sdo - inf cntrl
TRANSCRIPT

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 1/105
Infection Control in Dental
Health-Care Settings

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 2/105
Sets ³Guidelines for Infection Control in Dental Health-Care
Settings-Core´
Provide an overview of many of the basic principles of
infection control

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 3/105
Infection Control in DentalHealth-Care Settings: An Overview
Background
Personnel Health Elements
Blood borne Pathogens
Hand Hygiene Personal Protective Equipment
Sterilization and Disinfection
Environmental Infection Control
Dental Unit Waterlines
Special Considerations
Program Evaluation

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 4/105
B ACKGROUND
� 1918-1919 - People died more of infections than byaction in war
� 1936 - Penicillin
� 1950 - Eradiation of polio
� 1978 - Eradiation of small pox
� 1981 - Vaccine against HBV
� 1983 - HIV
DHCW -13%-25 %
General population± 5%
Thus, risk for unvaccinated member of dental team ± 2to 5 times more

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 5/105
1978-First ADA Infection Control Guideline
1981- CDC first reports on AIDS infections
1986 ± CDC Recommended Infection Control Practices
1987- CDC Universal Precautions Guidelines
1987 ± OSHA: Protection against occupational exposure to HBV and
HIV
1993 ± CDC - Infection Control practices for Dentistry
2003 ± CDC Guidelines for Infection Control in Dental
Settings
B ACKGROUND

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 6/105
Recommendations
� Improve effectiveness and impact of
public health interventions
� Inform clinicians, public health
practitioners, and the public
� Based on a range of rationale, from
systematic reviews to expert opinions

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 7/105
Why Is Infection Control Important
in Dentistry?� Both patients and dental health care
personnel (DHCP) can be exposed to
pathogens
� Contact with blood, oral and respiratory
secretions, and contaminated equipment
occurs� Proper procedures can prevent
transmission of infections among patients
and DHCP

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 8/105
Modes of Transmission
� Direct contact with blood or body fluids
� Indirect contact with a contaminatedinstrument or surface
� Contact of mucosa of the eyes, nose, or mouth with droplets or spatter
� Inhalation of airborne micro-organisms

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 9/105
Chain of InfectionChain of Infection
Pathogen
Source
ModeEntry
Susceptible Host
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 10/105
Standard Precautions
� Apply to all patients
� Integrate and expand UniversalPrecautions to include organismsspread by blood and also
±Body fluids, secretions, and excretions
except sweat, whether or not they containblood
±Non-intact (broken) skin
±Mucous membranes

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 11/105
Elements of StandardPrecautions
� Hand washing
� Use of gloves, masks, eye
protection and gowns� Patient care equipment
� Environmental surfaces
� Injury prevention

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 12/105
Personnel Health Elements of an
Infection Control Program
� Education and training
� Immunizations
� Exposure prevention and postexposuremanagement
� Medical condition management and work-
related illnesses and restrictions� Health record maintenance

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 13/105
Bloodborne Pathogens
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 14/105
Preventing Transmission of
Bloodborne Pathogens
� Are transmissible in health care
settings
� Can produce chronic infection� Are often carried by persons unaware
of their infection
Bloodborne viruses such as hepatitis B virus
(HBV), hepatitis C virus (HCV), and human
immunodeficiency virus (HIV)
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 15/105
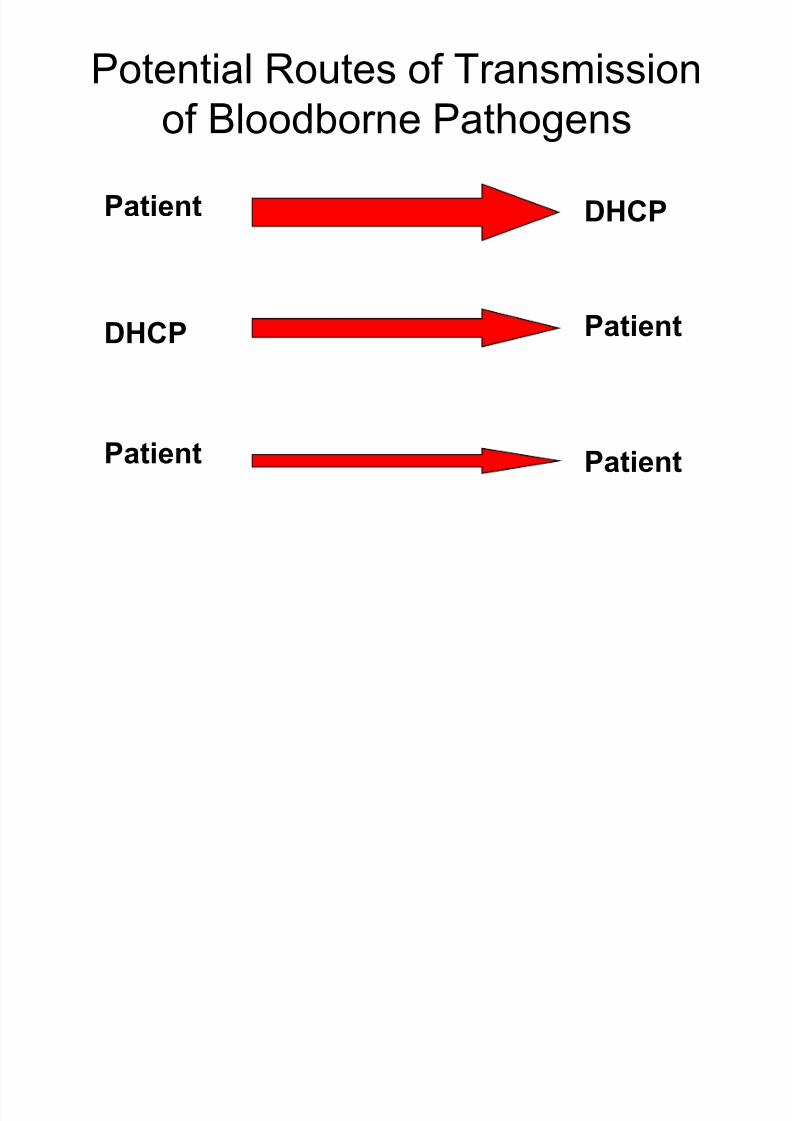
Potential Routes of Transmission
of B
loodborne PathogensPatient DHCP
DHCP Patient
Patient Patient

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 16/105
Contaminated instruments
Blood
Airborne infections
Inhalation route
Contact with splatter

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 17/105
Factors Influencing OccupationalRisk of Blood borne Virus Infection
� Frequency of infection among
patients
� Risk of transmission after a blood
exposure (i.e., type of virus)
� Type and frequency of bloodcontact

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 18/105
Average Risk of Bloodborne Virus
Transmission after NeedlestickSource Risk
HBV
HBsAg+ and
HBeAg+
22.0%-31.0% clinical hepatitis;37%-62% serological evidence
of HBV infection
HBsAg+ and
HBeAg-
1.0%-6.0% clinical hepatitis;
23%-37% serological
evidence of HBV infection
HCV 1.8% (0%-7% range)
HIV 0.3% (0.2%-0.5% range)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 19/105
Concentration of HBV in Body
Fluids
High Moderate Low/Not
Detectable
Blood Semen Urine
Serum Vaginal Fluid Feces
Wound exudates Saliva Sweat
TearsBreast Milk

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 20/105

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 21/105
Hepatitis B Vaccine
Vaccinate all DHCP who are at risk of
exposure to blood
Provide access to qualified health care
professionals for administration and
follow-up testing
Test for anti-HBs 1 to 2 months after 3rd dose

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 22/105
HEPATITIS B
Incubation period 2-6 monthsTransmission route parenteral, percutaneous or mucosal
Clinically ± 66% HBV cases are asymptomatic
- 1% Fulminant Hepatitis
- 33% symptomatic
If Serological markers persists for over 6 months hebecomes a chronic carrier
Treatment: Interferon-3 million units 3 times for 1 weeksuccess rate 30-40%
Vaccine
-Plasma derived vaccine
-Recombinant yeast vaccine

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 23/105
Unvaccinated HBIG X 1 dose Initiate HBV Initiate HBV
(1000-2000 IU I/M ± Adult) vaccine series vaccine series
( 32 ± 48 IU / Kg body wt ± Child)
initiate vaccine series
Vaccine status Antibody response status
Of exposed HCW __________________________________________________________________________________
Source HBsAg +ve Source HBsAg +ve Source unknown /unavailable for test
Previously vaccinated
Known responder No Rx No Rx No Rx
Known non-responder HBIG X 1 dose
initiate re-vac or HBIG X 2 doses
Antibody response Test exposed HCW for anti HBs No Rx Consider re-vac if
Unknown If adequate --- no Rx required known high risk
If inadequate ----- Adm. HBIG X 1 source ( Rx as HbsAg +ve )
and vaccine booster. Test for HBsAg

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 24/105
HCV Infection in
Dental Health Care Settings
� Prevalence of HCV infection
among dentists similar to that of
general population (~ 1%-2%)� No reports of HCV transmission
from infected DHCP to patients or
from patient to patient� Risk of HCV transmission appears
very low

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 25/105
Transmission of HIV from
Infected Dentists to Patients
� Only one documented case of HIV
transmission from an infected
dentist to patients
� No transmissions documented in
the investigation of 63 HIV-infected
HCP (including 33 dentists or
dental students)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 26/105
Health Care Workers with Documented andPossible Occupationally Acquired HIV/AIDS
CDC Database as of December 2009
* 3 dentists, 1 OMF Surgeon, 2 dental assistants
Documented Possible
Dental Worker 0 6 *
Nurse 24 35
Lab Tech, clinical 16 17
Physician, nonsurgical 6 12
Lab Tech, nonclinical 3 ±
Other 8 69Total 57 139

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 27/105
Seropositivity per 1000
106.83 Maharashtra
177.7 Manipur
50.19 Nagaland
43.7 Punjab
34.2 Pondicherry
15.53 Tamil Nadu
HIV

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 28/105
Risk Factors for HIV Transmission after Percutaneous Exposure to HIV-Infected Blood
� Deep injury
�
Visible blood on device� Needle placed in artery or vein
� Terminal illness in source patient
Source: Cardo, et al., N England J Medicine 1997;337:1485-90.

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 29/105
M ANAGEMENT OF EXPOSURES
TO HIV
� REPORTING OF EXPOSURES ±
a) Date and time of exposure
b) Details of procedure performedc) How the exposure occurred
d) Details of exposure, depth of wound and amount of
blood/fluid in contact
e) Details of exposure source- whether HIV or other bloodborne pathogens

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 30/105
Post Exposure Prophylaxis (PEP)
� Needle-stick injuries & cuts: immersed wash withsoap & water
� Splashes to nose, mouth or skin: flush with plentyof clean water
� Splash/injury to eye: irrigate with water / saline� Do not put injured finger into mouth
� Blood tests(3-5ml) for both immediately ,at 6weeks, 12 weeks and 6 months for HIV,HCV &
HBV� Report immediately to your immediate senior/to authorised medical attendant: it is anemergency!

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 31/105
M ANAGEMENT OF EXPOSURES
TO HIV� SHOULD BE TESTED FOR HIV ANTIBODY TO
ESTABLISH SERO STATUS BEFORE EXPOSURE
� FOLLOW UP TESTING DONE AT 6 ± 12 WEEKS AND
END OF 6 MONTHS TO DETERMINE WHETHER
INFECTION HAS OCCURRED
� B ASED ON RESULTS PEP ADVISED

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 32/105
Determining Exposure Code (EC) of an Injury NACO GUIDELINES
Determining Exposure Code
Is source material / blood / body fluid / instrument soiled by above ?
YES NO No PEP
What Kind of Exposure ?
MM or skin integrity
compromised
Intact skin only Percutaneous exposure ?
VOL ?No PEP
SEVERITY
Few drops,
Short time
Many drops,
Splash, several minutes
Less severe,
Solid needle
More severe,
EC 1 EC 2 EC 2 EC 3

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 33/105
Determining HIV Status Code (SC) of Source NACO GUIDELINES
HIV - ve HIV + ve Status Unknown Source Unknown
No PEP
Low Titer exposure :
Asymptomatic,
Normal CD4
High Titer exposure :
Advanced AIDS,
Low CD4,
High viral load
HIV SC 1 HIV SC 2 HIV SC Unknown
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 34/105
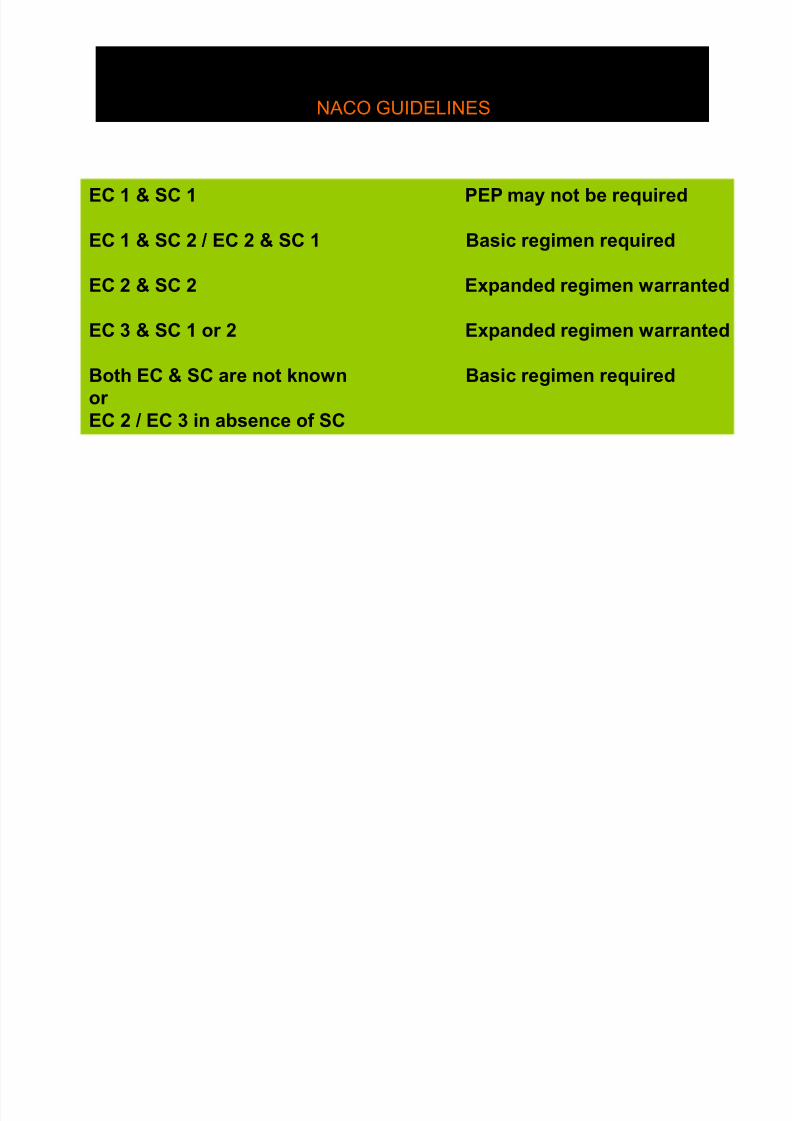
RECOMMENDATION OF PEP REGIMENS B ASED ON
EXPOSURE & STATUS OF SOURCE
NACO GUIDELINES
EC 1 & SC 1 PEP may not be required
EC 1 & SC 2 / EC 2 & SC 1 Basic regimen required
EC 2 & SC 2 Expanded regimen warranted
EC 3 & SC 1 or 2 Expanded regimen warranted
Both EC & SC are not known Basic regimen required
or
EC 2 / EC 3 in absence of SC

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 35/105
Regimens for PEP for HIV
� Basic regimen: Zidovudine(Retrovir, Zidovir, AZT, ZDV) 600mg / day in divided doses
Lamivudine (3TC, Epivir) 150 mgBD X 28 days

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 36/105
Regimens for PEP for HIV
� Expanded regimen: Zidovudine 600 mg/dayin divided doses
Lamivudine 150 mg BD X 28 days +
(Indinavir 800 mg TDS X 28 days
/ Nelfinavir 750 mg TDS X 28 days)
� Side effects of PEP: nausea, vomiting,diarrhoea, fatigue

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 37/105
Risk of HIV,HBV and HCV after
percutaneous exposure
� HIV: 0.3%
� For HCV: approx 3%� For HBV: upto 30% in unvaccinated
individuals (concentration of HBV in
blood may be >10,000,000 infectiousparticles /ml as against 10-100 inf
particles / ml in HIV)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 38/105
In the event of an exposure:
further advice to HCW
� HCW counseled to report again at intervals of 6 weeks, 12 weeks and 6 months for : Ab to
HIV, anti HCV and HB
sAg� Not to donate blood /internal organ/ semen
� To abstain from sexual intercourse/ usecondom persistently during entire observation
period� In pregnancy: PEP safe after first trimester
� If a lady, to avoid pregnancy duringobservation period & if lactating not to breast-
feed child during observation period

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 39/105
Exposure PreventionStrategies

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 40/105
Engineering Controls
� Isolate or remove the hazard
� Examples:
±Sharps container
±Medical devices with injury
protection features (e.g., self-
sheathing needles)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 41/105
Work Practice Controls
Change the manner of performing
tasks
Examples include:� Using instruments instead of fingers
to retract or palpate tissue
� One-handed needle recapping

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 42/105
Administrative Controls
� Policies, procedures, and
enforcement measures
� Placement in the hierarchy variesby the problem being addressed
±Placed before engineering controls
for airborne precautions (e.g., TB)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 43/105
� Wound management
� Exposure reporting
� Assessment of infection risk ±Type and severity of exposure
±Bloodborne status of sourceperson
±Susceptibility of exposed person
Post-exposure Management

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 44/105
Hand Hygiene
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 45/105
Why Is Hand Hygiene Important?
� Hands are the most common
mode of pathogen transmission
� Reduce spread of antimicrobial
resistance
� Prevent health care-associated
infections

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 46/105
Hands Need to be Cleaned
when««««««.
� Visibly dirty
� After touching
contaminated objectswith bare hands
� Before and after patient
treatment (before glove
placement and after
glove removal)

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 47/105
Hand Hygiene Definitions
� Handwashing ±Washing hands with plain soap and water
� Antiseptic handwash ±Washing hands with water and soap or other
detergents containing an antiseptic agent
� Alcohol-based handrub ± Rubbing hands with an alcohol-containing
preparation
� Surgical antisepsis ± Handwashing with an antiseptic soap or an
alcohol-based handrub before operations by
surgical personnel

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 48/105
Efficacy of Hand HygienePreparations in Reduction of
Bacteria
Good Better Best
Plain Soap Antimicrobialsoap
Alcohol-basedhandrub
Source: http://www.cdc.gov/handhygiene/materials.htm

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 49/105
Alcohol-based Preparations
� Rapid and
effective
antimicrobialaction
� Improved skin
condition
� More accessible
than sinks
� Cannot be used if
hands are visibly
soiled� Store away from
high temperatures
or flames
� Hand softeners
and glove powders
may ³build-up´
Benefits Limitations
S i l H d H i
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 50/105
Special Hand Hygiene
Considerations
� Use hand lotions to prevent skindryness
� Consider compatibility of hand careproducts with gloves (e.g., mineral oilsand petroleum bases may cause earlyglove failure)
� Keep fingernails short� Avoid artificial nails
� Avoid hand jewelry that may tear gloves

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 51/105
Personal Protective
Equipment

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 52/105
Personal
ProtectiveEquipment
� A major component of StandardPrecautions
� Protects the skin and mucous
membranes from exposure to infectious
materials in spray or spatter
� Should be removed when leaving
treatment areas

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 53/105
Masks, Protective Eyewear, FaceShields
� Wear a surgical mask and either eye
protection with solid side shields or a face
shield to protect mucous membranes of
the eyes, nose, and mouth
� Change masks between patients
� Clean reusable face protection between
patients; if visibly soiled, clean and
disinfect

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 54/105
Protective Clothing
� Wear gowns, lab coats, or uniforms that cover skinand personal clothing likely
to become soiled withblood, saliva, or infectiousmaterial
� Change if visibly soiled
� Remove all barriers beforeleaving the work area
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 55/105
Gloves
� Minimize the risk of health care personnel
acquiring infections from patients
� Prevent microbial flora from being
transmitted from health care personnel topatients
� Reduce contamination of the hands of
health care personnel by microbial flora that
can be transmitted from one patient toanother
� Are not a substitute for handwashing!

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 56/105
Recommendations for Gloving
� Wear gloves when contactwith blood, saliva, andmucous membranes is
possible� Remove gloves after
patient care
� Wear a new pair of glovesfor each patient

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 57/105
Recommendations for Gloving
Remove gloves that
are torn, cut or punctured
Do not wash, disinfector sterilize gloves for reuse

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 58/105
Sterilization and Disinfection
of Patient Care Items
Critical Instruments
Semi-critical Instruments
Non-critical Instruments andDevices

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 59/105
Critical Instruments
� Penetrate mucous membranes or
contact bone, the bloodstream, or
other normally sterile tissues (of the
mouth)
� Heat sterilize between uses or use
sterile single-use, disposable devices
� Examples include surgicalinstruments, scalpel blades,
periodontal scalers, and surgical
dental burs

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 60/105

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 61/105

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 62/105
Instrument Processing Area
� Use a designated processing area to
control quality and ensure safety
� Divide processing area into work areas
± Receiving, cleaning, and
decontamination
± Preparation and packaging
± Sterilization
± Storage

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 63/105
Automated Cleaning
� Ultrasonic cleaner
� Instrumentwasher
� Washer-
disinfector
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 64/105
Manual Cleaning
� Soak until ready to
clean
� Wear heavy-duty
utility gloves, mask,
eyewear, andprotective clothing

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 65/105
Preparation and Packaging
� Critical and semi-critical items thatwill be stored should be wrapped or placed in containers before heat
sterilization� Hinged instruments opened and
unlocked
� Place a chemical indicator inside thepack
� Wear heavy-duty, puncture-resistantutility gloves

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 66/105
Heat-Based Sterilization
� Steam under pressure
(autoclaving)
±Gravity displacement ±Pre-vacuum
� Dry heat
� Unsaturated chemical vapor

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 67/105
Liquid Chemical Sterilant / Disinfectants
� Only for heat-sensitive
critical and semi-critical
devices� Powerful, toxic chemicals
raise safety concerns
� Heat tolerant or disposable alternatives are
available
S

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 68/105
Sterilization MonitoringTypes of Indicators
� Mechanical ±Measure time, temperature, pressure
� Chemical
± Change in color when physical parameter isreached
� Biological (spore tests) ± Use biological spores to assess the
sterilization process directly
B. Steriothermophilus strips
Color coded strips

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 69/105
Environmental Infection
Control

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 70/105
Environmental Surfaces
� May become contaminated
� Not directly involved in infectious
disease transmission� Do not require as stringent
decontamination procedures

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 71/105
Clinical Contact Surfaces
Clinical contact
surfaces
High potential for
direct contamination
from spray or spatter
or by contact withDHCP¶s gloved hand
H k i S f

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 72/105
Housekeeping Surfaces
Housekeeping
surfaces
Do not come intocontact with
patients or devices
Limited risk of
disease
transmission
General Cleaning

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 73/105
General Cleaning
Recommendations
� Use barrier precautions
� Physical removal of microorganisms bycleaning is as important as the disinfection
process
� Follow manufacturer¶s instructions for proper use hospital disinfectants

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 74/105
Medical Waste
� Medical Waste: Not considered
infectious, thus can be discarded in
regular trash
� Regulated Medical Waste:Poses a potential risk of infection
during handling and disposal
Regulated Medical Waste

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 75/105
Regulated Medical Waste
Management
� Properly labeled containment
to prevent injuries and leakage
� Medical wastes are ³treated´ in
accordance with state and
local EPA regulations
� Processes for regulated waste
include autoclaving andincineration
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 76/105
WASTE CATEGORIES
1. Human anatomical waste
2. Microbiology/ biotechnology waste
3. Soiled waste
4. Waste sharps
5. Liquid waste
6. Discarded medicines and cytotoxic
drugs7. Incineration ash
8. Chemical waste
WASTE MANAGEMENT
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 77/105
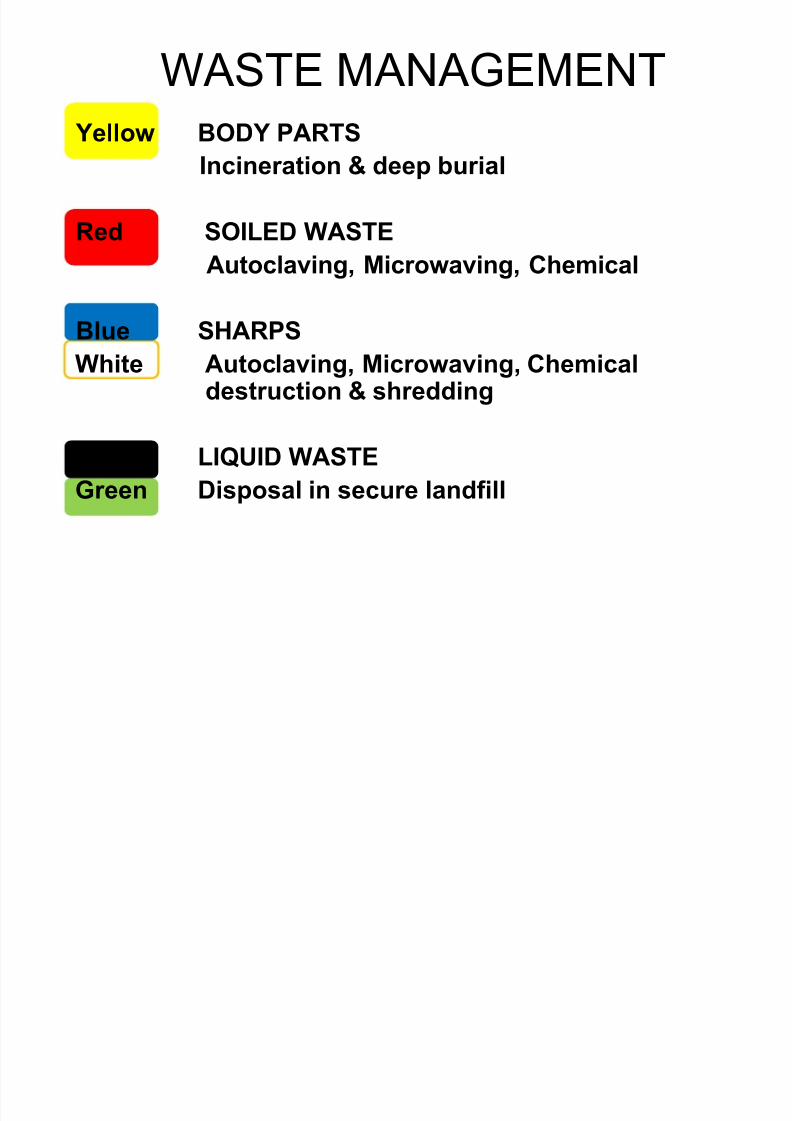
W ASTE M ANAGEMENT
Yellow BOD Y PARTS
Incineration & deep burial
Red SOILED WASTE
Autoclaving, Microwaving, Chemical
Blue SHARPS
White Autoclaving, Microwaving, Chemicaldestruction & shredding
Black LIQUID WASTE
Green Disposal in secure landfill

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 78/105
Dental Unit Waterlines,
Biofilm,
and Water Quality
D t l U it W t li

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 79/105
Dental Unit Waterlines
and Biofilm
� Microbial biofilms form
in small bore tubing of
dental units
� Biofilms serve as a
microbial reservoir
� Primary source of
microorganisms ismunicipal water
supply
D t l U it W t Q lit

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 80/105
Dental Unit Water Quality
� Using water of uncertain quality is
inconsistent with infection control
principles
� Colony counts in water from untreated
systems can exceed 1,000,000
CFU/mL
CFU=colony forming unit
� Untreated dental units cannot reliably
produce water that meets drinking
water standards
A il bl DUWL T h l
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 81/105
Available DUWL Technology
� Independent reservoirs
� Chemical treatment
� Filtration� Combinations
� Sterile water delivery systems
St il I i ti S l ti

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 82/105
Sterile Irrigating Solutions
� Use sterile saline or sterile
water as a coolant/irrigator
when performing surgicalprocedures
� Use devices designed for
the delivery of sterileirrigating fluids

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 83/105
Dental Handpieces and Other Devices
Attached to Air and Waterlines
� Clean and heat sterilize intraoraldevices that can be removed from
air and waterlines� Follow manufacturer¶s instructions
for cleaning, lubrication, and
sterilization� Do not use liquid germicides or
ethylene oxide
Components of Devices Permanently

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 84/105
Components of Devices Permanently
Attached to Air and Waterlines
� Do not enter patient¶s mouth butmay become contaminated
� Use barriers and changebetween uses
� Clean and intermediate-level
disinfect the surface of devices if visibly contaminated

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 85/105
Saliva Ejectors
� Previously suctioned
fluids might be retracted
into the patient¶s mouth
when a seal is created
� Do not advise patients to
close their lips tightly
around the tip of thesaliva ejector
D t l R di l
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 86/105
Dental Radiology
� Wear gloves and other appropriate
personal protective equipment as
necessary
� Heat sterilize heat-tolerantradiographic accessories
� Transport and handle exposed
radiographs so that they will notbecome contaminated
� Avoid contamination of developing
equipment

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 87/105
Precautions for ParenteralMedications
� IV tubings, bags,connections, needles, andsyringes are single-use,
disposable� Single dose vials
±Do not administer tomultiple patients even if
the needle on the syringeis changed
±Do not combine leftover contents for later use

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 88/105
Single-Use (Disposable) Devices
� Intended for use on one patient during a
single procedure
� Usually not heat-tolerant� Cannot be reliably cleaned
� Examples: Syringe needles, prophylaxis
cups, and plastic orthodontic brackets
P d l M th Ri

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 89/105
Pre-procedural Mouth Rinses
� Antimicrobial mouth rinses prior to a
dental procedure
±Reduce number of microorganisms inaerosols/spatter
±Decrease the number of microorganisms
introduced into the bloodstream
� Unresolved issue±no evidence that
infections are prevented
O l S i l P d

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 90/105
Oral Surgical Procedures
� Present a risk for microorganisms toenter the body
� Involve the incision, excision, or reflection of tissue that exposesnormally sterile areas of the oral cavity

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 91/105
Precautions for Surgical Procedures
Sterile IrrigatingSolutions
Sterile Surgeon¶sGloves
Surgical
Scrub

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 92/105
Handling Biopsy Specimens
� Place biopsy in sturdy,
leakproof container
� Avoid contaminating
the outside of the
container
� Label with a biohazard
symbol
E t t d T th

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 93/105
� Considered regulatedmedical waste
±Do not incinerate extracted teeth
containing amalgam ±Clean and disinfect before
sending to lab for shadecomparison
� Can be given back topatient
Extracted Teeth
Handling Extracted Teeth

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 94/105
Handling Extracted Teeth
in Educational Settings
� Remove visible blood and debris
� Maintain hydration
� Autoclave (teeth with no
amalgam)
�
Use Standard Precautions
Laser/Electrosurgery Plumes and

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 95/105
Laser/Electrosurgery Plumes and
Surgical Smoke
� Destruction of tissue creates smoke
that may contain harmful by-products
�
Infectious materials (HSV, HPV) maycontact mucous membranes of nose
� No evidence of HIV/HBV transmission
� Need further studies
8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 96/105
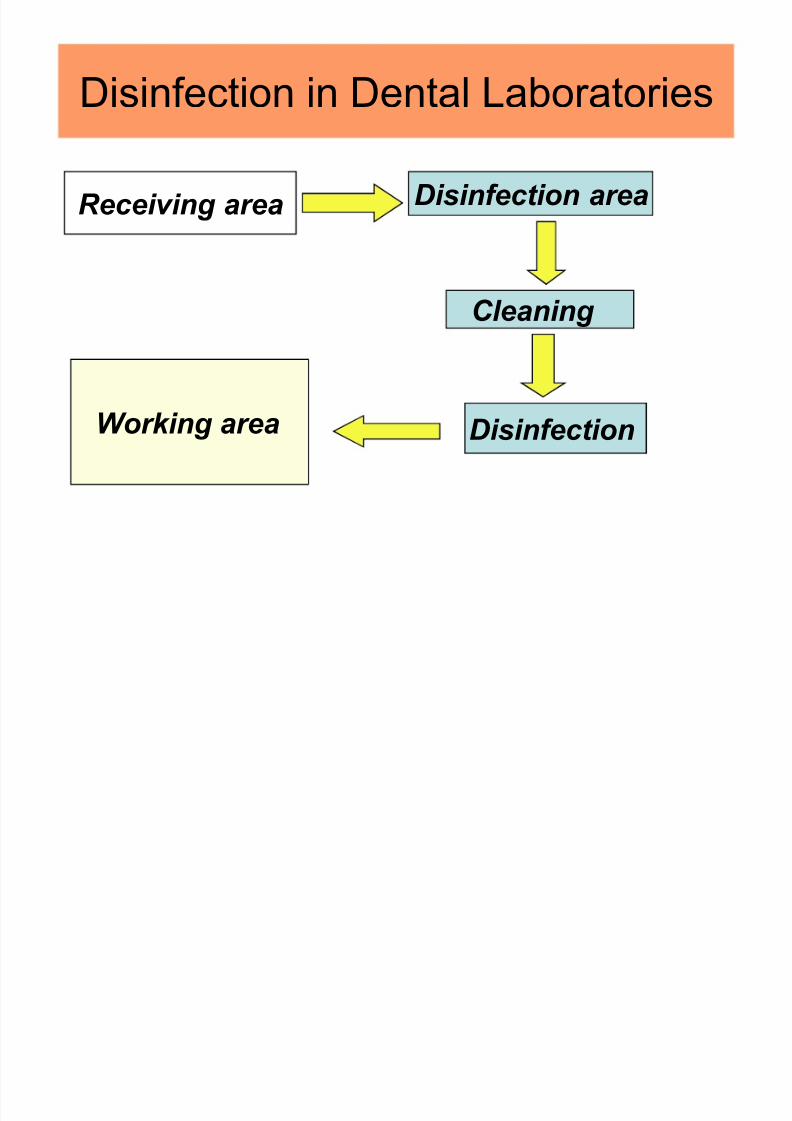
Disinfection in Dental Laboratories
Receiving area Disinfection area
Cleaning
DisinfectionWorking area
Recommended methods of

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 97/105
Recommended methods of
decontamination
Alginate, Zinc oxide eugenol paste, Zinc
oxide, eugenol paste, Stone casts ±
0.1% Sodium hypochlorite
Dentures, Wax bite block or Wafer-
Immerse in 0.1 % Sodium Hypochlorite
DENTAL LABORATORY

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 98/105
DENTAL LABORATORY
� All disinfection procedures are
accomplished prior to delivery to lab ± Done in dental operatory or professional work
area
�³O
nly Biologically Clean Items Permitted´ � Incoming :
1. Rinse under running tap water toremove blood/saliva
2. Disinfect as appropriate
3. Rinse thoroughly with tap water toremove residual disinfectant

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 99/105
Outgoing :
1. Clean and disinfect before
delivery to patient
2. After disinfection: rinse and
place in plastic bag with diluted
mouthwash until insertion
3. Do not store in disinfectant
before insertion
Metals

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 100/105
Metals
� Heat sterilize all metal and heat-stableinstruments that contact oral tissues,contaminated appliances, or potentiallycontaminated appliances should be heatsterilized after each use ± Facebow fork, metal impression trays, burs,
polishing points, rag wheels, laboratory knives
� For porcelain restorations that arecharacterized intraorally
± Take them directly to porcelainfurnace
± Sintering process sterilizesrestoration
SO G S

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 101/105
PERSONAL HYGIENE IN LABS
� Refrain from the following activities while in the
lab where there is potential for occupational
exposure:
± Eating ± Drinking
± Smoking
± Applying cosmetics or lip balm
± Handling contact lenses
I f ti C t l P G l

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 102/105
Infection Control Program Goals
� Provide a safe
working environment
±Reduce health care-associated infections
±Reduce occupational
exposures
Program Evaluation

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 103/105
Program Evaluation
� Strategies and Tools
± Periodic observational
assessments
± Checklists to documentprocedures
± Routine review of
occupational exposures
to bloodbornepathogens

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 104/105
³P rogram evaluation providesan opportunity to identify and
change inappropriate
practices, thereby improving
the effectiveness of your
infection control program.´

8/6/2019 sdo - inf cntrl
http://slidepdf.com/reader/full/sdo-inf-cntrl 105/105
Queries Queries Queries