rate, and Respiratory Rate, and ETCO2 Monitoring. Blood Pressure q5mins. Discharge: To procedural sedation recovery room after procedure.
FOR ALL ORDERS BELOW, USE DEXMEDETOMIDINE at a final concentration of 4 micrograms/ml in NS
1) □ Record baseline respiratory rate, heart rate, non-invasive blood pressure, mean arterial blood pressure, oxygen saturation.
2) □ Ketamine bolus 1 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 70 mg) □ Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 0.2 mg) 3) □ Assess patient’s level of sedation. Goal Riker Sedation-Agitation Score of 3 or less. □ If goal sedation score is NOT achieved, proceed to step 4 below. □ If goal sedation score is achieved, skip to step 6 and see monitoring orders below. 4) □ Dexmedetomidine 3 mcg/Kg x _____Kg = _____mcg IV x 1 over 10 minutes (usual maximum dose 240 mcg) 1 ml Calculation for Volume to be Infused = _____mcg x = _____ml IV over 10 minutes 4 mcg 5) □ Assess patient’s level of sedation. Goal Riker Sedation-Agitation Score of 3 or less. □ If goal sedation score is NOT achieved, notify prescriber. □ If goal sedation score is achieved, proceed to step 6 and see monitoring orders below. 6) □ Dexmedetomidine 2 mcg/Kg/hr x _____Kg = _____mcg/hr IV continuous infusion. (usual maximum dose 120 mcg/hr) Notify prescriber if infusion time exceeds 1 hour. Stop infusion after procedure is
complete. 1 ml Calculation for Volume to be Infused = _____mcg/hr x = _____ml/hr IV continuously
4 mcg
Monitoring Orders Once a Riker Sedation-Agitation Score of 3 or less is achieved, monitor and record every 5 minutes: respiratory rate, heart rate, non-invasive blood pressure, oxygen saturation, ECG, End Tidal CO2 Notify prescriber for any of the following circumstances: If heart rate or mean arterial blood pressure fluctuates by more than +/- 30% from baseline. If junctional (nodal) rhythm observed on ECG. If oxygen saturation decreases by 5% or more from baseline for 1 minute or longer.
APPROVED 4/08-595 ________________________________________________________ ________________________________ _________ _______ _______ SEDATION COMMITTEE CREDENTIALED PRESCRIBER SIGNATURE PRINTED NAME DATE TIME PAGER # ________________________________________________________ ________ ________ RN SIGNATURE DATE TIME Original: Medical Record
UNIVERSITY OF IOWA HOSPITALS AND CLINICS Yellow Copy: Pharmacy 200 Hawkins Dr., Iowa City, IA 52242 Blue Copy: Pharmacy
A-1a DOCTORS’ ORDERS
1. Write firmly, this form has many copies.
2. Affix date and signature to each set of orders.
3. Write orders to change or discontinue a current order on next blank line.
4. Medication orders must include the four character (alpha-numeric) prescriber’s code.
5. Medication orders for this patient expire as stated in the “Prescribing Medications for Hospitalized Patients” section of the current UIHC Formulary and Handbook.
File most recent sheet of this number ON BOTTOM
DATE
HOSP.#
NAME
BIRTH DATE
ADDRESS
IF NOT IMPRINTED, PLEASE PRINT DATE, HOSP. #, NAME AND LOCATION
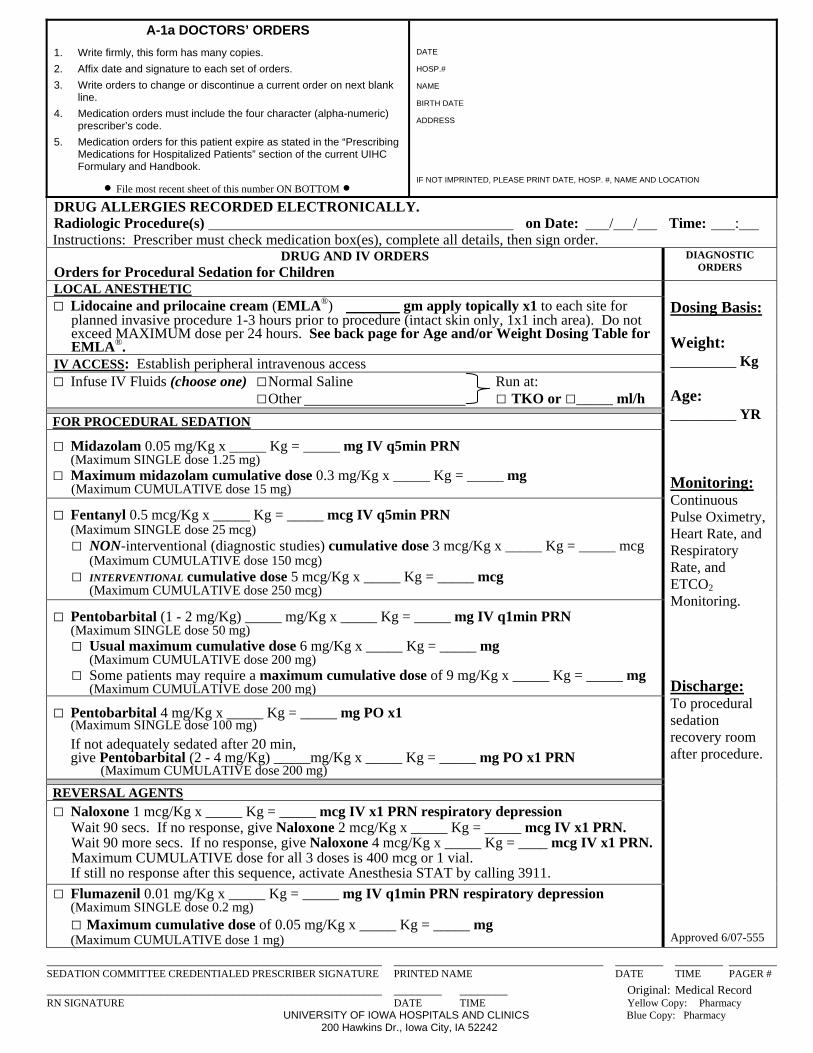
DRUG ALLERGIES RECORDED ELECTRONICALLY. Radiologic Procedure(s) on Date: / / Time: : Instructions: Prescriber must check medication box(es), complete all details, then sign order.
DRUG AND IV ORDERS Orders for Procedural Sedation for Children
DIAGNOSTIC ORDERS
LOCAL ANESTHETIC Dosing Basis: Weight: _________ Kg Age: _________ YR Monitoring: Continuous Pulse Oximetry,Heart Rate, and Respiratory Rate, and ETCO2 Monitoring. Discharge: To procedural sedation recovery room after procedure.
□ Lidocaine and prilocaine cream (EMLA®) gm apply topically x1 to each site for planned invasive procedure 1-3 hours prior to procedure (intact skin only, 1x1 inch area). Do not exceed MAXIMUM dose per 24 hours. See back page for Age and/or Weight Dosing Table for EMLA®.
IV ACCESS: Establish peripheral intravenous access □ Infuse IV Fluids (choose one) □ Normal Saline Run at:
□ Other □ TKO or □_____ ml/h
FOR PROCEDURAL SEDATION
□ Midazolam 0.05 mg/Kg x _____ Kg = _____ mg IV q5min PRN (Maximum SINGLE dose 1.25 mg) □ Maximum midazolam cumulative dose 0.3 mg/Kg x _____ Kg = _____ mg
(Maximum CUMULATIVE dose 15 mg)
□ Fentanyl 0.5 mcg/Kg x _____ Kg = _____ mcg IV q5min PRN (Maximum SINGLE dose 25 mcg) □ NON-interventional (diagnostic studies) cumulative dose 3 mcg/Kg x _____ Kg = _____ mcg (Maximum CUMULATIVE dose 150 mcg) □ INTERVENTIONAL cumulative dose 5 mcg/Kg x _____ Kg = _____ mcg (Maximum CUMULATIVE dose 250 mcg)
□ Pentobarbital (1 - 2 mg/Kg) _____ mg/Kg x _____ Kg = _____ mg IV q1min PRN (Maximum SINGLE dose 50 mg) □ Usual maximum cumulative dose 6 mg/Kg x _____ Kg = _____ mg (Maximum CUMULATIVE dose 200 mg) □ Some patients may require a maximum cumulative dose of 9 mg/Kg x _____ Kg = _____ mg (Maximum CUMULATIVE dose 200 mg)
□ Pentobarbital 4 mg/Kg x _____ Kg = _____ mg PO x1 (Maximum SINGLE dose 100 mg)
If not adequately sedated after 20 min, give Pentobarbital (2 - 4 mg/Kg) _____mg/Kg x _____ Kg = _____ mg PO x1 PRN (Maximum CUMULATIVE dose 200 mg)
REVERSAL AGENTS
□ Naloxone 1 mcg/Kg x _____ Kg = _____ mcg IV x1 PRN respiratory depression Wait 90 secs. If no response, give Naloxone 2 mcg/Kg x _____ Kg = _____ mcg IV x1 PRN. Wait 90 more secs. If no response, give Naloxone 4 mcg/Kg x _____ Kg = ____ mcg IV x1 PRN. Maximum CUMULATIVE dose for all 3 doses is 400 mcg or 1 vial.
If still no response after this sequence, activate Anesthesia STAT by calling 3911.
□ Flumazenil 0.01 mg/Kg x _____ Kg = _____ mg IV q1min PRN respiratory depression (Maximum SINGLE dose 0.2 mg) □ Maximum cumulative dose of 0.05 mg/Kg x _____ Kg = _____ mg (Maximum CUMULATIVE dose 1 mg)
Approved 6/07-555
________________________________________________________ ___________________________________ ________ ________ ________ SEDATION COMMITTEE CREDENTIALED PRESCRIBER SIGNATURE PRINTED NAME DATE TIME PAGER #
________________________________________________________ ________ ________ Original: Medical Record RN SIGNATURE DATE TIME Yellow Copy: Pharmacy UNIVERSITY OF IOWA HOSPITALS AND CLINICS Blue Copy: Pharmacy
200 Hawkins Dr., Iowa City, IA 52242
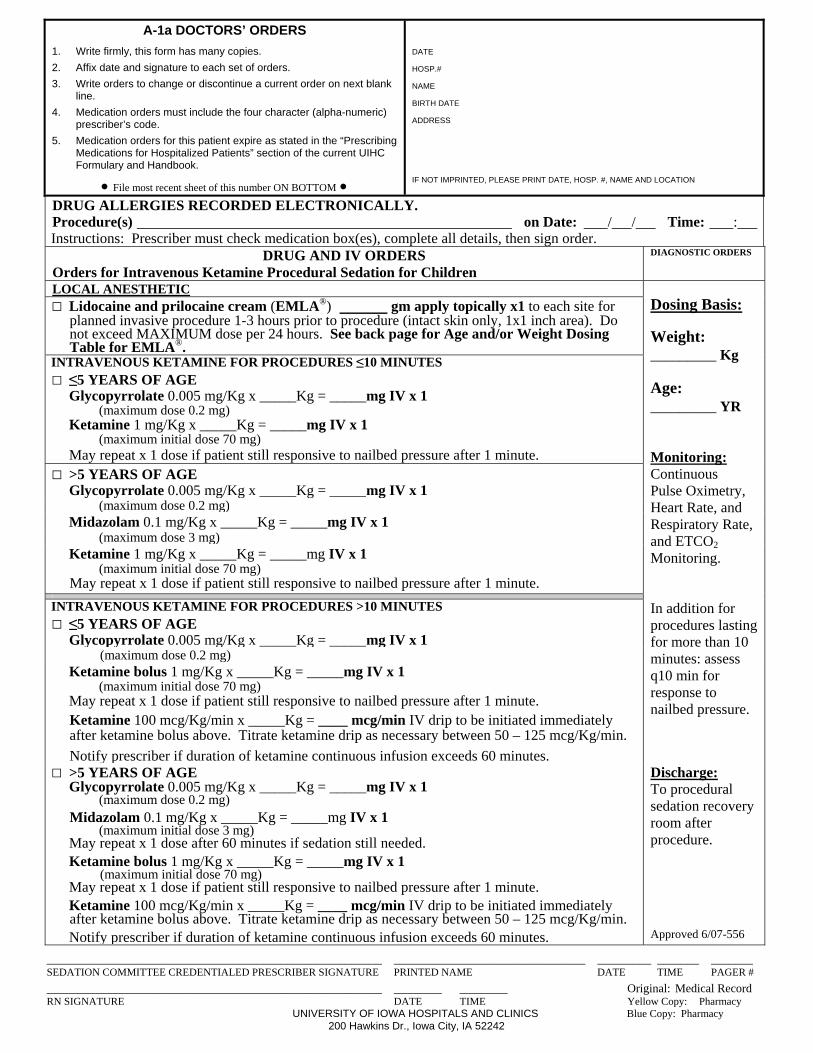
A-1a DOCTORS’ ORDERS
1. Write firmly, this form has many copies.
2. Affix date and signature to each set of orders.
3. Write orders to change or discontinue a current order on next blank line.
4. Medication orders must include the four character (alpha-numeric) prescriber’s code.
5. Medication orders for this patient expire as stated in the “Prescribing Medications for Hospitalized Patients” section of the current UIHC Formulary and Handbook.
File most recent sheet of this number ON BOTTOM
DATE
HOSP.#
NAME
BIRTH DATE
ADDRESS
IF NOT IMPRINTED, PLEASE PRINT DATE, HOSP. #, NAME AND LOCATION
DRUG ALLERGIES RECORDED ELECTRONICALLY. Procedure(s) on Date: / / Time: : Instructions: Prescriber must check medication box(es), complete all details, then sign order.
DRUG AND IV ORDERS Orders for Intravenous Ketamine Procedural Sedation for Children
DIAGNOSTIC ORDERS
LOCAL ANESTHETIC
Dosing Basis: Weight: _________ Kg Age: _________ YR Monitoring: Continuous Pulse Oximetry, Heart Rate, and Respiratory Rate, and ETCO2 Monitoring.
□ Lidocaine and prilocaine cream (EMLA®) gm apply topically x1 to each site for planned invasive procedure 1-3 hours prior to procedure (intact skin only, 1x1 inch area). Do not exceed MAXIMUM dose per 24 hours. See back page for Age and/or Weight Dosing Table for EMLA®.
INTRAVENOUS KETAMINE FOR PROCEDURES ≤10 MINUTES□ ≤5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 0.2 mg) Ketamine 1 mg/Kg x _____Kg = _____mg IV x 1 (maximum initial dose 70 mg)
May repeat x 1 dose if patient still responsive to nailbed pressure after 1 minute. □ >5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 0.2 mg)
Midazolam 0.1 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 3 mg) Ketamine 1 mg/Kg x _____Kg = _____mg IV x 1 (maximum initial dose 70 mg)
May repeat x 1 dose if patient still responsive to nailbed pressure after 1 minute.
INTRAVENOUS KETAMINE FOR PROCEDURES >10 MINUTES□ ≤5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IV x 1
In addition for procedures lasting for more than 10 minutes: assess q10 min for response to nailbed pressure.
(maximum dose 0.2 mg) Ketamine bolus 1 mg/Kg x _____Kg = _____mg IV x 1 (maximum initial dose 70 mg)
May repeat x 1 dose if patient still responsive to nailbed pressure after 1 minute.
Ketamine 100 mcg/Kg/min x _____Kg = ____ mcg/min IV drip to be initiated immediately after ketamine bolus above. Titrate ketamine drip as necessary between 50 – 125 mcg/Kg/min.
Notify prescriber if duration of ketamine continuous infusion exceeds 60 minutes.□ >5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IV x 1 (maximum dose 0.2 mg)
Midazolam 0.1 mg/Kg x _____Kg = _____mg IV x 1 (maximum initial dose 3 mg)
May repeat x 1 dose after 60 minutes if sedation still needed.
Ketamine bolus 1 mg/Kg x _____Kg = _____mg IV x 1 (maximum initial dose 70 mg) May repeat x 1 dose if patient still responsive to nailbed pressure after 1 minute.
Ketamine 100 mcg/Kg/min x _____Kg = ____ mcg/min IV drip to be initiated immediately after ketamine bolus above. Titrate ketamine drip as necessary between 50 – 125 mcg/Kg/min.
Notify prescriber if duration of ketamine continuous infusion exceeds 60 minutes.
Discharge: To procedural sedation recovery room after procedure.
Approved 6/07-556
________________________________________________________ ________________________________ _________ _______ _______ SEDATION COMMITTEE CREDENTIALED PRESCRIBER SIGNATURE PRINTED NAME DATE TIME PAGER #
________________________________________________________ ________ ________ Original: Medical Record RN SIGNATURE DATE TIME Yellow Copy: Pharmacy
UNIVERSITY OF IOWA HOSPITALS AND CLINICS Blue Copy: Pharmacy 200 Hawkins Dr., Iowa City, IA 52242
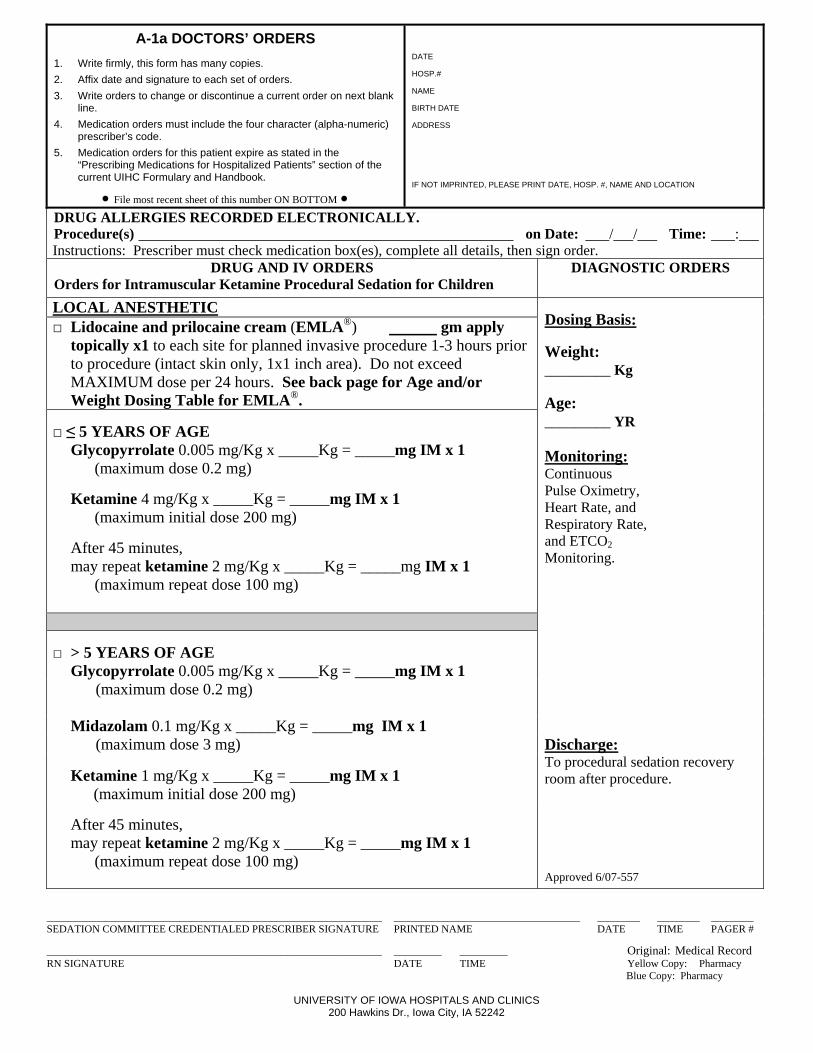
A-1a DOCTORS’ ORDERS
1. Write firmly, this form has many copies.
2. Affix date and signature to each set of orders.
3. Write orders to change or discontinue a current order on next blank line.
4. Medication orders must include the four character (alpha-numeric) prescriber’s code.
5. Medication orders for this patient expire as stated in the “Prescribing Medications for Hospitalized Patients” section of the current UIHC Formulary and Handbook.
File most recent sheet of this number ON BOTTOM
DATE
HOSP.#
NAME
BIRTH DATE
ADDRESS
IF NOT IMPRINTED, PLEASE PRINT DATE, HOSP. #, NAME AND LOCATION
DRUG ALLERGIES RECORDED ELECTRONICALLY. Procedure(s) on Date: / / Time: : Instructions: Prescriber must check medication box(es), complete all details, then sign order.
DRUG AND IV ORDERS Orders for Intramuscular Ketamine Procedural Sedation for Children
DIAGNOSTIC ORDERS
LOCAL ANESTHETIC
Dosing Basis: Weight: _________ Kg Age: _________ YR Monitoring: Continuous Pulse Oximetry, Heart Rate, and Respiratory Rate, and ETCO2 Monitoring.
□ Lidocaine and prilocaine cream (EMLA®) gm apply topically x1 to each site for planned invasive procedure 1-3 hours prior to procedure (intact skin only, 1x1 inch area). Do not exceed MAXIMUM dose per 24 hours. See back page for Age and/or Weight Dosing Table for EMLA®.
□ ≤ 5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IM x 1 (maximum dose 0.2 mg)
Ketamine 4 mg/Kg x _____Kg = _____mg IM x 1 (maximum initial dose 200 mg)
After 45 minutes, may repeat ketamine 2 mg/Kg x _____Kg = _____mg IM x 1 (maximum repeat dose 100 mg)
□ > 5 YEARS OF AGE Glycopyrrolate 0.005 mg/Kg x _____Kg = _____mg IM x 1
(maximum dose 0.2 mg)
Midazolam 0.1 mg/Kg x _____Kg = _____mg IM x 1 (maximum dose 3 mg) Discharge:
To procedural sedation recovery room after procedure.
Ketamine 1 mg/Kg x _____Kg = _____mg IM x 1 (maximum initial dose 200 mg)
After 45 minutes, may repeat ketamine 2 mg/Kg x _____Kg = _____mg IM x 1 (maximum repeat dose 100 mg)
Approved 6/07-557
_______________________________________________________________ ___________________________________ ________ ________ ________ SEDATION COMMITTEE CREDENTIALED PRESCRIBER SIGNATURE PRINTED NAME DATE TIME PAGER # ________________________________________________________ ________ ________ Original: Medical Record RN SIGNATURE DATE TIME Yellow Copy: Pharmacy
Blue Copy: Pharmacy
UNIVERSITY OF IOWA HOSPITALS AND CLINICS 200 Hawkins Dr., Iowa City, IA 52242
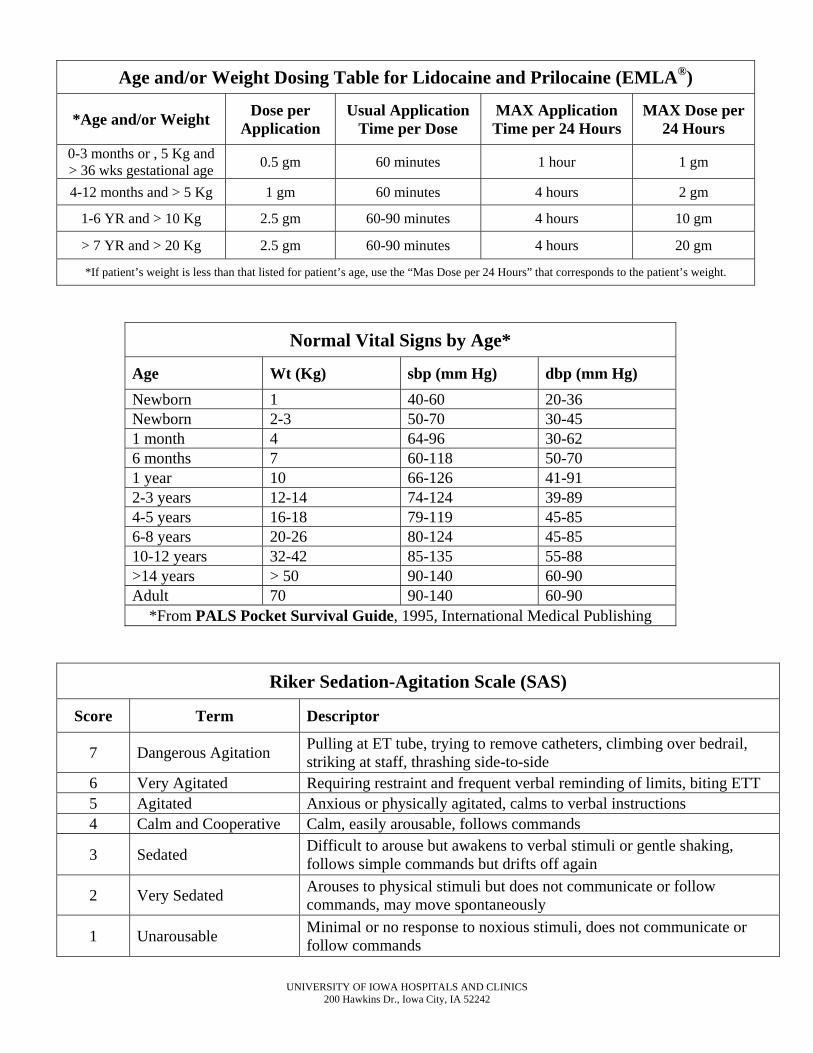
UNIVERSITY OF IOWA HOSPITALS AND CLINICS 200 Hawkins Dr., Iowa City, IA 52242
Age and/or Weight Dosing Table for Lidocaine and Prilocaine (EMLA®)
*Age and/or Weight Dose per
Application Usual Application
Time per Dose MAX Application Time per 24 Hours
MAX Dose per 24 Hours
0-3 months or , 5 Kg and > 36 wks gestational age
0.5 gm 60 minutes 1 hour 1 gm
4-12 months and > 5 Kg 1 gm 60 minutes 4 hours 2 gm
1-6 YR and > 10 Kg 2.5 gm 60-90 minutes 4 hours 10 gm
> 7 YR and > 20 Kg 2.5 gm 60-90 minutes 4 hours 20 gm
*If patient’s weight is less than that listed for patient’s age, use the “Mas Dose per 24 Hours” that corresponds to the patient’s weight.
Normal Vital Signs by Age*
Age Wt (Kg) sbp (mm Hg) dbp (mm Hg)
Newborn 1 40-60 20-36 Newborn 2-3 50-70 30-45 1 month 4 64-96 30-62 6 months 7 60-118 50-70 1 year 10 66-126 41-91 2-3 years 12-14 74-124 39-89 4-5 years 16-18 79-119 45-85 6-8 years 20-26 80-124 45-85 10-12 years 32-42 85-135 55-88 >14 years > 50 90-140 60-90 Adult 70 90-140 60-90
*From PALS Pocket Survival Guide, 1995, International Medical Publishing
Riker Sedation-Agitation Scale (SAS)
Score Term Descriptor
7 Dangerous Agitation Pulling at ET tube, trying to remove catheters, climbing over bedrail, striking at staff, thrashing side-to-side
6 Very Agitated Requiring restraint and frequent verbal reminding of limits, biting ETT 5 Agitated Anxious or physically agitated, calms to verbal instructions 4 Calm and Cooperative Calm, easily arousable, follows commands
3 Sedated Difficult to arouse but awakens to verbal stimuli or gentle shaking, follows simple commands but drifts off again
2 Very Sedated Arouses to physical stimuli but does not communicate or follow commands, may move spontaneously
1 Unarousable Minimal or no response to noxious stimuli, does not communicate or follow commands
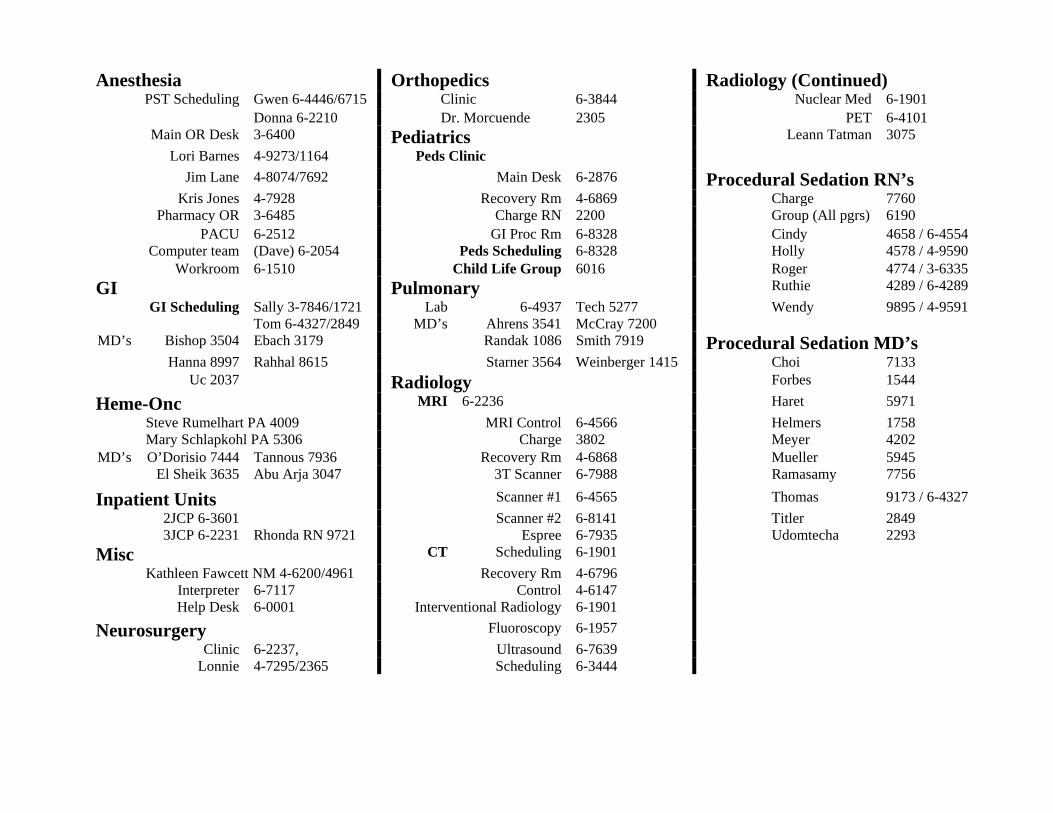
Anesthesia Orthopedics Radiology (Continued) PST Scheduling Gwen 6-4446/6715 Clinic 6-3844 Nuclear Med 6-1901
Donna 6-2210 Dr. Morcuende 2305 PET 6-4101 Main OR Desk 3-6400 Pediatrics Leann Tatman 3075
Lori Barnes 4-9273/1164 Peds Clinic
Jim Lane 4-8074/7692 Main Desk 6-2876 Procedural Sedation RN’s Kris Jones 4-7928 Recovery Rm 4-6869 Charge 7760 Pharmacy OR 3-6485 Charge RN 2200 Group (All pgrs) 6190 PACU 6-2512 GI Proc Rm 6-8328 Cindy 4658 / 6-4554 Computer team (Dave) 6-2054 Peds Scheduling 6-8328 Holly 4578 / 4-9590 Workroom 6-1510 Child Life Group 6016 Roger 4774 / 3-6335
GI Pulmonary Ruthie 4289 / 6-4289
GI Scheduling Sally 3-7846/1721 Lab 6-4937 Tech 5277 Wendy 9895 / 4-9591 Tom 6-4327/2849 MD’s Ahrens 3541 McCray 7200 MD’s Bishop 3504 Ebach 3179 Randak 1086 Smith 7919 Procedural Sedation MD’s
Hanna 8997 Rahhal 8615 Starner 3564 Weinberger 1415 Choi 7133 Uc 2037 Radiology Forbes 1544
Heme-Onc MRI 6-2236 Haret 5971
Steve Rumelhart PA 4009 MRI Control 6-4566 Helmers 1758 Mary Schlapkohl PA 5306 Charge 3802 Meyer 4202 MD’s O’Dorisio 7444 Tannous 7936 Recovery Rm 4-6868 Mueller 5945
El Sheik 3635 Abu Arja 3047 3T Scanner 6-7988 Ramasamy 7756
Inpatient Units Scanner #1 6-4565 Thomas 9173 / 6-4327
2JCP 6-3601 Scanner #2 6-8141 Titler 2849 3JCP 6-2231 Rhonda RN 9721 Espree 6-7935 Udomtecha 2293
Misc CT Scheduling 6-1901
Kathleen Fawcett NM 4-6200/4961 Recovery Rm 4-6796 Interpreter 6-7117 Control 4-6147 Help Desk 6-0001 Interventional Radiology 6-1901
Neurosurgery Fluoroscopy 6-1957
Clinic 6-2237, Ultrasound 6-7639 Lonnie 4-7295/2365 Scheduling 6-3444

Department of Radiology Policy on Intravenous Contrast in Adults
Purpose: The purpose of this policy is to:
1) Ensure appropriate premedication in patients with known/suspected allergic reactions;
2) Ensure contrast administration is performed according to hospital and departmental protocols with appropriate supervision by a licensed independent practitioner (LIP).
3) Ensure appropriate actions are undertaken in case of contrast reactions and extravasation of contrast;
4) Ensure laboratory testing requirements conducted in patients in whom contrast administration is considered.
Policy Statement: The policy will be based on the Manual on Contrast Media (ACR, 2006) and other relevant literature. The policy is specifically applicable to ADULT patients. Guidelines for administration of Intravenous contrast:
1. A radiologic technologist or radiology nurse may administer intravenous contrast under the supervision of a licensed independent practitioner and in accordance with procedure defined in this policy and following protocols that are based upon the type of examination order and define the type, dose and route of contrast.
2. The supervising LIP or his/her physician designee must be available to respond promptly to an adverse event related to contrast administration.
3. Protocols for administration of intravenous contrast must be reviewed by the Drug Information Center and approved by the P&T Subcommittee and by the appropriate radiologist or radiologists when the standards of care and application change or when the characteristics of the intravenous contrast change.
4. An LIP reviews all requests for radiology procedures with intravenous contrast to determine the appropriate protocol based on the clinical indications for the examination. Assigned protocol is indicated on the modality protocol sheet or the radiology requisition.
5. A radiologic technologist or radiology nurse will review patient’s current medications and clinical conditions for contraindications related to intravenous contrast administration.
6. If contraindications are identified, the supervising LIP will be contacted to determine appropriate IV contrast use.
7. Type of contrast and dose information is recorded in IPR on the Contrast Administration form by the nurse or technologist.
8. Contrast doses that are prepared and NOT immediately administered to patient must be labeled with:
a. Drug name, strength and amount (if not apparent from container) b. Expiration date when not used within 24 hours
c. Name of patient, medical record number, date of birth and location of the patient, if contrast dose is prepared based upon specific patient information.
Procedure: 1.Pre-administration Checks (4 Hs) The ACR manual describes the 4 Hs (history, hydration, have equipment and expertise ready, heads up). These checks have an effect on both the need for premedication, the risk of contrast extravasation, and the need for laboratory testing. 2.Renal failure-related Issues with iodinated contrast Significant contrast media induced nephrotoxicity may be defined as a >25% rise in serum creatinine from baseline (if < 1.5 mg/dl) or an absolute elevation of >1.0 mg/dl from baseline (if > 1.5 mg/dl) within 72 hours following administration. Risk factors for contrast induced renal failure include:
Pre-existing renal insufficiency Diabetes mellitus Dehydration Cardiovascular disease and use of diuretics Age > 70 years Myeloma Uncontrolled Hypertension Hyperuricemia (gout)
Indications for serum creatinine measurement before intravascular administration of iodinated contrast media include:
History of “kidney disease” as an adult, including tumor and transplant Family history of kidney failure Diabetes treated with insulin or other prescribed medications Paraproteinemia syndromes/diseases (e.g. myeloma) Collagen vascular diseases
Use of potentially nephrotoxic medications can increase the risk of iodinated contrast-induced renal failure. Drugs that may increase the risk include:
metformin NSAIDs including COX-2 selective agents (e.g. ibuprofen, naproxen,
ketorolac, fenoprofen, indomethacin, celecoxib, valdecoxib, etc.) nephrotoxic antimicrobials (gentamicin, tobramycin, amikacin,
amphotericin B, cidofovir). 3. Measures to Prevention/Ameliorate Nephrotoxicity
a. Hydration if required. Normally, this can be achieved by oral administration of 1-2 liters of fluids extra in the 24 hours prior to contrast injection. In some cases, this can

be achieved using 0.45% or 0.9% saline, 100ml/hr from 12 hours before until 12 hours after angiography b. Withhold furosemide c. Withhold metformin for 48 hours after the procedure and reinstitute only after renal function had been re-evaluated and determined to be normal. d. In patients with risk factors for contrast-induced renal failure (see #2 above), administer acetylcysteine, 600 mg by mouth twice daily on the day before and on the day of contrast administration (4 total doses). e. In patients who present acutely and who have an indication for acetylcysteine, patients with an ileus or non-intact GI tract, or patients who are unable to swallow and have no NG tube, two options are allowed:
1) No contrast is administered; this is the preferred option for patients who present acutely) 2) In life-threatening situations where a contrast-enhanced CT is required immediately (e.g., suspected pulmonary embolism, suspected aortic dissection, suspected aortic rupture, immediate requirement for vascular intervention), and where a 24-hour delay is unacceptable based on clinical grounds, one can consider administration of IVacetylcysteine (Acetadote® 150 mg/kg over 30 minutes immediately prior contrast administration, following by 50 mg/kg over 4 hours after). If IV acetylcysteine is administered (>$100/vial), one has to be prepared for anaphylactic reactions and the epinephrine should be readily available for injection: Epinephrine 1:1000 0.3 ml i.m. AND diphenhydramine (Benadryl) 50 mg IV.
4. Premedication Severe life-threatening reactions are relatively rare. Although overall adverse reactions are decreased following steroid premedication, the incidence of severe life-threatening adverse events has not been affected. The following regimes are suggested:
a. Planned contrast administration in patients with previous documented/suspected reaction:
Prednisone 40 mg by mouth at 12 hours and 2 hours prior to contrast injection
b. (Semi-) acute investigations in patients with previous documented/suspected reaction:
Hydrocortisone 200 mg IV 1 hour prior and 3 hours post contrast injection AND Diphenhydramine (Benadryl) 50 mg IV 1 hour prior to contrast administration AND Famotidine 20mg by mouth 1 hour prior to contrast administration IN THESE CIRCUMSTANCES PATIENTS ARE ADVISED NOT TO DRIVE.
5. Specific screening for administration of intravenous gadolinium-based contrast agents. There are possible serious side effects for patients receiving gadolinium-based contrasts who have impaired renal function. This population of patients are at risk for developing nephrogenic fibrosing dermopathy/nephrogenic systemic fibrosis (NFD/NFS). The following patients should have serum creatinine with GFR assessed prior to injection:
Patients > 65 years of age Patients with a history of renal insufficiency Patients with a history of diabetes
6.Methods to Decrease the Risk of Extravasation during Injection of Contrast Media Most CT protocols use power injectors. In angiography/intervention there is a mix of power and hand injections. There is preference for 20-G or larger catheters/cannulas with flow rates of 3 ml/second or higher. Patients should be instructed about potential extravasation and how to alert the technician. All injections should be monitored during the first 10-15 seconds of injection to ensure no extravasation occurs early. Communication with the patient should continue via intercom during injection. Use of central venous catheters should be discouraged, although some larger bore catheters may be used in exceptional circumstances. Several risk factors that have been identified for contrast extravasation include:
Inadequate communication (elderly, altered consciousness) Severely ill/debilitated patients Patients with abnormal circulation to limb to be injected (atherosclerosis,
Raynaud‘s disease, venous thrombosis/insufficiency, prior radiation therapy, previous [axillary] surgery)
More peripheral injection sites (hand, wrist, foot, ankle) Injection through line that has been present >24 hrs
6.Treatment of Contrast Extravasation Extravasations have incidence of 1/1000 to 1/106 patients when a power injector is used. Observation is required if extravasation <50 ml high osmolar or <100 low osmolar contrast media:
notify radiologist elevate affected limb apply ice packs intermittently if > 5 ml extravasated: observation for 2-4 hours
Surgical (plastic surgery) consultation is required in the following situations:
extravasation >50 ml high osmolar of >100 low osmolar contrast media increased swelling or pain after 2-4 hours altered tissue perfusion change in sensation or temperature
development of skin ulceration or blistering 7. Treatment of contrast media reaction Treatment is dependent on the extent and type of reaction (See Table 1). ALL reactions should be reported through standard reporting procedures. General treatment measures include:
maintain i.v. access observe vital functions (ABC) alert radiologist
Approved: __________________________________ _______________________ Laurie Fajardo, MD Date Chair Department of Radiology __________________________________ ________________________ Janet Roe Date Reviewed by Department of Pharmaceutical Care (March 2007) Reviewed by Department of Anesthesiology (April 2005) Approved by the Pharmacy and Therapeutics Subcommittee (March 2007) Approved by Radiology Quality Assurance Committee (June 2005)
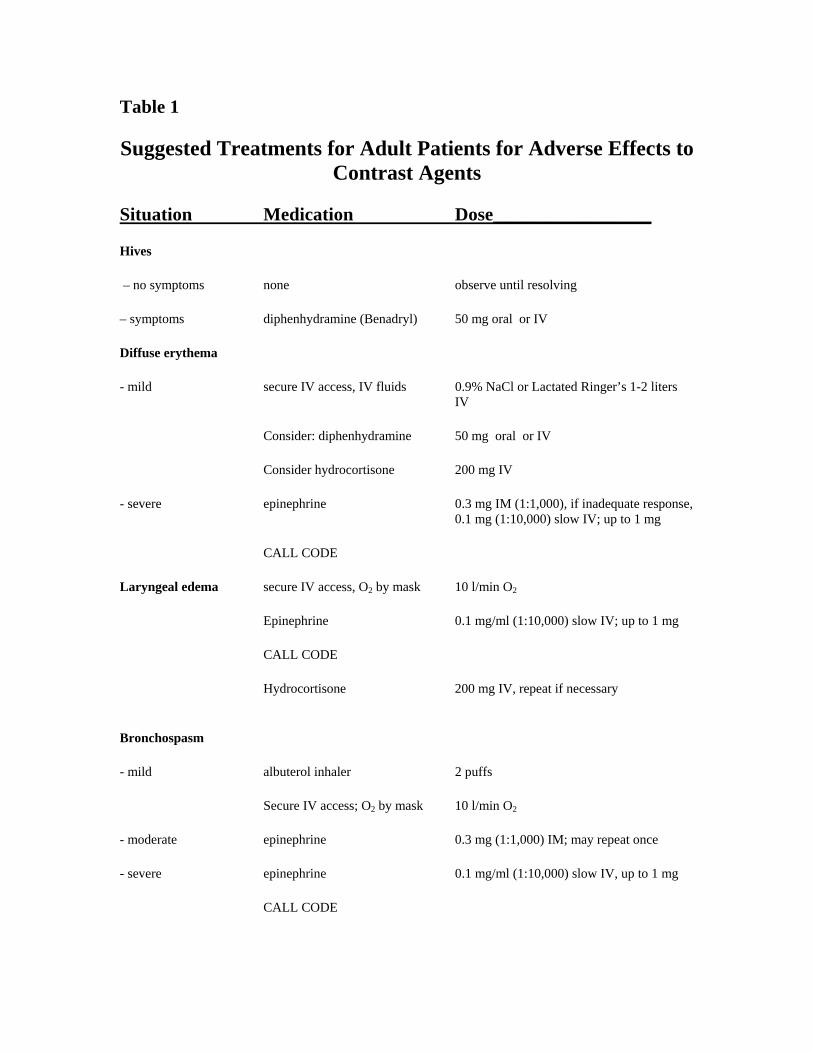
Table 1
Suggested Treatments for Adult Patients for Adverse Effects to Contrast Agents
Situation Medication Dose_________________
Hives
– no symptoms none observe until resolving
– symptoms diphenhydramine (Benadryl) 50 mg oral or IV
Diffuse erythema
- mild secure IV access, IV fluids 0.9% NaCl or Lactated Ringer’s 1-2 liters IV
Consider: diphenhydramine 50 mg oral or IV
Consider hydrocortisone 200 mg IV
- severe epinephrine 0.3 mg IM (1:1,000), if inadequate response, 0.1 mg (1:10,000) slow IV; up to 1 mg
CALL CODE
Laryngeal edema secure IV access, O2 by mask 10 l/min O2
Epinephrine 0.1 mg/ml (1:10,000) slow IV; up to 1 mg
CALL CODE
Hydrocortisone 200 mg IV, repeat if necessary
Bronchospasm
- mild albuterol inhaler 2 puffs
Secure IV access; O2 by mask 10 l/min O2
- moderate epinephrine 0.3 mg (1:1,000) IM; may repeat once
- severe epinephrine 0.1 mg/ml (1:10,000) slow IV, up to 1 mg
CALL CODE

Pulmonary Edema secure IV access; O2 by mask 10 l/min O2
Elevate head of bed
Furosemide 10-40 mg IV, slowly
Morphine 1-3 mg IV, repeat every 5-10 min as needed
Hydrocortisone 200 mg IV
CALL CODE
Hypotension with Bradycardia
- mild elevate legs, secure iv access
IV fluids 0.9% NaCl or Lactated Ringer’s 1-2 liters
O2 by mask 10 l/min O2
- severe atropine 0.6 mg – 1 mg IV, slow; up to 3 mg
Hypotension with Tachycardia
- mild elevate legs, secure IV access
IV fluids 0.9% NaCl or Lactated Ringer’s 1-2 liters
O2 by mask 10 l/min O2
- severe Epinephrine 0.1 mg/ml (1:10,000) slow IV; up to 1 mg
CALL CODE
Hypertension Crisis (diastolic BP > 120 mmHg)
Secure IV. access
O2 by mask 10 l/min O2
Furosemide 40 mg IV slowly
Nitroglycerin 0.4 mg sublingual; repeat after 5-10 min.
Suspected Pheochromocytoma
Phentolamine 5 mg/50 ml IV push
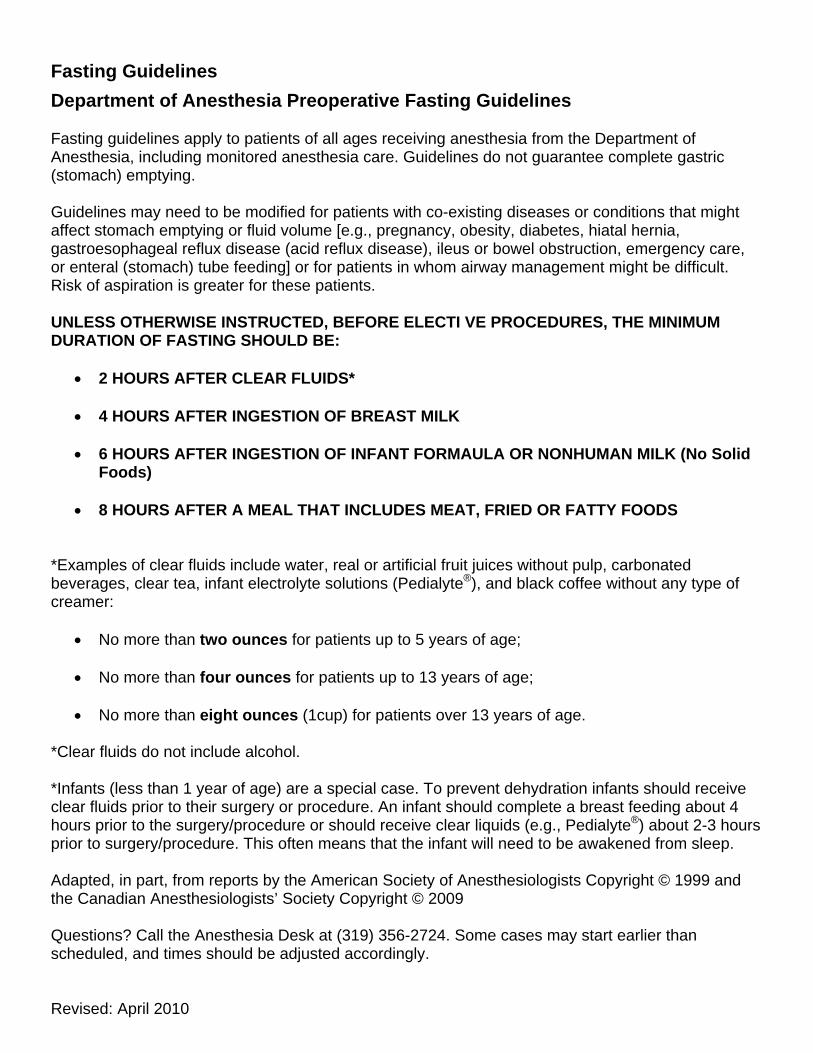
Fasting Guidelines
Department of Anesthesia Preoperative Fasting Guidelines
Fasting guidelines apply to patients of all ages receiving anesthesia from the Department of Anesthesia, including monitored anesthesia care. Guidelines do not guarantee complete gastric (stomach) emptying. Guidelines may need to be modified for patients with co-existing diseases or conditions that might affect stomach emptying or fluid volume [e.g., pregnancy, obesity, diabetes, hiatal hernia, gastroesophageal reflux disease (acid reflux disease), ileus or bowel obstruction, emergency care, or enteral (stomach) tube feeding] or for patients in whom airway management might be difficult. Risk of aspiration is greater for these patients. UNLESS OTHERWISE INSTRUCTED, BEFORE ELECTI VE PROCEDURES, THE MINIMUM DURATION OF FASTING SHOULD BE:
2 HOURS AFTER CLEAR FLUIDS*
4 HOURS AFTER INGESTION OF BREAST MILK
6 HOURS AFTER INGESTION OF INFANT FORMAULA OR NONHUMAN MILK (No Solid Foods)
8 HOURS AFTER A MEAL THAT INCLUDES MEAT, FRIED OR FATTY FOODS
*Examples of clear fluids include water, real or artificial fruit juices without pulp, carbonated beverages, clear tea, infant electrolyte solutions (Pedialyte®), and black coffee without any type of creamer:
No more than two ounces for patients up to 5 years of age;
No more than four ounces for patients up to 13 years of age;
No more than eight ounces (1cup) for patients over 13 years of age.
*Clear fluids do not include alcohol. *Infants (less than 1 year of age) are a special case. To prevent dehydration infants should receive clear fluids prior to their surgery or procedure. An infant should complete a breast feeding about 4 hours prior to the surgery/procedure or should receive clear liquids (e.g., Pedialyte®) about 2-3 hours prior to surgery/procedure. This often means that the infant will need to be awakened from sleep. Adapted, in part, from reports by the American Society of Anesthesiologists Copyright © 1999 and the Canadian Anesthesiologists’ Society Copyright © 2009 Questions? Call the Anesthesia Desk at (319) 356-2724. Some cases may start earlier than scheduled, and times should be adjusted accordingly. Revised: April 2010
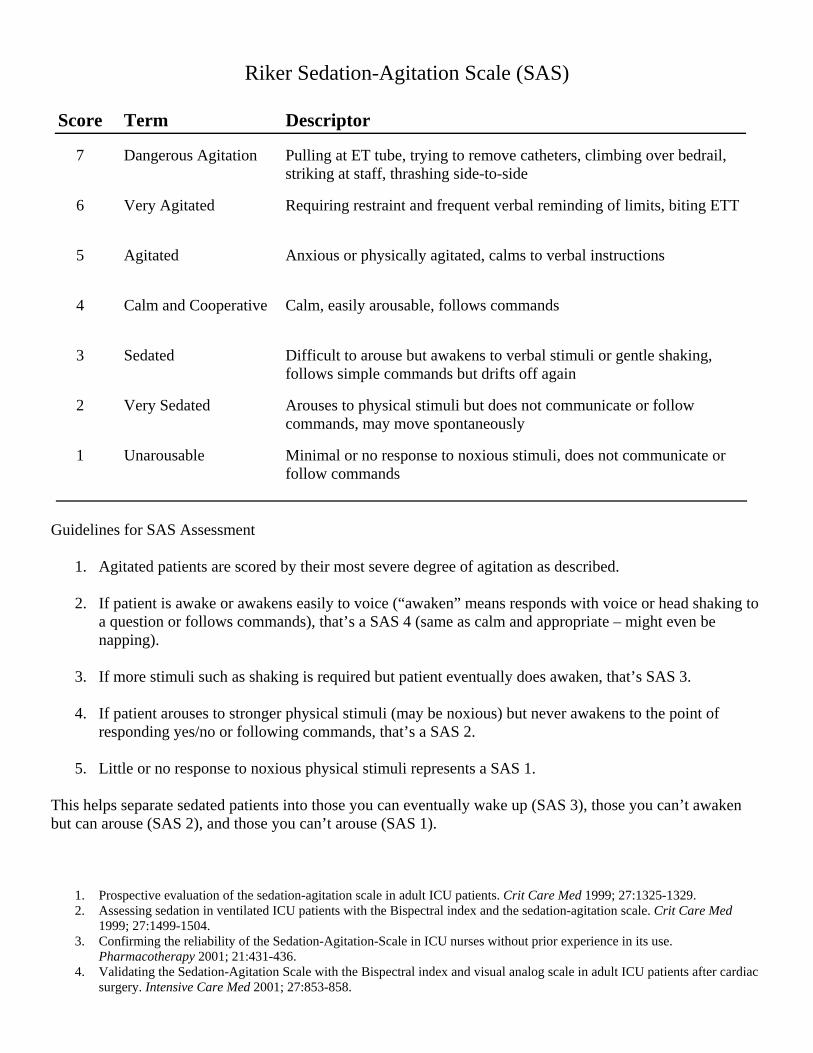
Riker Sedation-Agitation Scale (SAS)
Score Term Descriptor
7 Dangerous Agitation Pulling at ET tube, trying to remove catheters, climbing over bedrail, striking at staff, thrashing side-to-side
6 Very Agitated Requiring restraint and frequent verbal reminding of limits, biting ETT
5 Agitated Anxious or physically agitated, calms to verbal instructions
4 Calm and Cooperative Calm, easily arousable, follows commands
3 Sedated Difficult to arouse but awakens to verbal stimuli or gentle shaking, follows simple commands but drifts off again
2 Very Sedated Arouses to physical stimuli but does not communicate or follow commands, may move spontaneously
1 Unarousable Minimal or no response to noxious stimuli, does not communicate or follow commands
Guidelines for SAS Assessment
1. Agitated patients are scored by their most severe degree of agitation as described.
2. If patient is awake or awakens easily to voice (“awaken” means responds with voice or head shaking to a question or follows commands), that’s a SAS 4 (same as calm and appropriate – might even be napping).
3. If more stimuli such as shaking is required but patient eventually does awaken, that’s SAS 3.
4. If patient arouses to stronger physical stimuli (may be noxious) but never awakens to the point of responding yes/no or following commands, that’s a SAS 2.
5. Little or no response to noxious physical stimuli represents a SAS 1.
This helps separate sedated patients into those you can eventually wake up (SAS 3), those you can’t awaken but can arouse (SAS 2), and those you can’t arouse (SAS 1).
1. Prospective evaluation of the sedation-agitation scale in adult ICU patients. Crit Care Med 1999; 27:1325-1329. 2. Assessing sedation in ventilated ICU patients with the Bispectral index and the sedation-agitation scale. Crit Care Med
1999; 27:1499-1504. 3. Confirming the reliability of the Sedation-Agitation-Scale in ICU nurses without prior experience in its use.
Pharmacotherapy 2001; 21:431-436. 4. Validating the Sedation-Agitation Scale with the Bispectral index and visual analog scale in adult ICU patients after cardiac
surgery. Intensive Care Med 2001; 27:853-858.

University of Iowa Procedural Sedation Mon Tues Wed Thurs Fri
INTERVIEW COMPLETED______________________ PROCEDURE DATE_______________________ (DATE)
RN INITIALS_____ TIMES: PST____________ PROCEDURE____________________________________________ Remind parents to bring diaper, extra clothes, etc. PRE-INTERVIEW CALL SHEET WEIGHT _________kg ALLERGIES________________ NKA PATIENT NAME: ________________________________ AGE: ____ Years Months RECORD #____________
CONTACT NAME: _______________________________________ RELATIONSHIP__________________
CONTACT #______________________________ (HOME, CELL) CITY_____________________________
#______________________________ (HOME, CELL) COUNTY__________________________
PROCEDURE_____________________________________________________________________________
REASON FOR PROCEDURE________________________________________________________________
DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
POST-PROCEDURAL SEDATION PHONE CALL ASSESSMENT Date of procedure___________________________ Meds used_________________________________________________________ IV PO DID THE PATIENT HAVE ANY OF THE FOLLOWING PROBLEMS? (CHECK WHAT IS RELEVANT) NAUSEA: _________________________ VOMITING: __________________________ HYPERACTIVITY: _________________ IRRITABILITY: _______________________ SOMNOLENCE: ____________________ IV SITE PROBLEMS: ___________________ UNPLANNED ADMISSION: __________ OTHER: _________________________________________________________________________________ COMMENTS: (Include any comments made by the informant - (use actual patient quotes) ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ WAS THE PATIENT/INFORMANT SATISFIED WITH THE EXPERIENCE? – ON A SCALE OF 1 (worst) to 5 (best) (CIRCLE ONE) 1 2 3 4 5 DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
DATE/TIME CALLED_________________ UNABLE TO CONTACT NO MESSAGE LEFT NO ANSWER MACHINE MESSAGE LEFT TO: RETURN CALL OTHER _____________________________________________________________________ Initials__________
Procedural Sedation Pre-Interview PROCEDURE Procedure Name and Description: _______________________________________________________ Reason for Procedure: _________________________________________________________________ PRESEDATION PATIENT INFORMATION ASSESSMENT Confirmed With: _____________________________________________________________________ Procedure Date:__________________________________________________________________ Time of Procedure:_____________________________________ Arrival Time: __________________________________________ Patient’s Dominate Language: English Spanish Bosnian Korean Japanese Chinese Sign Language Fasting Guidelines: Patient/Family advised not to eat 8 hours prior or to give infant formula/non-human milk 6 hours prior or to give breast milk to 4 hours prior to procedure time. Patient/Family advised to follow Digestive Disease Clinic May Give Clear Liquids: 2 (0-5y) 4 (5-13y) 8 (>13y) ounces 2 hours prior to procedure. Name of Responsible Adult to Accompany Patient for Discharge: ______________________________ Prosthetic Appliances or Impairments: None, Glasses, Contacts, Hearing Aid, Dental, Metal Implants, Blindness, Deafness, Walker, Cane Patient Sexually Active: Yes No N/A Pregnant: Yes No N/A Last Menses Date: Weight:____________________ kg / lbs. Height:____________________ cm / inches Daily Functional Activity Adult: Light Intensity Activities: Walking slowly, Golf (powered cart), Swimming (slow treading), Gardening or pruning, Bicycling (very light effort), Dusting or vacuuming and Conditioning exercise (light stretching or warm-up) Moderate Intensity Activities: Walking briskly, Golf (pulling or carrying clubs), Swimming (recreational), Mowing lawn (power mower), Tennis (doubles), Bicycling 5-9 mph (level terrain or few hills), Scrubbing floors or washing windows, Weight lifting, Nautilus machines or free weights, Climbs 1 flight of stairs without stopping Vigorous Intensity Activities: Race walking, jogging or running, swimming laps, mowing lawn (hand rotary mower), tennis singles, bicycling more than 10 mph or up steep terrain, moving or pushing furniture and circuit training. Daily Functional Activity Child/Infant: -Tolerates Normal Infant Activities -Tolerates Normal Toddler Activities -Tolerates Normal Pre-School Activities -Tolerates Normal School Activities -Unable to Complete Normal Daily Activities
Patient premature: Not Applicable if > 1yr. age Yes No Post-Conception Age:_________ weeks Birth History Normal Vaginal Delivery C-Section RELEVANT HISTORY AND PREVIOUS EVALUATIONS Smoking History: Not applicable Currently smokes or uses smokeless tobacco____________ per day (p=pack, c=cans), years Alcohol Use: Not Applicable Yes: Drinks _________________(d=day, w=week, m=month) Illicit Drug Use: (Pt. to young or Incapacitated) Yes No Pt. Denies Any Illicit Drug Usage, Marijuana, Cocaine/Crack, Heroin, Methamphetamine, Non-Prescribed Prescription Medications Prior Surgeries: None ______________________________________________________ Anesthetic History: _______________________________________Malig. Hyperther. Yes No ALLERGIES: Yes NKDA Medication(s):___________________________________________________________________ LATEX: Yes No Comment:_____________________________________________________ MEDICATION LIST
SYSTEMS REVIEW Skin: Patient Denies Dermatitis, Birthmarks, Bruises, Scars, Hemangiomas, Vascular/Lymphatic Malformations or Abrasions. HEENT: Patient Denies Epistaxis, Otitis, Fever, Sore Throat, Loose Teeth, Braces, Deaf, Dysphagia, Apnea, Vision, Hoarseness, Nasal, Obstruction, Neck ROM/Pain. Pulmonary: Patient Denies Asthma, Sleep Apnea, Snores, Stridor, SOB, Cough, Recent URI, Wheezing, Edema, Bronchitis, Pneumonia, Croup, Aspiration, Tracheostomy, TB, RSV, Steroid Use, Cystic Fibrosis Cardiac: Patient Denies Angina, Arrhythmias, Congenital Defects, Heart Murmur, Valvular Disease/Prosthesis, Pacemaker, Dyspnea on Exertion, CHF Symptoms, Palpitations, Hypertension, Hypotension, Syncope. Musculoskeletal: Patient Denies Muscle Disease, Scoliosis, Myopathy, Fractures, Contractures, Gait, Neck, Deformities, Prosthesis, Kyphosis, Crutches, Wheelchair Bound, Rheumatoid Arthritis. Neurologic: Patient Denies Seizures, Weakness/Paresis/Gait, Asymmetry, Hydrocephalus, Myelodysplasia, Sacral Deformity/Neck Abnormalities, Hypotonia, Shunt. Gastrointestinal: Patient Denies GE Reflux, Diarrhea, Constipation, Nausea, Vomiting, Diversion, Abdominal Pain, Esophageal Varices, Enteral Feeding, Eating Disorder, Crohn’s, Poor Oral Intake. Genitourinary: Patient Denies Kidney Disease, UTI, Incontinence, Diversions, Clean Intermittent Catheterization, Dialysis, Reflux. Hepatic: Patient Denies Jaundice, Hepatitis, Increased Liver Function Tests. Hematologic: Patient Denies Sickle Cell Disease, G6PD Deficiency, Thalassemia, Blood Dyscrasia. HIV. Endocrine/Metabolic: Patient Denies Diabetes. Thyroid Disease, Congenital Adrenal Hyperplasia, Inborn Errors of Metabolism, Immune Deficiency. Syndromes: None Downs, Pierre-Robbin, Treacher-Collins, Goldenhars, Psycho/Social: Patient Denies Depression. Anxiety, Phobias, Psychosis, Developmental Delays, ADHD, Learning Disability, Aggressive Behavior, Autism, Communication Devices. Other Pertinent Patient History: _________________________________________________________ ____________________________________________________________________________________________________________________________________________________________________________ Pain: Patient indicates they do not have any pain Chronic Acute Intermittent Unable to Determine Pain: Pain Location: ________________________________________ Pain Scale (1=least. 10=worst):_________